
Protocol of Covid-19 for Yemen
14
1 | Page Prepared by Dr. Asia Al-Matari 1 Protocol of Covid-19 for Yemen Prepared by Dr. Asia Al-Matari Discussed with best internist (in and out- side of Yemen ) Date 26/05/2020 The purpose of the protocol is to assist physicians in management of patients with highly suspected or confirmed COVID-19 infection but in our situation because PCR test (not available for all suspected cases so, any case of fever and cough, sob ( see the score of covid 19) should be consider COVID-19 till prove otherwise , if fever only must first rule out other endemic causes like ( malaria and dengue, chikungunya or other source of infection either systemic or localized according to history and physical examination ). Those recommendations are based on case series, registered and observational trials on patients with MERS- CoV, SARS and COVID- 19 Strict infection control measures should be maintained all the time Important Notes: This protocol released after discussion with internal medicine consultants in Aden and outside of Yemen according to others protocols and this will be update in future according observation in our patients and update information of covid19 worldwide.
Transcript of Protocol of Covid-19 for Yemen
1 | P a g e
Prepared by Dr. Asia Al-Matari
1
Protocol of Covid-19 for Yemen
Prepared by Dr. Asia Al-Matari
Discussed with best internist (in and out- side of Yemen )
Date 26/05/2020
The purpose of the protocol is to assist physicians in management of patients with highly suspected or confirmed COVID-19 infection
but in our situation because PCR test (not available for all suspected cases so, any case of fever and cough, sob ( see the score of
covid 19) should be consider COVID-19 till prove otherwise , if fever only must first rule out other endemic causes like ( malaria and
dengue, chikungunya or other source of infection either systemic or localized according to history and physical examination ).
Those recommendations are based on case series, registered and observational trials on patients with MERS- CoV, SARS and COVID-
19
Strict infection control measures should be maintained all the time
Important Notes:
This protocol released after discussion with internal medicine consultants in Aden and outside of Yemen according to others
protocols and this will be update in future according observation in our patients and update information of covid19 worldwide.
2 | P a g e
Prepared by Dr. Asia Al-Matari
2
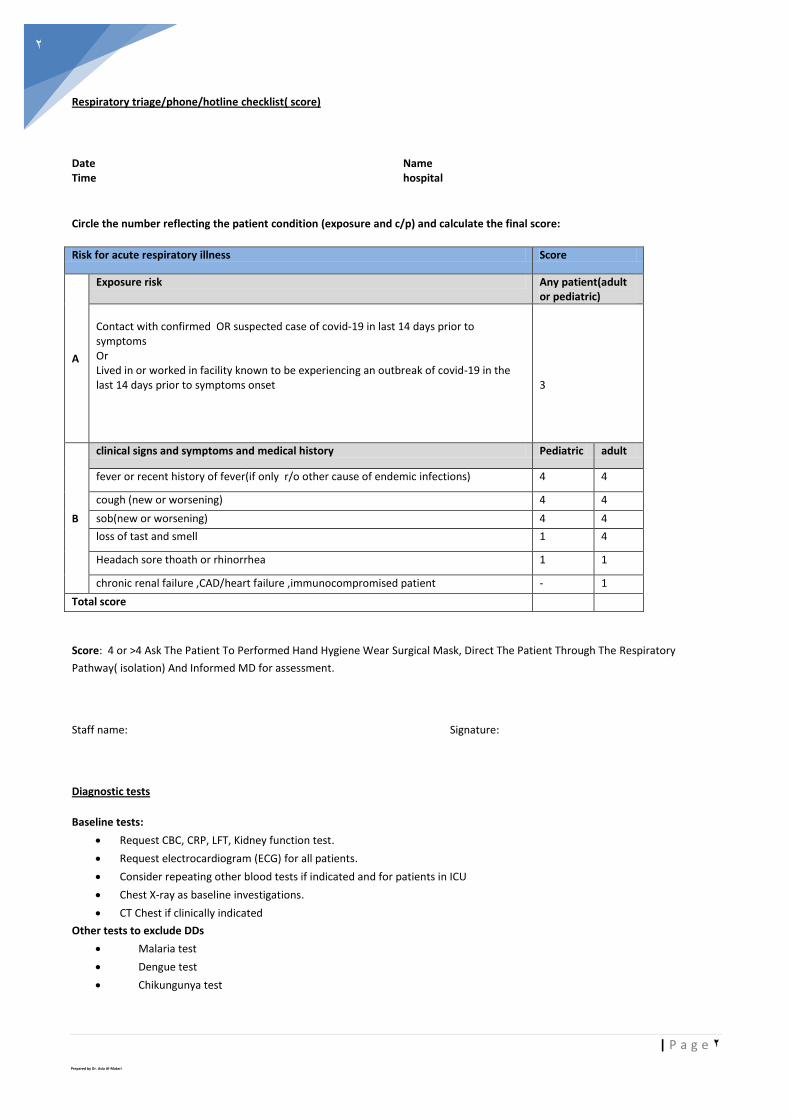
Respiratory triage/phone/hotline checklist( score)
Date Name Time hospital
Circle the number reflecting the patient condition (exposure and c/p) and calculate the final score:
Score Risk for acute respiratory illness
Any patient(adult or pediatric)
Exposure risk
A
3
Contact with confirmed OR suspected case of covid-19 in last 14 days prior to symptoms Or Lived in or worked in facility known to be experiencing an outbreak of covid-19 in the last 14 days prior to symptoms onset
