
Quality Improvement Updates Foley Discontinuation Protocol ... · Perform perineal meatal care with...
41
Quality Improvement Updates Quality Improvement Updates Foley Discontinuation Protocol Foley Discontinuation Protocol Surgical Care Improvement Surgical Care Improvement Project Project Barbara J Martin, RN, MBA Barbara J Martin, RN, MBA Quality Consultant, Center for Clinical Improvement Quality Consultant, Center for Clinical Improvement
Transcript of Quality Improvement Updates Foley Discontinuation Protocol ... · Perform perineal meatal care with...

Quality Improvement UpdatesQuality Improvement Updates Foley Discontinuation ProtocolFoley Discontinuation Protocol
Surgical Care Improvement Surgical Care Improvement ProjectProject
Barbara J Martin, RN, MBABarbara J Martin, RN, MBAQuality Consultant, Center for Clinical ImprovementQuality Consultant, Center for Clinical Improvement
Indwelling Urinary Catheters Indwelling Urinary Catheters Insertion, Care and Maintenance, and Insertion, Care and Maintenance, and
DiscontinuationDiscontinuation
Urinary Tract Infection Reduction Task ForceUrinary Tract Infection Reduction Task ForceRoger Dmochowski, MD ChairRoger Dmochowski, MD Chair

Insertion Policy Key PointsInsertion Policy Key Points••
Urinary Catheters require an orderUrinary Catheters require an order
••
Clinical Indications for indwelling catheter:Clinical Indications for indwelling catheter:•
Urinary retention not relieved with intermittent catheterization
•
Current regional / epidural anesthesia
•
Terminal illness receiving comfort care or withdrawal of care
•
Stage 3 or greater pressure ulcers
•
Critical illness AND a need for accurate monitoring of urinary output
Care and Management Key PointsCare and Management Key Points
••
Assess patient especially for continued need q 12 hr; w/ Assess patient especially for continued need q 12 hr; w/ caregiver change; or per unit standardcaregiver change; or per unit standard
••
Perform perineal meatal care with soap & water @ least Perform perineal meatal care with soap & water @ least q 12 hr; after BM; & PRNq 12 hr; after BM; & PRN
••
Anchor foley & maintain unobstructed urine flowAnchor foley & maintain unobstructed urine flow••
Use strict aseptic technique when opening or accessing Use strict aseptic technique when opening or accessing (for specimen) drainage system(for specimen) drainage system
••
Maintain drainage system above floor and below patient Maintain drainage system above floor and below patient bladder bladder at all timesat all times
including transport.including transport.

Discontinuation Protocol Discontinuation Protocol Purpose and PolicyPurpose and Policy
Implementation Date September 15Implementation Date September 15••
Reduction in catheterReduction in catheter--associated complications, associated complications, including infections from indwelling urinary including infections from indwelling urinary catheterscatheters
••
Patients with indwelling urinary catheters are Patients with indwelling urinary catheters are assessed for continued need and catheters are assessed for continued need and catheters are discontinued when clinical indications are no discontinued when clinical indications are no longer present longer present
Discontinuation ProtocolDiscontinuation Protocol
••
An order is required for indwelling urinary An order is required for indwelling urinary catheterizationcatheterization
••
When an indwelling urinary catheter is When an indwelling urinary catheter is ordered, the provider may order the ordered, the provider may order the discontinuation protocol. discontinuation protocol.
••
If the discontinuation protocol is not used, If the discontinuation protocol is not used, a specific order is required for to remove a specific order is required for to remove the catheter. the catheter.

foley
Typing “foley”, “urinary”, “catheter”, & similar search words will bring up list of indwelling urinary catheter options in the upper right
window
New foley orderables
FOLEY-REMOVE DATE/TIME:______FOLEY-REMOVE PER PROTOCOLFOLEY-REMOVE BY PROVIDER ORDER


Discontinuation ProtocolDiscontinuation Protocol
••
Patients are assessed by an RN for clinical Patients are assessed by an RN for clinical indications for continued use of the indications for continued use of the indwelling urinary catheter:indwelling urinary catheter:•
Upon admission
•
Every shift or with change in caregiver•
Change in level of care

Discontinuation ProtocolDiscontinuation Protocol••
After the catheter is d/cAfter the catheter is d/c’’d, the patient is d, the patient is assessed at intervals to determine ability to void, assessed at intervals to determine ability to void, to empty the bladder, and to maintain to empty the bladder, and to maintain continencecontinence•
If the patient is unable to void within six hours
after
the catheter is removed, the nurse may obtain an order for straight catheterization
•
If the patient is incontinent, the nurse takes measures to assist with strategies to improve urinary control.

