Pseudomonas aeruginosa infections
27
Pseudomonas aeruginosa infections Joanne Engel, M.D., Ph.D. Depts of Medicine and Microbiology/Immunology Case I • ID. Pt was a 63 yo AA female h/o CLL S/P splenectomy admitted for 3 day h/o fever, cough, and SOB • Meds on admission: Septra, ACV, neupogen, procrit • PE in ER • Vitals: T 38.3, RR28, 97% RA, HR114 • Labs WBC 20.4, Hb 10.3, Plts 131 • Lytes 136/4.4/105/19 BUN/Cr 34/2.3 (baseline 0.9) • LFTs AST 40, ALT24, ALK PHOS 205 • UA tr Hb, >300 protein, 11‐20 WBC • Allergies: PCN (hives) but tolerates cephalosporins Admission CXR Read as nl
Transcript of Pseudomonas aeruginosa infections
Pseudomonas aeruginosa infections
Joanne Engel, M.D., Ph.D.Depts of Medicine and Microbiology/Immunology
Case I
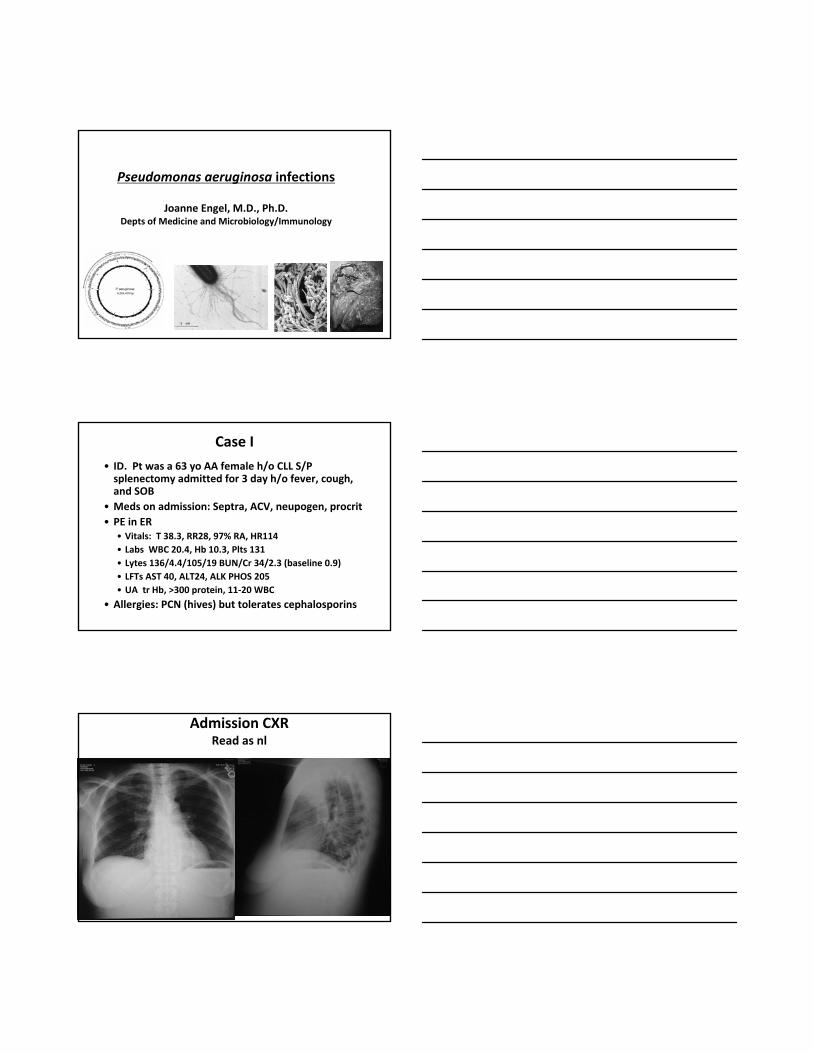
• ID. Pt was a 63 yo AA female h/o CLL S/P splenectomy admitted for 3 day h/o fever, cough, and SOB
• Meds on admission: Septra, ACV, neupogen, procrit• PE in ER
• Vitals: T 38.3, RR28, 97% RA, HR114• Labs WBC 20.4, Hb 10.3, Plts 131• Lytes 136/4.4/105/19 BUN/Cr 34/2.3 (baseline 0.9)• LFTs AST 40, ALT24, ALK PHOS 205• UA tr Hb, >300 protein, 11‐20 WBC
• Allergies: PCN (hives) but tolerates cephalosporins
Admission CXRRead as nl
Hospital Course
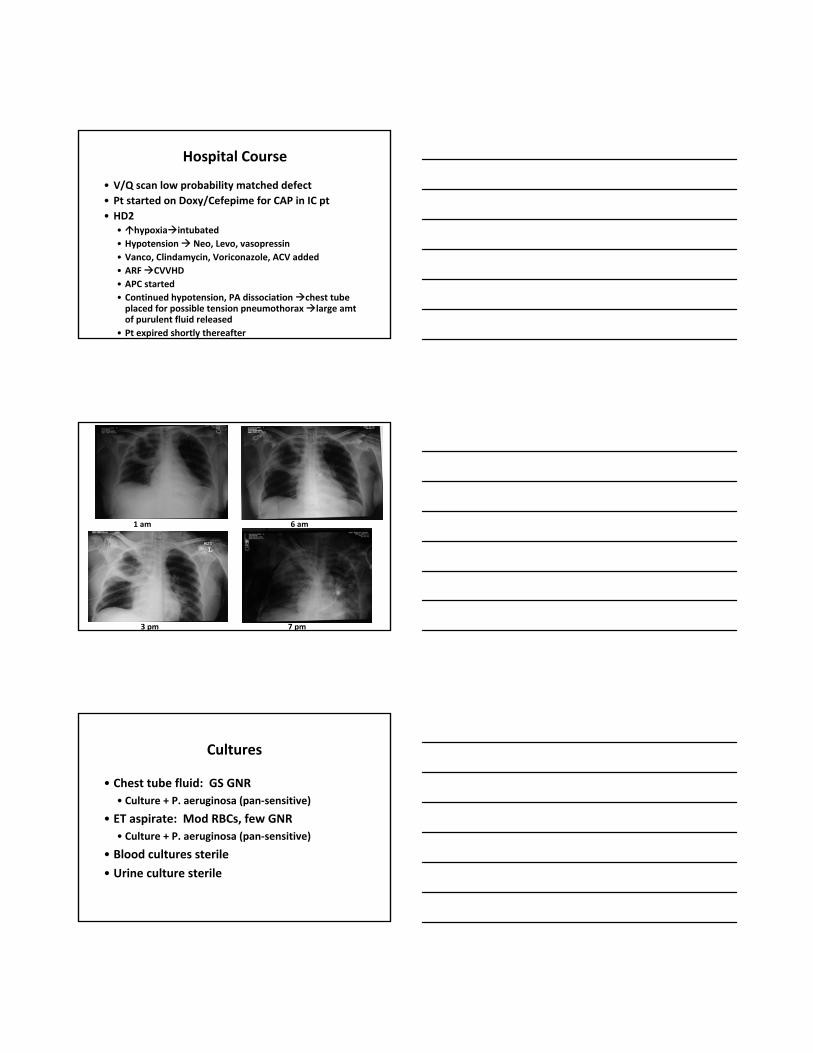
• V/Q scan low probability matched defect• Pt started on Doxy/Cefepime for CAP in IC pt• HD2
• hypoxia intubated• Hypotension Neo, Levo, vasopressin• Vanco, Clindamycin, Voriconazole, ACV added• ARF CVVHD• APC started• Continued hypotension, PA dissociation chest tube placed for possible tension pneumothorax large amt of purulent fluid released
• Pt expired shortly thereafter
1 am 6 am
7 pm3 pm
Cultures
• Chest tube fluid: GS GNR• Culture + P. aeruginosa (pan‐sensitive)
• ET aspirate: Mod RBCs, few GNR• Culture + P. aeruginosa (pan‐sensitive)
• Blood cultures sterile
• Urine culture sterile
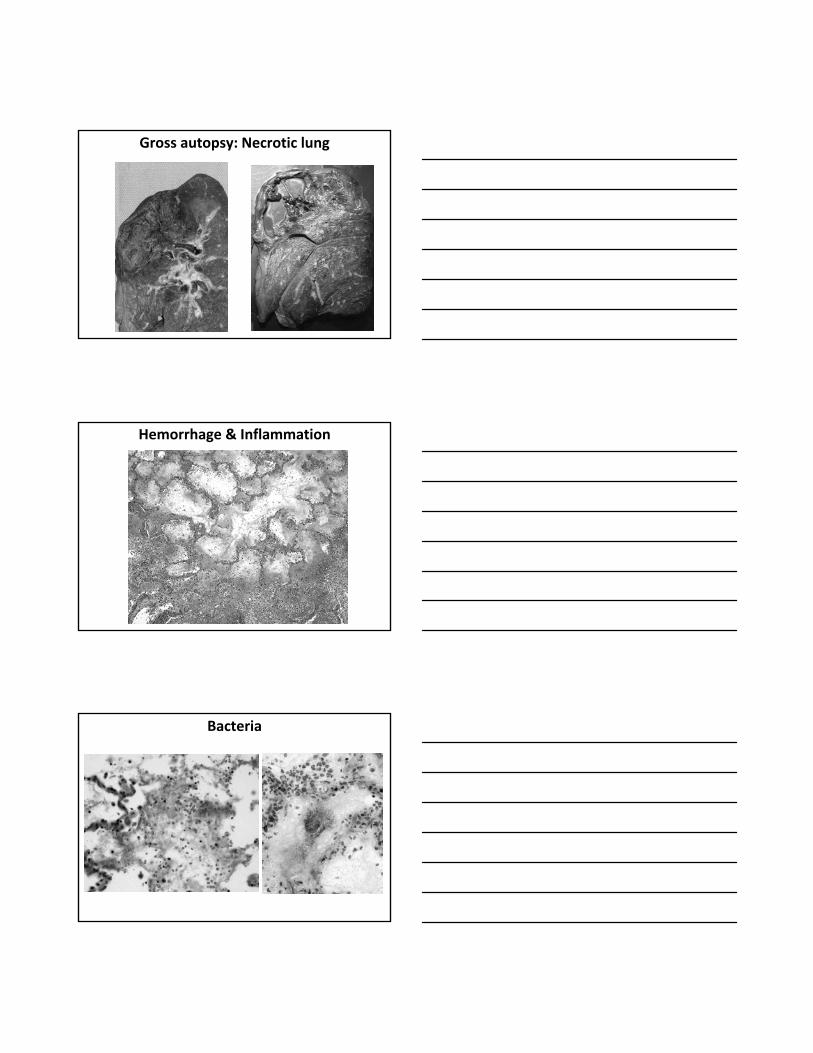
Gross autopsy: Necrotic lung
Hemorrhage & Inflammation
Bacteria
P. aeruginosa
• Microbiology
• Pathogenesis of infections• Spectrum of infections
• Principles of abx therapy
• Case studies
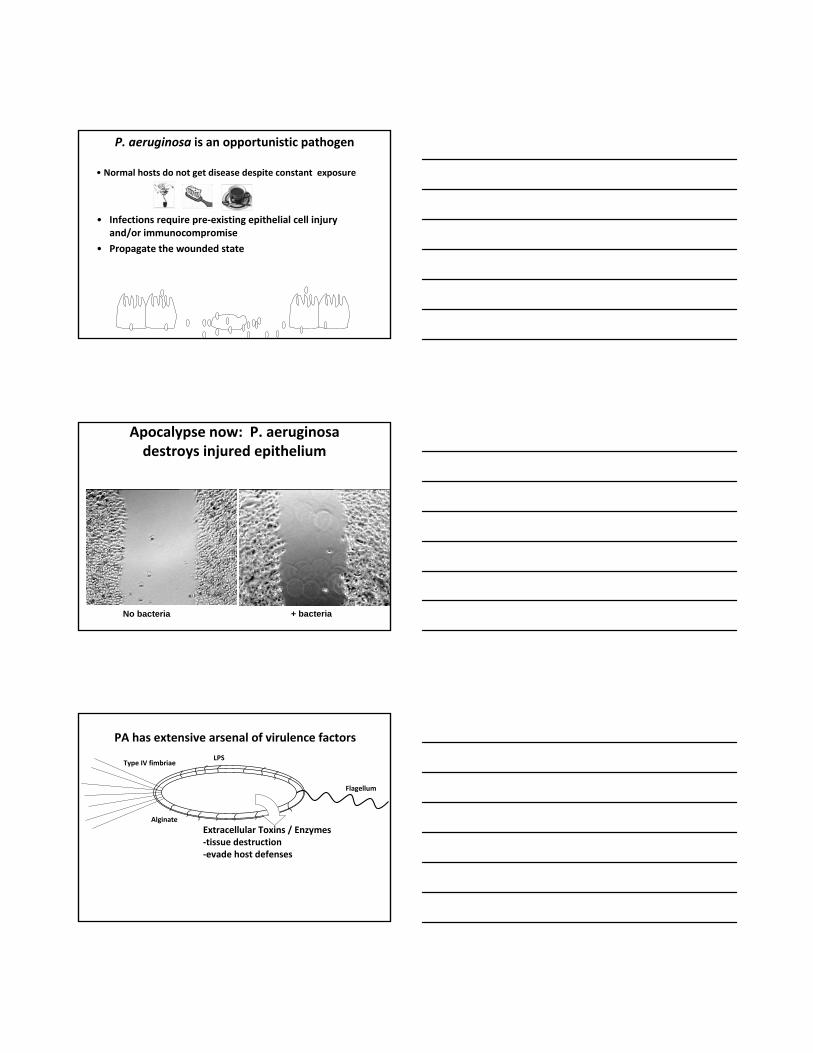
