Présentation PowerPoint - American Society of...
22
2/18/2018 1 Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Nature of Affiliation Unlabeled Product Usage • Abbott Vascular • Gore&Assoc • NaviGATE • Medtronic • Consultant/Advisory Board • None • Boston Scientific • GE Medical • Philips Healthcare • Speaker • None *Core lab for numerous trials, for which I receive no direct compensation from sponsors.
Transcript of Présentation PowerPoint - American Society of...

2/18/2018
1
Rebecca T. Hahn, MD, FACC, FASE
Director of Interventional Echo
Professor of Medicine
Columbia University
Company Nature of AffiliationUnlabeled Product
Usage
• Abbott Vascular
• Gore&Assoc
• NaviGATE
• Medtronic
• Consultant/Advisory
Board• None
• Boston Scientific
• GE Medical
• Philips Healthcare
• Speaker • None
*Core lab for numerous trials, for which I receive no direct compensation from sponsors.

2/18/2018
2
Parameter TTE TEE
Sedation during
TAVR
• None required (sedation for procedure only)
• General anesthesia, monitored anesthetic care or conscious sedation
Imaging Advantages • Standard windows for assessing ventricular and valvular structure & function
• Higher resolution with high frame rates for 2D and 3D imaging
• Pre-procedural imaging may avoid complications (i.e. paravalvular regurgitation, annular/aortic rupture, coronary occlusion)
• Immediate, accurate intra-procedural diagnosis of complications
Imaging
Disadvantages
• Image quality dependent on patient factors (i.e. chest morphology, lung hyperinflation, suboptimal patient positioning)
• Procedural delay during image acquisition (to minimize radiation exposure to imager)
• Non-continuous imaging during procedure• Low resolution with low frame rates for 2D
and 3D imaging• Limited imaging windows for non-
transfemoral access routes•
• Special windows required for assessing ventricular and valvular structure & function
• Image quality dependent on patient factors (i.e. calcific acoustic shadowing, cardiac position relative to esophagus and stomach)
• Probe interference with fluoroscopic imaging (minimized by articulation of probe)
Other Advantages • Early recovery and discharge • Continuous imaging throughout procedure, irrespective of access route
Other Disadvantages • Possible higher radiation exposure to imager
• Interference with sterile field
• Need for post-procedure monitoring (Note: may not be different than for TTE)
• Trauma to oropharynx, esophagus or stomach
Retroflexion Anteflexion
Right Flexion Left Flexion
Left+Ante Right+Ante
Continuous Imaging is KEY to early detection of complications

2/18/2018
3
DOI: 10.1016/j.echo.2017.10.022
Figure 4
Journal of the American Society of Echocardiography DOI: (10.1016/j.echo.2017.10.022)
Copyright © 2017 American Society of Echocardiography Terms and Conditions
Figure 5
Pre-procedural Imaging

2/18/2018
4
DOI: 10.1016/j.echo.2017.10.022
Journal of the American Society of Echocardiography DOI: (10.1016/j.echo.2017.10.022)
Copyright © 2017 American Society of Echocardiography Terms and Conditions
Figure 8
Post-procedural Imaging
Figure 12

2/18/2018
5
DOI: 10.1016/j.echo.2017.10.022
An 80-year-old female with a past medical history of
Severe mitral stenosis status-post valvuloplasty in Moscow in 1963
Atrial fibrillation on Coumadin
Hypertension
Chronic kidney disease
Complained of increased dyspnea on exertion and fatigue that started six months prior and had progressively worsened.

2/18/2018
6
Pre-procedural transthoracic echocardiogram showed:
Rheumatic mitral valve with stenosis and a mitral valvuloplasty score of 9 (Mobility = 2, Leaflet thickness = 2, Subvalvular thickening = 4 and Calcification = 2) Mean gradient 5 mmHg
Heavily calcified aortic valve. Severe aortic stenosis Peak/mean gradients of 96.4/43.8mmHg
Ejection fraction 65-70%
Given the findings on transthoracic echocardiogram the plan was to perform a transcatheter aortic valve implantation (TAVI).
Mitral valve area of 1.2 cm2
by continuity equation
Mitral valve area of 1.35 cm2 by 3D
planimetry
Dense “smoke” in markedly dilated LAA
(no MR)
Intra-procedural TEE showed:• Severe mitral stenosis by multiple methods• Dense “smoke” in the LAA consistent with
very slow flow but no thrombus• No mitral regurgitation
In light of TEE findings, an intra-procedural decision was made to perform a percutaneous
balloon mitral valvuloplasty (PBMV) prior to TAVR

