Providing information /psycho-education: What works?
43
Providing Providing information /psycho- information /psycho- education: What works? education: What works? Eutopa, Amsterdam, September 2008 Eutopa, Amsterdam, September 2008 Professor Graham Turpin Professor Graham Turpin Clinical Psychology Unit, Clinical Psychology Unit, University of Sheffield University of Sheffield [email protected] [email protected]
-
Upload
cally-allison -
Category
Documents
-
view
18 -
download
2
description
Providing information /psycho-education: What works?. Eutopa, Amsterdam, September 2008 Professor Graham Turpin Clinical Psychology Unit, University of Sheffield [email protected]. Aims of today’s talk:. Why provide information? Three RCTs assessing the impact of information - PowerPoint PPT Presentation
Transcript of Providing information /psycho-education: What works?

Providing information /psycho-Providing information /psycho-education: What works?education: What works?Eutopa, Amsterdam, September 2008Eutopa, Amsterdam, September 2008
Professor Graham TurpinProfessor Graham TurpinClinical Psychology Unit,Clinical Psychology Unit,University of SheffieldUniversity of [email protected]@shef.ac.uk

Aims of today’s talk:Aims of today’s talk:
• Why provide information?Why provide information?
• Three RCTs assessing the impact of Three RCTs assessing the impact of informationinformation
• Implications for clinical practice and Implications for clinical practice and guidelines development?guidelines development?

Draft guidelinesDraft guidelines
Recommendations*:Recommendations*:10 A supportive context is offered that consists of: 10 A supportive context is offered that consists of:
• Offering a listening ear, support and solace and being open to the immediate Offering a listening ear, support and solace and being open to the immediate practical needs of those affected,practical needs of those affected,
• Offering factual and up-to-date information about the shocking event,Offering factual and up-to-date information about the shocking event,• Mobilising social support from their own social surroundings’Mobilising social support from their own social surroundings’• Facilitating reuniting with people closest to them and keeping families Facilitating reuniting with people closest to them and keeping families
together,together,• Reassuring those affected who display normal stress reactions.Reassuring those affected who display normal stress reactions.
11 Information is offered to all those effected. Information should consist of:11 Information is offered to all those effected. Information should consist of:• A reassuring explanation of normal reactions.A reassuring explanation of normal reactions.• Saying when to seek help,Saying when to seek help,• Advising those affected to tackle the daily routine.Advising those affected to tackle the daily routine.
12 The study group does not recommend offering preventive psycho- 12 The study group does not recommend offering preventive psycho- education.education.
* These recommendations strongly endorsed by pre-meeting * These recommendations strongly endorsed by pre-meeting survey.survey.

IntroductionIntroduction• Many people will experience some form of Many people will experience some form of
traumatic event within their lives.traumatic event within their lives.
• Effective psychological interventions have been Effective psychological interventions have been developed for those suffering from the chronic developed for those suffering from the chronic reactions following exposure to trauma.reactions following exposure to trauma.
• However, these are costly and limited by However, these are costly and limited by restricted access to psychological therapies restricted access to psychological therapies
• Can providing information/ psycho-education Can providing information/ psycho-education reduce the prevalence of people presenting with reduce the prevalence of people presenting with chronic reactions following exposure to trauma?chronic reactions following exposure to trauma?

Why provide information?Why provide information?
• Positive reasons:Positive reasons:• Information: some clients will request information about Information: some clients will request information about
psychological sequelae and best coping?psychological sequelae and best coping?
• Prevention: information might promote positive coping Prevention: information might promote positive coping and decrease the likelihood of development of chronic and decrease the likelihood of development of chronic PTSD? PTSD? (NICE, 2005: Implementation guidelines - 150k (NICE, 2005: Implementation guidelines - 150k cases at a cost of £47/ cases at a cost of £47/ €€60 m per annum).60 m per annum).
• Self-help: more extensive self-help materials could Self-help: more extensive self-help materials could provide the basis of early intervention for people with provide the basis of early intervention for people with acute stress disorder etc. acute stress disorder etc. Early CBT interventions (e.g. Early CBT interventions (e.g. Bisson et al. 2005) might be implemented through self-Bisson et al. 2005) might be implemented through self-help delivery?help delivery?
• Promoting appropriate help seeking: “self-monitoring” Promoting appropriate help seeking: “self-monitoring” during watchful waiting?during watchful waiting?

