
Psychosocial Health and Work Conference, Ljubljana, 9 October 2008 The economic dimensions of mental...
34
Psychosocial Health and Work Conference, Ljubljana, 9 October 2008 The economic dimensions of mental health Dr Anita Patel Senior Lecturer in Health Economics Institute of Psychiatry, King’s College London
-
Upload
melanie-melton -
Category
Documents
-
view
214 -
download
0
Transcript of Psychosocial Health and Work Conference, Ljubljana, 9 October 2008 The economic dimensions of mental...

Psychosocial Health and Work Conference, Ljubljana, 9 October 2008
The economic dimensions of mental health
Dr Anita Patel
Senior Lecturer in Health Economics
Institute of Psychiatry, King’s College London
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Outline
1. Adults of working age
2. Children & young people
3. Older people

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Outline
1. Adults of working age
2. Children & young people
3. Older people

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Where does economics come in?
Mental health problems place a clinical and social burden on individuals, families and communities
All of these burdens have economic dimensions, which impact on all levels of society

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Health care
Products
Human resources/services

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Family burden
Time
Average weekly hours caring for person with schizophrenia:
Amsterdam 0.9
Leipzig 6.9
London 10.6
Verona 5.2
Lost work, leisure & education opportunities
Lost income
Out of pocket expenses
Family strain
Unpublished figures from the QUATRO Study (European Union QLG4-CT-2001-01734)
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
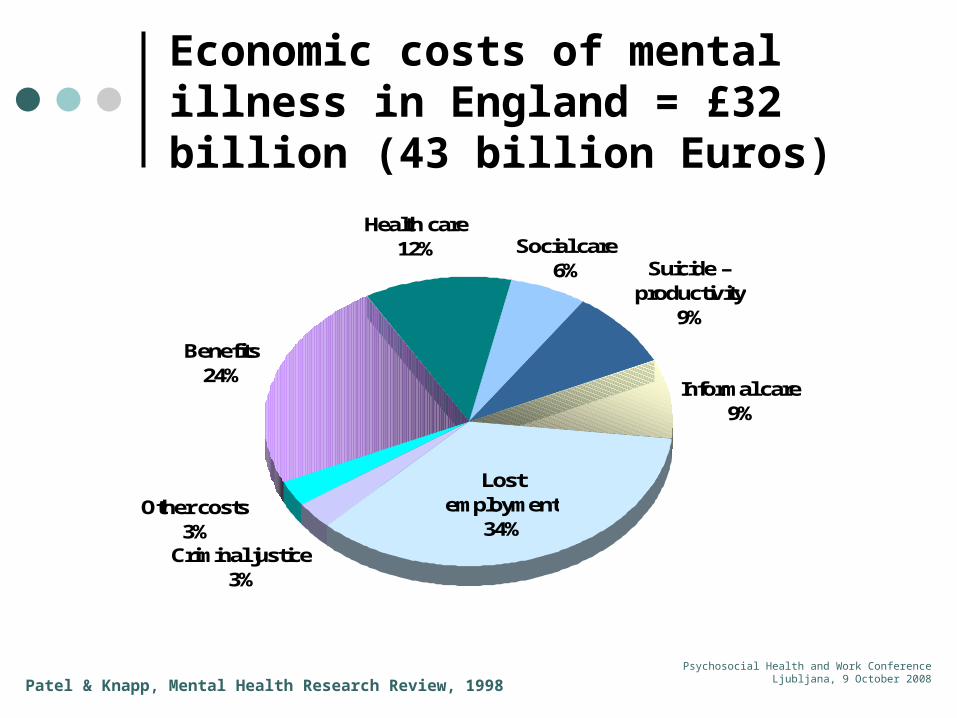
Economic costs of mental illness in England = £32 billion (43 billion Euros)
Informal care9%
Lost employment
34%Other costs
3%
Benefits24%
Health care12% Social care
6%
Criminal justice3%
Suicide – productivity
9%
Patel & Knapp, Mental Health Research Review, 1998
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
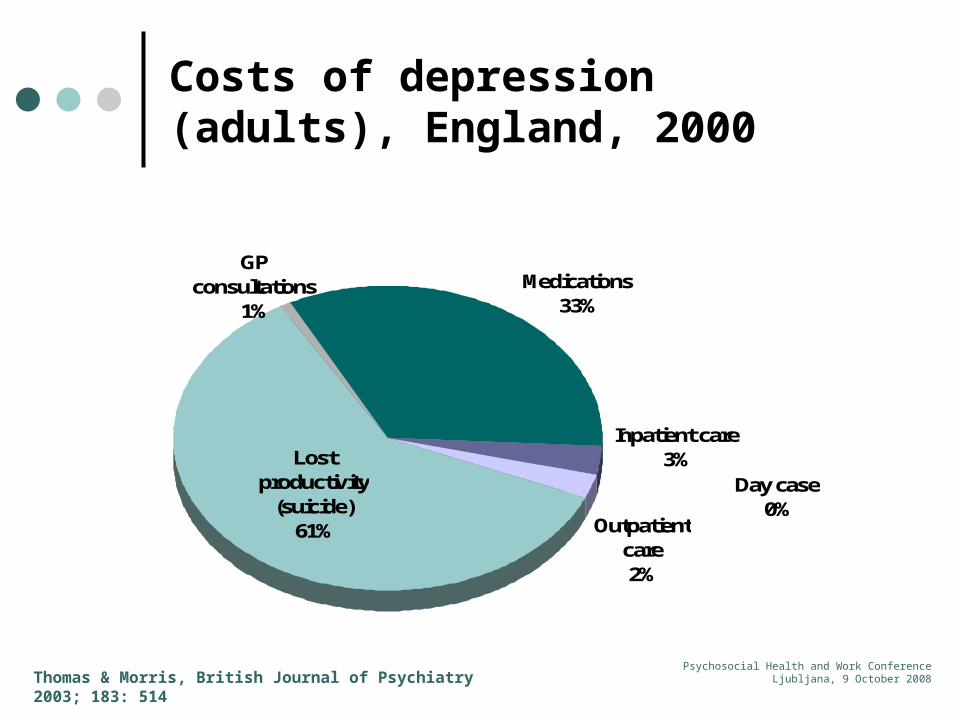
Costs of depression (adults), England, 2000
Day case0%
Outpatient care2%
Inpatient care3%Lost
productivity (suicide)
61%
Medications33%
GP consultations
1%
Thomas & Morris, British Journal of Psychiatry 2003; 183: 514

