Quick Compendium of CP: Chemistry Enzymes, Serum Proteins, Acid-Base and Electrolytes ZW 7/7/08.
101
Quick Compendium of Quick Compendium of CP: Chemistry CP: Chemistry Enzymes, Serum Enzymes, Serum Proteins, Acid-Base Proteins, Acid-Base and Electrolytes and Electrolytes ZW 7/7/08 ZW 7/7/08
-
Upload
zain-pullins -
Category
Documents
-
view
233 -
download
0
Transcript of Quick Compendium of CP: Chemistry Enzymes, Serum Proteins, Acid-Base and Electrolytes ZW 7/7/08.

Quick Compendium of CP: Quick Compendium of CP: ChemistryChemistry
Enzymes, Serum Proteins, Enzymes, Serum Proteins, Acid-Base and ElectrolytesAcid-Base and Electrolytes
ZW 7/7/08ZW 7/7/08

Enzymes: BasicsEnzymes: Basics
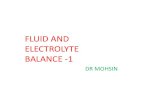
Michaelis-Menton kinetics: Michaelis-Menton kinetics: – The rate of enzyme activity varies linearly with The rate of enzyme activity varies linearly with
substrate concentration up to the point that substrate concentration up to the point that the enzyme is fully saturated with substratethe enzyme is fully saturated with substrate
– At this point, enzyme working as fast as it can At this point, enzyme working as fast as it can (Vmax)(Vmax)
– Rate of reaction at this point varies only with Rate of reaction at this point varies only with enzyme concentrationenzyme concentration

Michaelis-Menton KineticsMichaelis-Menton Kinetics

EnzymesEnzymes
Can measure enzyme concentration by:Can measure enzyme concentration by:– Using excess of substrateUsing excess of substrate– Or, measure whether a reaction has taken Or, measure whether a reaction has taken
placeplaceMeasure reaction productsMeasure reaction products
NAD to NADH to NAD (NADH absorbs light at NAD to NADH to NAD (NADH absorbs light at 340nm, NAD does not)340nm, NAD does not)

Coupled Enzyme Assay Coupled Enzyme Assay (NAD/NADH)(NAD/NADH)
Aspartate (Asp) + Aspartate (Asp) + -ketoglutarate -ketoglutarate oxaloacetate (OAA) + glutamateoxaloacetate (OAA) + glutamate– Does not utilize NADHDoes not utilize NADH
Aspartate (Asp) + Aspartate (Asp) + -ketoglutarate -ketoglutarate oxaloacetate (OAA) + glutamate + NADH oxaloacetate (OAA) + glutamate + NADH malate + NADmalate + NAD– Add excess NADH and Add excess NADH and KG, along with catalysts KG, along with catalysts
AST and MD AST and MD – The disappearance of NADH (absorbance at 340nm) The disappearance of NADH (absorbance at 340nm)
can be used as a reflection of AST (enzyme at first can be used as a reflection of AST (enzyme at first arrow)arrow)

Measurement of Enzyme AntigenMeasurement of Enzyme Antigen
The quantity of enzyme determined by The quantity of enzyme determined by immunoassay corresponds to the enzyme immunoassay corresponds to the enzyme ACTIVITYACTIVITY
Discordance between concentration and Discordance between concentration and ACTIVITY usually takes the form of the immuno ACTIVITY usually takes the form of the immuno assay overestimating the activityassay overestimating the activity– May be due to serum enzyme inhibitorsMay be due to serum enzyme inhibitors– Deficiency in necessary cofactorDeficiency in necessary cofactor– Defective enzymeDefective enzyme– Proteolytically inactivated enzymesProteolytically inactivated enzymes

Cofactors, CoenzymesCofactors, Coenzymes
Cofactors:Cofactors:– Substances that bind to an enzyme and Substances that bind to an enzyme and
enhance activityenhance activity– Include inorgantic cofactors like zinc, calcium, Include inorgantic cofactors like zinc, calcium,
magnesium, ironmagnesium, iron– Organic: also called coenzymesOrganic: also called coenzymes
Coenzymes:Coenzymes:– Organic cofactors, include NAD, protein S, Organic cofactors, include NAD, protein S,
pyridoxine (vit B6)pyridoxine (vit B6)

MacroenzymesMacroenzymes
Ordinary enzymes bound to antibodiesOrdinary enzymes bound to antibodies
Has 2 effects:Has 2 effects:– Makes it incapable of functioningMakes it incapable of functioning– Prevents it from being cleared from bloodPrevents it from being cleared from blood

Competitive INHIBITIONCompetitive INHIBITION

Non-competitive InhibitionNon-competitive Inhibition

Uncompetitive InhibitionUncompetitive Inhibition

Enzyme UnitsEnzyme Units
International Unit (IU):International Unit (IU):– The amount of enzyme that catalyzes the The amount of enzyme that catalyzes the
conversion of 1 micromole of substrate per conversion of 1 micromole of substrate per minuteminute
KatalKatal– 1 katal= the amount of enzyme that catalyzes 1 katal= the amount of enzyme that catalyzes
the conversion of 1 Mole of substrate per the conversion of 1 Mole of substrate per secondsecond
– 1IU = 16.7 katals1IU = 16.7 katals

Hepatic EnzymesHepatic Enzymes
Liver transaminasesLiver transaminases– AST and ALTAST and ALT– ASTAST
Cardiac muscle, liver, skeletal muscle, kidney, brain, lung, Cardiac muscle, liver, skeletal muscle, kidney, brain, lung, pancreas (in descending order)pancreas (in descending order)
Found within cytoplasm (20%)and mitochondria (80%)Found within cytoplasm (20%)and mitochondria (80%)
– ALTALTMORE SPECIFIC FOR LIVER, confined to liver and kidneyMORE SPECIFIC FOR LIVER, confined to liver and kidney
Found entirely within cytoplasmFound entirely within cytoplasm

Hepatic EnzymesHepatic Enzymes
In childrenIn children– AST activity is slightly higher than ALTAST activity is slightly higher than ALT– Pattern reverses at age 20Pattern reverses at age 20– In adults, AST activity a little lower than ALTIn adults, AST activity a little lower than ALT– May reverse with old ageMay reverse with old age
Both AST/ALT activities higher in adult Both AST/ALT activities higher in adult males over females, and in African-males over females, and in African-AmericansAmericansHemolysis raises AST/ALTHemolysis raises AST/ALT

Hepatic EnzymesHepatic Enzymes
Intra-individual variation more significant Intra-individual variation more significant for ALT than ASTfor ALT than AST– Marked diurnal variation (highest in afternoon) Marked diurnal variation (highest in afternoon)
and day-to-day variation up to 30%and day-to-day variation up to 30%
Both AST/ALT elevated in heparin therapy Both AST/ALT elevated in heparin therapy to around 3X baselineto around 3X baseline
In renal failure, both significantly lower In renal failure, both significantly lower than in healthy individualsthan in healthy individuals

Hepatic EnzymesHepatic Enzymes
Lactate dehydrogenase (LDH):Lactate dehydrogenase (LDH):– Present in numerous tissues, traditionally separated Present in numerous tissues, traditionally separated
into 5 isoenzymes by electrophoresisinto 5 isoenzymes by electrophoresis– Fastest moving are LD1 and LD2Fastest moving are LD1 and LD2
Found in heart, RBC, kidneyFound in heart, RBC, kidney
– Slower moving are LD4 and LD5Slower moving are LD4 and LD5LIVER and skeletal muscleLIVER and skeletal muscle
– LD3 in lung, spleen, lymphocytes, and pancreasLD3 in lung, spleen, lymphocytes, and pancreas– LD6- “sixth” LD is sometimes seen migrating cathodal LD6- “sixth” LD is sometimes seen migrating cathodal
to LD5to LD5PRESENCE THOUGHT TO BE A DIRE FINDING (hepatic PRESENCE THOUGHT TO BE A DIRE FINDING (hepatic insufficiency in setting of cardiovascular collapse)insufficiency in setting of cardiovascular collapse)