Why provide information?Why provide information?
• Negative reasons:Negative reasons:• Information: some people may not wish information Information: some people may not wish information
and the possibility of sensitisation should be and the possibility of sensitisation should be considered?considered?
• Could be seen as promoting the medicalisation of Could be seen as promoting the medicalisation of ordinary distress.ordinary distress.
• Disruption of natural recovery processes and Disruption of natural recovery processes and promoting medical intervention at the expense of promoting medical intervention at the expense of social/community support?social/community support?
• Promoting inappropriate help seeking and drain on Promoting inappropriate help seeking and drain on limited resources.limited resources.

What do we know already?What do we know already?
Early interventions?Early interventions?
Supported self-help?Supported self-help?
Self-help and mental health promotion?Self-help and mental health promotion?
Information - practical Information - practical vsvs therapeutic? therapeutic?

Early intervention and PTSDEarly intervention and PTSD
• One off sessions of individual psychological One off sessions of individual psychological debriefing have not resulted in reductions in debriefing have not resulted in reductions in PTSD symptoms (Sijbrandij et al., 2006), may PTSD symptoms (Sijbrandij et al., 2006), may even slow recovery.even slow recovery.
• Early CBT interventions (e.g. Bisson et al. Early CBT interventions (e.g. Bisson et al. 2005) have shown promising results, 2005) have shown promising results, especially when targeted at those at high risk especially when targeted at those at high risk of developing PTSD.of developing PTSD.
• Nevertheless, these still require access to Nevertheless, these still require access to scant psychological therapy resources.scant psychological therapy resources.

Self-help and informationSelf-help and information• NICE guidelines recommend watchful waitingNICE guidelines recommend watchful waiting
• Monitoring of symptoms is also a component of many stepped Monitoring of symptoms is also a component of many stepped care programmes for depression and anxietycare programmes for depression and anxiety
• Guided self-help information has been shown to be effective in Guided self-help information has been shown to be effective in dealing with mild symptoms of anxiety and depression in dealing with mild symptoms of anxiety and depression in primary care. Could it be applied to acute stress reactions and primary care. Could it be applied to acute stress reactions and subsequent PTSD?subsequent PTSD?
• Moreover, the NHS in the UK generally promotes the provision Moreover, the NHS in the UK generally promotes the provision of information and self-help booklets.of information and self-help booklets.
• Despite such information being available within Accident & Despite such information being available within Accident & Emergency Departments, no studies have been conducted Emergency Departments, no studies have been conducted assessing its efficacy in preventing subsequent chronic PTSD.assessing its efficacy in preventing subsequent chronic PTSD.

Self-help and PTSDSelf-help and PTSD
• The information that does exist is inconclusive:The information that does exist is inconclusive:
Ehlers et al (2003)Ehlers et al (2003)RCT of Cognitive Therapy (CT), SH and repeated assessments (RA)RCT of Cognitive Therapy (CT), SH and repeated assessments (RA)SH group showed improvement in symptoms, but not significantly greater SH group showed improvement in symptoms, but not significantly greater than RA groupthan RA group
O’Donnell et al (2003)O’Donnell et al (2003)SH versus “management as usual”SH versus “management as usual”Trend towards improved quality of life, increased perceived functioning at Trend towards improved quality of life, increased perceived functioning at work and reduced alcohol consumption in SH groupwork and reduced alcohol consumption in SH group
Robertson et al (2002)Robertson et al (2002)Evaluation of patient satisfaction with a SH leaflet for trauma survivorsEvaluation of patient satisfaction with a SH leaflet for trauma survivorsPatients reported high levels of satisfaction with all aspects of the leafletPatients reported high levels of satisfaction with all aspects of the leaflet

