Pure PBL, Hybrid PBL and Lecturing ... - BMC Medical Education
15
RESEARCH ARTICLE Open Access Pure PBL, Hybrid PBL and Lecturing: which one is more effective in developing cognitive skills of undergraduate students in pediatric nursing course? Mohsen Salari 1* , Amrollah Roozbehi 2 , Abdolvahed Zarifi 3 and Rohani Ahmad Tarmizi 4 Abstract Background: Nursing education in Iran has conventionally focused on lecture-based strategies. Improvements in teaching and learning over the years have led to an expansion of the pedagogies available to educators. Likewise, there has been a suggestion for a move toward more learner-centered teaching strategies and pedagogies that can result in improvement in learning. This study was undertaken to investigate the effects of Problem-Based Learning in developing cognitive skills in learning Pediatric Nursing among university students. Methods: In this quasi-experimental, posttest-only nonequivalent control group design, the subjects were undergraduate students who had enrolled in Pediatric Nursing II at Islamic Azad University in Iran. The experiment was conducted over a period of eight weeks, one two-hour session and two two-hour sessions. Two experimental groups, Pure Problem-Based Learning (PPBL) and the Hybrid Problem- Based Learning (HPBL), and one Lecturing or Conventional Teaching and Learning (COTL) group were involved. In the PPBL group, PBL method with guided questions and a tutor, and in the HPBL group, problem-based learning method, some guided questions, minimal lecturing and a tutor were used. The COTL group, however, underwent learning using conventional instruction utilizing full lecture. The three groups were compared on cognitive performances, namely, test performance, mental effort, and instructional efficiency. Two instruments, i.e., Pediatric Nursing Performance Test (PNPT) and Paas Mental Effort Rating Scale (PMER) were used. In addition, the two-Dimensional Instructional Efficiency Index (IEI) formula was utilized. The statistical analyses used were ANOVA, ANCOVA, and mixed between- within subjects ANOVA. Results: Results showed that the PPBL and HPBL instructional methods, in comparison with COTL, enhanced the students’ overall and higher-order performances in Pediatric Nursing, and induced higher level of instructional efficiency with less mental effort (p < 0.005). Although there was no significant difference in lower-order performance among the groups during the posttest (p = 0.92), the HPBL group outperformed the COTL group on the delayed posttest (p = 0.028). Conclusions: It may be concluded that both forms of PBL were effective for learning Pediatric Nursing. Moreover, PBL appears to be useful where there are shortages of instructors for handling teaching purposes. Keywords: Problem-based learning (PBL), Cognitive skills, Pediatric nursing course * Correspondence: [email protected] 1 Nursing Department, School of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran Full list of author information is available at the end of the article © The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Salari et al. BMC Medical Education (2018) 18:195 https://doi.org/10.1186/s12909-018-1305-0
Transcript of Pure PBL, Hybrid PBL and Lecturing ... - BMC Medical Education
RESEARCH ARTICLE Open Access
Pure PBL, Hybrid PBL and Lecturing: whichone is more effective in developingcognitive skills of undergraduate studentsin pediatric nursing course?Mohsen Salari1* , Amrollah Roozbehi2, Abdolvahed Zarifi3 and Rohani Ahmad Tarmizi4
Abstract
Background: Nursing education in Iran has conventionally focused on lecture-based strategies. Improvements inteaching and learning over the years have led to an expansion of the pedagogies available to educators. Likewise,there has been a suggestion for a move toward more learner-centered teaching strategies and pedagogies thatcan result in improvement in learning. This study was undertaken to investigate the effects of Problem-BasedLearning in developing cognitive skills in learning Pediatric Nursing among university students.
Methods: In this quasi-experimental, posttest-only nonequivalent control group design, the subjects wereundergraduate students who had enrolled in Pediatric Nursing II at Islamic Azad University in Iran. The experimentwas conducted over a period of eight weeks, one two-hour session and two two-hour sessions.Two experimental groups, Pure Problem-Based Learning (PPBL) and the Hybrid Problem- Based Learning (HPBL),and one Lecturing or Conventional Teaching and Learning (COTL) group were involved. In the PPBL group, PBLmethod with guided questions and a tutor, and in the HPBL group, problem-based learning method, some guidedquestions, minimal lecturing and a tutor were used. The COTL group, however, underwent learning usingconventional instruction utilizing full lecture. The three groups were compared on cognitive performances, namely,test performance, mental effort, and instructional efficiency. Two instruments, i.e., Pediatric Nursing PerformanceTest (PNPT) and Paas Mental Effort Rating Scale (PMER) were used. In addition, the two-Dimensional InstructionalEfficiency Index (IEI) formula was utilized. The statistical analyses used were ANOVA, ANCOVA, and mixed between-within subjects ANOVA.
Results: Results showed that the PPBL and HPBL instructional methods, in comparison with COTL, enhanced thestudents’ overall and higher-order performances in Pediatric Nursing, and induced higher level of instructionalefficiency with less mental effort (p < 0.005). Although there was no significant difference in lower-orderperformance among the groups during the posttest (p = 0.92), the HPBL group outperformed the COTL group onthe delayed posttest (p = 0.028).
Conclusions: It may be concluded that both forms of PBL were effective for learning Pediatric Nursing. Moreover,PBL appears to be useful where there are shortages of instructors for handling teaching purposes.
Keywords: Problem-based learning (PBL), Cognitive skills, Pediatric nursing course
* Correspondence: [email protected] Department, School of Nursing, Yasuj University of MedicalSciences, Yasuj, IranFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Salari et al. BMC Medical Education (2018) 18:195 https://doi.org/10.1186/s12909-018-1305-0

BackgroundNursing students encounter many clinical challenges incurrent healthcare atmosphere [1, 2]. It is unfortunatethat they often have no prior experience to deal withthese varying complex situations. More importantly,traditional teaching methods often fail to enable stu-dents to cope with these clinical conditions [3]. Subse-quently, these concerns call for an alternative approachwith higher efficacy in teaching nursing.Lecturing is the most common teaching strategy in the
nursing education, and problem based learning has notyet been of widespread use in Asia [4, 5]. In the currentnursing educational context of Iran, the main focus ofalmost all the universities for nursing education is onthe traditional teacher-based approach [6]. On the otherhand, it is often observed that the most importantbarriers to the implementation of student-centered strat-egies in Iran are students’ lack of familiarity with thenew strategies, inadequate skills in group work and ac-tive interaction, and the large number of students in aclass [7]. This is the case despite the fact that the worldtoday needs graduates who can take advantage of theirown diverse skills and in-depth or upper level academicknowledge in order to benefit from professional problemsolving and life-long learning. So, a comprehensivecurriculum should be accommodated to the future pro-fession and offers students learning opportunities to ac-quire problem solving skills so that they can improve thehealthcare systems they work with through appropriatedecision making [5, 8–11]. It is essential for nursing edu-cators to apply appropriate teaching methods to improvethe students’ performance in clinical nursing [12, 13].It is often argued that development, learning, and
higher mental functions take place through social inter-actions in a constructive environment by engaging in anactive process of discovering knowledge [14–17]. Also,student-centered strategies can enable the educators tohelp learners to be actively involved in promoting life-long learning, problem solving, critical thinking, groupprocess skills, creativity, information literacy, studentsuccess, and empowerment [18, 19]. Likewise, studentstend to prefer new approaches if they are more enjoy-able, have potentiality to grow enthusiasm and interestin students towards the course and its content [20, 21],enhance interactions between students and their instruc-tors, and increase students’ understanding of the coursecontent [22, 23].Likewise, educators need to serve as a facilitator or
apply a floating tutoring role in the context of smallgroups. Such a role is uncommon in traditional educa-tional approaches. One strategy in which the attentionshifts from teacher to student is Problem-Based Learn-ing (PBL). This strategy is able to get the graduates readyfor the uncertainties of future managerial practice and
facilitates the students’ construction and reconstructionof their own knowledge base [12]. In PBL, educators arefull partners in the learning process and not themajor holder of knowledge [24]. Some of the relatedstudies show that PBL can encourage students tolearn better and foster the retention and lifelonglearning skills that can be transferred into clinicalpractice and finally increases the quality of patientcare [18, 25–27]. PBL could help to bridge the gapsbetween education, practice, and knowledge developmentin professional schools including nursing, which is, inturn, able to prepare the learners for their future role asRegistered Nurses [28].PBL is highly flexible, and it can be used in different
ways and in different contexts [29, 30]. Some settingsuse the Traditional or Pure PBL strategy; some otherstend to modify the strategy by incorporating some trad-itional techniques. The results of these modificationscan improve the educational process for learners andinstructors, or result in unsuccessful attempts and apassing trend [31]. There are cases of institutions thathave successfully implemented PBL as a hybrid curricu-lum combined with other learning strategies like lec-tures, practical classes, etc. [32, 33]. In these contexts,educator, as a facilitator, strives to guide the students. Itis often argued that, the idea of scaffolding in the zoneof proximal development and the technique of facilitat-ing PBL groups are complementary processes [34]. Thisis because scaffolding takes shape through guidance, anddevelops faster to link students’ existing abilities withtheir intended goals [35]. This can result in a reductionof the learners’ cognitive load to easily solve the prob-lems which need high mental effort [36].It has been more than 40 years that PBL, as a stu-
dent-centered strategy, has been substituted for trad-itional ones, and there exists some empiricalresearch evidence in support of problem-based learn-ing [22, 33, 37–39]. Nevertheless, some researchfindings and meta-analyses have revealed a numberof gaps in the PBL literature. For instance, the re-sults were mixed and the performance on the examsof the fundamental courses of the students experien-cing PBL strategies appeared to be lower than thatof the students exposed to conventional approaches[5, 40–43]. Also, little has been done to reveal whatexactly takes place in a PBL class to nurture the necessaryskills. Moreover, to the best of our knowledge, no researchhas been carried out to compare the outcome of the appli-cation of Pure Problem-Based Learning (PPBL) andHybrid Problem-Based Learning (HPBL) strategies inteaching Pediatric Nursing (PN) course. In addition, noresearch has yet been done on the relevance of cognitiveload theory and instructional efficiency in nursing educa-tion in Iran [7].