P. aeruginosa: bacteriology• Gram Negative Rod
• Aerobic, indole+, Non‐lactose fermenter• Distinguish from acinetobacter, stenotrophomonas
• Produces pigments• Pyocyanin, pyoverdin
• Ubiquitous• Grows on most carbon sources
• Found everywhere: water, soil, plants
P. aeruginosa is an opportunistic pathogen
• Normal hosts do not get disease despite constant exposure
• Infections require pre‐existing epithelial cell injury and/or immunocompromise
Epithelial cell barrier
• Infections require pre‐existing epithelial cell injury and/or immunocompromise
• Propagate the wounded state
P. aeruginosa is an opportunistic pathogen
• Normal hosts do not get disease despite constant exposure
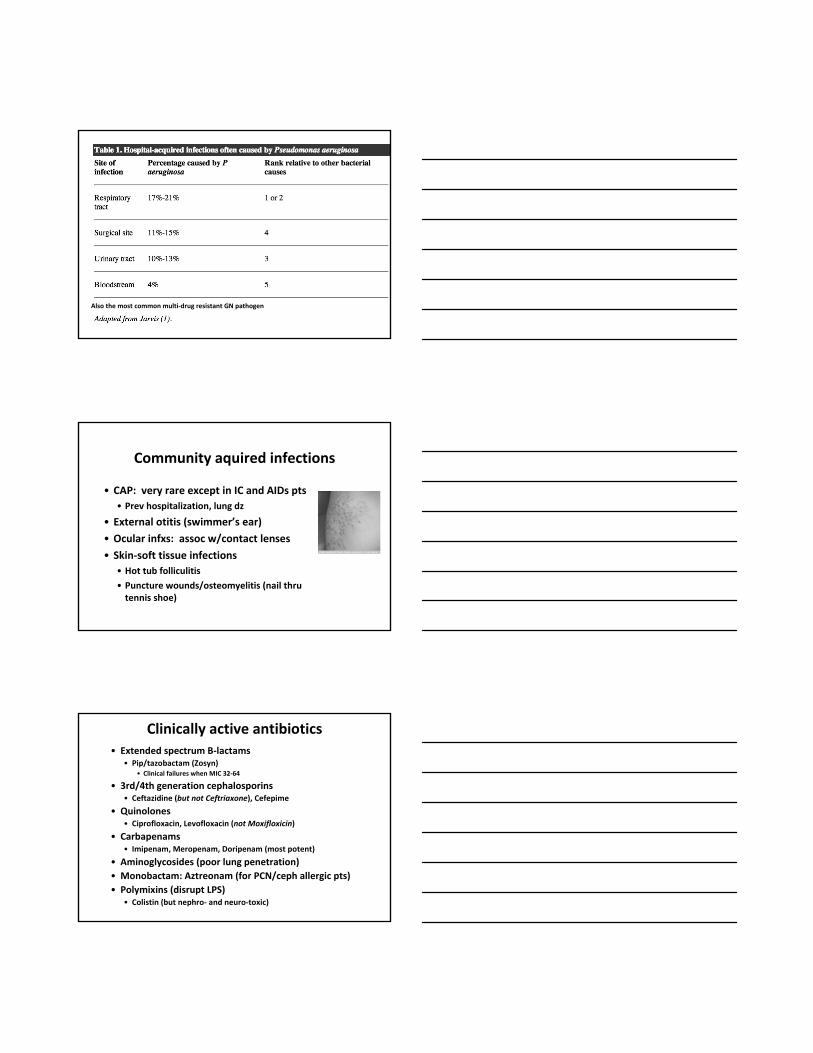
Apocalypse now: P. aeruginosa destroys injured epithelium
No bacteria + bacteria
PA has extensive arsenal of virulence factors
Alginate
Type IV fimbriae
Flagellum
LPS
Extracellular Toxins / Enzymes‐tissue destruction‐evade host defenses
Simple paradigm of pre‐exisiting epithelial injury + IC explains most PA acute Infections
Burn & wound infections
Corneal ulcers associated with contact lenses
Bladder infections
Sepsis (neutropenic pts)Endocarditis, meningitis
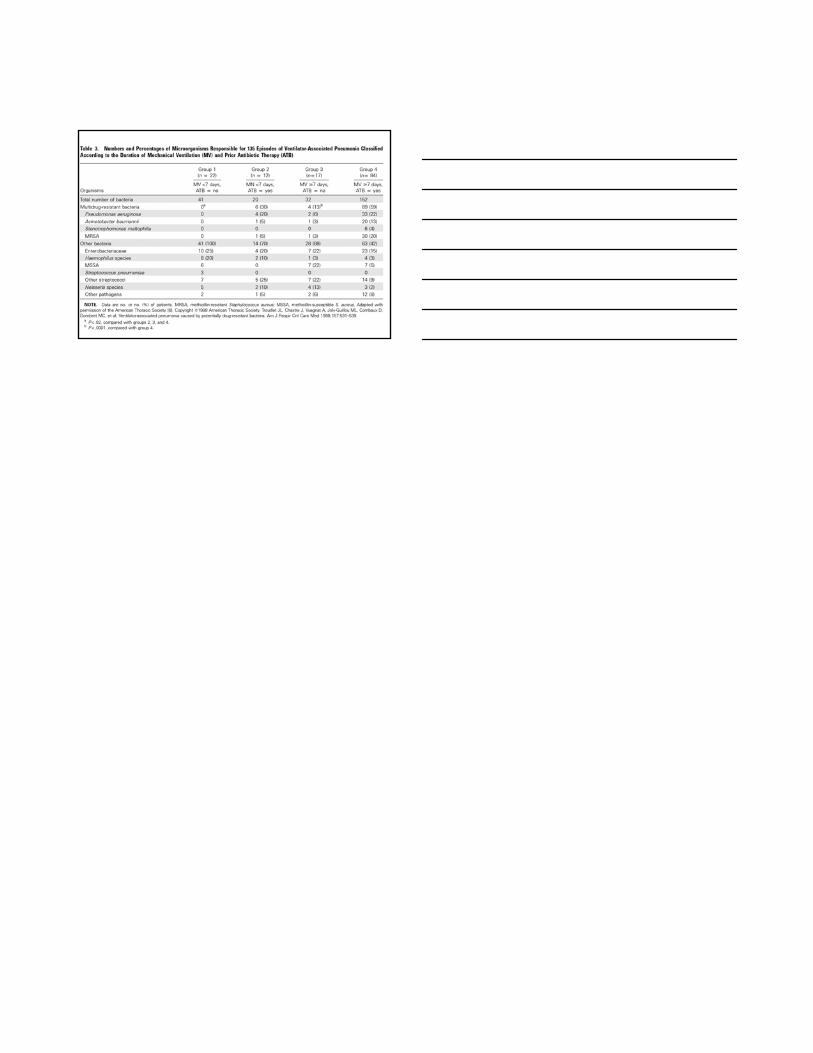
Nosocomial pneumoniaIn patients on respirators
Ecthyma gangrenosum
Chronic infections
• Chronic colonization/recurrent pneumonia in Cystic Fibrosis (CF) patients• Thought to form biofilms in the resp tract‐antibiotic resistant
• AIDS patients
Characteristic mucoid colonies
P. aeruginosa colonization in hospitalized pts
• Normal individuals out of the hospital have low colonization rate (<5%)• Moist areas: perineum, axilla, ear• Normal hosts do not get infected (intact immune system)
• Skin and GI tract colonization increases in the hospital• 4th most common nosocomial pathogen • 10% of hospital acquired infections• Hospital reservoirs: respiratory equip, sinks, veggies, flowers, whirlpools etc
Also the most common multi‐drug resistant GN pathogen
Community aquired infections
• CAP: very rare except in IC and AIDs pts• Prev hospitalization, lung dz
• External otitis (swimmer’s ear)• Ocular infxs: assoc w/contact lenses
