Quantitative Ultrasound and Mortality: A Prospective Study
7
Original Article Quantitative Ultrasound and Mortality: A Prospective Study D. C. Bauer 1,2 , L. Palermo 2 , D. Black 2 and J. A. Cauley 3 for the Study of Osteoporotic Fractures Research Group: Universities of California (San Francisco), Pittsburgh, Minnesota (Minneapolis), and Kaiser Center for Health Research, Portland 1 Division of General Internal Medicine and 2 Department of Epidemiology and Biostatistics, University of California, San Francisco; and 3 Department of Epidemiology, University of Pittsburgh, USA Abstract. Previous studies suggest that low bone mineral density (BMD) is associated with increased mortality, but the relationship between quantitative ultrasound (QUS) and mortality is unknown. We studied 5816 women over age 70 years enrolled in the Study of Osteoporotic Fractures. QUS of the calcaneus, and BMD of the calcaneus and hip, were measured at baseline, and women were contacted every 4 months to determine vital status. All reported deaths were confirmed by review of the death certificate or hospital records, and classified by ICD-9 code. During 5.0 years of follow-up, 677 women died. Women in the lowest quintile of QUS had the highest mortality during follow-up. After adjustment for age, grip strength, weight, height, health status, estrogen use, smoking, physical activity, and history of hypertension, diabetes, cardiovascular disease, cancer and stroke, each 1 SD reduction in broadband ultrasonic attenuation (BUA) was associated with a 16% increase in mortality (RH = 1.16; 95% CI: 1.07, 1.26). Mortality from cardiovascular disease, cancer and other causes were all increased among women with low QUS, but the association with cancer deaths was not statistically significant after multiple adjustments (RH = 1.09; CI: 0.93, 1.27). Low BMD was also associated with an increased risk of total and cause-specific mortality, but we found little evidence that BUA and BMD were independent predictors of mortality. Results were similar among women who did not fracture during follow-up. In this large population-based study of older women, low QUS is associated with both total and cause-specific mortality. This relationship was indepen- dent of other factors associated with mortality, such as age and health status, and suggests QUS and BMD may reflect some aspect of aging not captured by these traditional factors. Keywords: Bone mineral density; Mortality; Prospec- tive cohort; Quantitative ultrasound Introduction Bone mineral density (BMD) measurements in post- menopausal women reflect a number of complex processes and are determined by both peak bone mass levels and postmenopausal bone loss. In 1991, Browner and colleagues [1] observed that low wrist and heel BMD measurements were associated with increased mortality risk. Even after adjusting for a number of potential confounding factors, Browner et al. found that low bone mass increased both the cancer and cardiovascular mortality risk. These findings have since been confirmed in several other prospective studies [2,3], but the explanation for these results remains uncertain. Quantitative ultrasound (QUS) is a new noninvasive technique used to assess skeletal health [4–6]. Large prospective studies of older women have demonstrated that low QUS predicts increased risk of hip and other non-spine fractures [7,8]. Although QUS measurements do reflect bone mass [4], some studies suggest that QUS also assesses elements of bone quality, including trabecular thickness and connectivity [9,10]. To test the hypothesis that low QUS, like low BMD, is associated with increased mortality, we prospectively Osteoporos Int (2002) 13:606–612 ß 2002 International Osteoporosis Foundation and National Osteoporosis Foundation Osteoporosis International Correspondence and offprint requests to: Douglas C. Bauer, MD, UCSF, 74 New Montgomery, Suite 600, San Francisco, CA 94105, USA. Tel: +1(415) 597 9289. Fax: +1 (414) 597 9213. e-mail: [email protected]
Transcript of Quantitative Ultrasound and Mortality: A Prospective Study
Original Article
Quantitative Ultrasound and Mortality: A Prospective Study
D. C. Bauer1,2, L. Palermo2, D. Black2 and J. A. Cauley3 for the Study of Osteoporotic FracturesResearch Group: Universities of California (San Francisco), Pittsburgh, Minnesota (Minneapolis), andKaiser Center for Health Research, Portland1Division of General Internal Medicine and 2Department of Epidemiology and Biostatistics, University of California, SanFrancisco; and 3Department of Epidemiology, University of Pittsburgh, USA