LDHLDH
Concentrations:Concentrations:– LD2>LD1>LD3>LD4>LD5LD2>LD1>LD3>LD4>LD5– LD 1 elevation (with flipped LD ratio LD1>LD2):LD 1 elevation (with flipped LD ratio LD1>LD2):
Acute MIAcute MI
HemolysisHemolysis
Renal infarctionRenal infarction
– Elevated LD4 and LD5:Elevated LD4 and LD5:LIVER DAMAGE or skeletal insultLIVER DAMAGE or skeletal insult
– Elevated LD1 and LD5:Elevated LD1 and LD5:Acute MI with liver congestionAcute MI with liver congestion
Chronic alcoholismChronic alcoholism

Alkaline phosphataseAlkaline phosphatase
Two types of phosphatases:Two types of phosphatases:– Alkaline (optimum pH is 9):Alkaline (optimum pH is 9):
Bone, bile ducts, intestine, placentaBone, bile ducts, intestine, placenta
Separate reference ranges for women and childrenSeparate reference ranges for women and children
– Acid (optimum pH is 5):Acid (optimum pH is 5):Found in prostate, RBC, and boneFound in prostate, RBC, and bone
RBC acid phosphatase is susceptible to inhibition RBC acid phosphatase is susceptible to inhibition by 2% formaldehyde and resistance to inhibition by by 2% formaldehyde and resistance to inhibition by tartrate (this is also seen in hairy cell leukemia)tartrate (this is also seen in hairy cell leukemia)

Alkaline phosphataseAlkaline phosphatase
4 isoenzymes by electrophoresis:4 isoenzymes by electrophoresis:– Each displays characteristic degrees of Each displays characteristic degrees of
inactivation by heating, urea incubation, and l-inactivation by heating, urea incubation, and l-phenylalaninephenylalanine
– Heating produces significant inactivation of Heating produces significant inactivation of bone alk phos (bone burns), 50% inactivation bone alk phos (bone burns), 50% inactivation of biliary alk phos, and NO inactivation of of biliary alk phos, and NO inactivation of placental alk phos.placental alk phos.

Alkaline phosphataseAlkaline phosphatase
Biliary alk phos: Biliary alk phos: – Most sensitive marker of hepatic metastasesMost sensitive marker of hepatic metastases
Bone alk phos:Bone alk phos:– Produced by osteoBLASTS and reflects bone Produced by osteoBLASTS and reflects bone
reforming activityreforming activity– Highest levels seen in Paget’s disease of Highest levels seen in Paget’s disease of
bonebone– A specific immunoassay for bone alk phos A specific immunoassay for bone alk phos
availableavailable

Regan IsoenzymeRegan Isoenzyme
Observed in about 5% of individuals with Observed in about 5% of individuals with carcinomacarcinoma– Appears identical to placental alkaline Appears identical to placental alkaline
phosphatasephosphatase

Intestinal Alk PhosIntestinal Alk Phos
ElevationElevation– Can be factitious in non-fasting individuals, Can be factitious in non-fasting individuals,
particularly in Lewis positive type B or O ptsparticularly in Lewis positive type B or O pts– Ingesting a meal can elevate alk phos by 30% Ingesting a meal can elevate alk phos by 30%
in 2-12 hoursin 2-12 hours– Repeat fasting alk phosRepeat fasting alk phos

Alk PhosAlk Phos
Minor elevations are a common clinical Minor elevations are a common clinical problemproblem– Usually higher in men than womenUsually higher in men than women– Higher in African-AmericansHigher in African-Americans– Threshold of 1.5 times normal limit for further Threshold of 1.5 times normal limit for further
investigation (repeat in 6 months if borderline)investigation (repeat in 6 months if borderline)– Causes:Causes:
Pregnancy, CHF, hyperthyroidism, drugsPregnancy, CHF, hyperthyroidism, drugs

Alkaline phosphataseAlkaline phosphatase
Sensitive indicator for hepatic metastasesSensitive indicator for hepatic metastases
In women, investigation should include In women, investigation should include assay for anti-mitochondrial antibodiesassay for anti-mitochondrial antibodies

Gamma-glutamyl transferase Gamma-glutamyl transferase (GGT)(GGT)
GGT: GGT: – best test to confirm if elevate alk phos if of best test to confirm if elevate alk phos if of
biliary tree originbiliary tree origin– Found in biliary epithelial cell, particularly Found in biliary epithelial cell, particularly
those of the small interlobular bile ducts and those of the small interlobular bile ducts and ductulesductules
– Exquisitely sensitive to biliary injuryExquisitely sensitive to biliary injury– Also elevated in:Also elevated in:
Steatosis, diabetes, hyperthyroidism, RA, acute Steatosis, diabetes, hyperthyroidism, RA, acute MI, COPDMI, COPD

GGTGGT
Present within the smooth endoplasmic Present within the smooth endoplasmic reticulum of hepatocytesreticulum of hepatocytes– Whenever there is induction due to excess Whenever there is induction due to excess
toxin, GGT levels increasetoxin, GGT levels increase– This includes warfarin, barbiturates, dilantin, This includes warfarin, barbiturates, dilantin,
valproic acid, methotrexate, EtOHvalproic acid, methotrexate, EtOH– 2-3X normal limit in heavy drinkers2-3X normal limit in heavy drinkers– Returns to normal after 3 weeks abstinence Returns to normal after 3 weeks abstinence
and can be followed as marker for alcohol and can be followed as marker for alcohol consumptionconsumption

5’ Nucleotidase5’ Nucleotidase
Main source is biliary epitheliumMain source is biliary epithelium
Levels highest in cholestatic conditionsLevels highest in cholestatic conditions
Another test to confirm if elevated alk phos Another test to confirm if elevated alk phos is due to hepatobiliary diseaseis due to hepatobiliary disease
Low sensitivity, best as confirmatory test, Low sensitivity, best as confirmatory test, utility less than GGTutility less than GGT

AmmoniaAmmonia
Hyperammonemia nearly always due to liver Hyperammonemia nearly always due to liver failurefailure
In children, it should raise the suspicion for an In children, it should raise the suspicion for an INBORN ERROR IN METABOLISMINBORN ERROR IN METABOLISM
Sources of ammonia:Sources of ammonia:– Skeletal muscle and gutSkeletal muscle and gut
Bacteria in GI tract produce ammoniaBacteria in GI tract produce ammonia
– Normally functioning liver removes this ammonia and Normally functioning liver removes this ammonia and discards it in the form of urea which is excreted in discards it in the form of urea which is excreted in urineurine

AmmoniaAmmonia
Blood ammonia can become disastrously Blood ammonia can become disastrously high when:high when:– Too much collateral circulationToo much collateral circulation– Excess protein in gut (excess hemoglobin Excess protein in gut (excess hemoglobin
from variceal bleed)from variceal bleed)– SIGNIFICANT HEPATOCYTE DISFUNCTIONSIGNIFICANT HEPATOCYTE DISFUNCTION
In cirrhotic patients, these conditions are In cirrhotic patients, these conditions are often met, and neurotoxicity can resultoften met, and neurotoxicity can result

AMMONIAAMMONIA
Measurement requires a FRESH Measurement requires a FRESH specimen which has been CHILLED specimen which has been CHILLED during transport and has undergone NO during transport and has undergone NO hemolysishemolysisSmoking patients must abstain for several Smoking patients must abstain for several hours before drawhours before drawAnyone care to comment on the current Anyone care to comment on the current state of the ammonia level as it can or state of the ammonia level as it can or cannot be ordered?cannot be ordered?