• Skin‐soft tissue infections• Hot tub folliculitis
• Puncture wounds/osteomyelitis (nail thru tennis shoe)
Clinically active antibiotics• Extended spectrum B‐lactams
• Pip/tazobactam (Zosyn)• Clinical failures when MIC 32‐64
• 3rd/4th generation cephalosporins• Ceftazidine (but not Ceftriaxone), Cefepime
• Quinolones• Ciprofloxacin, Levofloxacin (not Moxifloxicin)
• Carbapenams• Imipenam, Meropenam, Doripenam (most potent)
• Aminoglycosides (poor lung penetration)• Monobactam: Aztreonam (for PCN/ceph allergic pts)• Polymixins (disrupt LPS)
• Colistin (but nephro‐ and neuro‐toxic)
NO activity
• PCN, ampicillin, amoxicillin
• 1st and 2nd generation cephalosporins, ceftriaxone• Moxifloxicin
• Tigecylcine, ertapenam
Reasonable two drug combinations
• Classical: b‐lactam (or cephalosporin)+aminoglycoside (synergy)• Issues: nephrotoxicity of AG, poor lung penetration
• (B‐lactam or Ceph) +quinoline (synergy or additive)• Issue: increasing quinolone resistance
• Avoid double b‐lactams• Don’t do Zosyn/cefepime or cetaz/cefepime or penam/cephalosporin
Dosing: high
• IV dosing (Assuming nl renal function)
• Pip/tazo 4.5 g q6• Ceftaz 2 q q8
• Cefepime 2q q12
• Meropenam/Imi 1 g q6• Cipro 400 q8
• Aminoglycosides (concentration dependent killing): once daily unless contra‐indications
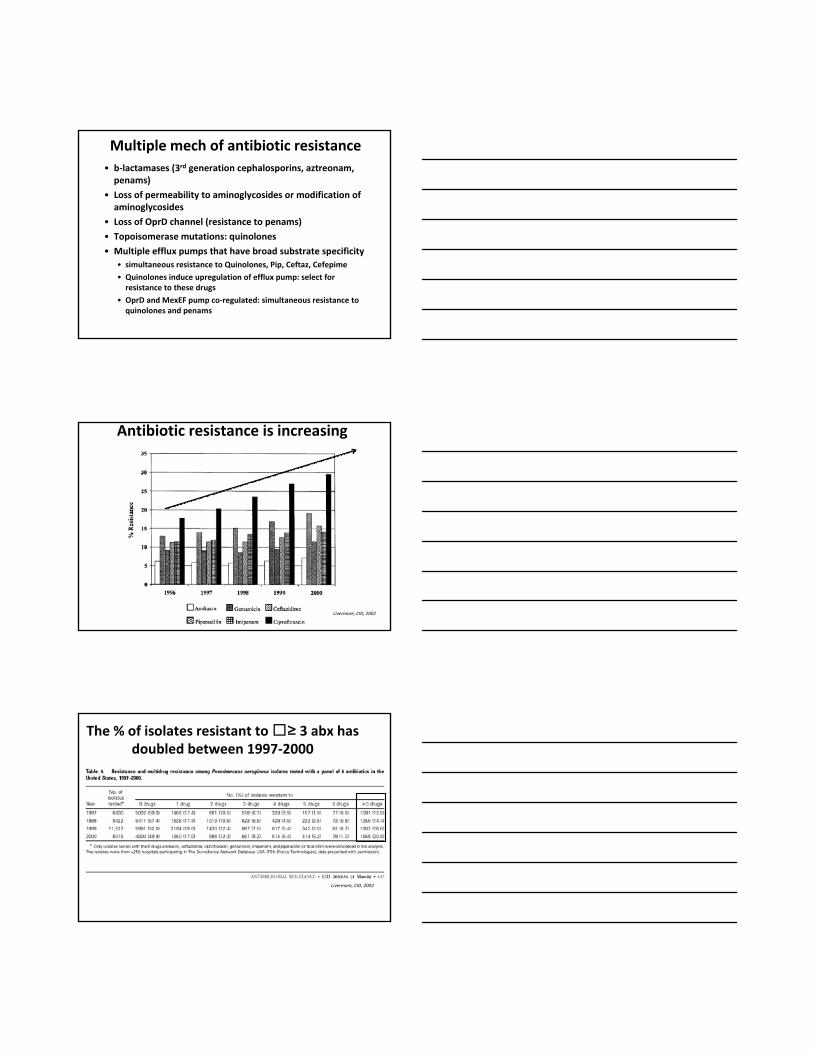
Multiple mech of antibiotic resistance• b‐lactamases (3rd generation cephalosporins, aztreonam, penams)
• Loss of permeability to aminoglycosides or modification of aminoglycosides
• Loss of OprD channel (resistance to penams)
• Topoisomerase mutations: quinolones
• Multiple efflux pumps that have broad substrate specificity • simultaneous resistance to Quinolones, Pip, Ceftaz, Cefepime
• Quinolones induce upregulation of efflux pump: select for resistance to these drugs
• OprD and MexEF pump co‐regulated: simultaneous resistance to quinolones and penams
Antibiotic resistance is increasing
Livermore, CID, 2002
The % of isolates resistant to ≥ 3 abx has doubled between 1997‐2000
Livermore, CID, 2002
Case II&III
• 63 yo f h/o AML s/p autologous SC transplant admitted with fevers, pancytopenia, peripheral blasts. Urine and 2/2 Blood cultures grow PA.