adult Pediatric clinical signs and symptoms and medical history
B
4 4 fever or recent history of fever(if only r/o other cause of endemic infections)
4 4 cough (new or worsening)
4 4 sob(new or worsening)
4 1 loss of tast and smell
1 1 Headach sore thoath or rhinorrhea
1 - chronic renal failure ,CAD/heart failure ,immunocompromised patient
Total score
Score: 4 or >4 Ask The Patient To Performed Hand Hygiene Wear Surgical Mask, Direct The Patient Through The Respiratory
Pathway( isolation) And Informed MD for assessment.
Staff name: Signature:
Diagnostic tests
Baseline tests:
Request CBC, CRP, LFT, Kidney function test.
Request electrocardiogram (ECG) for all patients.
Consider repeating other blood tests if indicated and for patients in ICU
Chest X-ray as baseline investigations.
CT Chest if clinically indicated
Other tests to exclude DDs
Malaria test
Dengue test
Chikungunya test

3 | P a g e
Prepared by Dr. Asia Al-Matari
3
Others according to local epidemiological status
Specific test (especially in Moderate-Critical cases):
- D-Dimer
- CPK
- S. Ferritin
- LDH
- ABGs
- COVID-19 PCR according to case definition indication
- Any other test as clinically indicated or as per treating physician decision/request.
Note: Appropriate PPE should be applied during laboratory investigation (specimen collection and transport) performing ECG and radiological investigations
Risk for sever disease:
Presentations:
Asymptomatic
Nasopharyngeal RT- PCR positive for SARS CoV2 but having no symptoms (isolation for 14 days), but in our country not all case can be tested so any case suspected or has contact should by isolated. Mild:
LAB Vitals Risk factors
1. D-dimer > 1000 mg/L 2. CPK > twice ULN 3. CRP > 100 4. LDH > 245 U/L 5. Elevated troponin 6. Admission absolute
lymphocyte count < 0.8 7. Ferritin > 500 ug/L
1. Respiratory rate > 24 breaths/min
2. Heart rate > 125 beats/min 3. SpO2 ≤ 93% on ambient air 4. 4. PaO2/FiO2 < 300 mmHg
1. Older adults Age > 55
2. Patients of all ages with underlying medical
conditions, particularly if not well controlled,
including:
2.1. Patients with chronic lung disease or
2.2. moderate to severe asthma
2.3. Patients who have serious heart conditions
2.4. Diabetes with HbA1c > 7.6%
2.5. History of hypertension
2.6. Patients with chronic kidney disease undergoing
dialysis
2.7. Patients with liver disease
3. immunocompromised patients, including cancer
treatment, smoking, bone marrow or organ
transplantation, immune deficiencies, poorly
controlled HIV or AIDS, and prolonged use of
corticosteroids and other immunosuppressant's
4. Obese patients (body mass index [BMI] of 30 or
higher))

4 | P a g e
Prepared by Dr. Asia Al-Matari
4
Presence of symptoms as fever, fatigue, cough (with or without sputum production), anorexia, malaise, muscle pain, sore throat,
dyspnea, nasal congestion, Loss of tast and smell or headache without any hemodynamic compromise, without need for oxygen
findings or chest xray findings.
