Psychiatric in MDR
11
INT J TUBERC LUNG DIS 8(6):749–759 © 2004 IUATLD Psychiatric issues in the management of patients with multidrug-resistant tuberculosis P. Vega,* A. Sweetland, † J. Acha, † H. Castillo, †‡ D. Guerra, † M. C. Smith Fawzi, § S. Shin †¶ * Neuropsychiatric Service, Department of Medicine, Ministry of Health, Lima, † Socios En Salud, Lima, ‡ Department of Health and Social Sciences, Universidad Peruana Cayetano Heredia, Lima, Peru; § Program in Infectious Disease and Social Change, Department of Social Medicine, Harvard Medical School, Boston, ¶ Division of Social Medicine and SUMMARY Health Inequalities, Brigham and Women’s Hospital, Boston, Massachusetts, USA INTRODUCTION: Psychiatric issues present a challenge in the treatment of patients with multidrug-resistant tuberculosis (MDR-TB). Both baseline psychiatric dis- orders and development of psychiatric complications related to anti-tuberculosis drugs and psychosocial fac- tors require aggressive management. SETTING: A community-based non-governmental health organization in Lima, Peru. OBJECTIVE: To review the literature for psychiatric com- plications associated with anti-tuberculosis medications, to describe the incidence and prevalence of depression, anxiety and psychosis among individuals receiving MDR- TB therapy, and to detail the management approach used in this cohort. METHODS: A retrospective case series was performed among the first 75 patients to receive individualized MDR- TB therapy in Lima, Peru, between 1996 and 1999. RESULTS: Baseline depression and baseline anxiety were observed in respectively 52.2% and 8.7% of this cohort. Most individuals with baseline depression experienced improvement of depressive symptoms during the course of TB therapy. The incidence of depression, anxiety and psychosis during MDR-TB treatment was 13.3%, 12.0% and 12.0%, respectively. While the majority of individu- als with depression, anxiety and psychosis required psy- chiatric pharmacotherapy, cycloserine was successfully continued in all but one case. CONCLUSION: Psychiatric comorbidities are not a contra- indication to MDR-TB therapy. Management of psychi- atric complications is possible without compromising anti-tuberculosis treatment. KEY WORDS: multidrug-resistant tuberculosis; psycho- sis; depression; anxiety; cycloserine; Peru; review MORE THAN 50 YEARS after the advent of effec- tive therapy, tuberculosis (TB) remains one of the leading causes of adult deaths in the world, dispro- portionately affecting people in poor countries. 1 Indi- viduals at highest risk for exposure and illness are thus precisely those with the least means to overcome the disease. Furthermore, drug-resistant strains are contributing increasingly to a global public health disaster. In a survey performed in 2000, multidrug- resistant TB (MDR-TB) was identified in each of the 72 countries surveyed. 2 Current estimates indicate that 273 000 new MDR-TB cases occur each year. 3 Al- though recently removed from the list of high-burden countries, 4 Peru continues to have one of the highest rates in the Americas, with 15% of reported cases, despite representing only 3% of the population. 5 By definition, MDR-TB refers to strains of Myco- bacterium tuberculosis that are resistant to at least isoniazid (INH) and rifampicin, the two most powerful anti-tuberculosis agents. Second-line anti-tuberculosis drugs, including cycloserine (CS), the fluoroquiono- lones, ethionamide/prothionamide (ETH), kanamycin/ amikacin, capreomycin and para-aminosalicylic acid, are generally weaker and more toxic than first-line agents. For this reason, prolonged therapy (18–24 months) and frequent adverse reactions are significant challenges to successful treatment of MDR-TB patients, particularly in resource-poor settings. Management of these side effects is complicated by the fact that discontinuation of the drug or treatment interruption may compromise treatment efficacy, especially in cases of high-grade drug resistance. Rather than suspending the suspected agent, which may be one of few thera- peutic resources available to treat the infection, med- ical providers are required to develop strategies to aggressively manage the symptoms through secondary medications and other biosocial interventions. While adverse effects associated with MDR-TB Correspondence to: Ms Annika Sweetland, Socios En Salud—Sucursal Perú, Avda Merino Reyna 575, Carabayllo, 06 Lima, Peru. Tel: (51) 1-612-5200. Fax: (51) 1-547-2121. e-mail: [email protected] Article submitted 22 July 2003. Final version accepted 23 November 2003.
-
Upload
arnab-chaudhuri -
Category
Documents
-
view
153 -
download
4
Transcript of Psychiatric in MDR

INT J TUBERC LUNG DIS 8(6):749–759© 2004 IUATLD
Psychiatric issues in the management of patientswith multidrug-resistant tuberculosis
P. Vega,* A. Sweetland,† J. Acha,† H. Castillo,†‡ D. Guerra,† M. C. Smith Fawzi,§ S. Shin†¶
* Neuropsychiatric Service, Department of Medicine, Ministry of Health, Lima, † Socios En Salud, Lima, ‡ Department of Health and Social Sciences, Universidad Peruana Cayetano Heredia, Lima, Peru; § Program in Infectious Disease and Social Change, Department of Social Medicine, Harvard Medical School, Boston, ¶ Division of Social Medicine and
S U M M A R Y
Health Inequalities, Brigham and Women’s Hospital, Boston, Massachusetts, USA
INTRODUCTION: Psychiatric issues present a challengein the treatment of patients with multidrug-resistanttuberculosis (MDR-TB). Both baseline psychiatric dis-orders and development of psychiatric complicationsrelated to anti-tuberculosis drugs and psychosocial fac-tors require aggressive management.SETTING: A community-based non-governmental healthorganization in Lima, Peru.OBJECTIVE: To review the literature for psychiatric com-plications associated with anti-tuberculosis medications,to describe the incidence and prevalence of depression,anxiety and psychosis among individuals receiving MDR-TB therapy, and to detail the management approach usedin this cohort.METHODS: A retrospective case series was performedamong the first 75 patients to receive individualized MDR-TB therapy in Lima, Peru, between 1996 and 1999.