• 65 yo m severe pancreatitis c/b abd abscesses. New JP drain placed in abscess; cultures grow PA.
• What is the appropriate initial empiric rx and subsequent targeted rx?
Which one of these scenarios is appropriate?
1. For the neutropenic pt, start meropenam/tobramycin and pare back to one active abx when sensitivities are known
2. For the neutropenic pt, start meropenam/tobramycin and continue for 2 wks with two active antibiotics
3. For the pt with abd abscess, start cipro and mero and continue for 2 wks with two active antibiotics
4. For the pt with abd abscess, start meropenam and cefepime and pare back to one active abx when sensitivities are known
Why would 2 drugs be better than 1
• Inherently better coverage (synergy)
• Better odds that you have at least 1 effective abx• Prevents development of resistance
One or two antibiotics for PA infections?
• Combination is superior: • Hilf et al. Am J Med 1989; 87: 542
• Combination is not superior:• Bodey et al. Arch Intern Med 1985; 145: 1621• Chatzinikolaou et al. Arch Intern Med 2000; 160: 501• Kuikka et al. Eur J Clin Microbiol Infect Dis 1998; 17:701• Leibovici et al. Antimicrob Agents Chemother 1997; 41: 1127• Siegman‐Igra et al. Intern J Infect Dis 1998; 2: 211• Vidal et al. Arch Intern Med 1996: 156: 2121• Chamot et al Antimicrob Agents Chemother 2003; 47: 2756• Micek et al. Antimicrob Agents Chemother 2005; 49: 1306
Serious flaws w/the one study suggesting that monotherapy is inferior
• Hilf et al, AJM, 1989• 200 consec pts w/PA bacteremia. 58% immunosuppressed
• Monotherapy mortality: 47%
• Combination therapy mortality: 27%
• Did not separate out whether initial monotherapy was effective
• PA therapy was limited (ticarcillin, aminoglycosides)
• Other predictors of poor outcome: neutropenia, site of infection, critical illness
What are risk factors for developing drug resistance to PA?
C. Van delden,CID 2001. 33:1859• Case control study of 267 episodes of PA bacteremia.
• 25% of episodes preceded by exposure to anti‐PA abx• Multivariate analysis showed that previous monotherapy w/anti‐PA abx was a risk factor for subsequent isolates being resistant
• TAKE HOME MESSAGE: avoid re‐administering prev prescribed abx when initiating empiric therapies for serious PA infections
General treatment guidelines JAC 64:229, 2009
• Empiric Rx for serious infections should start w/2 anti‐pseudomonas abx of different classes until sensitivities are known, then pare back to one effective abx• Delay in effective treatment correlates with poor outcome• ? prevent development of resistance• Choice of empiric abx depends on local resistance patterns and prior abx rx
• If choice exisits, quinolone before cephalosporin/zosyn before penem
• 2 Anti‐pseudomonas drugs of different classes for Pseudomonas bacteremia in neutropenic pts, endocarditis, meningitis• ? sepsis or pneumonia• May delay development of resistance• Avoid double b‐lactams
• Monotherapy with aminoglycosides not recommended for pneumonia• poor lung penetration
• For other infections, can change to monotherapy when abx sensitivities known
• 3 controlled studies suggest that resistance to penems develops more frequently than for ceftz, cipro, or piperacillin
General treatment guidelines JAC 64:229, 2009
Which one of these scenarios is appropriate?
1. For the neutropenic pt, start meropenam/tobramycin and pare back to one active abx when sensitivities are known
2. For the neutropenic pt, start meropenam/tobramycin and continue for 2 wks with two active antibiotics
3. For the pt with abd abscess, start cipro and mero and continue for 2 wks with two active antibiotics
4. For the pt with abd abscess, start meropenam and cefepime and pare back to one active abx when sensitivities are known
Which one of these scenarios is appropriate?
1. For the neutropenic pt, start meropenam/tobramycin and pare back to one active abx when sensitivities are known
2. For the neutropenic pt, start meropenam/tobramycin and continue for 2 wks with two active antibiotics
3. For the pt with abd abscess, start cipro and mero and continue for 2 wks with two active antibiotics
4. For the pt with abd abscess, start meropenam and cefepime and pare back to one active abx when sensitivities are known
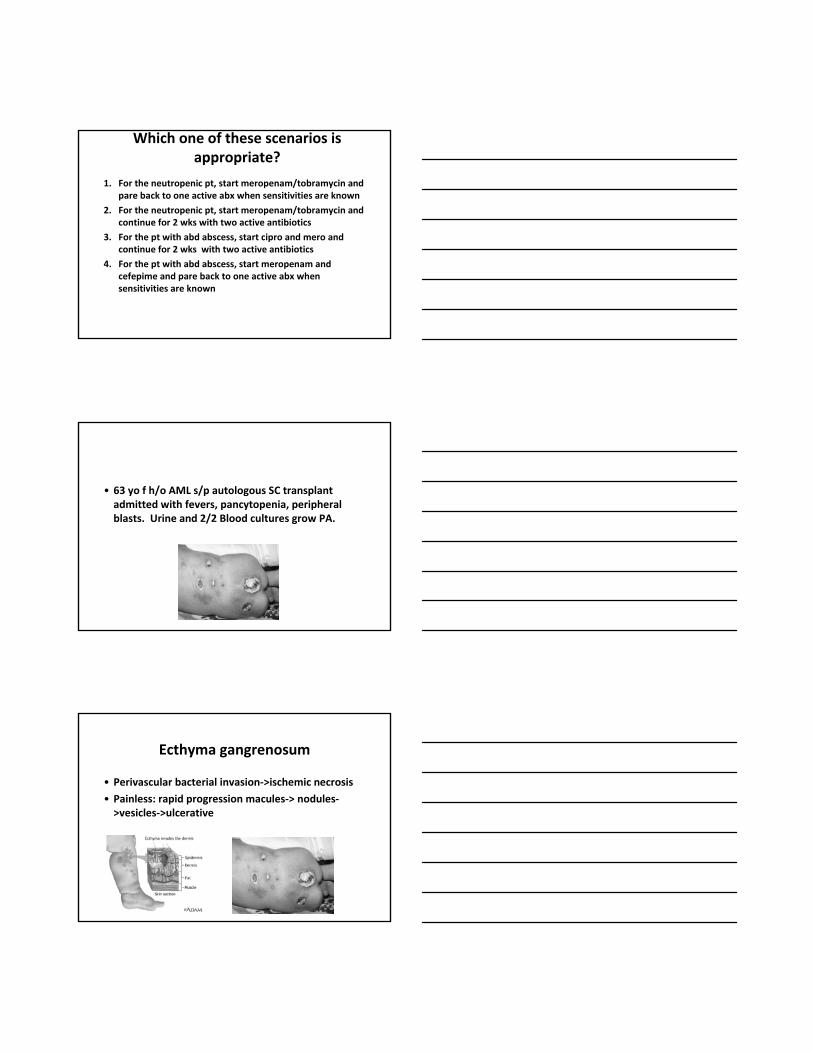
• 63 yo f h/o AML s/p autologous SC transplant admitted with fevers, pancytopenia, peripheral blasts. Urine and 2/2 Blood cultures grow PA.
Ecthyma gangrenosum
• Perivascular bacterial invasion‐>ischemic necrosis
• Painless: rapid progression macules‐> nodules‐>vesicles‐>ulcerative
Case presentation IV• 61 yo HIV+ on ARVs, quadriplegic (C3/4) trached h/o recurrent PNA and UTI’s tx’d to UCSF on 12/19/09 for hypoxemia, fever, hypotension. Placed back on ventilator. Empir Rx: Vanco/Mero/Azithro/Tamiflu• BC neg
• Mini‐BAL <10K organisms
• CXR: bilat pleural effusions; cult neg
• Urine: > 100 K PA (ceftaz‐S (MIC = 4), Tobra/Gent‐S, Pip‐S, mero‐R,Cipro/Levo‐R, ).
