Public Health In The 21st Century
58
PUBLIC HEALTH IN THE 21st CENTURY: towards a people's health paradigm THE FIRST DR. N. H. ANTIA MEMORIAL LECTURE (Indian Health Front and PHM Tamilnadu) Dr. Ravi Narayan Community Health Adviser Society for Community Health Awareness, Research and Action Bangalore 28 th February 2008
-
Upload
cphe -
Category
Health & Medicine
-
view
9.621 -
download
1
description
Transcript of Public Health In The 21st Century

PUBLIC HEALTH IN THE 21st CENTURY: towards a people's health paradigm
THE FIRST DR. N. H. ANTIA MEMORIAL LECTURE (Indian Health Front and PHM Tamilnadu)
Dr. Ravi NarayanCommunity Health Adviser
Society for Community Health Awareness, Research and Action Bangalore
28th February 2008

Dr. N.H. Antia, FRCS, FACS (HON)18th Feb 1922 - 26th June 2007
• Surgeon
• Plastic Surgeon
• Leprosy Rehabilitation
• Foundation for Medical Research
• Foundation for Research in Community Health
•Association for Rural Surgeons
• Health for All activist ( PHM)
• NRHM and Advisory group on Community Action.
• People’s Health Sector Proponent.

People’s Health in Peoples HandsA Tribute
Health cannot be ‘delivered’ to the people…. Decentralized people’s based
health care is desirable as well as feasible under the prevailing social and economic conditions and in a
democratic set up..….• …..the People’s sector can achieve
both outreach and accountability, far more effectively and at much lower cost….. because health like education, lends itself best to people’s small scale action, which is in their own interest….
source : Dr. N.H. Antia, 1993

People’s Health in Peoples HandsA Tribute
“ I feel that appropriate science
and technology in every form and of every system should be utilized to solve our country’s and its people’s problems: not to glorify western technology for its own sake while denigrating our own….. Elegance is trying to find simple solutions to complicated problems, not the reverse…..
source : Dr. N.H. Antia, 1998

Alma Ata, 1978
The International Conference on Primary Health Care calls for urgent action by all governments, all health and development workers, and the world community to protect and promote the health of all the people of the world by the year 2000.

1978- Alma Ata Declaration-I.
• Health for All • Primary Health Care• Health a Fundamental Human Right• Equity • Appropriate Technology • Inter-sectoral Development • Community Participation.

19811981-- Health for All – An Alternative Strategy Health for All – An Alternative Strategy The Prescription of ICSSR and ICMR in IndiaThe Prescription of ICSSR and ICMR in India
• “A Mass movement to reduce poverty inequality and spread education.
• Organize poor and underprivileged to fight for their basic rights
• Move away from the counter productive western model of health care and replace it by an alternative based in the community …..”
- (Dr. N.H.Antia was member secretary of this committee)

1984- Community Health Definition (CHC)
• “Community Health is a process of enabling people to exercise collectively their responsibility to their own health and to demand health as their right.
• Community health involves increasing of the individual family and community autonomy over health and over the organizations, the means, the opportunities, the knowledge and the supportive structure that makes health possible”.

“From Alma Ata to the Millennium Declaration”

“From Alma Ata to the Millennium Declaration”
Source: Community Health Cell, Bangalore (www.sochara.org)
Accessibility ?
Affordability

THE PUBLIC HEALTH CHALLENGES IN INDIA
1. The continuing disease burden – Malnutrition– Communicable diseases– Non-communicable diseases– Mental Health / psycho-social / conflicts
2. The continuing problem of access of large sectors of the population to the determinants of health– Food security– Safe water– Clean environment – Adequate wage, and – Healthy work environment etc
3. The effects of globalization on Health and Health services CHC (2008)

Globalization and its health effectsGlobalization and its health effects
• Corporate led globalization, • Neo-liberal economic reforms,• Negative macro-policies
• Corporate led globalization, • Neo-liberal economic reforms,• Negative macro-policies
Adversely affect the social majority,
nationally & globally
Livelihoods,Incomes,
Food security,Increased conflict,War and violence,Access to water,
Access to health care,Environmental degradation,

What are the people saying?What are the people saying?
Less Food No Jobs No water

Increasing Poverty and inequality ….. The Increasing Poverty and inequality ….. The greatest obstacle to Health for All and the greatest obstacle to Health for All and the
Millennium Development GoalsMillennium Development Goals
Poverty / Inequality