Discontinuation Key PointsDiscontinuation Key Points
••
Consider whether catheter is necessary Consider whether catheter is necessary prior to insertion prior to insertion
••
Default order is Default order is ““by provider orderby provider order””••
Ordering the protocol allows nursing staff Ordering the protocol allows nursing staff to assess need for catheter, and remove to assess need for catheter, and remove when need is no longer presentwhen need is no longer present
••
May order discontinuation at a specific May order discontinuation at a specific point in time (e.g., POD2 @ 0600)point in time (e.g., POD2 @ 0600)


ObjectivesObjectives
••
Review measures included in SCIP data Review measures included in SCIP data submission.submission.
••
Identify mechanisms for process review Identify mechanisms for process review and improvement relative to perioperative and improvement relative to perioperative care.care.
••
Describe internal monitoring for Describe internal monitoring for maintaining and improving compliance maintaining and improving compliance with surgical care metrics.with surgical care metrics.

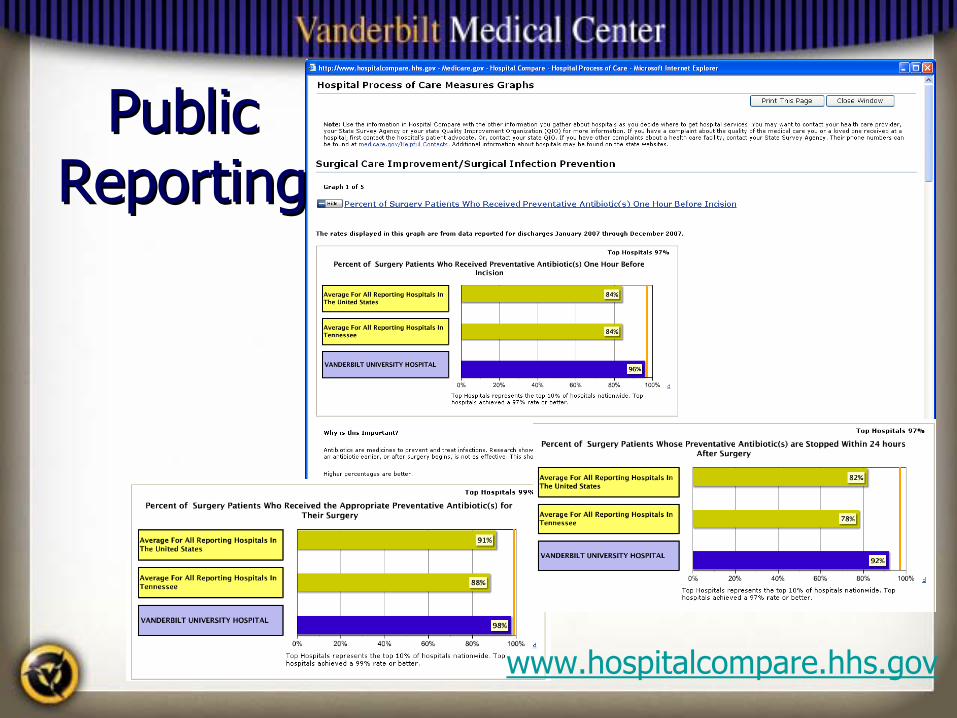
Core Measures: SCIPCore Measures: SCIP
••
Core measures are required by the Joint Core measures are required by the Joint Commission and based on CMS regulatory Commission and based on CMS regulatory requirementsrequirements
••
SIP (Surgical Infection Prevention) SIP (Surgical Infection Prevention) measures began in 2004 with antibiotic measures began in 2004 with antibiotic administration metricsadministration metrics
••
Changed to Changed to ““SCIPSCIP””
in 2006 with addition in 2006 with addition VTE and cardiac measuresVTE and cardiac measures

