PUNARJAGRAN
12
UNIVERSALIZING ACCESS TO QUALITY PRIMARY HEALTHCARE Team Details Proposed solution: Primary healthcare reforms based on PPP model and integrating medical students in the socio-corporate sector Vishnu Rajesh Upamanyu Mallik Sarosh Shashank Sripad Shubham Agarwal National Institute of Technology Karnataka
-
Upload
citizens-for-accountable-governance -
Category
Health & Medicine
-
view
3.402 -
download
1
Transcript of PUNARJAGRAN

UNIVERSALIZING ACCESS TO QUALITY PRIMARY HEALTHCARE
Team Details
Proposed solution: Primary healthcare reforms based on PPP model and
integrating medical students in the socio-corporate sector
Vishnu Rajesh
Upamanyu Mallik
Sarosh
Shashank Sripad
Shubham Agarwal
National Institute of Technology Karnataka

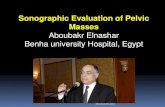
India suffers a shortfall of 2.6 million health workers.
31
7
13
6
47.2
72
32
87
48
4.1
0 50 100
Percentage of healthspending funded by public
sector
Physicians per 10000population
Nurses per 10000population
Hospital beds per 10000population
Infant Mortality Rate per1000 live births
OECD average India
Disgruntling facts about the Indian primary healthcare system:
Shortage of primary healthcare centres as envisaged in the 12th Five Year Plan. Only 23,109 PHCs as opposed to the proposed number of 40,000.
Severe shortage of doctors, nurses, paramedics. To live up to expected standards, the number of doctors across India are to be doubled (from 700,000 to 1.5 million), nurses tripled (from 800,000 to 2.5 million) and paramedics quadrupled (from 2.5 million to 10 million).
Very high infant mortality rate due to lack of access to maternity wards, primary healthcare centres. India’s infant mortality rate is 44.6 deaths/1000 live births as opposed to the OECD average of 4.6!
People prefer private sector healthcare, even in rural areas, in spite of various government subsidies. According to National Family Health Survey-3, the private medical sector remains the primary source of health care for 70% of households in urban areas and 63% of households in rural areas.
Shortage of ambulance services in government hospitals. According to an AIIMS study, 28% of SOS calls are ignored due to a shortage of ambulances.
Indian healthcare statistics against OECD averages

Outline of the three point solution proposed:
1. A public-private partnership model: private healthcare
providers are granted incentives to set up new Primary Health Care Centres, with a special focus on remote rural areas.
2. Students of private medical colleges are sent to various Primary Health Care Centres, as interns, on a short term basis to address the shortage of medical staff.
3. Students of government-run medical colleges are assigned the responsibility of organizing awareness programs regarding primary health facilities, sanitation and other related issues; along with the help of NGOs. Students of private colleges are encouraged to do the same.

1. A Public-Private Partnership model: private healthcare providers are granted incentives to set up new Primary Health
Care Centres, with a special focus on remote rural areas.
70% of urban population & 63% of rural population of India uses
private based healthcare facilities.
The inefficiency of the public healthcare facilities has led to the inception of the idea of ‘Public-Private Partnership’ model.
A 20 member committee
comprising retired IAS and IRS officers, headed by a retired Supreme Court Judge
This model is based on the
agreement that, 51% of voting equity rights will always be reserved by the Government.
GOVERNMENT
The central government allocates the funds to
the states
A ‘centralised body’ is set up to initialise,
manage, monitor, co-ordinate with state and
local bodies.
The central body is to survey and assign
internships.
PRIVATE
The private ‘sector’ establishes the
framework of the model
Infrastructure, organisational set-up
and daily management are under the private
‘players’
Profit balance is to be tilted in favour of the private ‘stakeholders’
Functions of the public and private sector

The required ‘governing’ bodies are established.
The ‘agreements’ regarding • 1.’Allocation’ of land/ infrastructure.
• With subsidised rates • 2.The share of ‘profits’ are decided; the private partner is
granted a slightly higher share of profits. • Direct corporate tax benefits
• 3. Discussions about ‘funding’ of the program. are tabled; ‘Part-investment’ by the private partner. The investment
will be made at subsidised prices (‘incentives’)
The allocated funds are utilised, and the ‘PHC’ is set-up.
The ‘P-P-P model’ based Primary Health Care centre
‘Centralised Body’ - Governing
Private ‘managerial’ body • ‘Organisational’ management • ‘Daily’ management
Subsidies are provided for the people who avail the services, & the process is aided by the Aadhar Card scheme’
SCHEME of IMPLEMENTATION

