
Prospective risk factors for post- deployment heavy ...
41
Prospective risk factors for post- deployment heavy drinking and alcohol or substance use disorder among US Army soldiers The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Campbell-Sills, Laura, Robert J. Ursano, Ronald C. Kessler, Xiaoying Sun, Steven G. Heeringa, Matthew K. Nock, Nancy A. Sampson, Sonia Jain, and Murray B. Stein. 2017. “Prospective Risk Factors for Post-Deployment Heavy Drinking and Alcohol or Substance Use Disorder Among US Army Soldiers.” Psychological Medicine (October 17): 1–12. doi:10.1017/s0033291717003105. Published Version doi:10.1017/S0033291717003105 Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:34864121 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Open Access Policy Articles, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#OAP
Transcript of Prospective risk factors for post- deployment heavy ...

Prospective risk factors for post-deployment heavy drinking
and alcohol or substance usedisorder among US Army soldiers
The Harvard community has made thisarticle openly available. Please share howthis access benefits you. Your story matters
Citation Campbell-Sills, Laura, Robert J. Ursano, Ronald C. Kessler, XiaoyingSun, Steven G. Heeringa, Matthew K. Nock, Nancy A. Sampson,Sonia Jain, and Murray B. Stein. 2017. “Prospective Risk Factorsfor Post-Deployment Heavy Drinking and Alcohol or SubstanceUse Disorder Among US Army Soldiers.” Psychological Medicine(October 17): 1–12. doi:10.1017/s0033291717003105.
Published Version doi:10.1017/S0033291717003105
Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:34864121
Terms of Use This article was downloaded from Harvard University’s DASHrepository, and is made available under the terms and conditionsapplicable to Open Access Policy Articles, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#OAP
1
Wordcount(textonly):43911
NumberofTables:32
NumberofFigures:23
NumberofSupplementaryTables:44
5
Prospectiveriskfactorsforpost-deploymentheavydrinkingandAlcoholorSubstanceUseDisorder6
amongU.S.Armysoldiers7
8
LauraCampbell-Sills,PhD19
RobertJ.Ursano,MD210
RonaldC.Kessler,PhD311
XiaoyingSun,MS412
StevenG.Heeringa,PhD513
MatthewK.Nock,PhD614
NancyA.Sampson,BA315
SoniaJain,PhD416
MurrayB.Stein,MD,MPH1,4,717
18
1DepartmentofPsychiatry,UniversityofCaliforniaSanDiego,LaJolla,CA,USA19
2CenterfortheStudyofTraumaticStress,DepartmentofPsychiatry,UniformedServicesUniversityof20
theHealthSciences,Bethesda,MD,USA21
3DepartmentofHealthCarePolicy,HarvardMedicalSchool,Boston,MA,USA22
4DepartmentofFamilyMedicineandPublicHealth,UniversityofCaliforniaSanDiego,LaJolla,CA,USA23
5UniversityofMichigan,InstituteforSocialResearch,AnnArbor,MI,USA24

2
6DepartmentofPsychology,HarvardUniversity,Cambridge,MA,USA25
7VASanDiegoHealthcareSystem,SanDiego,CA,USA26
27
Pleaseaddresscorrespondenceto:28
LauraCampbell-Sills,PhD29
UCSDDepartmentofPsychiatry30
9500GilmanDrive,MailCode085531
LaJolla,CA9209332
Phone:(858)534-6448;Fax:(858)534-646033
Email:[email protected]
35
ArmySTARRSwassponsoredbytheDepartmentoftheArmyandfundedundercooperativeagreement36
numberU01MH087981(2009-2015)withtheU.S.DepartmentofHealthandHumanServices,National37
InstitutesofHealth,NationalInstituteofMentalHealth(NIH/NIMH).Subsequently,STARRS-LSwas38
sponsoredandfundedbytheDepartmentofDefense(USUHSgrantnumberHU0001-15-2-0004).The39
contentsaresolelytheresponsibilityoftheauthorsanddonotnecessarilyrepresenttheviewsofthe40
DepartmentofHealthandHumanServices,NIMH,DepartmentoftheArmy,orDepartmentofDefense. 41
3
Abstract42
Background:Investigationsofdrinkingbehavioracrossmilitarydeploymentcyclesarescarce,andfew43
prospectivestudieshaveexaminedriskfactorsforpost-deploymentalcoholmisuse.Methods:44
Prevalenceofalcoholmisusewasestimatedamong4,645U.S.Armysoldierswhoparticipatedina45
longitudinalsurvey.Assessmentoccurred1-2monthsbeforesoldiersdeployedtoAfghanistanin201246
(T0),upontheirreturntotheU.S.(T1),3monthslater(T2),and9monthslater(T3).Weights-adjusted47
logisticregressionwasusedtoevaluateassociationsofhypothesizedriskfactorswithpost-deployment48
incidenceandpersistenceofheavydrinking(consuming5+alcoholicdrinksatleast1-2x/week)and49
AlcoholorSubstanceUseDisorder(AUD/SUD).Results:Prevalenceofpast-monthheavydrinkingatT0,50
T2,andT3was23.3%(SE=0.7%),26.1%(SE=0.8%),and22.3%(SE=0.7%);correspondingestimatesfor51
anybingedrinkingwere52.5%(SE=1.0%),52.5%(SE=1.0%),and41.3%(SE=0.9%).Greaterpersonallife52
stressduringdeployment(e.g.,relationship,family,orfinancialproblems)–butnotcombatstress–was53
associatedwithnewonsetofheavydrinkingatT2[perstandardscoreincrease:AOR=1.20,95%CI1.06-54
1.35,p=.003];incidenceofAUD/SUDatT2(AOR=1.54,95%CI1.25-1.89,p<.0005);andpersistenceof55
AUD/SUDatT2andT3(AOR=1.30,95%CI1.08-1.56,p=.005).Anybingedrinkingpre-deploymentwas56
associatedwithpost-deploymentonsetofHD(AOR=3.21,95%CI2.57-4.02,p<.0005)andAUD/SUD57
(AOR=1.85,95%CI1.27-2.70,p=.001).Conclusions:Alcoholmisuseiscommonduringthemonths58
precedingandfollowingdeployment.Timelyinterventionaimedatalleviating/managingpersonal59
stressorsorcurbingriskydrinkingmightreduceriskofalcohol-relatedproblemspost-deployment.60
61