SCIP ProceduresSCIP Procedures ICDICD--9 Principal Procedure Code9 Principal Procedure Code
••
Coronary Artery Coronary Artery BypassBypass
••
Other Cardiac SurgeryOther Cardiac Surgery••
Colorectal SurgeryColorectal Surgery
••
HysterectomyHysterectomy
••
Total Hip ArthroplastyTotal Hip Arthroplasty••
Total Knee Total Knee ArthroplastyArthroplasty
••
Vascular SurgeryVascular Surgery••
Major SurgeryMajor Surgery

Inclusion / ExclusionInclusion / Exclusion
••
Case / metric exclusion based on clinical Case / metric exclusion based on clinical and administrative factorsand administrative factors•
Infection prior to induction of anesthesia
•
Chronic anticoagulation
••
Procedure Procedure ––
specific metricsspecific metrics•
Cardiac surgery: postop glycemic control
•
Colectomies: Postoperative normothermia

SCIP MetricsSCIP Metrics••
SCIP 1: Prophylactic antibiotic administered SCIP 1: Prophylactic antibiotic administered within 1 hour prior to incision (2 hours for within 1 hour prior to incision (2 hours for vancomycin or fluoroquinolone antibiotics)vancomycin or fluoroquinolone antibiotics)
••
SCIP 2: Appropriate prophylactic antibiotic SCIP 2: Appropriate prophylactic antibiotic selectionselection
••
SCIP 3: Discontinuation of prophylactic antibiotics SCIP 3: Discontinuation of prophylactic antibiotics within 24 / 48 hours after surgery end timewithin 24 / 48 hours after surgery end time
••
SCIP 4: Cardiac surgery patients with controlled 6 SCIP 4: Cardiac surgery patients with controlled 6 A.M. postoperative serum glucoseA.M. postoperative serum glucose

SCIPSCIP
MetricsMetrics
••
SCIPSCIP--6: Appropriate hair removal6: Appropriate hair removal••
SCIPSCIP--7: Colorectal surgery patients with 7: Colorectal surgery patients with immediate postoperative normothermiaimmediate postoperative normothermia
••
SCIPSCIP--VTEVTE--1 and 2: Patients with recommended 1 and 2: Patients with recommended venous thromboembolism prophylaxis ordered venous thromboembolism prophylaxis ordered and receivedand received
••
SCIPSCIP--CARDCARD--2: Patients on beta blocker therapy 2: Patients on beta blocker therapy prior to admission who receive a beta blocker prior to admission who receive a beta blocker during the perioperative periodduring the perioperative period

Abstraction MethodologyAbstraction Methodology••
Weekly case sampling by discharge date (80 Weekly case sampling by discharge date (80 cases per month)cases per month)
••
Abstraction from electronic and paper medical Abstraction from electronic and paper medical recordrecord
••
Monthly reports sent to administrators, chairs, Monthly reports sent to administrators, chairs, and chiefs for reviewand chiefs for review
••
Patient data reviewed by clinicians before Patient data reviewed by clinicians before submission to CMSsubmission to CMS
••
Charts selected by CMS quarterly for validationCharts selected by CMS quarterly for validation

A Note about AbstractionA Note about Abstraction••
Abstraction is validated internally as well as Abstraction is validated internally as well as externallyexternally
••
Information must be part of the patientInformation must be part of the patient’’s s permanent medical recordpermanent medical record
••
Conflicting documentation is abstracted as Conflicting documentation is abstracted as ““unable to determineunable to determine””
••
Must abstract based on most reasonable Must abstract based on most reasonable interpretationinterpretation
••
No No ““appealappeal””
process for individual casesprocess for individual cases

SCIP InfSCIP Inf--1 and 2 1 and 2 Antibiotic AdministrationAntibiotic Administration
••
Patients with documented infection are excludedPatients with documented infection are excluded••
Must be started within 60 minutes of incision Must be started within 60 minutes of incision (120 for vancomycin, fluoroquinolones)(120 for vancomycin, fluoroquinolones)
••
Administered in OR by anesthesia ( vanc Administered in OR by anesthesia ( vanc /quinolones which are given in holding)/quinolones which are given in holding)
••
Verify infusion is started prior to incisionVerify infusion is started prior to incision••
Vancomycin usually requires justificationVancomycin usually requires justification•
MRSA colonization
•
Beta-lactam allergy
x