Three RCTs on the effectiveness Three RCTs on the effectiveness of information provision:of information provision:
Acknowledgements:Acknowledgements:
• Alison BuggAlison Bugg
• Maria DownsMaria Downs
• Suzanne MasonSuzanne Mason
• Alison RowlandsAlison Rowlands
• Cathy ScholesCathy Scholes

General aims of the 3 RCTsGeneral aims of the 3 RCTs
To explore whether providing self-help helpTo explore whether providing self-help help
information to patients attending Accident &information to patients attending Accident &
Emergency would result in reductions in Emergency would result in reductions in
symptoms of: symptoms of: • PTSDPTSD
• Anxiety &Anxiety &
• DepressionDepression
and improvements in:and improvements in:• Quality of lifeQuality of life

Specific aims of the 3 RCTsSpecific aims of the 3 RCTs
Study 1:Study 1:
Undifferentiated sample - information leafletUndifferentiated sample - information leaflet
Turpin et al. Br J Psychiatry, 2005, 187, 76 - 82Turpin et al. Br J Psychiatry, 2005, 187, 76 - 82
Study 2:Study 2:
Screened for ASD - Self-help orientated information bookletScreened for ASD - Self-help orientated information booklet
Scholes et al.,Scholes et al., BRAT, 2008BRAT, 2008, 45, 2527 – 2536., 45, 2527 – 2536.
Study 3:Study 3:
Screened for ASD - Self-help orientated information Screened for ASD - Self-help orientated information booklet, plus writing therapy.booklet, plus writing therapy.
Bugg et al., BRAT, under revision.Bugg et al., BRAT, under revision.

MethodsMethodsGeneral design principles:General design principles:
• Randomised Control TrialsRandomised Control Trials
• Studies adopted a between groups, repeated measures Studies adopted a between groups, repeated measures design over time - up to 6 months follow up post-injury. design over time - up to 6 months follow up post-injury. Baseline/ 4-6 weeks/6 mo post injury.Baseline/ 4-6 weeks/6 mo post injury.
• Major outcome variable: PTSD symptoms assessed by self-Major outcome variable: PTSD symptoms assessed by self-report (PDS). Secondary outcomes: anxiety, depression report (PDS). Secondary outcomes: anxiety, depression (HADS) and QoL (WHO).(HADS) and QoL (WHO).
• A small qualitative component was also used to look at what A small qualitative component was also used to look at what the patients thought about the information/interventions the patients thought about the information/interventions provided. provided.

MethodsMethodsParticipantsParticipants• Recruited from local Accident & Emergency UnitRecruited from local Accident & Emergency Unit
• Inclusion Criteria: RTAs, Assaults & Occupational Injuries, aged 16-65 years, Inclusion Criteria: RTAs, Assaults & Occupational Injuries, aged 16-65 years, English speaking.English speaking.• Study 1Study 1
• 2,818 patients invited to participate2,818 patients invited to participate
• Total sample = 142 (Intervention = 75, Control = 67)Total sample = 142 (Intervention = 75, Control = 67)
• Study 2Study 2
• 1934 patients invited to participate but screened1934 patients invited to participate but screened
• Total sample = 270 (HI = 89; HC = 93; LC = 88) Study 3Total sample = 270 (HI = 89; HC = 93; LC = 88) Study 3
• Study 3Study 3
• 1454 patients invited to participate but screened1454 patients invited to participate but screened
• Total sample = 148 (SH & W = 72; SH = 76)Total sample = 148 (SH & W = 72; SH = 76)
• Note relatively low take up - 20% allowing for screeningNote relatively low take up - 20% allowing for screening

