
Quarterly Collaborative Call #25 July 25, 2017 2:00 – 2:30 ...
23
Quarterly Collaborative Call #25 July 25, 2017 2:00 – 2:30 p.m. CST Screening Hospital ER and Outpatients for Fall Risk Optimizing Learning from Falls using the KNOW Falls System
Transcript of Quarterly Collaborative Call #25 July 25, 2017 2:00 – 2:30 ...

Quarterly Collaborative Call #25July 25, 2017 2:00 – 2:30 p.m. CST
Screening Hospital ER and Outpatients for Fall Risk
Optimizing Learning from Falls using the KNOW Falls System
AGENDA1. Housekeeping
– Quarterly Calls Feedback– Request for benchmarking data– 9/22 Fall Prevention Awareness
Day
2. Lessons Learned from your reporting1) Prevalence of OP and ED Falls2) How to optimize learning from
KNOW Falls
3. Open Discussion and Questions

Quarterly CallsAgenda1. Summarize your progress, what is going well,
what are the barriers?2. Feedback/discussion of event reports3. What have you learned by working together as a
team? Any changes in your team?
Purpose: to facilitate coordinating team reflection1. Objectives of fall risk reduction system2. Implementation successes and barriers3. Your ability to coordinate, collaborate, and cooperate4. Use data (study) to prioritize action plan items and
monitor progress toward your goals

Quarterly Calls Feedback• What went well with the call
– Scheduling and Agenda?– Data Summary?– Review of fall event?
• What didn’t go well?
• What should we do differently?
• Close the loop with UNMC!

Request for Benchmarking Data
Request Date 8/1/17Due Date 9/5/17
We will prepopulate what we have
Common mistakes to avoid…
• Patient days are not admissions
• Include observation hours
• Bruising and skin tears are minor injury
Fall Rate Data 2014 - 2016
Hospital Name: Enter Hospital NameCity: Enter Hospital City
Fall Rate Data 2014 2015 2016
- - - - - -
- - - - - -
Required Field Not
Required Field Not
Required Field Not q
Field Not Entered
q Field Not
Entered
q Field Not
Entered
N/A N/A N/A
*Required Fields
Calendar Year
Please complete the spreadsheet by entering your hospital data in the YELLOW cells. BLUE cells contain formulas which will automatically calculate. When complete, please save file and email as an attachment to Anne Skinner at [email protected].
CAPTURE Falls
Unassisted Fall Rate (Calculated)
If known, indicate how many of your total falls were assisted vs. unassisted:
Number of Assisted FallsNumber of Unassisted Falls
Unknown (Calculated)
Include ALL falls that result in minor, moderate, major harm and death
Total Inpatient Falls (from above)
Fall Rate/1000 Patient Days (Calculated)
Injurious Fall Rate/1000 Patient Days (Calculated)
*Inpatient Days
*Number of Total inpatient Falls
*Number of Injurious Patient Falls
This is the number of days inpatients and observation patients received care based on midnight census; include acute, skilled (swing bed), observation, and hospice patients; exclude newborns and acute rehab patients.
Observation HoursObservation Patient Days (Calculated)Total Patient Days (Calculated)
Include unassisted, assisted, non-injurious and injurious falls

Fall Prevention Awareness DaySept. 22, 2017National Council on Aging https://www.ncoa.org/healthy-aging/falls-prevention/falls-prevention-awareness-day/
Resource for photos, videos, handouts, infographics
Media Toolkit https://www.ncoa.org/healthy-aging/falls-prevention/falls-prevention-awareness-day/marketing-media/falls-prevention-awareness-day-media-toolkit/
10 Years Standing Together to Prevent Falls

Sample Infographic
https://www.ncoa.org/wp-content/uploads/6-Steps-to-Prevent-a-Fall.pdf

Lessons Learned from Reporting1. Falls occur among outpatients and
in the emergency room. What tools and policies can we share to decrease fall risk for these patients? 21/336 (6.3%) Hospital Falls = Outpatient
• Outpatient and ER falls will not be included in hospital inpatient benchmarks. What will be included: acute,
• Including outpatient and ER falls in KNOW Falls supports learning from these events