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Costs of depression (adults), England, 2000
Lost productivity (morbidity)
90%
Lost productivity
(suicide)6%
Treatment costs
4%
Thomas & Morris, British Journal of Psychiatry 2003; 183: 514
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
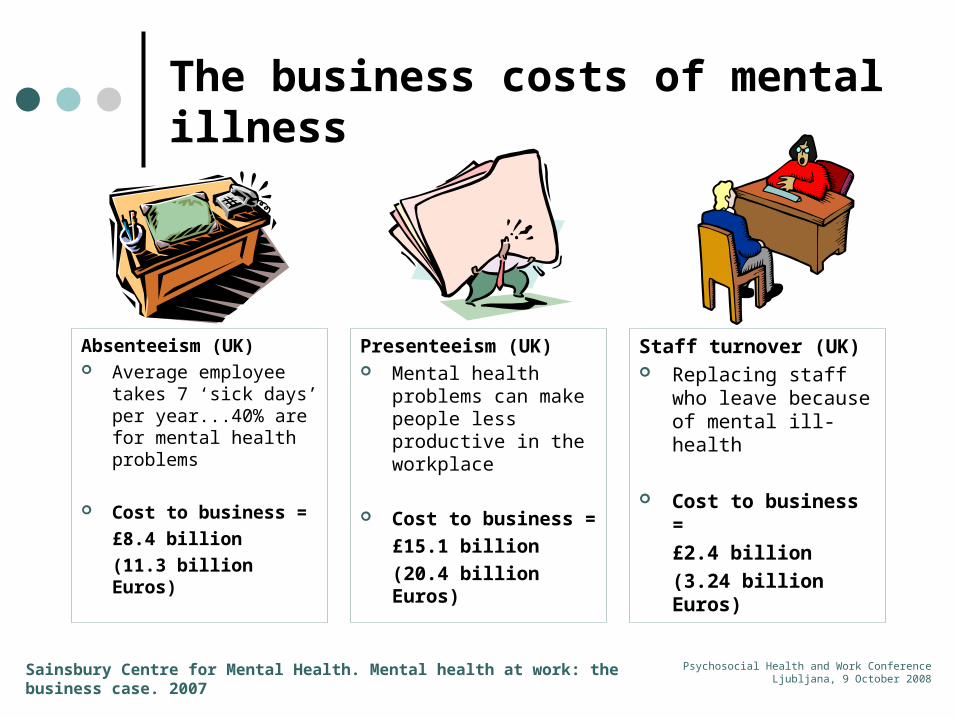
The business costs of mental illness
Absenteeism (UK) Average employee
takes 7 ‘sick days’ per year...40% are for mental health problems
Cost to business =
£8.4 billion
(11.3 billion Euros)
Presenteeism (UK) Mental health
problems can make people less productive in the workplace
Cost to business =
£15.1 billion
(20.4 billion Euros)
Staff turnover (UK) Replacing staff who
leave because of mental ill-health
Cost to business =
£2.4 billion
(3.24 billion Euros)
Sainsbury Centre for Mental Health. Mental health at work: the business case. 2007
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
A caution about interpreting lost productivity costs
Many lost productivity estimates are calculated as:
Number of days absent x average daily wage
This (‘human capital’) approach could lead to over-estimates
Workers may compensate for short term absence (Jacob-Tacken et al, 2005) Workers may be replaced. So only need to calculate costs of the intervening
(‘friction’) period e.g. advertising, recruiting, training, low productivity in early phase
Lost productivity due to schizophrenia-related deaths (1996)
Human capital approach = Canadian $105 million Friction cost approach = Canadian $1.53
(Goeree et al, 1999)