MethodsMethodsProceduresProcedures• Participants approached 1 week after attendance at A & E to Participants approached 1 week after attendance at A & E to
participate. Baseline questionnaires also sent. participate. Baseline questionnaires also sent.
• Studies 2 & 3 - screening with ASD > 50 Studies 2 & 3 - screening with ASD > 50
• On recruitment, participants randomly assigned to groups.On recruitment, participants randomly assigned to groups.
• Self-help interventions 4 - 6 weeks after attendance at A & E.Self-help interventions 4 - 6 weeks after attendance at A & E.
• For writing task, post intervention assessment 3 months post For writing task, post intervention assessment 3 months post injury.injury.
• Assessments also sent to control group (s).Assessments also sent to control group (s).
• 6 months post-injury follow-ups.6 months post-injury follow-ups.

Interventions: Information leafletInterventions: Information leaflet
Study 1Study 1
• Based on booklet developed by the Department of Psychology, Based on booklet developed by the Department of Psychology, Harrogate District Hospital.Harrogate District Hospital.
• Consisted of 550 words and 8 pages, and a Flesch-Kincaid reading Consisted of 550 words and 8 pages, and a Flesch-Kincaid reading age of 8 years.age of 8 years.
• Education/Normalisation regarding:Education/Normalisation regarding:• Common physiological & psychological reactions to traumatic injury.Common physiological & psychological reactions to traumatic injury.
• Behavioural reactions Behavioural reactions
• Advice regarding Advice regarding • Non-avoidance Non-avoidance
• Utilization of emotional supportUtilization of emotional support

Interventions: Self-Help BookletInterventions: Self-Help Booklet**
Study 2Study 2
• Information sheet replaced by more intensive self-Information sheet replaced by more intensive self-help booklet (O’Donnell and Creamer, help booklet (O’Donnell and Creamer, University of University of MelbourneMelbourne).).
• 31 pages long - Flesch Kincaid reading age 9 and 31 pages long - Flesch Kincaid reading age 9 and reading ease of 56.reading ease of 56.
• Booklet delivered earlier - under 4 vs 6 weeks.Booklet delivered earlier - under 4 vs 6 weeks.
• Emphasized the need to expose to trauma Emphasized the need to expose to trauma reminders -frequently and for long enough periods.reminders -frequently and for long enough periods.
** Both leaflet and booklet can be downloaded from: Both leaflet and booklet can be downloaded from:
http://www.shef.ac.uk/clinicalpsychology/researchhttp://www.shef.ac.uk/clinicalpsychology/research

Interventions: Writing taskInterventions: Writing task
Study 3Study 3
• Booklet delivered either alone or in conjunction Booklet delivered either alone or in conjunction with the “Pennebaker Writing Paradigm” with the “Pennebaker Writing Paradigm” (Pennebaker, 1997; (Pennebaker, 1997; Psychological SciencePsychological Science))
• Patients in the intervention group received 1 Patients in the intervention group received 1 face-to-face session where the “Writing face-to-face session where the “Writing Paradigm” is introduced.Paradigm” is introduced.
• Two follow-up telephone sessions around the Two follow-up telephone sessions around the “Writing paradigm”“Writing paradigm”

Results - samplesResults - samples
A synthesis of the three studies:A synthesis of the three studies:• Low recruitment rates (about 20%) but typical of Low recruitment rates (about 20%) but typical of
trauma studies.trauma studies.
• Some differences in responders vs non-Some differences in responders vs non-responders - younger, mail and assaults.responders - younger, mail and assaults.
• Few baseline differences, although large Few baseline differences, although large differences between high and low risk samples differences between high and low risk samples in studies 2 and 3in studies 2 and 3
• Sample consisted of road traffic accidents, Sample consisted of road traffic accidents, assaults and industrial accidents.assaults and industrial accidents.