2/18/2018
7
Valvuloplasty Valvuloplasty
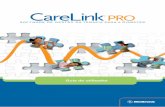
Percutaneous balloon mitral valvuloplasty was performed using a 23mm Inoue balloon. Two inflations were performed resulting in lateral
commissural fracture and improved valve opening
Pre-PBMV
Post-PBMV
Planimetered MVOA= 1.7 cm2
• Single jet of mild mitral regurgitation was seen (EROA by 3D = 13mm2)
• Smoke resolved
2/18/2018
8
Pre-PBMV Post-PBMV
MG 9.1 mmHg MG 4.9 mmHg
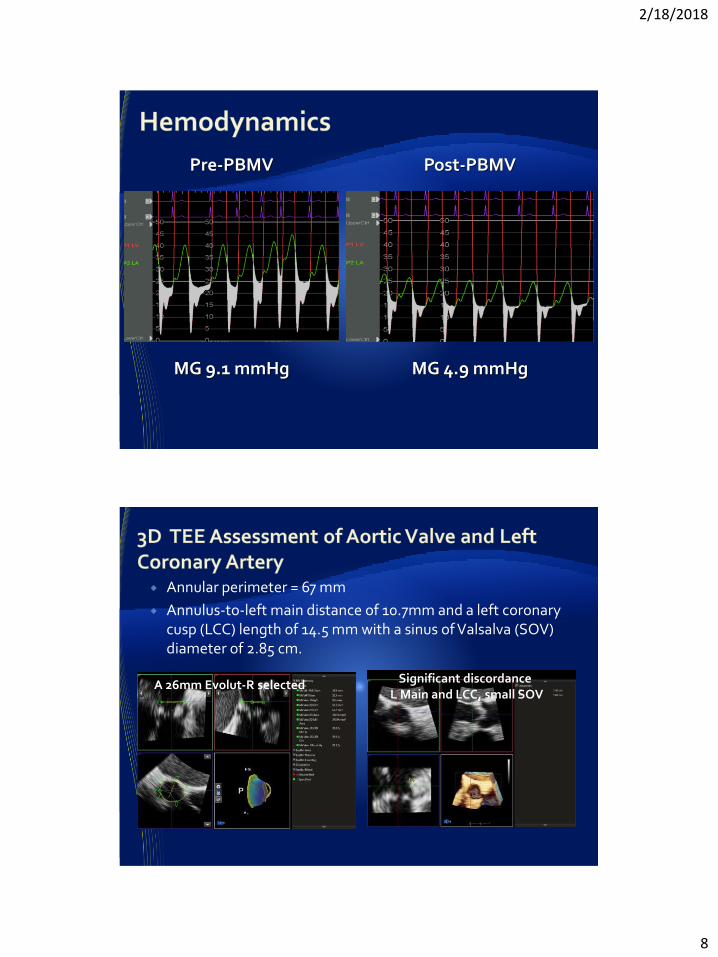
Annular perimeter = 67 mm
Annulus-to-left main distance of 10.7mm and a left coronary cusp (LCC) length of 14.5 mm with a sinus of Valsalva (SOV) diameter of 2.85 cm.
A 26mm Evolut-R selected Significant discordance L Main and LCC, small SOV

2/18/2018
9
20mm Z-Med IIballoon
During BAV the left main coronary ostium was covered by the left coronary cusp (yellow arrow) on TEE with slow/faint filling was seen
on contrast injection (red arrow).
• 6F JL 3.5
• 6F Guideliner
• 3.5 x 15mm DES placed in mLAD

2/18/2018
10
ST elevations noted on monitor
Evolut-R 26mm
Marked reduced flow in LM ostiumEvolut-R 26mm

2/18/2018
11
Deployed at 12 atm
Urgent stent deployment in LM
ST segments rapidly resolved and no wall motion abnormalities were detected

2/18/2018
12
Final AR Assessment
2+ ARNo Post-dilatation was
performed
83 year-old man
Class III heart failure
Known Severe AS for 2 years with preserved EF
PV 4.5 m/s
MG 43 mmHg
AVA 0.7cm2
EF 55%, Moderate MR. Mild pHTN.
Type II DM, CKD on HD, Morbid obesity, OSA on BiPAP
TAVR/SAVR were deferred in the past since he had Stevens-Johnson syndrome when exposed to contrast dye, twice.
In the past 5 months experienced increased fatigue after HD and was requiered to start on Midodrine.
STS 13%

2/18/2018
13
26 mm vs 29 mm valve

2/18/2018
14
Trivial agitated bubbles in the LV during BAVGood Annular Sealing – Aorta stretching

2/18/2018
15

2/18/2018
16
Trivial PVL
No central Ao Regurgitation
AVA 2.33 cm2
PV 1.6 m/s P/MG: 11/5 mmHg DI 0.44
Mild MR (No change during procedure)
HPI: 84 y/o F with Diastolic HF (NYHAIV,EF 50%), Aortic insufficiency, ESRD(on HD MWF, LUE AV fistula;still makes some urine),COPD(no intubations), HTN, hyperlipidemia, anemia, h/o GIB 2/2 to high consumption of NSAIDS(pt now reports allergy to ASA/NSAIDS
Experiencing increasing episodes of SOB, resulting in increased hospitalizations, on 2/5/18 pt presented to Outside Hospital ED c/o SOB was admitted
Echo showed worsening aortic regurgitation

2/18/2018
17

2/18/2018
18
3D EROA = 50 mm2
PISA EROA = 40 mm2Quantitative Doppler EROA = 51 mm2

2/18/2018
19
Repositioning required: Pacing used

2/18/2018
20
Complete Heart Block with lower position
Original Pacemaker Dislodged Removal of first Pacer

2/18/2018
21

2/18/2018
22