
· PDF fileACLS protocol performed for 10 minutes then patient ... ACS Principles & Practice...
54
Lya Crichlow, MD Kings County Hospital Center Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference www.downstatesurgery.org
Transcript of · PDF fileACLS protocol performed for 10 minutes then patient ... ACS Principles & Practice...

Lya Crichlow, MDKings County Hospital CenterKings County Hospital Center
September 3, 2009Morbidity and Mortality Conference
www.downstatesurgery.org
Case presentation56 year old male who presented with 1 week history of dysphagiaU bl l lid b bl l f di Unable to tolerate solids but able to tolerate soft diet and liquidsPMHx: DeniesPMHx: DeniesPSHx: L humeral ORIFMeds: NoneMeds: None
www.downstatesurgery.org

Case presentationSocial Hx
40 pack year smoking historyAlcohol abuse (1 pint of vodka per day/10 years)
Review of systems: d i ht l k10 pound weight loss over 2 weeks
Physical exam:CacheticCacheticNo diffuse lymphadenopathy
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

Case PresentationCT chest 6/12/09
Marked thickening of the middle third of the esophagus with distension of the esophagus proximal to this pointdistension of the esophagus proximal to this pointR hilar lymph node approximately 10 mm
EGD 6/16/09Large ulcerated, circumferential, partially obstructing mass at 28 cm from the gums, extending for approximately 6 cmStomach and duodenum were unremarkableStomach and duodenum were unremarkableUnable to pass adult scope due to stricturePathology
Moderately differentiated squamous cell carcinoma
www.downstatesurgery.org

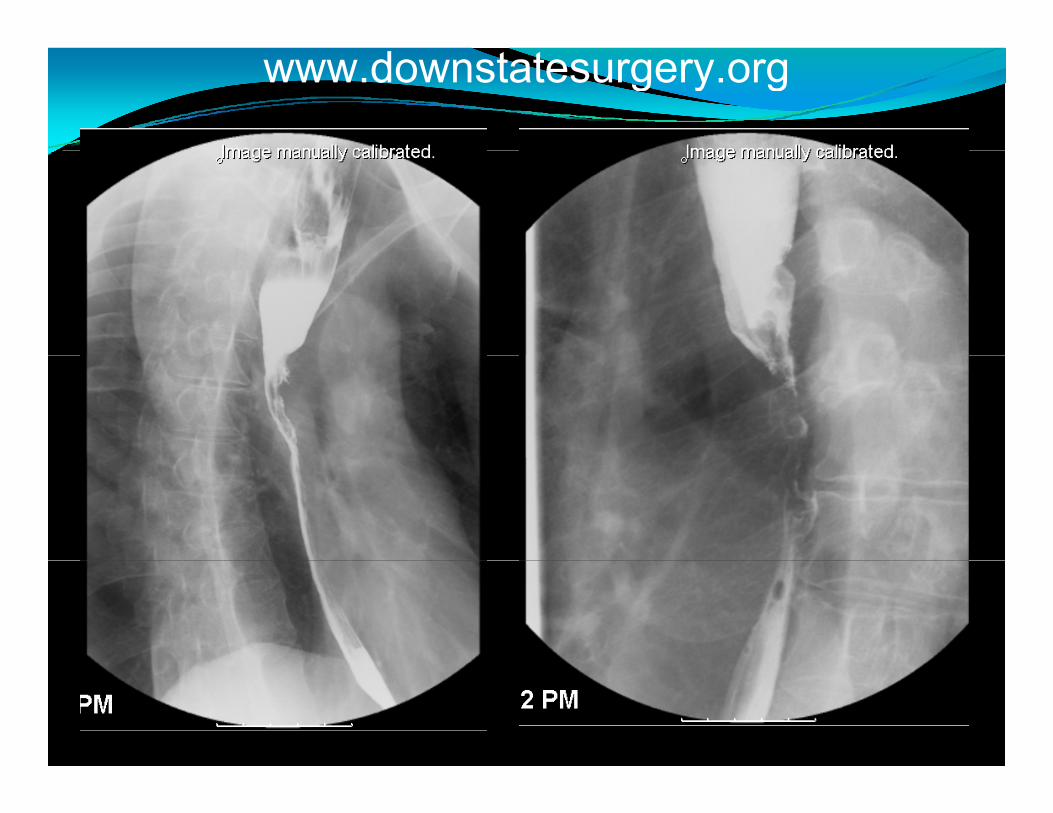
Case PresentationBarium swallow 6/15/2009
Infiltrating lesion midthoracic esophagus approximately i l th t di j t b l i9 cm in length extending just below carina
Tight stricture at central portion of the lesion, <5mm at most narrow pointp
www.downstatesurgery.org
www.downstatesurgery.org