Treatment of Mild cases
Isolation for 14 day
Rule out Infections eg malaria. Chikungunya , dengue ) check for and treat for possible of confections)
No antibiotic or investigation or investigonal covid drugs and give symptomatic treatment.
Symptomatic treatment:
1)Paracetamol 500mg _1000 mg po/iv tid prn
2)Vitamin supplement
A) Vitamin c oral daily /zinc ( dose 500 -1000mg daily and zinc 75-100mg /daily)Bid (dose according to available dose)
B) vitamin D3 (D3/ca 500mg/200 is or 600/400mg.Bid ( dose according to available dose )
If you will give 5 0.000 I u weekly dose tablets or cap (must do 25-hydroxycalciferol in blood (I think no suitable to do it in this time)
Mostly in Aden pat very poor and socioeconomic issue
3)Increase fluid intake: (water/ lemon juice and Ginger juice and honey) 4)Close monitoring: if any developed sever symptoms or risk factor of sever disease Monitoring oxygen level by oxiymetri, if any sob or decrease spo2 chest x-ray 5)NO role of chloroquin or hydroxychoroquin. 6) Monitoring oxygen level by oximetry and vital signs ( see pluse oximetry monitoring below ) 7) Educate patient on Home isolation: if any deterioration signs and symptoms to seek health advice.
Instruction for Home isolation: (should be explained by treating physician or caregiver clearly to family members)
Stay at home in a separate room to other family members, preferably one with an en-suite bathroom, and ensure proper
and regular ventilation
Avoid any direct contact with other family members
Don’t allow visitors into your house
Use your phone if you need to contact anyone else in the house
Ask others a family member or friend - to run errands for you like buying food or medicine
You must not leave your house. In the event of a medical emergency call Emergency hotline numbers.
Only one member of the family should be allowed to provide care to you.
Your caregiver should wear a facemask and gloves every time he or she enters your room and should dispose of the mask
and gloves and wash their hands immediately after leaving the room .
Discontinuation of home isolation should be discussed with your caregiver (usually after 2 weeks if no test done )
A distance of at least one-two meter shall always be maintained between you and your caregiver.
Moderate: (CURB-65 score 1-2)
Hypoxia (oxygen saturation ≤ 94%).Persistent high-grade fever for over 3 dayor mild infiltrate on chest x-ray.Patient with
moderate disease do not generally require hospital intervention they can managed in community with isolation and can treated as
below.
Treatment of Moderate Cases
1)If patient with high risk factors )for admission to hospital, if not for home isolation (see Instruction for Home isolation)
2) Check and treat for possible of confections like (malaria , dengue , Chikungunya fever or other infections) .