Abstract. Previous studies suggest that low bonemineral density (BMD) is associated with increasedmortality, but the relationship between quantitativeultrasound (QUS) and mortality is unknown. We studied5816 women over age 70 years enrolled in the Study ofOsteoporotic Fractures. QUS of the calcaneus, and BMDof the calcaneus and hip, were measured at baseline, andwomen were contacted every 4 months to determinevital status. All reported deaths were confirmed byreview of the death certificate or hospital records, andclassified by ICD-9 code. During 5.0 years of follow-up,677 women died. Women in the lowest quintile of QUShad the highest mortality during follow-up. Afteradjustment for age, grip strength, weight, height, healthstatus, estrogen use, smoking, physical activity, andhistory of hypertension, diabetes, cardiovascular disease,cancer and stroke, each 1 SD reduction in broadbandultrasonic attenuation (BUA) was associated with a 16%increase in mortality (RH = 1.16; 95% CI: 1.07, 1.26).Mortality from cardiovascular disease, cancer and othercauses were all increased among women with low QUS,but the association with cancer deaths was notstatistically significant after multiple adjustments (RH= 1.09; CI: 0.93, 1.27). Low BMD was also associatedwith an increased risk of total and cause-specificmortality, but we found little evidence that BUA andBMD were independent predictors of mortality. Resultswere similar among women who did not fracture duringfollow-up. In this large population-based study of olderwomen, low QUS is associated with both total and
cause-specific mortality. This relationship was indepen-dent of other factors associated with mortality, such asage and health status, and suggests QUS and BMD mayreflect some aspect of aging not captured by thesetraditional factors.
Keywords: Bone mineral density; Mortality; Prospec-tive cohort; Quantitative ultrasound
Introduction
Bone mineral density (BMD) measurements in post-menopausal women reflect a number of complexprocesses and are determined by both peak bone masslevels and postmenopausal bone loss. In 1991, Brownerand colleagues [1] observed that low wrist and heelBMD measurements were associated with increasedmortality risk. Even after adjusting for a number ofpotential confounding factors, Browner et al. found thatlow bone mass increased both the cancer andcardiovascular mortality risk. These findings have sincebeen confirmed in several other prospective studies [2,3],but the explanation for these results remains uncertain.
Quantitative ultrasound (QUS) is a new noninvasivetechnique used to assess skeletal health [4–6]. Largeprospective studies of older women have demonstratedthat low QUS predicts increased risk of hip and othernon-spine fractures [7,8]. Although QUS measurementsdo reflect bone mass [4], some studies suggest that QUSalso assesses elements of bone quality, includingtrabecular thickness and connectivity [9,10].
To test the hypothesis that low QUS, like low BMD, isassociated with increased mortality, we prospectively
Osteoporos Int (2002) 13:606–612� 2002 International Osteoporosis Foundation and National Osteoporosis Foundation Osteoporosis
International
Correspondence and offprint requests to: Douglas C. Bauer, MD,UCSF, 74 New Montgomery, Suite 600, San Francisco, CA 94105,USA. Tel: +1(415) 597 9289. Fax: +1 (414) 597 9213. e-mail:[email protected]

studied the relationship between QUS, bone massmeasurements and subsequent mortality among a large,well-characterized cohort of older women enrolled in theStudy of Osteoporotic Fractures. To further elucidate theconnection between these measurements and mortality,we also determined the independent effect of low QUSand BMD on total and cause-specific mortality.
Materials and Methods
Subjects
Participants were subjects in the multicenter Study ofOsteoporotic Fractures (SOF), a prospective study of riskfactors for fracture in women over age 65 years. Womenwere recruited from population-based listings at fourclinical centers located in Baltimore, Pittsburgh, Port-land and Minneapolis. The recruitment and character-istics of this population have been described previously[11].
A complete set of measurements for this analysiscome from the 5816 SOF participants who returned foradditional examinations at the fourth SOF visit approxi-mately 5 years after initial enrollment. This populationrepresents 92% of the participants who were seen at thatvisit, and 72% of the surviving original SOF participants.
Measurements
Women who agreed to participate were interviewed andexamined at one of the four clinical centers. Detaileddata about physician-diagnosed medical conditions andpast and present medication use were collected. Currentmedication use was then confirmed by examination ofpill bottles by trained interviewers. Participants wereasked specifically about previous diagnoses of heartdisease, cancer and stroke, as well as previous use ofestrogens. Grip strength was measured using a hand-helddynamometer, and height and weight were measuredusing standard protocols [11]. Weight loss wascalculated as the change in weight occurring betweenthe third and fourth SOF visits [12].