Case PresentationPET SCAN 6/19/09
Neoplastic range metabolic FDG uptake in middle third f th h (SUV 6 )of the esophagus (SUV 16.4)
Pulmonary Function testsFEV1 66 % of normalFEV1 ‐ 66 % of normalABG – 7.42/42/93/27/98%/3.1
www.downstatesurgery.org

www.downstatesurgery.org

SurgeryProcedure 6/25/09
BronchoscopyLaparotomySplenectomyPyloroplastyPyloroplastyFeeding jejunostomyRight thoracotomyRight thoracotomyEsophagectomyLeft neck explorationpCervical esophagogastric anastamosis
www.downstatesurgery.org

Pathology4 x 2.5 cm fungating mass invading muscular wallModerately differentiated squamous cell carcinomaNegative margins8 lymph nodes negative for tumorStage T2NOMx
www.downstatesurgery.org

Postoperative CoursePOD # 4: Remained mechanically ventilated, febrile to 102. Bilateral pleural effusionsPOD S i h k F b il POD # 5: Septic shock. Febrile to 103.5POD # 5: CT chest/abdomen/pelvis
Bil t l iBilateral pneumoniaNo evidence of abscess in abdomen/pelvis
www.downstatesurgery.org

www.downstatesurgery.org
PostOperative CourseSputum culture from POD # 5: Hemophilus parainfluenzaePOD B i ll N id f l kPOD # 6: Barium swallow: No evidence of leak
www.downstatesurgery.org

www.downstatesurgery.org

Postoperative CourseSputum culture from POD # 5: Hemophilus parainfluenzaePOD B i ll N id f l kPOD # 6: Barium swallow: No evidence of leakPOD # 18: TracheostomyPOD # B d di i f ll di POD # 29: Bradycardia progressing to full cardiac arrest. ACLS protocol performed for 10 minutes then patient was resuscitated. Responsive to painful patient was resuscitated. Responsive to painful stimuli
www.downstatesurgery.org

Postoperative CoursePOD # 29: Pt witnessed to have seizure activity after the code. Head CT showed no acute pathologyPOD R h d CT Diff l i jPOD # 35: Repeat head CT: Diffuse axonal injuryNeurology consulted. EEG performed showing no correlation between disorganized movements correlation between disorganized movements therefore no evidence of seizure activityUnable to control movements with benzodiazapenes, Unable to control movements with benzodiazapenes, clonopin or depakotePOD # 67: Discharge to skilled nursing facility
www.downstatesurgery.org

www.downstatesurgery.org
EpidemiologyIncidence in the United States is 20 per 100, 000Worldwide incidence: 160 per 100, 0002008: ~ 14, 300 deaths2 major histological types:
Squamous cell carcinomaAdenocarcinoma
www.downstatesurgery.org

SQUAMOUS CELL SQUAMOUS CELL CARCINOMA ADENOCARCINOMA
70 % found in upper & iddl / d f h
Distal 1/3rd and at the GE j imiddle 1/3rd of esophagus
Most common form of esophageal cancer worldwide
junctionMost common subtype in the US and Western worldg
Risk factorsSmokingAlcohol
Risk factorsBarrett’s esophagusGERDAlcohol
Food additives egnitrosamines (smoked food)
GERDObesity
www.downstatesurgery.org