3) Antipyretic :

5 | P a g e
Prepared by Dr. Asia Al-Matari
5
Paractamol 500m- 1000 q6 hrs po or iv),
NSAID: recommended that there be no difference in use of antipyretic strategies eg acetaminophen or NSAID),but if
patient on NSAID for other comorbidities continue therapy
4)Vitamin Supplement:
Vitamin c oral daily /zinc ( dose 500 mg daily and zinc 75-100mg /daily) ( dose can used available dose )
vit D3 supportive treatment: you can give it with D3/Ca 500mg/200 is or 600/400 ))dose can be use available dose )
If you will give 50 .000 I u weekly dose tablets or cap, do 25-hydroxycalciferol in blood ( so no suitable to do it in this time)
5)Anticough:( anti cough contained with codine ,honey )
6)Increase fluid intake: (water/ lemon juice and Ginger juice and honey) if can't take orally ivf
7)Close monitoring of oxygen saturation using pluse oximetry

6 | P a g e
Prepared by Dr. Asia Al-Matari
6
8)Antibiotic:
Doxycycline:((preferred )) start with 200mg day 1 then 100mg po bid for 5-7 days
or clarithromycin 500mg bid OR
azithromycin 500mg po daily for 5 day ,plus amoxicillin/clavulante or other oral penecillins
If physician need to add iv antibiotic for this patient this depending to the assessment (preferred method)
In patient with comorbidities can use levofloxacin 750 mg(respiratory dose) plus daily or amoxicillin/clavulanat 1 g bid for 5-7days
or ceftriaxone 1-2 g daily or q12hrs cefpodoxime 200mg po bid or cefuroxime 500mg po bid
Note:
(Choosing antibiotic also take account of local antimicrobial resistance data and other factors as their availability and physician
assessment according to his patient) ,after given it ,reviewed antibiotic every 2-3 day and if no improvement or there are culture
and sensitivity result modifying it accordingly
9)Antiviral: consider to use it ( triple combination)for 14 days
10)Hydroxychlorquin/chloruquin DO NOT USE IT
( Not preferable protocol as WHO recommendation against to use it)
11)Oseltamavir (Tamiflu) Controversial) no role if not associated with H1N1 but because no virology test and no pcr for rule out
other virus can be use if indicated (dose 75 mg bid for 5day po).
Steroid :Do not routinely give steroids ,at this time there is no robust evidence that corticosteroid are useful for covid19. If the
patient is on long term oral steroid for another indication there is no reason to stop the treatment .
12)Statin : recommend against use statins for treatment of covid 19 patient ,but if the patient on statin for other comorbidities
continue therapy
13)ACE inhibitors or ARBs be continued in people who have an indication for these medications. We do not currently routinely
recommend stopping these agents Treatment of co-morbidities if identified eg ( DM and HTN)
14)Monitoring oxygen level by oximetry and vital signs regularly.
