Public-Private Partnerships: A Handwashing and Hygiene Promotion Example April 26, 2007 Sara...
33
Public-Private Partnerships: A Handwashing and Hygiene Promotion Example April 26, 2007 Sara Abdoulayi, David Hostler, Stacey Succop, and Sarah Wilkins ENVR 890 003
-
date post
19-Dec-2015 -
Category
Documents
-
view
214 -
download
1
Transcript of Public-Private Partnerships: A Handwashing and Hygiene Promotion Example April 26, 2007 Sara...

Public-Private Partnerships: A Handwashing and Hygiene
Promotion Example
April 26, 2007Sara Abdoulayi, David Hostler,
Stacey Succop, and Sarah WilkinsENVR 890 003

Presentation Outline
• What is a public-private partnership?
• “Health in Your Hands” Handwashing Initiative
• Case studies from “Health in Your Hands”
• PPPs Problematic?
• Pros and cons of PPPs
• Recommendations and conclusions

What is a Public-Private Partnership?
• “…the combination of a public need with private capability and resources to create a market opportunity through which the public need is met and a profit is made.”
• According to the United Nations Development Program (UNDP), the broadest definition of a PPP includes agreement frameworks, traditional contracting, and joint ventures with shared ownership.
How does a public private partnership work?
• Public and private organizations work together to:
-determine a commonly-agreed upon goal for social benefit
-produce consumer research
-design and implement a promotional/educational campaign
-evaluate the campaign

Global handwashing partnership
• The World Bank and the Water and Sanitation Program $$
• Bank-Netherlands $$• USAID $$• London School of Hygiene and Tropical Medicine• Academy for Educational Development (AED)• UNICEF• CDC• Colgate-Palmolive• Proctor & Gamble• Unilever• National soap companies• National governments• NGOs

“Health in Your Hands”
• Global initiative for promoting handwashing and hygiene through public-private partnerships around the world
• Functioning for more than 5 years• Current projects in Ghana, Peru, Nepal• Project in Senegal is planned, but
delayed
“Health in Your Hands” Objectives
• To reduce the incidence of diarrheal disease, in particular among children under five, by making handwashing with soap at critical times universally recognized, promoted, and practiced.
• To implement large scale handwashing interventions and use lessons learned to promote the approach at the global level.
• Transparency among and equality of partners

Why partner to promote handwashing?
• Soap industry gains market expansion
• Public agencies benefit from the marketing expertise of the soap industry and thus have stronger capacity to relay health messages to target audiences via marketing campaign strategies
• Social responsibility

General Steps Followed by “Health in Your Hands”
• Catalyst initiates discussion (this can be an organization in the host country, an organization pursuing new projects, or a private company)
• Formation of a steering committee• Funds mobilization• Conduct handwashing behavioral study
(formative research)• Design communications strategy• Testing of communications strategy• Execution, monitoring, and evaluation

Case Study - Nepal
• Population: 28.9 million
• 1/3 below poverty line
• 75% subsistence farmers
• Remote and landlocked
• Civil strife• Susceptible to natural
disaster
Case Study – Nepal (2)
• 2003• Child mortality 91/1000 due to diarrheal
disease (DHS 2001)• 1 in 5 children suffer from diarrhea• More prone to diarrhea in households
with well-water source for drinking water

Case Study – Nepal (3)
• Public partners: UNICEF, World Bank, USAID/EHP
• Private partners: Nepal Lever Ltd., market leader (subsidiary of Unilever Inc.) and Aarti Soap and Chemicals, local company
Case Study – Nepal (4)
• Goal: To contribute to the reduction of diarrheal incidence through handwashing with soap at critical times and using correct techniques
• Objectives:• To generate awareness on importance of
handwashing with soap• Reach 5 million people, including 500,000
school children

