PUO in the Tropics - fidssa.co.za · Differential diagnosis Occult abscess –abdomen, bone ......
34
PUO in the Tropics Helen van der Plas
Transcript of PUO in the Tropics - fidssa.co.za · Differential diagnosis Occult abscess –abdomen, bone ......

PUO in the TropicsHelen van der Plas

Outline
• Case Presentation
• Approach to fever in traveller
• Discussion of differential diagnosis
• Brief discussion of diagnosis


72 yr old Namibian Vet Fever for 3 months
• Fever 39.8 C
• Sweats
• Lassitude
• Weight loss
• No significant clinical findings
• No focal source of infection
Diagnosing the tropical traveller with fever
• Symptoms - nature, onset, duration
• Travel departure and return dates
• Region of travel
• Rural/urban/forest/mountains - nature of terrain
• Duration of visit - risk increases with length of stay
• Purpose of travel: healthcare workers, adventure travel
• Behaviour and lifestyle of traveller – fresh water exposure
• Degree of contact with the local population
• Known disease contacts
• Known insect or animal bites, scratches or licks
• Unprotected intercourse
• Diet whilst travelling
• Vaccination history
• Malarial prophylaxis and compliance
• Injuries or illnesses during travel

72 year old vet with undifferentiated fever
• Past Medical History• Past prostate Cancer
• prostatectomy 10 yrs ago
• Dyslipidemia• Hypertension • Asymptomatic diverticulosis
• Surgery • Tonsillectomy & adenoidectomy• Appendectomy• ORIF of clavicle• Ankle ligament repair
• Medication • Atorvastatin • Perindopril/HCTZ
• Vaccinations• Yellow fever• Hepatits A & B• Typhoid• Rabies


Past Travel

Short: ≤ 10 days
Intermediate: 10– 21 days
Long: > 3 weeks
Variable: Weeks to years
Arboviral infections (dengue, chikungunya, Zika, West Nile Virus)Rickettsial infection Gastroenteritis, acute (bacterial, viral)Relapsing fever (borrelia)Respiratory infection (bacterial, viral)Malaria (P falciparum, 6-90 days, usually <30 days)VHF: Lassa fever, Marburg virusEbola virus (2-12 days)PlagueYellow fever (3-16 days)
Bacterial:BrucellosisEnteric fever (typhoid and paratyphoid)LeptospirosisQ fever (Coxiella burnetii)BartonellosisProtozoal:Malaria (P. falciparum)Trypanosoma (East African)Fungal:HistoplasmosisViral:VHF : YF,Marburg,Ebola,LassaHIV,EBV,CMVViral Hepatitis
Bacterial:BrucellosisTBFluke:Schistosomiasis (acute)Protozoal:Amoebic liver abscessMalaria (including P. falciparum, P malariae)Trypanosoma bruceigambiense (West African)Visceral leishmaniasisViral:HIV, viral hepatitisHepatitis B (A, C,E)
AmoebiasisBrucellosis Chronic schistosomiasis Trypanosomiasis FilariasisHIV MelioidosisSystemic fungal infections Rabies Tuberculosis
Causes of tropically acquired fever by incubation period

Initial evaluation
Examination: Fever 39C
Imaging : CXR & Abdominal US normal
Initial lab investigations
HB 14.7 WCC 3.6 neutropenia PL 147
ALT 125 ALP 157 tBR25 cBR 6
CRP 32 ESR 48 PCT 0.5
Malaria smear and Ag test negative x2
Ricketsia PCR and AB’s negative
Brucellosis IgM neg IgG pos
Borrelia recurrentis smear – negative
Coxiella Antibodies neg
Hepatitis ABC neg
Microbiology: Stool Urine Blood

WBC differential in fever of
returning travellers
Leucopenia Leucocytosis Eosinophilia
Malaria* Malaria* Schistosomiasis
Typhoid Fever Amoebiasis Filariasis
Arboviruses Pyogenic Hydatid Disease
Rickettsiosis Leptospirosis Strongyloidiasis
Brucellosis Borreliosis Trichinosis
Empiric treatment ensued
Antibiotic exposure:
no response to
• 1st month • Ciprofloxacin x 5 days
• Cefuroxime x 5 days
• 3rd Month • Doxy x 3 weeks
• Genta x 1 week
Bone marrow trephine
Normal trilineage haematopoeisis
No blasts or dysplasia
One small granuloma with lymphoid
aggregates
Stains negative for fungi and TB