Salari et al. BMC Medical Education (2018) 18:195 Page 2 of 15

The purpose of this study is, therefore, to investigatethe cognitive effects of PPBL, HPBL, and ConventionalTeaching and Learning (COTL) methods on learningPediatric Nursing.
MethodsStudy designThis study has adopted a quasi-experimental posttest-onlynonequivalent control group design to examine the effectsof PBL instructional strategies on measures of perform-ance, mental effort and instructional efficiency.
Participants, setting and measuresThe accessible population in this study consisted of allthe junior nursing students who attended the coursePediatric Nursing (PN) II in two branches of Islamic AzadUniversity (IAU) in Yasuj and Gachsaran, Kohgiluyeh-BoyerAhmad (KBA) province, Iran.The instructional strategies such as PPBL, HPBL, and
COTL as the independent variables and performance,mental effort and instructional efficiency as the dependentvariables were considered. In addition, threats to in-ternal and external validity were taken into accountand controlled. It should be pointed out that the ex-periment was conducted over a period of 8 weeks.
Inclusion criteriaThe participants were junior nursing students who hadpassed Pediatric Nursing I. They, however, had not re-ceived any training on problem-based learning beforethe main experiments.
Exclusion criteriaThe exclusion criteria in the study were missing two ormore class sessions, refusing to take one of the testsadministered, and failing to complete the questionnaires.It should be pointed that no participant appeared tohave these criteria.
Baseline testSince all the participants had already passed the PN (I)as a prerequisite course, their PN (I) scores were com-pared to make sure that they had similar prior PN know-ledge. Likewise, the students’ scores of Prior PerformanceTest on the three topics of PN course which had beentaught before the experiment were used as covariate toascertain that the students in all three groups were similarin their PN course knowledge.
SamplingThe sampling method was multistage cluster. At first,one of the regions of all the 13 regions of IAU was se-lected purposively. Then from the three provinces of thisregion, KBA province was chosen randomly. Among the
five IAU universities in KBA province, Gachsaran andYasuj Universities had between two to three classes ofabout 30 to 40 Junior Nursing students in each semester.So, three out of the five intact classes in these univer-sities were chosen by the fish-bowl method. Subse-quently, they were randomly assigned to the threegroups of the study, i.e., PPBL = 30, HPBL = 30 and COTL= 35. These students were of the same socio-economicstatus, ethnic background and common abilities [44].These classes were tested for homogeneity through com-paring their scores on PN I and Prior Performance Test.
Instruments of the studyThe Pediatric Nursing Performance Test (PNPT) andThe Paas Mental Effort Rating Scale (PMER) were utilizedas the instruments. In addition, the two-DimensionalInstructional Efficiency Index (IEI) was used to calculatethe instructional efficiency. The PNPT comprised 22multiple-choice items in order to assess the lower-ordercognitive domain performance and 22 open-ended ques-tions to determine the higher-order cognitive domainperformance. One point was assigned to each correctanswer of the multiple-choice items and three points tothe open-ended questions. Therefore, the overall perform-ance test for the PNPT ranged between 0 and 88. Thehigher-order cognitive domain performance referred tostudents’ ability to analyze, synthesis, and evaluate the PNproblems, while the lower-order cognitive domain per-formance referred to students’ ability to recall, compre-hend, and apply [45, 46] the PN problems. Hence, thetotal scores for low and higher-order cognitive domainswere 22 and 66, respectively.The PMER was used to measure the cognitive load by
recording the perceived mental effort which was exertedto solve the problems given during the experiments.This is a 9- point symmetrical Likert scale measurementthrough which subjects rate their mental effort used inperforming a special learning task [47]. The numericalvalues and labels assigned to the categories ranges fromvery, very low mental effort (1) to very, very high mentaleffort (9). Moreover, two kinds of subjective rating ofmental effort were also employed. Once, the subjectiverating of mental effort was given during the learning inthe assessment phase for each main topic. Once more itwas given during the test phase. The mental effort perproblem or question was obtained by dividing the per-ceived mental effort by the total number of problemstried at each assessment phase during the learning andthe test phases.Moreover, the two-dimensional (two-D) IEI [48] was
applied to compare the effects of different instructionalconditions on learning as instructional efficiency. Forthis purpose, the grand mean was subtracted from eachscore and the result was divided by the overall standard
Salari et al. BMC Medical Education (2018) 18:195 Page 3 of 15

deviation yielding corresponding z-scores for effort (R)and performance (P). Finally, a performance efficiencyscore, E, was computed for each participant using theformula E = [(P-R)/2½]. High efficiency was indicated bya relatively high test performance in combination witha relatively low mental effort rating. In contrast, lowefficiency was indicated by a relatively low test per-formance in combination with a relatively high mentaleffort rating.
Pilot studyIn this study, a pilot study was conducted to validate theexperimentation procedures and process. Besides, theinstruments used in the experiments were validated, andtheir reliability was ascertained. Besides, some experi-mental evidence of the appropriateness of the PediatricNursing topics in the learning area of organ dysfunctionwas provided. It also presented a sound basis for struc-turing the practice and evaluation phases incorporatingPBL strategy in the teaching and learning of organ dys-function in Pediatric Nursing.In the pilot study, the researcher offered the same
topics of Pediatric Nursing to a group of 40 junior nurs-ing students of one intact class who were not includedin the actual study. Then the questions on the topicswere given to the students to assess their mental efforts.This enabled the researcher to evaluate the validity, reli-ability, item difficulty, clarity, and feasibility of the testitems for the experiment. The Content Validity Ratio(CVR) was (0.99), the reliability of the multiple-choicetests were 0.81 (KR 20 was used), and the reliability ofthe open-ended questions were 0.88 (Cronbach’s alphawas used). In addition, item difficulty and discriminationindices were shown to be appropriate, ranging from .32to .70 and .92 to .94, respectively. In addition, usingCronbach’s alpha, the reliability of the mental effort forlower-order questions, higher-order questions and thetotal questionnaire were calculated to be 0.92, 0.94, and0.96, respectively.
Training curriculumThe PN core course is given to junior nursing students.It focuses on caring for children suffering from variousphysiological and system disorders. Its content consistsof nine main topics about disturbance or dysfunction indifferent systems or organs and their nursing care, fromwhich the four high prevalent conditions such as dis-turbance of fluid and electrolytes, renal dysfunction, re-spiratory dysfunction, and gastrointestinal dysfunctionwere selected for intervention [49, 50].The course plans, lesson plans, scenarios and Patients
Information Sheets (PISs), and tests to provide the gen-eral guidelines for teaching the topics on PN for conven-tional, PPBL, and HPBL strategies, and timetable for all
the groups were prepared in advance. Each set of thelesson plans involved five phases of induction, acquisi-tion, practice, closure, and assessment.In PPBL and HPBL, each group had a leader and a
scriber to manage the group activities and take note oftheir performance, respectively. For the PPBL group, thefacilitator started the induction phase by delivering thetrigger to the students at the introduction of each maintopic for about 5–10 min. He continued the rest of thesessions by asking the learners to recall the materialslearned and presenting the information about the relatedproblem to the class. In the acquisition phase, the facili-tator managed to give some PISs to the students basedon their needs. Then the students detected the conceptsby inquiry, self-directed learning and group discussion,worked on trigger to separate known from unknownissues, extracted learning issues during the brainstorm-ing, did research to find the target unknown variables,and recognized all the resources and information theyneeded to solve the problem. Next, they figured out thebest way to achieve the main goal based on the informa-tion gathered (hypotheses generation process) andgenerate the most viable solutions. In the following ses-sions, the results of each individual’s search had to becommunicated to the group members so that the datacould be analyzed and incorporated into the process ofproblem solving. After several cycles of data collectionand analysis, possible solutions to the problems weregenerated and formulated. Finally, the students exam-ined the outcome of their solutions. This general subjectpresentation took for 75–95 min depending on thesessions and the methods that were used.In the practice phase, the facilitator reinforced the
understanding of the students by discussing the similar-ities and differences among PISs, eliciting performanceand justification of the decision made in about 5 min. Inthe closure phase, the important concepts about the sce-nario were highlighted or presented by the students inabout 10–15 min. After each main topic, the assessmentquestions were given to the students to process, workand present the problems individually, and discuss themwith the whole class during 10 min.For the HPBL group, the induction phase started with
an example related to the real world problems of con-cern to the learners so that they could take ownership oftheir learning. For example, a picture of a child withsunken eyes was first showed to the students for 5–10 min as a trigger to gain their attention. Then somegeneral subjects such as biological development, asses-sing child with highlighting the differences betweenchildren and adults for each specific organ dysfunctionwith some examples were presented and discussedthrough mini-lectures in 10 min in conjunction withprior knowledge and scenarios. Moreover, at the end of
Salari et al. BMC Medical Education (2018) 18:195 Page 4 of 15

each HPBL lesson, a short corrective feedback sessionand summarization of about 15 min were provided bythe lecturer. The rest of the specific topics were, how-ever, presented as in the PPBL strategy through triggersunder the guidance of the facilitator.In the control group, the lecturer informed the stu-
dents of the objectives of the lesson and gave them anexample to gain their attention and activate their priorknowledge. In next sessions, the facilitator started theinduction phase by asking the students to recall the ma-terials learned and continued to lecture in the acquisi-tion phase in a whole-class instruction by explaining thePN concepts and discussing the steps of processingnursing problems related to the acquired concepts. Inthe practice phase, the students were asked to processthe problem individually and highlight the importantaspects. Then, the lecturer handled the discussion ofproblem solving and made some possible conclusions ofthe lesson. Finally, at the end of each main topic, eachstudent was required to assess and solve the problemsusing paper and pencil method. The content and the for-mat of the assessment were the same for all the groups,nonetheless (see Additional file 1).