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Other large financial impacts
Early retirement – lost productivity
Disability pensions
Disability-related social security benefits
(Approximately 40% of people receiving Incapacity Benefit in UK is due to mental illness)
Lost tax income for government
Insurance payouts
Centre for Economic Performance, LSE, 2006
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Economic burden of mental illness
We now know something about:
How large this burden is
How the burden is distributed across the economy
The potential savings from tackling some of the problems
But what can we do about it?
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
What can we do about it?
There are numerous examples of health care, social care, educational and vocational interventions that work
But we can’t pay for them all
Firstly, there are not enough professional, pharmaceutical and other resources to meet all assessed needs
Secondly, even if local, national & Europe-wide budgets were greatly increased, we still need to decide how to allocate these extra funds as effectively as possible
Thirdly, we need to consider equity, not only within mental health sphere but also outside of it…other health and welfare programmes may equally deserve more investment
Economic evaluation can help inform such decisions by considering costs as well as effectiveness
Example….
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
EQOLISE: evaluation of a supported employment scheme
Sample of 312 people
Adults with diagnosis of psychotic illness Minimum 2 years duration Living in community Not been in competitive employment in previous year Expressing desire to enter competitive employment
Randomised controlled trial
Individual placement and support (IPS) versus existing rehabilitation and vocational services
6 European cities: Zurich, London, Ulm, Sofia, Rimini, Groningen
Burns et al., Lancet 2007; 370:1146

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
EQOLISE: effectiveness
Employment rate 27% higher Average of 100 more days of work
0
20
40
60
80
100
120
140
% worked Mean days
IPS
Vocational services
Burns et al., Lancet 2007; 370:1146
IPS worked…
No significant differences between the two groups in other outcomes
But some association between working more and better social functioning, clinical and quality of life outcomes

