Providing controversial health care: Abortion services since 1973
6
Providing Controversial Health Care: Abortion Services Since 1973 Jacqueline Darroch Forrest, PhD Vice-President for Research Alan Guttmacher Institute New York, New York Stanley K. Henshaw, PhD Deputy Director of Research Alan Guttmacher Institute New York, New York O f the 6.4 million pregnancies that occur each year in the United States, more than half are unintended. This means that roughly 6% of US women age 15-44 have an unintended pregnancy each year. At current rates, a group of 100 women beginning their reproductive lives will have had 131 unintended pregnancies by the time they reach age 45. Not surprisingly, this results in an enormous demand for abor- tion services. Almost half of all unintended pregnancies in the United States end in induced abortion. At current rates, 100 women beginning their repro- ductive lives will have had 76 abortions by the time they reach 45, and almost half will have had at least one abortion. Nationally, this amounts to about 1.6 million abortions a year. When abortion was legalized nationally by Roe v Wade in 1973, it was expected that most of the demand for services would be met by hospitals, where most other surgery was performed. Most hospitals, however, preferred to leave it to others to provide this controversial service. In 1973 and the first quarter of 1974, only 1284 of the country's 5401 non-Catholic, short-term general hospitals provided any abortion services, and a fourth of these per- formed no more than five abortions during the first quarter of 1974.1 The number of hospitals offering abortion services increased gradually to a peak of 1687 in 1976 and has declined steadily since then to a 1988 figure of 1040 (see Figure 1). With hospitals in many areas unwilling to meet the need for abortion services, specialized abortion clinics became increasingly common. Experience in New York State, where abortion had been legalized in 1970, and in the District of Columbia proved that safe services could be provided in freestand- ing clinics, which became the model for the creation of clinics in all parts of the country. In addition, other nonhospital clinics added abortion to the services they offered, and some physicians began to provide the service in © 1993 by The Jacobs Institute of Women's Health 1049-3867/93/$6.00 152 FORREST AND HENSHAW: ABORTION SERVICES WHI Vol. 3, No. 3 Fall 1993
Transcript of Providing controversial health care: Abortion services since 1973

Providing Controversial Health Care: Abortion Services Since 1973 Jacqueline Darroch Forrest, PhD Vice-President for Research Alan Guttmacher Institute New York, New York
Stanley K. Henshaw, PhD Deputy Director of Research Alan Guttmacher Institute New York, New York
O f the 6.4 million pregnancies that occur each year in the United States, more than half are unintended. This means that roughly 6% of US women age 15-44 have an unintended pregnancy each year. At current rates, a group of 100 women beginning their
reproductive lives will have had 131 unintended pregnancies by the time they reach age 45. Not surprisingly, this results in an enormous demand for abor- tion services. Almost half of all unintended pregnancies in the United States end in induced abortion. At current rates, 100 women beginning their repro- ductive lives will have had 76 abortions by the time they reach 45, and almost half will have had at least one abortion. Nationally, this amounts to about 1.6 million abortions a year.
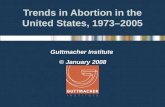
When abortion was legalized nationally by Roe v Wade in 1973, it was expected that most of the demand for services would be met by hospitals, where most other surgery was performed. Most hospitals, however, preferred to leave it to others to provide this controversial service. In 1973 and the first quarter of 1974, only 1284 of the country's 5401 non-Catholic, short-term general hospitals provided any abortion services, and a fourth of these per- formed no more than five abortions during the first quarter of 1974.1 The number of hospitals offering abortion services increased gradually to a peak of 1687 in 1976 and has declined steadily since then to a 1988 figure of 1040 (see Figure 1).
With hospitals in many areas unwilling to meet the need for abortion services, specialized abortion clinics became increasingly common. Experience in New York State, where abortion had been legalized in 1970, and in the District of Columbia proved that safe services could be provided in freestand- ing clinics, which became the model for the creation of clinics in all parts of the country. In addition, other nonhospital clinics added abortion to the services they offered, and some physicians began to provide the service in
© 1993 by The Jacobs Institute of Women ' s Health 1049-3867/93/$6.00
152 FORREST AND HENSHAW: ABORTION SERVICES WHI Vol. 3, No. 3 Fall 1993

2000, - - - - i
1500 I i , T I
1000 ~-
500 t ÷
0 '1973 '74
~ J
! - - I ~ J I I
'75 '76 '77 '78 '79 '80 '81 '82 '84 '85 '87 '88
Hospital - - - Nonhospital
Figure 1. Number of Abortion Pro- viders, by Type, 1973-1988. (Source: Henshaw SK, Van Vort j,7 pp. 190- 1.)
their private offices. The number of such nonhospi ta l providers increased to about 1500 in 1981 and has remained at about that level.