• C. diff neg
• Resp DFA and Resp PCR neg
• Abx changed to Vanco/Zosyn
• F/U urine cult 12/21 neg
• Repeat mini‐BAL 12/28: >10 K serratia (Pip‐S); Zosyn continued
• Defervesced but failed to wean from ventilator• ET asp 1/2/10: >10 K PA (Mero‐R, Pip‐R, Cipro/Levo R, Tobra/Gent‐S,Cefepime‐S (MIC=4)
• Chest CT: multilobar consolidation
• 1/5/10: Dev new fevers and higher PEEP rqt
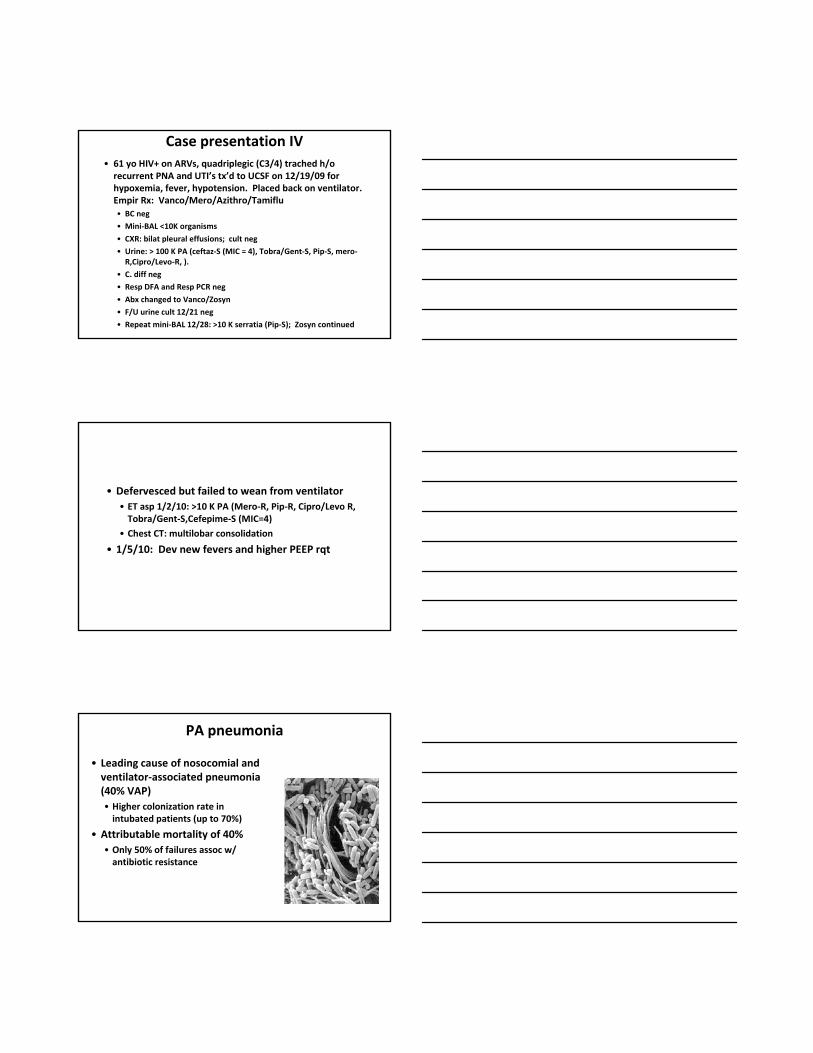
PA pneumonia
• Leading cause of nosocomial and ventilator‐associated pneumonia (40% VAP)• Higher colonization rate in intubated patients (up to 70%)
• Attributable mortality of 40%• Only 50% of failures assoc w/ antibiotic resistance

Guidelines for choosing effective rx
• Infxns usually occur w/colonizing strain• Routine endotracheal aspirates (1‐2/wk) may be helpful in predicting abx susceptibility in VAP • Chest 2005. 127; 589‐97• Intensive Care Med 2009. 35:101‐107
• Prior abx history useful in determining empiric rx• Local resistance patterns
Start w/2 drugs; narrow to 1 drug once abx sens known & pt responding to rx
• Garnacho‐Montero: Observational study of 183 episodes of PA VAP, use of 2 abx decr failure and incr survival; narrowing to monotherapy did not affect mortality, length of stay, development of resistance, recurrences (Crit Care Med 2007)
• Arts et al: Meta‐analysis: monotherapy not inferior to combination therapy (Crit Care Med 2008. 36:108)
• Heyland et al 740: pts w/VAP combination Rx (Mero/Cipro vs Mero). Overall monotherapy as good as combination rx. But for MDR GNR (PA, acinetobacter), higher freq of initial inadeq rx (84% vs 19%) & higher microbiological eradication (64% vs 30%). No difference in clinical outcomes (Critical Care Med 2008. 36:737)
How long to RxHow long to treat?
JAMA 2003. 290:2588
• Rx for 8‐14 d• PA VAP was assoc w/higher recurrence in 8 d rx though no effect on mortality
• If shorter Rx, consider f/u mini‐BAL to assess efficacy of rx.
• 61 yo HIV+ on ARVs, quadriplegic (C3/4) trached h/o recurrent PNA and UTI’s tx’d to UCSF on 12/19/09 for hypoxemia, fever, hypotension. Tx/d w/Vanco/zosyn x 14 d. Defervesced but failed to wean from ventilator• ET asp 1/2/10: >10 K PA (Mero‐R, Pip‐R, Cipro/Levo R, Tobra/Gent‐S,Cefepime‐S (MIC=4)
• 1/5/10: Dev new fevers and higher PEEP rqt
• ID consult: Increase Cefepime to 2 G IV q12 and administer over 4 hrs