BilirubinBilirubin
Unconjugated (indirect) bilirubin:Unconjugated (indirect) bilirubin:– Water-insoluble form produced by breakdown Water-insoluble form produced by breakdown
of hemeof heme– Taken to liver tightly bound to albumin where Taken to liver tightly bound to albumin where
it under goes glucuronidation to produce it under goes glucuronidation to produce water-soluble (as in bile) conjugated (direct) water-soluble (as in bile) conjugated (direct) bilirubinbilirubin
– Conjugated bili excreted in bile where Conjugated bili excreted in bile where intestinal bacteria convert to urobilinogen intestinal bacteria convert to urobilinogen

BilirubinBilirubin
Urobilinogen ends up in feces, some of Urobilinogen ends up in feces, some of which is reabsorbed and excreted in urinewhich is reabsorbed and excreted in urine
Some urobilinogen is converted by colonic Some urobilinogen is converted by colonic bacteria into brown pigments (complete bacteria into brown pigments (complete biliary obstruction leads to yellow-white biliary obstruction leads to yellow-white stool- stool- the Silver Stool of Thompson)the Silver Stool of Thompson)

BilirubinBilirubin
Unconjugated bilirubin, even when it is quite high, does Unconjugated bilirubin, even when it is quite high, does NOT appear in urineNOT appear in urine– Thus, bilirubinuria indicates CONJUGATED hyperbilirubinemiaThus, bilirubinuria indicates CONJUGATED hyperbilirubinemia
2 test methods2 test methods– Diazo-colorimetric methods:Diazo-colorimetric methods:
Rely on formation of colored dye through reaction of bili with diazo Rely on formation of colored dye through reaction of bili with diazo compoundcompoundWithout the addition of an accelerator (alcohol), only conjugated Without the addition of an accelerator (alcohol), only conjugated bilirubin is measuredbilirubin is measuredAddition of accelerators measures combined unconj and conjugated Addition of accelerators measures combined unconj and conjugated (total) bilirubin(total) bilirubin
– Direct spectrophotometryDirect spectrophotometryBilirubin concentration measured by absorbance (455nm) Bilirubin concentration measured by absorbance (455nm)

Causes of HyperbilirubinemiaCauses of Hyperbilirubinemia
Unconjugated:Unconjugated:– Hemolysis (extravascular)Hemolysis (extravascular)– Blood shunting (cirrhosis)Blood shunting (cirrhosis)– Right heart failureRight heart failure– Gilbert syndromeGilbert syndrome– Drugs: rifampinDrugs: rifampin– Crigler-Najjar syndromeCrigler-Najjar syndrome– HypothyroidismHypothyroidism

Causes of HyperbilirubinemiaCauses of Hyperbilirubinemia
Conjugated:Conjugated:– Dubin-Johnson syndromeDubin-Johnson syndrome– HepatitisHepatitis– Endotoxin (sepsis)Endotoxin (sepsis)– Pregnancy (estrogen)Pregnancy (estrogen)– Drugs: estrogen, cyclosporineDrugs: estrogen, cyclosporine– Mechanical obstruction:Mechanical obstruction:
PBC, PSC, tumor, stricture, stonePBC, PSC, tumor, stricture, stone

Additional Hepatic Function TestsAdditional Hepatic Function Tests
PT:PT:– Factor VII has half life of 12 hours (ON RISE EXAM)Factor VII has half life of 12 hours (ON RISE EXAM)– Sensitive marker for impaired hepatic synthetic Sensitive marker for impaired hepatic synthetic
functionfunction– Impaired bile secretion can lead to Vit K deficiency Impaired bile secretion can lead to Vit K deficiency
(bile salts required for absorption)(bile salts required for absorption)– How do you distinguish between a prolonged PT How do you distinguish between a prolonged PT
because of cholestasis/impaired Vit K absorption and because of cholestasis/impaired Vit K absorption and hepatocyte injury?hepatocyte injury?
Add parental vit KAdd parental vit K
GammaglobulinsGammaglobulins– Serum gammaglobulins elevated in liver injury, Serum gammaglobulins elevated in liver injury,
especially autoimmuneespecially autoimmune

Neonatal Jaundice Neonatal Jaundice
Most cases of neonatal jaundice are Most cases of neonatal jaundice are entirely benign (“physiologic jaundice”)entirely benign (“physiologic jaundice”)– Hepatic enzymes not yet at full capacity Hepatic enzymes not yet at full capacity
leading to build-up of unconjugated bilirubinleading to build-up of unconjugated bilirubin– Usually noted between days 2-3 of neonatal Usually noted between days 2-3 of neonatal
lifelife– Usually peaks at 4-5 days; rarely exceeds 5-6 Usually peaks at 4-5 days; rarely exceeds 5-6
mg/dLmg/dL

Severe hyperbilirubinemia in Severe hyperbilirubinemia in neonatesneonates
Most common causes:Most common causes:– Hemolytic disease of the newborn (HDN)Hemolytic disease of the newborn (HDN)– SepsisSepsis
Poorly developed blood-brain barrier Poorly developed blood-brain barrier causes unconjugated bili to pass to CNS causes unconjugated bili to pass to CNS and cause damage (kernicterus)and cause damage (kernicterus)

When to worry about neonatal When to worry about neonatal jaundice?jaundice?
Appearance in first 24 hours of lifeAppearance in first 24 hours of life
Rising bili beyond 1 weekRising bili beyond 1 week
Persistance of jaundice past 10 daysPersistance of jaundice past 10 days
Total bili that exceeds 12 mg/dLTotal bili that exceeds 12 mg/dL
Single-day increase of >5 mg/dLSingle-day increase of >5 mg/dL
Conjugated bili (direct) that exceeds 2 Conjugated bili (direct) that exceeds 2 mg/dLmg/dL

Therapy for neonatal jaundiceTherapy for neonatal jaundice
Phototherapy:Phototherapy:– Consider when bili exceeds 10 mg/dL before Consider when bili exceeds 10 mg/dL before
12 hours of age; 12 mg/dL before 18 hours of 12 hours of age; 12 mg/dL before 18 hours of age; 14 mg/dL before 24 hours of ageage; 14 mg/dL before 24 hours of age
– Phototherapy converts unconj bili to a Phototherapy converts unconj bili to a molecule that can be excreted WITHOUT conjmolecule that can be excreted WITHOUT conj
– Not useful for conj hyperbiliNot useful for conj hyperbili
Exchange transfusion:Exchange transfusion:– When bili exceeds 20 mg/dLWhen bili exceeds 20 mg/dL

DDX of neonate hyperbiliDDX of neonate hyperbiliJaundice in 1Jaundice in 1stst 24 hours: 24 hours:– Erythroblastosis fetalisErythroblastosis fetalis– Concealed hemorrhageConcealed hemorrhage– SepsisSepsis– TORCH infectionTORCH infection
Jaundice between 3Jaundice between 3rdrd and 7 and 7thth day: day:– Bacterial sepsis (usually UTI origin)Bacterial sepsis (usually UTI origin)
Arising after 1Arising after 1stst week: week:– Breast milk jaundice, sepsis, extrahepatic biliary Breast milk jaundice, sepsis, extrahepatic biliary
atresia, cystic fibrosis, congenital paucity of bile ducts atresia, cystic fibrosis, congenital paucity of bile ducts (Alagille syndrome), neonatal hepatitis, glactosemia, (Alagille syndrome), neonatal hepatitis, glactosemia, inherited hemolytic anemia (PK def, hered. inherited hemolytic anemia (PK def, hered. Spherocytosis, G6PD def)Spherocytosis, G6PD def)