RESULTS: Baseline depression and baseline anxiety wereobserved in respectively 52.2% and 8.7% of this cohort.Most individuals with baseline depression experiencedimprovement of depressive symptoms during the courseof TB therapy. The incidence of depression, anxiety andpsychosis during MDR-TB treatment was 13.3%, 12.0%and 12.0%, respectively. While the majority of individu-als with depression, anxiety and psychosis required psy-chiatric pharmacotherapy, cycloserine was successfullycontinued in all but one case.CONCLUSION: Psychiatric comorbidities are not a contra-indication to MDR-TB therapy. Management of psychi-atric complications is possible without compromisinganti-tuberculosis treatment.KEY WORDS: multidrug-resistant tuberculosis; psycho-sis; depression; anxiety; cycloserine; Peru; review
MORE THAN 50 YEARS after the advent of effec-tive therapy, tuberculosis (TB) remains one of theleading causes of adult deaths in the world, dispro-portionately affecting people in poor countries.1 Indi-viduals at highest risk for exposure and illness arethus precisely those with the least means to overcomethe disease. Furthermore, drug-resistant strains arecontributing increasingly to a global public healthdisaster. In a survey performed in 2000, multidrug-resistant TB (MDR-TB) was identified in each of the72 countries surveyed.2 Current estimates indicatethat 273000 new MDR-TB cases occur each year.3 Al-though recently removed from the list of high-burdencountries,4 Peru continues to have one of the highestrates in the Americas, with 15% of reported cases,despite representing only 3% of the population.5
By definition, MDR-TB refers to strains of Myco-bacterium tuberculosis that are resistant to at leastisoniazid (INH) and rifampicin, the two most powerful
anti-tuberculosis agents. Second-line anti-tuberculosisdrugs, including cycloserine (CS), the fluoroquiono-lones, ethionamide/prothionamide (ETH), kanamycin/amikacin, capreomycin and para-aminosalicylic acid,are generally weaker and more toxic than first-lineagents. For this reason, prolonged therapy (18–24months) and frequent adverse reactions are significantchallenges to successful treatment of MDR-TB patients,particularly in resource-poor settings. Managementof these side effects is complicated by the fact thatdiscontinuation of the drug or treatment interruptionmay compromise treatment efficacy, especially in casesof high-grade drug resistance. Rather than suspendingthe suspected agent, which may be one of few thera-peutic resources available to treat the infection, med-ical providers are required to develop strategies toaggressively manage the symptoms through secondarymedications and other biosocial interventions.
While adverse effects associated with MDR-TB
Correspondence to: Ms Annika Sweetland, Socios En Salud—Sucursal Perú, Avda Merino Reyna 575, Carabayllo, 06 Lima,Peru. Tel: (�51) 1-612-5200. Fax: (�51) 1-547-2121. e-mail: [email protected] submitted 22 July 2003. Final version accepted 23 November 2003.

750 The International Journal of Tuberculosis and Lung Disease
treatment may be managed effectively,6,7 certain sideeffects require special attention. In particular, psychi-atric complications, such as anxiety, depression, andpsychosis, can greatly impact patient quality of life, aswell as physicians’ attitudes toward MDR-TB ther-apy. Successful control of psychiatric symptoms istherefore crucial not only for favorable patient out-come, but also for patients’ overall well-being andphysicians’ comfort with managing MDR-TB ther-apy. The most commonly reported management strat-egy to control psychiatric symptoms is to remove theoffending agent.8–10 However, a few published reportsdescribe management strategies that avoid the discon-tinuation of the drug, for example lowering the doseor simultaneously administering antidepressant orantipsychotic therapy.11–13 The use of B6 supplemen-tation to prevent neurotoxicity associated with ETH,INH and CS has also been advocated. Similar protec-tive effects may be observed with psychiatric symp-toms induced by these medications.10,14–17
Psychiatric complications have been associatedwith anti-tuberculosis therapy since the 1950s.18,19
Although significant psychiatric symptomatology hasbeen most commonly associated with CS and INH,other drugs implicated at the case report level includeETH, ethambutol (EMB) and the fluoroquinolones.Severe psychiatric manifestations—including halluci-nations, anxiety, depression, euphoria, behavioral dis-orders, and suicidal ideation and/or attempts—havebeen reported to occur in 9.7–50% of individualsreceiving CS.14,19–27 CS-associated neurotoxicity islikely due to diminished central nervous system(CNS) production of �-aminobutyric acid (GABA)caused by inhibition of glutamic decarboxylase andfacilitated by effective penetration of the blood-brainbarrier.28 In the majority of these cases, the drug wasdiscontinued, with rapid recovery of mental status andno recurring symptoms. Psychiatric symptoms appearmost likely to present within the first 3 months oftreatment.22,24,26,29 Increased risk of CNS toxicity maybe associated with supratherapeutic levels of CS,30
concomitant use of ETH,31 INH,31 or fluoroquino-lones,32 and ethanol ingestion.27
Less commonly, INH has been associated withneuropsychiatric side effects, including depression, irri-tability, obsessive-compulsive neurosis, and attemptedsuicide.8–10,33–36 In the Boston Collaborative DrugSurveillance Program performed in 1974, more than35% of adverse effects associated with INH were psy-chiatric in nature, with an incidence of 1.9%.37 Simi-larly, in Peru, severe psychiatric syndromes associatedwith INH occurred in approximately 1.0% of tuber-culosis cases between 1991 and 1999.38 Pallone,Goldman and Fuller performed a review of the litera-ture on INH-induced psychosis in 1993.39 They foundthat the most common psychiatric symptoms associ-ated with INH were delusions, generally presentingafter approximately 4 weeks of taking the drug, and
among patients of an average age of 35 years (range17–53). They summarize risk factors as receiving adose above 5 mg/kg; age 50 years or older; co-morbid disease including diabetes mellitus, hepaticinsufficiency, alcoholism, and hyperthyroidism; andpast psychiatric history. Several mechanisms havebeen proposed to account for INH-associated toxic-ity. INH may act as an monamine oxidase (MAO)inhibitor; alternatively, psychiatric effects may becaused by INH-induced pyridoxine deficiency, withsubsequently diminished production of norepineph-rine, serotonin, dopamine, and GABA.39 Furtherreview has uncovered several more case reports de-tailing psychotoxic reactions to INH with similarobservations.13,40–43
Several case reports associate the use of ETH withoccurrence of depression, anxiety, psychosis, and sui-cide.9,14,44–46 The mechanism for INH and ETH neuro-toxicity is likely the same.37 EMB may also be associ-ated with mania,47 confusion,15,31 and psychosis,48
although the mechanism for this effect is unknown.Finally, the fluoroquinolones have been implicated inrare occurrences of psychosis,49,50 depression,51 delir-ium,52,53 and nightmares.54 A large-scale retrospectivestudy by Hollweg et al. reported psychiatric distur-bance in 0.7% of 4189 individuals treated with eitherofloxacin or ciprofloxacin.55 In this study, while el-derly individuals were more likely to experience delir-ium or paranoia, younger individuals had greaterrates of depressive and manic syndromes. Underly-ing hepatic or renal dysfunction, concomitant anti-biotics or immunosuppressants, and baseline psychi-atric disorders or psychosocial stressors, were identifiedas risk factors for quinolone-associated psychiatricdisturbance.