Results - interventionsResults - interventions
A synthesis of the three studies:A synthesis of the three studies:• Study 1:Study 1:
• Intervention: post intervention improvement greater Intervention: post intervention improvement greater for control group but for control group but nono difference at difference at follow upfollow up for for PDS.PDS.
• Intervention group showed Intervention group showed greatergreater depression at depression at follow up.follow up.
• Studies 2 and 3:Studies 2 and 3:• Recovery effects in all groups but Recovery effects in all groups but nono differences differences
according to self-help or self-help plus writing according to self-help or self-help plus writing intervention when compared to controlsintervention when compared to controls

Results - acceptabilityResults - acceptability
A synthesis of the three studies:A synthesis of the three studies:• All studies:All studies:
• Feedback from participants showed high levels of Feedback from participants showed high levels of satisfaction with both the information leaflet and the satisfaction with both the information leaflet and the more extensive self-help booklet.more extensive self-help booklet.
• Normalisation and coping strategies valued.Normalisation and coping strategies valued.
• Participants reported reading the information and also Participants reported reading the information and also trying out advice and suggested activities.trying out advice and suggested activities.
• Writing task was acceptable and performed by Writing task was acceptable and performed by majority of participants. Rated as helpful.majority of participants. Rated as helpful.

Type of Injury - Study 1Type of Injury - Study 1
• RespondersResponders
• AssaultsAssaults - 67- 67
• Occupational InjuriesOccupational Injuries - 103- 103
• RTAsRTAs - 121- 121
• Non-respondersNon-responders
• AssaultsAssaults - 753- 753
• Occupational InjuriesOccupational Injuries - 1074- 1074
• RTAsRTAs - 700- 700

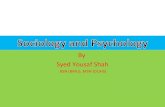
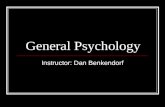
Results :Post interventionResults :Post interventionPTSD (caseness) - Study 1PTSD (caseness) - Study 1
Almost significant differencesAlmost significant differences between groups in between groups in relation to caseness on PDS (Fishers Exact , p =0.06).relation to caseness on PDS (Fishers Exact , p =0.06).
Control group 50% reductionControl group 50% reduction
Intervention group 20% reductionIntervention group 20% reduction
0
5
10
15
20
25
Baseline Post-intervention
Interventioncontrol

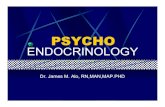
Results: follow-up - Study 1Results: follow-up - Study 1
PTSD casenessPTSD caseness24
20 19
10
14
10
0
5
10
15
20
25
Baseline Post-intervention
Follow-up
InterventionControl
No significant differences between the groups

Results: Post interventionResults: Post interventionSymptom severity - Study 1Symptom severity - Study 1 PDSPDS
• Significant reductionsSignificant reductions over time over time
• NoNo significant differences between groups significant differences between groups
AnxietyAnxiety
• Significant reductionsSignificant reductions over time over time
• NoNo significant differences between groups significant differences between groups
DepressionDepression
• Significant reductionsSignificant reductions over time over time
Almost significantAlmost significant difference (p=0.054) between difference (p=0.054) between groups: groups: intervention group more depressedintervention group more depressed..

Results: Follow-upResults: Follow-upSymptom severity - Study 1 Symptom severity - Study 1
PDSPDS
• SignificantSignificant reductions over time reductions over time
• NoNo significant differences between groups significant differences between groups
AnxietyAnxiety
• Significant Significant reductions over timereductions over time
• NoNo significant differences between groups significant differences between groups
DepressionDepression
• SignificantSignificant reductions over time reductions over time
Significantly greater reductions for control groupSignificantly greater reductions for control group
[F (1,98) = 3.14, p <0.05][F (1,98) = 3.14, p <0.05]