Procedures and data collectionThis study was conducted during the first semester ofthe 2010/11 academic year. First, after assigning the par-ticipants to three groups, a general briefing sessionabout the strategy was held, and then the trainingsessions on PPBL and HPBL strategies for two experi-mental groups were run. Further, it was explained andillustrated to all the students how to use the PMER.After that, the experimental groups received teaching onorgan dysfunction in Pediatric Nursing through thePPBL and HPBL strategies for 8 wk while the controlgroup was exposed to only conventional whole-classinstruction. All the three groups had similar conditionsin terms of the content materials and contact hours.Altogether, 4 main topics were covered during 12two-hour sessions in the study. After covering each ofthe four topics, the students were assessed for theirlearning rate of the contents. They were also required torate the amount of mental effort they exerted for eachproblem right after each question.At the end of the experiment, the PNPT and PMER
were administered. Next, the Instructional Efficiency wasestimated by two-Dimensional IEI. For each question inPNPT, the PMER was printed at the end of the question.After each question, the students were required to indi-cate the amount of mental effort invested for thatparticular question by responding to the nine-point sym-metrical scale. Finally, a delayed posttest was adminis-tered 8 wk after the experiment to assess their retentionof the materials [51]. The delayed posttest included the
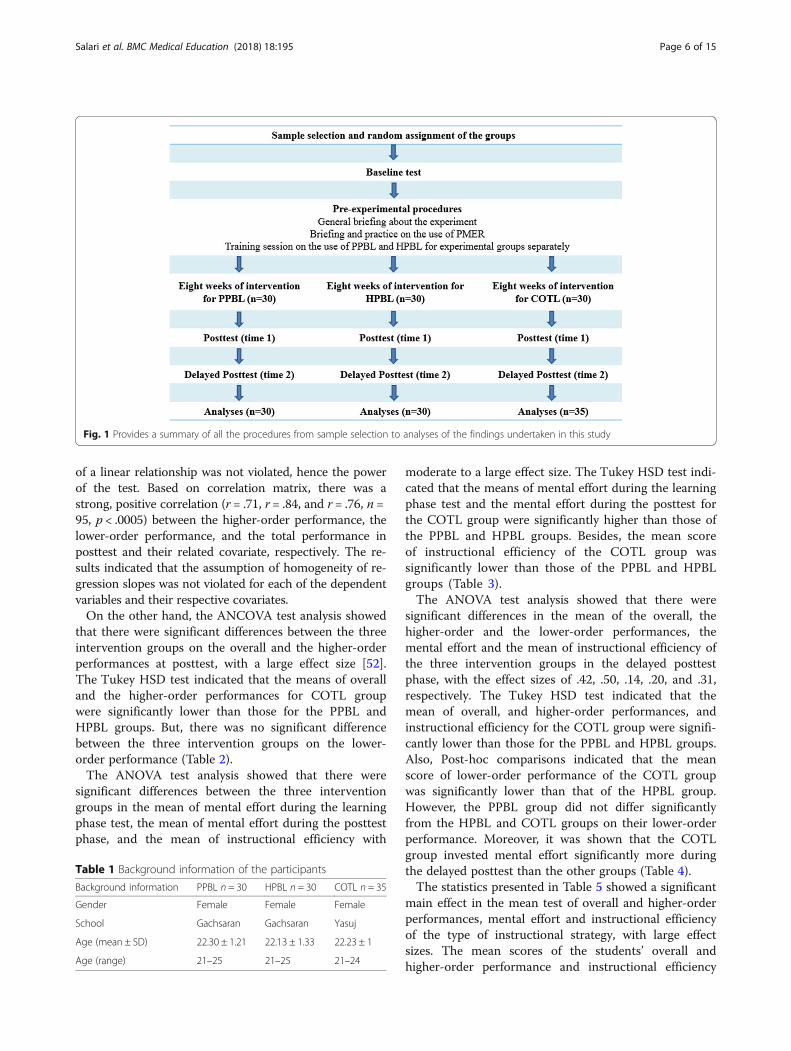
PNPT with PMER. After administering the tests, instruc-tional efficiency was measured using two-DimensionalIEI Formula. Figure 1 provides the flow chart of thestudy protocol.Since decay and interference concerning the posttest
and delayed posttest were assumed to be equally distrib-uted phenomena in the conventional and PBL groups,they did not serve as covariates in the experiment. Ac-cordingly, if the experimental groups’ learning remainseven after the 8 wk elapse, it could be concluded thatthe effects of strategies performed for experimentalgroups were more effective in the retention of learningthan those of the conventional strategy.
Data analysisUsing SPSS software version 17, the parametric statis-tical tests such as ANCOVA, One-way ANOVA, andMixed between-within subjects ANOVA were used. Forthese statistical tests with power analysis of Compromisemethod, with the effect size (ES) = 0.25 which is close tomedium, and β/α ratio of 1:1 that is also the default inbasic research, and for a total sample size of 95 for 3groups, the Power was calculated to be more than 0.80.It should be pointed out that alpha level for data analysiswas set at 0.05.
Ethical issuesTo carry out this study, same official permissions weretaken from the university chancellors. It should be men-tioned that the researchers were not allowed to reorgan-ize the student population of the classes. However, somecertain measures were taken not to treat the participantsunfairly. First, the assignment of the groups to themethods of intervention was purely random. Second, thesame amount of materials and time was provided for allthe three groups. In addition, written permission to usethe instruments in this study was attained from thedeveloper before using them.
ResultsTable 1 offers the demographic background informationof the participants. All the students were nursing majorand female. Their age ranged from 21 to 25 with a meanof 22.22. A majority (84.21%) of them were from the agegroup 21–23, whilst the rest (15.79%) were above 23.The result of ANOVA in the three groups of PPBL,
HPBL and COTL showed that there were no significantdifference between the mean of Pediatric Nursing Iscores (F (2, 92) = .34, p > .05), and the mean of PriorPerformance Test scores (F (2, 92) = .096, p > .05).The exploratory data analysis confirmed that the data
conformed to the preliminary assumptions of the para-metric tests. The relationship between each dependentvariable with its covariate was linear, thus the assumption
Salari et al. BMC Medical Education (2018) 18:195 Page 5 of 15
of a linear relationship was not violated, hence the powerof the test. Based on correlation matrix, there was astrong, positive correlation (r = .71, r = .84, and r = .76, n =95, p < .0005) between the higher-order performance, thelower-order performance, and the total performance inposttest and their related covariate, respectively. The re-sults indicated that the assumption of homogeneity of re-gression slopes was not violated for each of the dependentvariables and their respective covariates.On the other hand, the ANCOVA test analysis showed
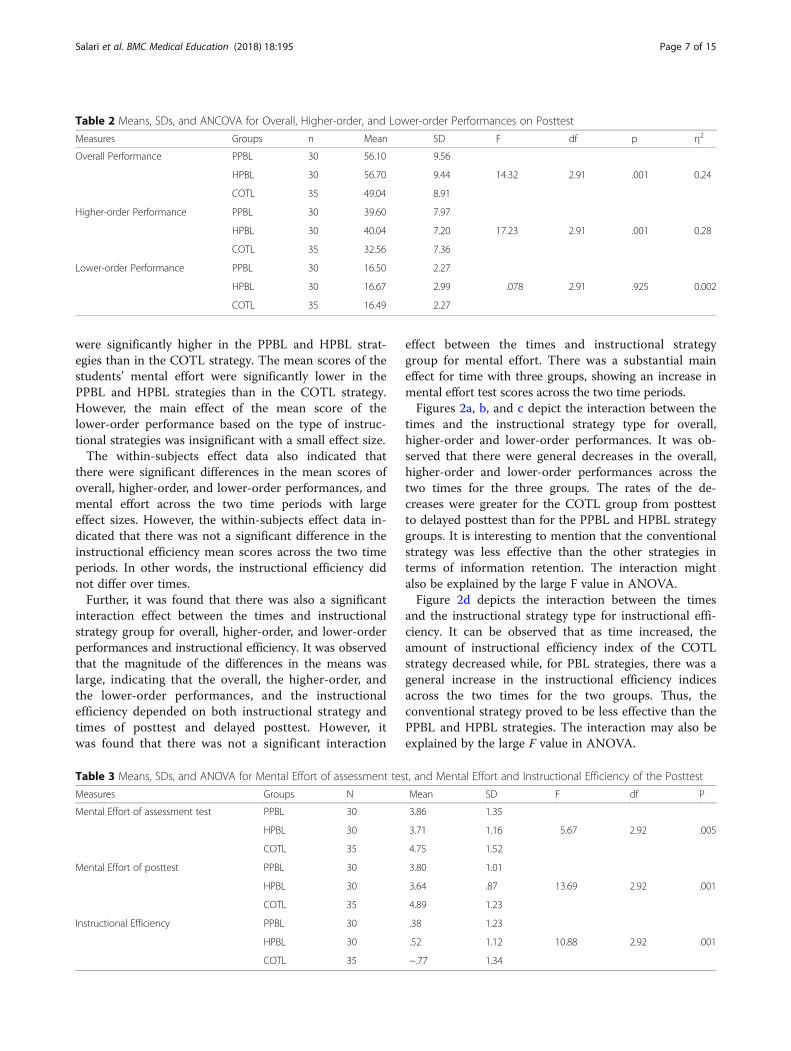
that there were significant differences between the threeintervention groups on the overall and the higher-orderperformances at posttest, with a large effect size [52].The Tukey HSD test indicated that the means of overalland the higher-order performances for COTL groupwere significantly lower than those for the PPBL andHPBL groups. But, there was no significant differencebetween the three intervention groups on the lower-order performance (Table 2).The ANOVA test analysis showed that there were