4
Introduction62
Theburdenofalcoholmisuseonournation’spublichealth(Grantetal.,2015,Okoroetal.,63
2004,Sacksetal.,2015)extendstotheU.S.ArmedForces,wherehazardousdrinkingposesthreatsto64
boththehealthofindividualservicemembersandtroopreadiness(Brayetal.,2013,Hurt,2015).65
Militarypersonnelwhodrinkheavilysuffermoreaccidents/injuries;occupational,relational,andlegal66
problems;andproductivitylossthanothers(Mattikoetal.,2011).Moreover,alcoholmisuseis67
associatedwithmentaldisorders(Sampsonetal.,2015,Steinetal.,2017),suicidalideation(Mashetal.,68
2014),andsuicide(LeardMannetal.,2013)amongservicemembers.Improvedunderstandingofscope69
andriskfactorsmayhelpreducealcoholmisuseanditssequelaewithinthemilitarypopulation.70
Deploymenttoacombatzoneincreasesriskofalcoholmisuseamongcertainsubgroups71
(Jacobsonetal.,2008).Yetsystematiccharacterizationsofdrinkingbehavioracrossmilitarydeployment72
cyclesarescarce(Harbertsonetal.,2016,Hurt,2015);andfewprospectivestudieshaveinvestigated73
riskfactorsforpost-deploymentalcoholmisuse.AnotableexceptionfromtheMillenniumCohortStudy74
examinedalcoholmisuseamong>48,000previouslynon-deployedU.S.servicememberssurveyedin75
2001-2003and2004-2006(Jacobsonetal.,2008).Deploymentwithcombatexposureduringthetime76
betweensurveyswasassociatedwithonsetofbingedrinkingamongactive-dutypersonnel;andwith77
onsetofbingedrinking,heavydrinking,andalcohol-relatedproblemsamongReserve/NationalGuard78
personnel.Riskswerenotelevatedamongpersonnelwhoweredeployedbutnotexposedtocombat.79
Non-combat-relatedstressalsomaycontributetoriskforalcoholmisuse.Independentof80
combatstressexposure,personallifestressorswereassociatedwithsubsequentAlcoholUseDisorder81
(AUD)amongOhioNationalGuardmemberswhohaddeployedtoIraqorAfghanistan(Cerdaetal.,82
2014).Similarly,changesinalcoholconsumptionwereassociatedwithpersonallifeeventsbutnot83
deploymenttoIraq/AfghanistanamongUKmilitarypersonnel(Thandietal.,2015).Vulnerabilityto84
post-deploymentalcoholmisusealsomaydependonsocio-demographicandmilitaryservice85

5
characteristics(BoulosandZamorski,2016,Jacobsonetal.,2008)ormentalhealthfactorssuchas86
posttraumaticstressdisorder(PTSD)andmajordepressivedisorder(MDD),whichareconsistently87
linkedtoalcoholmisuseinmilitarysamples(Jacobsonetal.,2008,Kehleetal.,2012,Thandietal.,2015,88
Thomasetal.,2010,Steinetal.,2017).89
TheArmyStudytoAssessRiskandResilienceinServicemembers(ArmySTARRS)Pre/Post90
DeploymentStudy(Kessleretal.,2013a,Ursanoetal.,2014)affordsopportunitiestoexaminedrinking91
behavioracrossthedeploymentcycleandprospectiveriskfactorsforpost-deploymentalcoholmisuse.92
Weestimatedprevalenceofbingedrinking,heavydrinking,andalcoholorsubstanceusedisorder93
(AUD/SUD)amongsoldiersshortlybeforetheirdeploymenttoAfghanistan,andapproximately3and994
monthsfollowingtheirreturntotheU.S.Additionally,weevaluatedassociationsofsocio-demographic95
characteristics,priordeploymenthistory,combat/deploymentstress,personallifestressduring96
deployment(e.g.,relationship,family,financialproblems),pre-andperi-deploymentmentalhealth,and97
pre-deploymentbingedrinkingwithriskofincidenceandpersistenceofbothheavydrinkingand98
AUD/SUDat3monthspost-deployment.Tofurtherextendtheliteratureonmilitarydeploymentand99
alcoholmisuse,weutilizedthemultiplepost-deploymentPPDSassessmentstodeterminewhichofthe100
pre-andperi-deploymentriskfactorscontributedtopredictionofchronicheavydrinkingandAUD/SUD101
(i.e.,alcoholmisusethatwaspresentatboth3and9monthspost-deployment).102
Method103
ParticipantsandProcedures104
ThePre/PostDeploymentStudy(PPDS)isamulti-wavepanelsurveyofU.S.Armysoldiersin3105
BrigadeCombatTeams(BCTs).Baseline(T0)assessmentwasconductedduringQ1of2012,1-2months106
beforedeploymentoftheBCTstoAfghanistan.Follow-upassessmentoccurredwithin1monthofre-107
deploymentoftheBCTstotheU.S.(T1)andatapproximately3monthspost-deployment(T2)and9108
monthspost-deployment(T3).Participantsgavewritten,informedconsentfortheself-administered109
6
questionnaires(SAQs).BaselineSAQrespondentsalsowereaskedforconsentforcollectionofblood110
samples,linkageofArmyandDepartmentofDefense(DoD)administrativerecordstotheirSAQ111
responses,andcontactforparticipationinfutureassessments.Procedureswereapprovedbythe112
HumanSubjectsCommitteesofallcollaboratingorganizations.113
AtT0,9949soldierswerepresentfordutyinthe3BCTsand9488(95.3%)consentedtotheSAQ.114
Ofthosewhoconsented,8558(86.0%)providedcompletedataandconsentforArmy/DoDrecord115
linkage.ThesubpopulationofinterestforthisinvestigationwasT0participantswithcompleteSAQdata116
whosubsequentlydeployedtoAfghanistan(n=7742).Becausetheanalysisuseddatafromallwaves,the117
samplewasrestrictedtothe60.0%ofdeployedsoldierswhocompletedallfollow-ups(n=4645).118
Tomitigateimpactsofselectionfactorsandenhancegeneralizabilityofresultstothebroader119
populationofdeployedsoldiers,weightsweredevelopedandappliedinallanalyses(Heeringaetal.,120
2010).Combinedanalysisweightsinclude:(1)apropensity-basedweightingadjustmentforbaseline121
attritionduetoincompletesurveysandinabilitytolinktoadministrativedata(e.g.,duetoabsenceof122
soldierconsent);(2)post-stratificationtomaptheobservedsampleof7742eligiblePPDSsoldierstokey123
demographicandArmyservicecharacteristicsofsoldiersinthethreecombinedBCTsthatdeployedto124
AfghanistanaftertheT0interviewdates;and(3)apropensity-basedattritionadjustmenttoaccountfor125
thefactthat3097ofthe7742T0deployedcohortdidnothavecompletedatainoneormoreofthe3126
follow-upwaves.MoreinformationaboutweightingofArmySTARRSdatacanbeobtainedelsewhere127
(Kessleretal.,2013b).128
Measures129
Alcoholuseoutcomes.TheT0,T2,andT3surveysassessedfrequencyofalcoholbinges(5or130
moredrinksofalcoholonthesameday)duringthepast30days(never,lessthan1dayaweek,1-2days131
aweek,3-4daysaweek,andeveryornearlyeveryday;coded0-4).FollowingtheSubstanceAbuseand132
MentalHealthServicesAdministrationdefinitionsofbingedrinking(5ormorealcoholicdrinksonthe133

