Prostate Cancer G Bauman
55
A Cancer Care Ontario Partner Achieving the Acheivable: Prostate Glenn Bauman, MD Associate Professor and Chair, Department of Oncology London Regional Cancer Program University of Western Ontario
-
Upload
fondas-vakalis -
Category
Health & Medicine
-
view
1.541 -
download
3
Transcript of Prostate Cancer G Bauman
A Cancer Care Ontario Partner
Achieving theAcheivable:
ProstateGlenn Bauman, MD
Associate Professor and Chair, Department of Oncology
London Regional Cancer ProgramUniversity of Western Ontario
A Cancer Care Ontario Partner
Objectives
• We’re we’ve been• What we’ve learned• What we should do • Where we should go
• External beam• Brachytherapy• Postoperative radiotherapy• Related issues
A Cancer Care Ontario Partner
The Future is a Moving Target…
A Cancer Care Ontario Partner
Where we’ve been…
A Cancer Care Ontario Partner
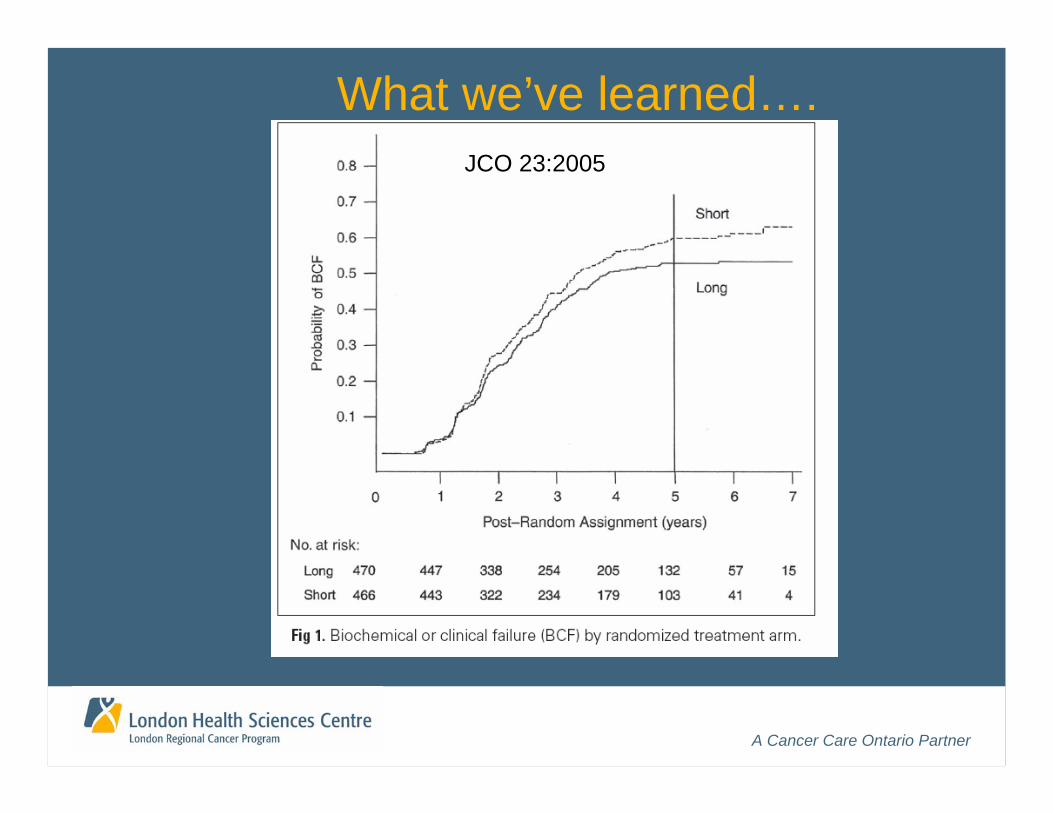
What we’ve learned….JCO 23:2005

A Cancer Care Ontario Partner
Risk stratification• Low risk
• T1-T2; PSA<10; Gleason<6• (% cores or PSA velocity*)
• Intermediate risk• T1/T2; PSA<20; Gleason <7; not otherwise low risk• (% cores or PSA velocity*)
• High risk• PSA >20 or T3 or Gleason >8;
>50% cores positive or PSA velocity >2ng/ml/yr upstages*
