MDCT venography in the evaluation of inferior vena cava in Budd ...
Upload
jeffrey-cunninghamCategory
view
226download
0
Quality Assurance in Dural Venous Sinus Imaging – Comparison of
MR Venography Techniques
Dr. Jonathan Kim, Dr. Rafeeque Bhadelia, Dr. David Hackney, Dr. Rafael Rojas
Control #: 1700eEdE#: eEdE-39

Disclosures
• No financial disclosures to report.

Outline
• General diagnostic pitfalls of MR imaging of dural venous sinus thrombosis
• Acquisition factors and artifact profiles– Time-of flight– Phase Contrast– Contrast enhanced 3D MP-RAGE

Dural Venous Sinus Thrombosis (DVST)
• Relatively rare with an estimated annual incidence of 2-7 cases per million
• Clinical presentation is nonspecific and diagnosis is highly reliant on imagine
• Gold standard for diagnosis is cerebral venous angiography, an invasive technique
• Modern diagnostic technique has been largely supplanted with MR angiographic studies
• As DVST is potentially fatal, prompt diagnosis is key
1. Leach et al.

General Diagnostic Pitfalls
Normal anatomic variants: Right, left and codominant transverse sinuses. Sinus asymmetry should not be confused for occlusion.
2. Ayanzen et al.

General Diagnostic Pitfalls
• Flow gaps may be observed in the nondominant sinus and may be indistinguishable from thrombus on flow dependent techniques
2. Ayanzen et al.

General Diagnostic Pitfalls
• Normal structures including pacchonian granulations and chordae willisii demonstrate well defined filling defects
• Seen in at least 90% of patients
7. Leach et al.

General Diagnostic Pitfalls
• Venographic phase of a cerebral angiogram demonstrates preserved flow where MRV demonstrated a flow gap
2. Ayanzen et al.
Time-of Flight
• 2D-TOF MR venography is the most commonly used technique for evaluation of DVST
• Gradient echo sequence with imaging differential created by difference between saturated and non-saturated blood– Non-saturated blood entering the imaging slice creates in-
flow contrast– Arterial flow is nulled with a pre-saturation pulse adjacent to
the slab of interest• High sensitivity for slow-flow• Most sensitive to flow perpendicular to the image acquisition
plane (important technical factor)
7. Leach et al.

Time-of Flight
• 2D-TOF imaging is sensitive to slow flow, but there is a lower limit (roughly 3 cm/s)– Below this, flow gaps
become apparent• This can be minimized by
decreasing slice thickness– Signal loss is due to blood
pool spin loss before pulse repetition time, so imaging a smaller slice decreases the probability of signal loss
3. Rollins et al.
Time-of Flight
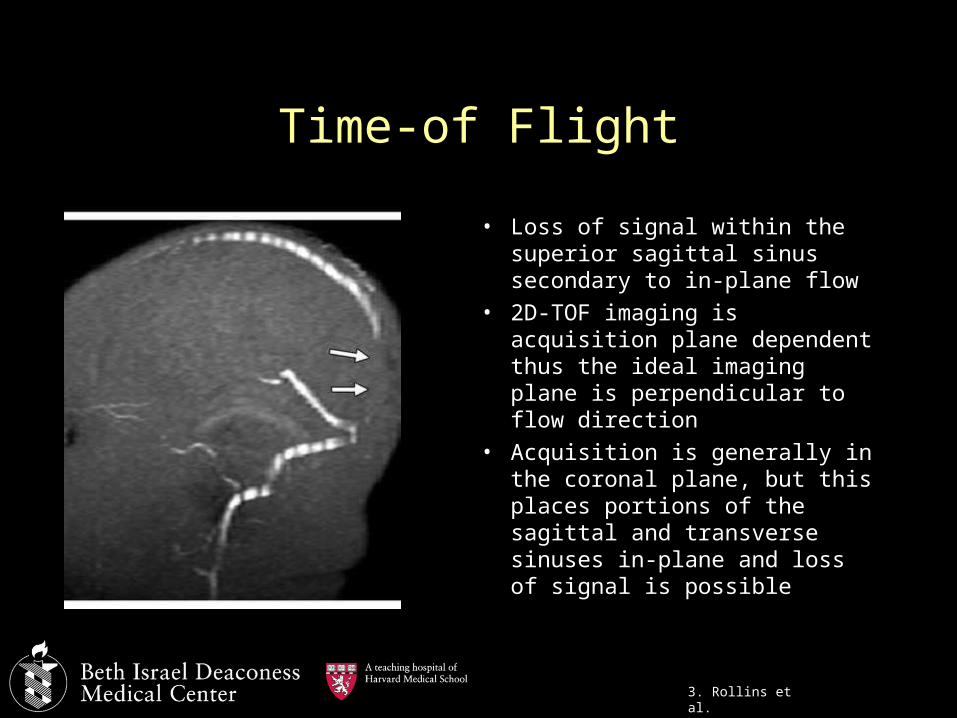
• Loss of signal within the superior sagittal sinus secondary to in-plane flow
• 2D-TOF imaging is acquisition plane dependent thus the ideal imaging plane is perpendicular to flow direction
• Acquisition is generally in the coronal plane, but this places portions of the sagittal and transverse sinuses in-plane and loss of signal is possible
3. Rollins et al.