Other Considerations: Preop ABXOther Considerations: Preop ABX
••
Patients on antibiotic therapyPatients on antibiotic therapy•
Appropriate coverage provided?
•
Redosing indicated?•
Is indication documented prior to surgery?
••
Appropriate weightAppropriate weight--based dosingbased dosing••
Redosing prior to incision when Redosing prior to incision when prophylaxis is given in the EDprophylaxis is given in the ED

SCIP
Inf
SCIP
Inf
-- 2 2
Antib
iotic
Sel
ectio
nAn
tibio
tic S
elec
tion
Specifications Manual for National Hospital Quality Measures Discharges 10-01-
09(3Q09) through 03-31-10(2Q10)

SCIP InfSCIP Inf--3 Antibiotic 3 Antibiotic DiscontinuationDiscontinuation
Cardiac Surgery Patients:Cardiac Surgery Patients:Five doses for antibiotics given every 8 hours; ORThree doses for antibiotics given every 12 hours; OR Seven doses for antibiotics given every 6 hours.
All Other Surgery Patients: All Other Surgery Patients: Two doses for antibiotics given every 8 hours; OROne dose for antibiotics given every 12 hours; ORThree doses for antibiotics given every 6 hours.

Antibiotic DiscontinuationAntibiotic Discontinuation
••
NoNo
indication for prophylaxis beyond 24 indication for prophylaxis beyond 24 hourshours
••
Therapeutic antibiosis must be justifiedTherapeutic antibiosis must be justified•
Document known or suspected infection
•
Signs, symptoms and interventions will not meet CMS requirements
••
If consulting service extends antibiotics, If consulting service extends antibiotics, reason must be documentedreason must be documented

Hair removalHair removal
••
If hair removal required, clippers or If hair removal required, clippers or depilatory must be useddepilatory must be used
••
All cases evaluatedAll cases evaluated••
Compliance for FY 2008: 100%Compliance for FY 2008: 100%
••
All razors removed from ORAll razors removed from OR••
Abstracted from OR Nursing RecordAbstracted from OR Nursing Record

Postoperative NormothermiaPostoperative Normothermia
••
Currently colorectal surgery onlyCurrently colorectal surgery only••
Within 15 minutes of leaving the ORWithin 15 minutes of leaving the OR
•• ≥≥
3636°°
C Route not specifiedC Route not specified
••
If no temp documented within 15 minutes, If no temp documented within 15 minutes, measure failsmeasure fails
VTE ProphylaxisVTE Prophylaxis
••
Mechanical and PharmacologicMechanical and Pharmacologic•
Procedure-specific
Cardiac and vascular excludedProcedure dictates required prophylaxis
•
Heparin / enoxaparin/ warfarin (requires order to be abstracted)
•
SCDs / TEDs•
Order within 48 hours, start within 24 hours
•
Preop administration meets criteria

Perioperative Beta BlockadePerioperative Beta Blockade••
All cases evaluatedAll cases evaluated
••
Patients on beta blockers prior to surgery Patients on beta blockers prior to surgery must have administration of a beta blocker must have administration of a beta blocker documented within 24 hours before documented within 24 hours before surgery through discharge from PACU, or surgery through discharge from PACU, or within six hours after surgery if not in within six hours after surgery if not in PACU postoperativelyPACU postoperatively

Beta Blocker DocumentationBeta Blocker Documentation••
Patients admitted day of surgeryPatients admitted day of surgery•
Document BB taken at home on the day of surgery.
•
If taken the night before, requires time taken••
Contraindications must be specifically Contraindications must be specifically documenteddocumented
••
Bradycardia (HR < 50) is a contrainidcationBradycardia (HR < 50) is a contrainidcation

SCIP Performance FY 2009SCIP Performance FY 2009Indicator FY O9
SCIP‐Inf‐1: Abx within 1 hour before incision 96.9%
SCIP‐Inf‐2 Appropriate proph abx 98.5%
SCIP‐Inf‐3 Proph abx d/c within 24 / 48 hours 96.1 %
SCIP‐Inf‐4 Controlled glucose: Cardiac surgery 90.2%
SCIP‐Inf‐6 Hair removal 100%
SCIP‐Inf‐7 Postop Normothermia: Colorectal surgery 75.4%
SCIP‐Card‐2 Perioperative beta blockade 81.5%
SCIP‐VTE‐1: VTE ppx ordered 99.0%
SCIP‐VTE‐2: VTE ppx received 98.0%
SCIP Perfect Care 88.4%