significant differences between the three interventiongroups in the mean of mental effort during the learningphase test, the mean of mental effort during the posttestphase, and the mean of instructional efficiency with
moderate to a large effect size. The Tukey HSD test indi-cated that the means of mental effort during the learningphase test and the mental effort during the posttest forthe COTL group were significantly higher than those ofthe PPBL and HPBL groups. Besides, the mean scoreof instructional efficiency of the COTL group wassignificantly lower than those of the PPBL and HPBLgroups (Table 3).The ANOVA test analysis showed that there were
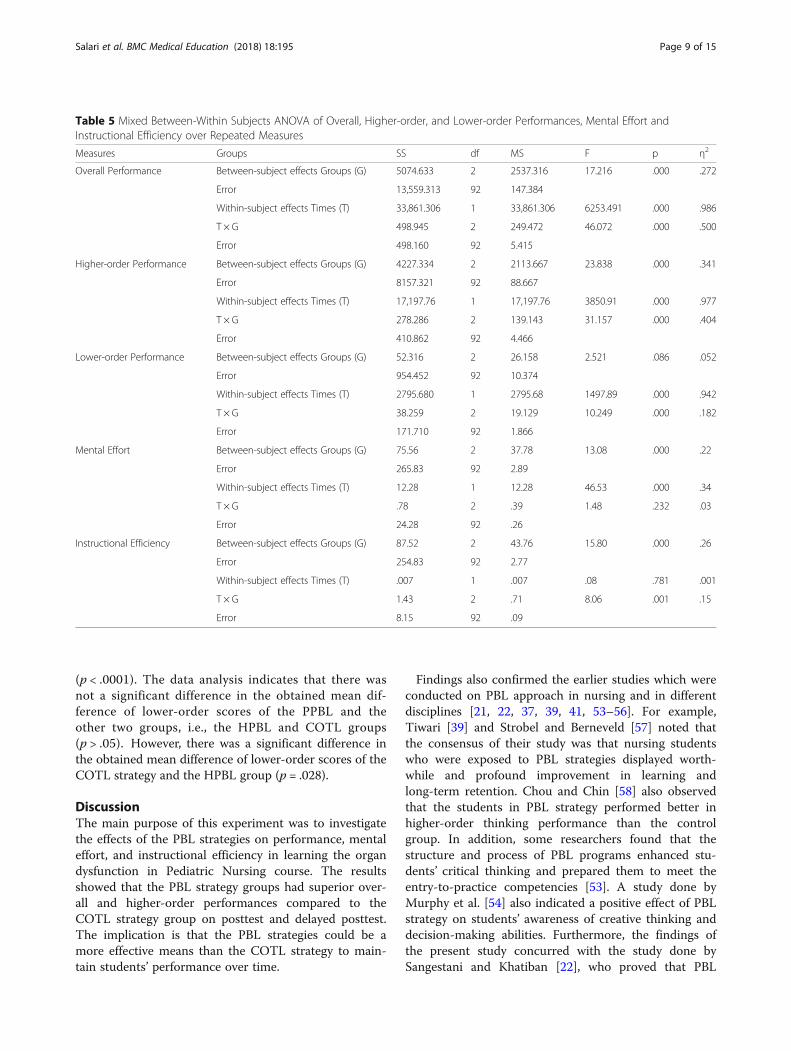
significant differences in the mean of the overall, thehigher-order and the lower-order performances, themental effort and the mean of instructional efficiency ofthe three intervention groups in the delayed posttestphase, with the effect sizes of .42, .50, .14, .20, and .31,respectively. The Tukey HSD test indicated that themean of overall, and higher-order performances, andinstructional efficiency for the COTL group were signifi-cantly lower than those for the PPBL and HPBL groups.Also, Post-hoc comparisons indicated that the meanscore of lower-order performance of the COTL groupwas significantly lower than that of the HPBL group.However, the PPBL group did not differ significantlyfrom the HPBL and COTL groups on their lower-orderperformance. Moreover, it was shown that the COTLgroup invested mental effort significantly more duringthe delayed posttest than the other groups (Table 4).The statistics presented in Table 5 showed a significant
main effect in the mean test of overall and higher-orderperformances, mental effort and instructional efficiencyof the type of instructional strategy, with large effectsizes. The mean scores of the students’ overall andhigher-order performance and instructional efficiency
Fig. 1 Provides a summary of all the procedures from sample selection to analyses of the findings undertaken in this study
Table 1 Background information of the participants
Background information PPBL n = 30 HPBL n = 30 COTL n = 35
Gender Female Female Female
School Gachsaran Gachsaran Yasuj
Age (mean ± SD) 22.30 ± 1.21 22.13 ± 1.33 22.23 ± 1
Age (range) 21–25 21–25 21–24
Salari et al. BMC Medical Education (2018) 18:195 Page 6 of 15
were significantly higher in the PPBL and HPBL strat-egies than in the COTL strategy. The mean scores of thestudents’ mental effort were significantly lower in thePPBL and HPBL strategies than in the COTL strategy.However, the main effect of the mean score of thelower-order performance based on the type of instruc-tional strategies was insignificant with a small effect size.The within-subjects effect data also indicated that
there were significant differences in the mean scores ofoverall, higher-order, and lower-order performances, andmental effort across the two time periods with largeeffect sizes. However, the within-subjects effect data in-dicated that there was not a significant difference in theinstructional efficiency mean scores across the two timeperiods. In other words, the instructional efficiency didnot differ over times.Further, it was found that there was also a significant
interaction effect between the times and instructionalstrategy group for overall, higher-order, and lower-orderperformances and instructional efficiency. It was observedthat the magnitude of the differences in the means waslarge, indicating that the overall, the higher-order, andthe lower-order performances, and the instructionalefficiency depended on both instructional strategy andtimes of posttest and delayed posttest. However, itwas found that there was not a significant interaction
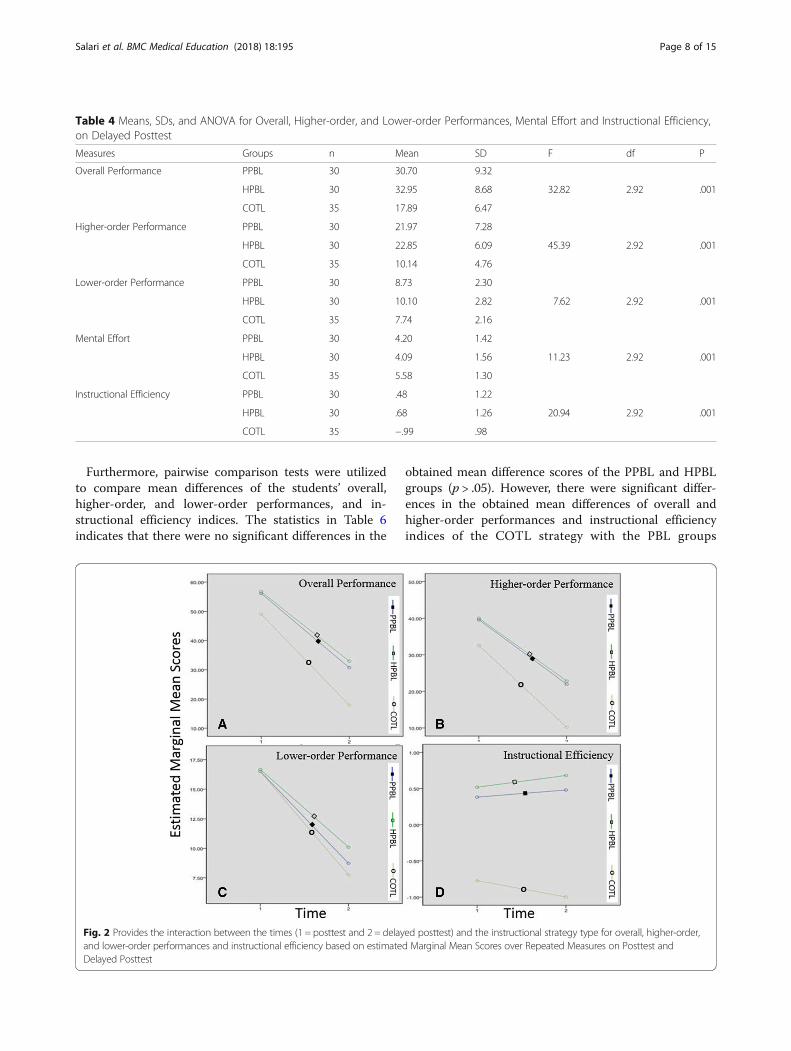
effect between the times and instructional strategygroup for mental effort. There was a substantial maineffect for time with three groups, showing an increase inmental effort test scores across the two time periods.Figures 2a, b, and c depict the interaction between the
times and the instructional strategy type for overall,higher-order and lower-order performances. It was ob-served that there were general decreases in the overall,higher-order and lower-order performances across thetwo times for the three groups. The rates of the de-creases were greater for the COTL group from posttestto delayed posttest than for the PPBL and HPBL strategygroups. It is interesting to mention that the conventionalstrategy was less effective than the other strategies interms of information retention. The interaction mightalso be explained by the large F value in ANOVA.Figure 2d depicts the interaction between the times
and the instructional strategy type for instructional effi-ciency. It can be observed that as time increased, theamount of instructional efficiency index of the COTLstrategy decreased while, for PBL strategies, there was ageneral increase in the instructional efficiency indicesacross the two times for the two groups. Thus, theconventional strategy proved to be less effective than thePPBL and HPBL strategies. The interaction may also beexplained by the large F value in ANOVA.