7
sameoccasiononatleast1dayinthepast30days)andheavydrinking(5ormoredrinks…5ormore134
daysinthepast30days),ratings>1werecodedpositiveforpast-monthBingeDrinking(BD)andratings135
>2werecodedpositiveforpast-monthHeavyDrinking(HD).Missingalcoholbingefrequencydatawere136
rare(<0.5%ateachwave)andcoded“0”toyieldconservativeestimates.137
DiagnosesofAUD/SUDwerebasedonitemsfromtheself-administeredCompositeInternational138
DiagnosticInterviewScreeningScales(CIDI-SC;KesslerandUstun,2004),whichassessednegative139
consequencesofalcoholand/ordruguseandsymptomsofdependence.Analgorithmemploying140
respondents’ratingswasusedtodiagnoseAUD/SUDandresultswerevalidatedagainststructured141
clinicalinterviewsintheArmySTARRSclinicalreappraisalstudy(Kessleretal.,2013c).IntheT0survey,142
respondentsendorsinganylifetimealcoholordruguseratedAUD/SUDitemsinreferencetotheperiod143
whentheyusedthemostalcohol(forthosewithnolifetimeuseofotherdrugs),drugs(forthosewith144
nolifetimeuseofalcohol),oralcoholordrugs(forthosewithlifetimealcoholandotherdruguse);145
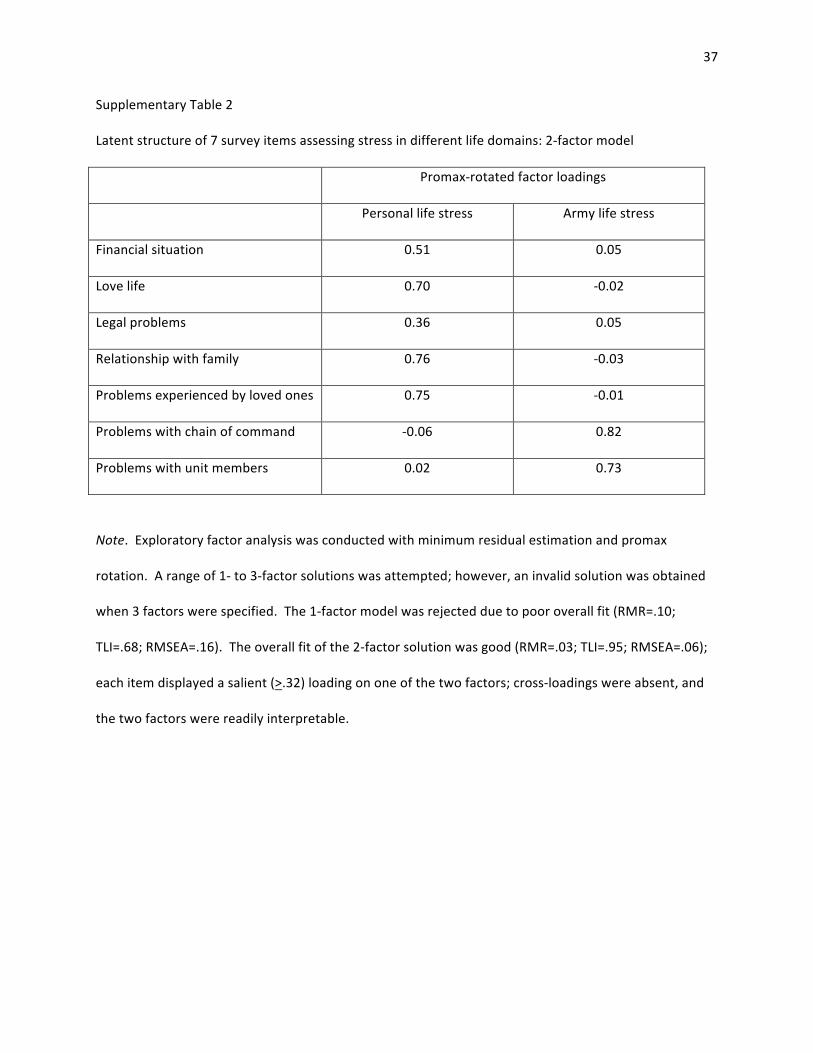
yieldinglifetimeAUD/SUDdiagnoses.ForT2andT3surveys,AUD/SUDitemswereratedinreferenceto146
thepast30days,yieldingpast-monthAUD/SUDdiagnoses.AUD/SUDwasnotassessedatT1.147
BecausethesurveysdidnotestablishwhetherAUD/SUDsymptomswereduetoalcoholordrug148
use(orboth),non-alcoholdrugusewasexaminedamongrespondentswithAUD/SUDatT2andatT3.149
TheT2andT3surveysassessedpast30-dayuseofmarijuana/hashish;spice/syntheticmarijuana;and150
anyotherillegaldrug;andpast30-daymisuseofprescriptionstimulants,tranquilizers/sedatives,and151
analgesics.AmongrespondentswithAUD/SUDatT2,10.0%endorseduseofanynon-alcoholdrug1-152
2x/weekormoreduringthemonthpriortoassessment.Thesameproportion(10.0%)ofthosewith153
AUD/SUDatT3endorsednon-alcoholdruguse1-2x/weekormoreinthemonthpriortotheT3154
assessment.ThesedatasuggestthatalargemajorityofAUD/SUDwasinfactAUD.155
8
Socio-demographicandArmyservicevariables.Age,sex,race,ethnicity,maritalstatus,highest156
educationaldegree,andnumberofpriordeploymentswereconsideredaspredictorsofalcoholmisuse.157
BCTwasadjustedforinallmodels.158
Combat/deploymentstressandlifestress.TheT1surveyinquiredhowmanytimessoldiers159
hadexperienced14highlystressful/traumaticeventsduringtheindexdeployment.Frequencyratings160
werediscretized(0/1or0/1/2)andsummedtocreateaDeploymentStressScale(DSS;range=0-16;161
SupplementaryTable1).TheT1surveyalsoassessedstressduringdeploymentthatarosefrom7162
domainsofsoldiers’lives(ratednone,mild,moderate,severe,orverysevere;coded0-4).Exploratory163
factoranalysisusingminimumresidualestimationandpromaxrotationindicatedthat2latentfactors164
bestexplainedthecovarianceoftheseratings(SupplementaryTable2).Twolifestressvariableswere165
thereforederived.ThefirstwasPersonalLifeStress(PLS),quantifiedasthesumofratingsofstressfrom166
finances,romanticrelationships,legalproblems,familyrelationships,andproblemsexperiencedby167
lovedones(range=0-20;Cronbach’sα=.76).ThesecondwasMilitaryLifeStress(MLS),orthesumof168
ratingsofstressfromproblemswithchainofcommandandfellowunitmembers(range=0-8;α=.73).For169
regressionanalysis,DSS,PLS,andMLSscoreswerestandardizedtofacilitateinterpretationofresults.170
Standardscoresof1.0and2.0wereconsidered“above-averagestress”and“highstress,”respectively.171
Pre-andperi-deploymentmentalhealth.Regressionmodelsincludedavariableindicating172
presenceversusabsenceofanypast-monthPTSD,majordepressiveepisode(MDE),generalizedanxiety173
disorder(GAD),orsuicidalideation(SI)atT0(Steinetal.,2015).PTSD,MDE,andGADdiagnoseswere174
basedonitemsfromtheCIDI-SC(KesslerandUstun,2004)andPTSDChecklist(Weathersetal.,1993).175
Validationofthesediagnoseswasthefocusofapriorreport(Kessleretal.,2013c).SIwasestablished176
withanexpandedself-reportversionoftheColumbiaSuicidalSeverityRatingScale(Posneretal.,2011).177
Modelsalsoincludedindicatorsofsoldiers’mentalhealthduringdeployment.TheT1survey178
contained5itemsassessingPTSDsymptomsduringdeployment;ratingsoftheseitemsweresummedto179