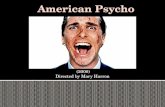
Results: Effects of the intervention Results: Effects of the intervention - Study 2- Study 2
Comparisons of HI vs HCComparisons of HI vs HC
Analyses of completer sampleAnalyses of completer sampleSymptom severity: Symptom severity: MANOVA on improvement scores for PDS, MANOVA on improvement scores for PDS,
HADS-A and HADS-D. HADS-A and HADS-D. No significant group differenceNo significant group difference found at found at post-intervention or follow-up post-intervention or follow-up (Post-intervention: Wilks’ Lambda=0.98, (Post-intervention: Wilks’ Lambda=0.98, F(3,110)= 0.99, ns; Follow-up: Wilks’ Lambda=0.96, F(3,85)= 1.17, ns) F(3,110)= 0.99, ns; Follow-up: Wilks’ Lambda=0.96, F(3,85)= 1.17, ns)
Repeated Measures ANOVAs: Repeated Measures ANOVAs: Significant main effect for timeSignificant main effect for time in in all cases all cases (p<0.001)(p<0.001), but , but nono significantsignificant main effect for group or main effect for group or group x time interactions group x time interactions (all p>0.46)(all p>0.46)
Caseness: Caseness: No significant differencesNo significant differences in PTSD, anxiety or depression in PTSD, anxiety or depression at post-intervention or follow-upat post-intervention or follow-up
Quality of life: Quality of life: No significant differencesNo significant differences

PDS scores for HI & HC groups
0
5
10
15
20
25
30
Baseline Post-intervention 6 months
Time
PD
S S
ev
eri
ty S
co
re
HIHC

Results: Effects of the intervention Results: Effects of the intervention - Study 3- Study 3
Comparisons of WI vs IComparisons of WI vs I
Analyses of completer sampleAnalyses of completer sampleSymptom severity: Symptom severity: MANOVA on improvement scores for PDS, MANOVA on improvement scores for PDS,
HADS-A and HADS-D. HADS-A and HADS-D. No significant group differenceNo significant group difference found at found at post-intervention or follow-up.post-intervention or follow-up.
Repeated Measures ANOVAs: Repeated Measures ANOVAs: Significant main effect for timeSignificant main effect for time in in all cases all cases (p<0.001)(p<0.001), but , but nono significantsignificant main effect for group or main effect for group or group x time interactions. group x time interactions.
Caseness: Caseness: No significant differencesNo significant differences in PTSD, anxiety or depression in PTSD, anxiety or depression at post-intervention or follow-upat post-intervention or follow-up
Quality of life: Quality of life: No significant differencesNo significant differences

Results: Booklet ratings - Study 1Results: Booklet ratings - Study 1
• 8 patients choose not to read the booklet8 patients choose not to read the booklet
• Out of 75 patients who did, 66% rated it Out of 75 patients who did, 66% rated it useful.useful.
• 38% gave further qualitative feedback:38% gave further qualitative feedback:• 47% valued the information and advice47% valued the information and advice
• 32% valued the normalisation of responses32% valued the normalisation of responses

Results: Patient perception of the Results: Patient perception of the self-help booklet - Study 2self-help booklet - Study 2
Rating of Rating of usefulnessusefulness
(1-5)(1-5)
Number of participants (%)Number of participants (%)
11 (not at all useful)(not at all useful)
22 (a little bit useful)(a little bit useful)
33 (moderately useful)(moderately useful)
4 4 (very useful)(very useful)
55 (extremely useful)(extremely useful)
Section on psychological sequelaeSection on psychological sequelae
1 (1.92%) 1 (1.92%)
2 (3.85%) 2 (3.85%)
22 (42.31%) 22 (42.31%)
19 (36.54%) 19 (36.54%)
8 (15.38%) 8 (15.38%)
Mean (SD) Mean (SD) = 3.60 (0.87)= 3.60 (0.87)
Section on coping strategiesSection on coping strategies
1 (2.00%)1 (2.00%)2 (4.00%)2 (4.00%)
17 (34.00%)17 (34.00%)21 (42.00%) 21 (42.00%)
9 (18.00%)9 (18.00%)
Mean (SD) Mean (SD) = 3.70 (0.89)= 3.70 (0.89)