Table 2 Means, SDs, and ANCOVA for Overall, Higher-order, and Lower-order Performances on Posttest
Measures Groups n Mean SD F df p η2
Overall Performance PPBL 30 56.10 9.56
HPBL 30 56.70 9.44 14.32 2.91 .001 0.24
COTL 35 49.04 8.91
Higher-order Performance PPBL 30 39.60 7.97
HPBL 30 40.04 7.20 17.23 2.91 .001 0.28
COTL 35 32.56 7.36
Lower-order Performance PPBL 30 16.50 2.27
HPBL 30 16.67 2.99 .078 2.91 .925 0.002
COTL 35 16.49 2.27
Table 3 Means, SDs, and ANOVA for Mental Effort of assessment test, and Mental Effort and Instructional Efficiency of the Posttest
Measures Groups N Mean SD F df P
Mental Effort of assessment test PPBL 30 3.86 1.35
HPBL 30 3.71 1.16 5.67 2.92 .005
COTL 35 4.75 1.52
Mental Effort of posttest PPBL 30 3.80 1.01
HPBL 30 3.64 .87 13.69 2.92 .001
COTL 35 4.89 1.23
Instructional Efficiency PPBL 30 .38 1.23
HPBL 30 .52 1.12 10.88 2.92 .001
COTL 35 −.77 1.34
Salari et al. BMC Medical Education (2018) 18:195 Page 7 of 15
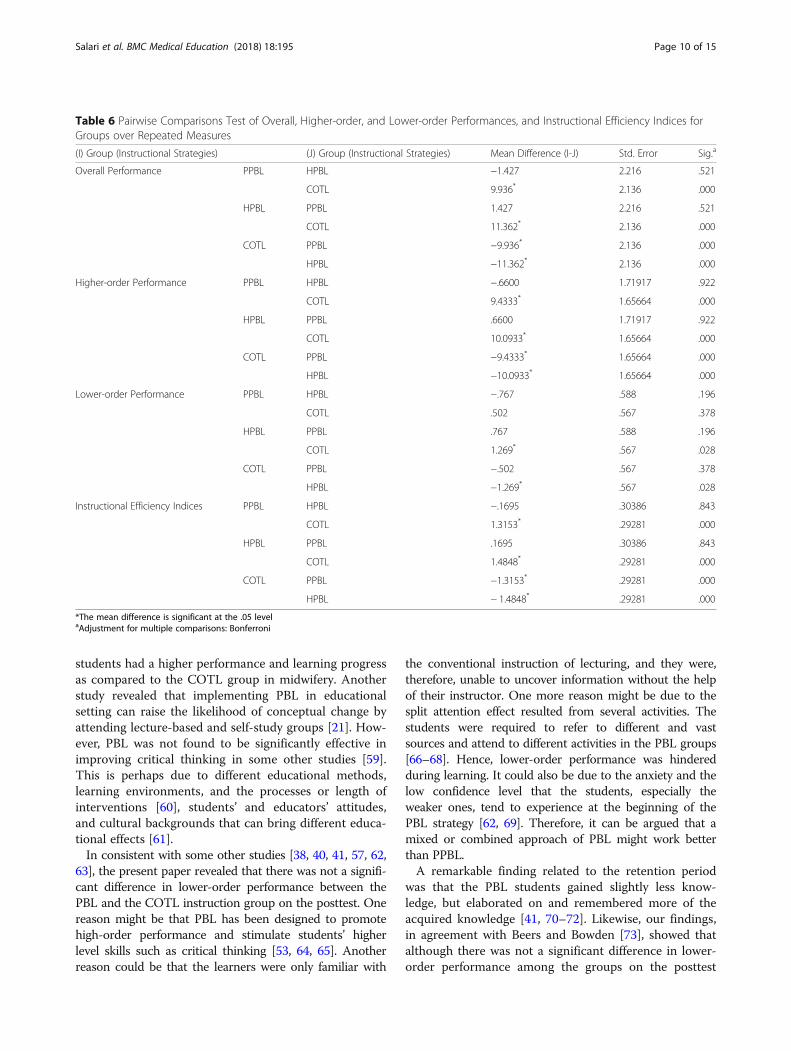
Furthermore, pairwise comparison tests were utilizedto compare mean differences of the students’ overall,higher-order, and lower-order performances, and in-structional efficiency indices. The statistics in Table 6indicates that there were no significant differences in the
obtained mean difference scores of the PPBL and HPBLgroups (p > .05). However, there were significant differ-ences in the obtained mean differences of overall andhigher-order performances and instructional efficiencyindices of the COTL strategy with the PBL groups
Table 4 Means, SDs, and ANOVA for Overall, Higher-order, and Lower-order Performances, Mental Effort and Instructional Efficiency,on Delayed Posttest
Measures Groups n Mean SD F df P
Overall Performance PPBL 30 30.70 9.32
HPBL 30 32.95 8.68 32.82 2.92 .001
COTL 35 17.89 6.47
Higher-order Performance PPBL 30 21.97 7.28
HPBL 30 22.85 6.09 45.39 2.92 .001
COTL 35 10.14 4.76
Lower-order Performance PPBL 30 8.73 2.30
HPBL 30 10.10 2.82 7.62 2.92 .001
COTL 35 7.74 2.16
Mental Effort PPBL 30 4.20 1.42
HPBL 30 4.09 1.56 11.23 2.92 .001
COTL 35 5.58 1.30
Instructional Efficiency PPBL 30 .48 1.22
HPBL 30 .68 1.26 20.94 2.92 .001
COTL 35 −.99 .98
Fig. 2 Provides the interaction between the times (1 = posttest and 2 = delayed posttest) and the instructional strategy type for overall, higher-order,and lower-order performances and instructional efficiency based on estimated Marginal Mean Scores over Repeated Measures on Posttest andDelayed Posttest
Salari et al. BMC Medical Education (2018) 18:195 Page 8 of 15
(p < .0001). The data analysis indicates that there wasnot a significant difference in the obtained mean dif-ference of lower-order scores of the PPBL and theother two groups, i.e., the HPBL and COTL groups(p > .05). However, there was a significant difference inthe obtained mean difference of lower-order scores of theCOTL strategy and the HPBL group (p = .028).
DiscussionThe main purpose of this experiment was to investigatethe effects of the PBL strategies on performance, mentaleffort, and instructional efficiency in learning the organdysfunction in Pediatric Nursing course. The resultsshowed that the PBL strategy groups had superior over-all and higher-order performances compared to theCOTL strategy group on posttest and delayed posttest.The implication is that the PBL strategies could be amore effective means than the COTL strategy to main-tain students’ performance over time.
Findings also confirmed the earlier studies which wereconducted on PBL approach in nursing and in differentdisciplines [21, 22, 37, 39, 41, 53–56]. For example,Tiwari [39] and Strobel and Berneveld [57] noted thatthe consensus of their study was that nursing studentswho were exposed to PBL strategies displayed worth-while and profound improvement in learning andlong-term retention. Chou and Chin [58] also observedthat the students in PBL strategy performed better inhigher-order thinking performance than the controlgroup. In addition, some researchers found that thestructure and process of PBL programs enhanced stu-dents’ critical thinking and prepared them to meet theentry-to-practice competencies [53]. A study done byMurphy et al. [54] also indicated a positive effect of PBLstrategy on students’ awareness of creative thinking anddecision-making abilities. Furthermore, the findings ofthe present study concurred with the study done bySangestani and Khatiban [22], who proved that PBL
Table 5 Mixed Between-Within Subjects ANOVA of Overall, Higher-order, and Lower-order Performances, Mental Effort andInstructional Efficiency over Repeated Measures
Measures Groups SS df MS F p η2
Overall Performance Between-subject effects Groups (G) 5074.633 2 2537.316 17.216 .000 .272
Error 13,559.313 92 147.384
Within-subject effects Times (T) 33,861.306 1 33,861.306 6253.491 .000 .986
T × G 498.945 2 249.472 46.072 .000 .500
Error 498.160 92 5.415
Higher-order Performance Between-subject effects Groups (G) 4227.334 2 2113.667 23.838 .000 .341
Error 8157.321 92 88.667
Within-subject effects Times (T) 17,197.76 1 17,197.76 3850.91 .000 .977
T × G 278.286 2 139.143 31.157 .000 .404
Error 410.862 92 4.466
Lower-order Performance Between-subject effects Groups (G) 52.316 2 26.158 2.521 .086 .052
Error 954.452 92 10.374
Within-subject effects Times (T) 2795.680 1 2795.68 1497.89 .000 .942
T × G 38.259 2 19.129 10.249 .000 .182
Error 171.710 92 1.866
Mental Effort Between-subject effects Groups (G) 75.56 2 37.78 13.08 .000 .22
Error 265.83 92 2.89
Within-subject effects Times (T) 12.28 1 12.28 46.53 .000 .34
T × G .78 2 .39 1.48 .232 .03
Error 24.28 92 .26
Instructional Efficiency Between-subject effects Groups (G) 87.52 2 43.76 15.80 .000 .26
Error 254.83 92 2.77
Within-subject effects Times (T) .007 1 .007 .08 .781 .001
T × G 1.43 2 .71 8.06 .001 .15
Error 8.15 92 .09
Salari et al. BMC Medical Education (2018) 18:195 Page 9 of 15
students had a higher performance and learning progressas compared to the COTL group in midwifery. Anotherstudy revealed that implementing PBL in educationalsetting can raise the likelihood of conceptual change byattending lecture-based and self-study groups [21]. How-ever, PBL was not found to be significantly effective inimproving critical thinking in some other studies [59].This is perhaps due to different educational methods,learning environments, and the processes or length ofinterventions [60], students’ and educators’ attitudes,and cultural backgrounds that can bring different educa-tional effects [61].In consistent with some other studies [38, 40, 41, 57, 62,
63], the present paper revealed that there was not a signifi-cant difference in lower-order performance between thePBL and the COTL instruction group on the posttest. Onereason might be that PBL has been designed to promotehigh-order performance and stimulate students’ higherlevel skills such as critical thinking [53, 64, 65]. Anotherreason could be that the learners were only familiar with
the conventional instruction of lecturing, and they were,therefore, unable to uncover information without the helpof their instructor. One more reason might be due to thesplit attention effect resulted from several activities. Thestudents were required to refer to different and vastsources and attend to different activities in the PBL groups[66–68]. Hence, lower-order performance was hinderedduring learning. It could also be due to the anxiety and thelow confidence level that the students, especially theweaker ones, tend to experience at the beginning of thePBL strategy [62, 69]. Therefore, it can be argued that amixed or combined approach of PBL might work betterthan PPBL.A remarkable finding related to the retention period
was that the PBL students gained slightly less know-ledge, but elaborated on and remembered more of theacquired knowledge [41, 70–72]. Likewise, our findings,in agreement with Beers and Bowden [73], showed thatalthough there was not a significant difference in lower-order performance among the groups on the posttest
Table 6 Pairwise Comparisons Test of Overall, Higher-order, and Lower-order Performances, and Instructional Efficiency Indices forGroups over Repeated Measures
(I) Group (Instructional Strategies) (J) Group (Instructional Strategies) Mean Difference (I-J) Std. Error Sig.a
Overall Performance PPBL HPBL −1.427 2.216 .521
COTL 9.936* 2.136 .000
HPBL PPBL 1.427 2.216 .521
COTL 11.362* 2.136 .000
COTL PPBL −9.936* 2.136 .000
HPBL −11.362* 2.136 .000
Higher-order Performance PPBL HPBL −.6600 1.71917 .922
COTL 9.4333* 1.65664 .000
HPBL PPBL .6600 1.71917 .922
COTL 10.0933* 1.65664 .000
COTL PPBL −9.4333* 1.65664 .000
HPBL −10.0933* 1.65664 .000
Lower-order Performance PPBL HPBL −.767 .588 .196
COTL .502 .567 .378
HPBL PPBL .767 .588 .196
COTL 1.269* .567 .028
COTL PPBL −.502 .567 .378
HPBL −1.269* .567 .028
Instructional Efficiency Indices PPBL HPBL −.1695 .30386 .843
COTL 1.3153* .29281 .000
HPBL PPBL .1695 .30386 .843
COTL 1.4848* .29281 .000
COTL PPBL −1.3153* .29281 .000
HPBL − 1.4848* .29281 .000
*The mean difference is significant at the .05 levelaAdjustment for multiple comparisons: Bonferroni
Salari et al. BMC Medical Education (2018) 18:195 Page 10 of 15

and between the PPBL and COTL on the delayed post-test, the HPBL group had better scores on lower-orderperformance as compared to COTL group on the delayedposttest. One possible explanation could be attributed tothe attention on elaboration in HPBL which tends to pro-mote the recall of declarative knowledge. The implicationis that HPBL strategy could be a more effective meansthan COTL strategy to prevent from a drastic decrease instudents’ lower-order performance over time (posttest anddelayed posttest).The results also showed that the performance levels of