Short: ≤ 10 days
Intermediate: 10– 21 days
Long: > 3 weeks
Variable: Weeks to years
Arboviral infections (dengue, chikungunya, Zika, West Nile Virus)Rickettsial infection Gastroenteritis, acute (bacterial, viral)Relapsing fever (borrelia)Respiratory infection (bacterial, viral)Malaria (P falciparum, 6-90 days, usually <30 days)VHF: Lassa fever, Marburg virusEbola virus (2-12 days)PlagueYellow fever (3-16 days)
Bacterial:BrucellosisEnteric fever (typhoid and paratyphoid)LeptospirosisQ fever (Coxiella burnetii)BartonellosisProtozoal:Malaria (P. falciparum)Trypanosoma (East African)Fungal:HistoplasmosisViral:VHF : YF,Marburg,Ebola,LassaHIV,EBV,CMVViral Hepatitis
Bacterial:BrucellosisTBFluke:Schistosomiasis (acute)Protozoal:Amoebic liver abscessMalaria (including P. falciparum, P malariae)Trypanosoma bruceigambiense (West African)Visceral leishmaniasisViral:HIV, viral hepatitisHepatitis B (A, C,E)
AmoebiasisBrucellosis Chronic schistosomiasis Trypanosomiasis FilariasisHIV MelioidosisSystemic fungal infections Rabies Tuberculosis
Causes of tropically acquired fever by incubation period

Upon review in Cape Town 3 months into illness
His main symptoms:
ongoing daily fevers, sweats, lassitude, weight loss
new symptoms: dry cough and watery diarrhoea
Clinical findings
hepatomegaly tip of spleen palpable
few ecchymoses
NO adenopathy

Differential diagnosisOccult abscess – abdomen, bone
Subacute endocarditis
Typhoid
Brucellosis, Q-fever, leptospirosis , bartonella
Tuberculosis
Atypical mycobacterial infection
Fungal infection: histoplasmosis, cryptococcosis
Viral: HIV, EBV, CMV
Visceral Leishmaniasis
Malaria
Temporal Arteritis Polymyalgia rheumaticaAdult’s Still’s diseasePolyarteritis nodosa & VasculitisSarcoidosis
Haematological maligancye.g lymphoma, myeloma, leukemia,myelodysplastic syndromesRenal cell Ca or Hepatocellular Ca
Hemophagocytic lymphohistiocytosis
Atrial MyxomaMulticentric Castleman’s (HHV8)Thrombosis

Imaging
CXR normal
CT Sinuses: normal
CT chest: normal
CT abdomen and pelvis
Splenomegaly
Echocardiogram
No vegetations
10 days later CT chest abdomen, pelvis
No adenopathy
Spleen bigger

Cultures remain sterile
• Blood• Bacterial, fungal, mycobacterial
• Urine
• Stool
• Sputum

Repeat lab workPancytopenia
Transamintits with raised canalicularenzymes
Hyponatremia
ESR and CRP both ~100 now
Ferritin ~6500.
CK normal
SEP - inflammatory
Renal function & TFT normal
HIV neg Hepatitis ABC neg
Malaria smear & PCR negative
Brucellosis IgG pos only x2
Coxiella negative
Toxoplasma negative
EBV,CMV neg
Rickettsia negative
Serum BD glucan and Clat negative
Syphilis negative
Autoimmune markers incl. ANCA negative
S-ACE normal

And the counts continue to drop…..

Head for tissue
Granulomatous hepatitis Special stains and TB PCR negativeFungal and TB cultures pending
Mildly hypercellularSeveral reactive lymphoid aggregates Special stains negativeTB, HHV8 and bartonella PCR negative


And the GI tract
Both investigations normal
Histology duodenum and colon normal
PCR for Tropheryma whipplei negative
C. difficile toxin negative

You have friends - always ask for help!!