Results: Booklet and “writing” ratings Results: Booklet and “writing” ratings - Study 3- Study 3
• High compliance with booklet: WI 90%; I 89%High compliance with booklet: WI 90%; I 89%
• More in the WI group read it carefully (52% vs 25%)More in the WI group read it carefully (52% vs 25%)
• Info on trauma: 72% (I) & 68% (WI) - Info on trauma: 72% (I) & 68% (WI) - moderately/very/extremely usefulmoderately/very/extremely useful
• Coping strategies: 75% (I) & 68% (WI) - Coping strategies: 75% (I) & 68% (WI) - moderately/very/extremely usefulmoderately/very/extremely useful
• 71% of the Writing Group rated the writing as 71% of the Writing Group rated the writing as very/extremely useful.very/extremely useful.
• Only 2 (6.5%) participants found it too Only 2 (6.5%) participants found it too distressing/emotional.distressing/emotional.

Discussion - Study 1Discussion - Study 1• Rates of PTSD for sample (31%) consistent with Rates of PTSD for sample (31%) consistent with
traumatised groups and other local research. traumatised groups and other local research.
• Results in opposite direction to that hypothesised: trend Results in opposite direction to that hypothesised: trend for caseness for PDS to be lower in control, with lower for caseness for PDS to be lower in control, with lower levels of depressionlevels of depression
• Although relatively high symptom severity , the majority Although relatively high symptom severity , the majority of patients did not meet criteria for PTSD. This may have of patients did not meet criteria for PTSD. This may have reduced statistical power. However, based on small reduced statistical power. However, based on small effect size of .27, a total sample of 120 would be effect size of .27, a total sample of 120 would be sufficient for .80 power at an alpha level of 0.05.sufficient for .80 power at an alpha level of 0.05.
• Lack of significant gains for the self-help group Lack of significant gains for the self-help group consistent with prior research.consistent with prior research.

Discussion - Study 1Discussion - Study 1
Other factors:Other factors:• Many A&E attenders had minor injuries and not exposed Many A&E attenders had minor injuries and not exposed
to trauma.to trauma.
• Information sheet may have been ineffective as a tool.Information sheet may have been ineffective as a tool.
• Patients may not have complied with advice given.Patients may not have complied with advice given.
• Information sheet may have been delivered too late.Information sheet may have been delivered too late.
• Intervention group may have been more likely to report Intervention group may have been more likely to report symptoms following psycho-education.symptoms following psycho-education.
• Reliance on self-report assessmentReliance on self-report assessment

Discussion - Study 2Discussion - Study 2
• No evidence obtained to support beneficial No evidence obtained to support beneficial effects of providing self-help information as an effects of providing self-help information as an early intervention for traumatic injury survivors early intervention for traumatic injury survivors with symptoms of ASDwith symptoms of ASD
• Participants’ subjective ratings of the usefulness Participants’ subjective ratings of the usefulness of the booklet were very highof the booklet were very high
• ASDS screening measure may be an effective ASDS screening measure may be an effective early discriminator of long-term psychological early discriminator of long-term psychological difficulties in this populationdifficulties in this population

Discussion - Study 2Discussion - Study 2
Strengths of the studyStrengths of the study• Large sample sizeLarge sample size• Focus on highly symptomatic groupFocus on highly symptomatic group• Use of ‘optimal’ self-help bookletUse of ‘optimal’ self-help booklet
LimitationsLimitations• Reliance on self-report outcome measuresReliance on self-report outcome measures• Fairly low initial response rate and relatively high attrition Fairly low initial response rate and relatively high attrition • Lack of a ‘no assessment’ control groupLack of a ‘no assessment’ control group

Discussion - Study 3Discussion - Study 3
• No evidence obtained to support beneficial No evidence obtained to support beneficial effects of providing either self-help information or effects of providing either self-help information or in combination to “writing therapy” as an early in combination to “writing therapy” as an early intervention for traumatic injury survivors with intervention for traumatic injury survivors with symptoms of ASDsymptoms of ASD
• Participants’ subjective ratings of the usefulness Participants’ subjective ratings of the usefulness of the booklet and writing task were very high.of the booklet and writing task were very high.
• Was the “dose” of “writing” sufficient for PTSD?Was the “dose” of “writing” sufficient for PTSD?