Lab Eval of Acute Liver InjuryLab Eval of Acute Liver Injury
May be symptomatic, Jaundice, Elevated May be symptomatic, Jaundice, Elevated transaminasestransaminasesMay be due to viral hepatitis (HAV, HBV, May be due to viral hepatitis (HAV, HBV, HCV), autoimmune hep, toxin, drug, HCV), autoimmune hep, toxin, drug, ischemia, or Wilson diseaseischemia, or Wilson diseaseLabs:Labs:– Hepatitis serologies, ANA, ceruloplasmin, Hepatitis serologies, ANA, ceruloplasmin,
clinical history (new drugs usually cause clinical history (new drugs usually cause damage within 4 months of starting)damage within 4 months of starting)

Acute liver injury labsAcute liver injury labs
Acute viral hepatitis due to HAV, HBV most often Acute viral hepatitis due to HAV, HBV most often leads to complete recoveryleads to complete recoveryAcute HCV goes to chronic HCV in >80% of Acute HCV goes to chronic HCV in >80% of casescasesSerologic testing for HAV, HBV are very Serologic testing for HAV, HBV are very dependable for diagnosing acute infx (IgM anti-dependable for diagnosing acute infx (IgM anti-HAV, IgM anti-HBc, HBsAg)HAV, IgM anti-HBc, HBsAg)Anti-HCV test only about 60% sensitive for acute Anti-HCV test only about 60% sensitive for acute infxinfxHCV RNA testing 90-95% sensitiveHCV RNA testing 90-95% sensitive

TransaminasesTransaminases
Acute hepatic injury due to ischemic or toxic Acute hepatic injury due to ischemic or toxic injury produce PROFOUND elevations in injury produce PROFOUND elevations in transaminases- often >100X upper limit of transaminases- often >100X upper limit of normal (RARE in acute hepatitis)normal (RARE in acute hepatitis)AST > 3,000 U/L = toxin in 90% of casesAST > 3,000 U/L = toxin in 90% of casesAST 10X upper limit of normal in acute viral AST 10X upper limit of normal in acute viral hepatitis, but reaches this level RARELY in hepatitis, but reaches this level RARELY in alcoholic hepatitisalcoholic hepatitisAST:ALT ratio is over 2 in 80% of pts with toxic, AST:ALT ratio is over 2 in 80% of pts with toxic, ischemic, and EtOH hepatitis (<1 in viral hep)ischemic, and EtOH hepatitis (<1 in viral hep)Amount of transam elevation poorly correlates Amount of transam elevation poorly correlates with LEVEL of injurywith LEVEL of injury

PT/BILIRUBINPT/BILIRUBIN
PT (protime)- PT (protime)- – Probably the best indicator of prognosis in acute Probably the best indicator of prognosis in acute
hepatic injuryhepatic injury– >4.0 secs indicates severe injury/unfav prog>4.0 secs indicates severe injury/unfav prog
BILIBILI– Jaundice in 70% of pts with EtOH, HAVJaundice in 70% of pts with EtOH, HAV– Jaundice in <20% of pts with HBV, HCVJaundice in <20% of pts with HBV, HCV– Jaundice rare in kids with acute viral hep, rare in toxic Jaundice rare in kids with acute viral hep, rare in toxic
or ischemic injuryor ischemic injury– >15 mg/dL indicates severe liver injury, bad prognosis>15 mg/dL indicates severe liver injury, bad prognosis

Pancreatic EnzymesPancreatic Enzymes
AMYLASE:AMYLASE:– Serum amylase = salivary and pancreatic Serum amylase = salivary and pancreatic
isoenzymesisoenzymes– On electrophoresisOn electrophoresis 6 bands result 6 bands result
11stst three are salivary three are salivary
Slower 3 are pancreaticSlower 3 are pancreatic
– Can be separated by inhibition as wellCan be separated by inhibition as wellSalivary amylase sensitive to inhibition by wheat Salivary amylase sensitive to inhibition by wheat germ lectin (germ lectin (treticum vulgaristreticum vulgaris))
– Assays based on monoclonal Abs directed Assays based on monoclonal Abs directed against specific isoenzymes are very accurateagainst specific isoenzymes are very accurate

Serum AmylaseSerum Amylase
Rises within 2-24 hours of onset of acute Rises within 2-24 hours of onset of acute pancreatitispancreatitis
Returns to normal in 2-3 daysReturns to normal in 2-3 days
Higher levels don’t correlate with severityHigher levels don’t correlate with severity
Higher levels are more specific for acute Higher levels are more specific for acute pancreatitispancreatitis
Persistance in elevation suggests Persistance in elevation suggests complication like pseudocystcomplication like pseudocyst

Urine amylaseUrine amylase
Nearly all pts have concomitant increase Nearly all pts have concomitant increase in urine amylasein urine amylase
Amylase primarily cleared by glomeruliAmylase primarily cleared by glomeruli– Renal insufficiency = spurious amylase Renal insufficiency = spurious amylase
elevationelevation
Fractional excretion of compound (x) = FEFractional excretion of compound (x) = FExx

AmylaseAmylase
Sensitivity of serum amylase for acute Sensitivity of serum amylase for acute pancreatitis is 90-98%pancreatitis is 90-98%
Specificity is only around 70-75%Specificity is only around 70-75%
Specificity of urine amylase and Specificity of urine amylase and FEamylase is higherFEamylase is higher

Additional causes of increased Additional causes of increased amylaseamylase
Diabetic ketoacidosis, peptic ulcer dz, Diabetic ketoacidosis, peptic ulcer dz, acute cholecystitis, ectopic pregnancy, acute cholecystitis, ectopic pregnancy, salpingitis, bowel ischemia, intestinal salpingitis, bowel ischemia, intestinal obstruction, macroamylasemia, and renal obstruction, macroamylasemia, and renal insufficiency, opioid analgesics insufficiency, opioid analgesics (contraction of sphincter of oddi)(contraction of sphincter of oddi)

Pancreatic EnzymesPancreatic Enzymes
LIPASE:LIPASE:– Unlike amylase, essentially specific for Unlike amylase, essentially specific for
pancreaspancreas– Rise parallels rise in amylase, but remains Rise parallels rise in amylase, but remains
elevated for 14 dayselevated for 14 days– Less reliant on renal clearance than amylaseLess reliant on renal clearance than amylase– Often considered superior to amylase in dx of Often considered superior to amylase in dx of
acute pancreatitisacute pancreatitis

Lab Eval for Acute PancreatitisLab Eval for Acute Pancreatitis
Amylase limited in sensitivity and specificityAmylase limited in sensitivity and specificity– Hypertriglyceridemia (common cause of acute Hypertriglyceridemia (common cause of acute
pancreatitis) interferes with amylase assay (false pancreatitis) interferes with amylase assay (false negative)negative)
Lipase remains elevated longer giving greater Lipase remains elevated longer giving greater sensitivitysensitivity
Others: trypsinogen-2 and elastase-1 (not used Others: trypsinogen-2 and elastase-1 (not used often) but have excellent negative predictive often) but have excellent negative predictive valuevalue

Acute Pancreatitis PrognosisAcute Pancreatitis Prognosis
Ranson Criteria:Ranson Criteria:– Aggressive managementAggressive management
ICU admissionICU admissionParenteral feedingParenteral feedingSystemic antibioticsSystemic antibiotics
– Provides specificity of 90%Provides specificity of 90%– Cannot be assigned until 48 hours after Cannot be assigned until 48 hours after
admissionadmission– Serum amylase/lipase are poor predictors of Serum amylase/lipase are poor predictors of
outcomeoutcome

Etiology of Acute PancreatitisEtiology of Acute Pancreatitis
StonesStones
EtOHEtOH
VirusesViruses
Inherited diseases:Inherited diseases:– Mutations in Mutations in
Cationic trypsinogen (PRSS-1)Cationic trypsinogen (PRSS-1)
Pancreatic secretory trypsin inhibitor (PSTI)Pancreatic secretory trypsin inhibitor (PSTI)
Cystic fibrosis transmembrane conductance Cystic fibrosis transmembrane conductance regulator (CFTR)regulator (CFTR)

Pancreatic EXOCRINE functionPancreatic EXOCRINE function
Tests include:Tests include:– Secretin-cholecystokinin (secretin CCK, Secretin-cholecystokinin (secretin CCK,
secretin pancreozymin), fecal elastase-1, secretin pancreozymin), fecal elastase-1, fecal fatfecal fat
– FECAL FAT:FECAL FAT:Oil-red O stain and 72 hour fecal fat quantOil-red O stain and 72 hour fecal fat quant
Stain has sensitivity of 70%Stain has sensitivity of 70%
Fecal fat quant quite sensitive for panc. Insuff.Fecal fat quant quite sensitive for panc. Insuff.