• Add Tobramycin
• Pt initially had good response (repeat mini‐BAL 1/14/10 neg) though he redeveloped fevers
New uses for old abx you can teach an old dog new tricks
• Aminoglycosides (gentamycin, tobramycin, amikacin)• Poor permeability into lung
• Nephro (kidney) and oto (ear) toxic
• Requires close monitoring of serum levels (peak and trough)
• Once daily dosing for maximal benefit
• Can be given inhaled to increase lung concentrations and to limit systemic toxicity
• Colistin• No cross‐resistance to other classes
• Very nephro and neurotoxic
• Resistance through modification of LPS
• Can be given inhaled to increase lung concentrations and to limit systemic toxicity
• Synergy or beneficial effect when co‐adminstered w/2nd
effective drug
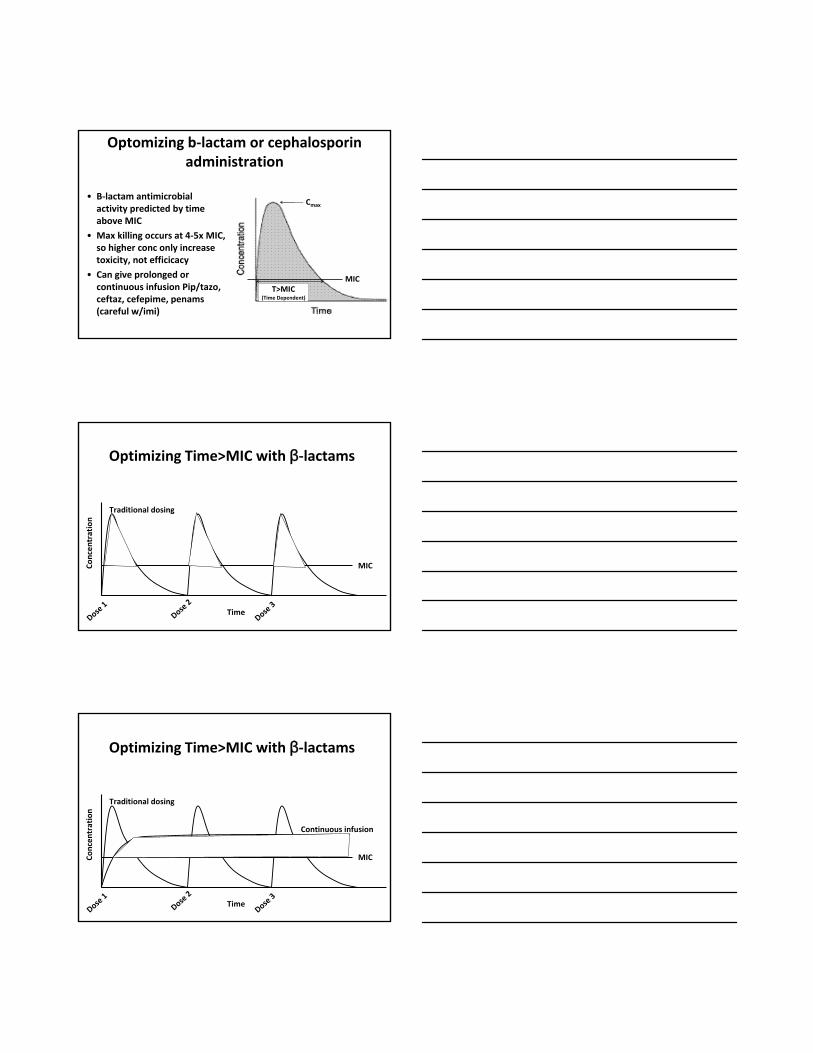
Optomizing b‐lactam or cephalosporin administration
• B‐lactam antimicrobial activity predicted by time above MIC
• Max killing occurs at 4‐5x MIC, so higher conc only increase toxicity, not efficicacy
• Can give prolonged or continuous infusion Pip/tazo, ceftaz, cefepime, penams (careful w/imi)
Cmax
MICT>MIC
(Time Dependent)
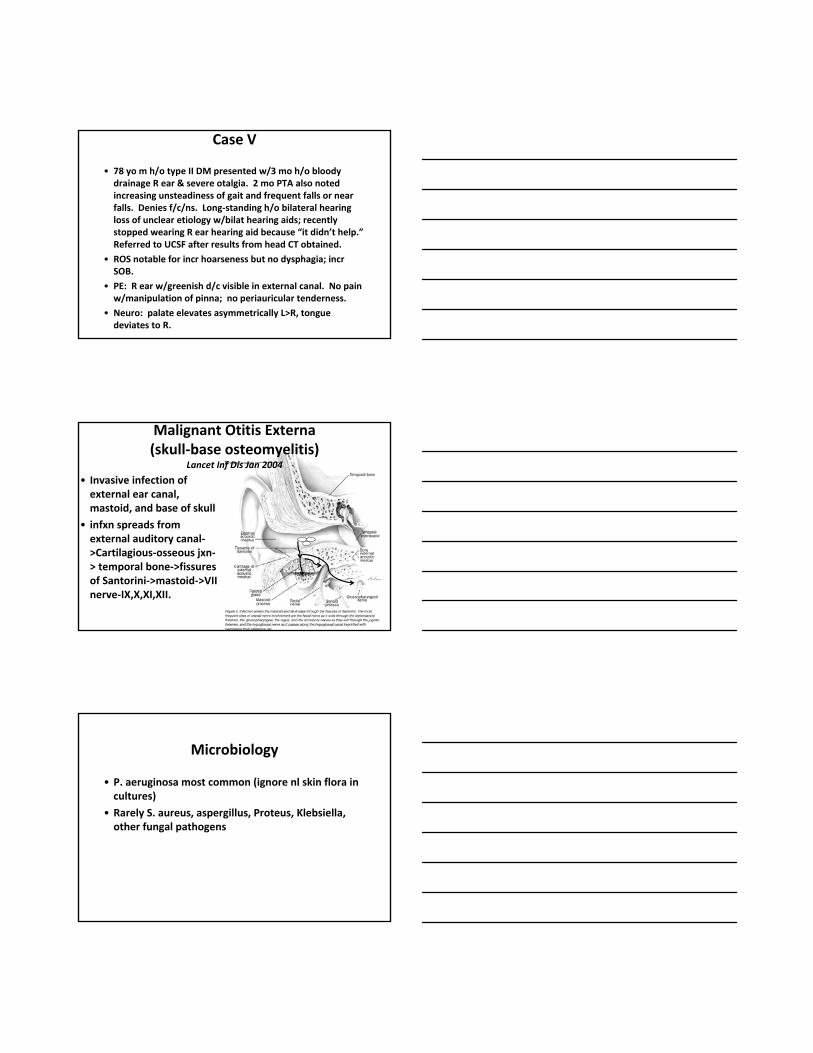
Optimizing Time>MIC with β‐lactams
Concen
tration
Time
Traditional dosing
MIC
Dose 1
Dose 2
Dose 3
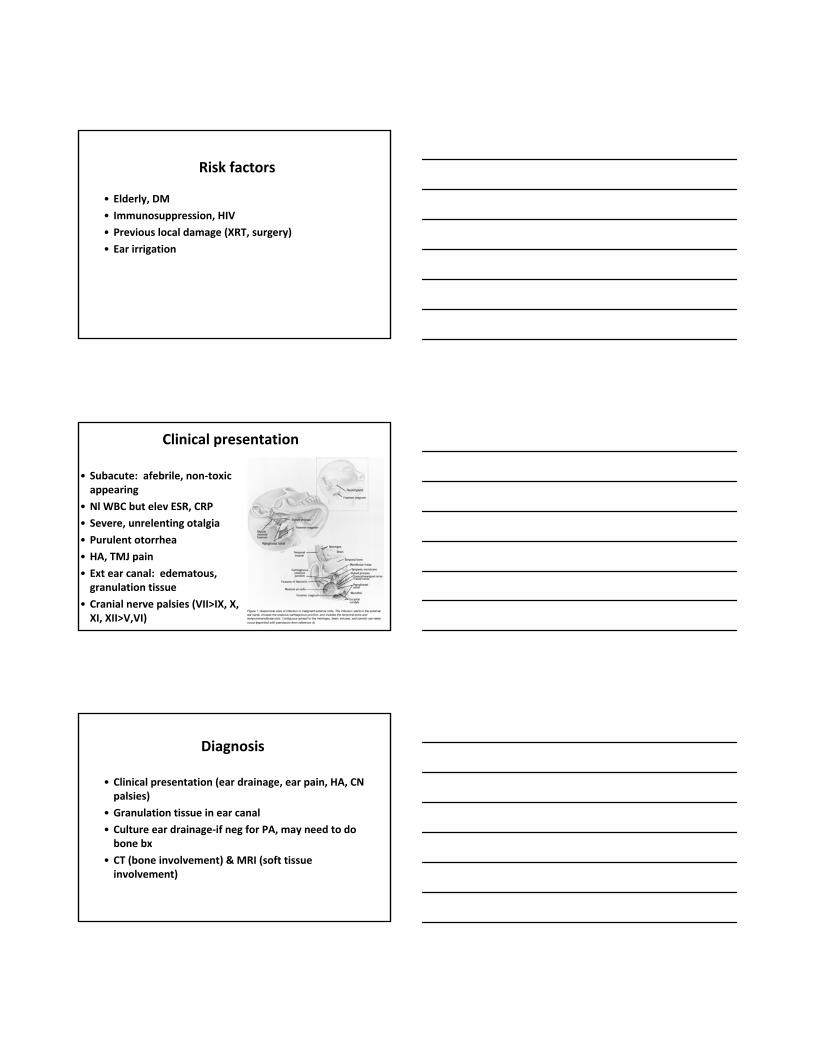
Optimizing Time>MIC with β‐lactams
Concen
tration
Time
Continuous infusion
Traditional dosing
MIC
Dose 1
Dose 2
Dose 3
Case V
• 78 yo m h/o type II DM presented w/3 mo h/o bloody drainage R ear & severe otalgia. 2 mo PTA also noted increasing unsteadiness of gait and frequent falls or near falls. Denies f/c/ns. Long‐standing h/o bilateral hearing loss of unclear etiology w/bilat hearing aids; recently stopped wearing R ear hearing aid because “it didn’t help.”Referred to UCSF after results from head CT obtained.
• ROS notable for incr hoarseness but no dysphagia; incr SOB.
• PE: R ear w/greenish d/c visible in external canal. No pain w/manipulation of pinna; no periauricular tenderness.
• Neuro: palate elevates asymmetrically L>R, tongue deviates to R.
• Invasive infection of external ear canal, mastoid, and base of skull
• infxn spreads from external auditory canal‐>Cartilagious‐osseous jxn‐> temporal bone‐>fissures of Santorini‐>mastoid‐>VII nerve‐IX,X,XI,XII.