•“ A retreat from the goal of national health and drug policies as a part of an overall social policy;
•A lack of insight into the inter-sectoral nature of health problems and the failure to make health a priority in all sectors of society;
•The failure to promote participation and genuine involvement of communities in their own health development;
•Reduced state responsibilities at all levels as a consequence of wide spread - and usually inequitable - privatization of health policies;
•A narrow, top-down, technology - oriented view of health”
RECOGNISING THE CRISIS IN INDIA-1990’SRECOGNISING THE CRISIS IN INDIA-1990’S

Meeting the challenges of India today
• Farmers Suicides
•Childhood Malnutrition
•The Virus of Communalism & Social Conflicts
•Life style Diseases Epidemics
•Resurgence / return of the vector borne diseases
•Development related displacement & ill health
•Pollution impacted communities And ……………………..
We need new paradigms and a new understanding!

The New Epidemiology
“ The primary determinants of disease are mainly economic and social and therefore its remedies must also be economic and social …
Medicine and politics cannot and should not be kept apart.”
- Prof. Geoffrey Rose, 1992The Strategy of Preventive Medicine

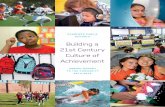
Researching levels of analysis and solutions
Levels of analysis of tuberculosis
Casual understanding of tuberculosis
Solutions / Control strategies for tuberculosis
Surface phenomenon (medical and public health problem)
Infectious disease / germ theory
BCG, case finding and domiciliary chemotherapy
Immediate cause Under nutrition/ low resistance, poor housing, low income / poor purchasing capacity
Development and welfare – income generation / housing
Underlying cause (symptom of inequitable relations)
Poverty / deprivation, unequal access to resources
Land reforms, social movements towards a more egalitarian society
Basic cause (international problem)
Contraindications and inequalities in socio-economic and political systems at international, national and local levels
More just international relations, trade relations etc.

What evidence?Disease?Ill-health?
Or social determinants like
Poverty?Gender bias?
Conflict?Stigma?
Social exclusion?
“From Alma Ata to the Millennium Declaration”

ARBO
VIRUSES
AGRICULTURAL DEVELOPMENT
ANIMAL HUSBANDRY
DEVELOPMENT
PROJECTS
FORE-STRY
LABOUR MIGRATION
URBANIZATION (including larger villages)
INTERNATIONAL TRAVEL/ ECO
TOURISM
WILD LIFE
SPORTS
(Hunting, Hiking)
CHANDIPURA
WEST NILECHIKUN
GUNYA
ALPHA
VIRUSES
?
KFD DENGUE
JE
New challenges of Globalization….INEQUALITY
MARGINALISATIONNEW ECONOMIC POLICIES
(Liberalization, Privatization, Globalization)
DIS
AS
TE
RS
:N
AT
UR
AL
&
MA
N-M
AD
EC
OM
ME
RC
IAL
IZA
TIO
N
OF
HE
AL
TH
CA
RE
DECREASED INVESTMENT IN SOCIAL SECTOR
PRIVATIZATION OF HEALTH CARE AND SOCIAL SECURITY
MO
RE
TR
AV
EL
LE
RS
/ M
OR
E D
ES
TIN
AT
ION
S
UN
SU
ST
AIN
AB
LE
D
EV
EL
OP
ME
NT
AN
D
DIS
PL
AC
EM
EN
T

An Agenda for Change -1998
“ A need for strong countervailing movement initiated by health and development professionals and activists, consumer and people’s organizations to bring health care and medical education and their right orientation high on the political agenda of the country and to ensure that the health policy choices are led by people’s health needs, not market factors”

2000-Preparing Campaign Materials for Health Mobilization

2000- Jan Swasthya Sabha, Kolkata
Over 2000 participants in 5 peoples health trains Mobilization across 19
states Adopted 20 point Indian
People’s Charter Launched the Jan Swasthya Abhiyan, campaigning for
Health for All Now
Health as a Fundamental
Human Right

Indian People’s Health Charter… We reaffirm our inalienable right to and demand for comprehensive health care that includes food security; sustainable livelihood options including secure employment opportunities; access to housing, drinking water and sanitation; and appropriate medical care for all; in sum - the right to Health For All, Now! …
… We declare health as a justiciable right and demand the provision of comprehensive health care as a fundamental constitutional right of every one of us. We assert our right to take control of our health in our own hands…
… Ethical guidelines for research involving human subjects be drawn up and implemented after an open public debate…
December 2000Kolkota, India

The First Global People’s Health Assembly
In 2000 December 1454 health activists from 75 countries met in Savar, Bangladesh to discuss the challenge of attaining Health for All, Now! Over 250 Indian delegates attended