15)Anticoagulant:
A) patient has no risk factors and active, oxymetri and d-dimer is no need OR prophylactic dose .
B)mandatory for patient with risk factors of VTE , high level of d-dimer or abnormal spo2 need anticoagulant
C)Any in patient also need anticoagulant ( in patient floor prophylactic dose or therapeutic dose depending on D-dimer level if
available ,otherwise you can give if no contraindications.
7 | P a g e
Prepared by Dr. Asia Al-Matari
7
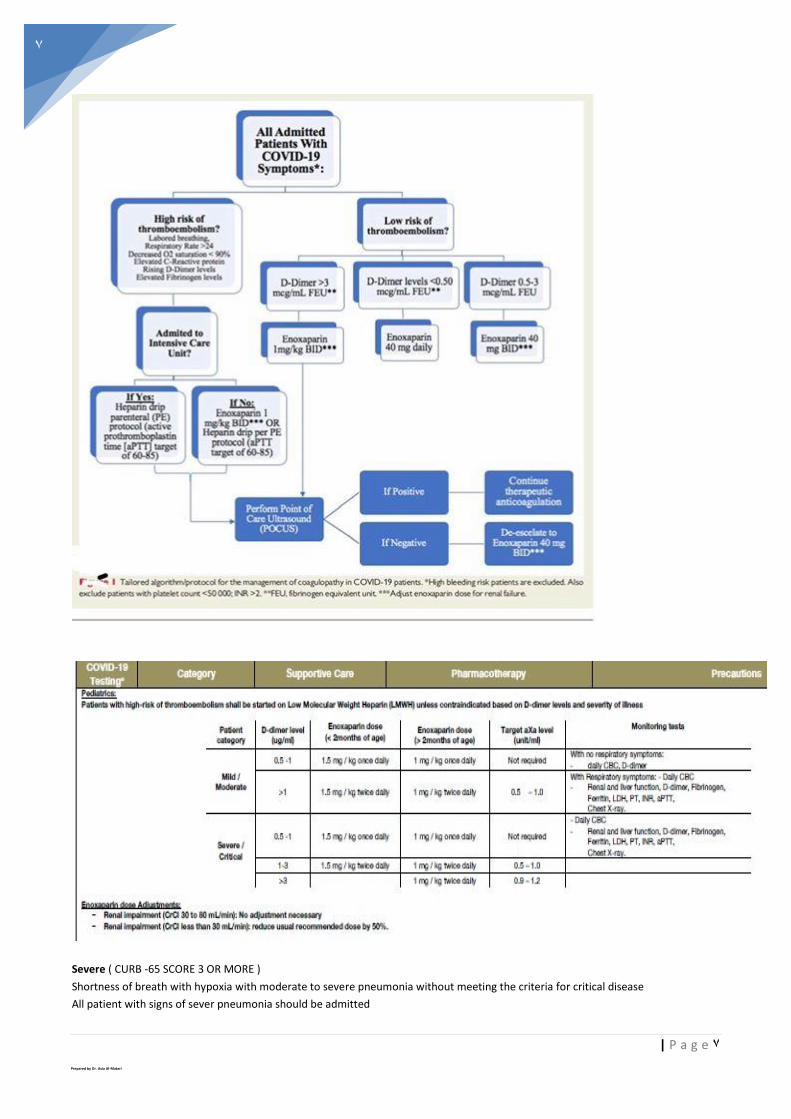
Severe ( CURB -65 SCORE 3 OR MORE )
Shortness of breath with hypoxia with moderate to severe pneumonia without meeting the criteria for critical disease
All patient with signs of sever pneumonia should be admitted
8 | P a g e
Prepared by Dr. Asia Al-Matari
8
Critical (admission in Icu)
Presence of any of the following with COVID
Respiratory rate > 30 breaths/min
Severe respiratory distress )can’t speak in sentences)
Central cyanosis
Confusion, agitation, restlessness
CURB 3 or 4 score
Widespread infiltrates on CXR.
Evidence of heart failure (Raised JVP, Gallop rhythm.
Signs of shock: Delayed capillary refill, Cold, clammy peripheries; Mottled skin; Systolic BP less than 90 or less than 40mm
Hg of baseline in hypertensive; Urine output < 0.5 ml/kg/hr
Treatment of Severe & Critical Cases
1) Early admission to icu and early supportive therapy and monitoring
2) Assess the need for oxygen supplementation in line
3) Supplemental oxygen : Medical management of hospitalized adult covid-19 (for inpatient in word). patients To reach
the SpO2 target range, different devices are available (with humidifier if >3L/min):
• Nasal cannula : 1 to 5 L/min
• Simple facemask: 6 to 10 L/min. Not to use with flow less than 5L/min because of risk of re-inspiration of
CO2.
• Non-rebreather facemask: 8 to 20 L/min (two 10 L oxygen concentrators can be Y-connected to generate
higher flows).
• In some advanced settings, other oxygenation techniques are possible: non invasive ventilation (including
CPAP = continuous positive airway pressure, type CPAP O-Two®), high flow by nasal canula (HFNC) with a
specific device type AIRVO®, or invasive mechanical ventilation
Mechincal ventaltion for icu patient :
4)Recommendations for oxygen use
SpO2 is less than 90% without signs of respiratory failure: face mask 6l/mint target spo2 ( 92-95%)
Clinical signs of respiratory failure are present: non rebreather mask 15l/mint
Indications for MV :
1 .Increase work of breathing & sign of organ failure (e.g altered mental status, low BP, Increase lactate, sign of
cardiac ischemia)
2. Acute hypoxic respiratory failure not responding to HFNC nor NIV for maximum of 2 hours.
3. Hypoxia with acute decrease level of conscious and cannot protect his airway.
4.Hypoxia with large copious secretions.