Myocardial EnzymesMyocardial Enzymes
CK (creatine kinase):CK (creatine kinase):– Three isoenzymes distinguishable by electrophoresisThree isoenzymes distinguishable by electrophoresis
CK-MM, CK-MB, CK-BBCK-MM, CK-MB, CK-BBFastest migrating is BB (CK1), then MB (CK2), then MM Fastest migrating is BB (CK1), then MB (CK2), then MM (CK3)(CK3)CK-BB: found primarily in brain, with lesser amounts in CK-BB: found primarily in brain, with lesser amounts in bladder, stomach, and prostate.bladder, stomach, and prostate.CK-MM (CK3) found in skeletal muscle and cardiac muscle CK-MM (CK3) found in skeletal muscle and cardiac muscle (Skel.muscle: 99% MM, cardiac: 70%MM). In normal (Skel.muscle: 99% MM, cardiac: 70%MM). In normal subjects, serum CK is 100% MMsubjects, serum CK is 100% MMCK-MB (CK2) found in cardiac and skeletal muscle (card: CK-MB (CK2) found in cardiac and skeletal muscle (card: 30%, skel: 1%), skeletal muscle is source of nearly all MB in 30%, skel: 1%), skeletal muscle is source of nearly all MB in circulation in serumcirculation in serum

CKCK
Now use immunoassays to measure CKNow use immunoassays to measure CK– Much faster and more accurate than Much faster and more accurate than
electrophoresis (particularly in low/clinical electrophoresis (particularly in low/clinical range)range)
– Total CKTotal CK enzymatic assay enzymatic assay– Ratio of CK-MB to total CK (RI: relative index) Ratio of CK-MB to total CK (RI: relative index)
adds to ability to distinguish MIadds to ability to distinguish MI– RI of 2% is usually cut-offRI of 2% is usually cut-off

Troponin ITroponin I
Group of enzymes consisting of Group of enzymes consisting of – Troponin T (TnT)Troponin T (TnT)– Troponin I (TnI)Troponin I (TnI)– Troponin C (TnC)Troponin C (TnC)
Involved in mediating the actin-myosin Involved in mediating the actin-myosin interactions that result in muscle interactions that result in muscle contractioncontraction
Immunoassays distinguish cardiac Immunoassays distinguish cardiac troponins (cTnI and cTnT) from skeletal troponins (cTnI and cTnT) from skeletal muscle troponinsmuscle troponins

TroponinTroponin
Vast majority of cardiac muscle troponin is Vast majority of cardiac muscle troponin is bound to actin/mysosinbound to actin/mysosin
Very small amount free in cytoplasmVery small amount free in cytoplasm
So:So:– Immediate release of cytoplasmic troponin in Immediate release of cytoplasmic troponin in
MI (4-8 hours)MI (4-8 hours)– And sustained release of bound troponin over And sustained release of bound troponin over
next 10-14 daysnext 10-14 days

Cardiac Troponin ICardiac Troponin I
Only cTnI is currently widely available for Only cTnI is currently widely available for use in clinical diagnosisuse in clinical diagnosis
cTnT marginally less cardiospecificcTnT marginally less cardiospecific
cTnI NOT elevated in skeletal muscle cTnI NOT elevated in skeletal muscle injuryinjury
cTnI may be elevated in other forms of cTnI may be elevated in other forms of cardiac muscle injury(contusion, cardiac muscle injury(contusion, myocarditis)myocarditis)

MyoglobinMyoglobin
Mgb is THE MOST SENSITIVE of the Mgb is THE MOST SENSITIVE of the cardiac markers cardiac markers
Earliest marker of acute MIEarliest marker of acute MI
Myoglobin should be elevated as soon as Myoglobin should be elevated as soon as an infarcting patient present to EDan infarcting patient present to ED
LEAST CARDIOSPECIFIC of cardiac LEAST CARDIOSPECIFIC of cardiac markers!markers!

Ischemia-modified albumin (IMA)Ischemia-modified albumin (IMA)
When albumin circulates through harsh When albumin circulates through harsh environments (acidosis, hypoxemia, free environments (acidosis, hypoxemia, free radicals, altered calcium- all seen in radicals, altered calcium- all seen in ischemia), its ability to rapidly and tightly ischemia), its ability to rapidly and tightly bind cobalt is alteredbind cobalt is alteredAltered Cobalt Binding (ACB) assay:Altered Cobalt Binding (ACB) assay:– Add cobalt, measure unbound amountAdd cobalt, measure unbound amount– Measurement reflects ischemia modified Measurement reflects ischemia modified
albuminalbumin

B-type Natriuretic Peptide (BNP)B-type Natriuretic Peptide (BNP)
Natriuretic peptides:Natriuretic peptides:– Cause vasodilation and sodium excretionCause vasodilation and sodium excretion
A-type: stored in granules in atrial myocytes, affected by A-type: stored in granules in atrial myocytes, affected by atrial filling pressure, ventrilar wall tensionatrial filling pressure, ventrilar wall tensionB-type: synthesized in ventricular myocytesB-type: synthesized in ventricular myocytes
– Correlates directly with ventricular wall tensionCorrelates directly with ventricular wall tension– N-terminal peptide fragment (N-terminal pro-BNP) is cleaved N-terminal peptide fragment (N-terminal pro-BNP) is cleaved
from pro-BNP to make active hormone BNPfrom pro-BNP to make active hormone BNP– N-terminal pro-BNP is more stable, provides more longitudinal N-terminal pro-BNP is more stable, provides more longitudinal
infoinfo
– Elevated in heart failureElevated in heart failureDistinguishes between cardiac/non-cardiac dyspneaDistinguishes between cardiac/non-cardiac dyspneaProvides prognostic info for pts with CHF and acute coronary Provides prognostic info for pts with CHF and acute coronary syndrome (ACS)syndrome (ACS)

ACSACS
Acute coronary syndrome:Acute coronary syndrome:– Encompasses many clinical situations with myocardial Encompasses many clinical situations with myocardial
ischemic damageischemic damageStable angina, unstable angina, acute MI, sudden cardiac Stable angina, unstable angina, acute MI, sudden cardiac deathdeathLab assays good at diagnosing MI, bad at diagnosing the Lab assays good at diagnosing MI, bad at diagnosing the remainderremainder
– Usual biomarkers for necrosis (MB, myoglobin, Usual biomarkers for necrosis (MB, myoglobin, troponin) are overall poor markers for non-AMI ACStroponin) are overall poor markers for non-AMI ACS
– BNP is predictive for both recurrence and higher BNP is predictive for both recurrence and higher likelihood of sudden cardiac death in non-AMI ACSlikelihood of sudden cardiac death in non-AMI ACS
– C-reactive proteinC-reactive protein good predictor of development of good predictor of development of ACS in healthy individualsACS in healthy individuals