BUA of the right heel was measured with a WalkerSonix UBA 575 machine using the scanning protocolprovided by the manufacturer (Hologic, Waltham, MA).Two measurements with repositioning were obtained on93% of participants (n = 5748); if the first twomeasurements differed by 10 dB/MHz or more, a thirdmeasurement was obtained. We assessed short-termreproducibility by obtaining three measurements withrepositioning on 40 unselected SOF subjects (10 at eachsite). The coefficient of variation for each clinic rangedfrom 4.1 to 5.6, and the mean coefficient of variation(CV) was 5.0. Acoustic phantoms provided by themanufacturer were scanned weekly at each site.
BMD was measured on the same visit at which QUSwas measured; BMD of the hip was performed withHologic QDR 1000 densitometers (Hologic, Waltham,
MA) using dual-energy X-ray absorptiometry (DXA),while calcaneal BMD was measured using single X-rayabsorptiometry (Osteoanalyzer, Dove Medical, NewburyPark, CA). Calcaneal BMD was measured on the samefoot as QUS. Quality assurance phantom scans wereperformed on a daily basis, and inter-site variabilityprecision was assessed by measuring BMD on twovisiting research staff, and by circulation of a single setof hip phantoms [13]. The CV for femoral neck BMD ofthe two research staff was 1.2%. The CV for the femoralneck phantom was 0.8%.
Ascertainment of Deaths
Women were contacted by postcard very 4 months. If aparticipant died, copies of the official death certificateand hospital records, if available, were requested. Aphysician investigator at the coordinating center,unaware of the participant’s ultrasound or densitometryresults, determined the cause of death.
Causes of death were assigned and classified by theInternational Classification of Disease, 9th revision.They were grouped into three main categories: (1)cardiovascular mortality, which included diagnoses ofcoronary artery disease, congestive heart failure, suddendeath and other cardiovascular outcomes, (2) cancermortality, including any malignancy, and (3) othercauses of death, including a wide variety of infectiousdiseases, pulmonary disease, and so forth.
Analysis
The distributions of all variables were plotted andexamined. Continuous variable means were compared byStudent’s t-tests for statistical significance. We used age-adjusted and multivariable-adjusted Cox proportionalhazard models to determine the relative hazard (RH) and95% confidence intervals (95% CI) of all-cause mortalityper standard deviation reduction in BUA or BMD.Covariates were selected for inclusion in final multi-variate models if they were strongly associated withmortality (p50.05) and they had been previouslydemonstrated to be associated with bone mass in theSOF cohort [11,14]. The proportionality assumption wasnot violated. Separate models were constructed forcause-specific mortality classified as cardiovascular,cancer or other.
To determine the independent contribution of BUAand BMD to mortality, both variables were entered intohazard models adjusted for other covariates.
The funding agency and QUS device manufacturerhad no role in the design, analysis or reporting of thisstudy.
QUS Predicts Total and Cause-Specific Mortality as Well as BMD 607

Results
Baseline Characteristics
Six thousand three hundred and thirty women wereexamined at the fourth SOF visit between 1992 and1994. Five thousand eight hundred and sixteen of thesewomen successfully completed QUS of the calcaneus,SPA of the heel and DXA of the proximal femur. Thecorrelation between calcaneal BUA and hip BMD wasmodest (r = 0.43), while the correlation between BUAand heel BMD was somewhat stronger (r = 0.70).Six hundred and seventy-seven women died during a
mean of 5.0 years of follow-up. Death certificates todetermine cause of death were available for all but 5deceased women. The baseline characteristics of theparticipants who did and did not survive during follow-up are detailed in Table 1. As expected, women who didnot survive were on average older, weaker, and morelikely to report a history of tobacco use, diabetes,cardiovascular disease and cancer, while less likely toexercise or use estrogens. For example, in multiplyadjusted models each 5-year increment of age wasassociated with a 50% increase in total mortality (RH =1.49; 95% CI: 1.38, 1.62).