New SCIP Measures: Oct 2009New SCIP Measures: Oct 2009
••
SCIP Inf 9:SCIP Inf 9:
Urinary Catheter Removed on Urinary Catheter Removed on POD 1 or POD 2POD 1 or POD 2
ExclusionsExclusions•
Urologic, gynecologic, and perineal procedures
•
Infection prior to surgery•
ICU and on diuretics
•
Documentation of continued need for catheter
New SCIP Measures: Oct 2009New SCIP Measures: Oct 2009
••
SCIP Inf 10:SCIP Inf 10:
Surgery Patients with Surgery Patients with Perioperative Temperature MeasurementPerioperative Temperature Measurement•
Documentation of active warming intraoperatively, or documentation of at least one temperature > 36°C within the last 30 minutes prior to or the 15 minutes immediately after Anesthesia End Time.

Outpatient Surgery MeasuresOutpatient Surgery Measures
••
OP 6 Antibiotic TimingOP 6 Antibiotic Timing••
OP 7 Antibiotic SelectionOP 7 Antibiotic Selection
Included ProceduresIncluded Procedures•
Cardiac (PPM / AICDs)
•
Orthopedic/Podiatry•
Genitourinary
•
Gastric / Biliary
• Head and neck• Neurological• Gynecological• Vascular

External Metrics: Internal ReviewExternal Metrics: Internal Review

Maintaining ComplianceMaintaining Compliance
••
RemindersReminders•
Electronic forcing functions
•
Redose
reminders
••
Concurrent reportingConcurrent reporting•
VPIMS SCIP reports
•
M & M Review of failures•
Service chief follow-up of successes / failures
Surgical servicesAnesthesiology

Opportunities Opportunities ••
Antibiotic administrationAntibiotic administration•
Inpatient antibiotic redosing
/ timing / selection•
Emergency Department –> OR antibiotic timing•
Holding room to incision timing for administration
••
Glucose controlGlucose control•
Evaluate protocol compliance•
Monitor patient variables affecting hyperglycemia timing
••
Beta blockadeBeta blockade•
Preoperative instruction•
Documentation mechanisms in VPIMS
••
NormothermiaNormothermia•
Evaluate system and process issues r/t
equipment and documentation

Future SCIP Measures?Future SCIP Measures?
••
Expanded beta blockade requirementExpanded beta blockade requirement••
Intraoperative antibiotic Intraoperative antibiotic redosingredosing
••
Surgical site infection rateSurgical site infection rate••
Postoperative VTE RatePostoperative VTE Rate

Beyond SCIPBeyond SCIP
••
Wash your handsWash your hands••
Control the environmentControl the environment
••
Monitor and enforce infection prevention Monitor and enforce infection prevention practicespractices
••
Address breaches yourself, or have them Address breaches yourself, or have them addressedaddressed
••
Be constantly vigilantBe constantly vigilant
Every Patient, Every TimeEvery Patient, Every Time

SCIP Improvement InitiativesSCIP Improvement InitiativesR. Daniel Beauchamp, MD, FACS R. Daniel Beauchamp, MD, FACS
Chair, Section of Surgical SciencesChair, Section of Surgical Sciences
Michael S. Higgins, MD, MPHMichael S. Higgins, MD, MPHChair, Department of AnesthesiologyChair, Department of Anesthesiology
Nancye Feistritzer, MSN, RNNancye Feistritzer, MSN, RNAssociate Hospital DirectorAssociate Hospital Director
Stephanie Randa, RN, MHAStephanie Randa, RN, MHAAdministrative Director, Operative Services Administrative Director, Operative Services
Susie LemingSusie Leming--Lee, MSN, RN, CPHQLee, MSN, RN, CPHQDirector, Perioperative Quality ManagementDirector, Perioperative Quality Management
Thomas R. Talbot, III, MD, MPHThomas R. Talbot, III, MD, MPHChief Hospital EpidemiologistChief Hospital Epidemiologist


