the PBL strategy groups were achieved with a lowermean mental effort during the learning and test phases.They also suggested that the higher performance wasachieved with a reduction in cognitive load (mental ef-fort). These findings were supported by the significantlyhigher level of two-D instructional condition efficiencyindex reported by the PBL instructional strategy groupsas opposed to the COTL strategy group. Therefore, thestudy yielded additional empirical evidence in support ofHPBL strategy in learning Pediatric Nursing contents.The results of this study also revealed that the PBL
groups achieved better performance on the posttest anddelayed posttest. In line with the predictions made bythe cognitive load theory, the PBL strategies reduced thelearners’ mental effort during learning activities, henceallowing for an increase in overall performance. This con-tention was further supported by the significantly higherlevel of two-D instructional condition efficiency indexreported by the PBL strategy as opposed to the COTLstrategy. There is still more research evidence indicatingthat PBL increases conceptual change in learners throughengaging them cognitively in problem-solving tasks,involving them in group discussions, activating their priorknowledge and providing them with enough opportunityto be able to deeply process the information at hand [21].The findings of the study further support the conten-
tion that cognitive load theory is a useful tool in design-ing efficient instruction. These findings are congruentwith an earlier study conducted by McMullan, Jones andLea [74] reporting the effect of an interactive e-drug cal-culations package on nursing students’ drug calculationability and self-efficacy. As Harasym, Tsai and Munshi[75] and Yuan et al. [5] indicated nursing/medical stu-dents in PPBL strategy experienced a heavy workload,had difficulty to search for information and developtasks and hand-outs, felt too stressed, had difficulty tocatch the key points, grasped knowledge incompletely,received vague information and lacked confidence inclarifying the information. In answer to the necessityraised by these researchers, the current study used acombined instructional strategy (HPBL) to minimizeworking memory overload and decrease students’ splitattention for better performance [37, 62, 75].
One reason for the significantly better performance ofthe PBL groups could be that the PBL strategies had theeffect of increasing germane cognitive load. In line withthe PBL strategies, the learners were encouraged toanalyze, interpret, guess and hypothesize meaning.Moreover, the students were required to link new ideaswith previous knowledge, use open-ended questions topromote learners’ participation in class discussion andkeep themselves active in the process of learning. Inother words, the most important tasks of the tutors werestimulating active and self-directed learning [76]. Also,the researchers, by facilitating the communicationamong the group members, caused the distribution ofcognitive load among the members of the group, fos-tered learning and increased germane cognitive loadthrough construction of schemata. Therefore, the extra-neous or ineffective cognitive load was minimized.In PBL strategies, the tutors manage to guide the
learners through the instructional help in order to re-duce the cognitive load by controlling and decreasingthe extraneous load and increasing the germane load[25, 48]. Doing so, the learner can solve the problems inneed of high mental effort with less effort. This study isin concordance with Martenson et al. [77] who showedthat PBL learners’ long-term retention rate was higherthan that of the conventional learners. The reason couldbe that distributing learning over time in PBL strategytypically benefits long-term retention [78]. Generally, theresults of the current experiment support the contentionthat the use of PBL strategies in the learning of PediatricNursing course can reduce cognitive load and lead tobetter overall and higher-level thinking performance.Another alternative explanation for better performance
among the PBL groups could be the design of PBLinstructional strategy which is based on constructivismand Vygotsky’s theory. In this study, by interaction be-tween the learners and the facilitator in class as a socialcontext, and through guided instruction that increasedinteraction between them, the students were able tounderstand and learn the content materials more quicklyand more correctly in the zone of proximal developmentthrough more effective instruction [34]. One reasoncould be that through guidance, scaffolding takes shapeand develops sooner to enable students to “bridge thegap between their current abilities and the intendedgoal” [35]. It is essential to note that the need for astructured and comprehensive feedback and guidancefor PBL facilitators has been considered vital in PBLrelated research [79, 80]. Similarly, this study supportsthe role of the facilitator as a guide or coach toencourage learners’ progress. Moreover, use of real-world examples, collaborative learning, and class dis-cussions allow facilitators to maintain a sense of con-trol and transition to constructivist teaching [81]. In
Salari et al. BMC Medical Education (2018) 18:195 Page 11 of 15

addition, instructional designers should develop differ-ent instructional models and resources that couldcreate a constructivist environment [82].The present findings highlight the static form of in-
struction used in the conventional method of teachingPediatric Nursing. Instructor-based teaching, that re-quires students to study and then recite what they havealready learned, encourages them to merely memorizethe textbook contents. It was also observed during theexperiment that the students in the conventional strat-egy group played a more passive role where they wereexpected to be told what to do and look for the rightanswers. Dunkin and Biddle [83] also support the notionthat students, as a context variable, need to be consid-ered in the teaching and learning process. They also addthat passivity among students often induces lowerlearner involvement. However, they suggest that studentis not the only element that should be considered;rather, the process of teaching with the use of effectivestrategies ought to be taken into account.To make a long story short, the findings of this study
was consistent with Dunkin and Biddle [83] model forthe study of classroom teaching, Constructive theory,Vygotsky’s theory [14] and Cognitive Load theory (1988).The most significant conclusion that can be drawn fromthis study is that using PPBL and an intelligent combin-ation of lecture and problem-based learning that mayhelp to facilitate the learning of Pediatric Nursing canresult in more effective instruction. As Borhan [84] sug-gests, Hybrid PBL and PBL approaches should graduallycrawl into the academic curriculum in order to developlearners’ ability to solve problems in a large classroomsetting [85].In a word, the PBL strategies prove to be effective in
the students’ overall and higher-order achievement. Inaddition, although the performance of all the groupsdecreased and their invested mental effort increased overtime, the decrease of the performance and the increaseof the invested mental effort for the PBL groups weresignificantly less than those of the conventional group.Therefore, PBL instructional strategies are deemed to bemore efficient with better instructional efficiency indices.
Implications for medical educationThe findings of this study revealed that a simple shift intheoretical emphasis from minimal guidance construct-ivism to guidance in the zone of proximal developmentleads to a reconceptualization of PBL which is practicallyin line with the role of facilitator to guide novicelearners to fill in the gap [86]. Furthermore, the findingshighlighted that integrating cognitive load theory in de-signing HPBL programs has an innovative effect. From ateaching viewpoint, it is very essential to discover therules for fostering the germane load. Thus, HPBL was
designed based on CLT to ensure that HPBL leads tomore knowledge acquisition, better learning transfer,and lower mental effort, hence the efficiency of studentlearning. In HPBL, gaining learners’ attention beforethey learn, as well as giving a brief lecture along with anexample by the facilitator in the early stages of learning,could reduce irrelevant processing by highlighting essen-tial materials and linking between previous and newknowledge [87].The primary practical implication of the present study
has to do with the instructional strategies. Both PPBLand HPBL strategies created impressive results in stu-dents’ performance, mental effort, and instructional effi-ciency. The findings of this study revealed that the useof PBL strategies could significantly enhance students’achievement. Therefore, the PBL strategies are preferredover conventional strategy for instruction in PediatricNursing.In line with the above arguments, a major concern for
nursing educators could be how to effectively move froma traditional lecture style to a PBL approach. Since theimplementation of PPBL is a time-consuming processand needs additional tutors, the HPBL and PPBL withone floating tutor in a large classroom may be adoptedto overcome these concerns.
LimitationsIn this study, four main topics of organ dysfunction withhigh prevalence in Pediatric Nursing syllabus were of-fered through PBL strategies, and the intervention wasdone for only 8 wk of teaching sessions. Although themajority of the students benefited from this teachingapproach, the results might be suitably generalized onlyto courses of similar contents and level. In addition, theresearchers were not allowed to change the official pro-grams of the universities to randomize the assignment ofthe subjects to different groups, and the course was ob-ligatory for all the classes, the students did not have thechance to decide to participate in the study; yet, to befair enough, as it was already mentioned, the assignmentof the classes to each approach was purely randomized.
