Q mentum uarterly Health Care - Quality Compassqualitycompass.hqontario.ca/Documents/EN/Tools... ·...
34
Transitions of care Summer 2013 Q mentum uarterly Quality in Health Care
Transcript of Q mentum uarterly Health Care - Quality Compassqualitycompass.hqontario.ca/Documents/EN/Tools... ·...

Transitions of care
Summer 2013
Qmentumuarterly
Quality inHealth Care

Lean Green Belt Certification
Ottawa, Ontario (English) October 28–November 1, 2013 December 9–13, 2013 January 20-24, 2014 (15 day course) Use comprehensive tools and techniques to achieve the best results in your quality improvement initiatives. Facilitated by a Six Sigma Master Black Belt, this course employs a hands-on approach using quality improvement projects identified by the participants. Receive your Green Belt certification upon successful project completion.
Lean Yellow Belt Certification Ottawa, Ontario (English) November 4-7, 2013 This course has been very popular! Be among the increasing number of health care professionals from across the country that is certified by this Accreditation Canada and Six Sigma Canada partnership program.
Ethics at the Frontline Ottawa, Ontario (English) November 13 and 14, 2013 Are you pulled every which way? Sometimes feel ill-equipped to deal with ethical conflicts that arise at work? If so, you share the thoughts and feelings of many health care workers across the country. This workshop provides an opportunity to take a step back, reflect, and develop the tools to cope with these day-to-day pressures.
Ethics for Leaders Ottawa, Ontario (English) November 15, 2013 Health care organizations are special, values-rich enterprises where each aspect of practice and each decision represent our values, the things we really care about. This workshop places those values front and centre and challenges leaders to reflect on and develop the tools to put them into practice.
For more information visit the Accreditation Canada website under Educational Resources.

Accreditation Canada is an independent, not-for-profit organization that provides health services organizations across Canada and internationally with a rigorous and comprehensive accreditation process. It fosters ongoing quality improvement based on evidence-based standards and external peer review. Accredited by the International Society for Quality in Health Care, Accreditation Canada has helped organizations strive for excellence for more than 55 years.
Volume 6, Number 1Qmentumuarterly
Quality inHealth Care
Table of contents: Transitions of care
5 Improve safety at transitions
Wendy Nicklin
6 Improving patient transitions in British Columbia
Kelly McQuillen Gordon Hoag
12 Transitions in cancer care: What happens after treatment?
Lynn McCabe
18 Improved medication safety during transitions to long-term care
Cathy Coote Crystal Richter
24 Successfully transferring medication information during care transitions
Heather Howley
30 Building a community of stroke care
Sylvia Quant Sybil Edmonds Nadia Norcia Radovini Sharron Runions
34 Moving forward
Bernadette MacDonald

4
SUM
MER
2013
Volume 6, Number 1
Publisher:Accreditation Canada
Managing Editor:Jil Beardmore
Contributing Editors:Gail WilliamsSandra Morrison
Administrative Assistant:Jennifer Laviolette
LayoutGinette Laplante
President and CEO of Accreditation Canada:Wendy Nicklin
Vice-President, Business and Engagement:Paula McColgan
Vice-President, Innovation and Development:Bernadette MacDonald
Director, Business Development:Paul Payette
Legal Deposit:Qmentum QuarterlyLibrary and Archives CanadaISSN 1918-039X
Qmentum Quarterly: Quality in Health Care is an avenue for sharing expertise, innovation, and leading practices across Canada. The publication provides a forum for health and social services organizations that are committed to learning about improving quality and patient safety.
Qmentumuarterly
Quality inHealth Care

5
SUM
MER
2013
Patients face tremendous potential risks when they transition between care
providers or facilities. This can occur at points such as a shift change, or during major adjustments like moving from acute to long-term care or from paediatric to adult care. These high-risk points increase the vulnerability of patients to adverse events brought on by a gap in transition points during care.
There are many ways to improve safety at transition points, including implementing medication reconciliation and developing processes to share accurate information between health care providers across the continuum of care. When care is fragmented or poorly aligned, patients, their families, and health care providers suffer the consequences.
By focusing on these interfacing points in care, we can address the underlying ways in which our health care system is actually putting patients at risk. In this issue, the authors offer us innovative and effective ways to mitigate these risks to patients.
Kelly McQuillen and Gordon Hoag outline several initiatives that are improving patient transitions in British Columbia. They are the result of the Shared Care Committee’s work to foster and support effective connections between family practitioners and specialists. This is leading to the more effective movement of patients between care providers and settings.
Lynn McCabe offers a unique perspective on the transition from active to post-cancer care. For many patients, this is a
difficult transition, as they leave behind much of the support they received during active treatment. It can be a daunting time, and the PEI Cancer Treatment Centre is working to increase patient satisfaction around this shift in care.
Cathy Coote and Crystal Richter provide insight into the Saskatoon Health Region’s streamlined medication reconciliation process for clients moving from acute to long-term care facilities. They were able to decrease the number of steps in this process by 60%, and have also reduced the number of medication discrepancies experienced by clients.
Heather Howley presents information about the medication reconciliation Required Organizational Practices (ROPs) used in the Accreditation Canada Qmentum program. Major efforts are underway across Canada to raise the bar in terms of medication reconciliation at risk points.
Sylvia Quant, Sybil Edmonds, Nadia Norcia Radovini, and Sharron Runions talk about three programs at the Sunnybrook Health Sciences Centre that target transition points for stroke patients. Through a navigation tool, a peer-support program, and information sharing around job roles, they are working to improve patient experiences and outcomes.
These authors have faced common challenges, and their solutions can be applied to many health care organizations. I invite you to give some thought to
Introduction
Improve safety at transitions
Wendy NicklinPresident and Chief Executive Officer,Accreditation Canada

6
SUM
MER
2013
Improving patient transitions in British Columbia

7
SUM
MER
2013
Patients often face challenges at transition points, particularly when care is
fragmented (i.e., lacking effective coordination and communication between care
providers). The Shared Care Committee—a partnership of the British Columbia
Medical Association (BCMA) and BC’s Ministry of Health—is working to support
better connections between family practitioners and specialists. These physicians
are working together in their communities to identify and address local challenges
to the effective and seamless transition of patients between care providers and
settings. These Shared Care initiatives have had remarkable results thus far.
Kelly McQuillen Gordon Hoag
The effective transition of patients between care providers and settings is integral to improved
health outcomes. Patients sometimes face challenges at transition points, particularly when care is fragmented; they feel the impact of this disrupted care. This is particularly true for patients with chronic diseases and complex care needs. What’s more, disjointed care burdens taxpayers as it is inefficient and adds costs to the health care system.
With funding and project support from the Shared Care Committee—a partnership of the BCMA and BC’s Ministry of Health—many family and specialist physicians are working together to improve care. They are implementing projects in their communities to address local challenges to the effective and seamless transition of patients between care providers and settings.
The Shared Care quality improvement initiatives focus on patients who are moving:
1. Between community-based practitioners (usually from a family physician to a specialist)
2. Into, through, and out of acute care
3. From the paediatric care system into the adult care system
While transition settings vary, the approach to improving quality remains consistent: Shared Care initiatives are based on collaboration among those involved in the care process. While these are primarily family and specialist physicians, additional stakeholders include provincial health authority leaders, clinical support representatives, and patients and their family members.