2. Students of private medical colleges are sent to various Primary Health Care Centres, as interns, on a short term basis to address
the shortage of medical staff.
• This proposal of sending private medical college students to intern at PHCs adheres to two problems: • Severe shortage of staff at
rural PHCs. PHCs cater to basic healthcare issues, and the contribution of medical interns would thus be significant.
• Lack of practical skills amongst medical students.
1. Categorizing PHCs according to shortage of
staff 2. Assigning
students appropriately
to suitable PHCs
1. Ensuring fully staffed
PHCs
2. Ensure smooth
running of and coordination
between state bodies
Central body
State government

• Each state government has these primary functions:
A. To classify the PHCs of its state according to staff shortage as: i. Sufficient staff ii. Slight shortage of staff iii.Severe shortage of staff and to submit a report of the same to the central body.
B. Students are to be assigned to PHCs, preferably nearby their colleges. Severely understaffed PHCs are to get 2 medical interns, slightly low on staff PHCs are to get 1 intern, and sufficiently staffed PHC do not require any intern.
• The central body is to coordinate with the private institutions and take the responsibility of the overall governing of the internship program.
• Students are to get a stipend of Rs. 30,000/month and are to serve in the PHCs for a period of 2 months, which is part of the 1 year mandatory internship.
18 states were identified for special focus by the NRHM in India. The model shall retain this provision and the PHCs will be set up accordingly.

3. Students of government-run medical colleges are assigned the
responsibility of organizing awareness programs regarding primary health, sanitation and other related issues; along with the help of local NGOs.
Students of private colleges are encouraged to do the same.
Interact with the local NGO setup & find out the core problems in that particular community and bring out awareness
Awareness programmes like street plays, puppet shows, putting up billboards, school visits and organizing small games for young children.
Preventive health care awareness is crucial. Also special focus on woman and child health awareness programmes
Students must give a strong emphasis on Information, Education including hygiene education and effective communication for behaviour change of locals along with involvement of Panchayati Raj Institutions (PRIs).
Students should make localities aware of the problems due to open defecation such as diseases like diarrhoea and try in helping them create better facilities for defecation
Twice a year a group of students from medical college, preferably with knowledge of the local language are sent to the district to spread awareness among the local village people
Private college student participation can be encouraged by giving community certificates issued by the government under the programme.

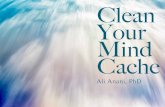
FUNDING
INDIA BRAZIL SRILANKA
MALI RUSSIA CHINA
15
335
38 18
306
85
Per Capita Public Spending onHealth (US$)
(Report from World Bank metadata)
₹16 bn for sending students as interns to PHCs
• 45,000 interns will be paid ₹30,000 a month
₹200 mn for organizing awareness programs
• 3000 students in groups of 15 will be sent for awareness programs to rural areas
₹200 bn for government subsidies and incentives to establish PHCs under PPP model
• 10,000 new PHCs to be set up
₹2 bn to set up a central body to supervise and allocate funds.
• Setting up the 20 member centralized body
₹373.33 bn has been allocated for public healthcare in the 2013 union budget. Our proposal aims at an increase to ₹600 bn in line
with the 12th five year plan

IMPACT
A major restructuring of budget will increase per capita public healthcare spending from US$ 21 (as envisaged in the budget) to US$ 34.
The interns from private medical colleges serving in PHCs will address the severe shortage of staff in the public healthcare system.
As a result the annual budget required for public healthcare will have to be increased to ₹600 bn.
By sending students to rural areas, the medical community will play a more direct role in improving the quality of primary healthcare.
The PPP model will instil a sense of socio-corporate responsibility amongst private healthcare providers.
The setting up of10,000 new PHCs at target locations, will improve accessibility to healthcare .

Challenges and risks
Mitigation factors
Government might be hesitant to fund the model.
As per the latest budget the government has already proposed a hike in public spending on healthcare from 1.6% to 2.2%
Initially corporate sector may not be attracted to the proposal.
Incentives and long-term benefits
Low co-operation in volunteering from private college students for awareness campaigns
Government issued certificate, awards.
Non-medical specific corporate houses can enter this partnership to avail the gain.
Proper auditing under the central body

Appendix:
o http://www.oecd.org/els/health-systems/Briefing-Note-INDIA-2013.pdf
o http://www.indiahealthprogress.in/reports-and-papers/primary-healthcare-needs-top-priority
o http://esango.un.org/irene/?page=viewContent&nr=380&type=2§ion=2
o http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3299104/
o http://www.data.worldbank.org