Time-of Flight
• 2D-TOF acquired in the axial plane demonstrates in-plane signal loss in areas of the straight and transverse sinuses as opposed to the previous example of coronal acquisition
• Flow gaps demonstrated in at least 31% of TOF studies
7. Leach et al.

Time-of Flight
• T1 shine through from subacute thrombus may produce intravascular signal that can be confused for preservation of flow
7. Leach et al.

Phase Contrast
• Phase contrast images are sensitive to flow• Moving protons in a region of interest generate phase shift
artifacts in the plane of the magnetization gradient• Degree of phase shift is proportional to the velocity which is
then used to generate angiographic images
Phase Contrast
• Acquisition of phase contrast venography images depends on a priori selection of velocity encoding (VENC) values
• VENC serves as a center point to the estimated velocity of blood flow to be imaged
• If VENC is incorrectly selected, flows that are much higher or lower may not be seen
• VENC should be roughly 25% than expected Vmax for ideal imaging
• Since flow is not known prior to imaging, multiple acquisitions with varying VENC may be required causing increased imaging time
4. Lotz et al.

Phase Contrast
• 3D-PC images with VENC values of 15 and 40 cm/s, respectively demonstrate areas of signal loss when flow is too far outside the selected VENC range
5. Fera et al.

Phase Contrast
• Phase contrast images are not dependent on imaging plane and demonstrate excellent image quality with proper VENC selection

3D CE MP-RAGE
• Post-gadolinium 3D magnetization prepared rapid gradient-echo sequences depend on the T1 shortening effect of gadolinium to provide enhancement of intravascular structures
• As intravascular signal depends on contrast concentration, CE MP-RAGE is not susceptible to the artifact profile of TOF or PC such as vessel angle compared to the acquisition plane, nor is it related to flow velocities
• As gadolinium is required, some patient populations are not amenable to this technique, such as pregnant patients
6. Liang et al.

3D CE MP-RAGE
• Flow gap seen in the left transverse sinus on 2D-TOF whereas CE MP-RAGE clearly demonstrates intravascular enhancement of a hypoplastic vessel
• Patent venous sinus is confirmed on venous phase DSA
6. Liang et al.

3D CE MP-RAGE
• MP-RAGE is also useful for direct visualization of thrombus in conjuction with other sequences
• Apparent flow gap in 2D-TOF image is indeterminate, but clearly demonstrates thrombosis on MP-RAGE
6. Liang et al.

Summary
• DVST is a rare entity, but diagnostically important as early treatment is related to eventual outcomes
• TOF and PC are non-contrast, flow related techniques with acquisition parameters and artifact profiles that are important to keep in mind during interpretation
• 3D CE MP-RAGE is not flow dependent, and is potentially superior to TOF and PC, but requires gadolinium contrast
References
1. Leach, James L., et al. "Imaging of Cerebral Venous Thrombosis: Current Techniques, Spectrum of Findings, and Diagnostic Pitfalls 1." Radiographics 26.suppl_1 (2006): S19-S41.
2. Ayanzen, R. H., et al. "Cerebral MR venography: normal anatomy and potential diagnostic pitfalls." American Journal of Neuroradiology 21.1 (2000): 74-78.
3. Rollins, Nancy, et al. "Cerebral MR Venography in Children: Comparison of 2D Time-of-Flight and Gadolinium-enhanced 3D Gradient-Echo Techniques 1."Radiology 235.3 (2005): 1011-1017.
4. Lotz, Joachim, et al. "Cardiovascular Flow Measurement with Phase-Contrast MR Imaging: Basic Facts and Implementation 1." Radiographics 22.3 (2002): 651-671.
5. Fera, Francesco, et al. "Comparison of different MR venography techniques for detecting transverse sinus stenosis in idiopathic intracranial hypertension."Journal of neurology 252.9 (2005): 1021-1025.
6. Liang, Luxia, et al. "Evaluation of the intracranial dural sinuses with a 3D contrast-enhanced MP-RAGE sequence: prospective comparison with 2D-TOF MR venography and digital subtraction angiography." American journal of neuroradiology 22.3 (2001): 481-492.
7. Leach, James L., et al. "Imaging of Cerebral Venous Thrombosis: Current Techniques, Spectrum of Findings, and Diagnostic Pitfalls 1." Radiographics26.suppl_1 (2006): S19-S41.