8
SUM
MER
2013
Shared Care initiatives use a framework adapted from the Institute for Healthcare Improvement’s Triple Aim Initiative. The goal is to provide a positive heath care experience for physicians and patients, improve population health, and reduce the per-capita cost of care. The Shared Care Committee conducts ongoing evaluations of the initiatives at the provincial and local (i.e., project site) level.
Transitions among community-based practitionersA number of Shared Care initiatives improve access to input and care from specialists, and refine the flow between primary care practitioners and specialists.
Partners in CareIn the Partners in Care initiative, physicians are working to better coordinate the shared care of patients by revising referral and consult processes, shared care planning and re-referral criteria, diagnostic standards and communications, telephone advice protocols, and more.
These physician teams are able to develop, test, and implement new processes and systems and, in many cases, build on successful models of care being used elsewhere by other members of the Partners in Care initiative. More than 1600 family physicians and 200 specialists are involved in the initiative. Work is underway at 12 sites across BC, with projects being developed at another 12 sites. The evaluation of local referral and consult improvement projects has demonstrated an improved patient and provider experience as follows:
• Of the family physicians surveyed as part of a specialist telephone consult project, 60% said
using the service helped avoid unnecessary face-to-face patient consults, 32% said it helped avoid emergency department visits, 83% believed the service helped manage care for their patients, and over 90% were satisfied with the quality and efficiency of the telephone advice and would recommend this program to their colleagues (Araki & Lear, 2012).
• A local project to refine the computed tomography and ultrasound requisition process reduced the number of family physician referrals to the emergency department for these tests: 70% of respondents did not refer to the emergency department for the tests and 92% said the project made a positive difference in their experience and in their patients’ care (Penny Lane & Associates, 2011).
Rapid Access to PsychiatryThe Rapid Access to Psychiatry (RAP) initiative supports expedited access to psychiatric assessment (i.e., within 4-6 weeks), effective intervention, and follow-up for patients with mild to moderate mood disorders. With a referral from a family physician, and following an assessment by a psychiatrist, patients can attend drop-in psychiatric group medical visits (GMVs) for treatment, with the option of follow-up treatment via GMVs or email with the psychiatrists involved in the initiative. The model
This model of care is more than four times cheaper for severe cases than traditional outpatient department psychiatric care.

9
SUM
MER
2013
of care used in this initiative enables one full-time equivalent psychiatrist to assess 6.7 times as many new patients and conduct 553 more follow-up visits per annum than a traditional outpatient department psychiatrist. It is almost three times less costly, per annum, for moderate cases and more than four times cheaper for severe cases than traditional outpatient department psychiatric care.
Surveyed patients were satisfied with the wait time for referrals and very satisfied with the quality of medical information and consultations provided; 67% reported attending the GMVs because of faster access to psychiatric care. Family physicians indicated a high level of satisfaction with their patients’ prompt access to care (Araki, Bruce & Lear, 2011).
TeledermatologyThe Teledermatology initiative is improving access to specialist consults for family physicians in remote, rural, and urban areas, and eliminating the need for patients to travel long distances for in-person treatment by a dermatologist. An online “store and forward” process lets family physicians send photos of patients’ unusual skin conditions to a dermatologist for diagnosis and treatment recommendations. Close to 250 family doctors from BC use the online consult process and, as of May 2013, more than 380 consults had been done.
The average turnaround time for a Telederma-tology consultation is approximately 24 hours, and the online consult process, as of May 2013, had a diagnostic accuracy rate near 90%. Ninety-five percent of patients surveyed agreed
or strongly agreed that “store and forward” Teledermatology was more convenient than a traditional consult and 86% were satisfied with the Teledermatology consult. A cost analysis—based on 78 Teledermatology patients in a remote community—found that the program saved about $20,000 when compared with patients travelling to an urban centre for dermatology appointments (Barclay, 2012).
Transitions in CareThe Shared Care Transitions in Care initiative focuses on quality improvement processes that enhance the patient journey into, through, and out of acute care. The initiative currently comprises 12 projects at eight different sites throughout the province, with 18 additional projects expected to begin in 2013-14. While the clinical populations impacted range from infants to frail seniors, all Transitions in Care projects are aligned in their focus on quality transitions between care providers. This ideally includes preparation for a transition, a brief period of joint/shared care, and the transfer of clinical notes or discharge summaries (Moli et al., 2013). This transition process is distinct from the practice of transferring patients, which generally involves the termination of one service and the initiation of another; this becomes a transaction between services that lacks the qualitative aspects of therapeutic intent found in an efficient transition (Moli et al., 2013).
Youth TransitionsThe Shared Care Youth Transitions initiative aims to improve the transition from paediatric to adult care for youth and young adults (age 10-24) with chronic health conditions and/or disabilities.

10
SUM
MER
2013
In BC, youth can access paediatric care services until their eighteenth birthday, when they must transfer to adult care services provided by regional health authorities. Each year, approximately 1700 patients with complex conditions make this transition and face challenges that include:
• Adapting to a new culture of care in adult medicine
• Attaching to adult primary and specialist care physicians
• Accessing appropriate community-based health care resources
• A possible deterioration in their health status after their transfer from paediatric care
Family physicians, paediatric and adult sub-specialists, patients and their families, and allied health professionals are involved in this initiative.
Together, they are developing, prototyping, and evaluating processes and resources to improve:
• The transfer of medical information from paediatricians to family physicians and adult specialists
• The shared care of patients between family physicians and adult specialists
• Patient attachment to family physicians
SummaryTo generate effective solutions, everyone who is involved in the transitions process must be involved in any changes made to that process. When physicians and their health care partners are able to participate fully in quality improvement projects, the level of engagement, ownership, peer-to-peer support, and general enthusiasm is palpable and highly effective at bridging relationships across care settings.