PresentationAsymptomaticDysphagia especially to solids (60 % of the lumen
b l d d)must be occluded)Retrosternal painD d l i kDecreased parenteral intakeWeight lossHHoarsenessAspiration pneumonia
www.downstatesurgery.org

DiagnosisEsophagram
Recommended for any patient presenting with d h idysphagiaDifferentiate intramural vs intraluminal lesionsDifferentiate intrinsic vs extrinsic compressionDifferentiate intrinsic vs extrinsic compression
EndoscopyVisualize the lesionsua e t e es oLocationBiopsy
www.downstatesurgery.org

Staging2 Classification systems exist:
TNM systemd hT – tumor depth
N – Involvement of regional lymph nodesM – Disease to nonregional lymph nodes & distant sitesg y p
WNM system (Ellis system)W – Wall penetrationN – number of positive lymph nodesM – Distant disease
www.downstatesurgery.org

TNM staging
Townsend: Sabiston Textbook of Surgery 18th Edition 2007
www.downstatesurgery.org

Comparison of TNM & WNM pstaging systems
Townsend: Sabiston Textbook of Surgery 18th Edition 2007
www.downstatesurgery.org

Staging: CTChest/Abdomen/Pelvis
Length of the tumorEsophageal thickness and thickness of the stomachEsophageal thickness and thickness of the stomachRegional lymph node statusDistant metastasis
www.downstatesurgery.org

Staging: PET scanUptake of fluorodeoxyglucoseEvaluate primary mass, regional lymph nodes and di didistant diseaseDetection of metastatic disease: Sensitivity 88 %, Specificity 93 %Specificity 93 %Rizk et al 2006 examined if SUV levels can predict survival after esophagectomy. Pts with SUV < 4.5 more survival after esophagectomy. Pts with SUV < 4.5 more likely to have early stage disease and less lymph node involvement. Overall survival better than in high SUV group
www.downstatesurgery.org

Overall survival of all patientsOverall survival of all patients based on maximum SUV
ConclusionPET SUV could predict predict clinical/pathologic stage and overall survival in pts with esophageal cancer
Rizk et al Preoperative 18[F]-fluorodeoxyglucose positron emission tomograpy standardized uptake values predict survival after esophageal adenocarcinoma resection Ann Thorac Surg 2006: 81 (3) 1076 - 81
www.downstatesurgery.org

Staging: Endoscopic UltrasoundDetermine depth of tumorStatus of regional lymph nodes
Able to biopsy regional lymph nodesDisadvantage:
d Tends to overstage T statusUnderstage N status
Zuccaro et al 2006 compared EUS staging vs pathology Zuccaro et al 2006 compared EUS staging vs pathology after esophagectomy in 266 patients. T2 tumors only identified correctly in 42 % of patients by EUS, 54 % of y 4 p y , 54cases they were overstaged as T3
www.downstatesurgery.org

Townsend: Sabiston Textbook of Surgery 18th Edition 2007
www.downstatesurgery.org

History of esophageal resectionCzerny 1877 – 1st esophageal resection. Cervical tumorTorek 1911 – Resection of thoracic esophagus. Pt had
i l h & E l cervical esophagostomy & gastrostomy. External rubber tube connected the 2. Pt lived for 10 yearsTurner 1933 Transhiatal esophagectomyTurner 1933 – Transhiatal esophagectomyOshawa 1933 – Thoracic resection with anastomosisIvor Lewis 1946 Described Ivor Lewis esophagectomyIvor Lewis 1946 – Described Ivor Lewis esophagectomy
www.downstatesurgery.org

Surgical TherapyModified McKeown/Triincisional TechniqueTranshiatal EsophagectomyIvor‐Lewis EsophagectomyEn Bloc ResectionLeft thoracoabdominal approach
www.downstatesurgery.org