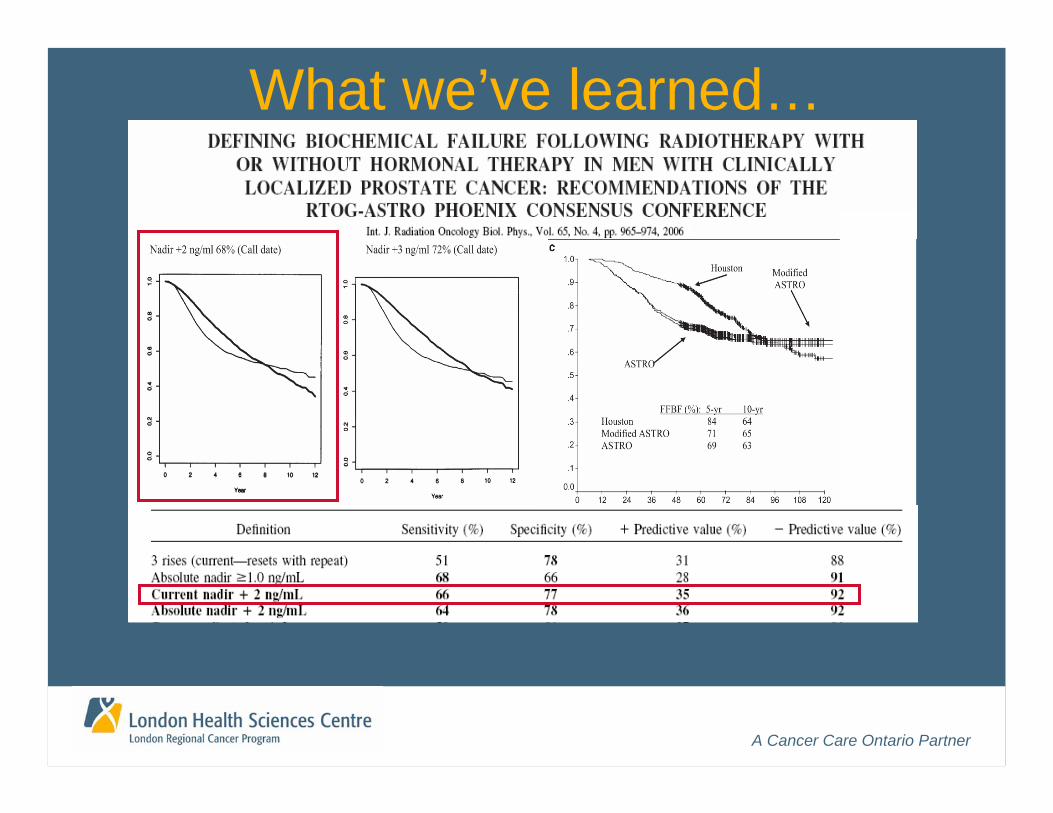
What we’ve learned….
A Cancer Care Ontario Partner
What we’ve learned…
A Cancer Care Ontario Partner
EBXRT: Current Standard:3D - conformal
A Cancer Care Ontario Partner
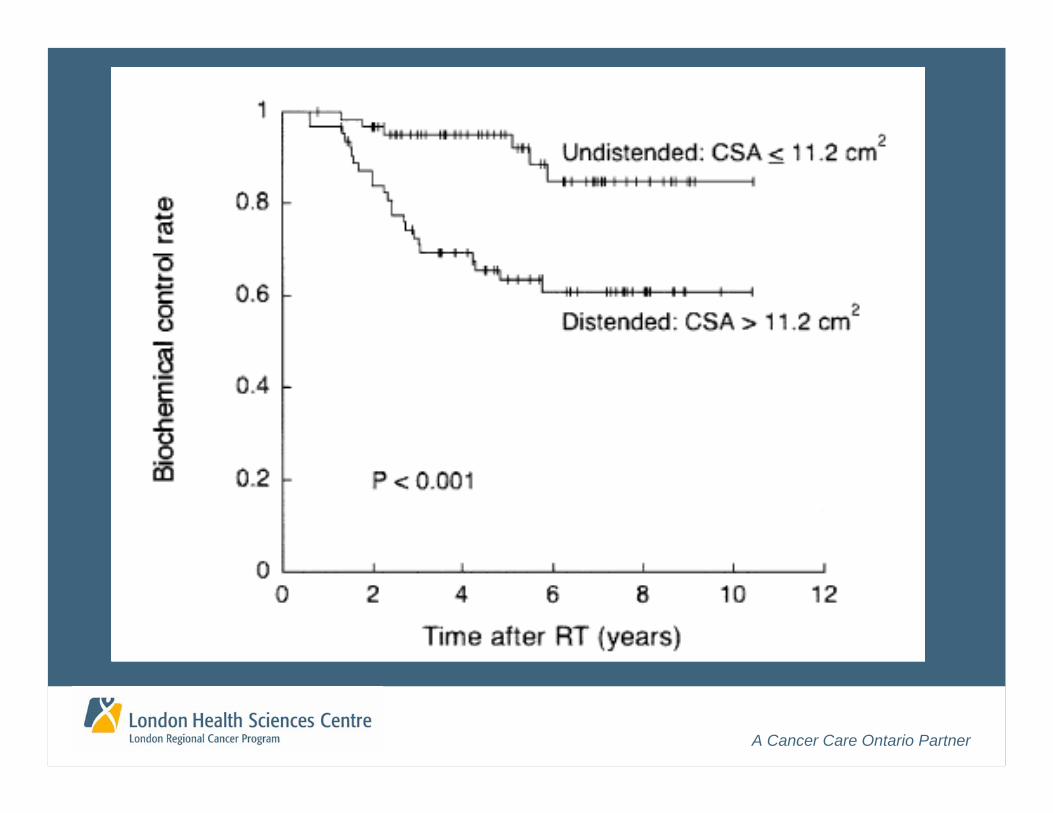
CT simulation• Simple immobilization sufficient• Patient instructions for bladder/rectum filling• Minimize iatrogenic perturbations• Flag “outliers” (rectal volume or CSA)
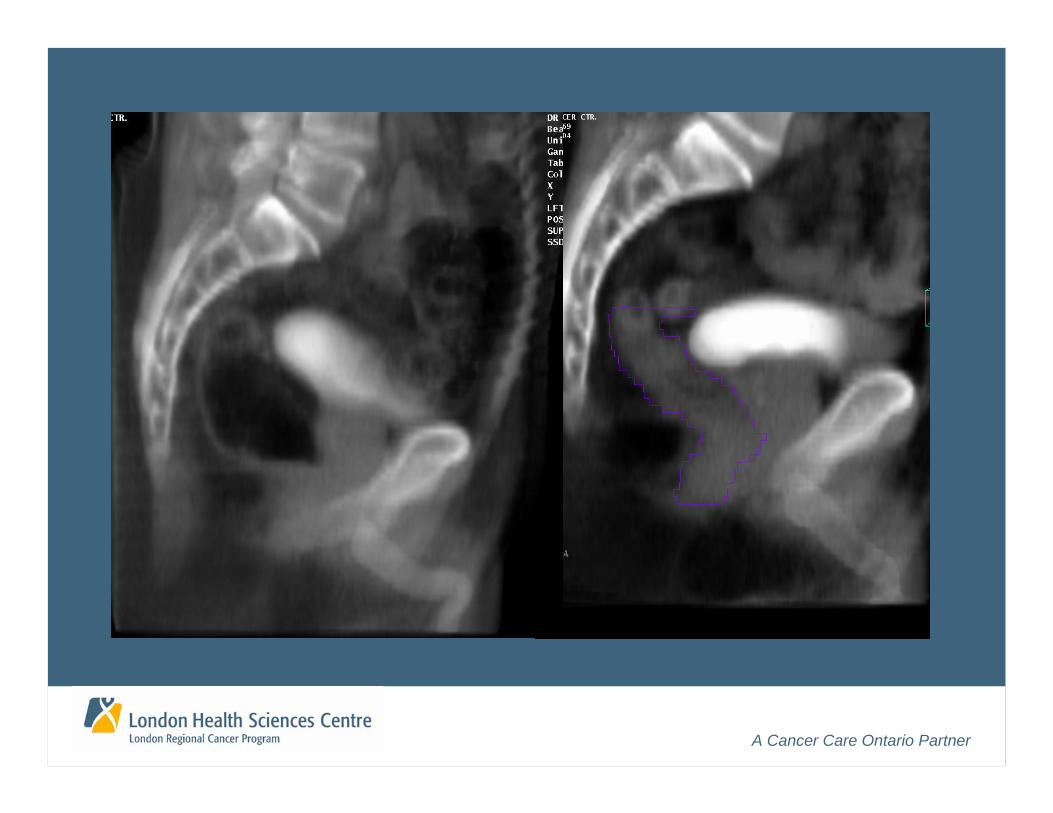
Contouring conventions (prostate + OAR)• Modality dependent• Apex and base definition• Seminal vesicles and nodes• Wall vs. solid OAR
A Cancer Care Ontario Partner
A Cancer Care Ontario Partner
A Cancer Care Ontario Partner
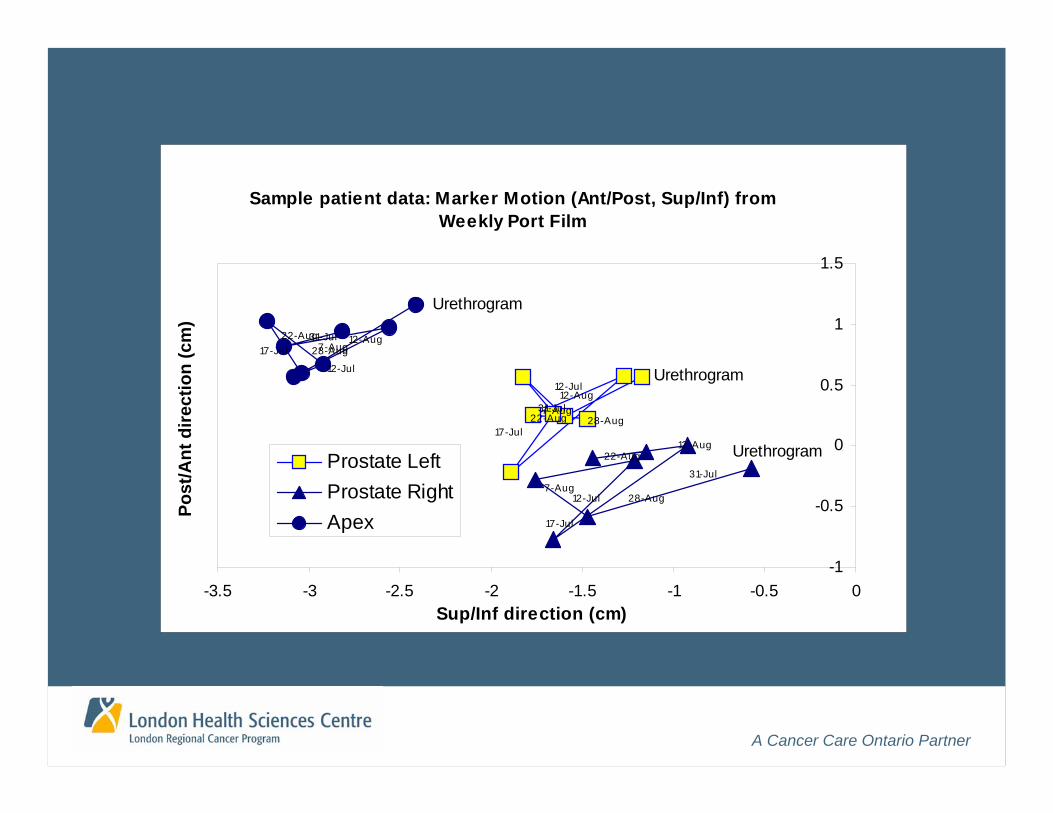
Sample patient data: Marker Motion (Ant/Post, Sup/Inf) from Weekly Port Film
22-Aug
12-Aug7-Aug
Urethrogram
17-Jul
31-Jul
12-Jul
28-Aug
12-Jul
22-Aug
17-Jul
28-Aug
31-Jul
Urethrogram
7-Aug
12-Aug
31-Jul
12-Jul
7-Aug17-Jul 28-Aug
Urethrogram
12-Aug22-Aug
-1
-0.5
0
0.5
1
1.5
-3.5 -3 -2.5 -2 -1.5 -1 -0.5 0Sup/Inf direction (cm)
Post
/Ant
dire
ctio
n (c
m)
Prostate LeftProstate RightApex
A Cancer Care Ontario Partner
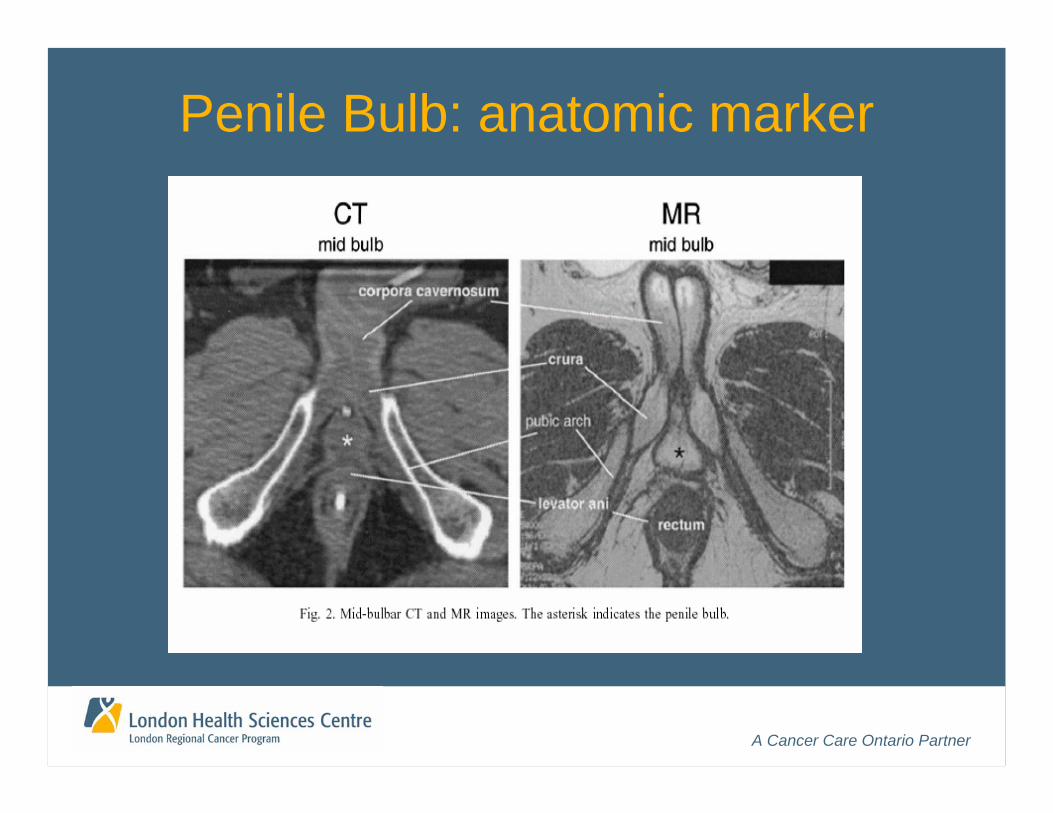
Penile Bulb: anatomic marker
A Cancer Care Ontario Partner
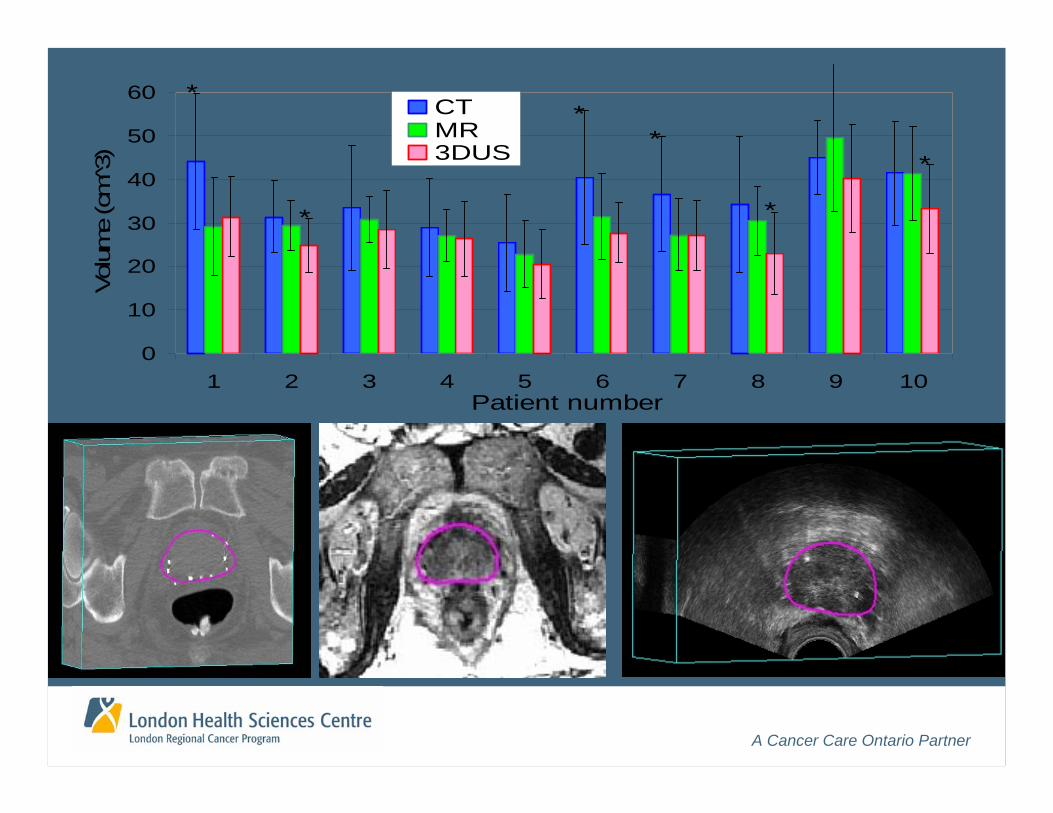