QUS and Mortality
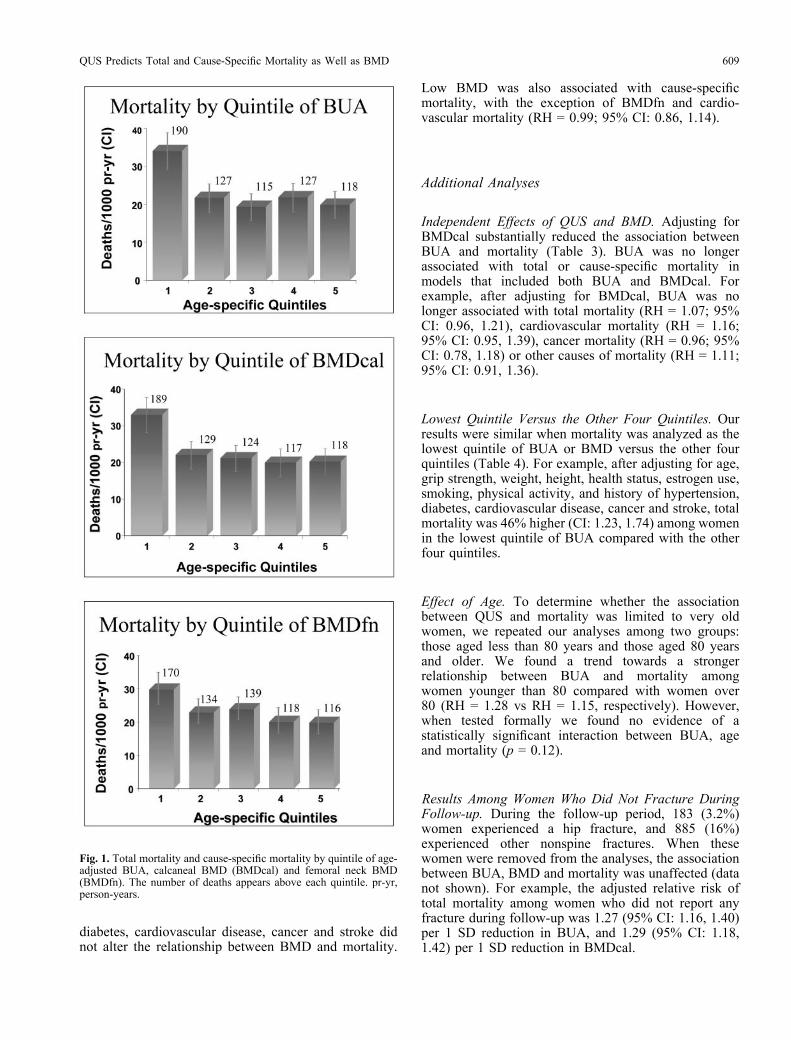
After adjustment for age, lower BUA was found to beassociated with an increased risk of mortality (Fig. 1).After sorting into and examining BUA measurementsby quintile, we found that women in the lowest quintile(552.0 dB/MHz) had the greatest risk of mortalityduring follow-up. Since the quintile analyses suggesteda possible threshold effect, we also analyzed our datacomparing the mortality in the lowest quintile of BUAwith the other four quintiles (see below). The
difference in total mortality between the lowest andhighest quartile of BUA was 72 deaths per 1000person-years.
The association between low BUA and increasedmortality persisted after adjusting for potential con-founders (Table 2). In multivariate models for adjustedfor age, grip strength, weight, height, health status,estrogen use, smoking, physical activity, and history ofhypertension, diabetes, cardiovascular disease, cancerand stroke, each 1 SD reduction in BUA was associatedwith a 16% increase in total mortality. Results weresimilar when multivariate models were adjusted forweight loss rather than baseline weight. We observed anon-significant trend towards fewer deaths amongestrogen users both before (RH = 0.79; 95% CI: 0.62,1.00) and after adjustment for BUA (RH = 0.83; 95% CI:0.065, 1.05).
The findings were similar for cause-specific mortality(Table 2). After adjustment for potential confounders,each 1 SD reduction in BUA was associated with astatistically significant 19% increase in cardiovasculardeath and a 23% increase in deaths from other causes.Each 1 SD reduction in BUA was associated with a 9%increase in cancer mortality, but this did not reachstatistical significance (95% CI: 0.93, 1.27).