Transhiatal EsophagectomyBetter surgical option for patients with poor pulmonary function i.e. FEV1 < 800C i di iContraindications:
Severe CAD or valvular diseaseBulky tumors of midesophagus difficult to dissectBulky tumors of midesophagus difficult to dissect
www.downstatesurgery.org

Transhiatal Esophagectomy
ACS Principles & Practice of Surgery 2009
www.downstatesurgery.org

Transhiatal Esophagectomy
Selke: Sabiston & Spencer Surgery of the Chest; 7th Edition 2005
www.downstatesurgery.org

Transhiatal Esophagectomy
ACS Principles & Practice of Surgery 2009
www.downstatesurgery.org
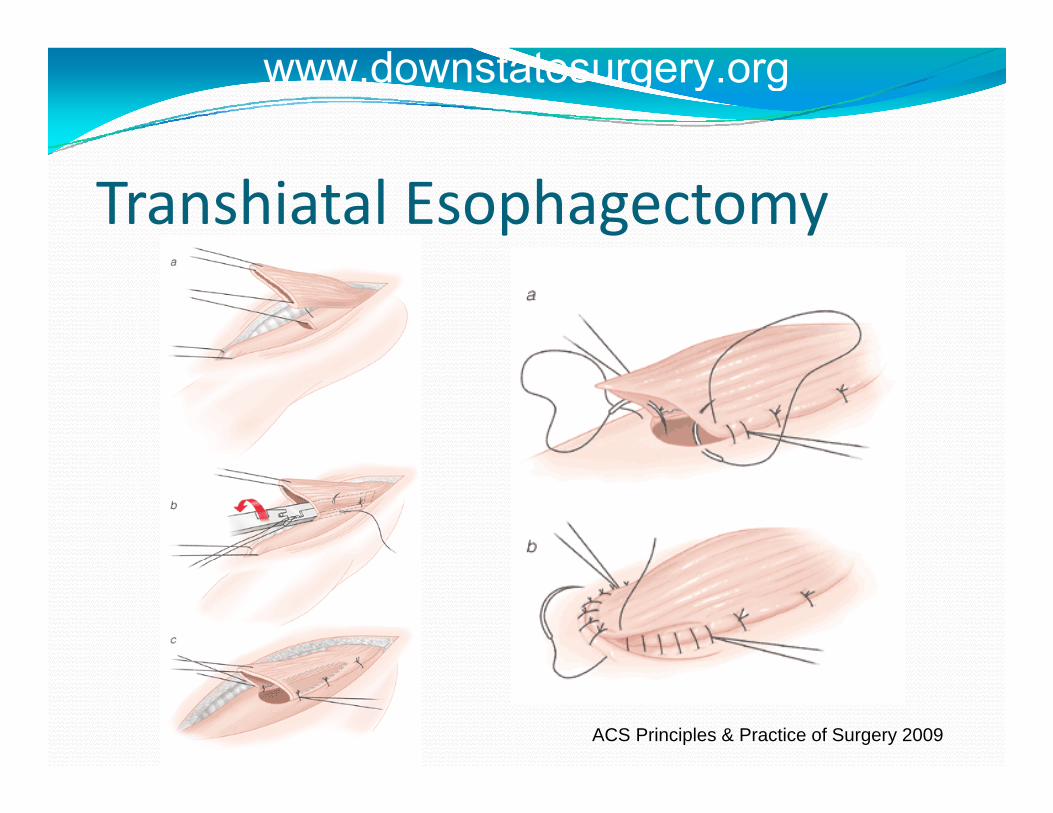
Transhiatal Esophagectomy
ACS Principles & Practice of Surgery 2009
www.downstatesurgery.org
Modified McKeown/TriincisionalModified McKeown/Triincisional Technique
Combination of Ivor‐Lewis and transhiatal approachesUseful for tumors at any level of the esophagusConsists of:
Laparotomy with construction of gastric neoesophagusRi h hRight thoracotomyCervical anastomosis
www.downstatesurgery.org