A Cancer Care Ontario Partner
0
10
20
30
40
50
60
1 2 3 4 5 6 7 8 9 10Patient number
Volu
me
(cm̂
3)CTMR3DUS
*
*
**
*
*
A Cancer Care Ontario Partner
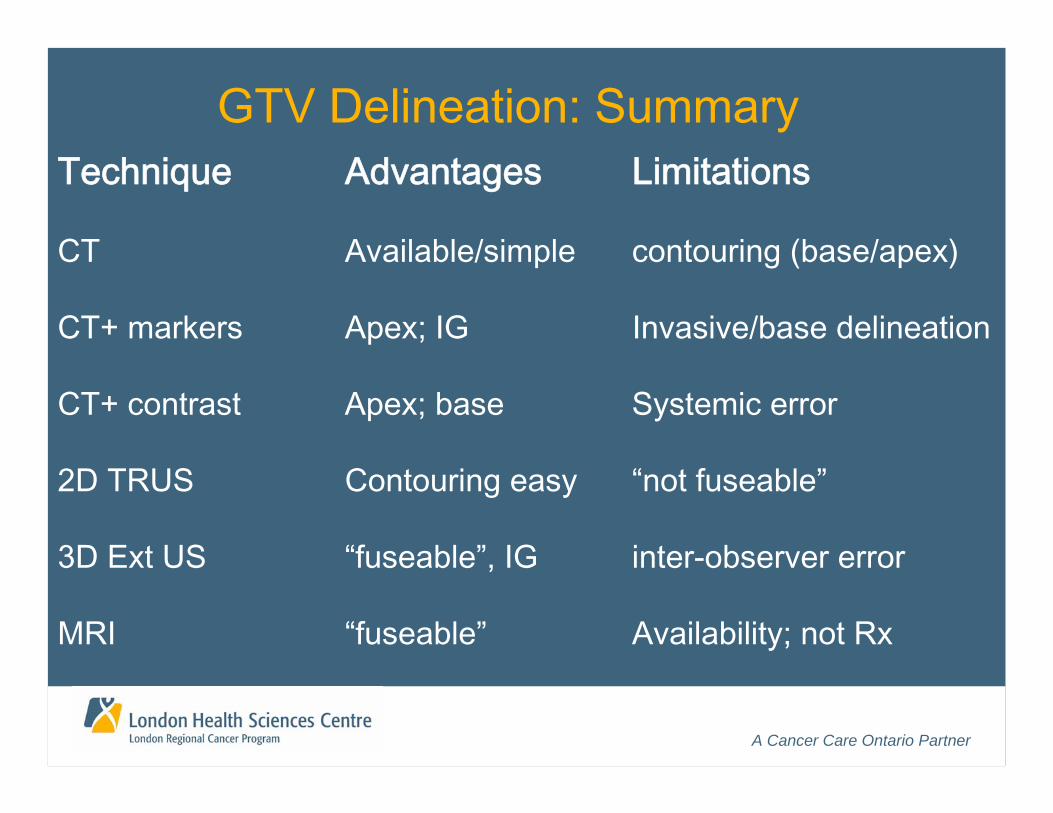
GTV Delineation: SummaryTechnique Advantages Limitations
CT Available/simple contouring (base/apex)
CT+ markers Apex; IG Invasive/base delineation
CT+ contrast Apex; base Systemic error
2D TRUS Contouring easy “not fuseable”
3D Ext US “fuseable”, IG inter-observer error
MRI “fuseable” Availability; not Rx
A Cancer Care Ontario Partner
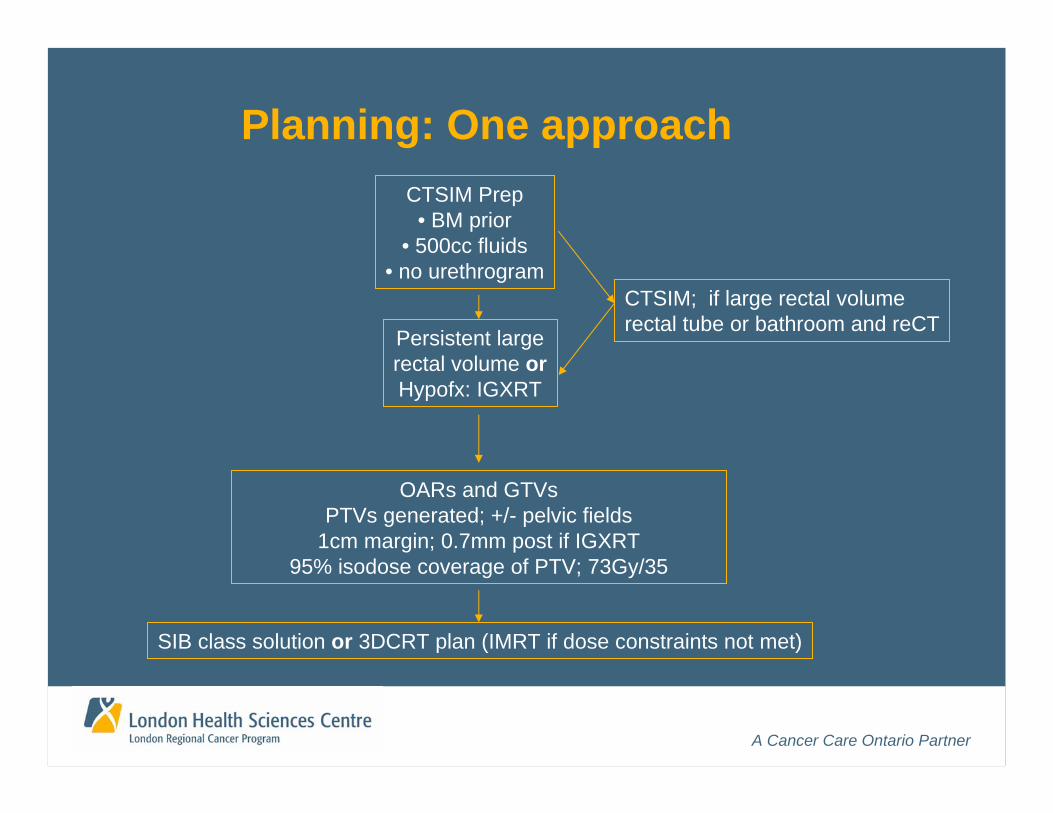
CTSIM Prep• BM prior
• 500cc fluids• no urethrogram
Persistent large rectal volume orHypofx: IGXRT
OARs and GTVsPTVs generated; +/- pelvic fields
1cm margin; 0.7mm post if IGXRT95% isodose coverage of PTV; 73Gy/35
SIB class solution or 3DCRT plan (IMRT if dose constraints not met)
CTSIM; if large rectal volumerectal tube or bathroom and reCT
Planning: One approach
A Cancer Care Ontario Partner
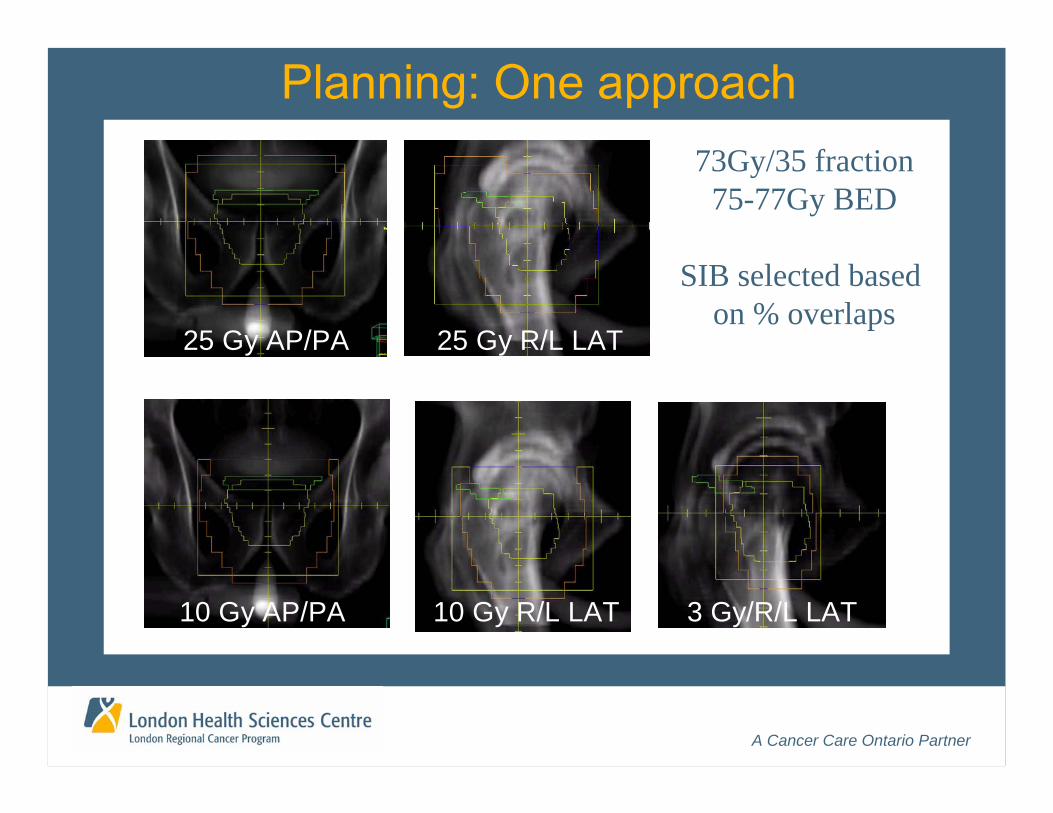
10 Gy AP/PA 10 Gy R/L LAT 3 Gy/R/L LAT
25 Gy AP/PA 25 Gy R/L LAT
Phase I:50Gy/25
Phase II:23Gy/10
Planning: One approach73Gy/35 fraction
75-77Gy BED
SIB selected based on % overlaps
A Cancer Care Ontario Partner
EBXRT Minimum Standards