Malignant Otitis Externa (skull‐base osteomyelitis)
Lancet Inf Dis Jan 2004
Microbiology
• P. aeruginosa most common (ignore nl skin flora in cultures)
• Rarely S. aureus, aspergillus, Proteus, Klebsiella, other fungal pathogens
Risk factors
• Elderly, DM
• Immunosuppression, HIV• Previous local damage (XRT, surgery)
• Ear irrigation
• Subacute: afebrile, non‐toxic appearing
• Nl WBC but elev ESR, CRP• Severe, unrelenting otalgia
• Purulent otorrhea• HA, TMJ pain
• Ext ear canal: edematous, granulation tissue
• Cranial nerve palsies (VII>IX, X, XI, XII>V,VI)
Clinical presentation
Diagnosis
• Clinical presentation (ear drainage, ear pain, HA, CN palsies)
• Granulation tissue in ear canal• Culture ear drainage‐if neg for PA, may need to do bone bx
• CT (bone involvement) & MRI (soft tissue involvement)
Rx
• 6‐10 wks PO (if Cipro/Levo sens) or IV Rx w/single drug
• Inpatient severe disease‐bx, debridement, IV rx• 2 drugs initially (can narrow if abx sensitivities obtained)
• Increasing quinolone resistance—only options are IV Rx
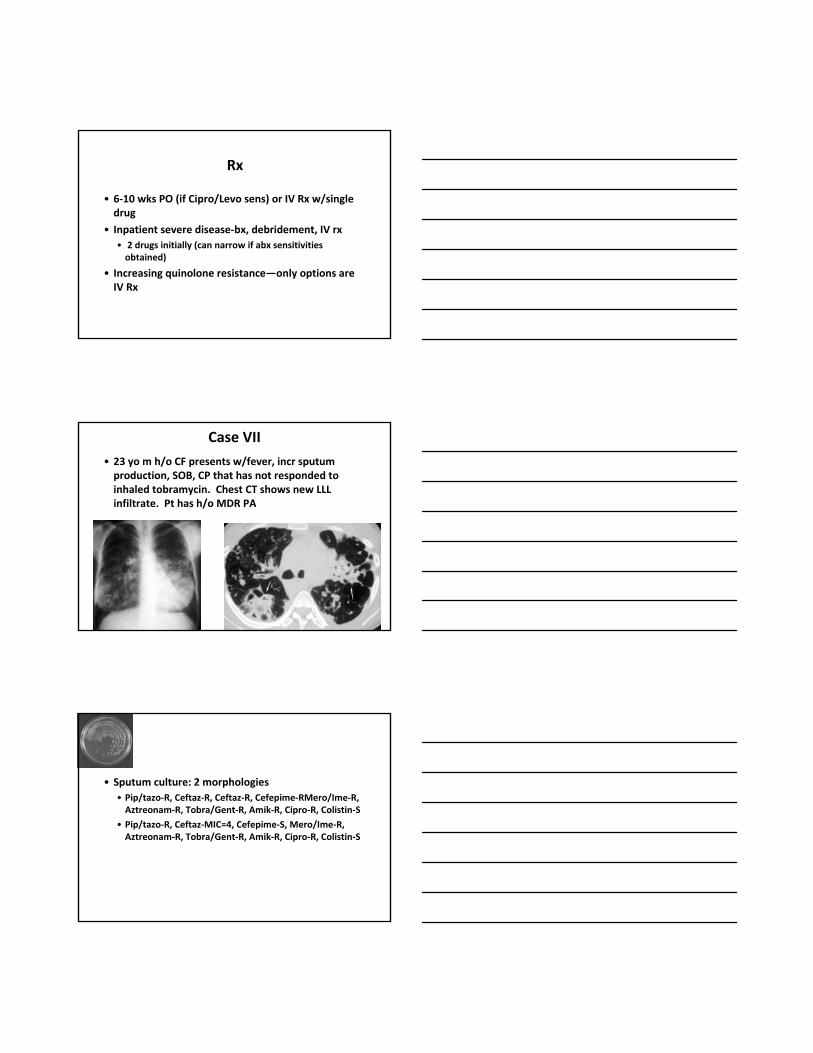
Case VII
• 23 yo m h/o CF presents w/fever, incr sputum production, SOB, CP that has not responded to inhaled tobramycin. Chest CT shows new LLL infiltrate. Pt has h/o MDR PA
• Sputum culture: 2 morphologies• Pip/tazo‐R, Ceftaz‐R, Ceftaz‐R, Cefepime‐RMero/Ime‐R, Aztreonam‐R, Tobra/Gent‐R, Amik‐R, Cipro‐R, Colistin‐S
• Pip/tazo‐R, Ceftaz‐MIC=4, Cefepime‐S, Mero/Ime‐R, Aztreonam‐R, Tobra/Gent‐R, Amik‐R, Cipro‐R, Colistin‐S
100
80
60
40
20
00‐1 2‐5 6‐10 11‐17 18‐24 25‐34 35‐44 >45
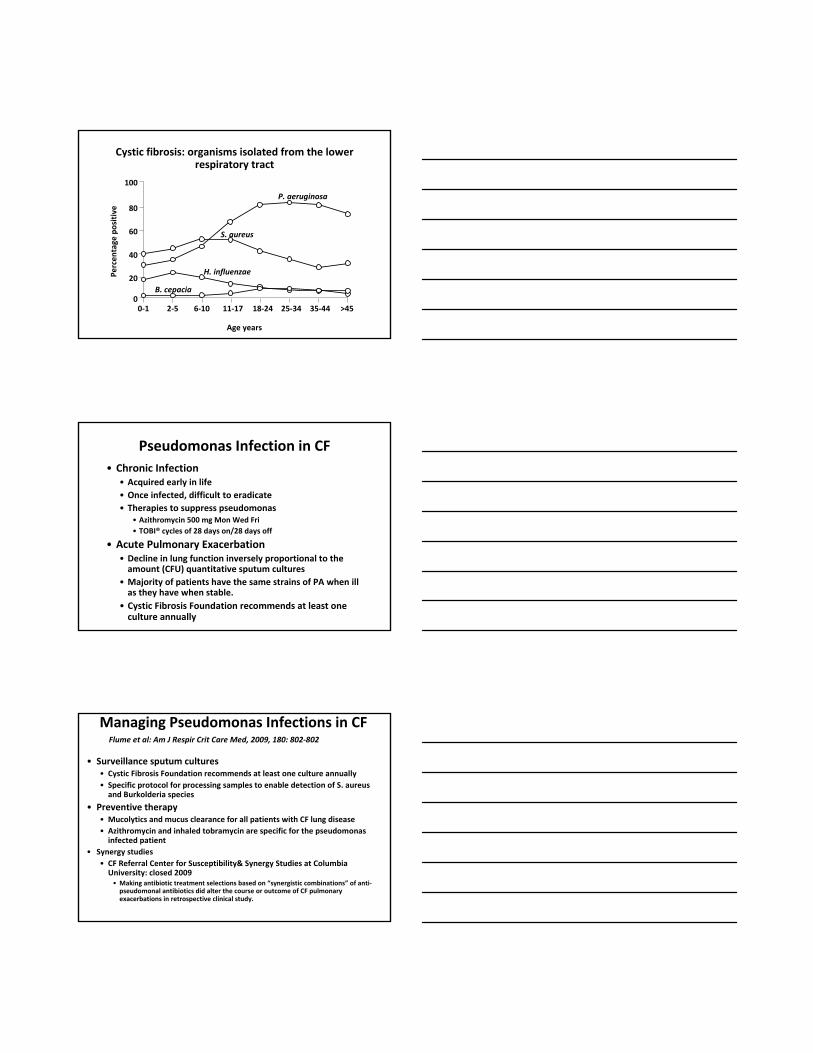
P. aeruginosa
S. aureus
H. influenzae
B. cepacia
Age years
Percen
tage
positive
Cystic fibrosis: organisms isolated from the lower respiratory tract
Pseudomonas Infection in CF• Chronic Infection
• Acquired early in life• Once infected, difficult to eradicate• Therapies to suppress pseudomonas
• Azithromycin 500 mg Mon Wed Fri• TOBI® cycles of 28 days on/28 days off
• Acute Pulmonary Exacerbation• Decline in lung function inversely proportional to the amount (CFU) quantitative sputum cultures
• Majority of patients have the same strains of PA when ill as they have when stable.
• Cystic Fibrosis Foundation recommends at least one culture annually
Managing Pseudomonas Infections in CF
• Surveillance sputum cultures • Cystic Fibrosis Foundation recommends at least one culture annually • Specific protocol for processing samples to enable detection of S. aureus and Burkolderia species
• Preventive therapy • Mucolytics and mucus clearance for all patients with CF lung disease• Azithromycin and inhaled tobramycin are specific for the pseudomonas infected patient
• Synergy studies• CF Referral Center for Susceptibility& Synergy Studies at Columbia University: closed 2009• Making antibiotic treatment selections based on “synergistic combinations” of anti‐pseudomonal antibiotics did alter the course or outcome of CF pulmonary exacerbations in retrospective clinical study.
Flume et al: Am J Respir Crit Care Med, 2009, 180: 802‐802
Treatment Guidelines of Pulmonary Exacerbation in CF
• 2 drug rx to enhance activity and reduce selection of resistant organisms• CF Referral Center for Susceptibility& Synergy Studies at Columbia University: closed 2009• Making antibiotic treatment selections based on “synergistic combinations”of anti‐pseudomonal antibiotics did alter the course or outcome of CF pulmonary exacerbations retrospective clinical study.
• Dosing of antibiotics• Once daily doing of aminoglycoside is preferred.• Insufficient evidence exists to support continuous infusion of ß‐lactam antibiotics
• Duration of therapy• Variable practice among CF Centers nationwide with insufficient evidence to endorse or refute the value of shorter duration of therapy.
Summary
• Serious infections: start w/2 abx, then narrow to one• Exceptions: neutropenic bacteremia, meningitis, endocarditis
• If recently exposed to anti‐pseud abx, use others
• Gnarly MDR bugs: extended infusion b‐lactams, aminoglycosides, colistin
Length of Rx
• UTI: pull catheter; 3‐5 d rx
• Urosepsis: 10‐14 d• Pyelonephritis: 14‐21 d
• Perinephric abscess: possibliy longer
• Prostatitis: 6‐12 wks oral quinolone• Endocarditis: surgery + 6 wks 2 drug rx
• VAP: 8‐14 d
• Meningitis: 21 d Meropenam (not Imi). • Difficult choice for 2nd drug: Quinolones‐not much experience; AG‐poor CSF penetration, requires IV or IT administration
• Ocular infxns: consult opthamologist
• Endopthalmitis: Cipro, Ceftaz, Imipenam have reasonable intraocular levels; • Direction injuection of abx
• Otitis externa: ear drops
• Malignant otitis externa: 6‐10 wks oral quinolones or IV rx
• Hot tub folliculitis: local care, or topical polymixin B, or 5‐7 d oral quinolone
• Puncture wounds/osteo: abx w/local debridement• Ecthyma gangrenosum/nec fascitis: 2 drugs IV
• Burns: topical agents, early/freq debridement of necrotis tissue• Treat overt infxns w/2 drugs
A few extra slides
Lots of studies suggest NO
• Vidal et al, Archives Int Med 1996• 189 consec episodes of PA bacteremia. 15% w/HIV
• Overall mortality 18% (much lower than older studies: better drugs, more rapid pos BC
• Predictors of poor outcome: fatal underlying disease, surgery, pneumonia, severe sepsis, ineffective definitive rx unless catheter‐associated
• Neutropenia was NOT a risk factor
• No improvement in survival if 1 vs 2 abx used.