Ivor Lewis EsophagectomyContraindications
Tumors in upper 1/3rd of esophagusLong segment Barrett’s esophagus with extension into cervical esophagus
TechniqueTechniqueLaparotomyR thoracotomyR t o acoto yAnastomosis is made in the chest
www.downstatesurgery.org

Ivor‐Lewis Esophagectomy
ACS Principles & Practice of Surgery 2009
www.downstatesurgery.org
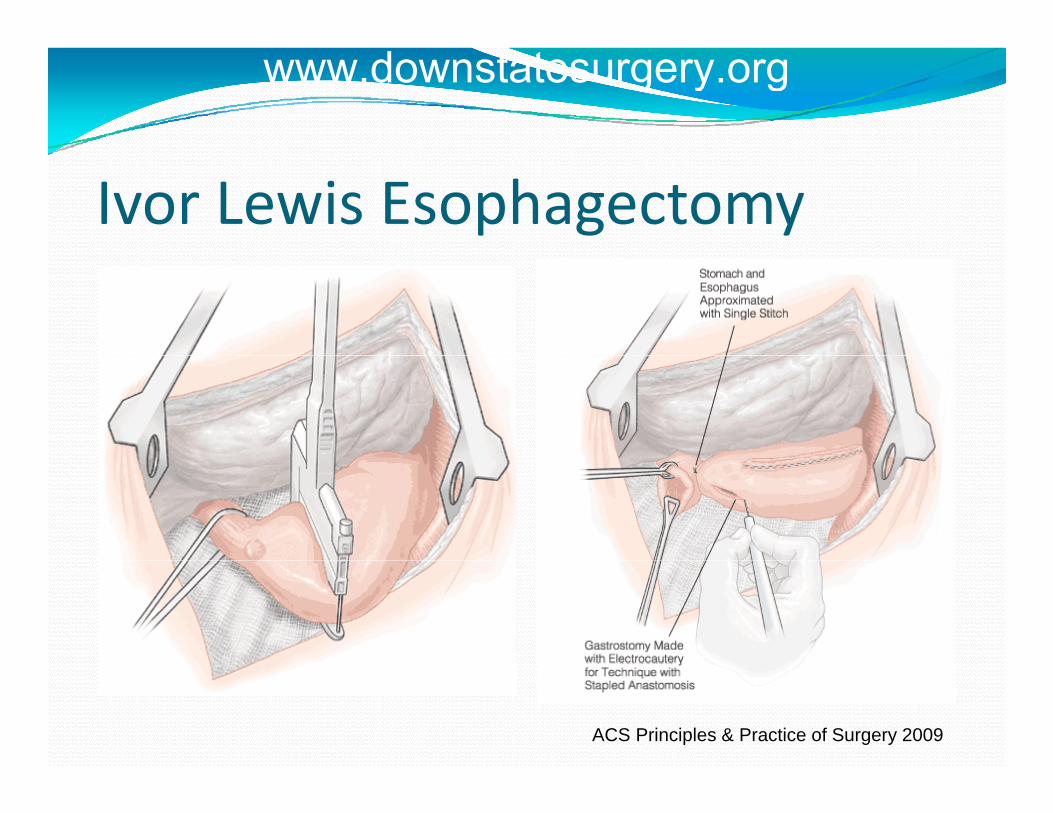
Ivor Lewis Esophagectomy
ACS Principles & Practice of Surgery 2009
www.downstatesurgery.org
En Bloc ResectionAdvocated by some surgeons as there are some studies which show removal of lymph nodes improves survival T h iTechnique
TriincisionalLigation of azygos hemiazygos intercostal veinsLigation of azygos, hemiazygos, intercostal veinsRemoval of mediastinal lymph nodesExcision of rim of diaphragmExcision of rim of diaphragmRemoval of paracardial, left gastric, portal, common hepatic, celiac, splenic lymph nodesCervical esophagogastric anastomosis
www.downstatesurgery.org
Complications of EsophagectomyMortality
Historically 15 – 40 %Experienced centers: 3 – 4 %Advances in ICU care have improved mortality significantlysignificantly
Anastomotic leakIvor‐Lewis: Mediastinitisvo e s: ed ast t sCervical leaks can be drained
www.downstatesurgery.org