Enterprising virologist

Visceral Leishmaniasis

Leishmaniasis: visceral,cutaneous,mucocutaneous
VL 95% fatality if left untreated



Clinical manifestation
• Incubation period is usually 2 - 6 months (few weeks to several years).
• Insidious onset
• Visceral leishmaniasis (kala-azar): • fever, weight loss, hepatosplenomegaly,
pancytopenia, hypergammaglobulinemia
• Viscerotropic leishmaniasis: • Nonspecific abdominal tenderness; fever, rigors,
fatigue, malaise,
• nonproductive cough, intermittent diarrhea, headache, arthralgias, myalgias, nausea, adenopathy, transient hepatosplenomegaly
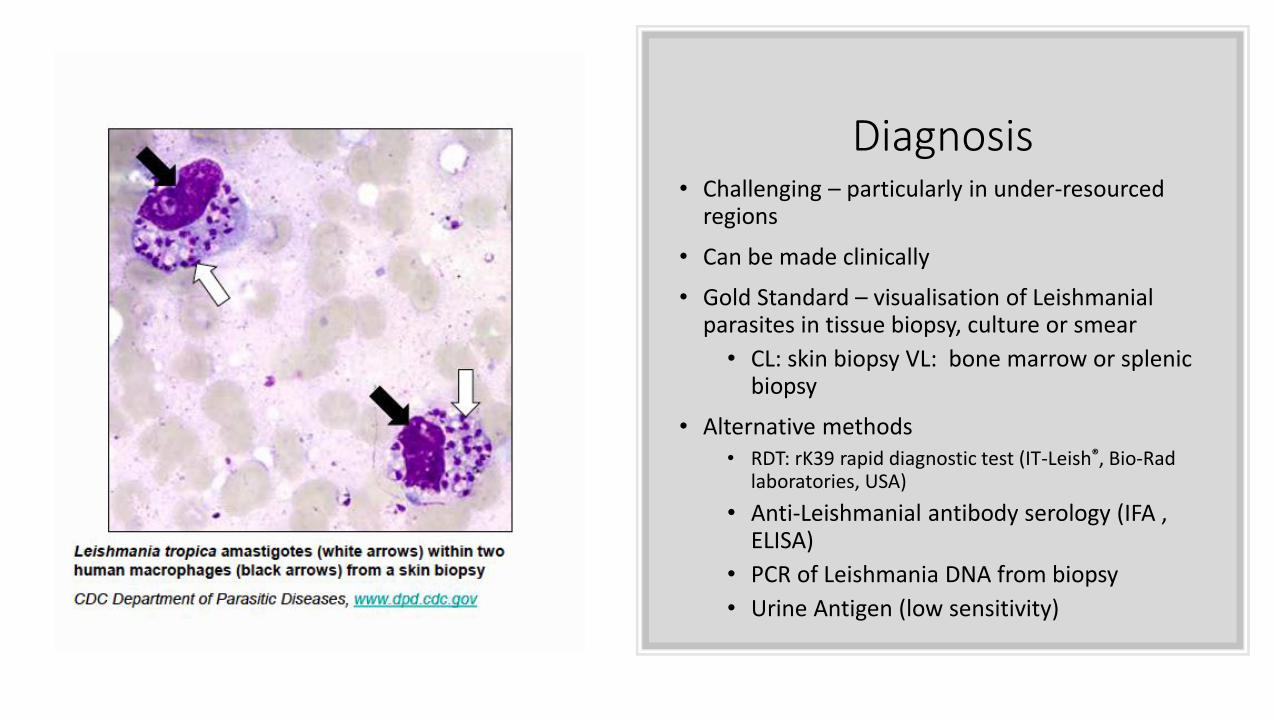
Diagnosis• Challenging – particularly in under-resourced
regions
• Can be made clinically
• Gold Standard – visualisation of Leishmanial parasites in tissue biopsy, culture or smear
• CL: skin biopsy VL: bone marrow or splenic biopsy
• Alternative methods • RDT: rK39 rapid diagnostic test (IT-Leish®, Bio-Rad
laboratories, USA)
• Anti-Leishmanial antibody serology (IFA , ELISA)
• PCR of Leishmania DNA from biopsy
• Urine Antigen (low sensitivity)

Treatment
• Liposomal Amphotericin B • 3mg/kg/day infusion
• Day 1 - 5
• Day 14
• Day 21
• Alternatives
• Miltefosine orally 100mg/d x 28 days
• Sodium Stibogluconate 20mg/kg/day x 30 days

Back to our vet…..
• Defervescence
• Overall feeling better
• Extensive mucocutaneous Herpes
• Blood counts recovered
• No relapse or complications

Thank you
• Lucille Blumberg and John Frean
• Wendy Spearman and Michael Locketz
• Craig Corcoran