Similarly, the percentage of abortions provided in nonhospi ta l facilities increased sharply dur ing the 1970s and has cont inued to increase up to the present (see Figure 2). The percentage in physicians' offices where small numbers are per formed (fewer than 400 a year; physicians' offices providing more than 400 abortions are def ined here as clinics) has remained stable at about 4%. The percentage in specialized abortion clinics, on the other hand, has g rown over time to 60% in 1985 and 64% in 1988. Another 22% occur in other clinics where abort ion patients represent fewer than half of all the visits.
Al though there are some 2600 providers in all, the bulk of abortions are concentrated in a small propor t ion of the facilities. Most of the providers who do abortions in the United States do very few each year; about a quarter provide fewer than 30. Eighty percent of women receive their abortions from
100%
80%
60%
40%
20%
0% 1973 '74 '75 '76 '77 '78 '79 '80 '81 '82 '84 '85 '87 '88
YEAR
Hospitals ~ Clinics ~ MD of f ices
Figure 2. Percentage Distribution of Abortions by Type of Facility, 1973- 1988. (Source: Henshaw SK, Van Vort j.6).
WHI Vol. 3, No. 3 Fall 1993 FORREST AND HENSHAW: ABORTION SERVICES 153

Table 1. SITE OF ABORTION SERVICES
Weeks LMP Percent Outside a Hospital
<13 92 13-14 83 15-16 72 17-18 61 19-20 57 >20 60
LMP, last menstrual period.
the 20% of all providers that provide at least 1000 abortions each year. There are only about 500 such providers, but these serve the overwhelming majority of patients, whereas most facilities, especially the hospitals and small private physician offices where abortion is performed, are relatively small providers.
In part because of the reluctance of hospitals to offer abortion services and in part to increase their business, many abortion clinics have expanded their services to include middle and late second-trimester procedures. In 1985, 32% of abortion clinics offered services as late as 17 weeks from the last menstrual period (LMP); this percentage increased to 40% in 1988. Most sec- ond-trimester procedures are now performed outside of hospitals. A special tabulation of data compiled by the National Center for Health Statistics on 296,000 abortions performed in 14 states in 1988 shows that even at 20 weeks LMP or later, 60% of abortions are performed in clinics or doctor's offices (Table 1).
The safety record of abortion services, including the nonhospital facilities, has been excellent. Between 1980 and 1987, there were only 0.6 deaths re- ported by the Centers for Disease Control and Prevention 2 per 100,000 abor- tions. Mortality has been found to be no higher in nonhospital facilities than in hospitals. 3 Major complications are also uncommon. Statistics compiled by the National Abortion Federation for 1992 indicated that complications re- quiring hospitalization occurred in 0.32% of abortions with follow-up infor- mation, or 0.11% of all abortions. 4 If one assumes that almost all serious complications would be known to the providers, the lower figure would be the more accurate.
Even with the growth of nonhospital abortion services, there are serious problems of access for many women. Of all women aged 15-44, 31% live in counties with no abortion provider, and an additional 11% live in counties with only a small provider that reported fewer than 400 abortions in 1988. Providers of fewer than 400 abortions are unlikely to advertise or to be listed in the yellow pages. Providers who do two or three abortions a year, or even 10-20, may well do them only for existing private patients, may not offer services to new patients, or may not be visible enough in the community for women to find them readily.