BMD and Mortality
The relationship between bone mass and mortality wasvery similar to that observed with QUS (Table 2). Aspreviously reported [1], women in the lowest quintile ofBMD at the calcaneus (BMDcal) or femoral neck(BMDfn) had the highest risk mortality, suggesting apossible threshold effect. Further adjustment for age,grip strength, weight, height, health status, estrogen use,smoking, physical activity, and history of hypertension,
Table 1. Characteristics of participants by survival during follow-up
Variable Alive(n = 5139)
Any death(n = 677)
CV death(n = 250)
Cancer death(n = 189)
Other death(n = 238)
Age, years (SD) 76.2 (4.4) 79.1 (5.6)* 79.7 (5.7)* 77.2 (5.0)* 79.9 (5.5)*Grip strength, kg (SD) 18.5 (4.0) 16.8 (4.2)* 16.5 (4.2)* 18.2 (4.1) 16.2 (3.9)*Weight, kg (SD) 66.7 (12.5) 63.8 (12.4)* 65.0 (12.4)* 65.7 (12.0) 60.9 (12.1)*Height, cm (SD) 158.5 (6.0) 157.1 (6.3)* 156.8 (6.4)* 158.3 (5.9) 156.6 (6.4)*Activity, kcal/week (SD) 1355 (1510) 877 (1087)* 734 (1079)* 1155 (1203)* 803 (954)*Current smoker (%) 267 (5.2) 55 (8.1)* 19 (7.6) 16 (8.5)* 20 (8.4)*History of diabetes (%) 255 (5.0) 76 (11.3)* 34 (13.7)* 18 (9.5)* 24 (10.1)*History of hypertension (%) 2226 (43.3) 363 (53.8)* 163 (65.5)* 81 (42.9) 119 (50.2)*History of cancer (%) 1060 (20.6) 179 (26.5)* 56 (22.5) 73 (38.6)* 50 (21.1)History of heart disease (%) 335 (6.5) 77 (11.4)* 47 (18.9)* 9 (4.8) 21 (8.9)History of stroke (%) 220 (4.3) 59 (8.7)* 25 (10.0)* 5 (2.6) 29 (12.2)*Self-reported health (% good–excellent) 4299 (83.7) 472 (69.8)* 172 (68.8)* 141 (75.0)* 159 (66.8)*Current estrogen use (%) 985 (19.2) 89 (13.1)* 30 (12.0)* 24 (12.7)* 35 (14.7)BUA, dB/MHz (SD) 67.1 (16.5) 62.1 (17.1)* 62.3 (17.0)* 65.1 (16.7) 59.5 (17.2)*BMDcal, g/cm2 (SD) 0.381 (0.092) 0.345 (0.098)* 0.351 (0.104)* 0.361 (0.087)* 0.327 (0.098)*BMDfn, g/cm2 (SD) 0.636 (0.116) 0.601 (0.115)* 0.615 (0.120)* 0.609 (0.097)* 0.581 (0.121)*
CV, cardiovascular; BMDcal, BMD of the calcaneus; BMDfn, BMD of the femoral neck.*p<0.05 compared with women who were alive at the end of follow-up.
608 D. C. Bauer et al.
diabetes, cardiovascular disease, cancer and stroke didnot alter the relationship between BMD and mortality.
Low BMD was also associated with cause-specificmortality, with the exception of BMDfn and cardio-vascular mortality (RH = 0.99; 95% CI: 0.86, 1.14).
Additional Analyses
Independent Effects of QUS and BMD. Adjusting forBMDcal substantially reduced the association betweenBUA and mortality (Table 3). BUA was no longerassociated with total or cause-specific mortality inmodels that included both BUA and BMDcal. Forexample, after adjusting for BMDcal, BUA was nolonger associated with total mortality (RH = 1.07; 95%CI: 0.96, 1.21), cardiovascular mortality (RH = 1.16;95% CI: 0.95, 1.39), cancer mortality (RH = 0.96; 95%CI: 0.78, 1.18) or other causes of mortality (RH = 1.11;95% CI: 0.91, 1.36).
Lowest Quintile Versus the Other Four Quintiles. Ourresults were similar when mortality was analyzed as thelowest quintile of BUA or BMD versus the other fourquintiles (Table 4). For example, after adjusting for age,grip strength, weight, height, health status, estrogen use,smoking, physical activity, and history of hypertension,diabetes, cardiovascular disease, cancer and stroke, totalmortality was 46% higher (CI: 1.23, 1.74) among womenin the lowest quintile of BUA compared with the otherfour quintiles.