In addition to drug toxicity, psychosocial factorscontribute to psychiatric complications during MDR-TB therapy, and consequently patients’ adherence tothese regimens. Two early reports on sanatorium carediscuss several emotional aspects associated with TB,including depression, anxiety, and suicidal ideation.56,57
Considering that these reports pre-date the develop-ment of effective antibiotics for the treatment of TB,it is apparent that psychiatric complications occureven in the absence of drug therapy. Some of the psy-chosocial issues that are often prominent concerns ofindividuals with MDR-TB include: social stigma anddiscrimination; fear and guilt associated with infec-tious risk; the socio-economic and psychological bur-dens of living with a chronic, life-threatening illness;increased dependence on others; multiple treatmentfailures and being told in health centers that no fur-ther therapy was available; losing family members tothe disease; and concomitant poverty. The impact ofsocial stigma has been examined with regard to otherinfectious diseases, such as the human immunodefi-ciency virus and the acquired immune-deficiency syn-drome (HIV/AIDS), the impact of which include

Psychiatric issues in MDR-TB therapy 751
depression, low self esteem, and shame.58–61 Fear ofinfection is one of the factors contributing to socialstigma, which may produce social isolation, dimin-ished marriage prospects, limited social support, andresult therefore in the denial of diagnosis and conse-quent rejection of treatment.62,63 Despite the fact thatTB infection is not necessarily associated with specific‘risk behaviors’, TB patients are still generally heldresponsible for their illness and blamed for not takingbetter care of themselves.63 Further, poverty alone hasbeen demonstrated to have a clear association withincreased risk for mental illness.64 Several authorshave described how these psychosocial factors com-plicate adherence to drug regimens, and emphasizethe importance of attention to mental health needs toensure positive treatment outcomes.62,63,65,66 Adher-ence is especially important in the case of MDR-TB,as this is often a patient’s last treatment option; fail-ure to complete this treatment leads to a high rate offatality, in addition to ongoing transmission of highlydrug-resistant strains.
Despite such challenges, a community-based initia-tive in Lima, Peru, has demonstrated successful out-comes in treating MDR-TB patients,67 in part throughcomprehensive management of psychiatric side effectsand psychosocial factors.63 One of the fundamentalcomponents of this program has been the aggressivemanagement of adverse reactions using protocols andcommunity-based outreach to minimize the need fortreatment interruption or discontinuation of anti-tuberculosis drugs.68,69 Here, we describe the inci-dence, characteristics, and management of psychosis,depression, and anxiety occurring among patientsreceiving individualized treatment for MDR-TB inLima, Peru.
METHODS
Study populationAll patients had documented MDR-TB and wereenrolled in treatment between 1 August 1996 and 31January 1999 through collaborative effort betweentwo non-governmental organizations (Partners InHealth and Socios En Salud—Sucursal Perú) and thePeruvian Ministry of Health’s National TuberculosisProgram (NTP). The catchment area included threedistricts of Northern Lima (Carabayllo, Comas andIndependencia), a shanty town hosting roughly 762000people in 1997 with high rates of poverty, violence,unemployment, and mental illness.70–73 In addition,through active case finding, this area was identified asa ‘hot spot’ for the disease in Peru, with estimated TBrates higher than the national incidence.74
Treatment protocolAll patients were referred by the NTP for suspicion ofMDR-TB based on history of treatment failure orhousehold contact with a known MDR-TB patient.
Comorbidities, including psychiatric conditions, werenot a contraindication to treatment. Written informedconsent was obtained from all patients and one familymember prior to initiating therapy. Multidrug resis-tance was confirmed by conventional or BACTECmethods performed by the Massachusetts State Lab-oratory Institute on sputum specimens.74 Individual-ized therapy was based on each patient’s resistancepattern. Of note, individuals with resistance to INHonly at low concentrations received high-dose INH (900mg twice a week) as part of their regimens. Pyridoxine(150–300 mg/day) was administered with MDR-TBregimens. All patients participated in an unstructuredclinical interview with a psychiatrist to screen for base-line psychiatric disorders prior to initiation of indi-vidualized therapy. Patients received treatment underthe auspices of the Peruvian NTP: community-baseddirectly observed therapy delivered in health centersand in patients’ houses by community health work-ers.75,76 All treatment was provided to patients free ofcharge.
Patients were evaluated at least once a month byan NTP physician trained in the management ofMDR-TB. These evaluations included screening forpsychosis, depression, and anxiety. Patients were addi-tionally assessed for any side effects identified byhealth care workers. Patients with psychiatric symp-toms were referred to a psychiatrist at the physician’sdiscretion. The psychiatrist used clinical criteria basedon DSM-IV77 to diagnose psychiatric syndromes. Ingeneral, symptoms were managed according to proto-cols that were developed by the physicians trained atSocios En Salud in the management of MDR-TB (seeAppendices 1 and 2). Anti-depressants, anxiolytics,anti-psychotics, and psychotherapy were prescribedby both primary MDR-TB physicians and psychia-trists, and provided free of charge.
Study design and data collectionA case series with a retrospective chart review wasconducted among all patients who had initiated indi-vidualized treatment between 1 August 1996 and 31January 1999. All patients had completed treatmentat the time of chart review. The follow-up period forall patients who were still alive was at least 18months after completion of treatment. All charts werereviewed by a physician trained in the managementof MDR-TB, then all cases with suspected new onsetof psychiatric disorders were further reviewed by thetreating psychiatrist. The case definition of psychosiswas based on DSM-IV criteria by a physician.77 Cate-gorization of depression was based on DSM-IV criteriaby a psychiatrist, and included the following diag-noses: major depressive disorder, dysthymia, adjust-ment disorder with depressed mood, and substance-induced mood disorder with depressive features.The diagnosis of anxiety was also based on DSM-IVcriteria for generalized anxiety disorder or substance-

752 The International Journal of Tuberculosis and Lung Disease
induced anxiety disorder by a psychiatrist. Other vari-ables extracted from the chart review for all patientsincluded age, sex, drugs in the individualized regimen,number of previous treatment regimens, treatmentoutcome, baseline psychiatric illness using DSM-IVcriteria according to a psychiatrist, history of alcoholor drug abuse, hypothyroidism (before or duringtreatment), HIV, diabetes mellitus, and malnutrition.The charts of all cases of psychiatric disorders werereviewed in more detail with respect to timing andduration of presentation of symptoms, clinical man-agement, and treatment outcome.
Statistical analysisThe following risk factors were analyzed for associa-tion with incidence of depression, psychosis or anxi-ety: sex; age; baseline depression; education level;unemployment; marital status; presence of dependentchildren; presence of TB household contacts; pres-ence of household contacts who died of TB; hypothy-roidism; presence of comorbidities (i.e., diabetes, HIV,malnutrition, history of alcoholism or drug abuse);history of institutionalization (i.e., incarceration orextended hospitalization) or homelessness; receipt ofmedications associated in the literature with psychiat-ric side effects (i.e., CS, INH, EMB, ETH, fluoroqui-nolones); and CS dose. Multivariable analysis foroccurrence of each side effect was also performedusing a multiple regression model including all vari-ables associated with a P value �0.05 or an odds ratio(OR) �2.0 on univariate analysis.