9
quantifyoverallseverityofPTSDsymptomsduringdeployment(range=0-20;α=.84).TheT1survey180
itemsassessingMDEandGADsymptoms(7itemstotal)hadexcellentinternalconsistency(α=.90)and181
weresummedtoquantifyoverallseverityofMDE/GADsymptomsduringdeployment(range=0-28).The182
peri-deploymentPTSDandMDE/GADsymptomseveritymeasureswerestandardizedpriortoregression183
analysistofacilitateinterpretationofresults.184
DataAnalysis185
Weightedprevalenceofthefollowingwascalculated:30-dayBDandHDatT0,T2,andT3;186
lifetimeAUD/SUDatT0;and30-dayAUD/SUDatT2andT3.Weights-adjustedlogisticregression187
modelswerefittoestimateassociationsofhypothesizedriskfactorswithonsetandpersistenceofHD188
andAUD/SUD.ModelsofonsetofHDwereestimatedforsoldierswhodeniedpast-monthHDatT0;189
modelsofonsetofAUD/SUDwereestimatedforsoldierswithoutlifetimeAUD/SUDatT0,and190
persistencemodelswereestimatedforsoldierswhoendorsedtheoutcomeunderconsiderationatT0.191
OnsetandpersistenceofHDandAUD/SUDatT2weretheprimaryoutcomes.Toascertainwhichrisk192
factorswereassociatedwithchronicpost-deploymentalcoholmisuse,HDandAUD/SUDthatwere193
presentatbothT2andT3wereconsideredsecondaryoutcomes.194
Thefollowingindependentvariableswereincludedinallmodels:sex,age,race,ethnicity,195
education,maritalstatus,BCT,numberofpriordeployments,andpre-deploymentemotionaldisorder196
(fromT0);andcombat/deploymentstress,personallifestress,militarylifestress,peri-deploymentPTSD197
symptomseverity,andperi-deploymentMDE/GADsymptomseverity(fromT1).Pre-deploymentpast-198
monthBDwasincludedinmodelsofnew-onsetHDandAUD/SUD.199
PPDSdataareclustered(byBCTandadministrationsession)andweighted;therefore,the200
design-basedTaylorserieslinearizationmethodwasusedtoestimatestandarderrors.Multivariable201
significancewasexaminedusingdesign-basedWaldΧ2tests.Two-tailedp<.05wasconsidered202
significant.AnalyseswereconductedusingRVersion3.3.2(RCoreTeam,2013).203