11
SUM
MER
2013
The Shared Care Committee’s work to modify transition points between care providers and settings in BC is growing. As early successes and lessons learned are shared across project sites and across the suite of Shared Care initiatives, an increasing number of family and specialist physicians are becoming change-makers. They are working to improve health outcomes and to create a seamless patient journey through the health care system. Visit www.bcma.org/partners-patients for more information. Q
Kelly McQuillenKelly McQuillen is the Executive Director of Primary Health Care and Specialist Services, BC Ministry of Health, and Co-chair of the Shared Care Committee, a joint committee of the BC Medical Association and the Ministry of Health. She has worked at the director and executive director level in the federal, provincial, and territorial governments for the past 24 years and is committed to patient and provider partnerships in care, quality improvement, and system redesign.
Gordon HoagGordon Hoag, MD, FRCPC, is Medical Director of the Department of Laboratory Medicine, Pathology and Medical Genetics for the Vancouver Island Health Authority. He is also Co-chair of the Shared Care Committee, a joint committee of the BC Medical Association and the Ministry of Health. Dr. Hoag is also a clinical professor in the Faculty of Medicine at the University of British Columbia, and former President of the Canadian Association of Pathologists and the BC Association of Laboratory Physicians.
ReferencesAraki, Y., Bruce, R., Lear, S. (2011). Program evaluation of the MDABC psychiatric clinic on demand. Vancouver, Canada; British Columbia Alliance on Telehealth Policy and Research.
Araki, Y., Lear, S. (2012). Program evaluation of the PHC Shared Care Partnership: final report. Vancouver, Canada; British Columbia Alliance on Telehealth Policy and Research.
Barclay, S. (2012). Teledermatology for BC: A pilot project sponsored by the Shared Care Committee of the BCMA and Ministry of Health. PowerPoint presentation.
Moli, P., Ford, T., Kremaer, T., et al. (2013). Transfer and transitions between child and adult mental health services. Br J Psych, 202: s36-s40.
Penny Lane & Associates. (2011). Shared Care evaluation final report. C.O. Division of Family Practice. Unpublished.

12
SUM
MER
2013
Transitions in cancer care: What happens after treatment?

13
SUM
MER
2013
The transition from active to post-cancer treatment can be daunting for patients
who have come to rely on support networks associated with cancer care. The PEI
Cancer Treatment Centre (PEICTC) has worked since 2009 to make this transition
easier for patients, and has had excellent results in terms of patient satisfaction.
Most people assume that achieving clinical remission by the end of cancer treatment
is a happy and carefree occasion. Surprisingly, for many—if not most—cancer survivors, this is not the case. Dr. Elizabeth McKinley shared her feelings at the completion of her final radiation treatment:
“Ironically, I also cried because I would not be coming back to that familiar table where I had been comforted and encouraged. Instead of joyous, I felt lonely, abandoned, and terrified. This was the rocky beginning of cancer survivorship for me” (Rowland, 2006).
In 2009, a Cancer Patient Navigation program was implemented on Prince Edward Island. It aimed to address the needs of people diagnosed with cancer as they entered and left active cancer treatment.
In the fall of 2009, the Canadian Partnership Against Cancer (CPAC) invited the PEICTC to participate in their program, Cancer Transitions:
Moving Beyond Treatment™. It was originally developed by the Cancer Support Community and LIVESTRONG in the United States and was adapted for use in Canada by the BC Cancer Agency, in partnership with CPAC. PEICTC agreed to send two staff members—a social worker and a cancer patient navigator—to a workshop in Ottawa to be trained as facilitators.
The CPAC (2013) included “survivorship” in its strategic initiatives for 2007–2012 because:
“Physical, emotional, and financial challenges often persist after cancer diagnosis and treatment. These challenges are wide ranging and may include practical issues related to personal finances and employment, psychological struggles, strains on personal relationships, and the fear of recurrence. With close to one million cancer survivors in Canada, a number that is expected to increase to nearly two million by 2020, there is a growing requirement to address the needs of patients and their families when active treatment in the cancer system ends.”
Lynn McCabe
14
SUM
MER
2013
Cancer Transitions: Moving Beyond Treatment is an important addition to the navigation program, as it addresses crucial transition points. It supports the integration of services across the continuum of care for cancer survivors, as set out in the Accreditation Canada Cancer Care and Oncology Services Standards.
The program uses what developers refer to as a “patient-active approach,” meaning it helps patients become more informed, engaged, and in control as they participate in their care after active treatment. The first series was offered in Charlottetown in the fall of 2011 to support people transitioning out of active cancer treatment.
The PEI experienceTo quote the participant’s workbook, “Cancer Transitions: Moving Beyond Treatment was created by the Cancer Support Community and LIVESTRONG to support, educate, and empower people during the transition period following treatment—especially as people live longer and stronger lives after being treated for cancer.” The program covers the benefits of exercise, nutrition, emotional support, and medical management in six sessions. It is led by a facilitator and health professionals with expertise in each subject area. More detailed information is available on the Cancer Support Community website.
There was no budget in PEI for the Cancer Transitions: Moving Beyond Treatment program when it began. Participants were charged $20 to help defray the cost of workbooks and pedometers. Space and food were donated by local businesses, and the services of a yoga instructor were funded by a year-to-year grant
from Go!PEI, a community-based, healthy living program that still funds the activity portion of the program.
The first step in developing the program for PEI was to enlist the support of health professionals on staff at the PEICTC who would help deliver the program with a Cancer Patient Navigator as a facilitator. With specialty staff at the PEICTC, this step went smoothly from the beginning. The social worker and spiritual care professional presented “Session 3: Emotional Health and Well-Being: From Patient to Survivor,” and “Session 4: Nutrition Beyond Cancer” was offered by the dietitian at the Centre. The Nurse Practitioner facilitated “Session 5: Medical Management Beyond Cancer.”
When the program moved to smaller satellite centres in rural communities (e.g., Summerside, O’Leary), speaker recruitment became more challenging. As the program developed across the province, the presenters included staff from the Prince County Hospital (satellite oncology site for the PEICTC) and Health PEI staff in West Prince, along with a physiotherapist and local yoga instructors. The program includes detailed outlines and speaking notes for these presenters, along with slides for each session. This helps greatly in the recruitment of speakers and ensures the program’s consistency. The participant’s workbook also contains highly detailed information.
Why yoga?A review of some of the participants found that a number of individuals who had experienced recent and extensive breast surgeries had limited functional abilities, weight issues, or health concerns such as osteoporosis. As a result of these