Options to screen hospital ER patients and outpatientsA. Memorial ED Fall Risk Assessment Tool
Memorial ED Fall Risk Assessment Tool
Factor Poin
ts
Factor Poin
ts
History of Falling (3 months) 0-3 Impaired Gait 1
Confusion/Disorientation 5 Mobility Assist Devise Used 1
Intoxicated/Sedated 3 Altered Elimination 1
Source: Flarity et al. Advanced Emergency Nursing Journal; 2013. 35:57–66
Signage, bed alarm, rounding, pt/family education, gait belt and assistive device for transfers and ambulation
1-2 points = low risk3-4 points = moderate risk5+ points = high risk

Options to screen hospital ER patients and outpatients
1. Patients sit in a straight-backed waiting room chair, the nurse observe him/her:1) Get up ( without use of arm rests, if possible)2) Stand momentarily3) Walk into clinic4) Sit down in clinic chair
2. Nurse asks the following questions:1) Single or recurrent falls in past 3 months?2) Circumstances of the fall.3) Injury due to the fall.4) Benefit from assistive device?
3. Nurse decides:1) Assistive devices needed2) Difficulty walking when first gets up3) Medications may be related to the fall4) Recent vision changes5) Shortness of breath upon exertion6) Dizziness
Meador, et al. Fall Risk Assessment in the Outpatient Setting. The Oklahoma Nurse. 2010:10-11.
B. Fall Risk Screen-Outpatient

Options to screen hospital ER patients and outpatientsC. CAH Fall Risk Screen for Outpatients • One CAH in our collaborative does the following: In
the ED we ask: “Have you fallen in the last 6 months?” If Yes, then the ED/radiology/lab staff taking care of
the patient are aware of the risk and have access to the following interventions Gait belt and assistive device that patient normally uses Hoyer lift Gripper socks
• Consider 3 questions from STEADI Screening tool:1. Have you fallen in the past year?2. Do you feel unsteady when standing or walking?3. Do you worry about falling? Answer Yes to any of the 3 and consider that patient is at
risk for falling
Option to screen primary care clinic outpatients…STEADIStopping Elderly Accidents, Deaths, & Injuries (STEADI) is a toolkit intended to integrate fall risk assessment and treatment into primary care. Developed by CDC and available at https://www.cdc.gov/steadi/materials.html
• Screening Algorithms• Medication Review• Fact Sheets • Functional Assessments

STEADI Graphic
13https://www.cdc.gov/steadi/images/graphics/falls_preventable_problem-800x512.jpg

STEADI Algorithmhttps://www.cdc.gov/steadi/pdf/Algorithm_2015-09-print.pdf
14

Lessons Learned from Reporting2. Learning from events is a 3-step
dynamic process, which requires redefining, clarifying, and routinizing
Identify need for innovation (Gap Analysis)
Match innovations to need and bridge performance gap (Action Plan)
Restructureorganization to fit innovation (Coordinating team, post-fall huddles, policy/ procedure)
Make roles and tasks associated with innovation clear
Hard-wire:audits, job descriptions,performance appraisals
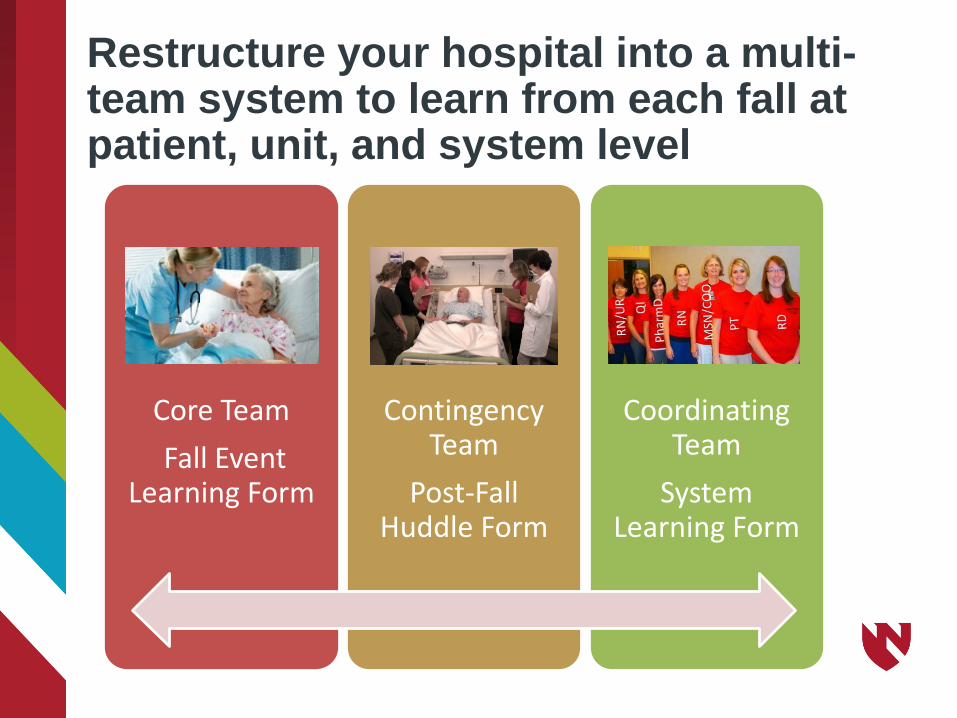
Restructure your hospital into a multi-team system to learn from each fall at patient, unit, and system level
Core TeamFall Event
Learning Form
Contingency Team
Post-Fall Huddle Form
Coordinating Team
System Learning Form