10
Results204
Descriptivefindings205
Weightedprevalenceofpast-monthbingedrinking,heavydrinking,andAUD/SUDisshownin206
Table1.MorethanhalfofsoldiersendorsedBDatpre-deploymentand3monthspost-deployment;207
lowerprevalencewasobserved9monthspost-deployment.TherateofHDwasrelativelystable,with208
approximatelyone-quarterofsoldiersendorsingpast-monthHDateachwave.Past-monthAUD/SUD209
wasslightlymoreprevalentat9monthspost-deploymentthanat3monthspost-deployment.Past-210
monthAUD/SUDwasnotassessedatthepre-deploymentassessment;however,prevalenceoflifetime211
AUD/SUDatT0was20.4%(SE=0.7%).212
DemographicdifferencesinprevalenceofBD,HD,andAUD/SUDwereexaminedandfullresults213
appearinSupplementaryTables3and4.WomenexhibitedlowerprevalenceofBD,HD,andAUD/SUD214
thanmenatallwaves(seeFigure1forBDandHDresults).RelativetoWhitesoldiers,BlackandAsian215
soldiersdisplayedlowerprevalenceofBD(allwaves),HD(allwavesexceptT3),andlifetimeAUD/SUDat216
T0.WhereasotheragegroupsexhibitedstableordecliningratesofBDandHDfrompre-deploymentto217
9monthspost-deployment,theyoungestsoldiers(aged18-20)displayedsubstantialincreasesinBDand218
HDoverthesameperiod(seeFigure2forHDresults).219
Nearly1in10soldiers(9.6%,SE=0.4%)hadpast-monthPTSD,MDE,GAD,orSIatT0.On220
average,soldierswereexposedto4combat/deploymentstressorsduringtheirdeploymentto221
Afghanistan[meanDSS=3.98,SD=2.72,observedrange=0-15].Notethatthisvaluerepresentsdistinct222
typesofcombat/deploymentstressorsencountered–nottotalnumberofstressfulexperiences,which223
couldhavebeenhigherinnumber(seeSupplementaryTable1forDSSscoringdetails).Reportedlevels224
ofpersonallifestress,militarylifestress,PTSDsymptoms,andMDE/GADsymptomsduringdeployment225
weregenerallymild[meanPLS=2.68,SD=2.68,range=0-20;meanMLS=1.73,SD=1.89,range=0-8;mean226
T1PTSDscore=3.18,SD=3.63,range=0-20;meanT1MDE/GADscore=5.56,SD=5.20,range=0-28].227
228

11
Riskfactorsforonsetandpersistenceofheavydrinking229
New-onsetofHDpost-deployment.Malesex,youngerage,never-marriedstatus,pre-230
deploymentBD,andgreaterpersonallifestressduringdeploymentwereassociatedwithincreasedodds231
ofonsetofHDatT2amongsoldierswhodeniedHDatT0(Table2).Theadjustedodds-ratio232
characterizingtheassociationofpersonallifestresswithHDonsetindicatesthatsoldierswithabove-233
average(z=1.00)andhighpersonalstress(z=2.00)duringdeploymentexhibited20%and44%increased234
riskofpost-deploymentHDonset,relativetothosewithaveragepersonalstressduringdeployment.235
Otherdemographiccharacteristics,priordeployments,combat/deploymentstress,militarylifestress,236
andpre-andperi-deploymentmentalhealthfactorswerenotsignificantlyrelatedtoonsetofHD.237
Most(62.0%)newHDobservedatT2hadremittedbyT3–i.e.,frequencyofalcoholbinges238
droppedbackbelowthethresholdforHD.WhenonsetofchronicHD(presentatT2andT3)was239
specifiedastheoutcome,similarriskfactorswereevident.Malesex,youngerage,nevermarried240
status,andpre-deploymentBDweresignificantlyassociatedwithonsetofchronicHD.However,the241
associationofpersonallifestressduringdeploymentwithonsetofchronicHDwasnotstatistically242
significant(p=.079;Table2).243
PersistenceofHDfrompre-to-postdeployment.Thehypothesizedriskfactorsgenerallylacked244
substantiveassociationswithpersistenceofHDfrompre-topost-deployment.Onlyperi-deployment245
MDE/GADsymptomswereassociatedwithpersistenceofHDatT2amongsoldierswhoendorsedHDat246
T0(Table2).Soldierswithabove-average(z=1.00)andhighMDE/GADsymptoms(z=2.00)during247
deploymentexhibited20%and43%increasedriskofHDpersistenceatT2,relativetothosewith248
averagedistressduringdeployment.MDE/GADsymptomswerenotassociatedwithchronicpersistence249
ofHDatT2andT3(p=.13;Table2).250
251