15
SUM
MER
2013
challenges, the exercise component was adjusted to better meet the group’s needs. One of the oncologists at the PEICTC suggested yoga as an option. A yoga instructor with a background in kinesiology and experience as a physiotherapy assistant was recruited to provide a specialized yoga practice and present “Session 2: Exercise for Wellness—Customized Exercise.”
Subsequent research supports using yoga as an option for this type of group. A systematic review of randomized controlled trials indicates that yoga provides cancer survivors with significant reductions in distress, anxiety, and depression; moderate reductions in fatigue; moderate increases to their general quality of life; and serves an emotional and social function (Buffart, 2012).
Participant evaluation and feedbackParticipant evaluation of the Cancer Transitions: Moving Beyond Treatment program showed that 92% agreed or strongly agreed that the topics and materials were helpful.
The interplay of body, mind, and spirit involved in the yoga practice was an excellent match for the majority of the participants. Following the pilot, evaluation results showed that yoga was a very important part of the experience, with 94% of participants agreeing or strongly agreeing with the statement, “The exercise portion of the class was helpful for me.” Six percent were neutral. Sixty-eight percent mentioned yoga when asked which portion of the sessions they felt were most helpful.

16
SUM
MER
2013
Facilitator/speaker observationsParticipant concerns ranged from physical to emotional, practical, and spiritual issues. A fear of recurrence and cognitive changes were the most common. As suggested by Hewitt (2005), resuming the routine of work and family life is often challenging and anxiety about recurrence runs high at this time. For many, the group support was most helpful, as expressed by one participant who said, “To hear other people’s stories helped me not to feel so alone and especially knowing that some of my feelings were more common than I realized.”
The publication From Cancer Patient to Cancer Survivor: Lost in Transition (Hewitt, 2005), identifies four essential components of survivorship care:
1. Prevention and detection of new cancers and recurrent cancer
2. Surveillance for cancer spread, recurrence, or new cancers
3. Intervention for consequences of cancer and its treatment (e.g., medical problems such as lymphedema and sexual dysfunction, symptoms like pain and fatigue, psychological distress experienced by cancer survivors and their caregivers, and concerns related to employment and insurance)
4. Coordination between specialists and primary care providers to ensure that all of the survivor’s health needs are met (e.g., health promotion, immunizations, screening for both cancer and non-cancerous conditions, and the care of concurrent conditions)
Resuming the routine of work and family life is often challenging and anxiety about recurrence runs high at this time.
Traditionally, the health care system has focused on the first two components. However, programs like Cancer Transitions: Moving Beyond Treatment are being developed as a result of a growing awareness of the long-term consequences of cancer treatment and the psycho-social impacts of cancer during and after treatment. Cancer Transitions: Moving Beyond Treatment—Next Steps Toward Survivorship (a section from the program workbook) helps participants understand the role they can play in the fourth component. Many patients are not aware of their care plan, and recent research by Urquhart (2012) indicates that this situation is not unique to PEI. There are many organizations recommending that survivors receive a survivorship care plan (Kirsch, 2012), including The American College of Surgeons, the American College of Clinical Oncology, and the Office of Cancer Survivorship at the National Institutes of Health.
For many survivors and health care practitioners, the cancer diagnosis continues to be the focus even after treatment, sometimes to the detriment of their other health needs. Cancer care is also more and more affected by oncologist shortages in many parts of Canada, increasing numbers of survivors, and a trend of transferring follow-up care to family practitioners.

17
SUM
MER
2013
ReferencesBuffart, L.M., van Euffelen, J.G.Z., Riphagen, I.I., Brug, J., van Mechelen, W., Brown, W.J., et al. (2012). Physical and psychosocial benefits of yoga in cancer patients and survivors, a systematic review and meta-analysis of randomized controlled trials. BMC Cancer, 12: 559. Retrieved from www.biomedcentral.com/1471-2407/12/559/prepub.
Canadian Partnership Against Cancer: Priorities—Survivorship [Internet]. (2013). CPAC; Toronto, Ontario. Retrieved from www.partnershipagainstcancer.ca/priorities/2007-2012-initiatives/strategic-initiatives-2/survivorship-2/#_ftn1.
Hewitt, M., Greenfield, S., Stovall, E. (2005). Editors, Committee on Cancer Survivorship: Improving Care and Quality of Life. Institute of Medicine, National Research Council; Washington, DC. Retrieved from www.nap.edu/catalog.php?record_id=11468.
Kirsch, B. (2012). Many US survivors still lost in transition. The Lancet, 379: 1865-1866. Retrieved from www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60794-6/fulltext.
Urquhart, R., Folkes, A., Babineau, J., Grunfeld, E. (2012). Views of colorectal cancer survivors on their routine follow-up care. Current Oncology, 19; 294–301. Retrieved from www.current-oncology.com/index.php/oncology/article/view/1051/1040.
As survivors move through the patient-active process of the Cancer Transitions: Moving Beyond Treatment program, they develop an awareness of the importance of being informed and engaged in their own care. This helps them better navigate the many layers of the health care system throughout their journey as a cancer survivor. Q
Lynn McCabeLynn McCabe, BSc, MHSM, recently retired from the position of Provincial Cancer Patient Navigator for Health PEI at the PEICTC in Charlottetown. After receiving a BSc (Nutrition) from Acadia University, Lynn completed an internship in Community Nutrition at The Montreal Diet Dispensary. After working as a registered dietician in community, clinical, and mental health settings, she completed a Masters in Health Services Management. In 2009 she began working as a Cancer Patient Navigator. Her successor, Wendy Holmes, can be reached at [email protected].

18
SUM
MER
2013
Improved medication safety during transitions to long-term care

19
SUM
MER
2013
A team in Saskatoon significantly streamlined the Saskatoon Health Region’s medication reconciliation (Med Rec) process at transfer and discharge. Originally, there were 29 steps in the Med Rec process when a client was discharged from an acute care facility to a long-term care (LTC) home in Saskatoon. The team was able to reduce this number to 10, thereby saving time and money and reducing medication errors.
Communicating information about medications across transitions of care presents a challenge to caregivers and patients alike. This process—known as medication reconciliation or Med Rec—is an important patient safety initiative and is a Required Organizational Practice in the Accreditation Canada Qmentum program. When applied at all transition points, Med Rec helps provide accurate and comprehensive information about medications as patients move through the health care system.
Since 2006, the Saskatoon Health Region has implemented Med Rec on admission in its urban and rural acute care facilities. As this became an established practice within the health region, the necessity to develop a process for patients being transferred or discharged from these facilities became apparent. The Saskatchewan Ministry of Health and the Saskatoon Health Region prioritized the development of a process to
Crystal RichterCathy Coote
complete Med Rec for all clients being discharged from an acute care facility to a LTC home.1
The intent of Med Rec at transfer and discharge is to reconcile medications the client was taking prior to admission with those initiated, changed, or stopped during hospitalization. This helps ensure clients will receive the appropriate medications when they transition to another unit, another facility, or back to their home. Med Rec is meant to decrease confusion and errors resulting from therapeutic duplications, omissions, and unnecessary medications being prescribed.
The Med Rec Lead for the health region brought stakeholders together in early 2012 to form
1 The Saskatoon Health Region uses “patient” to describe a person in an acute care facility and “resident” to describe a person in a LTC home. For consistency, the authors use “client” in this article to describe a person in either an acute care facility or a LTC home.