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
EQOLISE: costs
Mean difference in health & social care costs (£) over 18 months
-10000
-7500
-5000
-2500
0
2500
5000
Burns et al., Report to EC 2006 (Project QLRT-2001-00683)
And it cost less…so IPS is cost-effective
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
A caution about interpreting international evidence
EQOLISE: effectiveness varied across the centres (socio-economic factors, such as GDP growth per capita and local unemployment rate, explained some of this variation)
Costs also varied across sites, with no cost savings in Groningen
This is not an unusual finding….
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
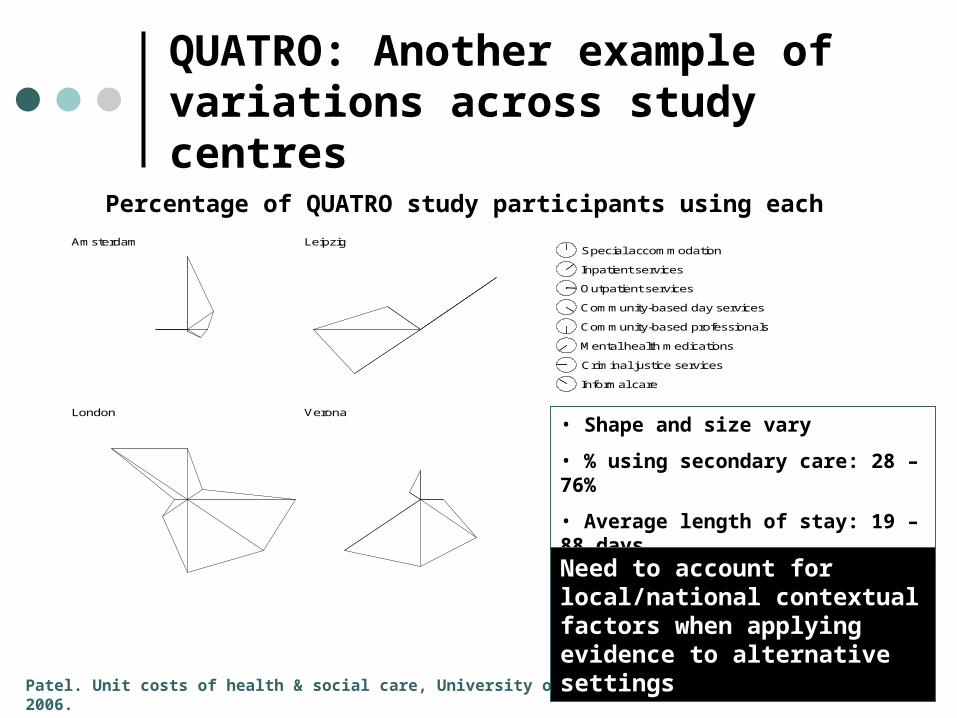
QUATRO: Another example of variations across study centres
Percentage of QUATRO study participants using each resource
Patel. Unit costs of health & social care, University of Kent, 2006.
Special accommodation
Inpatient services
Outpatient services
Community-based day services
Community-based professionals
Mental health medications
Criminal justice services
Informal care
Amsterdam Leipzig
London Verona
• Shape and size vary
• % using secondary care: 28 – 76%
• Average length of stay: 19 – 88 days
Need to account for local/national contextual factors when applying evidence to alternative settings
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Outline
1. Adults of working age
2. Children & young people
3. Older people
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Children & young people
How many people are affected? 10-20% of European children and adolescents suffer from
mental health problems Suicide is one of the 3 most common causes of death Other family members are affected
With what consequences? Poor quality of life; damaged family relations Disrupted education; failure to fulfil potential Enduring problems into adulthood High costs to individuals, families, State & economy
See Jane-Llopis & Braddick, EC Consensus Paper, 2008
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
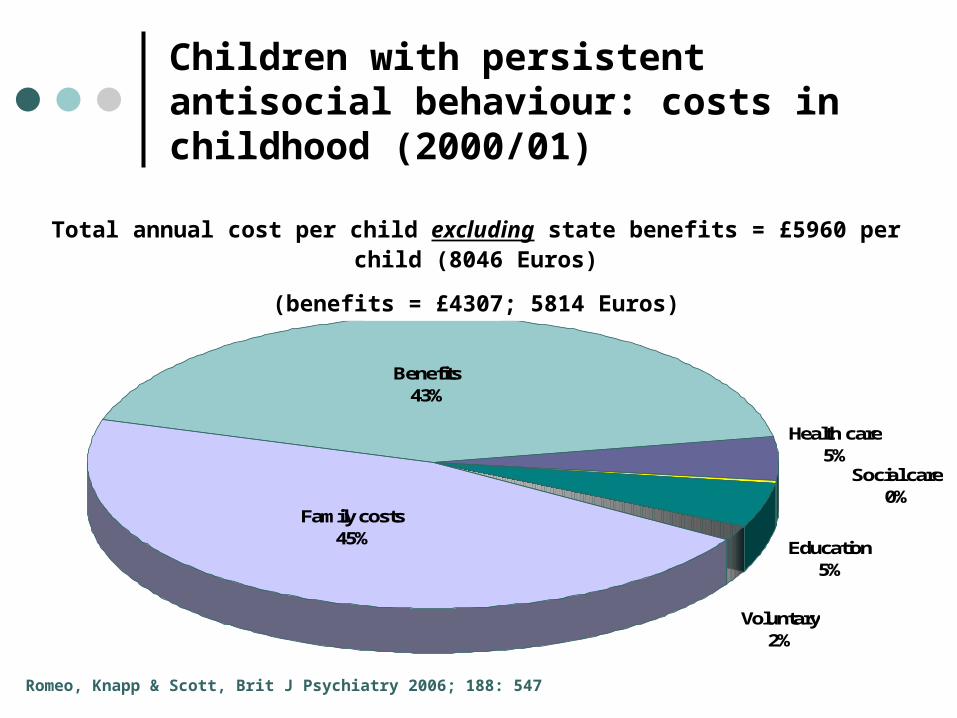
Children with persistent antisocial behaviour: costs in childhood (2000/01)
Health care5%
Social care0%
Benefits43%
Voluntary2%
Education5%
Family costs45%
Romeo, Knapp & Scott, Brit J Psychiatry 2006; 188: 547
Total annual cost per child excluding state benefits = £5960 per child (8046 Euros)
(benefits = £4307; 5814 Euros)