Suggestions for future researchThe current study suggests that incorporating the use ofdifferent PBL approaches can be a useful instructionalstrategy in the teaching and learning of PediatricNursing at university level. Therefore, further research iswelcome to assess the effectiveness of this approach inother nursing subjects in other instructional contexts tospecify its weak and strong aspects.Furthermore, new research may intend to examine the
long-term effects of problem-based learning on students’higher-level thinking or on using randomized controlledtrials to control threats according to different nursing
Salari et al. BMC Medical Education (2018) 18:195 Page 12 of 15

educational settings as noted in Kong et al. [88]. Inaddition, other studies with a mixed method designcould be conducted to reveal richer student perceptionsof the problem-based experience. Moreover, the resultsdelivered a much-needed pattern and starting point foreducators presenting active learning approaches forPediatric Nursing courses to build on student knowledgeand skills. A combination of PBL and concept map mayoffer nursing students a variety of ways of learning.Finally, future studies on PBL strategies could involvenot only nursing students but also graduated and regis-tered nurses taking part in retraining programs.
ConclusionsThis study established that using PPBL and HPBL in alarge classroom setting with one tutor had several positiveoutcomes. PBL instructional strategies enhanced students’overall and higher-order performances, induced less men-tal effort during learning and test phase, and as a resultincreased two-dimensional instructional efficiency indexin learning Pediatric Nursing. Although, there appeared tobe no significant difference in lower-order performanceamong the groups on the posttest, the HPBL group gainedhigher scores on lower-order performance as compared tothe COTL group on the delayed posttest. The implicationis that HPBL strategy could be a more effective meansthan COTL strategy to enable students to continue toenjoy a better lower-order performance over time.
Additional file
Additional file 1: Major differences among COTL, HPBL, and PPBL. Theinformation in the additional file provides a brief account of some of themajor differences like objectives, teacher’s and students’ roles andresponsibilities, etc. among the three instructional approaches of COTL,HPBL, and PPBL that were employed in the study. (DOCX 17 kb)
AbbreviationsCOTL: Conventional Teaching and Learning; HPBL: Hybrid Problem-basedlearning; IAU: Islamic Azad University; IEI: Instructional efficiency index; KBAprovince: Kohgiluyeh-BoyerAhmad province; PBL: Problem-based learning;PIS: Patient information sheets; PMER: Paas Mental Effort Rating Scale;PN: Pediatric Nursing; PNPT: Pediatric Nursing Performance Test; PPBL: PureProblem-based learning
AcknowledgmentsThe authors wish to thank all the accessible nursing students for their timeand participation in this study. Thanks also are due to the chancellors ofGachsaran and Yasuj Islamic Azad Universities for granting the researchersthe permission to conduct the study.
Availability of data and materialsThe datasets used and analyzed during the current study are available fromthe corresponding author on reasonable request.
Authors’ contributionsMS, AR, AZ, and RAT provided substantial input into study design andinterpretation of the findings. MS especially implemented the course andcollected and analyzed the data. AR contributed to the planning of thestudy procedure and designing the tables and Figs. AZ contributed to the
theoretical concepts of the study and redrafted and edited the manuscript.RAT helped the project by establishing the design of the study andreviewing the manuscript. All the authors contributed to drafting and criticalreview of the manuscript. They have also read and approved the finalmanuscript.
Ethics approval and consent to participateEthical approval for this study was granted by the Deputy Chancellors ofYasuj and Gachsaran Azad Universities with reference numbers 9/864 and26,112, respectively. In addition, all the participants were provided withdetailed information about the aims of the study and that data would beanalyzed anonymously. Verbal consent to participate was gained from allparticipants. They also gave their consent to participate in the study byfilling out and sending back the questionnaires. Because of the approvalfrom the universities, the verbal consent from the participants, and theresearchers’ commitment to keep their personal information confidential, therights and privacy of the participants were protected as required by theaffiliated IRB.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Nursing Department, School of Nursing, Yasuj University of MedicalSciences, Yasuj, Iran. 2Education Development Center, School of Medicine,Yasuj University of Medical Sciences, Yasuj, Iran. 3English LanguageDepartment, Faculty of Humanities, Yasouj University, Yasouj, Iran. 4Faculty ofEducational Studies, University Putra Malaysia, Serdang, Selangor, Malaysia.
Received: 17 January 2018 Accepted: 30 July 2018
References1. Cheraghi M, Salasli M, Ahmadi F. Iranian nurses’ perceptions of theoretical
knowledge transfer into clinical practice: a grounded theory approach. NursHealth Sci. 2007;9(3):212–20.
2. Kessenich CR, Guyatt GH, DiCenso A. Teaching nursing students evidence-based nursing. Nurse Educ. 1997;22(6):25–9.
3. Creedy D, Horsfall J, Hand B. Problem-based learning in nurse education: anaustralian view. J Adv Nurs. 1992;17(6):727–33.
4. Klunklin A, Subpaiboongid P, Keitlertnapha P, Viseskul N, et al. Thai nursingstudents’ adaption to problem-based learning: a qualitative study. NurseEduc Pract. 2011;11(6):370–4.
5. Yuan HB, Williams BA, Yin L, Liu M, et al. Nursing students’ views on theeffectiveness of problem-based learning. Nurse Educ Today. 2011;31(6):577–81.
6. Dehkordi AH, Heydarnejad MS. The impact of problem based learning andlecturing on the behavior and attitudes of iranian nursing students, arandomized controlled trial. Dan Med Bull. 2008;55(4):224–6.
7. Aien F, Noorian C. Problem-based learning: a new experience in educationof pediatric nursing course to nursing students. Shahrekord Univ Med Sci J.2006;8(2):16–20.
8. Bastable SB. Nurse as educator: principles of teaching and learning fornursing practice. 3rd ed. Burlington, MA: Jones & Bartlett Publishers; 2007.
9. Bengtsson M, Ohlsson B. The nursing and medical students motivation toattain knowledge. Nurse Educ Today. 2010;30(2):150–6.
10. Tiwari A, Lai P, So M, Yuen K. A comparison of the effects of problem-basedlearning and lecturing on the development of students' critical thinking.Med Educ. 2006;40(6):547–54.
11. Quintero GA. Medical education and the healthcare system - why does thecurriculum need to be reformed? BMC Med. 2014;12(1):213.
12. Patel VL, Groen GJ, Norman GR. Reasoning and instruction in medicalcurricula. Cogn Instr. 1993;10(4):335.
Salari et al. BMC Medical Education (2018) 18:195 Page 13 of 15
13. Baker CM, Pesut DJ, McDaniel AM, Fisher ML. Evaluating the impact ofproblem-based learning on learning styles of master’s students in nursingadministration. J Prof Nurs. 2007;23(4):214–9.
14. Vygotsky LS. Mind in society: the development of higher mental processes.Cambridge, MA: Harvard University Press; 1978.
15. Smagorinsky P. The development of social and practical concepts inlearning to teach: a synthesis and extension of vygotsky’s conception. LearnCult Soc Interact. 2013;2(4):238–48.
16. DeVries R. Vygotsky, piaget, and education: a reciprocal assimilation oftheories and educational practices. New Ideas Psychol. 2000;18(2):187–213.
17. Brandon AF, All AC. Constructivism theory analysis and application tocurricula. Nurs Educ Perspect. 2010;31(2):89–92.
18. Young LE, Patterson BL. Teaching nursing: developing a student-centeredlearning environment. Philadelphia, PA: Lippincott Williams & Wilkins; 2007.
19. Gagnon GW, Collay M. Constructivist learning design: key questions forteaching to standards. New Bury Park, CA: Corwin Press; 2006.
20. Nie Y, Lau S. Diffrential relations of constructivist and didactic instruction tostudents’ cognition, motivation, and achievement. Learn Instr. 2010;20(5):411–23.
21. Loyens SMM, Jones SH, Mikkers J, van Gog T. Problem-based learning as afacilitator of conceptual change. Learn Instr. 2015;38:34–42.
22. Sangestani G, Khatiban M. Comparison of problem-based learning andlecture-based learning in midwifery. Nurse Educ Today. 2013;33(8):791–5.
23. Muis KR, Duffy MC. Epistemic climate and epistemic change: instructiondesigned to change students' beliefs and learning strategies and improveachievement. J Educ Psychol. 2013;105(1):213–25.
24. Yilmaz K. Constructivism: its theoretical underpinnings, variations, andimplications for classroom instruction. Educ Horiz. 2008;86(3):161–72.
25. Hmelo-Silver C. Problem-based learning: what and how do students learn?Educ Psychol Rev. 2004;16(3):235–66.
26. Cónsul-Giribet M, Medina-Moya JL. Strengths and weaknesses of problembased learning from the professional perspective of registered nurses1. RevLatino-Am Enfermagem. 2014;22(5):724–30.
27. Qalehsari MQ, Khaghanizadeh M, Ebadi A. Lifelong learning strategies innursing: a systematic review. Electron Physician. 2017;9(10):5541–50.
28. Staun M, Bergström B, Wadensten B. Evaluation of a pbl strategy in clinicalsupervision of nursing students: patient-centred training in student-dedicated treatment rooms. Nurse Educ Today. 2010;30(7):631–7.
29. Barrows HS. A taxonomy of problem-based learning methods. Med Educ.1986;20(6):481–6.
30. Dolmans DH, De Grave W, Wolfhagen IH, Van Der Vleuten CP. Problem-based learning: future challenges for educational practice and research.Med Educ. 2005;39(7):732–41.
31. Camp G. Problem-based learning: a paradigm shift or a passing fad? MedEduc Online. 1996;1(1):4282.
32. Armstrong E. A hybrid model of problem-based learning. In: Boud D, FelettiG, editors. The challenge of problem-based learning. 2nd ed. London:Kogan Page; 1997. p. 137–50.