20
SUM
MER
2013
a working group. It included representatives from hospital and community pharmacies, nursing, Seniors’ Health and Continuing Care, a physician representative, and the region’s Client/Patient Access Service (CPAS, which oversees the transition from acute care to LTC). With support from senior leadership, the working group began reviewing baseline practices and identified the following issues:
1. Approximately 29 Med Rec steps were required to discharge one client from an acute care facility to a LTC home in Saskatoon. Many of these steps required rework and workarounds for the health care professionals involved, which resulted in frustration for them, the client, and the client’s family.
2. When most clients discharged into LTC homes, they did not have a physician in place to oversee their care, and a discharge prescription was not provided. Therefore,
medications were not reaching newly admitted clients in a timely fashion. On average, there was a delay of 5.8 hours between when the client was admitted to the LTC home and the writing of admission orders. Approximately four medications that should have been administered to each client were missed on the day of their admission (range 0-16).
3. The receiving LTC physician had no familiarity with the client and would write the admitting orders based on the medication administration record (MAR) provided by the acute care facility. This often resulted in unnecessary medications being ordered, particularly “take-as-required” medications which were ordered in hospital, but never used. A number of these medications were unnecessary, and this had financial implications for the client.

21
SUM
MER
2013
4. Each client experienced an average of 2.25 unintentional discrepancies.
It was obvious that an improved process was required for clients transitioning into LTC. When piloting new methods for Med Rec at discharge, the following goals were critical:
1. Improving collaboration among health care team members
2. Providing a safe and consistent approach to Med Rec on client transfer
3. Ensuring the timely delivery of the correct medications
After several pilots, and having gathered lessons learned, the team settled on a process that was
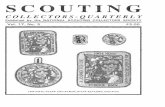
effective and efficient (it was piloted in November 2012). In the final process, only 10 Med Rec steps were required to discharge a client from acute care to LTC—a 60% reduction in steps (see Figure 1).
The final processHospital pharmacists now prepare the Med Rec discharge information for each client. Once complete, it is provided to the discharging physician to review and sign. This signed form becomes the client’s admitting orders at the new LTC home. These orders are valid for up to one month, allowing time for the new LTC physician to appropriately assess their new client. The goal is to have Med Rec completed at least one day
Figure 1
Acute Care MostResponsiblePhysician reviewsDischarge/TransferMedicationReconciliation Orderform and indicates:
- if agree with orderdocuments quantityand refill amount(maximum 1 month)- if disagree withorder – puts linethrough medication- add medicationssuch as PRNs ifrequired.
**Physician to signand date bottom ofform to make avalid prescription**
HospitalPharmacist
faxes allforms to
Acute CareMost
ResponsiblePhysician.
End ofprocess
LTCPhysicianwill visitpatient
within onemonth andreconcilemeds for
admissionto LTChome.
Patienttransferred
to LTCfacility
Hospital pharmacistcompletes Discharge/Transfer MedicationReconciliation Orderform after reconciling:- 24 hr MAR- Allergy/Intolerancerecord- Admission Med Recform and/or List ofMeds Prior toadmission.
Completes form with:- Patient Information- Name and faxnumber of: LTChome, Acute Carephysician, communitypharmacy
Also completes:- Fax cover letter tophysician- Pharmacist/NurseRecommendationsform- Fax cover letter toLTC Home
MAR
ReconciledDischarge/Transfer
MedicationReconciliation
Order form
Allergy/Intolerance
record
Pharmacist/Nurse
Recommendsform
CPAS orAcute Care
Nursecontacts
SaskatoonCity
Hospitalpharmacist
abouttransfer
Discharge/Transfer Medication Reconciliation Processfrom Acute Care to LTC (Urban) 2012
Acute CarePhysicianor supportstaff faxesforms to
CommunityPharmacy
CompletedDischarge/Transfer
MedicationReconciliation
Order form
Communitypharmacist
receivesDischarge/Transfer
MedicationReconciliationOrder form -dispenses
medications,prepares MARand sends toLTC home
with copy ofcompletedDischarge/Transfer
MedicationReconciliation
Order form.
Allergy/Intolerance
record
Pharmacist/Nurse
Recommendsform
Fax Coverletter
Fax Coverletter
Medication
LTC Nursewill receiveDischarge/Transfer
MedicationReconciliation
Order formand accept asvalid ordersfor 1 month.The orders
will be placedinto ordersection of
chart.
Bedavailablein LongTermCare(LTC)homeand
patient /familyaccept
Physician orphysician
support staffreceive fax.
**Forms areto be
reviewed andcompleted by
4:00PM theday they arereceived.**
HospitalPharmacistfaxes LTC
cover letter toLTC Home tomake home
aware ordersare coming
fromphysican.
LTC FaxCover letter
CompletedDischarge/Transfer
MedicationReconciliation
Order form
Pharmacist/Nurse
Recommendsform