All data were entered in Microsoft Excel 97(Microsoft Corporation, Seattle, WA, USA); all statis-tical analysis was performed using SAS, version 8.2(SAS Institute, Cary, NC, USA). Reported P valueswere based on two-sided Fishers exact tests, orfor continuous variables, t-tests or, if non-parametric,the Wilcoxon test. For binary variables, ORs with95% confidence intervals (95%CIs) were alsocalculated.
RESULTS
Baseline characteristics, incidence of psychiatric complications, and treatment outcomesBetween August 1996 and January 1999, 75 patientsinitiated treatment. Charts were available and reviewedfor all cases. The baseline prevalence, as well as inci-dence during treatment of psychosis, depression andanxiety, are summarized in Table 1. Of note, roughlyhalf of the cohort had a baseline diagnosis of depression,including three individuals who also had a co-existinganxiety disorder. None had baseline psychosis. Dur-ing the course of MDR-TB therapy, 10 (13.3%)patients developed depression, nine (12.0%) devel-oped anxiety disorders, and nine (12%) experiencedpsychosis. While psychosis tended to occur earlier inMDR-TB treatment (mean 3.6 months, range 1–8),
the onset of depression and anxiety was more vari-able. For both depression and anxiety, the mean timeof presentation was 7.3 months, with a range of 1–17and 2–16 months, respectively.
Table 2 summarizes the demographic and clinicalcharacteristics of this cohort and has been described inmore detail elsewhere.67 MDR-TB regimens includedCS in all but one case, with a median daily dose of1000 mg. Twenty-five patients (33.3%) received highdoses of INH, 52 (69.3%) received ETH, 11 (14.7%)received EMB, and 72 (96.%) received a fluoroquino-lone. While the occurrence of psychiatric complica-tions during MDR-TB therapy was not significantlyassociated with adverse treatment outcome, therewas a trend toward increased risk of default amongindividuals who developed psychosis (OR � 6.0,95%CI 0.9–42.3).
Risk factors and managementof psychiatric complications
PsychosisAmong the nine patients (12%) who developed psy-chosis during treatment, younger age (average 24.1 vs.29.7 years among those with and those without psy-chosis, P � 0.008) was identified as a risk factor. Fur-thermore, none of the individuals who developed psy-chosis were married vs. 36.4% among those who didnot de-velop psychosis (P � 0.05). In a multivariableanalysis, including female sex, age, baseline depres-sion, unmarried status, number of dependent children,and presence of an MDR-TB household contact, novariable was found to be significantly associated withpsychosis. In three (33.3%) cases CS was suspendedtemporarily, in two (22.2%) the CS dose was de-creased, and in one (11.1%) the drug was suspendedthen resumed at a lower dose (Table 3). It was nevernecessary to discontinue CS indefinitely. No changes inother TB drugs were required. Only one (11.1%)patient was hospitalized due to psychosis, while therest were managed through close monitoring by com-munity health promoters, nurses, and doctors in thepatients’ homes. All but one individual received anti-psychotic drug therapy. Psychotic episodes recurredin two (22.2%) individuals, but were effectively
Table 1 Prevalence and incidence of psychosis, depression and anxiety among MDR-TB patients
Prevalenceprior toMDR-TBtherapy(n � 69)
n (%)
Persistentsymptoms
among thosewith baseline
diagnosisn (%)
Incidenceduring
MDR-TB therapy(n � 75)
n (%)
Prevalence during
MDR-TBtherapyn (%)
Psychosis 0 (0) 0 (0) 9 (12.0) 9 (12.0)Depression 36 (52.2) 12/36 (33.3) 10 (13.3) 22 (29.3)Anxiety 6 (8.7) 3/6 (50.0) 9 (12.0) 12 (16.0)
MDR-TB � multidrug-resistant tuberculosis (defined as resistance to at leastisoniazid and rifampicin).

Psychiatric issues in MDR-TB therapy 753
Table 2 Baseline characteristics among 75 patients receiving individualized MDR-TB therapy
Characteristic n (%) Median (range)
Age, years 26.8 (11.8–65.1)
SexMale 37 (49.3)Female 38 (50.7)
Education level (n � 53)Completed elementary school or less 7 (13.2)Some high school or more 46 (86.8)
Household size (n � 70) 7 (2–20)
Marital statusMarried/living with partner 24 (34)Unmarried (single, divorced, widowed, separated) 47 (66)
OccupationNot working 12 (16.0)Student 19 (25.3)Homemaker 14 (18.7)Worker, aside from professional 30 (40.0)Professional 0 (0.0)
Number of dependent children 0 (0–7)TB and MDR-TB household contacts 58 (77.3)Household contacts who died of TB 28 (37.3)Number of previous treatment regimens 3.0 (0–8)Number of drugs to which patient is resistant 6.0 (2–12)Comorbidity* 23 (30.7)Hypothyroidism before or during ITR 11 (14.7)Prior institutionalization or homelessness 9 (12.0)Maximum cycloserine dose (mg) 1000 (750–1000)Cycloserine 74 (98.7)Isoniazid (high dose) 25 (33.3)Ethionamide 52 (69.3)Ethambutol 12 (16.0)Fluoroquinolones 72 (96.0)
* Chronic disease included diabetes mellitus (1), HIV (1), malnutrition (15), and history of alcoholism or drug use (7).MDR-TB � multidrug-resistant tuberculosis; TB � tuberculosis; ITR � individualized treatment regimen; HIV � humanimmunodeficiency virus.
Table 3 Characteristics and management of psychiatric symptoms (n � 75)
Management
New psychosis(n � 9) n (%)
New depression(n � 10)
n (%)
New anxiety(n � 9)n (%)
Baselinedepression with
persistentsymptomatology
(n � 12)n (%)
Baseline anxiety withpersistent
symptomatology(n � 3)n (%)
Reduced dose of cycloserine 3 (33.3) 1 (10.0) 4 (44.4) 10 (8.3) 0 (0)Temporary suspension of cycloserine 4 (44.4) 0 (0) 0 (0) 0 (0) 0 (0)Terminated dose of cycloserine 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)Required psychiatric medications 9 (88.9) 8 (80) 8 (88.9) 6 (50) 3 (100)Persistent psychiatric symptoms
throughout MDR-TB treatmentrequiring psychiatric medications 3 (33.3) 1 (10.0) 3 (33.3) 2 (16.7) 0 (0)
Required hospitalization due topsychiatric symptoms 1 (11.1) 0 (0) 0 (0) 0 (0) 0 (0)
MDR-TB � multidrug-resistant tuberculosis.
managed in both cases. While patients receiving anti-psychotic medications at the conclusion of therapygenerally continued their use for an additional 30–45days, in only one (11.1%) case was it necessary for thepatient to continue taking anti-psychotic medicationsbeyond this window. Psychosis resolved in eight
(88.9%) of the cases, with a median duration of psy-chotic symptoms of 4 weeks (range 0.71–28). Two(22.2%) patients who experienced psychosis aban-doned treatment, one (11.1%) of whom was psychoticat the time of default. Of note, three (33.3%) of thesecases occurred among sisters in one family.