Case Study – Nepal (5)
• Phase I: Consumer Baseline Survey• Phase II: Marketing Strategy
• Mass media advertising including posters, brochures, radio spots, and tv commercials
• Community-based outreach: female health volunteers, sanitation motivators, door-to-doorvisits, demonstrations in schools
• Phase III: Program Lauch (2004)• National Sanitation Action Week in May
2005
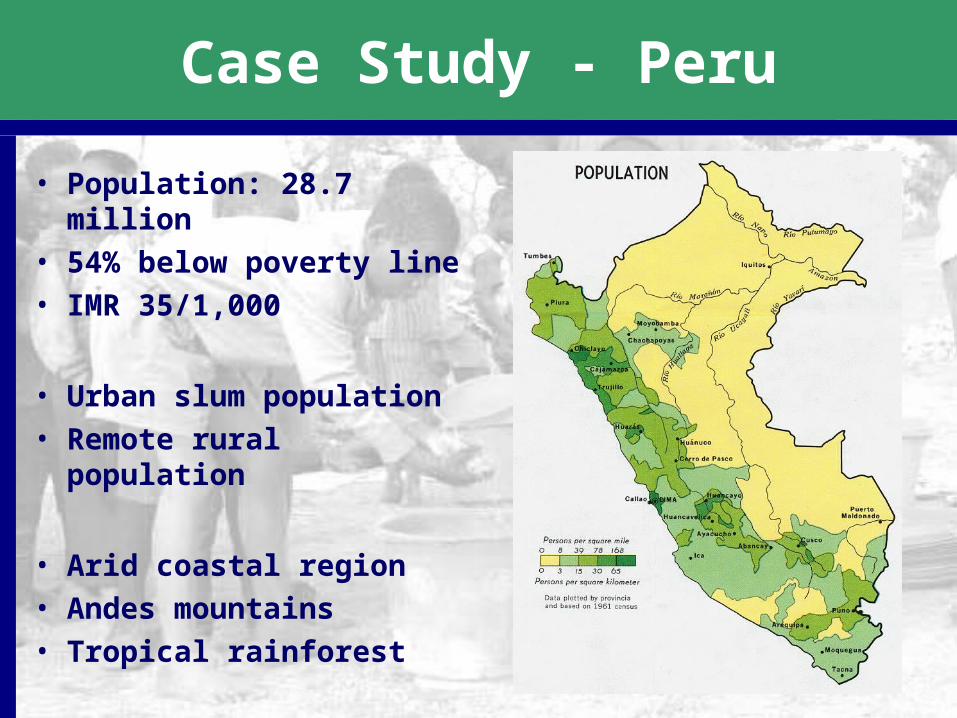
Case Study - Peru
• Population: 28.7 million
• 54% below poverty line• IMR 35/1,000
• Urban slum population• Remote rural
population
• Arid coastal region• Andes mountains• Tropical rainforest

Case Study – Peru (2)
• Need:• Diarrheal disease was the 3rd leading cause
of childhood disease
• Rationale:• Past efforts to improve water infrastructure
have not reduced diarrheal disease• Peruvian government expressed interest in
a PPP at World Bank Water Forum

Case Study – Peru (3)
• Timeline• Government expressed interest: May 2002• Project inception: March 2003• Formative research results: September 2004• Bidding for PPP design: July 2005• Formal launch of campaign: July 18, 2005• Evaluation: TBD
Case Study – Peru (4)
• Drivers• Mothers are judged by their children’s
grooming and health• Dirt, feces, and germs are widely
understood to cause disease
• Obstacles• “Soap and water are limited resources.”• “I’m careful when I defecate.”• “Doing laundry counts.”

Case Study – Peru (5)
• Public partners• Peruvian Ministry of Health (lead agency)• USAID (funds for formative research)• JSDF (funds for developing communications)
• Private partners• Colgate-Palmolive (printed materials/soap)• Boga Comunicaciones SA (cable TV)• Radio Programmas Peru (local radio)

Case Study - Ghana
• Population: 22.9 million
• Skewed towards young
• IMR 53/1,000
• 60% subsistence farmers
• Large refugee population from Liberia, Togo, etc.
Case Study – Ghana (2)
• Need: 25 % of deaths are due to diarrheal disease in children under age 5; 9 million cases of dd per year, and rising.
• Partnership initiated by Ghanaian government agency- Community Water and Sanitation Agency (CWSA) in 2001
• Rationale: • Reduce infant morbidity and mortality with
the end goal of reducing poverty.• Compliments the rural H20 sector strategy:
H20, Sanitation, Hygiene