ACUTE MIACUTE MITypical rise and fall of CK-MB or troponin with ischemic Typical rise and fall of CK-MB or troponin with ischemic symptomssymptomsECG changesECG changesOr interventionally demonstrated coronary artery Or interventionally demonstrated coronary artery abnormalityabnormalityTROPONINS: single positive troponin is highly specific TROPONINS: single positive troponin is highly specific for AMIfor AMI– Single low troponin has low sensitivity for negative predictorSingle low troponin has low sensitivity for negative predictor
CK-MB: increase detectable within 3-6 hours of AMI, CK-MB: increase detectable within 3-6 hours of AMI, peaks at 20-24 hours, returns to normal in 72 hours; peaks at 20-24 hours, returns to normal in 72 hours; sensitivity using serial measurements approaches 100%sensitivity using serial measurements approaches 100%Myoglobin: rapidly released from damaged muscle, early Myoglobin: rapidly released from damaged muscle, early indicator, negative predictive value 2 hours post indicator, negative predictive value 2 hours post symptoms approaches 100%symptoms approaches 100%

SERUM PROTEINSSERUM PROTEINS
Protein quantitation:Protein quantitation:– Nitrogen count (Kjeldahl technique) is gold Nitrogen count (Kjeldahl technique) is gold
standard; involves acid digestion of protein to standard; involves acid digestion of protein to release ammonium ions which are quantifiedrelease ammonium ions which are quantified
Assumption is serum proteins are 16% nitrogen by Assumption is serum proteins are 16% nitrogen by massmass
– Colorimetry (Biuret technique) is Colorimetry (Biuret technique) is recommended routine method for measuring recommended routine method for measuring total proteintotal protein
Absorbance from chelate with copper at 540 nm is Absorbance from chelate with copper at 540 nm is proportional to total proteinproportional to total protein

Protein SeparationProtein SeparationUse PRECIPITATIONUse PRECIPITATION
Electrophoresis: Electrophoresis: – Movement of proteins due to electrical potentialMovement of proteins due to electrical potential– Charge applied across a medium composed of solid Charge applied across a medium composed of solid
support (gel) and fluid buffer. Charge creates support (gel) and fluid buffer. Charge creates electromotive forceelectromotive force
– Solid support has slight neg charge and is drawn Solid support has slight neg charge and is drawn towards the anode (+ pole), but being solid, cannot towards the anode (+ pole), but being solid, cannot movemove
Compensatory flow of fluid buffer towards negative pole Compensatory flow of fluid buffer towards negative pole (cathode)(cathode)
This flow is called endosmosis- has capacity to carry This flow is called endosmosis- has capacity to carry substances suspended in mediumsubstances suspended in medium

Protein SeparationProtein Separation
If proteins added, two forces are on the proteins: If proteins added, two forces are on the proteins: – Electromotive forceElectromotive force– Endosmotic forceEndosmotic force
Most proteins have negative chargeMost proteins have negative charge– Electromotive force pulls towards anodeElectromotive force pulls towards anode– Endosmosis pulls towards cathodeEndosmosis pulls towards cathode
Gammaglobulins= weak net negative chargeGammaglobulins= weak net negative charge– Electromotive force exceeds endosmotic forceElectromotive force exceeds endosmotic force– Move to variable extent towards anodeMove to variable extent towards anode

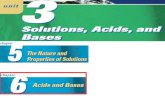
Serum Protein ElectrophoresisSerum Protein Electrophoresis
SPEP:SPEP:– When electrophoresis is carried out on serum When electrophoresis is carried out on serum
at pH 8.6 on agarose gel, then fixed and at pH 8.6 on agarose gel, then fixed and stained:stained:
Five distinct bands can be seenFive distinct bands can be seen
Fastest moving band is albuminFastest moving band is albumin
Next fastest- two Next fastest- two bands (a1 and a2)bands (a1 and a2)
Then the Then the band band
Then the Then the band (move very slowly) band (move very slowly)

Serum Protein ElectrophoresisSerum Protein Electrophoresis

Protein ElectrophoresisProtein Electrophoresis
Increasing endosmosis is used to separate Increasing endosmosis is used to separate gamma globulins into oligoclonal bands in gamma globulins into oligoclonal bands in CSF electrophorsisCSF electrophorsis
Capillary electrophoresis can also be used Capillary electrophoresis can also be used if there isif there is– Small sample sizeSmall sample size– Needed automationNeeded automation– Need for speedNeed for speed

Immunofixation ElectrophoresisImmunofixation Electrophoresis
IFEIFE– Method for characterizing a suspected monoclonal Method for characterizing a suspected monoclonal
band observed in SPEP or UPEPband observed in SPEP or UPEP– Much simpler to interpret than IEPMuch simpler to interpret than IEP– Place pt serum into six wells in agarose gelPlace pt serum into six wells in agarose gel– Five different monospecific antisera are appliedFive different monospecific antisera are applied
Anti-IgG, IgA, IgM, Kappa, and lambdaAnti-IgG, IgA, IgM, Kappa, and lambda
– Entire gel is stainedEntire gel is stained
IEP (immunoelectrophoresis)- not commonly IEP (immunoelectrophoresis)- not commonly used anymoreused anymore

IFEIFE

Serum ProteinsSerum Proteins
AlbuminAlbumin– Most abundant protein in human plasmaMost abundant protein in human plasma– 2/3 of total plasma protein2/3 of total plasma protein– Many functions:Many functions:
Maintains serum osmotic pressure, carries multiple Maintains serum osmotic pressure, carries multiple substancessubstances
Congenital absence NOT a serious problem (mild anemia Congenital absence NOT a serious problem (mild anemia and hyperlipidemia)and hyperlipidemia)
– Several allotypes:Several allotypes:Most common is Albumin AMost common is Albumin A
When variant is present, might get 2 peaksWhen variant is present, might get 2 peaks

AlbuminAlbumin
Clinical utility:Clinical utility:– Nutritional status (half-life is 17 days)Nutritional status (half-life is 17 days)– Hepatic synthetic function (ESLD)Hepatic synthetic function (ESLD)– Diabetic controlDiabetic control
In normal pts, up to 8% of albumin is glycosylatedIn normal pts, up to 8% of albumin is glycosylated
In diabetics with poor control, up to 25% may be In diabetics with poor control, up to 25% may be glycosylatedglycosylated
– Negative acute phase reactant (decreases in Negative acute phase reactant (decreases in inflammatory conditions)inflammatory conditions)

PrealbuminPrealbumin
Fastest migrating protein on SPEPFastest migrating protein on SPEPSparse, not normally seen on traditional SPEPSparse, not normally seen on traditional SPEPBinds T4 and T3Binds T4 and T3Binds and carries retinal-binding protein:vitamin Binds and carries retinal-binding protein:vitamin A complexA complexAlso, prealbumin is the precursor protein in Also, prealbumin is the precursor protein in senile cardiac amyloidosissenile cardiac amyloidosisShort ½ life of 48 hoursShort ½ life of 48 hoursTrue elevations seen in chronic EtOH, steroidsTrue elevations seen in chronic EtOH, steroidsNegative acute phase reactantNegative acute phase reactant

11 antitrypsin (AAT) antitrypsin (AAT)
Major component of the a1 bandMajor component of the a1 band
Main function is to inactivate various Main function is to inactivate various proteases like tyrpsin and elastaseproteases like tyrpsin and elastase
SPEP can be used to screen for AAT SPEP can be used to screen for AAT deficiencydeficiency
Markedly positive acute phase reactantMarkedly positive acute phase reactant

acid glycoprotein (orosomucoid)acid glycoprotein (orosomucoid)
Briskly positive acute phase reactantBriskly positive acute phase reactant
Minor component of a1 bandMinor component of a1 band
Major component of increased a1 band Major component of increased a1 band seen in inflammationseen in inflammation
May be used to monitor chronic May be used to monitor chronic inflammatory conditions like ulcerative inflammatory conditions like ulcerative colitiscolitis

macroglobulinmacroglobulin
Protease inhibitorProtease inhibitor
Serum concentration elevated in liver and Serum concentration elevated in liver and renal diseaserenal disease
Large size prevents its loss in nephrotic Large size prevents its loss in nephrotic syndrome, leading to a 10-fold increase in syndrome, leading to a 10-fold increase in concentrationconcentration