754 The International Journal of Tuberculosis and Lung Disease
DepressionAmong the 36 (52.2%) patients with baseline depres-sion, two thirds (66.7%) did not require psychiatricattention or medications for depressive symptomsduring therapy due to mild symptomatology or remis-sion. Ten (13.3%) patients without baseline symp-tomatology experienced a new onset of depressionduring TB therapy; no significantly associated riskfactor was identified on univariate analysis. In amultivariable analysis including number of depen-dent children, hypothyroidism, and presence of a TBhousehold contact, no variable was identified to besignificantly associated with depression. The dose ofCS was lowered in one (10.0%) new case for theduration of treatment; no other modification of TBtherapy was made for other patients presenting withdepression during treatment. Anti-depressive medica-tions were indicated in 80% of the new cases, althoughsymptoms were generally effectively managed and theywere not needed throughout treatment. Finally, nopatients in this cohort were hospitalized for depression.
AnxietyOf the six (8.7%) patients with baseline anxiety, half(50.0%) had persistent symptoms requiring psychiatricintervention, and one (16.7%) experienced a manicepisode. Furthermore, nine (12%) patients had a newonset of anxiety during treatment. Risk factors signif-icantly associated with onset of anxiety during MDR-TB treatment were having more dependent children(P � 0.007) and a higher average dose of CS (972 mgvs. 884 mg among those with and those without anx-iety, P � 0.04). Eight of nine patients (88.9%) werereceiving CS at the maximum dose of 1000 mg. Themultivariable analysis included the following factors:age, married status, number of dependent children,CS dose, TB household contact, and lack of chronicdisease. Among these variables, only higher dose of CS(P � 0.01) and greater number of dependents (P �0.002) were significantly associated with occurrenceof anxiety. In four (44.4%) cases, the dose of CS waslowered for the duration of treatment; no other changesin anti-tuberculosis therapy were made. While anxi-olytic medications were necessary in eight (88.9%)of the nine cases, only three (33.3%) required med-ications for the duration of treatment. There were nohospitalizations due to anxiety.
DISCUSSION
The baseline prevalence of depression observed in ourcohort was greater than the prevalence in the generalpopulation of Lima, Peru (52.2% vs. 6.7%).71 On theother hand, baseline rates of anxiety and psychosiswere comparable to those of the general populationof Lima.71 High rates of depression and anxietyamong tuberculosis patients have been reported else-where,78 and are likely related to social stigma, inad-
equate social support, and the physiologic impactof chronic disease.62,63,66,79 Interestingly, two thirds ofthose with baseline depression actually experiencedan improvement in their depressive symptoms duringtreatment, presumably as they recovered from tuber-culosis and were able to resume important social rolesin their family and community.
Development of depression during treatment, ob-served in 13.3% of our cohort, could be influenced bysimilar psychosocial forces, as well as drug-relatedfactors. However, a clearer association can be observedbetween anti-tuberculosis drugs and both anxiety andpsychosis: anxiety occurred more frequently amongthose receiving higher doses of CS, and psychosisresponded to temporary suspension of CS and/orreduction of CS dose. Nevertheless, the role of psy-chosocial factors should not be underestimated. Forinstance, having more dependent children was a riskfactor for anxiety, likely reflecting the stress of fulfill-ing a caregiving role while sick. Indeed, the combinedinfluence of polypharmacy and psychosocial factorshighlights the need for integrated responses to psychi-atric complications, including both pharmacologicaland psychosocial components.
Three main strategies have been used to managepsychiatric complications during MDR-TB therapy inthis program. First, community health workers havebeen crucial in the identification, referral and man-agement of psychiatric disorders. All community healthworkers are trained to recognize early manifestationsof adverse reactions, including psychiatric symptoms.Importantly, they provide direct supervision of psy-chiatric medications, in addition to emotional sup-port and counselling, for patients and family members.
The second strategy has been the use of psychiatricmedications in the majority of incident cases, oftenmanaged by a psychiatrist. For psychosis, low-dose ris-peridone has replaced haloperidol as the favored ther-apy, due to fewer extrapyramidal symptoms associ-ated with long-term use. For depression, serotonin-uptake inhibitors, such as sertraline and fluoxetine, arewell tolerated and effective, with minimal pharmacolog-ical interactions. Among anxiolytics, lorazepam offersthe advantage of a short half-life, while clonazepammay be appropriate in individuals with concomitantpsychotic or depressive symptoms.31 Adequate psy-chopharmacotherapy has allowed CS to be successfullycontinued in all but one case, in which CS was sus-pended only because an adequate regimen remained.
Finally, many patients are referred to a psycho-social support group comprised of patients in treat-ment and cured individuals. This methodology,described elsewhere,63 has been effective in combat-ing the psychosocial impact of the disease, includingmarginalization and stigma, hopelessness and griev-ing, as well as contemplation of suicide or treatmentdefault.
There are several limitations to this study. First, the

Psychiatric issues in MDR-TB therapy 755
small sample size limits the analysis of risk factorsand effect of psychiatric complications on treatmentoutcome. A larger cohort will likely be necessary toidentify risk factors associated with development ofdepression and psychosis. Moreover, given the retro-spective nature of this study, the incidence of psychi-atric complications could be underestimated becauseof lack of reporting or appropriate diagnosis.
CONCLUSIONS
Baseline prevalence of depression, anxiety, and psy-chosis in our cohort was 52.5%, 8.7% and 0%,respectively. Nonetheless, the presence of a baselinepsychiatric disorder was not a contraindication toMDR-TB therapy nor to the use of CS. Furthermore,individuals with initial depression and/or anxiety oftenexperienced an improvement in their symptoms dur-ing the course of MDR-TB treatment. Depression,anxiety and psychosis each occurred in approxi-mately 12–13% of our cohort during treatment.Aggressive use of psychiatric medications (in particu-lar for psychosis), in addition to psychosocial sup-port, has permitted successful resolution of symp-toms, usually without the need for hospitalization.Compared with other MDR-TB cohorts, our cohortexperienced higher or comparable rates of psychiatriccomplications, and yet discontinuation of medications,in particular CS, occurred less frequently.12,80–82 Thus,psychiatric disorders among patients with MDR-TB canbe successfully managed without endangering effectiveMDR-TB therapy.