Effect of Age. To determine whether the associationbetween QUS and mortality was limited to very oldwomen, we repeated our analyses among two groups:those aged less than 80 years and those aged 80 yearsand older. We found a trend towards a strongerrelationship between BUA and mortality amongwomen younger than 80 compared with women over80 (RH = 1.28 vs RH = 1.15, respectively). However,when tested formally we found no evidence of astatistically significant interaction between BUA, ageand mortality (p = 0.12).
Results Among Women Who Did Not Fracture DuringFollow-up. During the follow-up period, 183 (3.2%)women experienced a hip fracture, and 885 (16%)experienced other nonspine fractures. When thesewomen were removed from the analyses, the associationbetween BUA, BMD and mortality was unaffected (datanot shown). For example, the adjusted relative risk oftotal mortality among women who did not report anyfracture during follow-up was 1.27 (95% CI: 1.16, 1.40)per 1 SD reduction in BUA, and 1.29 (95% CI: 1.18,1.42) per 1 SD reduction in BMDcal.
Fig. 1. Total mortality and cause-specific mortality by quintile of age-adjusted BUA, calcaneal BMD (BMDcal) and femoral neck BMD(BMDfn). The number of deaths appears above each quintile. pr-yr,person-years.
QUS Predicts Total and Cause-Specific Mortality as Well as BMD 609

Discussion
In this large prospective study of older women, we foundthat low QUS was associated with an increased risk ofmortality. The increased risk of mortality with low QUSpersisted even after adjustment for other factorsassociated with increased mortality, such as age,weight, strength and existing medical conditions.Among women with low BUA, cardiovascular mortality,cancer mortality and other causes of death were similarlyincreased, and our results were similar when women whofractured during follow-up were excluded.Our results are consistent with previous studies
examining the relationship between BMD and mortality[1–3]. For example, in a previous report from the SOF
cohort, Browner et al. [1] found that each 1 SD reductionin BMD of the radius or calcaneus was associated with a20% increase in mortality. Von der Recke et al. [2]reported that each 1 SD reduction in bone mineralcontent of the forearm in perimenopausal women wasassociated with a 43% increase in mortality. Our studyextends those results in that we found a similarrelationship between QUS and mortality. AlthoughBUA and BMD measurements are only modestlycorrelated with each other (r = 0.4–0.7), they appear tobe equally associated with mortality. We found noevidence that BUA was a better predictor of mortalitythan BMD.
The strengths of the associations between BUA, BMDand mortality were not only statistically significant but
Table 2. Multiply adjusted associations between BUA, BMD and mortality (per 1 SD reduction)
Site Relative hazard (95% confidence interval)a
Total mortality(n = 677)
CV mortality(n = 250)
Cancer mortality(n = 189)
Other mortality(n = 238)
BUAb 1.16 (1.07, 1.26) 1.19 (1.04, 1.37) 1.09 (0.93, 1.27) 1.23 (1.06, 1.42)BMDcalb 1.19 (1.09, 1.31) 1.17 (1.01, 1.37) 1.20 (1.00, 1.43) 1.26 (1.08, 1.48)BMDfnb 1.11 (1.01, 1.22) 0.99 (0.86, 1.14) 1.24 (1.04, 1.49) 1.18 (1.00, 1.39)
CV, cardiovascular; BUA, broadband ultrasound attenuation; cal, calcaneus; fn, femoral neck.a.Adjusted for age, grip strength, weight, height, health status, estrogen use, smoking, physical activity, and history of hypertension, diabetes,cardiovascular disease, cancer and stroke.b.Per 1 SD decrease, each site and outcome analyzed in separate models.
Table 3. Independent associations between calcaneal BUA, calcaneal BMD and mortality (per 1 SD decrease)
Site Relative hazard (95% confidence interval)a
Total mortality(n = 677)
CV mortality(n = 250)
Cancer mortality(n = 189)
Other mortality(n = 238)
BUAb 1.07 (0.96, 1.21) 1.16 (0.96, 1.39) 0.96 (0.78, 1.18) 1.11 (0.91, 1.36)BMDcalb 1.13 (0.99, 1.29) 1.06 (0.86, 1.29) 1.24 (0.98, 1.58) 1.16 (0.94, 1.45)
CV, cardiovascular; BUA, broadband ultrasound attenuation; cal, calcaneus; fn, femoral neck.a.Model includes both BUA and BMDcal, and is adjusted for age, grip strength, weight, height, health status, estrogen use, smoking, physicalactivity, and history of hypertension, diabetes, cardiovascular disease, cancer and stroke.b.Per 1 SD decrease.