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Children & young people
How many people are affected? 10-20% of European children and adolescents suffer from mental health problems Suicide is one of the 3 most common causes of death Other family members are affected
With what consequences? Poor quality of life; damaged family relations Disrupted education; failure to fulfil potential Enduring problems into adulthood High costs to individuals, families, State & economy individuals, families, State & economy
See Jane-Llopis & Braddick, EC Consensus Paper, 2008
What can we do about it? Parenting support Prevent bullying & violence Support in schools
Work with communities Tackle poverty Better treatment access
But we can’t do everything…so need cost-effectiveness evidence
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Outline
1. Adults of working age
2. Children & young people
3. Older people

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Older people
How many people are affected? 5 million or more older Europeans have dementia 10-15% of people aged 65+ have depression Suicide rate is highest for older people
With what consequences? Again – devastating impacts on quality of life Heavy burdens falling to family carers But often these consequences remain hidden High costs to individuals, families, State & economy
Knapp, Prince et al, Alzheimer’s Society, 2007
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
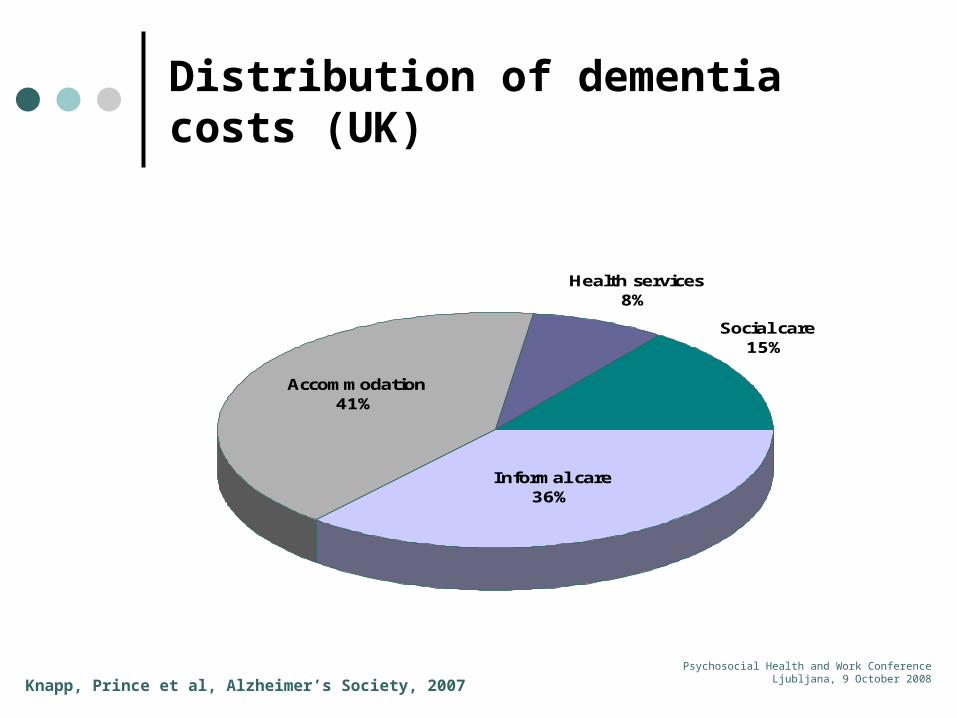
Distribution of dementia costs (UK)
Accommodation41%
Social care15%
Health services8%
Informal care36%
Knapp, Prince et al, Alzheimer’s Society, 2007
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
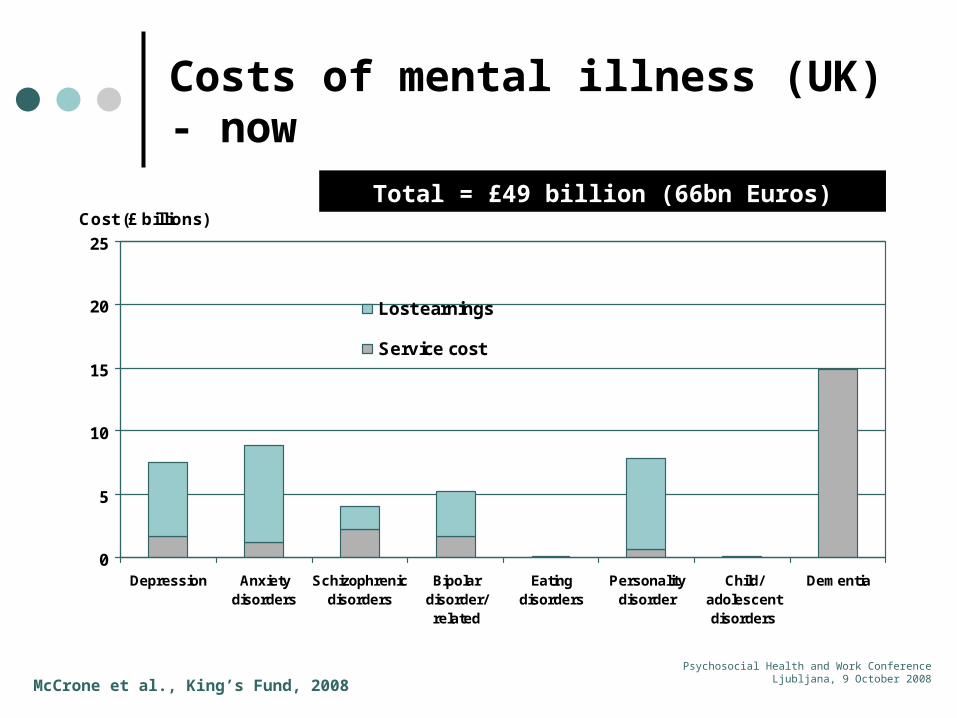
Costs of mental illness (UK) - now
McCrone et al., King’s Fund, 2008
0
5
10
15
20
25
Depression Anxietydisorders
Schizophrenicdisorders
Bipolardisorder/related
Eatingdisorders
Personalitydisorder
Child/adolescentdisorders
Dementia
Cost (£ billions)
Lost earnings
Service cost
Total = £49 billion (66bn Euros)
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
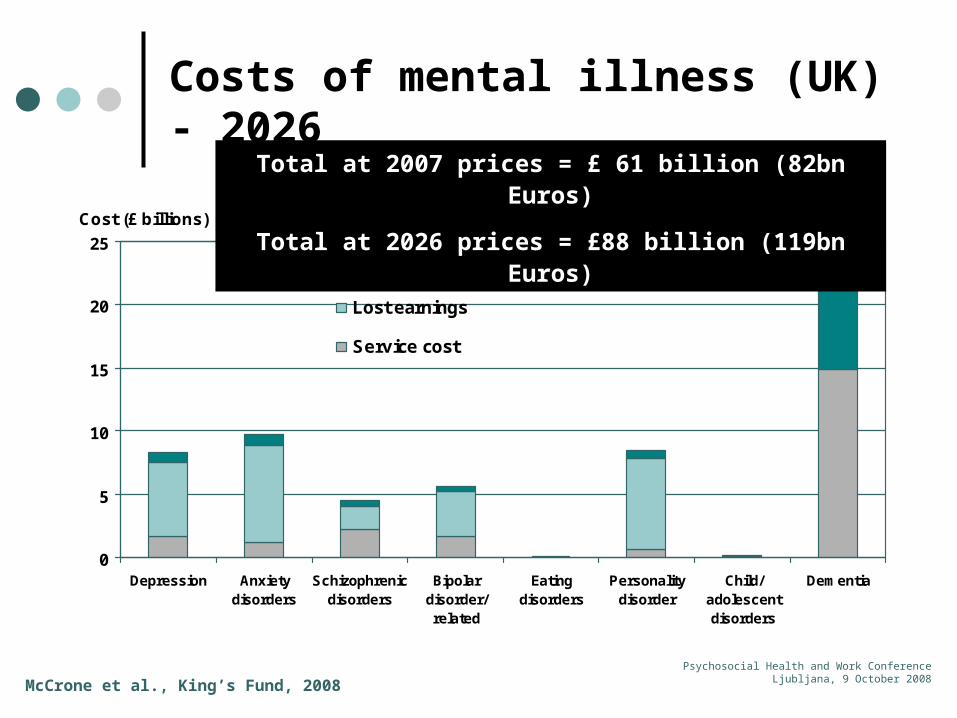
Costs of mental illness (UK) - 2026
McCrone et al., King’s Fund, 2008
0
5
10
15
20
25
Depression Anxietydisorders
Schizophrenicdisorders
Bipolardisorder/related
Eatingdisorders
Personalitydisorder
Child/adolescentdisorders
Dementia
Cost (£ billions)
Additional cost in 2026 (2007 prices)
Lost earnings
Service cost
Total at 2007 prices = £ 61 billion (82bn Euros)
Total at 2026 prices = £88 billion (119bn Euros)