AcknowledgementsThe authors wish to thank the Bill & Melinda Gates Foundation,as well as Thomas White, for their generous support. In addition,we would like to thank the Peruvian Ministry of Health for theircollaboration, and the community health workers, whose valiantefforts made this work possible. Finally, we wish to thank ourpatients for the inspiration that they have given us to continue pro-viding high quality TB care for patients living in poverty.
References1 Benatar S R. Prospects for global health: lessons from tubercu-
losis. Thorax 1995; 50: 487–489.2 Espinal M A, Simonsen L, Laszlo A, et al. for the World Health
Organization/International Union Against Tuberculosis andLung Disease Global Working Group on Anti-tuberculosisDrug Resistance Surveillance. Anti-tuberculosis drug resistancein the world. Report No. 2. WHO/TB/2000.278. Geneva, Swit-zerland: WHO, 2000. http://www.who.int/gtb/publications/drugresistance/ Accessed March 2004.
3 Dye C, Espinal M A, Watt C J, Mbiaga C, Williams B. World-wide incidence of multidrug-resistant tuberculosis. J Infect Dis2002; 185: 1197–1202.
4 World Health Organization. WHO Report 2002. Globaltuberculosis control: surveillance, planning, and financing.WHO/CDS/TB/2002.295. Geneva, Switzerland: WHO, 2002.
5 World Health Organization. Health, a key to prosperity: suc-cessful stories in developing countries. WHO/CDS/2000.4.Geneva, Switzerland: WHO, 2002.
6 Shin S S, Hyson A M, Castañeda C, et al. Peripheral neuro-pathy associated with treatment for multidrug-resistant tuber-culosis. Int J Tuberc Lung Dis 2003; 7: 347–353.
7 Furin J J, Mitnick C D, Shin S S, et al. Occurrence of seriousadverse effects in patients receiving community-based therapyfor multidrug-resistant tuberculosis. Int J Tuberc Lung Dis2001; 5: 648–655.
8 Weidorn W S, Ervin F. Schizophrenic-like psychotic reactionswith administration of isoniazid. Arch Neurol Psychiat 1954;72: 321–324.
9 Lees A W. Ethionamide and isoniazid in previously untreatedcases of pulmonary tuberculosis. Dis Chest 1964; 45: 247–250.
10 Reilly D K. Isoniazid-related CNS toxicity. Drug Ther 1979; 9:187–188.
11 Aceto J N, Covert D F. Observations on cycloserine-isoniazidin pulmonary tuberculosis. Antibiot Med Clin Ther 1960; 7:705–712.
12 Pasechnikov A D, Malinovskaya T Z, Kostornoy O S. Sideeffects in multiple drug resistant TB treatment in TomskOblast. Moscow, Russian Federation: 17th Russian Congresson Tuberculosis, 2003.
13 Duggal H S, Nizamie S H. Novel antipsychotic drugs and INH-related psychosis. Aust N Z J Psychiatry 2000; 34: 343–344.
14 Johnson D A. Drug-induced psychiatric disorders. Drugs1981; 22: 57–69.
15 Patel A M, McKeon J. Avoidance and management of adversereactions to antituberculosis drugs. Drug Safety 1995; 12: 1–25.
16 Ministerio de Salud 1995. Actualización de la doctrina, nor-mas y procedimientos para el control de la tuberculosis en elPerú. Rev Soc Per Tis Neu E T 1996; 40: 19–41.
17 Ministerio de Salud. Actualización de la doctrina, normas yprocedimientos para el control de la tuberculosis en el Perú:2001. Lima, Peru: Ministerio de Salud del Peru, 2001: pp 71–77.
18 Weidorn W S, Ervin F. Schizophrenic-like psychotic reactionwith administration of isoniazid. Arch Neurol Psychiat 1954;72: 321.
19 Lewis W C, Calden G, Thurslan J R, Gibson W E. Psychiatricand neurological reaction to cycloserine in the treatment oftuberculosis. Dis Chest 1957; 32: 172–177.
20 Riska N. Tolerance to cycloserine. Scand J Respir Dis 1970; 71(Suppl): 209–216.
21 Stephanopoulos C, Zoumbouloglou H. Clinical tolerance tocycloserine. Scand J Respir Dis 1970; 71 (Suppl): 235–238.
22 Dissmann E. Experience with cycloserine. Scand J Respir Dis1970; 71 (Suppl): 239–243.
23 Bethlem N. Results of treatment of pulmonary tuberculosiswith cycloserine in association with other drugs. Scand JRespir Dis 1970; 71 (Suppl): 244–249.
24 Helmy B. Side effects of cycloserine. Scand J Respir Dis 1970;71 (Suppl): 220–225.
25 Pasargiklian M, Biondi L. Neurologic and behavioral reactionsof tuberculosis patients treated with cycloserine. Scand J RespirDis 1970; 71 (Suppl): 201–208.
26 Leston J M, Rey J C, Gonzalez Montaner L J, Grondona A,Zavalla P N. Psychosomatic reactions to cycloserine in thetreatment of tuberculosis. Scand J Respir Dis 1970; 71 (Suppl):231–234.
27 Nariman S. Adverse reactions to drugs used in the treatment oftuberculosis. Adverse Drug React Acute Poisoning Rev 1988;4: 207–227.
28 Berning S E, Peloquin C A. Antimycobacterial agents: Cyclo-serine. In: Yu V L, Merigan J R, Barriere S L, eds. Antimicrobialtherapy and vaccines. Baltimore, MD: Williams & Wilkins,1999: pp 638–642.
29 Snavely S R, Hodges G R. The neurotoxicity of antibacterialagents. Ann Intern Med 1984; 101: 92–104.

756 The International Journal of Tuberculosis and Lung Disease
30 Sweetman S. Martindale—The complete drug reference. 33rded. London, UK: Pharmaceutical Press, 2002.
31 Medical Economics Staff, PDR Staff, eds. Physicians’ Desk Refer-ence 2003. 57th ed. Oradell, NJ: Medical Economics Co, 2003.
32 Yew W W, Wong C F, Wong P C, Lee J, Chau C H. Adverseneurological reactions in patients with multidrug-resistant pul-monary tuberculosis after coadministration of cycloserine andofloxacin. Clin Infect Dis 1993; 17: 289–290.