• Every patient planned• 3D dose distribution and DVH• PTV and OAR DVH constraint based
• Choose a class solution and stick with it• 4-6 field 3DCRT
• Motion management strategy• Minimum dose BED > 74 Gy• PTV margins 1.0cm; 0.5-0.7 posterior
A Cancer Care Ontario Partner
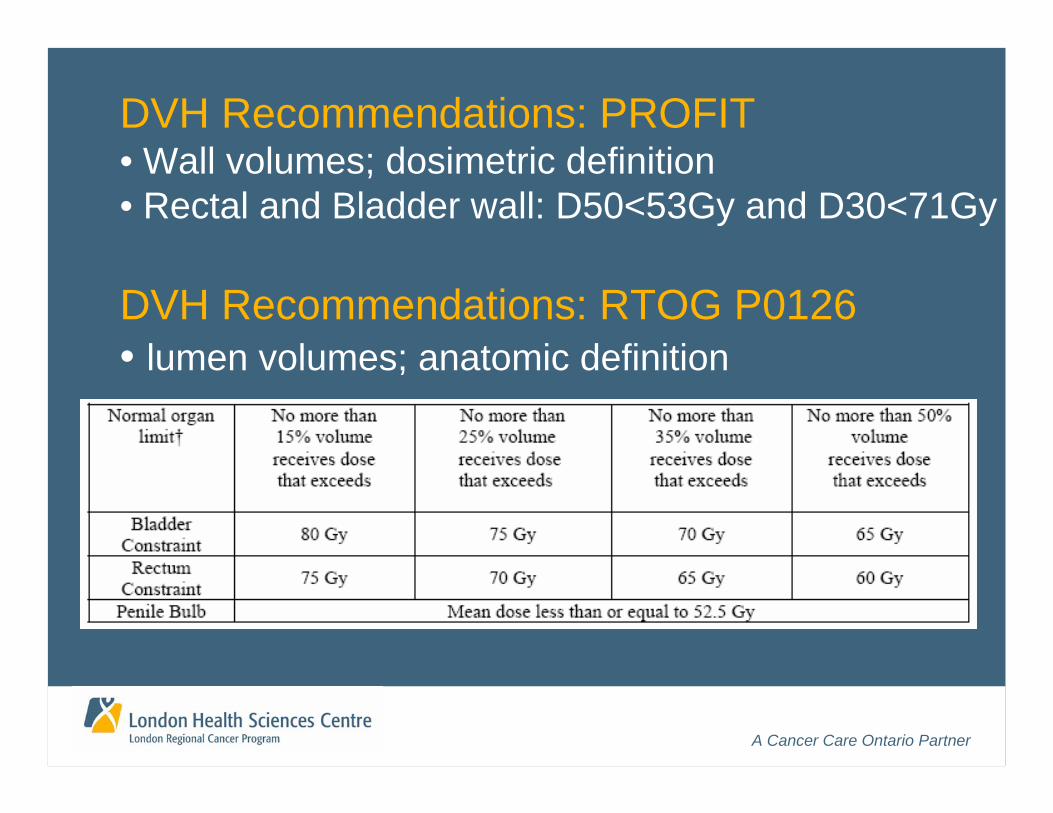
DVH Recommendations: PROFIT• Wall volumes; dosimetric definition• Rectal and Bladder wall: D50<53Gy and D30<71Gy
DVH Recommendations: RTOG P0126• lumen volumes; anatomic definition
A Cancer Care Ontario Partner
30 40 50 60 70 80
“Dosimetric”
Anatomic
0%10%20%30%40%50%60%70%80%90%
100%
0 20 40 60 80 100
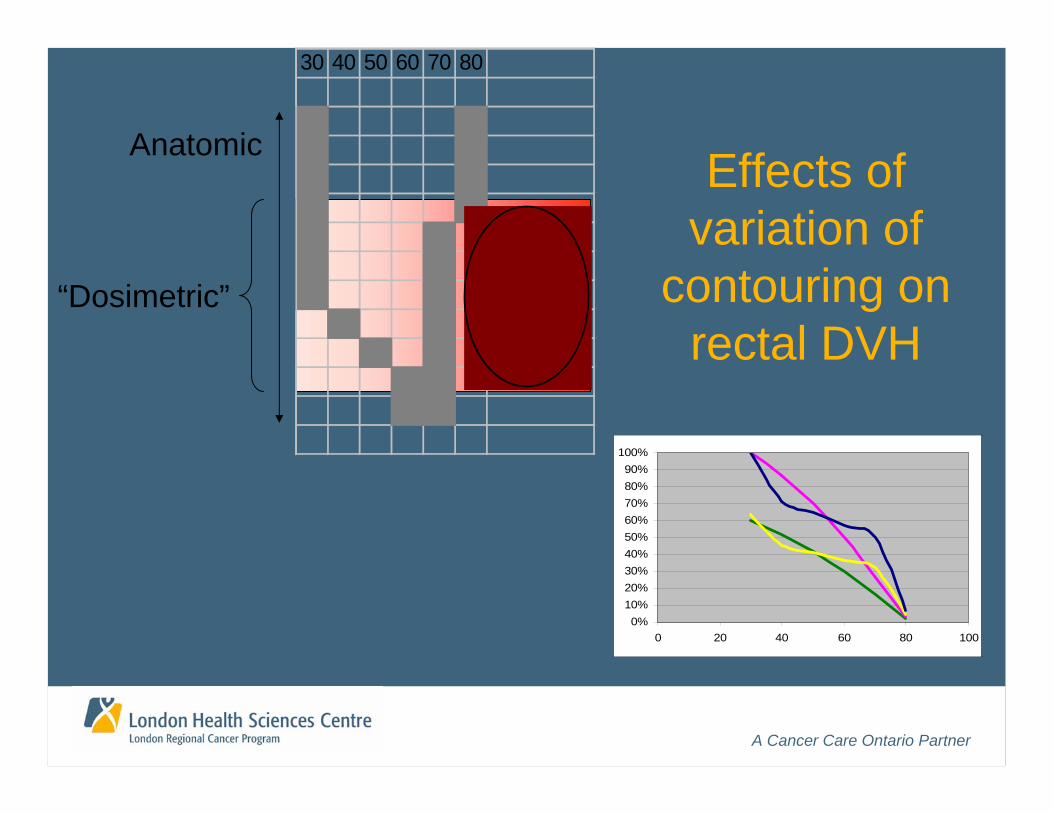
Effects of variation of
contouring on rectal DVH
A Cancer Care Ontario Partner
Clinical Data Supporting Conformal XRT
(www.cancercare.on.ccopgi.on)
A Cancer Care Ontario Partner
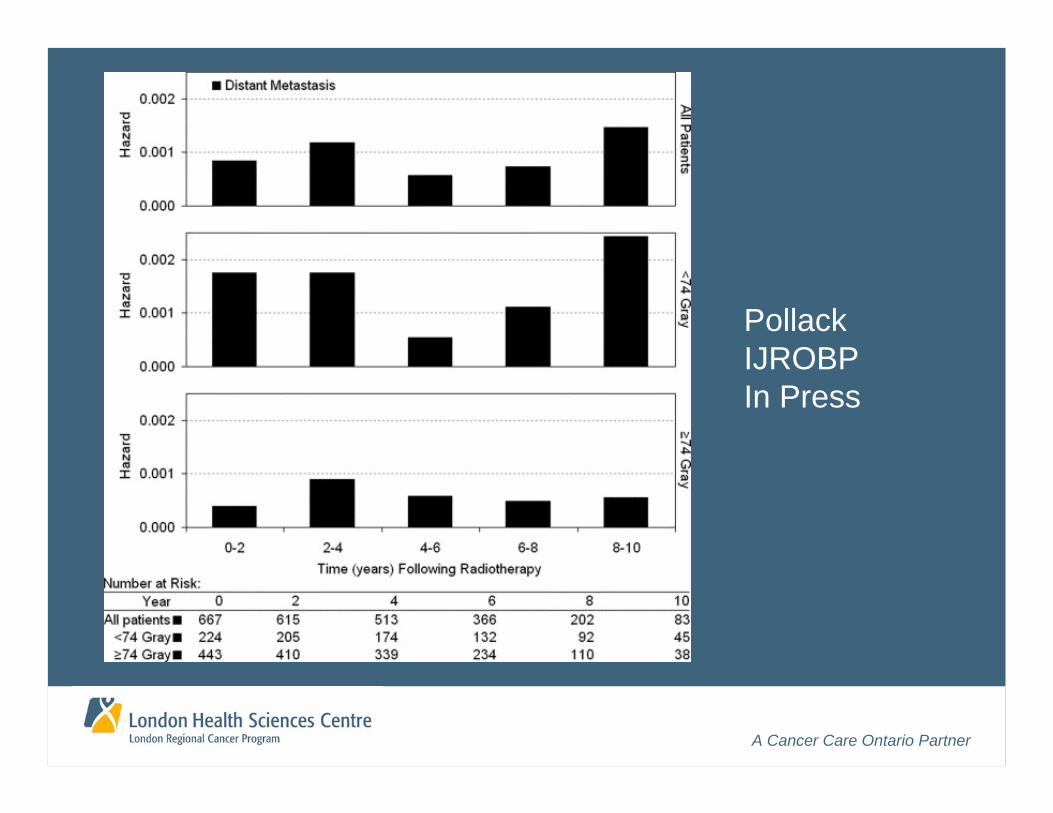
A Cancer Care Ontario Partner
PollackIJROBPIn Press
A Cancer Care Ontario Partner
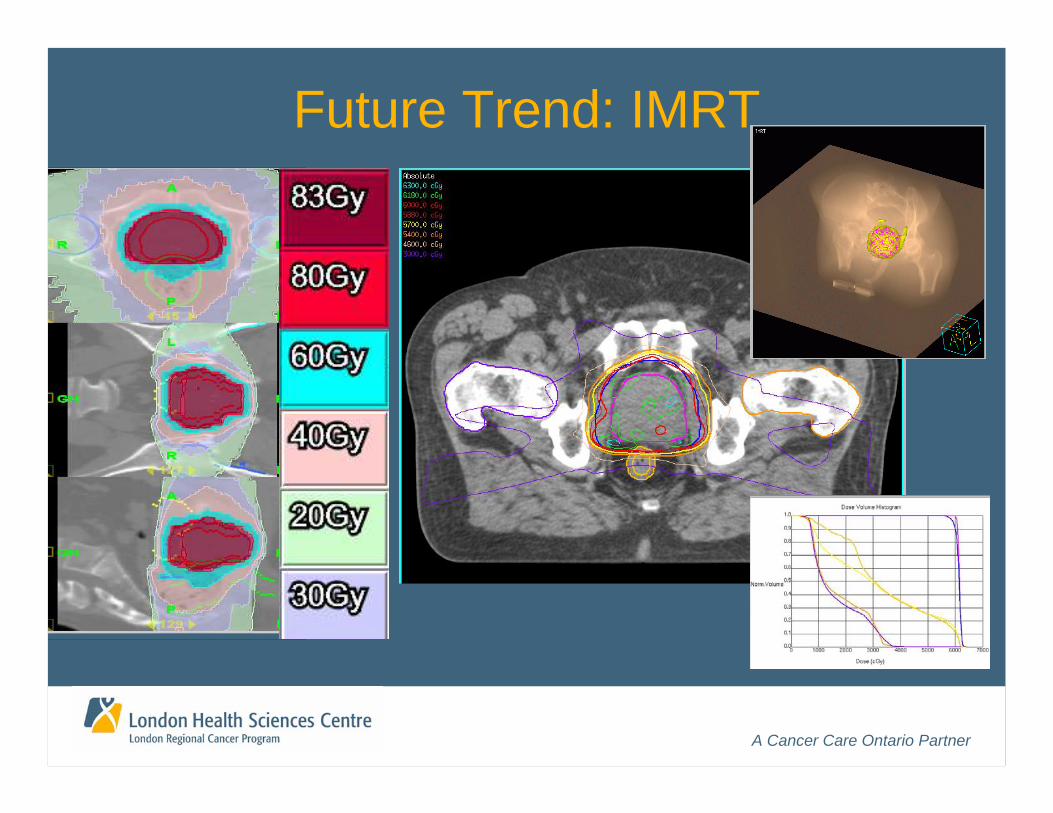
Future Trend: IMRT
A Cancer Care Ontario Partner
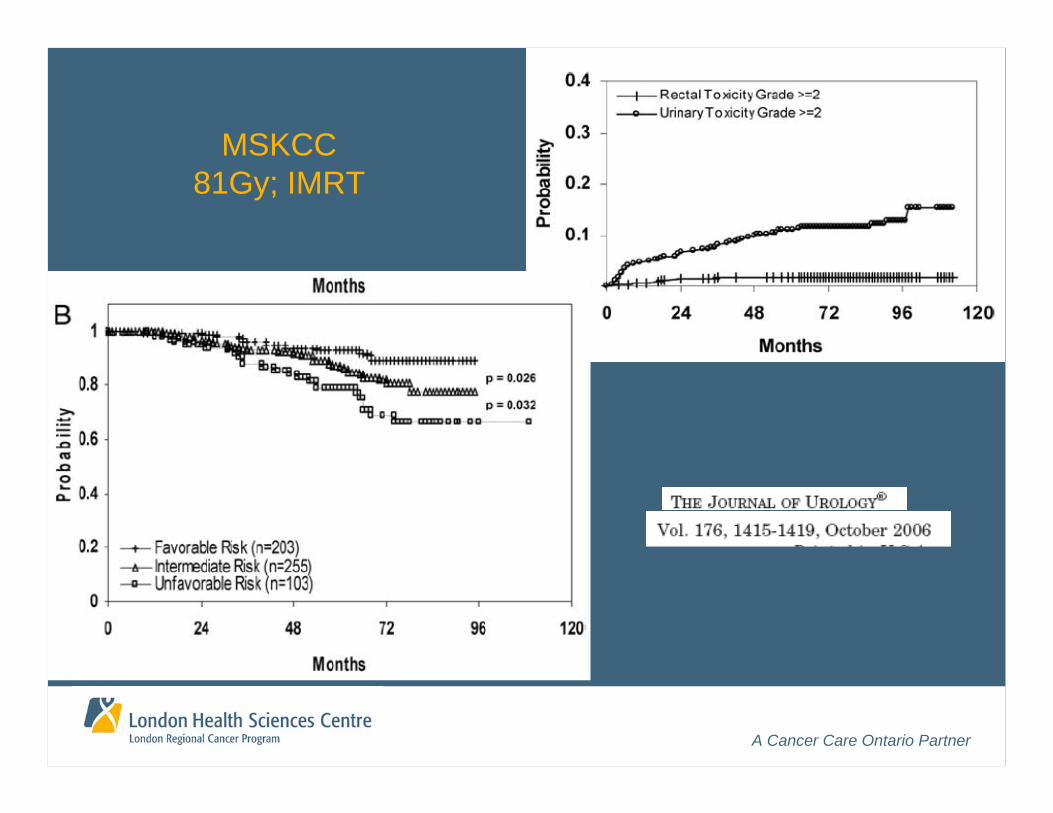
MSKCC81Gy; IMRT
A Cancer Care Ontario Partner
“If you can’t see it, you can’t hit it.If you can’t hit it, you can’t cure it”
H.E. Johns or W. Powers
“If it’s moving, you can’t hit it.If you can’t hit it, you can’t cure it”