Table 4. Multiply adjusted associations between BUA, BMD and mortality (lowest quintile vs the other four quintiles)
Site Relative hazard (95% confidence interval)a
Total mortality(n = 677)
CV mortality(n = 250)
Cancer mortality(n = 189)
Other mortality(n = 238)
BUAb 1.46 (1.23, 1.74) 1.28 (0.96, 1.73) 1.35 (0.95, 1.91) 1.87 (1.40, 2.49)BMDcalb 1.42 (1.19, 1.70) 1.39 (1.03, 1.87) 1.21 (0.84, 1.75) 1.75 (1.30, 2.35)BMDfnb 1.20 (1.01, 1.45) 1.13 (0.84, 1.53) 0.99 (0.68, 1.44) 1.49 (1.11, 2.00)
CV, cardiovascular; BUA, broadband ultrasound attenuation; cal, calcaneus; fn, femoral neck.a.Per 1 SD decrease.b.Adjusted for age, grip strength, weight, height, health status, estrogen use, smoking, physical activity, and history of hypertension, diabetes,cardiovascular disease, cancer and stroke.
610 D. C. Bauer et al.

of sufficient magnitude to be clinically meaningful.Although the relationship between BUA and mortality isnot as strong as that observed for age and mortality, therelationship between women in the lowest quintile ofBUA and all-cause mortality was similar to thatobserved between hypertension and mortality (about a25% increase).
Low bone mass may reflect low lifetime exposure toendogenous estrogens [15]. Others have hypothesizedthat low lifetime exposure to estrogens predisposeswomen to osteoporosis and cardiovascular disease, whilesimultaneously protecting them from hormone-relatedmalignancy [16–20]. However, our study finds thatmortality from cancer and other causes are alsoincreased among women with low QUS and BMD.Adjustment for exogenous estrogen use had little effecton the associations between BUA and mortality,suggesting the beneficial effects of high BUA are notthe result of hormone replacement therapy. Furthermore,although the interaction term was not statisticallysignificant, the associated between BUA and mortalityappeared to be somewhat stronger in women less thanage 80 years (RH = 1.28) compared with those aged >80years (RH = 1.15). These findings suggest that low QUSand BMD reflect a fundamental aspect of aging notspecifically tied to cardiovascular disease, cancer orother causes of mortality. Our findings are consistentwith the hypothesis that low QUS and BMD reflect anaspect of frailty that is in part independent of age and thepresence of common chronic medical conditions.
We used an older fixed-transducer, water bath QUSdevice that did not measure speed or sound (SOS) orother parameters that combine BUA and SOS. However,during the sixth SOF visit we measured QUS with theSahara, a newer dry device (Hologic, Waltham, MA). Inpreliminary analyses of the 81 deaths that have occurredsince the Sahara measurements (mean follow-up of 1.7years), the risk of death from any cause wasapproximately 50% higher for each 1 SD reduction inBUA (RH = 1.46; 95% CI: 1.14, 1.89), 30% higher foreach 1 SD reduction in SOS (RH = 1.28; 95% CI: 1.00,1.63) and 30% higher for each 1 SD reduction in QUI, acombined BUA and SOS parameter (RH = 1.33; 95%CI: 1.04, 1.70).
Our study has several other limitations. We attemptedto define a specific cause of death, but by the nature ofdeath certificates this classification was imprecise.Additionally, our study was comprised only of olderwhite women, and these results may not apply to othergroups. Future studies of this topic should carefullyexamine specific causes of mortality and determinewhether these finding apply to other populations,including men. Although it is unlikely that interventionsthat specifically increase BUA or BMD will reducemortality, this hypothesis needs to be examined further.
In summary, we found that, like low BMD, low QUSis associated with an increased risk of mortality. Thishigh risk of mortality is not limited to cardiovasculardisease, and is observed for both cancer and other causesof mortality. Furthermore, the higher risk of mortality
observed with low QUS or BMD is not attributable toother factors known to be associated with increasedmortality, such as weight loss or poor health status, nor isthe increased risk attributed to fracture-related mortality.Additional studies are needed to explain this interestingobservation and further elucidate the mechanism.
Acknowledgements. Supported by Public Health Service GrantsAG05394, AR35582, AR35583 and AR35584. The Walker-Sonixdevices used in this study were donated by the manufacturer. Thiswork was presented at the 2000 Annual Meeting of the AmericanSociety for Bone and Mineral Research in Toronto, Ontario.