• Bodey et al, Arch Int Med 1985• 410 episodes of PA bacteremia
• Cure rate:• 67% if received effective abx
• 14% of received ineffective abx
• Effect of delay in rx• 1‐2 d delay in effective rx reduced cure rate from 74% to 46%
• Anti‐pseud b‐lactam better than aminoglycoside; no benefit of the combination
• Poor prognosis: shock, pneumonia, persistent neutropenia
Monotherapy vs B‐lactam‐aminoglycoside combination
• Leibovici et al, AAC 1997• Prospective observational study of GN bacteremia
• Combination Rx only beneficial for neutropenic pts or pts w/PA
• Mortality rates• B‐lactam only: 13%
• B‐lactam+AG: 15%
• AG only: 23%
Are two drugs worse than one?
• Bliziotis et al, CID, 2005• Meta‐analysis of RCT to determine effect of AG‐b‐lactam therapy vs b‐lactam therapy on delaying or preventing development of antimicrobial resistance
• B‐lactam monotherapy not associated w/greater emergence of resistance than b‐lactam/AG combination
• B‐lactam monotherapy had decr superinfections and fewer treatment failures
But delay in effective Rx is bad
• Kang et al, CID 2003• Retrospective study of 136 pts PA bacteremia
• Multivariate analysis of risk factors for mortality: severe sepsis, pneumonia, delay in startive effective antimicrobial rx in neutropenic pts (worse w/longer delays), receipt of ineffective definitive rx, higher apache score
• Mortality• 27% for pts who received initial effective empirical rx
• 43% for pts who received delayed effective rx
• No difference in mortality for pts receiving 1 vs 2 drugs
• While combination therapy has not been found to be superior, there are some exceptions• Aminoglycoside monotherapy is inferior to combination
• Neutropenic patients should receive combination therapy
• A few days of empiric combination therapy and then monotherapy may be the best option
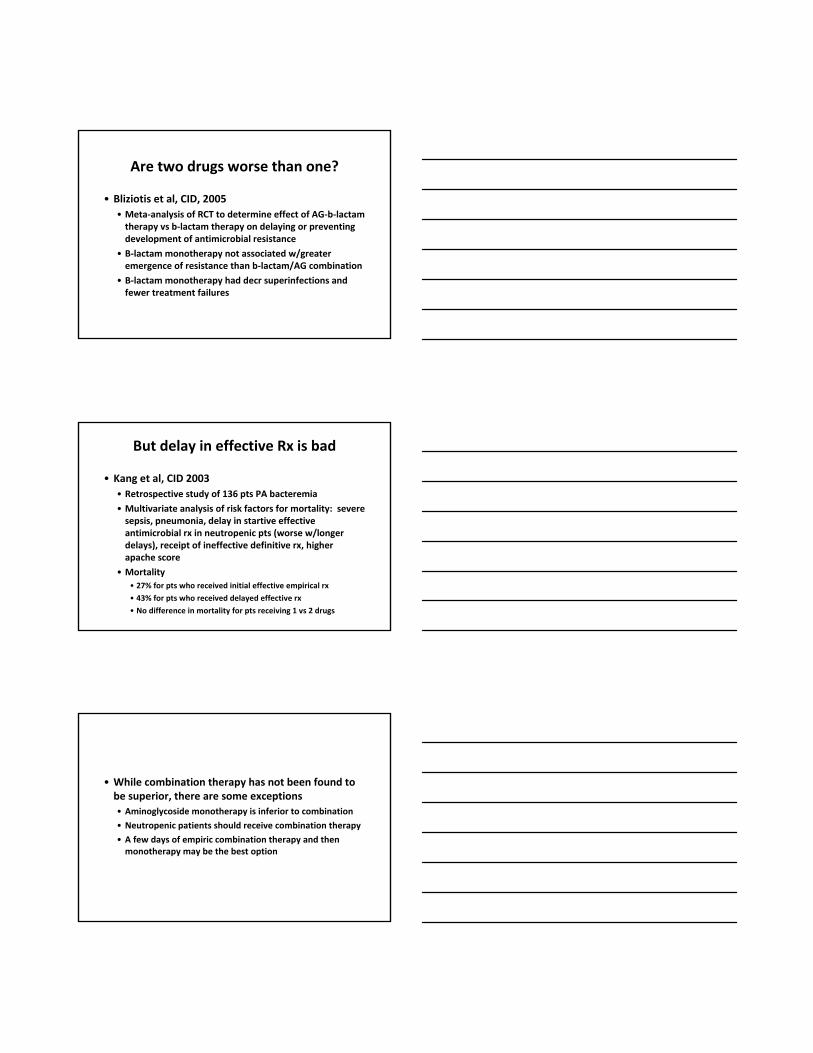
4/22 4/28
Pip/tazo S R
Ceftazidine S R
Tobramycin S S
Levofloxicin R R
Ciprofloxicin R R
Imipenam NR I
Meropenam NR R
Cefipime NR I
Colistin NT S
Treatment PipTazo Colistin/Cefepime
• 38 yo f severe encephalitis on a ventilator• Developed increasing respiratory failure and sputum (mini‐bal) showed >10,000 CFU PA
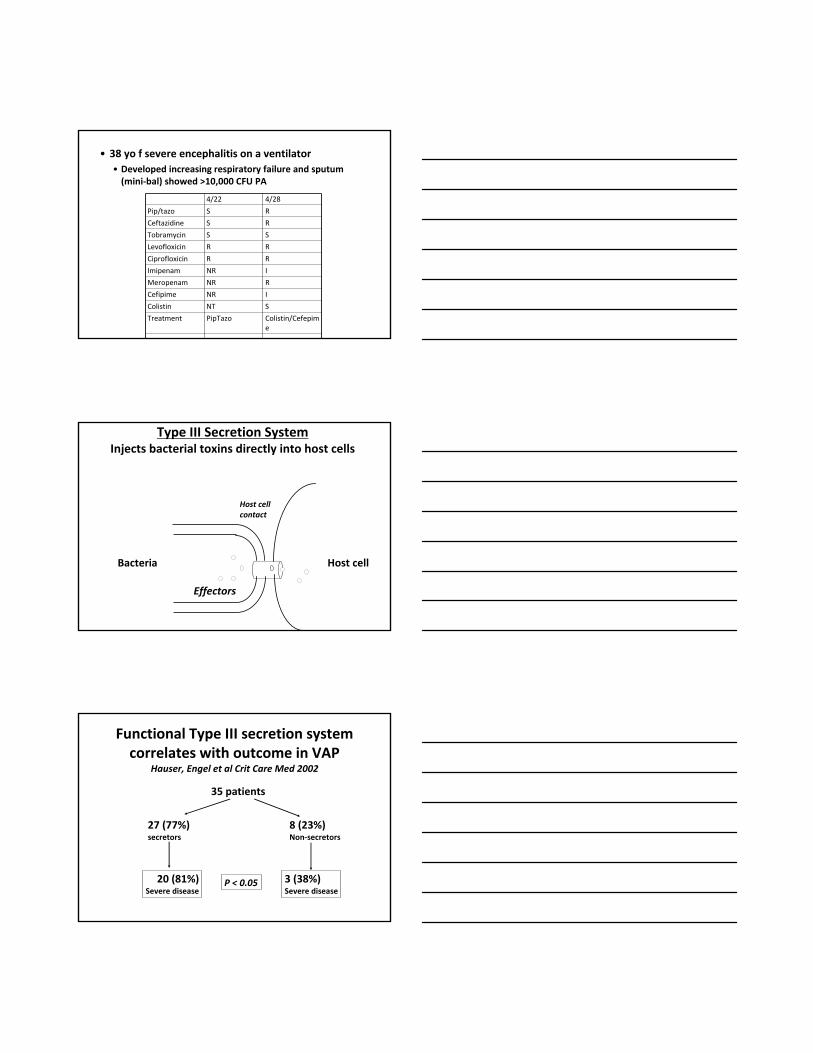
Bacteria Host cell
Type III Secretion SystemInjects bacterial toxins directly into host cells
Effectors
Host cell contact
Functional Type III secretion system correlates with outcome in VAP
Hauser, Engel et al Crit Care Med 2002
35 patients
27 (77%)secretors
8 (23%)Non‐secretors
20 (81%)Severe disease
3 (38%)Severe disease
P < 0.05