12
RiskfactorsforincidenceandpersistenceofAUD/SUD252
IncidenceofAUD/SUDpost-deployment.Pre-deploymentBDandgreaterpersonallifestress253
duringdeploymentwereassociatedwithincreasedriskofAUD/SUDatT2amongsoldierswithout254
lifetimeAUD/SUDatT0(Table3).Relativetoaveragepersonalstressduringdeployment,above-255
averagepersonalstresswasassociatedwith54%increasedriskofincidenceofAUD/SUDandhigh256
personalstresswasassociatedwithmorethandoubled(AOR=2.36)oddsofincidenceofAUD/SUD.257
Nearlytwo-thirds(64.0%)ofnew-onsetAUD/SUDpersistedatT3.Thesamefactors–pre-258
deploymentBDandpersonalstressduringdeployment–wereassociatedwithincreasedriskof259
incidenceofchronicAUD/SUD(i.e.,atT2andT3;Table3).OddsofincidenceofchronicAUD/SUDwere260
72%higheramongsoldierswithabove-averagepersonalstressandnearlytripled(AOR=2.94)for261
soldierswithhighpersonalstress,relativetothosewithaveragepersonalstressduringdeployment.262
PersistenceofAUD/SUDfrompre-topost-deployment.Amongsoldierswithlifetime263
AUD/SUDatT0,onlygreatermilitarylifestressduringdeploymentwassignificantlyassociatedwith264
persistenceofthedisorderatT2(Table3).Comparedtosoldierswithaveragemilitarylifestress,odds265
ofpersistenceofAUD/SUDatT2were20%and45%higheramongsoldierswithabove-averageandhigh266
militarylifestress,respectively.Theassociationofpersonallifestressseveritywithpersistenceof267
AUD/SUDatT2wasnotstatisticallysignificant(p=.062);however,greaterpersonallifestressduring268
deploymentwassignificantlyassociatedwithchronicpersistenceofAUD/SUDatT2andT3(Table3).269
Relativetothosewithaveragepersonallifestressduringdeployment,oddsofpersistenceofAUD/SUD270
atbothT2andT3were30%and69%higheramongsoldierswithabove-averageandhighpersonal271
stress,respectively.272
Discussion273
Thisprospective,longitudinalstudyofU.S.ArmysoldiersfromthreeBrigadeCombatTeams274
revealsassociationsbetweenpersonallifestressduringdeploymentandarangeofpost-deployment275

13
alcoholmisuseoutcomes.AmongsoldierswithnolifetimeAUD/SUDpre-deployment,highlevelsof276
personallifestressduringdeployment(definedasstandardscoreof2.00orhigheronthePLSmeasure)277
wereassociatedwithdoubledriskofincidenceofAUD/SUDat3monthspost-deployment;andnearly278
tripledriskofincidenceofchronicAUD/SUDobservedat3and9monthspost-deployment.Inaddition,279
personallifestressduringdeploymentpredictedonsetofheavydrinkingamongsoldierswhodenied280
drinkingheavilypre-deploymentandchronicpersistenceofAUD/SUD(atboth3and9monthspost-281
deployment)amongsoldierswiththedisorderearlierinlife.Bingedrinkingshortlybeforedeployment282
alsoportendedonsetofmoreseriousalcoholmisusepost-deployment;reflectedintripledoddsofonset283
ofheavydrinkingandnearlydoubledoddsofincidenceofAUD/SUD.Inadditiontopredictingthese284
outcomesatasinglepost-deploymenttimepoint,pre-deploymentbingedrinkingpredictedonsetof285
chronicheavydrinkingandAUD/SUDthatwerepresentatboth3and9monthspost-deployment.286
ThePPDSsurveydidnotpermitdifferentialdiagnosisofAUDversusSUDduetonon-alcohol287
druguse.AvailableevidencesuggeststhelargemajorityofAUD/SUDinthissamplewasinfactAUD;288
only10%ofrespondentswithAUD/SUDateitherpost-deploymentassessmentendorsedregularuseof289
anynon-alcoholdrug.PriorworkalsoindicatesthatAUDismorecommonthandrugabuse/dependence290
amongservicemembers(Finketal.,2016).Chronicity(persistenceatT3)oftwo-thirdsofAUD/SUDwith291
post-deploymentonsetarguesagainstcharacterizationofthesenewdisordersastransientreactions;292
andmayreflectmoreenduringstress/adjustmentdemandsassociatedwithdeploymenttoacombat293
zoneandsubsequentre-deploymenttotheU.S.WhilechronicitywasthenormforAUD/SUDwithpost-294
deploymentonset,aminorityofnew-onsetheavydrinkingpersistedatT3.Consideredtogether,these295
findingssuggestthatpresenceofabuseordependencesymptomsshortlyfollowingreturnfrom296
deployment–asopposedtoincreasedalcoholconsumptionperse–meritgreatestconcern.297
Theabsenceofassociationsofcombatstressseveritywiththealcoholmisuseoutcomesis298
counterintuitive,butlargelyconvergeswithresultsoftwootherstudiesthatjointlyexaminedpredictive299