22
SUM
MER
2013
• In acute care settings, pharmacists do not always receive discharge notices in time to complete safe and accurate Med Rec in the requested time frame; work with CPAS is ongoing to initiate a standardized notification process with appropriate time lines.
• Many Med Rec forms are faxed to physicians’ offices for signing, so engaging the office’s clerical staff members is necessary to ensuring that the forms reach physicians in a timely fashion. If this happens, there are usually fewer delays in forwarding the signed prescription to the community pharmacist. An updated version of the standard work document was developed to include a section for clerical staff.
• Due to the high number of staff members in many LTC homes, communication regarding new processes can be complex and can take time to spread. Continuous communication has therefore played an important role in making new initiatives successful. We also work with stakeholders to educate staff about these processes.
• Many LTC homes would not accept the Discharge/Transfer Med Rec Order form from the discharging physician; they would attempt to locate a LTC physician to admit the client and write orders. This resulted in unnecessary delays for the client. We have conducted educational outreach in this area and improvements have occurred.
We continue to refine our process, and have seen improvements since we initiated this work in 2012. Since that time, the number of “take-as-needed” medications ordered for newly admitted clients has decreased by 40%. The number of errors has also decreased from 2.25 discrepancies per client during discharge to almost zero.
prior to the client’s discharge, thereby providing time for the community pharmacy to receive the orders, dispense the medication(s), and make a delivery to the LTC home prior to the client’s arrival.
As this process was developed, standardized steps were created for each health care professional involved, including physicians, nurses, hospital pharmacists, CPAS, directors of care, and personnel not employed by the health region (community pharmacists and clerical staff at physicians’ offices). Educational tools (PowerPoint presentations, process map, and poster) were developed and used to educate staff about Med Rec changes in a seamless and timely manner. The availability of these tools also ensures sustainability and continuity as time passes and new health care professionals are hired.
Barriers and learning pointsWe continue to address the following challenges in the LTC setting:
• Engaging physicians in this process has been challenging because many who regularly discharge clients to LTC homes are only available on their unit once or twice per week. This results in difficulties in obtaining their review of Med Rec orders and their signature. We continue to explore alternatives around this process.
The number of errors has decreased from 2.25 discrepancies per client during discharge to LTC to almost zero.

23
SUM
MER
2013
Clients now receive their medications in a timely manner. The most recent audit found that 80% of clients had their medications available to them at their LTC home on the day of admission.
Since November 2012, this process has expanded to rural parts of the Saskatoon Health Region, where acute care nurses complete the Discharge/Transfer Med Rec Order form. In April 2013, the final roll out in the urban setting was completed within the Saskatoon Health Region. Since that time, all new admissions to LTC from acute care have been expected to have their discharge/transfer Med Rec completed prior to discharge, and medications available at the time of their admission to a LTC home.
The development of this process has been rewarding for everyone involved. Health care professionals have appreciated the decreased number of steps needed to achieve better care. Now that Med Rec has been streamlined, less money is being spent on unused medication upon clients’ transitions to LTC.
Reducing the steps involved at this transition point, while improving the process and working as a collaborative team has had a positive impact on client care. We have created a smooth discharge Med Rec process for the Saskatoon Health Region’s clients who are moving to LTC. Q
Cathy CooteCathy Coote, BSc(Pharm), CCRP, is a Clinical Manager in the Department of Pharmaceutical Services, Saskatoon Health Region. Cathy graduated from the Faculty of Pharmacy at the University of Manitoba and has also completed a Specialized Residency in Drug Information. She has worked in community and hospital settings, focussing predominantly in the areas of drug information, geriatrics, long-term care, and clinical research. She has been a Certified Clinical Research Professional (CCRP) since 2002.
Crystal RichterCrystal Richter, BSP, ACPR, is the Lead Medication Reconciliation Pharmacist for the Saskatoon Health Region. Crystal graduated from the College of Pharmacy and Nutrition at the University of Saskatchewan and completed the Accredited Canadian Pharmacy Residency program in Edmonton, Alberta. For the past seven years, Crystal specialized in cardiology and intensive care, and in 2012 she became the Lead Medication Reconciliation pharmacist. She is passionate about improving patient care through consistent, high-quality medication reconciliation.

24
SUM
MER
2013
Successfully transferring medication information during care transitions

25
SUM
MER
2013
Communicating accurate information about client medications is essential to providing safe care. Medication discrepancies and adverse drug events at transitions of care pose a significant safety risk, and medication reconciliation can improve patient care and outcomes at these points (Boockvar et al., 2003; Etchells et al., 2012; Feldman et al., 2012; Pronovost et al., 2003).
Medication reconciliation is a critical component of the care transition process.
It involves health care providers partnering with clients, families, and caregivers to achieve an accurate and complete transfer of medication information. Together, they conduct a systematic and comprehensive review of all the medications a client is taking, to ensure that any medications being added, changed, or discontinued are carefully assessed and documented. Medication reconciliation is recognized by the World Health Organization as one of its five patient safety challenges, by the Canadian Patient Safety Institute (CPSI) as a core objective, and by many health jurisdictions in Canada as a key patient safety priority.
Medication reconciliation was introduced into the Accreditation Canada Qmentum program in 2006, based on the recommendations of the Patient Safety Advisory Committee and emerging evidence that medication reconciliation reduced
medication errors. Updated versions will be released in 2014 to address the need for wider implementation throughout the continuum of care.
Since 2006, there has been a gradual, but steady increase in the number of health care organizations implementing and complying with medication reconciliation processes. In 2011, the medication reconciliation Required Organizational Practices (ROPs) showed the greatest improvement in compliance out of the 37 ROPs in the Qmentum accreditation program (Accreditation Canada, 2012).
Feedback from across the country indicates that these ROPs have been a crucial lever in advancing medication reconciliation. Canadian health care organizations participating in the Qmentum program are commended for their near 15-point increase in national compliance rates for all aspects of medication reconciliation (see Figure 1).
Heather Howley

26
SUM
MER
2013
Figure 1: Compliance with the Qmentum medication reconciliation ROPs
ROPCompliance (%)*
2009 2010 2011
Medication Reconciliation as an Organizational Priority (1 + 1 + a plan)
n/a 61 77
Medication Reconciliation at Admission
46 47 60
Medication Reconciliation at Transfer or Discharge
44 36 50
*Some variation is expected in ROP compliance rates from year to year because different organizations undergo on-site surveys each year. The data in Figure 1 is from the Canadian Health Accreditation Report.
Compliance data from 2012 on-site surveys will be available in the Canadian Health Accreditation Report to be published later this year.
Medication reconciliation ROPs in 2013Until the end of 2013, Accreditation Canada surveyors will assess compliance with medication reconciliation using the three ROPs listed in Figure 1. Medication Reconciliation as an Organizational Priority (found in the Leadership Standards and referred to as “1 + 1 + a plan”) requires organizations to implement medication reconciliation in one client service area at admission and one client service area at transfer/discharge. They must also have a documented plan to implement medication reconciliation
across the organization, including locations and timelines.
The other two ROPs—Medication Reconciliation at Admission and Medication Reconciliation at Transfer or Discharge—are found in the service-level standards and outline the steps of the medication reconciliation process, such as completing a “Best Possible Medication History” and communicating up-to-date medication lists to the next care provider. These two service-level ROPs are customized to reflect the differences in the medication reconciliation process in different sectors, namely acute care, ambulatory care, home care, and long-term care.
An ongoing challenge in enhancing Qmentum is to find that balance between achievability and excellence.
Revising the medication reconciliation ROPs in 2013-14The revised versions of these ROPs were released in January 2013, and will go into effect for on-site surveys starting in 2014.
Consultation was undertaken with CPSI, Institute for Safe Medication Practices (ISMP), medication reconciliation leaders from across Canada, and the Accreditation Canada Accreditation Program Advisory Committee, in order to enhance the ROPs and position them even more strongly as a continuing catalyst to improve medication safety. The consultations focused on better aligning the ROPs with the