33. Gwee MCE. Problem-based learning: a strategic learning system design forthe education of healthcare professionals in the 21st century. Kaohsiung JMed Sci. 2009;25(5):231–9.
34. Harland T. Vygotsky's zone of proximal development and problem-basedlearning: linking a theoretical concept with practice through actionresearch. Teach High Educ. 2003;8(2):263–72.
35. Rosenshine B, Meister C. The use of scaffolds for teaching higher-levelcognitive strategies. Educ Leadersh. 1992;49(7):26–33.
36. Schnotz W, Kirschner C. A reconsideration of cognitive load theory. EducPsychol Rev. 2007;19(4):469–508.
37. Hwang SY, Kim MJ. A comparison of problem-based learning and lecture-based learning in an adult health nursing course. Nurse Educ Today. 2006;26(4):315–21.
38. Shin I-S, Kim J-H. The effect of problem-based learning in nursing education: ameta-analysis. Adv Health Sci Educ Theory Pract. 2013;18(5):1–18.
39. Tiwari A, Chan S, Wong E, Wong D, et al. The effect of problem-basedlearning on students' approaches to learning in the context of clinicalnursing education. Nurse Educ Today. 2006;26(5):430–8.
40. Colliver JA. Effectiveness of problem-based learning curricula: research andtheory. Acad Med. 2000;75(3):259–66.
41. Dochy F, Segers M, Van den Bossche P, Gijbels D. Effects of problem-basedlearning: a meta-analysis. Learn Instr. 2003;13(5):533–68.
42. Kirschner PA, Sweller J, Clark RE. Why minimal guidance during instructiondoes not work: an analysis of the failure of constructivist, discovery,
problem-based, experiential, and inquiry-based teaching. Educ Psychol.2006;41(2):75–86.
43. Choi E, Lindquist R, Song Y. Effects of problem-based learning vs. traditionallecture on korean nursing students’ critical thinking, problem-solving, andself-directed learning. Nurse Educ Today. 2014;34(1):52–6.
44. Statistical informations of iau. 2009. https://stat.iau.ir. Accessed 10 Apr 2009.45. Gronlund NE. Writing instructional objectives for teaching and assessment.
7th ed. New Jersey, NJ: Pearson Education, Inc; 2004.46. Bloom BB. Taxonomy of educational objectives: the classification of
educational goals. Philadelphia, PA: David McKey Company, INC; 1966.47. Paas FG. Training strategies for attaining transfer of problem-solving skill in
statistics: a cognitive-load approach. J Educ Psychol. 1992;84(4):429–34.48. Kirschner F, Paas F, Kirschner PA. Individual and group-based learning from
complex cognitive tasks: effects on retention and transfer efficiency.Comput Hum Behav. 2009;25(2):306–14.
49. Higher Council of Planning in Medical Sciences. Integrated curriculum fornursing students: Curriculum specifications, nursing bachelorette. Tehran:Ministry of Health and Medical Education; 2007.
50. Higher Council of Planning in Medical Sciences. Integrated curriculum fornursing students: Curriculum specifications, nursing bachelorette. 1st ed.Tehran: Ministry of Health and Medical Education; 2014.
51. Novak JD. Learning, creating, and using knowledge: concept maps asfacilitative tools in schools and corporations. 2nd ed. New York, NY:Routledge; 2010.
52. Cohen J. Statistical power analysis for the behavioral sciences. ErlbaumAssociates: Hillsdale, NJ; 1988.
53. Applin H, Williams B, Day R, Buro K. A comparison of competenciesbetween problem-based learning and non-problem-based graduate nurses.Nurse Educ Today. 2011;31(2):129–34.
54. Murphy S, Hartigan I, Walshe N, Flynn AV, et al. Merging problem-basedlearning and simulation as an innovative pedagogy in nurse education. ClinSimul Nurs. 2011;7(4):e141–e8.
55. Tarmizi RA, Bayat S. Effects of problem-based learning approach inlearning of statistics among university students. Procedia Soc Behav Sci.2010;8:384–92.
56. Zhou J, Zhou S, Huang C, Xu R, et al. Effectiveness of problem-basedlearning in chinese pharmacy education: a meta-analysis. BMC Med Educ.2016;16(1):23.
57. Strobel J, Barneveld AV. When is pbl more effective? A meta-synthesis ofmeta-analyses comparing pbl to conventinal classrooms. Interdiscip JProblem-based Lear. 2009;3(1):44–58.
58. Chou F-H, Chin C-C. Experience of problem-based learning in nursingeducation at Kaohsiung medical university. Kaohsiung J Med Sci. 2009;25(5):258–63.
59. Lee J, Lee Y, Gong S, Bae J, et al. A meta-analysis of the effects of non-traditional teaching methods on the critical thinking abilities of nursingstudents. BMC Med Educ. 2016;16(1):240.
60. Kong LN, Qin B, Zhou YQ, Mou SY, et al. The effectiveness of problem-based learning on development of nursing students’ critical thinking: asystematic review and meta-analysis. Int J Nurs Stud. 2014;51(3):458–69.
61. Chan ZC. A systematic review of critical thinking in nursing education. NursEduc Today. 2013;33(3):236–40.
62. Rowan CJ, McCourt C, Beake S. Problem based learning in midwifery - thestudents' perspective. Nurse Educ Today. 2008;28(1):93–9.
63. Beers GW. The effect of teaching method on objective test scores: problem-based learning versus lecture. J Nurs Educ. 2005;44(7):305–9.
64. Peen TY, Arshad MY. Teacher and student questions: a case study inmalaysian secondary school problem-based learning. Asian Soc Sci. 2014;10(4):174–82.
65. Chan ZC. Role-playing in the problem-based learning class. Nurse EducPract. 2012;12(1):21–7.
66. Cooper G. Research into cognitive load theory and instructional design atUNSW. Sydney: University of New South Wales; 1998
67. Sweller J. Cognitive load theory, learning difficulty, and instructional design.Learn Instr. 1994;4(4):295–312.
68. Smith L, Coleman V. Student nurse transition from traditional to problem-based learning. Learn Health Soc Care. 2008;7(2):114–23.
69. Rowan CJ, McCourt C, Bick D, Beake S. Problem based learning in midwifery- the teachers perspective. Nurse Educ Today. 2007;27(2):131–8.
70. Gagne ED. Long-term retention of information following learning Fromeprose. Rev Educ Res. 1978;48(4):629–65.
Salari et al. BMC Medical Education (2018) 18:195 Page 14 of 15

71. Schmidt HG. Innovative and conventional curricula compared: What can besaid about their effects? In: Nooman HGS ZH, Ezzat ES, editors. Innovation inmedical education: An evaluation of its present status. New York, NY:Springer; 1990. p. 1–7.
72. Wittrock MC. Generative processes of comprehension. Educ Psychol. 1989;24(4):345–76.
73. Beers GW, Bowden S. The effect of teaching method on long-termknowledge retention. J Nurs Educ. 2005;44(11):511–4.
74. McMullan M, Jones R, Lea S. The effect of an interactive e-drug calculationspackage on nursing students' drug calculation ability and self-efficacy. Int JMed Inform. 2011;80(6):421–30.
75. Harasym PH, Tsai T-C, Munshi FM. Is problem-based learning an ideal formatfor developing ethical decision skills? Kaohsiung J Med Sci. 2013;29(10):523–9.
76. Boelens R, De Wever B, Rosseel Y, Verstraete AG, et al. What are the mostimportant tasks of tutors during the tutorials in hybrid problem-basedlearning curricula? BMC Med Educ. 2015;15(1):84.
77. Martenson D, Eriksson H, Ingelman-Sundberg M. Medical chemistry:evaluation of active and problem-oriented teaching methods. Med Educ.1985;19(1):34–42.
78. Dunlosky J, Rawson KA, Marsh EJ, Nathan MJ, et al. Improving students’learning with effective learning techniques promising directions fromcognitive and educational psychology. Psychol Sci Public Interest. 2013;14(1):4–58.
79. Anderson V, Reid K. Students' perception of a problem-based learningscenario in dental nurse education. Eur J Dent Educ. 2012;16(4):218–23.
80. Mubuuke AG, Louw AJN, Van Schalkwyk S. Utilizing students’ experiencesand opinions of feedback during problem based learning tutorials todevelop a facilitator feedback guide: an exploratory qualitative study. BMCMed Educ. 2016;16(1):6.
81. Ertmer PA, Newby TJ. Behaviorism, cognitivism, constructivism: comparingcritical features from an instructional design perspective. Perform Improv Q.2013;26(2):43–71.
82. Herndon VL. Changing places in teaching and learning: a qualitative studyon the facilitation of problem-based learning. Minnesota: Capella University;2016.
83. Dunkin MJ, Biddle BJ. The study of teaching. New York, NY: Holt, Rinehart &Winston; 1974.
84. Borhan MT. Problem based learning (pbl) in malaysian higher education: areview of research on learners' experience and issues of implementations.ASEAN J Eng Educ. 2012;1(1):48–53.
85. Klegeris A, Hurren H. Impact of problem-based learning in a large classroomsetting: student perception and problem-solving skills. Adv Physiol Educ.2011;35(4):408–15.
86. Dolmans DHJM, Grave WD, Wolfhagen IHAP, Vleuten CPM. Problem-basedlearning: future challenges for educational practice and research. Med Educ.2005;39(7):732–41.
87. Jalani NH, Sern LC. The example-problem-based learning model: applyingcognitive load theory. Procedia Soc Behav Sci. 2015;195:872–80.
88. Kong L-N, Qin B, Zhou Y-q, Mou S-y, et al. The effectiveness of problem-based learning on development of nursing students’ critical thinking: asystematic review and meta-analysis. Int J Nurs Stud. 2013;51(3):458–69.
Salari et al. BMC Medical Education (2018) 18:195 Page 15 of 15