DiscussionDiscussion
Clinical implicationsClinical implications• Self-help may not be effective in addition to Self-help may not be effective in addition to
natural recoverynatural recovery• But self-help information valued by majority but But self-help information valued by majority but
not all attenders.not all attenders.• May have other benefits not captured by May have other benefits not captured by
outcome measures?outcome measures?• Early self-help interventions may not be directly Early self-help interventions may not be directly
effective; but possible important role of self-help effective; but possible important role of self-help information in ‘watchful waiting’? NICE estimate information in ‘watchful waiting’? NICE estimate of 10 min follow-up appointment: £636kof 10 min follow-up appointment: £636k
• Potential usefulness of ASDS as screening toolPotential usefulness of ASDS as screening tool• Need to consider more potent interventions such Need to consider more potent interventions such
as brief CBT (Bisson et al, 2005).as brief CBT (Bisson et al, 2005).

DiscussionDiscussion
Future researchFuture research
• Ways of enhancing effectiveness of self-help Ways of enhancing effectiveness of self-help approaches - assisted self-help. approaches - assisted self-help.
• Computerised self-help and Internet-therapy?Computerised self-help and Internet-therapy?• Understanding the discrepancy between the Understanding the discrepancy between the
subjective usefulness of self-help interventions subjective usefulness of self-help interventions and objective outcome?and objective outcome?
• Effects of repeated assessments in aiding Effects of repeated assessments in aiding recovery?recovery?

Implications for guidelinesImplications for guidelines
Recommendations:Recommendations:10 A supportive context is offered 10 A supportive context is offered
that consists of: that consists of: • Offering a listening ear, Offering a listening ear,
support and solace and being support and solace and being open to the immediate open to the immediate practical needs of those practical needs of those affected,affected,
• Offering factual and up-to-date Offering factual and up-to-date information about the shocking information about the shocking event,event,
• Mobilising social support from Mobilising social support from their own social surroundings’their own social surroundings’
• Facilitating reuniting with Facilitating reuniting with people closest to them and people closest to them and keeping families together,keeping families together,
• Reassuring those affected Reassuring those affected who display normal stress who display normal stress reactions.reactions.
Relevance of the studies:Relevance of the studies:
• Studies demonstrate the Studies demonstrate the perceived usefulness of perceived usefulness of information provisioninformation provision
• Need to be careful about Need to be careful about sensitisation?sensitisation?
• However, context was However, context was individual trauma and not a individual trauma and not a disaster situationdisaster situation
• Practical information and Practical information and social disruption less relevantsocial disruption less relevant

Implications for guidelinesImplications for guidelines
Recommendations:Recommendations:11 Information is offered to all those 11 Information is offered to all those
effected. Information should effected. Information should consist of:consist of:• A reassuring explanation of A reassuring explanation of
normal reactions.normal reactions.• Saying when to seek help,Saying when to seek help,• Advising those affected to Advising those affected to
tackle the daily routine.tackle the daily routine.
12 The study group does not 12 The study group does not recommend offering preventive recommend offering preventive psycho- education.psycho- education.
Relevance of the studies:Relevance of the studies:
• How much information should How much information should be provided and for what be provided and for what purpose?purpose?
• A booklet maybe sufficient for A booklet maybe sufficient for normalisation and advice on normalisation and advice on help seeking?help seeking?
• Should we be attempting to Should we be attempting to introduce more effective introduce more effective forms of psycho-education for forms of psycho-education for target groups?target groups?
• Supported self-help and Supported self-help and internet access?internet access?

Thank youThank you