“Health is a social, economic and political issue and above all a fundamental human right.”
The People’s Charter for Health

“Health for all means that powerful interests have to be challenged, that globalisation has to be opposed, and that political and economic priorities have to be drastically changed.”
The People’s Charter for Health

PEOPLE’S CHARTER FOR HEALTH PRINCIPLES
HEALTH IS FUNDAMENTAL HUMAN RIGHT
PRIMARY HEALTH CARE(1978 Alma Ata
Declaration)BASIS FOR POLICY
GOVERNMENTS FUNDAMENTAL
RESPONSIBILITY TO ENSURE ACCESS AND
QUALITY
PEOPLE AND PEOPLES ORGANISATIONS ESSENTIAL
TO FORMULATION, IMPLEMENTATION,
EVALUATION OF HEALTH PROGRAMMES
POLITICAL / ECONOMIC SOCIAL / ENVIRONMENT ARE PRIMARY DETERMINANTS OF HEALTH AND MUST GET TOP PRIORITY IN POLICY MAKING
ACTION AT ALL LEVELS TO TACKLE CRISIS
-Individual-Community-National-Global

PHC in the New MillenniumNew Challenges
• Health as a human right• Tackling broader determinants of health – Economic, Social
and Political challenges• Tackling environmental challenges and unsustainable
developments• Countering war, violence, conflict and natural disasters.• Rediscovering Universal and Comprehensive Primary Health
Care• People’s organisations, People’s Movements and Civil Society
involvement in dialogue, analysis, action, monitoring and evaluation.

Publications

People’s Health Movement (Global) from 2000 AD:
1. People’s Charter for health2. Global Health Watch3. International People’s Health University

Globalizing solidarity from over 80 countries at the Second People’s Health Assembly,
Cuenca Ecuador

Peoples voices at national levelPeople’s health tribunals in India

Peoples Health Tribunals 2004“Jan Sunwais”
Objectives
Bring ‘Public’ back into ‘Public Health’
Evidence gathering on the denial of Right to Health Care and other discriminations.
Increase pressure on government to make health systems responsive to ethics and human rights paradigm.

PHM India
• Dialogue with political parties
• State and national health policy Dialogue
• Right to Health Care Campaign with National Human Rights Commission
• People’s Rural Health Watch
• Support to Campaigns: Right to Food; Against Water Privatization; Access to Essential Medicines- Patents/TRIPS; Environment issues; Gender; HIV / AIDS; Women’s Health

The People’s Health Paradigm:some Challenges
• Rights • Ethics
• Political Economy • Medical Pluralism
• People Oriented Professionals• Community Participation and
Monitoring.

Right to Health MovementRight to Health Movement

Countering Commercialization by Medical Ethics
CHC Advocacy with Health University to introduce ethics in undergraduate curriculum (1999)
Ordinance
“The Doctor should be trained to analyze the ethical problems as they arise and deal with them in an acceptable manner. It is therefore recommended that teaching of Medical Ethics be introduced n Phase I and continued throughout the course including the internship period”.
Syllabus
Includes Introduction, perspectives, ethics of individuals, ethics of human life, ethics of family and society, death and dying, professional ethics, research ethics and ethical case work
-RGUHS (1997-98)

THE POLITICAL ECONOMY CHALLENGE
• Countering the market economy in health system development
• Countering market needs that take over from people’s needs
• Strengthening equity, gender and the rights paradigms in health policy.

“Respect communities and its diversities….
Support, recognize and promote traditional and holistic healing systems and practioners and their integration into Primary Health Care “
Medical Pluralism Challenge.(AYUSH in Public Health)
Source: PCH- Dec 2000.

Community Orientation of Health Teams
Medico Friends Circle reflections (1991)
recommends:
• Community oriented, Socially conscious, primary health care provider
• Multi-disciplinary health analysis and collective societal solution
• Political economy, ethics and value orientation
• Medical teachers – ethics and value orientation and learning facilitation
• Links with peripheral hospitals and community projects
• Institution part of community health/ people’s health network

Political Will
“ We recognize health as an inalienable human right that every individual can justly claim.
So long as wide health inequalities exist in our country and access to essential health care is not universally assured, we would fall short in both economic planning and in our moral obligations to all citizens”
- Dr. Manmohan Singh at AIIMS recently

New Challenges: National Rural Health Mission (NRHM) Civil Society Engagement.
• Members of Task Force and Advisory Committee
• Shifted the missions focus from Demography to Public Health
• Community Monitoring• People Rural Health Watch• ASHA Mentoring Group