27
SUM
MER
2013
National Medication Reconciliation Strategy,1 as well as creating opportunities to offer improved support to client organizations as they implement medication reconciliation.
An ongoing challenge in enhancing Qmentum is to find that balance between achievability and excellence. In health care organizations, a number of factors—support from leadership, access to pharmacists, physician engagement, and access to electronic medical records—all contribute to enabling the successful implementation of medication reconciliation. To reflect this reality, the Medication Reconciliation as an Organizational Priority ROP has been revised (and renamed). It will be called Medication Reconciliation as a Strategic Priority and will outline the steps needed to implement and sustain medication reconciliation throughout an organization.
Feedback has also indicated that the separate ROPs for medication reconciliation at admission and at transfer or discharge created artificial transitions and were barriers to the process of accurately communicating client medications across transitions of care. These two ROPs have been combined into one, called Medication Reconciliation at Care Transitions, that spans all care transitions and better reflects the process of providing care.
Expectations for on-site surveys from 2014 onwardThere were extensive consultations with national partners, client organizations, and surveyors throughout 2012 and this feedback was used to revise the medication reconciliation ROPs—
1 This national strategy is co-led by CPSI and ISMP Canada, and is supported by numerous health care organizations across the country, including Accreditation Canada.
changing their structure and widening the parameters around their implementation.
Increased scope of implementation
The definition of “service area” within the Accreditation Canada Qmentum program has been broadened to include all sites/units/floors within a service. In addition, full implementation of medication reconciliation will be added to the program in two phases:
• Phase 1: For on-site surveys between 2014 and 2017, medication reconciliation should be fully implemented in one service (using the definition above).
• Phase 2: For on-site surveys in 2018 and beyond, medication reconciliation should be fully implemented across all services.
Changes to the ROP structure
Medication Reconciliation as a Strategic Priority, the revised ROP for the Leadership Standards, focuses on the steps needed to implement and sustain medication reconciliation throughout an organization, including:
• A policy and process to accurately transfer information about clients’ medications
• Clear roles and responsibilities
• A well-defined implementation and sustainability plan
• Interdisciplinary implementation
• Documented evidence of staff education
• Monitoring of the medication reconciliation process
The Medication Reconciliation at Care Transitions ROP combines the requirements from the Medication Reconciliation at Admission

28
SUM
MER
2013
Your partner in reducing medication errors
1 Canadian Patient Safety Institute, Institute for Safe Medication Practices Canada, Canada Health Infoway, & Safer Healthcare Now, 2011
accreditation.ca
Mitigate the risk
Unintentional medication discrepancies continue to
put 40%-50% of Canadians admitted to hospital at risk
of harmful side effects.1
ReferencesAccreditation Canada. (2012). Canadian Health Accreditation Report — Required Organizational Practices: Emerging Risks, Focused Improvements. Ottawa, ON: Accreditation Canada.
Boockvar, K., Fishman, E., Kyriacou, C.K., et al. (2004). Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med., 164: 545-550.
Etchells, E., et al. (2012). The Economics of Patient Safety in Acute Care. Technical Report. Ottawa, ON: Canadian Patient Safety Institute. Retrieved from www.patientsafetyinstitute.ca.
Feldman, L.S., Costa, L.L., Feroli, E.R., Nelson, T., Poe, S.S., Frick, K.D., et al. (2012). Nurse-pharmacist collaboration on medication reconciliation prevents potential harm. J. Hosp. Med., 7: 396–401.
Pronovost, P., Weast, B., Schwarz, M., Wyskiel, R.M., Prow, D., Milanovich, S.N., et al. (2003). Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care, 18(4): 201-5.
and Medication Reconciliation at Transfer or Discharge ROPs. As before, the ROP outlines the steps of the medication reconciliation process. The sector-specific tailoring was retained and improved, as health care organizations indicated they appreciated the customization of medication reconciliation ROPs for different settings (acute care, ambulatory care, home and community care, long-term care, and substance misuse).
SummaryThe improvements made to the medication reconciliation ROPs help organizations of any size to integrate safe medication reconciliation processes into existing systems. To see the current ROPs, refer to the Accreditation Canada 2013 ROP Handbook; the revised medication reconciliation ROPs can be found in the Supplement to the ROP Handbook. Both documents are available here. Q
Heather HowleyHeather Howley, BSc, MSc, is a Health Services Research Specialist at Accreditation Canada. Her primary role is developing and providing ongoing support for the Required Organizational Practices, as well as developing an indicator strategy for Qmentum. Prior to joining Accreditation Canada in 2008, she worked for 10 years in academia, conducting epidemiological and health services research. Heather holds a Master of Science in Physiology from the University of Ottawa and has additional graduate training in epidemiology.

Your partner in reducing medication errors
1 Canadian Patient Safety Institute, Institute for Safe Medication Practices Canada, Canada Health Infoway, & Safer Healthcare Now, 2011
accreditation.ca
Mitigate the risk
Unintentional medication discrepancies continue to
put 40%-50% of Canadians admitted to hospital at risk
of harmful side effects.1

30
SUM
MER
2013
Building a community of stroke care

31
SUM
MER
2013
Three projects are making a tremendous difference in the lives of stroke patients who receive care at Sunnybrook Health Sciences Centre. A patient navigation tool, a peer-support program, and processes to enhance professional collaboration have all contributed to a more cohesive and smooth continuum of stroke care, particularly at transition points.
Sunnybrook Health Sciences Centre has recently implemented a new initiative to improve after-
care for patients who have had a stroke.
Last fall, as a Regional Stroke Centre, Sunnybrook began implementing the Toronto Stroke Networks’ “Transition Improvement for Continuity of Care (TICC)” initiative. This multi-site initiative improves communication among acute care, rehabilitation, and the community, with the ultimate goal of improving the patient experience and outcomes for those living with stroke.
“Stroke recovery is a complex process that involves extensive coordination through the care continuum and over time,” says Beth Linkewich, Director of the North and East Greater Toronto Area Stroke Network and the Regional Stroke Centre at Sunnybrook. “It is critical for us to identify and support transitions … to ensure access to timely and appropriate stroke care, including interprofessional stroke units, intense
rehabilitation, and outpatient programs. TICC is the glue that holds the system together.”
According to Jeff Upshaw, the Patient Care Manager at Sunnybrook’s Acute Stroke Unit on C4 of the Bayview campus, implementing TICC has strengthened their relationship with rehab facilities in the Greater Toronto Area (GTA). Overall, this creates a more streamlined transition process between acute care, rehabilitation, and the community.
The stroke team from Sunnybrook’s newest program area, St. John’s Rehab, also participates in this quality improvement initiative. “Through TICC, we have been able to open the lines of communication with our acute care partners and therefore ease our patients’ transition through the continuum of care,” says Jennifer Moebs, Occupational Therapist at St. John’s Rehab’s A3 Neurology and Oncology Rehab program.
As part of TICC, three projects were introduced in the fall and winter of 2012-13 to improve
Sylvia Quant Sybil Edmonds Nadia Norcia Radovini
Sharron Runions