5. Hypercapnic respiratory failure not responding to HFNC nor NIV.
6. Hemodynamic ally unstable
7. Consider for patient on HFNC or NIV therapy and for transfer

9 | P a g e
Prepared by Dr. Asia Al-Matari
9
3) Assess the need for fluid replacement/resuscitation
If patient can take orally give him orally.
If patient can't take orally
The initial IV hydration is limited to 1L/day (either [D5W500 ml + Ringer 500ml]/ day or [Ringer 1L + 100 ml
D5W]/day) or . It can be expanded to 1.5L/day (rarely more), or depending of assessment of physician, be care to
avoid risk of fluid overload and respiratory deterioration.
If patient has septic shock administer IV bolus of crystalloid 30 ml/kg ( R/L or N/SALINE ),after intial fluid resuscitation
administer vasopresser ( norepinephrine is the first choice ) to maintain (MAP)more than65 mmhg.
Re-assess volume status and tissue perfusion regularly.
4) Consider empirical antimicrobial treatment
Check for and treat for possible of co-infections (like malaria dengue fever , TB)
(Empirical therapy should be de-escalated on the basis of microbiology results and clinical judgment
For patients in whom COVID-19 infection is confirmed and there are no indications of antibiotic unless secondary bacterial
infection which common associated with covid -19 , stopping empirical antibiotics early should be considered if there is culture
result or side effect of it ).
Inpatient non- icu
Levofloxacin respiratory dose 750mgiv ( respiratory dose) or azithromycin plus cefoxaxime, or ceftriaxone
or ampicillin –sulbactam iv)
you can use cefipime or ceftazidime if patient has HAP or HAIs instead of ceftriaxone
In patient icu:
As inpatient non -icu
OR
Piperacillin / tazobactam (Tazocin) dose 4.5 g iv q 6h iv (adjustment of dose according renal function
(anti-pseudomonas B- lactam ) , cefepime 1-2 g iv q8 hrs
or imipenem 500mg iv q6hrs (not use in patient with history of seizure or risk) Meropenem 1 g iv q 8 hrs
Pulse either ciprofloxacin 400mg iq 12hrs or levofloxacin 750mg iv qd
If co -MRSA is consider:
Vancomycin 15mg/kg q12hrs adding ( need f/u vancomycin level every 4th
dose ( 15-20) or linezolid 600mg
iv q12hr .
If patient has severe sepsis or septic shock you can start directly tazocin or meropenem plus vancomycin after extracting blood for
C/S
(see shock treatment)
5. Corticosteroids
High-dose corticosteroids should not be routinely given to treat viral pneumonia or ARDS: their effectiveness is unproven and they
are possibly harmful.
Low-dose corticosteroids may be given if indicated for another reason
6. Anticoagulant therapy:
Increased concerns about hyper coagulability in COVID-19 patients (lower limb deep vein thrombosis and/or or pulmonary
embolism). Due to suspected prothrombotic effects in COVID patients (ie. increased risks of clotting), preventive (prophylactic)
antithrombotic dose should be given systematically to all admitted patients, unless they have signs of acute active bleeding
7) Control and treatment of comorbidities ( HTN,DM ,IHD)
8) Statin and ACE , ARB : be continued in people who have an indication for these medications.

11 | P a g e
Prepared by Dr. Asia Al-Matari
10
9) Antiviral: (depend on availability) till now no any antiviral available in Aden .
*Triple combination of lopinavir/Ritonavir(dose400/100 bid po and 400mg bid po for 14 days /interferon beta ( interferon beta-
1b 8 mcg s/c every other day for 3 dose)
*Remdesivir : not recommend for the treatment of mild or moderate covid-19
Dose adult dosing ( 200 mg loading dose iv with in 3mint )folled by 100mg iv daily for 5-10 days
Consider favipiravir (once available )*
Adult dose 1600mg /dose twic day on day 1 followed by 600mg/dose bid for 7-10 days .