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Older people
How many people are affected? 5 million or more older Europeans have dementia 10-15% of people aged 65+ have depression Suicide rate is highest for older people
With what consequences? Again – devastating impacts on quality of life Heavy burdens falling to family carers But often these consequences remain hidden High costs to individuals, families, State & economy
See Jane-Llopis & Gabilondo, EC Consensus Paper, 2008
What can we do about it? Better treatment access Better preventative efforts Support for carers
Social integration Choice and control
But we can’t do everything…so need cost-effectiveness evidence

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Potential annual savings from selected interventions
Condition and interventions 2007 2026
Depression
Medication for those currently untreated £5 – 36 m £8 – 61 m
Medication + psychological therapy for those currently untreated £1 – 9 m £2 – 16 m
Anxiety disorders
Medication for those currently untreated £8 – 66 m £13 – 102 m
Medication + psychological therapy for those currently untreated £1 – 7 m £2 – 11 m
Schizophrenia
Expansion of crisis intervention teams £4 – 22 m £7 – 37 m
Expansion of early intervention services £0 m £13 – 65 m
Introduction of detection services £0 m Up to £19 m
Bipolar disorder
Expansion of crisis intervention teams £2 – 10 m £3 – 16 m
Expansion of early intervention services £0 m £8 – 31 m
Introduction of detection services £0 m Up to £4 m
Dementia
Reduction in prevalence among those aged 65-74 £0.2 – 0.6 bn £0.4 – 1.2 bn
Reduction in prevalence among those aged 65-84 £0.8 – 2.4 bn £1.7 – 5.2 bn
Range depends on how many more patients are treated andhow quickly new services are introduced
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Conclusions
Mental health problems…
devastating - for individuals of all ages burdensome - for families challenging - for communities very expensive - for economies

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
MentalHealth care
MainstreamHealth care
Educationsystem
Social caresystem
Familycaregivers
Communitysupport
Criminaljustice
Housingprovision
Incomesupport
Mental health care
Sits among a complex array of support agents
Crosses multiple boundaries
Conclusions
Danger is that individual sectors may be reluctant to invest if benefits are felt elsewhere and/or much later, leading to low
overall investment
Employers
NEED FOR COORDINATED CROSS-AGENCY ACTION
WITH A VIEW TO THE LONG TERM

Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
References
Burns, Catty, Becker, Drake, Fioritti, Knapp, Lauber, Rössler, Tomov, van Busschbach, White, Wiersma, EQOLISE Group. Lancet 2007; 370 (9593):1146-1152.
Burns, Becker, Catty, Fioritti, Knapp, Lauber, Rössler, Tomov, van Busschbach, White, Wiersma, EQOLISE Group. Final Report to European Commission, Project code QLRT-2001-00683, 2006.
Centre for Economic Performance, London School of Economics, 2006
Goeree, O’Brien, Blackhouse, Agro, Goering. Canadian Journal of Psychiatry 1999; 44: 455-463
Jacob-Tacken, Koopmanschap, Meerding, Severens. Health Eocnomics 2005; 14: 435-443
Jane-Llopis & Braddick, EC Consensus Paper, 2008
Jane-Llopis & Gabilondo, EC Consensus Paper, 2008
Knapp, Prince et al. Dementia UK. Alzheimer’s Society, 2007
McCrone, Dhanasiri, Patel, Knapp, Lawton-Smith. Paying the price. The King’s Fund, 2008.
Patel. Unit costs of health & social care. University of Kent, 2006.
Patel & Knapp. Mental Health Research Review 1998; 5: 4-10.
Romeo, Knapp & Scott. British Journal of Psychiatry 2006; 188: 547
Sainsbury Centre for Mental Health. Mental health at work: the business case. 2007
Thomas & Morris. British Journal of Psychiatry 2003; 183: 514
Psychosocial Health and Work ConferenceLjubljana, 9 October 2008
Appendix A
EQOLISE outcome measures
Positive and Negative Syndrome Scale (PANSS) Global Assessment of Functioning (GAF) Hospital Anxiety and Depression Scale (HADS) Lancashire Quality of Life Profile - European Version
(LQoLP-EU) Rosenberg Self-Esteem Scale (RSE) Camberwell Assessment of Need (CAN-EU) Groningen Social Disability Schedule (GSDS) Helping Alliance Scale (HAS)


