32
SUM
MER
2013
transition points throughout the stroke patient’s care journey. Each project was based on information from interviews with people with stroke and their caregivers:
1. My Stroke Passport: A patient-mediated communication and navigation tool (in the form of a binder) that facilitates seamless, holistic, and meaningful care for people with stroke and their caregivers. The tool supports patient self-management, education, and care collaboration between the patient/caregiver and health care providers. It helps patients manage their own care by keeping track of their health, recovery, goals, and rehab plans as they move between hospitals and the community. It also includes a resource guide that provides information on stroke-related services.
2. Knowing Each Other’s Work (KEOW): A series of initiatives for health care providers from various disciplines to build their relationships, foster learning, and enhance meaningful collaboration and communication across the system. By learning from each other’s practice environments, KEOW enables health care providers to deliver the most seamless and optimistic care possible throughout patients’ journeys across the continuum of care. The goal is to ensure that essential conversations occur during clinical handover so health care professionals at all levels understand what has taken place, in order to better meet the needs of people with stroke and their caregivers.
3. Peers Fostering Hope: A volunteer program linking stroke patients and their caregivers with peer supporters who have also experienced a stroke. Through a partnership between the Toronto Stroke Networks and the March of Dimes Canada, peers can
connect and offer timely support to people and caregivers living with stroke, in either acute care or rehabilitation. This program aims to transform the image of stroke to one of possibility; it provides patients with hope, reassurance, and first-hand knowledge of what it is like to experience and live with a stroke. The process is meant to be reciprocal in that the peers gain self-confidence and a personal sense of worth and satisfaction, and are also able to reinforce their own coping strategies. Peer support groups have been shown to have many positive outcomes.
A full evaluation of TICC is set to be completed by March 2014. The results will provide specific indicators around the value and benefits of these projects, and will inform ongoing quality improvement. Currently, anecdotal feedback from patients, their families, and staff has been very positive, and seems to suggest that the benefits of the projects are greater than anticipated. Further planning is underway to implement, sustain, and expand TICC to other sites within the GTA.
At this point, mid-cycle, we are confident in having improved the quality of care for stroke patients at the Regional Stroke Centre at Sunnybrook. The centre has seen a culture shift
The centre has experienced a cultural shift toward more collaboration between sites, which in turn provides a strong survivor voice and more hopeful, optimistic care.

33
SUM
MER
2013
towards more collaboration between sites, which in turn provides a strong survivor voice and more hopeful, optimistic care.
For more information on these projects or other related initiatives, please visit the Toronto Stroke Networks’ website at www.tostroke.com. Q
Sylvia QuantSylvia Quant, PhD, MSc, BSc(PT), is a Rehab & Community Re-engagement Coordinator for the North and East Greater Toronto Area Stroke Network, and a lecturer at the Department of Physical Therapy, University of Toronto. Sylvia has been involved in provincial, regional, and local initiatives to enhance the integration of stroke best practices across the continuum of care. She was the Site Lead for coordinating the implementation of TICC within Sunnybrook Health Sciences Centre.
Sybil EdmondsSybil Edmonds, MA, has been a Communications Advisor at Sunnybrook Health Sciences Centre since 2011. She worked with the Brain Sciences Program for one year, and now manages communications for the hospital’s Women & Babies Program.
Nadia Norcia RadoviniNadia Norcia Radovini, MSc(PR), has been a Communications Advisor at Sunnybrook Health Sciences Centre for 11 years. She had previous communications roles at Credit Valley Hospital, the Insurance Bureau of Canada, Catholic Children’s Aid Society of Toronto, and the Canadian Hearing Society. Nadia manages communications for the hospital’s Brain Sciences Program and the Department of Nursing’s initiatives, and is a branding advisor.
Sharron RunionsSharron Runions, RN, MSc(N), CNN(c) is a Clinical Nurse Specialist with the North and East Greater Toronto Area Stroke Network. She has extensive experience in neuroscience nursing, with previous Clinical Nurse Specialist roles at the Montreal Neurological Institute and Hospital and the Montreal General Hospital of the McGill University Health Centre. Her current areas of practice include the Inpatient Stroke Unit and the Secondary Stroke Prevention Clinic at the Sunnybrook Health Sciences Centre.

34
SUM
MER
2013
34
Moving forward
In closing
Bernadette MacDonaldVice-President, Innovation and Development
We chose to focus on transitions of care in this issue in recognition of
the serious risks associated with health care at transition points. Because gaps in information exchange at care transitions are such clear points of risk across the care continuum, they are an ideal target for quality improvement initiatives. I hope you were inspired by the articles and discovered some solutions for issues you may be facing in your organization.
As always, our goal with Qmentum Quarterly is to provide opportunities for you to learn from your colleagues across Canada. This type of knowledge sharing is integral to our mission in driving quality improvement.
In addition to Qmentum Quarterly, we also offer education sessions aimed at strengthening capacity to implement quality improvement initiatives within organizations. To that end, we are running two of our most popular sessions again this fall—Lean Yellow and Green Belt training. They are designed for health care professionals who want to learn how to analyze and address inefficiencies.
Also, in partnership with the Canadian Standards Association, we will offer French webinars in September about improving the safety of endoscope reprocessing. English webinars on this topic were held in June and were extremely successful.
Finally, two ethics workshops will take place in Ottawa in November. The first is “Ethics at the Frontline,” intended for frontline care providers and mid-level management; the second is “Ethics for Leaders.” They focus on the unique challenges faced by these groups, and are opportunities to develop skills for delivering care within a robust and appropriate ethical framework.
Visit our website for more information about these workshops. I hope you will consider connecting with us in the fall to take advantage of these learning opportunities.
Until then, I wish you a wonderful summer!
Together in quality and safety,