CeruloplasminCeruloplasmin
a2 proteina2 proteinFunctions in copper transportFunctions in copper transportDecreased serum ceruloplasmin important Decreased serum ceruloplasmin important marker for Wilson disease, ddx includes:marker for Wilson disease, ddx includes:– Hepatic failureHepatic failure– malnutritionmalnutrition– Menke syndromeMenke syndrome
Acute phase reactant:Acute phase reactant:– Elevated in inflammation and pregnancyElevated in inflammation and pregnancy

HaptoglobinHaptoglobin
Third major component of a2Third major component of a2Binds free hemoglobinBinds free hemoglobinDecreased or absent in acute intravascular Decreased or absent in acute intravascular hemolysishemolysisVery sensitive marker for hemolysisVery sensitive marker for hemolysisHaplotypes I and II:Haplotypes I and II:– Phenotypes 1-1, 1-2, 2-2Phenotypes 1-1, 1-2, 2-2– 2-2 phenotype is independent risk factor for CAD in 2-2 phenotype is independent risk factor for CAD in
diabetesdiabetes
Acute phase reactantAcute phase reactant

TransferrinTransferrinMajor Major globulin globulinFunctions to transport ferric iron (Fe3); normally Functions to transport ferric iron (Fe3); normally 30% saturated30% saturatedMarked increase in Fe def.; abnormally Marked increase in Fe def.; abnormally masquerades as an M-proteinmasquerades as an M-proteinIncreased in pregnancy and estrogen txIncreased in pregnancy and estrogen txDecreases in acute phase; but rises is Decreases in acute phase; but rises is inflammation persistsinflammation persistsBlood brain barrier transports transferrin to CSF Blood brain barrier transports transferrin to CSF in a modified form (Tau-protein)in a modified form (Tau-protein)Carbohydrate-deficient transferrin: superior to Carbohydrate-deficient transferrin: superior to GGT as marker for EtOH abuseGGT as marker for EtOH abuse

FibrinogenFibrinogen
Also called Also called globulin globulinIn normal course of events, no fibrinogen in In normal course of events, no fibrinogen in serum as it is consumed by formation of clotserum as it is consumed by formation of clot– If specimen clots incompletely (heparinized pt) If specimen clots incompletely (heparinized pt)
fibrinogen may be seenfibrinogen may be seen
Can straddle the Can straddle the interface interfaceWhen present in serum, may be misinterpreted When present in serum, may be misinterpreted as an M-proteinas an M-proteinMay be seen in serum in:May be seen in serum in:– Dysfibrinogenemia, APL syndrome, liver dz, vitamin K Dysfibrinogenemia, APL syndrome, liver dz, vitamin K
def, or heparindef, or heparin

C-reactive protein (CRP)C-reactive protein (CRP)
Produced in liverProduced in liverPredictive value of low level elevations (>2-3 Predictive value of low level elevations (>2-3 mg/L) for cardiac eventsmg/L) for cardiac eventsHigh sensitivity CRP (hsCRP) now available with High sensitivity CRP (hsCRP) now available with sensitivity of <0.5 mg/Lsensitivity of <0.5 mg/LDistribution NOT Gaussian curve-Distribution NOT Gaussian curve-– Curve skewed significantly with dense cluster in very Curve skewed significantly with dense cluster in very
lowest CRP levels and long tail extending into >10 lowest CRP levels and long tail extending into >10 rangerange
Half of population has CRP >2Half of population has CRP >2

CRPCRP
Three categories based on CRP:Three categories based on CRP:– Normal CRP <3 mg/LNormal CRP <3 mg/L– High CRP >10 mg/L (active inflammation)High CRP >10 mg/L (active inflammation)– Low-level elevations 3-10 mg/L (cellular stress)Low-level elevations 3-10 mg/L (cellular stress)
Low level elevation may indicate:Low level elevation may indicate:– Minor disease states Minor disease states – Genetic factorsGenetic factors– Demographic variablesDemographic variables– Behavioral pattersBehavioral patters
Individuals normal set point is inheritedIndividuals normal set point is inherited

CRPCRP
Low-level CRP elevation predicts poor Low-level CRP elevation predicts poor outcome following cardiovascular eventsoutcome following cardiovascular events– Also correlates with mortality in non-cardiac Also correlates with mortality in non-cardiac
dzsdzs

SPEP PatternsSPEP Patterns
Normal serum:Normal serum:– Invisible prealbumin bandInvisible prealbumin band– Very large albumin bandVery large albumin band– Then, small peaked a1, a2, a bimodal B, and Then, small peaked a1, a2, a bimodal B, and
a broad gamma banda broad gamma band
Bisalbuminemia:Bisalbuminemia:– Seen in heterozygotes for albumin allotypesSeen in heterozygotes for albumin allotypes– Double albumin spikeDouble albumin spike– No clinical consequenceNo clinical consequence

SPEP PatternsSPEP Patternsa1-antitrypsin (AAT) deficiency:a1-antitrypsin (AAT) deficiency:– AAT is the major component of a1 bandAAT is the major component of a1 band– Genotype PiZZ individuals have a visibly and Genotype PiZZ individuals have a visibly and
quantitatively decreased bandquantitatively decreased band
Nephrotic syndrome:Nephrotic syndrome:– Massive loss of small proteins, particularly albuminMassive loss of small proteins, particularly albumin– Minimal change disease: especially high loss of Minimal change disease: especially high loss of
albuminalbumin– With other forms of nephrotic syndrome, gamma With other forms of nephrotic syndrome, gamma
globulins also lostglobulins also lost– LARGE PROTEIN MOLECULES RETAINEDLARGE PROTEIN MOLECULES RETAINED– Result: dimming of all electrophoretic bands, with Result: dimming of all electrophoretic bands, with
exception of a2 which contains a2-MACROglobulinexception of a2 which contains a2-MACROglobulin

SPEP PatternsSPEP Patterns
Acute inflammation:Acute inflammation:– Acute phase reactants account for increases in a1, a2 Acute phase reactants account for increases in a1, a2
bandsbands– Albumin slightly increasedAlbumin slightly increased– Prolonged inflammation shows polyclonal gamma Prolonged inflammation shows polyclonal gamma
globulin increaseglobulin increase
Beta-gamma bridging (BODOR noted this has Beta-gamma bridging (BODOR noted this has been on several Board Exams):been on several Board Exams):– Hallmark of CIRRHOSISHallmark of CIRRHOSIS– Also, hypoalbuminemia, blunted a1 and a2Also, hypoalbuminemia, blunted a1 and a2– Beta-gamma bridging mainly due to increase serum Beta-gamma bridging mainly due to increase serum
IgAIgA

Monoclonal GammopathyMonoclonal Gammopathy
SPEP shows a prominent discrete dark band (M-SPEP shows a prominent discrete dark band (M-spike, m-protein) usually within the gamma spike, m-protein) usually within the gamma region (sometimes in B or a2)region (sometimes in B or a2)A monoclonal gammopathy (paraprotein) shows A monoclonal gammopathy (paraprotein) shows immunochemically homogeneous immunochemically homogeneous immunoglobulin (M-protein) in serumimmunoglobulin (M-protein) in serumMay be result of:May be result of:– Multiple myelomaMultiple myeloma– Neoplastic proliferations like solitary plasmactyoma, Neoplastic proliferations like solitary plasmactyoma,
MGUS, Waldenstroms macroglobulinemia MGUS, Waldenstroms macroglobulinemia (lymphoplasmacytic lymphoma), and CLL/SLL(lymphoplasmacytic lymphoma), and CLL/SLL