J. Battista
Future Trend: 4D Adaptive RT
A Cancer Care Ontario Partner
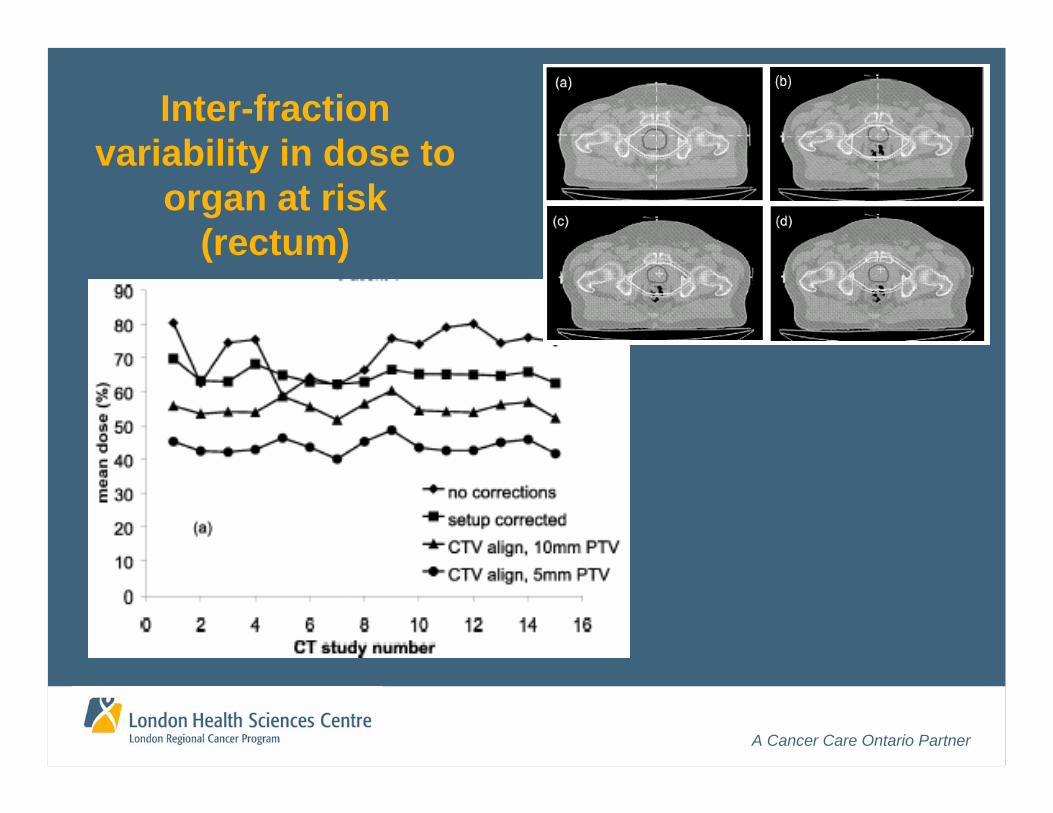
Inter-fraction variability in dose to
organ at risk (rectum)
A Cancer Care Ontario Partner
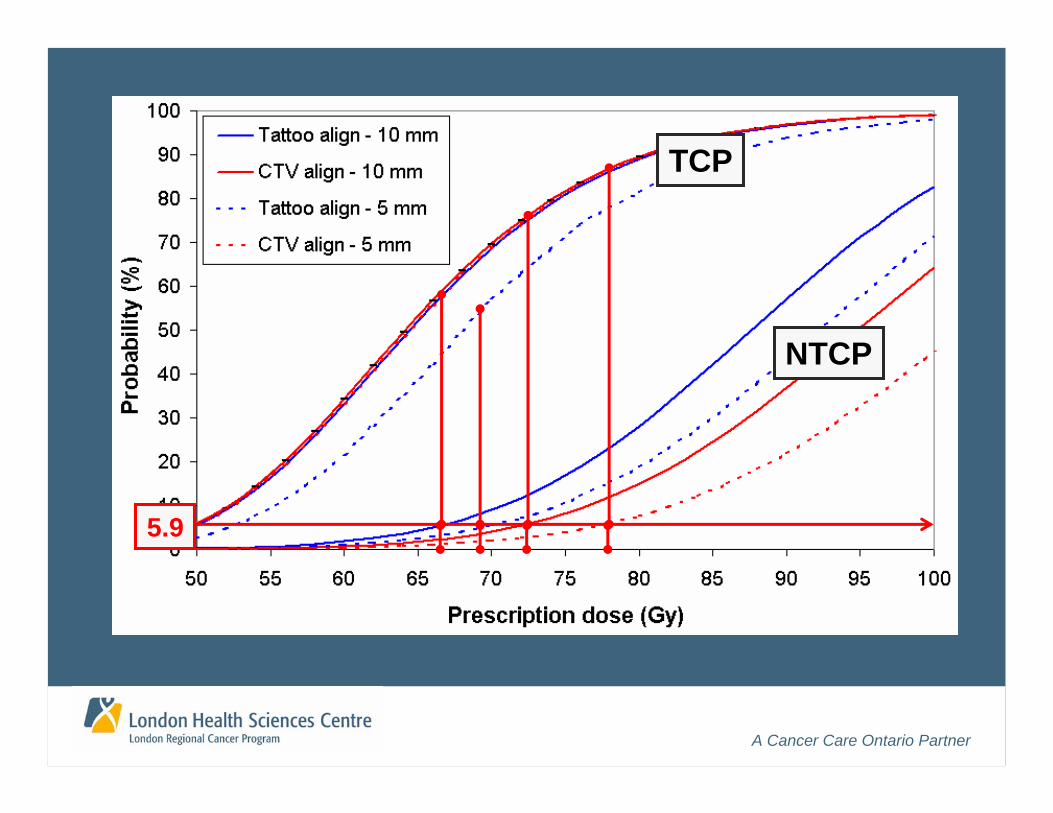
5.9
TCP
NTCP

A Cancer Care Ontario Partner
Strategy: Tracking fiducial markers
A Cancer Care Ontario Partner
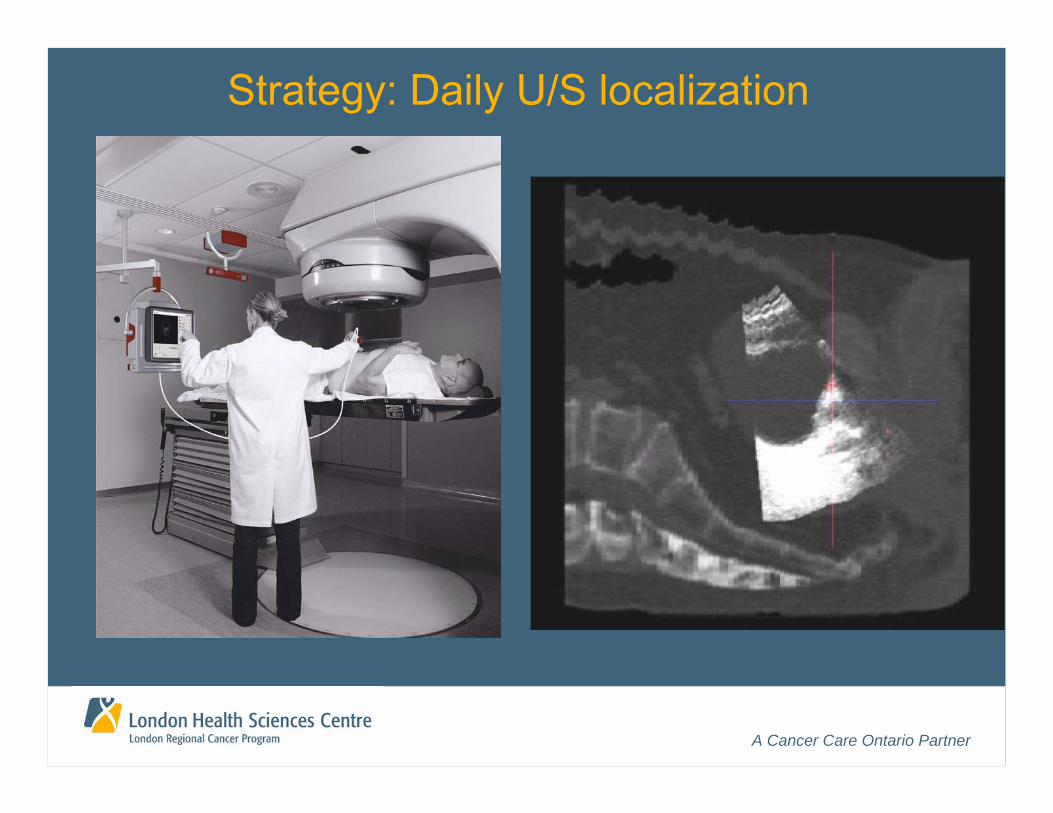
Strategy: Daily U/S localization
A Cancer Care Ontario Partner
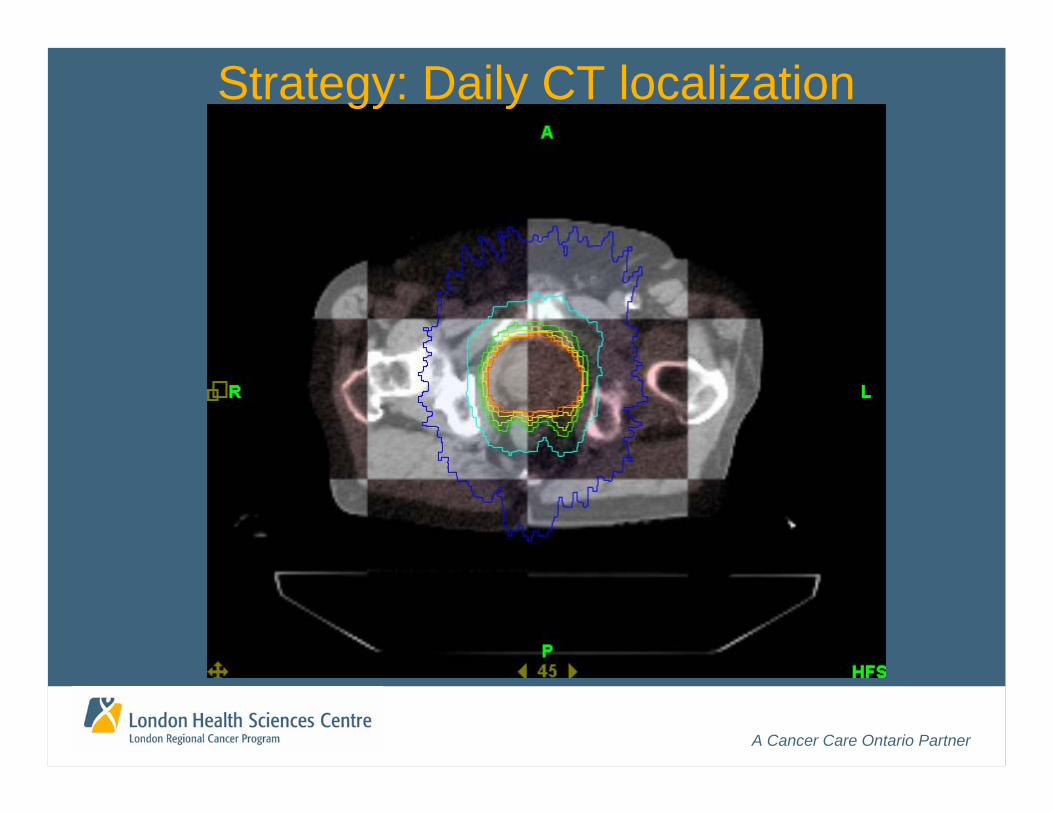
Strategy: Daily CT localization
A Cancer Care Ontario Partner
A Cancer Care Ontario Partner
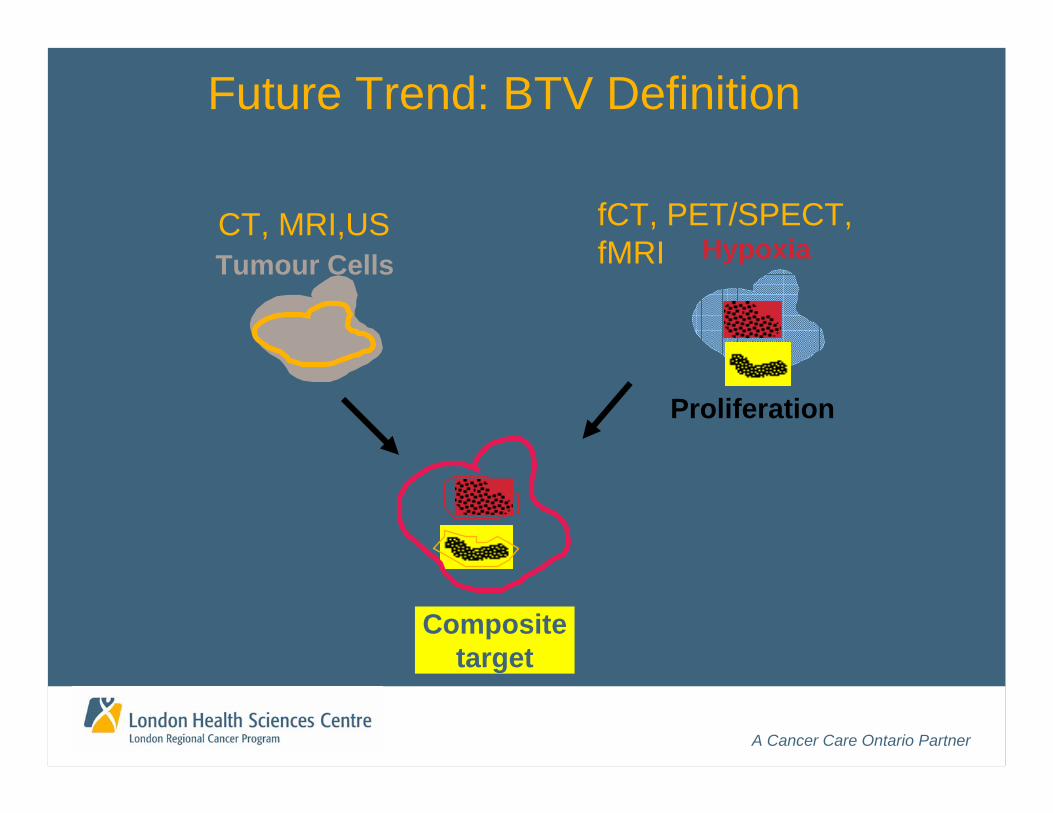
Future Trend: BTV Definition
HypoxiaTumour Cells
Proliferation
fCT, PET/SPECT, fMRI
CT, MRI,US
Composite target

A Cancer Care Ontario PartnerDawson, Lancet Oncol, 7 2006
A Cancer Care Ontario Partner
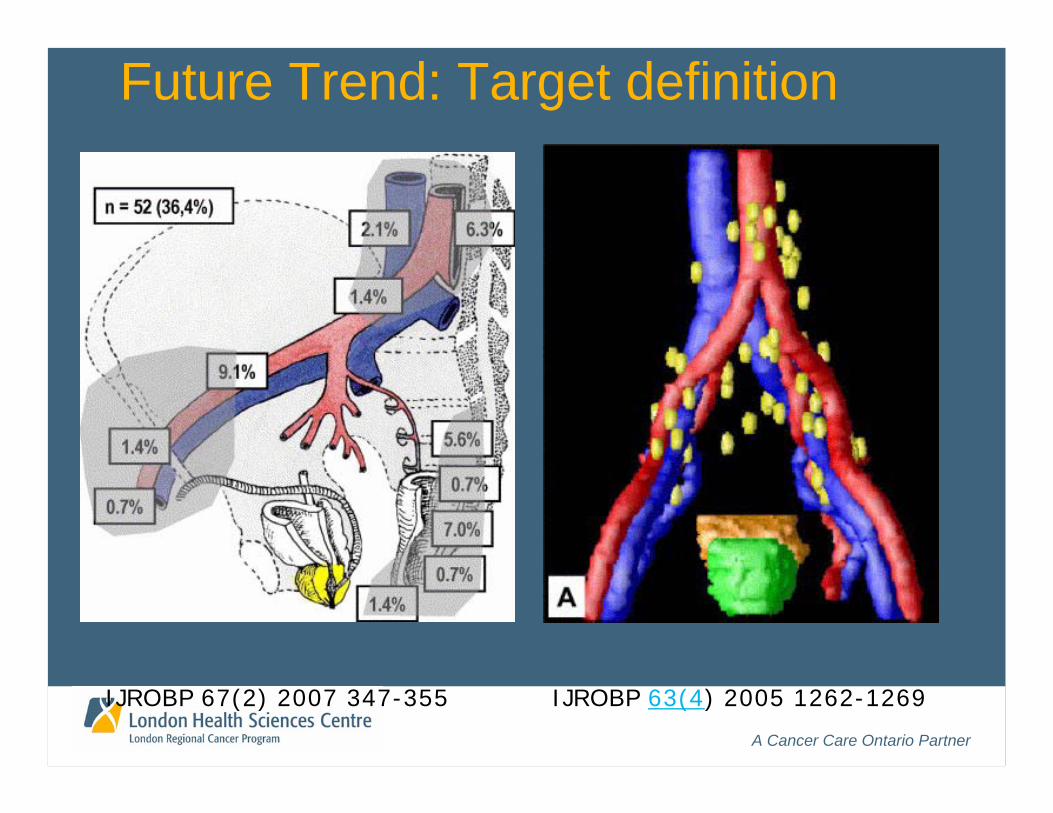
Future Trend: Target definition
IJROBP 63(4) 2005 1262-1269IJROBP 67(2) 2007 347-355
A Cancer Care Ontario Partner
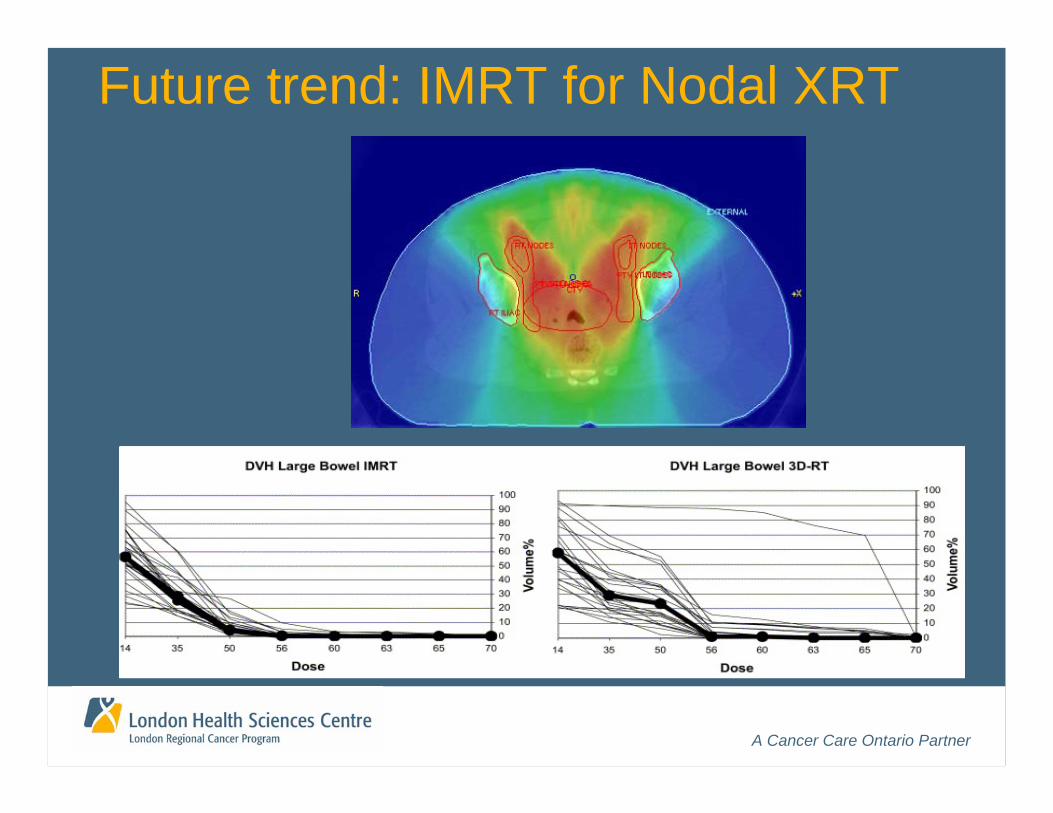
Future trend: IMRT for Nodal XRT

A Cancer Care Ontario Partner
Future trend: Hypofractionation
* Fowler J, et al. Int J Radiat Oncol Biol Phys 2003;56:1093-1104.
Iso-late-complicationsTum
or C
ontr
ol P
roba
bilit