14
effectsofcombatandpersonalstress(Cerdaetal.,2014,Thandietal.,2015).Althoughunderlying300
explanationsforthegreaterapparentinfluenceofpersonal(versuscombat)stressorswerenotexplored301
inthecurrentanalysis,somepossibilitiesmeritingfuturestudyare:continuanceofpersonalstressors302
intothepost-deploymentperiod(versusoffsetofdeploymentstress);soldierperceptionofdrinkingasa303
moreeffectivecopingtoolforeverydaystressthanforcombatstress;concentrationofother304
vulnerabilitycharacteristics(e.g.,traitspredisposingindividualstoalcoholmisuse)amongsoldierswith305
greaterpersonalstress;andincreasedresilienceamongthosewithlowstressarisingfromtheirpersonal306
lives(e.g.,relationshipsarestable/supportive).307
Whileweconcludethatseverityofcombatstresswasnotindependentlyassociatedwithpost-308
deploymentalcoholmisuseinthiscohort,wemakenoinferenceregardingtheeffectsofdeployment309
(withorwithoutcombatexposure)perseonriskofalcoholmisuse.Apreviouslarge-scaleprospective310
analysisfromtheMillenniumCohortStudy(MCS)addressedthatquestionandfoundthat,relativeto311
notdeploying,deploymentwithcombatexposure(butnotdeployingwithoutcombatexposure)was312
associatedwithincreasedriskofonsetofbingedrinkingamongactive-dutypersonnel;andwithonsetof313
bingedrinking,heavydrinking,andalcohol-relatedproblemsamongReserve/NationalGuardpersonnel314
(e.g.,Jacobsonetal.,2008).Wecannotmakesimilarcomparisons,asallsoldiersinthecurrentstudy315
deployedtoAfghanistan–withmostreportingexposuretoseveralcombatstressors.Futureresearch316
shouldexaminetheeffectsofpersonallifestressandotherriskfactorsforalcoholmisuseinsamplesof317
servicemembersdeployedtonon-combatpositions.318
Contrarytoexpectation,pre-deploymentemotionaldisorderwasnotassociatedwithincreased319
riskofpost-deploymentheavydrinkingorAUD/SUD.Peri-deploymentPTSDsymptomsalsolacked320
associationswiththealcoholmisuseoutcomes;andperi-deploymentMDE/GADsymptomsonly321
exhibitedanassociationwithpersistenceofHDfrompre-deploymentto3monthspost-deployment.322
TheselargelynullfindingsdivergefromresultsofpriorstudiesthatfoundrelationshipsbetweenPTSD,323

15
MDE,andalcoholmisuse.Among358NationalGuardsoldiersdeployedtoIraq,PTSDsymptomseverity324
wasassociatedwithincreasedriskofnew-onsetAUD(Kehleetal.,2012).BaselinesymptomsofPTSD325
and/orMDEcontributedtopredictionofincidenceofalcohol-relatedproblems(endorsing1ormore326
indicatorsofalcoholabuse)–butnotincidenceofbingeorheavydrinking–intheaforementionedMCS327
investigationthatincludedbothdeployedandnon-deployedservicemembers(Jacobsonetal.,2008).328
Disparitiesinstudyresultsmayreflectdifferencesinsamplecharacteristicsorintheconsiderationor329
operationalizationofmentalhealthandotherpredictorvariables.Althoughrobustpredictiveeffectsof330
mentalhealthvariableswerenotfoundinthisanalysis,alcoholmisusedisplaysconsistentcross-331
sectionalassociationswithPTSD,MDE,andotherdisordersinmilitarysamples(Steinetal.,2017;332
Thomasetal.,2010);thus,co-occurringmentalhealthproblemsmustbeconsideredinclinical333
interventionsandothereffortstoreducehazardousdrinkingandAUD/SUD.334
Male,younger,andnever-marriedsoldiersdisplayedincreasedoddsofonsetofheavydrinking335
post-deployment,convergingwithpreviousfindingsofelevatedriskofhazardousdrinkinginthese336
subgroups(BoulosandZamorski,2016,Jacobsonetal.,2008).Themarkedincreaseinriskydrinking337
pre-topost-deploymentamongsoldiersaged18-20distinguishesthemfromothersandsignalsthat338
youngsoldierswhodeploy(particularlythosepossessingotherriskfactors)maybeasubgroupto339
considerfortargetedpreventionefforts,eveniftheriseispartlyattributabletosomeofthemattaining340
legaldrinkingagebetweenassessments.341
Moregenerally,thisstudyconveysinformationregardingthescopeofalcoholmisuseamong342
Armysoldiersshortlybeforeandatmultiplepointsaftertheirdeploymenttoacombatzone.343
Approximatelyhalfofrespondentsreportedbingedrinkingandnearlyone-quarterendorsedheavy344
drinkingduringthemonthbeforepre-deploymentassessment.Althoughdifferencesinstudydesign345
precludedefinitivecomparisons,pre-deploymentprevalenceofheavydrinkinginthissample(23%)346
16
appearssimilartoprevalenceofarelatedoutcome(regularbingedrinking;27%)amongNavy/Marine347
Corpspersonnelpreparingtodeploy(Harbertsonetal.,2016).348
TypicalschedulingoftheArmy’sPost-DeploymentHealthReassessment(PDHRA)placesitin349
closestproximitytothePPDST2assessment.Giventhatsoldiersendorsingheavydrinkingwouldlikely350
scoreinthehigh-riskrange,itisstrikingthatT2prevalenceofheavydrinkingwastwicethereported351
rateof“highriskforalcoholabuse”amongPDHRArespondentsduring2008-2014(Hurt,2015).This352
maysignalunder-estimationofthetruescopeofalcoholmisusewhennon-confidentialformsof353
assessmentsuchasthePDHRAareused(Warneretal.,2011).354
Finally,substantiallyhigherratesofpast-monthbingeandheavydrinkingwereobservedamong355
PPDSrespondents(atallwaves)comparedtoacohortofnewsoldiers(Steinetal.,2017).Higher356
prevalenceofhazardousdrinkingamongPPDSrespondentscouldreflectincreasedalcoholmisusewith357
longerArmytenure,selectionoflightdrinkers/abstainersoutofArmyservice,ordifferencesin358
demographiccompositionorothercharacteristicsofthetwosamples.Potentialcontributionsofthese359
factorsshouldbeexploredinfutureresearch.360
Novelaspectsofthecurrentinvestigationincludeavailabilityofoutcomedataatboth3and9361
monthspost-deployment;inclusionofnumberofpriordeploymentsasapotentialriskfactor;increased362
granularityinmeasurementofcombatstressexposure(0-16indexversusdichotomouscharacterization363
ofdeploymentstatusorcombatexposure);andjointconsiderationofarangeofperi-deployment364
stressorsandsymptomsinrelationtopost-deploymentheavydrinkingandAUD/SUD.365
Thestudyalsohasseverallimitations.ConclusivedifferentialdiagnosisofAUDversusSUDwas366
notpossible.Retrospectiveself-reportdataarevulnerabletorecallandresponsebiases;inthecaseof367
alcoholanddruguseassessment,under-reportingmayoccur.Estimatesofnon-alcoholdrugusemight368
bemoresusceptibletothisbiasthanestimatesofalcoholusegivenfearofrepercussionsforadmitting369
druguseinlightoftheArmy’szero-tolerancepolicy.Under-reportingofbothalcoholanddruguse370