33 Goldman A L, Braman S S. Isoniazid: a review with emphasison adverse effects. Chest 1972; 62: 71–77.
34 Reilly D K. Isoniazid-related CNS toxicity. Drug therapy 1979;9: 187–188.
35 Bhatia M S. Isonizid-induced obsessive compulsive neurosis. JClin Psych 1990; 51: 387.
36 Madan A, Jain N K, Sharma T N, Sharma D K, Madan R. At-tempted suicide following treatment with isoniazid. Tubercle1989; 70: 147–149.
37 Holdiness M R. Neurological manifestations and toxicities ofthe antituberculosis drugs. Med Toxicol 1987; 2: 33–51.
38 Bonilla C, Portocarrero P G, Suárez P G, Molero D. Reac-ciones adversas a fármacos antituberculosos (RAFA) en trata-mientos directamente observados (DOTS). Peru 1991–1999.Tuberculosis en el Perú: Informe 1999. Lima, Peru: Ministeriode Salud del Perú, 2000: pp 99–106.
39 Pallone K A, Goldman M P, Fuller M A. Isoniazid-associatedpsychoses: case report and review of the literature. Ann Phar-macother 1993; 27: 167–169.
40 Ibrahim Z Y, Menke J J. Comment: Isoniazid-induced psycho-sis. Ann Pharmacother 1994; 28: 1311.
41 Gnam W, Flint A, Goldbloom D. Isoniazid-induced hallucino-sis: response to pyridoxine. Psychosomatics 1993; 34: 537–539.
42 Alao A O, Yolles J C. Isoniazid-induced psychosis. Ann Phar-macother 1998; 32: 889–891.
43 Bourgeois J A, Zelenko M, Waraich B S. Psychotic disorderassociated with isoniazid. Mil Med 1996; 161: 707.
44 Sharma G S, Gupta P K, Jain N K, Shanker A, Nanawati V.Toxic psychosis to isoniazid and ethionamide in a patient withpulmonary tuberculosis. Tubercle 1979; 60: 171–172.
45 Lansdown F S, Beran M, Litwak T. Psychotoxic reaction duringethionamide therapy. Am Rev Respir Dis 1967; 95: 1053–1055.
46 Narang R K. Acute psychotic reaction probably caused byethionamide. Tubercle 1972; 53: 137–138.
47 Pickles R W, Spelman D W. Suspected ethambutol-inducedmania. Med J Aust 1996; 164: 445–446.
48 Hsu C W, Chu K A, Lu T, Lai R S, Lu J Y. Ethambutol-inducedpsychosis: a case report [abstract]. Zhonghua Yi Xue Za Zhi1999; 62: 724–727.
49 Mulhall J P, Bergmann L S. Ciprofloxacin-induced acute psy-chosis. Urology 1995; 46: 102–103.
50 Zaudig M, von Bose M, Weber M M, Bremer D, Zieglgans-berger W. Psychotoxic effects of ofloxacin. Pharmacopsychia-try 1989; 22: 11–15.
51 Feinberg S S. Fluoroquinolone-induced depression. Am J Psy-chiatry 1995; 152: 954–955.
52 Jay G T, Fitzgerald J M. Ciprofloxacin-induced delirium. AnnPharmacother 1997; 31: 252.
53 Fennig S, Mauas L. Ofloxacin-induced delirium. J Clin Psychi-atry 1992; 53: 137–138.
54 Dey S K. Nightmare due to ciprofloxacin in young patients.Indian Pediatr 1995; 32: 918–920.
55 Hollweg M, Kapfhammer H P, Krupinski M, Moller H J. Psy-chopathological syndromes in treatment with gyrase inhibitors[abstract]. Nervenarzt 1997; 68: 38–47.
56 Todd G S, Wittkower E. The psychological aspects of sanato-rium management. Lancet 1948; 254: 49–53.
57 Ludwig A O. Emotional factors in tuberculosis. Public HealthRep 1948; 63: 883–888.
58 Lang N G. Stigma, self-esteem and depression: psychosocialresponses to risk of AIDS. Hum Org 1991; 51: 66–72.
59 Ingram D, Hutchinson S A. HIV-Positive women and stigma.Health Care Women Int 1999; 20: 93–103.
60 Fife B L, Wright E. The dimensionality of stigma: a comparisonof its impact on the self of persons with HIV/AIDS and cancer.J Health Soc Behav 2000; 41: 50–67.
61 Lawless S, Kippax S, Crawford J. Dirty, diseased, and unde-serving: the positioning of HIV positive women. Soc Sci Med1996; 43: 1371–1377.
62 Liefooghe R, Michiels N, Habib S, Moran M B, De Muynck A.Perception and social consequences of tuberculosis: a focusgroup study of tuberculosis patients in Sialkot, Pakistan. SocSci Med 1995; 41: 1685–1692.
63 Sweetland A, Acha D, Guerra D. Enhancing adherence: therole of group psychotherapy in the treatment of MDR-TB inurban Peru. In: Cohen A, Kleinman A, Saraceno B, eds. WorldMental Health Casebook: Social and Mental Health Inter-ventions in Low-Income Countries. New York, NY: KluwerAcademic/Plenum Press, 2002: pp 51–79.
64 Patel V, Kleinman A. Poverty and common mental disordersin developing countries. Bull World Health Organ 2003; 81:609–615.
65 Fullilove M T, Young R, Panzer P G, Muskin P. Psychosocial is-sues in the management of patients with tuberculosis. J LawMed Ethics 1993; 21: 324–331.
66 Barnhoorn F, Adriaanse H. In search of factors responsible fornoncompliance among tuberculosis patients in Wardha Dis-trict, India. Soc Sci Med 1992; 34: 291–306.
67 Mitnick C, Bayona J, Palacios E, et al. Community-based therapyfor multidrug-resistant tuberculosis in Lima, Peru. N Engl JMed 2003; 348: 119–128.
68 Partners In Health, Harvard Medical School, Bill and MelindaGates Foundation. A DOTS-Plus Handbook: Guide to theCommunity-Based Treatment of MDR-TB. Boston, MA: Part-ners In Health, 2002.
69 Partners In Health/Program in Infectious Disease and SocialChange, Harvard Medical School. The PIH Guide to the Med-ical Management of Multidrug-Resistant Tuberculosis. Bos-ton, MA: PIH/PIDSC, 2003.
70 Instituto Nacional de Estadística e Informática. Proyeccionesde población por años calendario según departamentos, pro-vincias, y distritos (Periodo, 1990–2002). Lima, Peru: InstitutoNacional de Estadística e Informática, 2001. Boletín EspecialNo. 16: p. 63.
71 Saavedra J E, Instituto Especializado de Salud Mental “Hono-rio Delgado—Hideyo Noguchi.” Estudio epidemiológico met-ropolitano en salud mental 2002. Anales de Salud Mental2002; 18: 1–197.