y (%
)
A Cancer Care Ontario Partner
Standards: Prostate I125
• Prostate Volume < 50 cc• Clinical Stage T1c or T2a• PSA < 10• Gleason Score < 6• No Nodal or distant metastases• No previous TURP
A Cancer Care Ontario Partner
• Ultrasound Volume Study • Pubic Arch Interference Assessment• Pre-plan: 145Gy to periphery of prostate• Ordering I-125 seeds and calibration• Needle loading• Ultrasound guided Implantation• CT post-planning
Standards: Prostate I125
A Cancer Care Ontario Partner
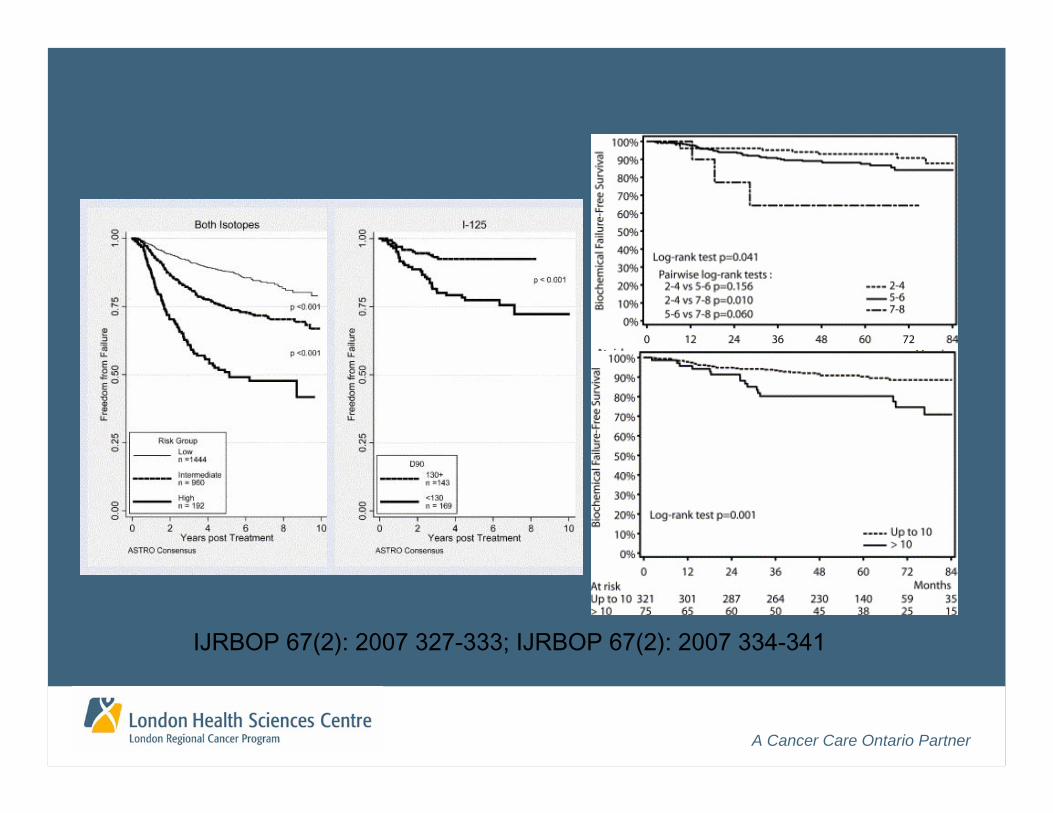
IJRBOP 67(2): 2007 327-333; IJRBOP 67(2): 2007 334-341
A Cancer Care Ontario Partner
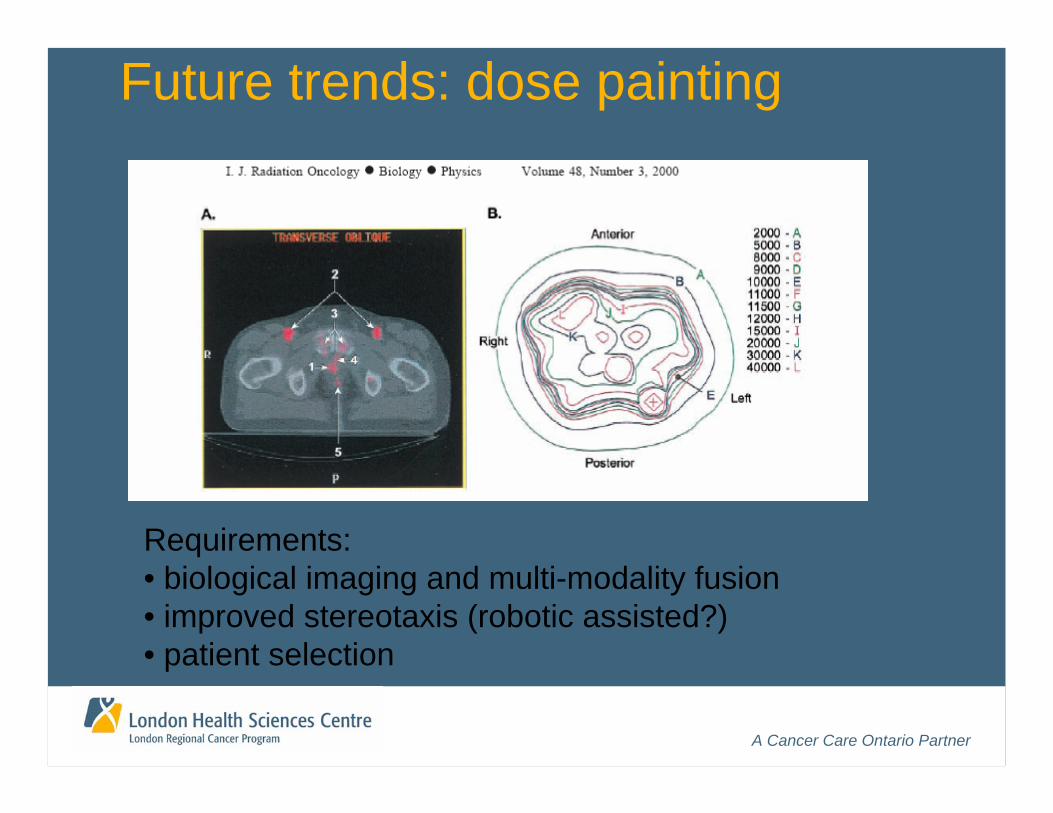
Future trends: dose painting
Requirements:• biological imaging and multi-modality fusion• improved stereotaxis (robotic assisted?)• patient selection
A Cancer Care Ontario Partner
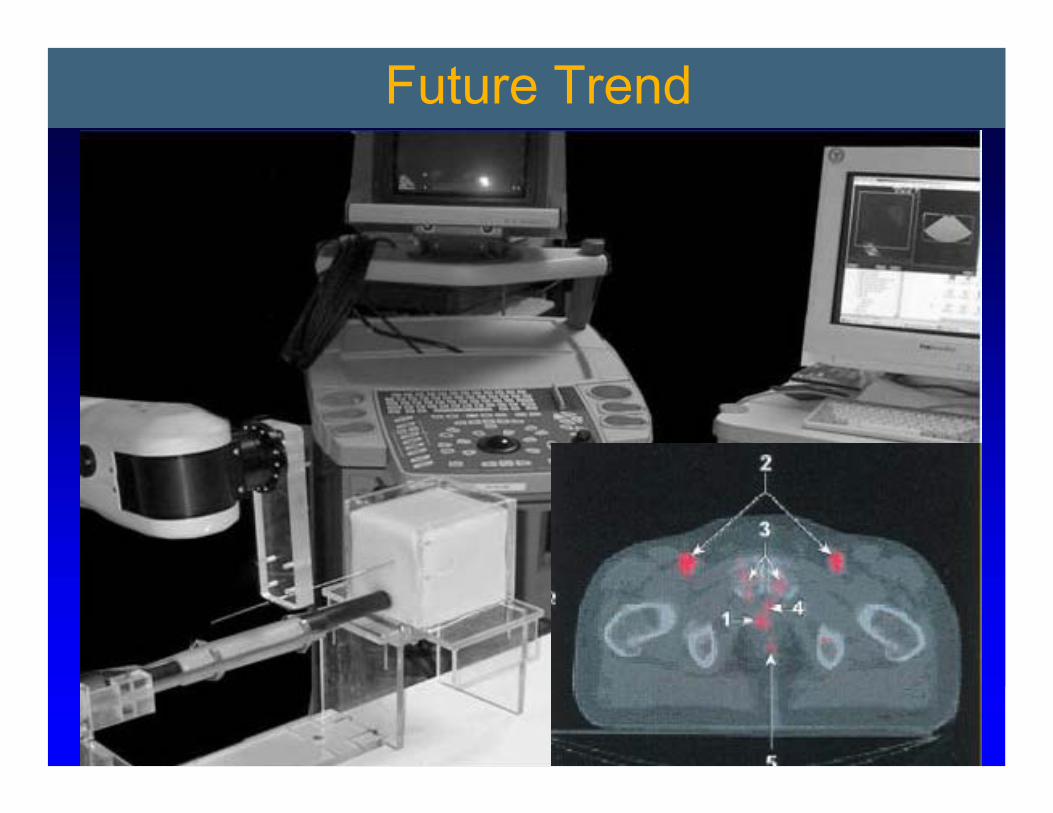
Future Trend
A Cancer Care Ontario Partner
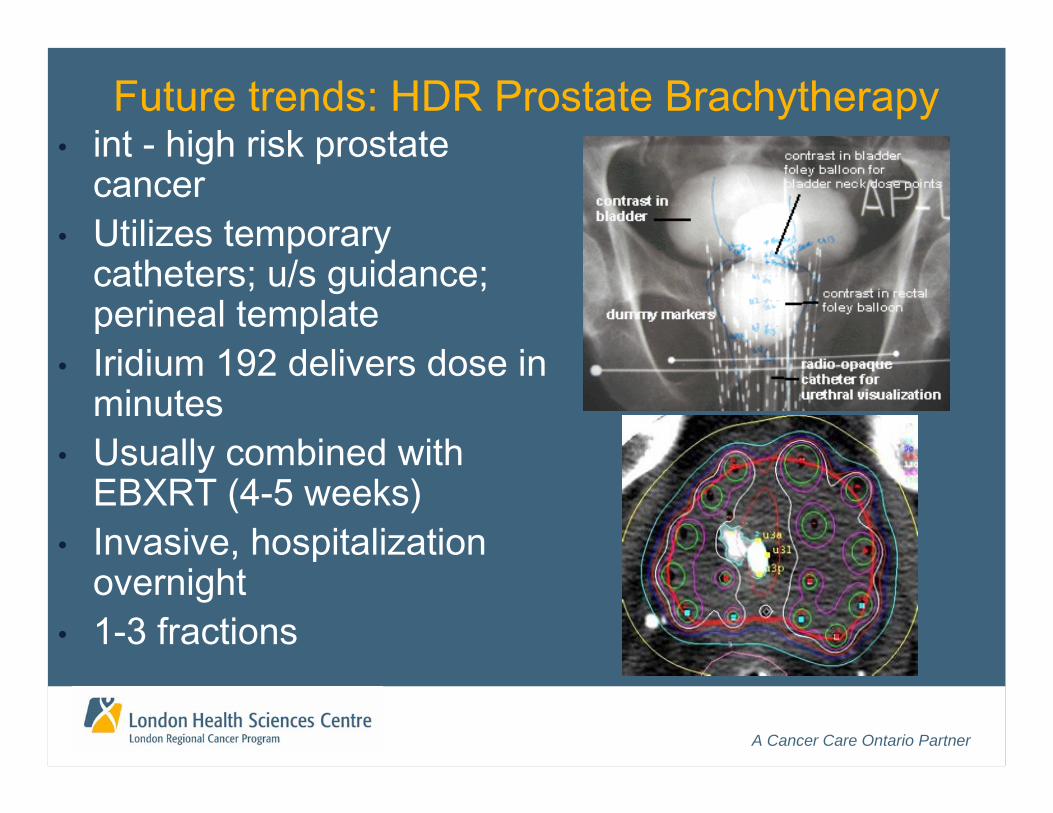
Future trends: HDR Prostate Brachytherapy• int - high risk prostate
cancer• Utilizes temporary
catheters; u/s guidance; perineal template
• Iridium 192 delivers dose in minutes
• Usually combined with EBXRT (4-5 weeks)
• Invasive, hospitalization overnight
• 1-3 fractions
A Cancer Care Ontario Partner