The scarcity of providers means that many women who have abortions have to travel to find services. In 1988, 6% of women having abortions went outside their home state to do so, and approximately 33% traveled to another county within their home state. In 12 states, 20% or more of the women having abortions went to other states for services. An estimated 9% of women travel more than 100 miles for abortions, and 18% travel 50-100 miles, s
Abortion providers are concentrated in large metropolitan areas, and 98% of abortions occur in metropolitan counties. Only 17% of nonmetropolitan women live in a county with a provider. Even some of the smaller metropolitan areas have inadequate services. In 1988, there were 70 standard metropolitan
154 FORREST AND HENSHAW: ABORTION SERVICES WHI Vol. 3, No. 3 Fall 1993

statistical areas with no abortion provider and an additional 20 areas with no facility that served as many as 50 women seeking abortions. 6
There is evidence that the shortage of abortion providers has been in- creasing in recent years. The number of metropolitan areas with few or no services increased from 81 in 1985 to 90 in 1988. The number of providers in nonmetropolitan counties has fallen from a peak of 555 in 1978 to 271 in 1988. 7 Two states, North and South Dakota, now have only one provider; the clinic in North Dakota must fly in physicians from other states to provide services. Clinics have found it increasingly difficult to find physicians to perform abor- tions, and it is not uncommon for physicians to be flown in from other states.
One of the remaining public health concerns about legal abortion is that 11% of abortions are performed during the second trimester, including 4% after 15 weeks LMP. Although abortions even up to about 20 weeks LMP are safer than childbearing, the risk of mortality and complications increases with gestational age. One of the reasons women are delayed is the absence of any abortion service in many areas. A survey of women having abortions after 15 weeks LMP found that for almost half, a reason for the delay or lateness in getting an abortion was a problem in arranging for the abortion; about a third had problems in terms of fear of telling their partners or their parents; a quarter needed the extra time to make the decision. Seventy-one percent, the largest proportion, said that they were late in recognizing the pregnancy or in realizing how advanced it was.
Further information was collected on why women found it hard to ar- range for an abortion: They needed time to raise the money; they tried to get an abortion from a different physician or clinic, maybe from a physician who would not perform it, from a clinic whose cost was too high, or from a clinic with a gestational limit below the stage of pregnancy; they had difficulty arranging transportation because there was no provider nearby; they didn't know where to get an abortion; they couldn't get an appointment earlier; or they had to take extra time to notify or get consent of parents or make ar- rangements, to get child care, or, in states where abortions are funded through the state Medicaid system, to get a Medicaid card to pay for the abortion. The 71% of the women who said that they were late in recognizing their pregnancy gave the following types of reasons: They didn't think they were pregnant; they didn't feel physical changes; they were hoping that they weren't pregnant or that their period would come; their periods were irregular and therefore they had difficulty knowing whether they were late or not; they had some spotting or bleeding and thought that they had had their period; they'd seen a physician who had underestimated the gestation of the preg- nancy; they were practicing contraception and had no idea or no expectation that they would become pregnant; or that they had a pregnancy test that was negative, but they had difficulty knowing how and where to get another pregnancy test. 8
One reason for the scarcity of abortion services is that many physicians have personal reasons for not wanting to perform the procedure. A 1983 survey of a national random sample of obstetrician-gynecologists in private practice found that 42% did perform at least some abortions in their offices, in a hospital, or in a clinic. Forty-one percent, which is about 70% of the total who didn't perform abortions, said they did not perform abortions because of moral or religious reasons. About 30% had other reasons, such as that the hospital with which they were affiliated did not allow abortions, they had little demand among their patients, a partner in their group did abortions, they did no surgery, or they weren't trained. 9
Since 1983, harassment by antiabortion activists may have become a more prominent reason for physicians and other health care providers to avoid performing abortions. Among nonhospital facilities that performed 400 or
WHI Vol. 3, No. 3 Fall 1993 FORREST AND HENSHAW: ABORTION SERVICES 155

more abortions a year, 81% reported having been picketed by antiabortion groups in 1988, 46% had experienced picketing with physical contact or block- ing of patients, 38% had demonstrations resulting in arrests, 36% had bomb threats, 34% had vandalism, and 17% had picketing of the homes of staff members. The amount of vandalism increased between 1985 and 1988, whereas bomb threats decreased in frequency, s
Another possible reason for declining interest in providing abortion ser- vices is the relatively low level of remuneration. In 1989, women paid on average $251 for a first-trimester abortion with local anesthesia. In 1976, the same abortion cost $165, but when the inflation in medical care costs is taken into account, the 1976 charge represented $474 in 1989 dollars. In 1973, phy- sicians were generally paid on the order of $50 per procedure when they performed abortions in clinics; today they are paid about the same amount, although a dollar is worth only about a third as much in purchasing power. These trends indicate a sharply reduced financial incentive to perform abor- tions.