Complications of EsophagectomyAnastomotic StrictureRecurrent Laryngeal Nerve InjuryRespiratory
Incidence reported 2 – 47 %hHemorrhage
Delayed emptying of the conduit
www.downstatesurgery.org
Chemotherapy & RadiationRadiation as a sole therapy mainly for poor sugicalcandidates or those in need of palliationRTOG dRTOG 85‐01 study
Randomized control trial over 5 yearsRadiation (64 Gy) vs radiation (50 Gy) plus Radiation (64 Gy) vs radiation (50 Gy) plus chemotherapy (cisplatin, fluorouracil)T1‐3N0 – 1M03At 5 years, survival for combination therapy group was 26 % vs 0 % for radiation alone
www.downstatesurgery.org

Does chemotherapy followed pyby surgery offer any benefit?
American Intergroup 0113 trialRandomized control studyCompared surgery alone vs preoperative chemotherapy followed by surgeryNo significant difference between 2 groups in terms of No significant difference between 2 groups in terms of survival
Meta‐analyses have shown a some survival benefit to preoperative chemotherapy
www.downstatesurgery.org

What is the role of chemoradiation?2 most important prognostic factors:
Tumor invasionLymph node metastasis
T stageCh di th f T l i b ( Chemoradiotherapy for T2 lesions or above (some surgeons advocate en bloc resection has as good results as chemoradiotherapy for T2 lesions)Chemoradiotherapy for any evidence of lymph node disease
www.downstatesurgery.org

ConclusionImprovements in surgical critical care, resection technique and multimodal therapy have improved the survival of esophageal cancersurvival of esophageal cancerSurgery remains a crucial element in the treatment of the diseasethe diseaseCurrent studies show that lymph node status and depth of tumor invasion are the most important p pprognostic factors
www.downstatesurgery.org

ReferencesRizk et al Preoperative 18[F]‐fluorodeoxyglucose positron emission tomograpy standardized uptake values predict survival after esophageal adenocarcinoma resection Ann Thorac Surg 2006: 81 (3) 1076 – 81Zuccaro et al Endoscopic ultrasound errors in esophageal caner Am J Gastroenterol 2005; 100 (3): 601 – 6Selke: Sabiston & Spencer Surgery of the Chest: 7th EditionTownsend: Sabiston Textbook of Surgery: 18th EditionTownsend: Sabiston Textbook of Surgery: 18 EditionCooper et al Chemoradiatotherapy of locally advanced esophageal cancer: long term follow‐up of a prospective randominzed trial (RTOG 85‐01). Radiation Therapy Oncology Group JAMA 1999; 281 (17): 1623 – 7Kelsen et al Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 1998; 339 (27): 1979 – 84D b t l M d S f E h l C G t t l Cli N A ( 8) 6 8Dubecz et al Modern Surgery for Esophageal Cancer Gastroenterol Clin N Am 37 (2008) 965 – 987Quiros et al Multidisciplinary Approach to Esophageal and Gastric Cancer Surg Clin N Am 89 (2009) 79 ‐ 96
www.downstatesurgery.org






![Resection and reconstruction of pelvic and extremity soft ......et al[2] describing the earliest initial series of en bloc resection of tumour with involved vascular structures. Although](https://static.fdocuments.us/doc/165x107/5e8302a97ac30b5c06610947/resection-and-reconstruction-of-pelvic-and-extremity-soft-et-al2-describing.jpg)