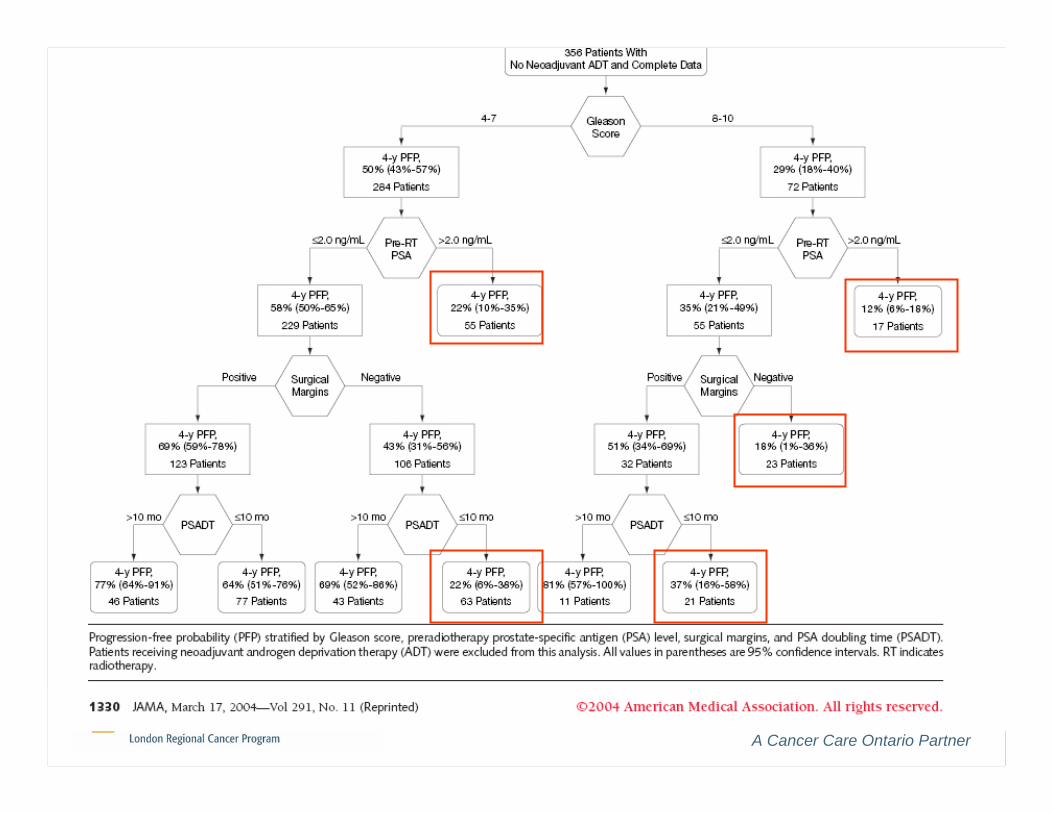
Postoperative/Salvage Radiation
Postoperative: • 3 RCT supporting adjuvant radiation• pT3 or margin positiveSalvage• Case series only (Stephenson, JAMA)• Margin positive, PSA < 2.0, post RP kinetics
CTSIM; 60-66Gy/30=33; 3DCRT
A Cancer Care Ontario Partner
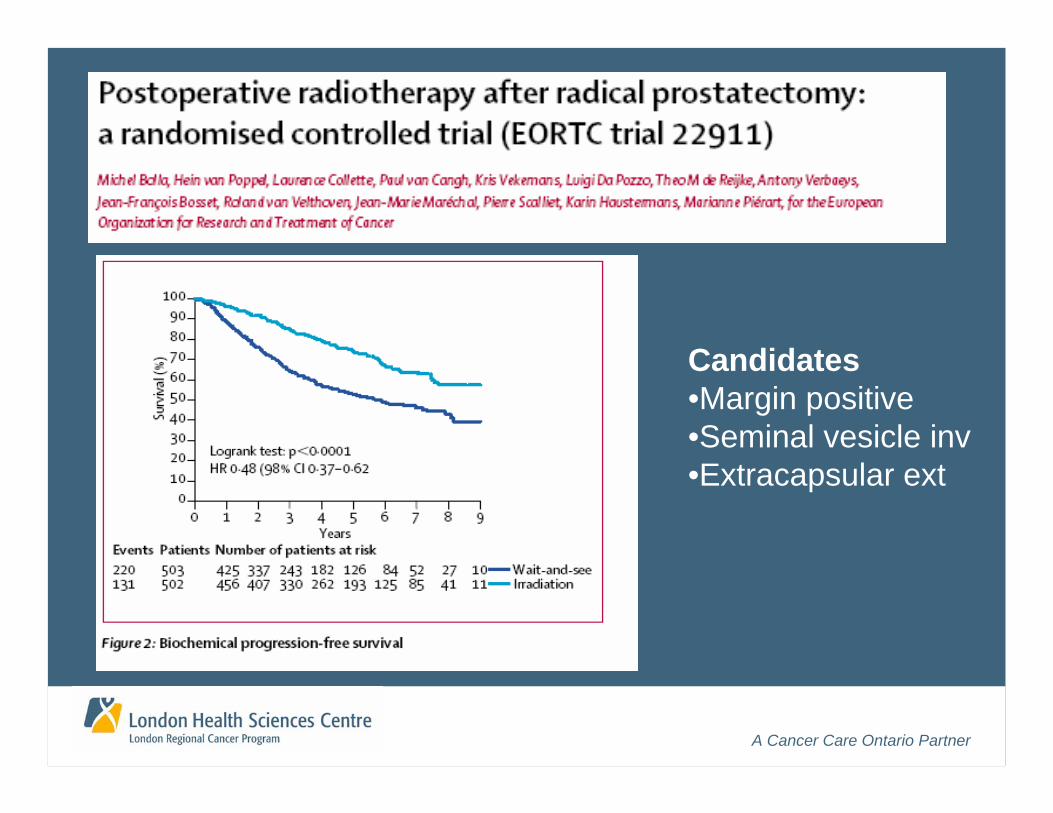
Candidates•Margin positive•Seminal vesicle inv•Extracapsular ext
A Cancer Care Ontario Partner
A Cancer Care Ontario Partner
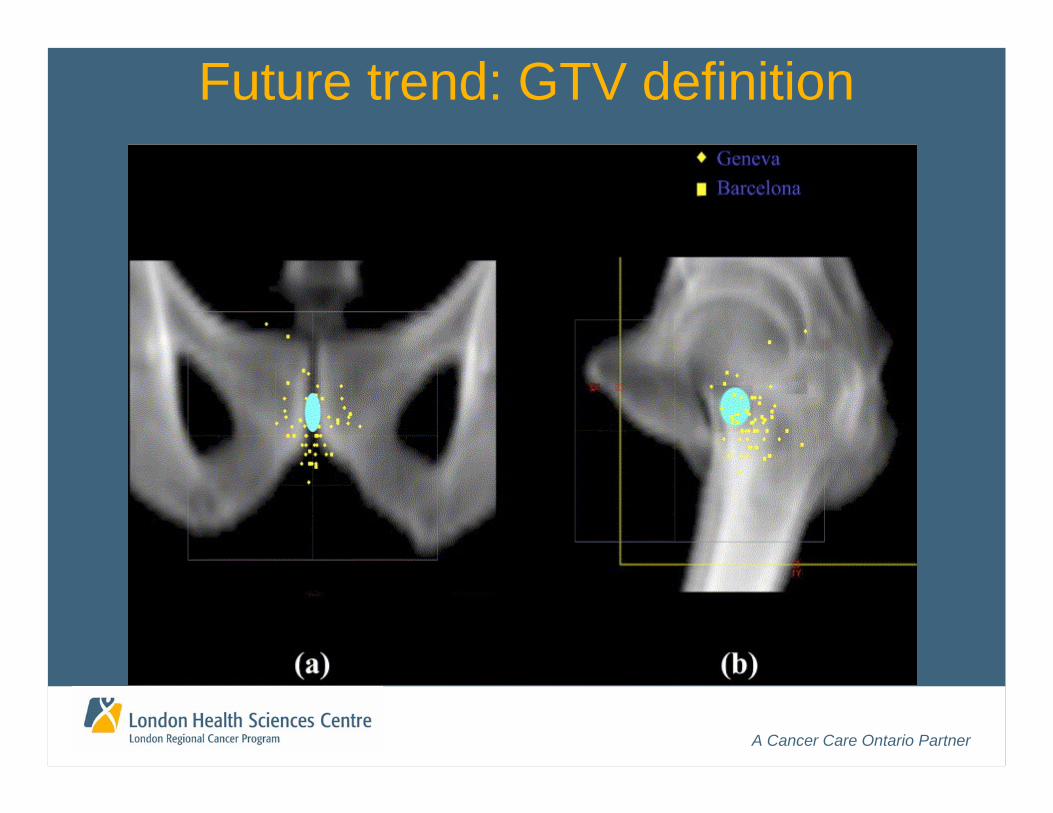
Future trend: GTV definition
A Cancer Care Ontario Partner
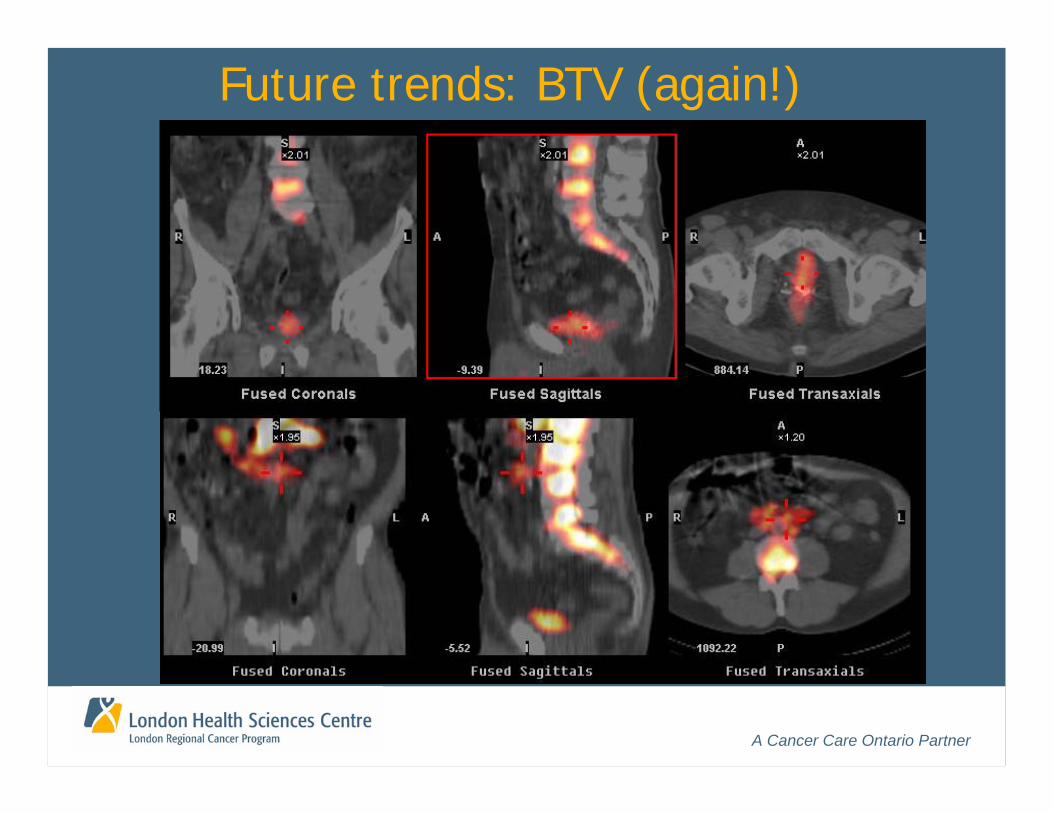
Future trends: BTV (again!)
A Cancer Care Ontario Partner
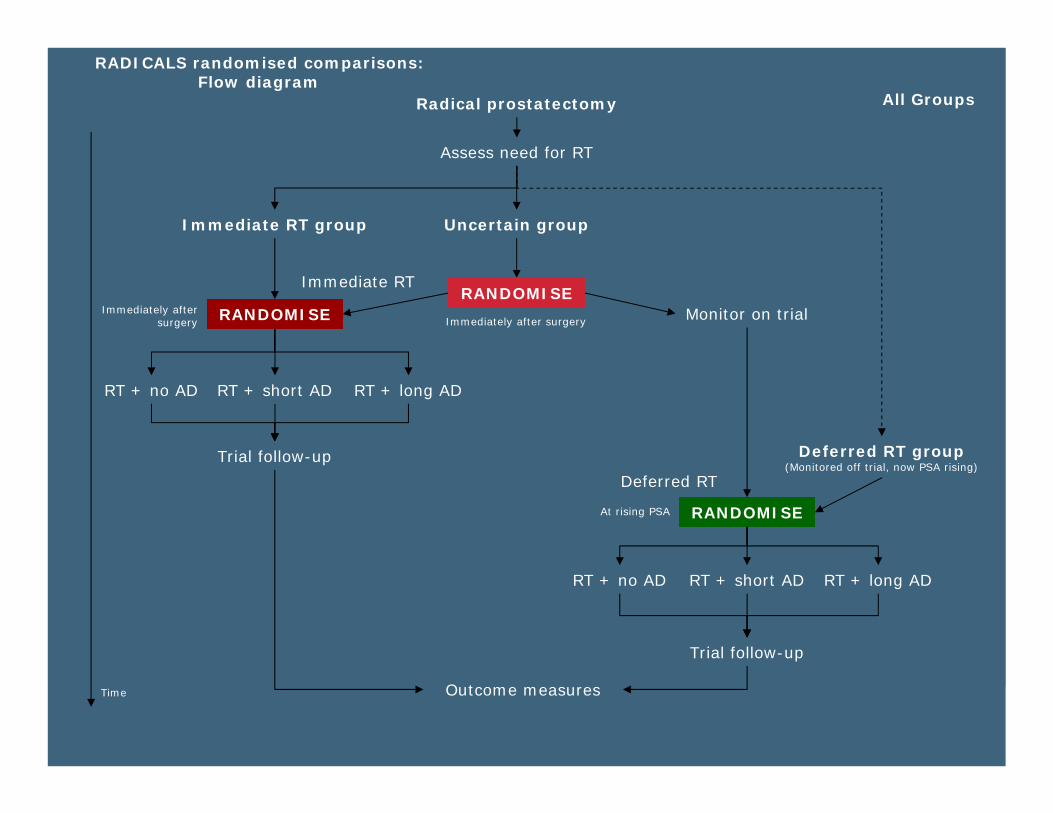
Radical prostatectomy
Assess need for RT
Uncertain groupImmediate RT group
Trial follow-up
RANDOMISEImmediately after surgery
RANDOMISE
Outcome measures
RT + no AD RT + short AD RT + long AD
Trial follow-up
Monitor on trial
Immediate RT
Deferred RT
Time
All Groups
RANDOMISE
Immediately after surgery
RT + no AD RT + short AD RT + long AD
RADICALS randomised comparisons: Flow diagram
At rising PSA
Deferred RT group (Monitored off trial, now PSA rising)
A Cancer Care Ontario Partner
What is needed?