For women, on the other hand, although reduced fees bring abortion within reach for more women, cost is still a barrier for many. Only 13 states now pay for abortions for a significant number of low-income women. At $250, an abortion equals more than half the $400 a month received by a woman on Aid for Families with Dependent Children. The fees for abortion are higher for women who seek services during the second trimester, reaching over $900 at 20 weeks LMP. A study of the effects of the cutoff of Medicaid funding for abortion in 1978 found that about 80% of the women who would have had Medicaid abortions either miscarried or found a way to pay for a private abortion, whereas about 20% carried their pregnancies to term.l° Clinics are therefore caught in a dilemma: To increase the incentive for physicians to perform abortions, they would have to raise prices, but this would make it more difficult for some women to use the services.
Looking to the future, several issues face the abortion service system other than the continuing problem of antiabortion harassment. First, lack of financing for low-income women is perhaps the most damaging of the legal restrictions on abortion that are now in effect. A federal policy to include abortion services in Medicaid coverage is the most important measure that could be taken to improve access to services. Short of that, the resumption of Medicaid funding by as many states as possible would be helpful.
A related issue is the way abortion services will be treated in any future national health insurance program. If they are included in the basic benefit package, access will be improved for the many low-income women who are not now covered by public or private insurance. Even if universal coverage is provided, however, bureaucratic barriers could still make it difficult to utilize the insurance. At present, many women with insurance prefer to self- pay rather than make a claim against their insurance or seek services through a health maintenance organization; this is evidently because of concerns about possible delay and loss of confidentiality caused by the procedures established by insurance companies and employers for obtaining reimbursement. It is important that the universal insurance plan be structured to minimize the need for referral, approval, or screening for a woman seeking abortion ser- vices.
Another issue is the increasing number of restrictions on women seeking abortions and on abortion providers. These include informed consent re- quirements that specify information that must be provided to patients, waiting periods, facility licensing requirements, Occupational Safety and Health Administration (OSHA) regulations, regulations relating to laboratory tests, fetal-tissue disposal requirements, and zoning ordinances, among others. Many of these restrictions make it more expensive and difficult to provide
156 FORREST AND HENSHAW: ABORTION SERVICES WHI Vol. 3, No. 3 Fall 1993

abort ion services. Because small facilities m a y not be able to afford or justify the cost of comply ing with all these requi rements , a likely effect is to p romo te a cont inuat ion of the t rend toward larger clinics that pe r fo rm an increasing propor t ion of all abort ions. This m a y have an adverse effect on the availability of services in smaller cities and areas that are at p resen t served only by facilities that pe r fo rm only a small n u m b e r of abort ions.
REFERENCES
1. Weinstock E, Tietze C, Jaffe FS, Dryfoos J. Legal abortions in the United States since the 1973 Supreme Court decisions. Fam Plann Perspect 1975;7:23-31.
2. Koonin LM, Smith JC, Ramick M, Lawson HW. Abortion surveillance--United States, 1989. MMWR CDC Surveill Summ 1992;41(SS-5):1-33.
3. Grimes DA, Cares W Jr, Selik RM. Abortion facilities and the risk of death. Fam Plann Perspect 1981;13:30-2.
4. National Abortion Federation. Summary of annual complication statistics, 1992. Washington, DC: NAF, 1993.
5. Henshaw SK. The accessibility of abortion services in the United States. Fam Plann Perspect 1991;23:246-52, 263.
6. Henshaw SK, Van Vort J. Abortion services in the United States, 1987 and 1988. Fam Plann Perspect 1990;22:102-8, 142.
7. Henshaw SK, Van Vort J, editors. Abortion factbook, 1992 edition: Readings, trends, and state and local data to 1988. New York: The Alan Guttmacher Institute, 1992:182-3.
8. Torres A, Forrest JD. Why do women have abortions? Fam Plann Perspect 1988;20:169-76.
9. Orr MT, Forrest JD. The availability of reproductive health services from US private physicians. Fam Plann Perspect 1985;17:63-9.
10. Trussell J, Menken J, Lindheim BL, Vaughan B. The impact of restricting Medicaid financing for abortion. Fam Plann Perspect 1980;12:120-30.
WHI Vol. 3, No. 3 Fall 1993 FORREST AND HENSHAW: ABORTION SERVICES 157