References
1. Browner WS, Seeley DG, Vogt TM, Cummings SR. Non-traumamortality in elderly women with low bone mineral density.Lancet 1991;338:355–8.
2. von der Recke P, Hansen MA, Hassager C. The associationbetween low bone mass at the menopause and cardiovascularmortality. Am J Med. 1999;106:273–8.
3. Johansson C, Black D, Johnell O, Oden A, Mellstrom D. Bonemineral density is a predictor of survival. Calcif Tissue Int1998;63:190–6.
4. Gluer CC. Quantitative ultrasound techniques for the assessmentof osteoporosis: expert agreement on current status. TheInternational Quantitative Ultrasound Consensus Group. J BoneMiner Res 1997;12:1280–8.
5. Cheng S, Tylavsky F, Carbone L. Utility of ultrasound to assessrisk of fracture. J Am Geriatr Soc 1997;45:1382–94.
6. Phillipov G, Holsman M, Phillips PJ. The clinical role ofquantitative ultrasound in assessing fracture risk and bone status.Med J Aust 2000;173:208–11.
7. Bauer DC, Gluer CC, Cauley JA, et al. Broadband ultrasoundattenuation predicts fractures strongly and independently ofdensitometry in older women: a prospective study. TheOsteoporotic Fractures Research Group. Arch Intern Med1997;157:629-34.
8. Hans D, Dargent-Molina P, Schott AM, et al. Ultrasonographicheel measurements to predict hip fracture in elderly women: theEPIDOS prospective study. Lancet 1996;348:511–4.
9. Hans D, Arlot M, Schott A, Roux J, Meunier P. Ultrasoundmeasurements on the os calcis reflect more the microarchitectureof bone than the bone mass. J Bone Miner Res 1993;8(Suppl1):S156.
10. Bouxsein ML, Radloff SE. Quantitative ultrasound of thecalcaneus reflects the mechanical properties of calcanealtrabecular bone. J Bone Miner Res 1997;12:839–46.
11. Bauer DC, Browner WS, Cauley JA, et al. Factors associated withappendicular bone mass in older women. Ann Intern Med1993;118:657–65.
12. Ensrud KE, Cauley J, Lipschutz R, Cummings SR. Weightchange and fractures in older women. Study of OsteoporoticFractures Research Group. Arch Intern Med 1997;157:857–63.
13. Steiger P, Cummings SR, Black DM, Spencer NE, Genant HK.Age-related decrements in bone mineral density in women over65. J Bone Miner Res 1992;7:625–32.
14. Orwoll ES, Bauer DC, Vogt TM, Fox KM. Axial bone mass inolder women. Study of Osteoporotic Fractures Research Group.Ann Intern Med 1996;124:187–96.
15. Cummings SR, Browner WS, Bauer D, et al. Endogenoushormones and the risk of hip and vertebral fractures amongolder women. Study of Osteoporotic Fractures Research Group. NEngl J Med 1998;339:733–8.
16. Cauley JA, Lucas FL, Kuller LH, Vogt MT, Browner WS,Cummings SR. Bone mineral density and risk of breast cancer inolder women: the Study of Osteoporotic Fractures. Study ofOsteoporotic Fractures Research Group. JAMA 1996;276:1404–8.
QUS Predicts Total and Cause-Specific Mortality as Well as BMD 611

17. Olsson H, Hagglund G. Reduced cancer morbidity and mortalityin a prospective cohort of women with distal forearm fractures.Am J Epidemiol 1992;136:422–7.
18. Persson I, Adami HO, McLaughlin JK, Naessen T, Fraumeni JFJr. Reduced risk of breast and endometrial cancer among womenwith hip fractures (Sweden). Cancer Causes Control 1994;5:523–8.
19. Zhang Y, Kiel DP, Kreger BE, et al. Bone mass and the risk ofbreast cancer among postmenopausal women. N Engl J Med1997;336:611–7.
20. Barengolts EI, Berman M, Kukreja SC, Kouznetsova T, Lin C,Chomka EV. Osteoporosis and coronary atherosclerosis inasymptomatic postmenopausal women. Calcif Tissue Int1998;62:209–13.
Received for publication 16 March 2001Accepted in revised form 19 February 2002
612 D. C. Bauer et al.