Lost Opportunities to learn when each team does not reflect on the fall…
336
203
740
50
100
150
200
250
300
350
400
Reported Falls Falls with IdentifiedCause
Falls with IdentifiedError Type
Num
ber o
f Fal
ls
Lost Opportunities to Understand and Share Patient Level Knowledge
Lost Opportunities to Understand and Share System Level Knowledge
Unanticipated - 18Accidental - 46
Anticipated - 172
Task - 39Judgement - 29
Care Coordination - 14System - 19
135 Post-fall huddles with more than 1 participant

InteractionPr
oces
s Unc
erta
inty Low
Low HighTask Error Coordination Error
High
Judgment Error System Interaction
18
Types of Human Errors
MacPhail LH, & Edmondson AC. Learning domains: The importance of work context in organizational learning from error. In D. A. Hofmann & M. Frese, Errors in Organizations. New York: Routledge; 2011:177-198.

InteractionPr
oces
s Unc
erta
inty Low
Low (Individual) High (Multiple People)Task Execution: Individualperforms well understood, routine tasksTask Error Example: Forget to turn on bed alarm for patients at high risk for falls (stated in policy)
Coordination: Process knowledge needs to be shared between teams/groupsCoordination Error Example: Information about previous fall not shared between shifts/departments
High
Judgment: Individuals perform unfamiliar process that requires decision makingJudgment Error Example: New patient at high risk for falls left alone in bathroom (policy does not address this issue)
System Interaction: Multiple people involved in unfamiliar/ unexpected activitySystem Error Example: No policy/ procedure to use bed scale instead of standing scale for patients at high risk for falls
19
Types of Human Errors
MacPhail LH, & Edmondson AC. Learning domains: The importance of work context in organizational learning from error. In D. A. Hofmann & M. Frese, Errors in Organizations. New York: Routledge; 2011:177-198.

KNOW Falls Best PracticesGoal: Learn from each fall at patient AND system level
Standardize your approach, the ideal…1. Staff who discovered the fall complete the
Fall-Event Learning Form (likely to be paper)
2. Huddle participants determine cause of fall (unanticipated physiological, environmental, anticipated physiological) and actions to prevent recurrence, then huddle facilitator completes Post-Fall Huddle Form
3. Coordinating team reflects on Fall Event and Post-fall Huddle Forms, then decides on error types and completes System-Learning form
Discussion Assistance is an email away!
21
http://news.discovery.com/tech/virtual-moderator-helps-discussions-130506.htm
• Contact us for more information about implementation and best practices (including outpatient and ED Assessments, and RCA) …Katherine ([email protected])
• KNOW Falls and Online Learning (RedCAP) … Anne ([email protected])

Quarterly Collaborative Calls:
• Tuesday July 25, 2017 14:00 CST• Tuesday Oct. 24, 2017 14:00 CST• Tuesday Jan. 23, 2018 14:00 CST• Tuesday April 17, 2018 14:00 CST
Review the tools created with your assistance
http://www.unmc.edu/patient-safety/capturefalls/tool-inventory.html
C A P T U R ECollaboration and Proactive Teamwork Used to Reduce Falls
REMINDERS

University of Nebraska Medical Center
C A P T U R ECollaboration and Proactive Teamwork Used to Reduce
Fallshttp://www.unmc.edu/patient-safety/capturefalls/Enter “capture falls” in google


