WHO Recommendation
We recommend that the following drugs not be administered as treatment or prophylaxis for COVID-19, outside of the context of
clinical trials:
A) Recommendation against use of Chloroquine and hydroxychloroquine (+/- azithromycin)
B)Antivirals, including but not limited to:
*Lopinavir/ritonavir 400/100mg po bid for10days
*Remdesivir : Loading dose on the first day of 200 mg followed by a maintenance dose of 100 mg once daily for 5
*Favipiravir: Adult dose 1600mg /dose twic day on day 1 followed by 600mg/dose bid for 7-10 days .
o Immunomodulators, including but not limited to:

11 | P a g e
Prepared by Dr. Asia Al-Matari
11
*Tocilizumab: if cytokine release syndrome is suspected or conformed consider it.
dose 4-8 mg/kg loading Single maximum dose 800 mg. Repeat once after 12 hours (usaal dose 400m and maximum dose
800mg ) if the response to the first dose was poor, maximum two cumulative doses(for 2 doses)
*Interferon-β-1a: interferon beta-1b 8 mcg s/c every other day for 3 dose)
o Plasma therapy
Existing published literature on these agents is mostly observational in nature, with few clinical trials; and does not provide
high-quality evidence in favour of any of these agents.
In Addition, Important Side-Effects Have Been Described
Chloroquine and hydroxychloroquine +/- azithromycin: each can cause QT prolongation and taken together can
increase the risk of cardiotoxicity. ( WHO Not Recommended It )
Lopinavir/ritonavir: the most common adverse effects are gastrointestinal.
Remdesivir: elevation of hepatic enzymes, GI complications, rash, renal impairment and hypotension.
Umifenovir: diarrhoea, nausea.
Favipiravir: QT interval prolongation.
Interferon-β-1a: pyrexia, rhabdomyolysis.
Tocilizumab: URT infections, nasopharyngitis, headache, hypertension, increased alanine aminotransferase (ALT),
injection site reactions
Discharge Criteria for COVID19 confirmed cases
if COVID19 PCR test from nasopharyngeal sample or lower respiratory sample is positive, repeat samples after 5 days and
every 72 hours thereafter.
− Once a sample becomes negative, collect after 24 hours
− Patient can be discharged once they have :
o consecutive Negative tests for COVID 19 that are more than 24 hours apart.
o Patient is afebrile for more than 3 days and
o Patient has minimal respiratory symptoms and
o Pulmonary imaging (CXR/ HRCT) shows significant improvement
o Discharged patients to be seen in the clinic in the hospital after 2 weeks, unless patient develops respiratory
symptoms to attend earlier.
o If asymptomatic at 2 weeks, no more follow up
o All patients after discharge should be quarantined at home for 14 days from discharge date and instructions
and quarantine undertaking to be given to the patient and documented in medical record .
19 With Comorbidities Treatment Of Covid
12 | P a g e
Prepared by Dr. Asia Al-Matari
12
:1) Hypertension
Hypertension is a risk factor for developing severe COVID-19. The patient may already be on long term antihypertensive therapy
ACE inhibitors/Angiotensin Receptor Blockers: should be continued if the patient is already on them (however choose
other agent (calcium channel blocker eg. amlodipine) on the rare occasion that you need to initiate new antihypertensive
treatment)
Stop temporarily any antihypertensive treatment if the patient is hypotensive
In the acute illness phase, avoid if possible the introduction of new antihypertensives drugs, unless there is a severe
persistent hypertensive emergency, as a sudden drop in blood pressure due to antihypertensives can be detrimental in an
acutely unwell patient (risk of hypotension, syncope, chest pain, ischemic stroke).
Search first for common causes of treatable hypertension (eg.pain)
In the event of a hypertensive emergency (BP persistently >180/110mmHg with associated end-organ signs eg acute visual
change, headache, acute chest pain), start hydralazine: slow intravenous injection: 5–10mg diluted with 10ml sodium chloride
0.9%; may be repeated after 20–30 minutes. Do not use if acute myocardial ischemia (may make ischemiaworse).)