• Common prep, contouring and DVH conventions• Multi-modality GTV definition (U/S or MRI)• IMRT enabled planning and LINACS• Efficient IMRT class solutions and QA/QC• Image guidance requirements:
• CL-PTV: repeat CTSIM and dosimetry capacity• CT: CB or MVCT Unit• U/S: US at LINAC and CTSIM• Seed: Marker placement (radiology)
• RT training: image interpretation; action levels; correction
A Cancer Care Ontario Partner
What else is needed – long term?• Better predictors of toxicity/common databases• Biological and functional multi-modality imaging• Complete ongoing RCT
• Dose escalation and hypofractionation
• New RCT• Multimodality (LDR/HDR/CTX/Sx)
• A new paradigm?• “Prostate Lumpectomy” + regional XRT
• Patient decision aids• EPR enabled follow-up

A Cancer Care Ontario Partner
Changes in CaP XRT• 66-70Gy• 4 field; blocks• Fluoroscopic • DRE
• 3D CRT• LDR• Hypofx (Part I)• Models
• MLC• TPS• CTS• RVS• Fiducials
• BED >78Gy• IGXRT• IMRT
• Multi-modal• BTV optimization• Prostate SRT• Gating
• Multi-modal imaging• Real time IGXRT• Multi-modal TPS• BTV TPS
• BED > 74 Gy• 4-6 fields; 3DCRT• CTSIM• Risk stratified, bDFS
• IGXRT• HDR• Dose escalation• Hypofx (Part II)
• dMLC• EPI/US/CBCT/MVCT• MR SIM/CT-US SIM
A Cancer Care Ontario Partner
http://www.youtube.com/watch?v=LQqq3e03EBQ
A Cancer Care Ontario Partner
Thank You!