72 Minobe K, Perales A, Sogi C, Warthon D, Llanos R, Sato T.Prevalencia de vida de trastornos mentales en Independencia.Anales de Salud Mental 1990; 6: 9–20.
73 Instituto Nacional de Salud Mental “Honorio Delgado—HideyoNoguchi.” Prevalencia de vida de trastornos mentales en Indepen-dencia (Lima, Peru). Anales de Salud Mental 1985; 1: 206–222.
74 Becerra M C, Freeman J, Bayona J, et al. Using treatment failureunder effective directly observed short-course chemotherapyprograms to identify patients with multidrug-resistant tubercu-losis. Int J Tuberc Lung Dis 2000; 4: 108–114.
75 Farmer P E, Bayona J, Shin S, et al. Preliminary results of com-munity-based MDR-TB treatment in Lima, Peru. Int J TubercLung Dis 1998; 2 (Suppl 2): S371.
76 Farmer P E, Walton D A, Becerra M C. International tubercu-losis control in the 21st century. In: Friedman L N, ed. Tuber-culosis: current concepts and treatment. 2nd ed. Boca Raton,FL: CRC Press, 2000: pp 475–496.
77 American Psychiatric Association. Diagnostic and StatisticalManual of Mental Disorders. 4th ed. Washington, DC: Amer-ican Psychiatric Association, 1994.

Psychiatric issues in MDR-TB therapy 757
78 Aghanwa H S, Erhabor G E. Demographic/socioeconomic fac-tors in mental disorders associated with tuberculosis in South-west Nigeria. J Psychosom Res 1998; 45; 353–360.
79 Aydin I O, Ulu ahin A. Depression, anxiety comorbidity, anddisability in tuberculosis and chronic obstructive pulmonarydisease patients: applicability of GHQ-12. Gen Hosp Psychia-try 2001; 23: 77–83.
80 Goble M, Iseman M D, Madsen L A, Waite D, Ackerson L,Horsburgh C R Jr. Treatment of 171 patients with pulmonary
s
tuberculosis resistant to isoniazid and rifampin. N Engl J Med1993; 328: 527–532.
81 Yew W W, Chan C K, Chau C H, et al. Outcomes of patientswith multidrug-resistant pulmonary tuberculosis treated withofloxacin/levofloxacin-containing regimens. Chest 2000; 117:744–751.
82 Tahaoglu K, Torun T, Sevim T, et al. The treatment of multi-drug-resistant tuberculosis in Turkey. N Engl J Med 2001; 345:170–174.
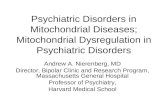
Appendix 1 Management of psychosis in individualized MDR-TB therapy (adapted fromreference 69). PO � per os; IV � intravenous; IM � intramuscular; TID � thrice daily; QD �four times daily; BID � twice daily.
APPENDICES

758 The International Journal of Tuberculosis and Lung Disease
R É S U M É
INTRODUCTION : Les problèmes psychiatriques repré-sentent un défi lors du traitement des patients atteints detuberculose à germes multirésistants (TB-MR). Une priseen charge vigoureuse s’impose à la fois pour les maladiespsychiatriques préexistantes et pour le développement decomplications psychiatriques liées aux médicaments anti-tuberculeux et aux facteurs psycho-sociaux.CONTEXTE : Une organisation de santé non-gouverne-mentale basée sur la collectivité à Lima, Pérou.OBJECTIF : Revue de la littérature concernant les compli-cations psychiatriques associées aux médicaments anti-tuberculeux, description de l’incidence et de la prévalencede la dépression de l’anxiété et de la psychose parmi lesindividus traités pour TB-MR et détails de l’approche deprise en charge utilisée dans cette cohorte.MÉTHODES : Une série rétrospective de cas a été forméepar les 75 premiers patients qui ont bénéficié d’un trai-tement individualisé pour TB-MR à Lima, Pérou, entre1996 et 1999.
RESULTATS : On a observé une dépression et une anxiétéinitiales chez respectivement 52.2% et 8.7% des patientsde cette cohorte. La plupart des individus ayant eu unedépression initiale ont ressenti une amélioration dessymptômes de dépression au cours du traitement de latuberculose. L’incidence de la dépression, de l’anxiété etde la psychose au cours du traitement de la TB-MR a étérespectivement de 13,3%, de 12,0% et de 12,0%. Alorsque la majorité des individus atteints de dépression,d’anxiété et de psychose ont nécessité une pharmacothé-rapie psychiatrique, on a pu poursuivre avec succès l’admi-nistration de cyclosérine dans tous les cas sauf un.CONCLUSION : Les comorbidités psychiatriques ne repré-sentent pas une contre-indication au traitement de laTB-MR. La prise en charge des complications psychia-triques est possible sans compromettre le traitementantituberculeux.
Appendix 2 Management of depression in individualized MDR-TB therapy (adapted from refer-ence 69).

Psychiatric issues in MDR-TB therapy 759
R E S U M E N
MARCO DE REFERENCIA : Las complicaciones psiquiá-tricas presentan un desafío en el tratamiento de pacientescon la tuberculosis multidrogo-resistente (TB-MDR).Trastornos psiquiátricos de inicio y también la presenta-ción de nuevas complicaciones psiquiátricas relaciona-das con las drogas anti-tuberculosas y factores psico-sociales requieren un manejo agresivo.LUGAR : Una organización no-gubernamental basada enla comunidad en Lima, Perú.OBJETIVO : Revisar la literatura para complicacionespsiquiátricas asociadas con los medicamentos anti-tuberculosos, describir la incidencia y prevalencia de ladepresión, ansiedad y psicosis entre los individuos reci-biendo terapia TB-MDR, y resumir con detalle los pro-tocolos de manejo usados con este cohorte.MÉTODOS : Una serie retrospectiva de casos fue reali-zada entre los primeros 75 pacientes que recibían tera-
pia TB-MDR individualizado en Lima, Peru, de 1996 a1999.RESULTADOS : Depresión y ansiedad de inicio fueronobservadas en 52,2% y 8,7%, respectivamente, de estecohorte. La mayoría de individuos con depresión de ini-cio experimentaron una mejoría de síntomas depresivosdurante el curso de su terapia antituberculosa. La inci-dencia de depresión, ansiedad y psicosis durante el trata-miento TB-MDR fue de 13,3%, 12,0%, y 12,0%, respec-tivamente. Aunque en la mayoría de individuos condepresión, ansiedad y psicosis requerían psicofármacos,se logró continuar el uso de cicloserina en todos menosun caso.CONCLUSIÓN : Comorbididades psiquiátricas no soncontraindicación para terapia TB-MDR. Manejo decomplicaciones psiquiátrica es posible sin comprometertratamiento anti-tuberculoso.