Case Study – Ghana (3)
• Lead Agency: CWSA- coordinator
• Public sector/World Bank: Ministries of Works & Housing, Women’s & Children’s Affairs, NCWSP II- World Bank- $$$Ministry of Health - local health servicesMinistry of Education: School Health Education Program
• Private sector: Unilever, PZ-Cussons, GETRADE, AGI-Provide technical assistance; in-kind.
• External Support Agencies: UNICEF: Support to schools component.DANIDA: Support to schools component CIDA & WHO
Case Study – Ghana (4)
Drivers• HW after eating• HW after contact with public toilets.• Using soap to feel clean/ beautiful. • Mothers prioritize their children’s health
Obstacles:• Children’s stools are not thought
dangerous• Soap is often kept hidden to prevent
misuse • Scented soaps- luxury items;
interfere with the taste of food

Case Study – Ghana (5)
Initiatives:
• Mass Media – aimed at mothers and school aged children
• Direct Consumer Contact- visits to 2 districts in each of the 6 regions- (health care facilities, schools) ….
• District Level Program (through schools, health centers and communities)
• Public Relations and Advocacy

Case Study – Ghana (6)
• Phase 1 carried out from September 2003 to August 2004
• August 2004 - Evaluation of media initiative looked successful
• Commercials re-aired in 2005 to reiterate message.

PPPs -Problematic?: Kerala (1)
Characteristics of Kerala as compared to rest of India:
• highest hygiene standards• lowest diarrheal deaths• highest awareness on prevention of diarrheal
diseases• lowest childhood mortality• highest female literacy.• highest access to safe water
SO WHY KERALA???

PPPs -Problematic?: Kerala (2)
Ethical Implications:
• Risk of privatization of traditional government responsibilities
• Destroying indigenous practices• Polluting environment with new
industrial products

Overall Pros of PPPs
• Financial and in-kind resources are contributed
• Local & international efforts are combined• Locals guide the development with expert
aid• Efforts are focused on a circumscribed
problem• Programs are compatible with the
population • Education is a durable good

Overall Cons of PPPs
• Selection of partners can be tricky• Conflicts of interest to ensure profit• Financial leverage affects decision-
making• Shifting of responsibilities from
governments• Sustainability is questionable• Ethical considerations• Bureaucracy
Recommendations
• Can PPPs be applied to capacity building and infrastructure strengthening?
• Ideals/values and grounds for rejecting partnership should be established before entering a PPP
• Third-party monitoring• Rigorous monitoring & evaluation

Conclusions
• “Health in Your Hands” has exhibited some success and evaluations continue
• Some keys to success include:• Partnership equality/transparency• Community involvement • Rigorous formative research• Comprehensive evaluation
• PPPs are a relatively new concept• PPPs have pros and cons and will
require more research to establish best practices

Example PPPs
• Health in Your Hands• Global Alliance for Vaccines and
Immunization• International AIDS Vaccine Initiative• Medicines for Malaria Venture• Global Alliance for TB Drug Development• Initiative on Public-Private Partnerships for
Health (database)• Public-Private Partnerships for the Urban
Environment (database)

References
• World Bank, 1994. World Development Report• Thomas A. Curtis V. Public-private partnerships for health; a review of
best practices in the health sector. July 2003• The global public-private partnership to promote handwashing with soap
[Online] [cited 2007 April 21]; Available from: URL:www.globalhandwashing.org
• Buse, K.; Waxman, A. “Public-Private Health Partnerships: A Strategy for WHO.” Bulletin of the World Health Organization. August 2001, 79 (8), 748-754.
• Roberts, M.J.; Breitenstein, A.G.; Roberts, C.S. “Chapter 4: The Ethics of Public-Private Partnerships.” Public-Private Partnerships for Public Health. April 2002, Harvard University Press, Boston, MA.
• Wheeler, C.; Berkley, S. “Initial Lessons from Public-Private Partnerships in Drug and Vaccine Development.” Bulletin of the World Health Organization. August 2001, 79 (8), 728-734.
• Widdus, R. “Public-Private Partnerships for Health: Their Main Targets, Their Diversity, and their Future Directions.” Bulletin of the World Health Organization. August 2001, 79 (8), 713-720.
• PRISMA. “Behavioral Study of Handwashing with Soap in Peri-urban and Rural Areas of Peru.” Joint Publication 11E. September 2004. 1-159.
• Shiva, V. "Saving lives or destroying lives? World Bank sells synthetic soap & cleanliness to Kerala: the land of health and hygiene”
• “PPPHW program: the story of Ghana.” Available at http://www.globalhandwashing.org/Country%20act/ghanapu.pdf.