For non-life threatening, persistent high BP, start a calcium channel blocker e.g. amlodipine 5mg (slow onset of action 6-
12hrs, duration of action24hrs)
. )Diabetes2
Two scenarios can occur:
91-known diabetes with risk of destabilization of glycemic control in the context of COVIDreviously P
New diagnosis of diabetes mellitus, discovered on admission or during hospitalization
It is recommended to systematically perform a blood glucose level for all patients hospitalized for management of COVID-19,
and to closely monitor blood glucose level if diabetes is known or suspected
-assess hydration level, overall tolerance and consciousness
perform dipstick analysis for ketones-
perform ionogram (potassium, creatinine-
Basal Plus Regimen:
Treatment management in case of previously known diabetes
Stop all oral anti-diabetic drugs (higher risk of hypo/hyperglycemia during acute phase, higher risk of acidosis with
metformin when associated with hypoxia
Continue and adapt insulin if already introduced
Management for patients with type one diabetes and patient with type 2 diabetes on insulin or patient with new significant
hyperglycemia more than 2 days
:A) Insulin Orders
Discontinue oral anti-diabetic drugs and non-insulin injected anti-diabetic medication on admission
Starting glargine insulin total daily dose (TDD): 0.25 units per kg of body weigh

13 | P a g e
Prepared by Dr. Asia Al-Matari
13
Reduce insulin TDD to 0.15 units per kg of body weight in patients ≥ 70 years ofage and/or with a serum creatinine ≥ 2.0
mg/dL.
Give insulin glargine once daily, at the same time of the day
B) Supplemental insulin
Give supplemental insulin short acting insulin following the “sliding scale” protocol )E) for blood glucose > 140 mg/dl
If a patient is able and expected to eat all, give supplemental short acting insulin before each meal and at bedtime
following the “usual” column
If a patient is not able to eat, give supplemental short acting insulin every 6 hours (6-12- 6-12) following the “sensitive”
column
. :C)Insulin adjustment
If the fasting and predinner BG is between 100 - 140 mg/dl in the absence of hypoglycemia the previous day: no change
If the fasting and predinner BG is between 140 - 180 mg/dl in the absence of hypoglycemia the previous day: increase
glargine TDD by 10% every day
If the fasting and predinner BG is >180 mg/dl in the absence of hypoglycemia theprevious day: increase glargine TDD dose
by 20% every day
If the fasting and predinner BG is between 70 - 99 mg/dl in the absence of hypoglycemia: decrease glargine TDD dose by
10% every day
If a patient develops hypoglycemia (BG <70 mg/dL), the glargine TDD should be decreased by 20%.
. D )Blood glucose monitoring. Blood glucose will be measured before each meal and at bedtime (or every 6 hours if a
patient is not eating) using a glucose meter
. :E) Supplemental Insulin Scale
A. Supplemental Insulin Scale
** Check appropriate column below and cross out other columnsThe numbers
in each column indicate the number of units of short acting insulin per dose.
Blood Glucose (mg/dL) Insulin Sensitive Usual Insulin Resistant
141-180 2 4 5
181-220 4 6 8
221-260 6 8 10
261-300 8 10 12
301-350 10 12 14
351-400 12 14 16
> 400 14 16 18

14 | P a g e
Prepared by Dr. Asia Al-Matari
14
Note: If basal insulin is not available, sliding scale can be used alone
At discharge:
In patient with previously known diabetes: restart usual treatment (without insulin if the patient did not receive insulin
before admission))
If diabetes diagnosed during hospitalization: stop insulin, start Metformin 500 mg BD daily if no renal insufficiency (provide
treatment for 1 month), and refer the patient for follow-up.
:Asthma/COPD
Inhaler treatment can be continued if required for control of the disease.
Nebulisation should not be done systematically (COVID-19 transmission risk with aerosol-generating procedures).
If needed, a metered dose inhaler with spacer is preferred )patient’s single use). If not available, a home made spacer can be
made from a clean plastic bottle
Steroids, although not currently recommended for COVID19 treatment, may be indicated for acute exacerbation of known
asthma/COPD following MSF clinical guidelines for asthma/COPD .


