Evolving Network of Schools of Public Health and MPH Courses
• Public Health Foundation of India (4 Indian Institutes of Public Health)
• ICMR Schools of Public Health ( 4 regional clusters including NIE,Chennai)
• Existing Schools being strengthened – AIIPH, AMCHSS , IHMR, and JNU – CSMCH
• Medical college based MPH courses or schools (CMC-Vellore, SJNAHS, MGR, PMC , MMC and KMC etc)
• New initiatives – NICD, TISS, NIMHANS,CHE

Engagement with Alternative Sector.
• “A wave of community health NGO movements has taken place to try alternative experiments and actions, and to
build capacity from communities and grass root workers….. These include PHM, SOCHARA, CEHAT and others….. Unless
the national apex institutions or schools of public health recognize these alternative sectors as strong resources and
involve them in training and research , a large portion of creative energy in public health will remain untapped".
Source: South East Asia Public Health Initiative 2004-2008, WHO-SEARO

Promoting new types of research
Not onlyDrug and vaccine trialsEpidemiological studies
Operations researchBut also
Health policy studiesHealth systems research
Research on social determinantsand political economy of health
Developing a research and advocacy agenda for Health

Developing a research and advocacy agenda for Health
Translating research into policy, advocacy and action to strengthen accountability

In Conclusion.
THE NEED FOR A PARADIGM SHIFT
Approach Biomedical Model Social Community Model
Focus Individual Community
Dimensions Physical / pathological Psycho- social, cultural, economic, political, ecological
Technology Drugs / vaccines Education and social processes
Type of service
Providing/ Dependence creating / Social marketing
Enabling / EmpoweringAutonomy Building
Link with people
Patient as passive beneficiary Community as active Participant
Programmes and Campaigns Social Movements
ARE WE READY FOR THIS CHALLENGE ?

“From Alma Ata to the Millennium Declaration”
Recognizing the People’s ParadigmWhy Renew PHC?
For many in the region there is a feeling that, “health is a social, economic and political issue and, above all, a fundamental right, and inequality, poverty, exploitation, violence, and injustice are at the root ill-health and the death of poor and marginalized people” pp:
(Quoting People’s Charter for Health in PAHO PHC document 2007, )

“From Alma Ata to the Millennium Declaration”
Recognizing the People’s ParadigmSuccessful PHC services:
-Encourage (community) participation
-Are accountable
-Have appropriate level of investment to guarantee adequate services
-Ensure services are accessible regardless of person’s ability to pay(Quoting People’s Charter for Health Quoting People’s Charter for Health in PAHO PHC document 2007, )

Recognizing the People’s Paradigm
The Peoples Health Movement is an international network of organization and individuals that came together in 2000 to reignite the call for the Health for All, Now. The goal of PHM is to reestablish the health and equitable development as top priorities at local, national and international policy making, with comprehensive primary health care as the strategy to achieve this priorities…….
It is transnational network …… and a good example of an emerging player in global civil society… On a day today basis the secretariat in Bangalore …… puts forward strategic campaigning priorities….
Source: Public Health Text Book - UK

Recognizing the People’s Paradigm
“A strong voice in the global health debate for free primary health care is the people’s health movement which in 2000, presented the Peoples Health Charter. The charter argues strongly for a publicly financed health services and for development policies that favors health…. This network presently led from Bangalore in India is a leading representative for NGO’s in the Global health debate. This global network is itself a new aspect of globalization”
Source: Public Health Text Book- Sweden.

Can the shift towards the People’s Health Paradigm become a power to counter the following ills of the existing
• Corruption
• Neglect of public health
• Distortions in primary health care
• Lack of equity process
• Implementation gap
• Need for ethical imperative
• Human resource development neglected
• Cultural gap and challenge of pluralism
• Ignoring political economy
• Exclusivism rather than partnerships
• Inadequate policy research….
Source: Karnataka Task force on Health and Family Welfare - 2001

People’s Health in Peoples HandsDr. Antia’s Response
• “Decentralized people based health care
• People operated health services• Demystification of Health to
strengthen people’s involvement• Humane, cost effective and
accessible health and medical care for all citizens
• From unaccountable top-down system to an accountable bottom-up system
• Small efficient people’s market not exploitative national or international market or distant centralized bureaucracy…..”
What will be your contribution ?

Shimoga - 2006

Thank you
www.phmovement.org

Health for All, Now !
JOIN US THANK YOU

For further information visitwww.sochara.org
www.phm-india.orgwww.phmovement.org
www.ghwatch.orgwww.iphcglobal.org