Biclonal GammopathyBiclonal Gammopathy
2 M-proteins2 M-proteins
Occurs in 3-4% of casesOccurs in 3-4% of cases
If biclonal gammopathy has IgA spikes If biclonal gammopathy has IgA spikes having a single light chain (by IFE):having a single light chain (by IFE):– Most likely due to appearance of both Most likely due to appearance of both
monomers and dimers in SPEPmonomers and dimers in SPEP– Should be considered monoclonalShould be considered monoclonal

SPEP HypogammaglobulinemiaSPEP Hypogammaglobulinemia
10% of SPEPs10% of SPEPsWhen not due to myeloma:When not due to myeloma:– May be due to congenital deficiency, May be due to congenital deficiency,
lymphoma, nephrotic syndrome, or lymphoma, nephrotic syndrome, or corticosteroidscorticosteroids
Pts with myeloma and Pts with myeloma and hypogammaglobulinemia are likely to have hypogammaglobulinemia are likely to have free-light chains in urine (Bence-Jones free-light chains in urine (Bence-Jones proteins)proteins)

IFEIFE
Indicated to characterize M-protein on SPEPIndicated to characterize M-protein on SPEP
Even if no m-spike is seen, do IFE if:Even if no m-spike is seen, do IFE if:– Strong suspicion of myeloma (lytic bone lesions in 80 Strong suspicion of myeloma (lytic bone lesions in 80
year old male)year old male)– Systemic AL amyloidosisSystemic AL amyloidosis– HypogammaglobulinemiaHypogammaglobulinemia
In pts with negative serum screens with high In pts with negative serum screens with high suspicion, do UPEP (for light chain disease)suspicion, do UPEP (for light chain disease)– May be losing all of light chain in urineMay be losing all of light chain in urine

M-proteinM-protein
Usually an intact immunoglobulin Usually an intact immunoglobulin composed of 2 heavy and 2 light chainscomposed of 2 heavy and 2 light chains
Sometimes, it is light chain only or very Sometimes, it is light chain only or very rarely, heavy chain onlyrarely, heavy chain only
Systemic amyloidosis may result from Systemic amyloidosis may result from monoclonal gammopathy, when M protein monoclonal gammopathy, when M protein produced has unusual (amyloidogenic) produced has unusual (amyloidogenic) propertiesproperties

After diagnosis:After diagnosis:
Protein electrophoresis is used to follow Protein electrophoresis is used to follow disease progression and efficacy of disease progression and efficacy of treatmenttreatment3 quantitive results are important:3 quantitive results are important:– M-protein concentrationM-protein concentration– Degree of suppression of other Degree of suppression of other
immunoglobulins (IgG, IgA, IgM, whichever is immunoglobulins (IgG, IgA, IgM, whichever is not involved)not involved)
– Quantity of free serum light chain, especially Quantity of free serum light chain, especially in light chain only myelomas (extremely in light chain only myelomas (extremely sensitive to myeloma recurrence after tx)sensitive to myeloma recurrence after tx)

Hyperviscosity syndromeHyperviscosity syndrome
Normally, viscosity of serum is 1.5-1.8 Normally, viscosity of serum is 1.5-1.8 centipoise (cp)centipoise (cp)
Hyperviscosity syndrome: exceeds 3.0 cpHyperviscosity syndrome: exceeds 3.0 cp
Symptoms: Symptoms: – Nasal bleeding, blurred vision, retinal vein Nasal bleeding, blurred vision, retinal vein
dilation, neurologic symptomsdilation, neurologic symptoms

CryoglobulinsCryoglobulins
May be looked for in pts with M-proteinsMay be looked for in pts with M-proteinsPrecipitate reversibly at low tempsPrecipitate reversibly at low tempsBlood is drawn and kept at 37 degrees C until Blood is drawn and kept at 37 degrees C until clottedclottedCentrifuged at 37 degreesCentrifuged at 37 degreesRemaining serum stored at 4 deg C for at least 3 Remaining serum stored at 4 deg C for at least 3 days, then centrifuged at 4 deg Cdays, then centrifuged at 4 deg CAny precipitate that is formed is Any precipitate that is formed is CRYOPRECIPITATE and can be subject to CRYOPRECIPITATE and can be subject to electrophoresiselectrophoresis

CryoglobulinsCryoglobulins
3 types:3 types:– Type I: monoclonal immunoglobulins Type I: monoclonal immunoglobulins
associated with MM or Waldenstromsassociated with MM or Waldenstroms– Type II: mix of monoclonal IgM and polyclonal Type II: mix of monoclonal IgM and polyclonal
IgG. IgM has Rheumatoid factor activity (anti-IgG. IgM has Rheumatoid factor activity (anti-IgG). This is the most common type of cryoIgG). This is the most common type of cryo
– Type III: mix of two polyclonal cryoglobulinsType III: mix of two polyclonal cryoglobulins

Mixed CryoglobulinemiaMixed Cryoglobulinemia
Types II & IIITypes II & IIIFound in variety of conditions:Found in variety of conditions:– Lymphoproliferative d/o, chronic infx, chronic liver dz, Lymphoproliferative d/o, chronic infx, chronic liver dz,
autoimmune dz (SLE)autoimmune dz (SLE)– Most common in women in 4Most common in women in 4thth-5-5thth decades of life decades of life– 30-50% of cases have underlying HepC virus (most 30-50% of cases have underlying HepC virus (most
common cause)common cause)– Clinical manifestation: palpable purpura, arthralgias, Clinical manifestation: palpable purpura, arthralgias,
hepatoslenomegaly, lymphadenopathy, anemia, hepatoslenomegaly, lymphadenopathy, anemia, sensoineural defects, and glomerulonephritissensoineural defects, and glomerulonephritis
Tx: corticosteroids, plasmapheresis, a-interferonTx: corticosteroids, plasmapheresis, a-interferon

UPEPUPEPIn proteinuria, UPEP can determine source of In proteinuria, UPEP can determine source of proteinprotein– Glomerular proteinuria pattern:Glomerular proteinuria pattern:
Strong albumin, a1, B bandsStrong albumin, a1, B bandsVery large and very small proteins don’t make it into Very large and very small proteins don’t make it into urine, leaving albumin, AAT, and transferrinurine, leaving albumin, AAT, and transferrin
– Tubular proteinuria pattern:Tubular proteinuria pattern:Weak albumin band, strong a1 and B bandsWeak albumin band, strong a1 and B bandsImpaired tubular reabsorption of LMW proteins normally Impaired tubular reabsorption of LMW proteins normally filtered freely by glomerulus (a2-macroglobulin, b2 filtered freely by glomerulus (a2-macroglobulin, b2 microglobulin, light chains)microglobulin, light chains)
– Overflow proteinuria pattern:Overflow proteinuria pattern:Monoclonal light chain (Bence Jones) Monoclonal light chain (Bence Jones) Remember that these back up into SPEP in MYELOMA Remember that these back up into SPEP in MYELOMA KIDNEYKIDNEY

CSF Protein electrophoresisCSF Protein electrophoresis
Different than serumDifferent than serum
All proteins in serum, but smaller All proteins in serum, but smaller quantitiesquantities
Prominent prealbumin band and double Prominent prealbumin band and double beta (transferrin) band (transferrin beta (transferrin) band (transferrin conjugated to Tau-protein on way into conjugated to Tau-protein on way into CSF)CSF)