17
couldhavebeenaccentuatedatthepre-deploymentassessment,duetoheighteneddesirestoappear371
“combat-ready”.372
Weightswereappliedtomitigateimpactsofattritionandtoenhancegeneralizabilitytothe373
broaderpopulationofdeployedsoldiers.Nevertheless,selectionfactorsmayhaveinfluencedthe374
results(i.e.,soldierswhocompletedallassessmentsmayhavedifferedfromthelargerpopulationof375
soldiersonvariablesnotadjustedforviaweightsorcovariates).TheT0surveydidnotassesslifetime376
HD;thus,new-onsetofHDcouldonlybedefinedinrelationtodrinkingduringthemonthbeforeT0377
assessment.Finally,lowrepresentationlimitedpowertodetectriskdifferencesforcertainsubgroups378
(e.g.,females).Moreresearchisneededtoinvestigatewhethersexdifferencesarepresentwithrespect379
toriskfactorsforpost-deploymentalcoholmisuse.380
Inconclusion,pre-andpost-deploymentalcoholmisusewascommonamongsoldiersfrom3381
U.S.ArmyBrigadeCombatTeamsthatdeployedtoAfghanistan.Severityofpersonallifestressduring382
deployment–butnotseverityofcombatstress–wasassociatedwithpost-deploymentonsetofheavy383
drinkingandincidenceandpersistenceofAUD/SUD.Pre-deploymentbingedrinkingalsopredicted384
onsetofheavydrinkingandAUD/SUDpost-deployment.Detectionofriskydrinkingoccurringshortly385
beforedeploymentwouldprovideanopportunityforearlyinterventiontopreventonsetofmoresevere386
alcohol-relatedproblems.Additionally,effortstoidentifyandassistsoldiersexperiencingsubstantial387
personallifestressduringdeploymentcouldprovebeneficialnotonlyforreductionofalcoholmisuse,388
butpossiblyforoverallmentalhealth.389
390

18
Acknowledgments391
TheArmySTARRSTeamconsistsofCo-PrincipalInvestigators:RobertJ.Ursano,MD(UniformedServices392
UniversityoftheHealthSciences)andMurrayB.Stein,MD,MPH(UniversityofCaliforniaSanDiegoand393
VASanDiegoHealthcareSystem)394
SitePrincipalInvestigators:StevenHeeringa,PhD(UniversityofMichigan),JamesWagner,PhD395
(UniversityofMichigan),andRonaldC.Kessler,PhD(HarvardMedicalSchool)396
Armyliaison/consultant:KennethCox,MD,MPH(USAPHC(Provisional))397
Otherteammembers:PabloA.Aliaga,MA(UniformedServicesUniversityoftheHealthSciences);COL398
DavidM.Benedek,MD(UniformedServicesUniversityoftheHealthSciences);LauraCampbell-Sills,PhD399
(UniversityofCaliforniaSanDiego);Chia-YenChenDSc(HarvardMedicalSchool);CarolS.Fullerton,PhD400
(UniformedServicesUniversityoftheHealthSciences);NancyGebler,MA(UniversityofMichigan);Joel401
Gelernter(YaleUniversity);RobertK.Gifford,PhD(UniformedServicesUniversityoftheHealth402
Sciences);PaulE.Hurwitz,MPH(UniformedServicesUniversityoftheHealthSciences);SoniaJain,PhD403
(UniversityofCaliforniaSanDiego);Tzu-ChegKao,PhD(UniformedServicesUniversityoftheHealth404
Sciences);LisaLewandowski-Romps,PhD(UniversityofMichigan);HollyHerbermanMash,PhD405
(UniformedServicesUniversityoftheHealthSciences);JamesE.McCarroll,PhD,MPH(Uniformed406
ServicesUniversityoftheHealthSciences);JamesA.Naifeh,PhD(UniformedServicesUniversityofthe407
HealthSciences);TszHinHinzNg,MPH(UniformedServicesUniversityoftheHealthSciences);Matthew408
K.Nock,PhD(HarvardUniversity);NancyA.Sampson,BA(HarvardMedicalSchool);CDRPatcho409
Santiago,MD,MPH(UniformedServicesUniversityoftheHealthSciences);JordanW.Smoller,MD,ScD410
(HarvardMedicalSchool);andAlanM.Zaslavsky,PhD(HarvardMedicalSchool).411
412
FinancialSupport:ArmySTARRSwassponsoredbytheDepartmentoftheArmyandfundedunder413
cooperativeagreementnumberU01MH087981(2009-2015)withtheU.S.DepartmentofHealthand414

19
HumanServices,NationalInstitutesofHealth,NationalInstituteofMentalHealth(NIH/NIMH).415
Subsequently,STARRS-LSwassponsoredandfundedbytheDepartmentofDefense(USUHSgrant416
numberHU0001-15-2-0004).Thecontentsaresolelytheresponsibilityoftheauthorsanddonot417
necessarilyrepresenttheviewsoftheDepartmentofHealthandHumanServices,NIMH,Departmentof418
theArmy,orDepartmentofDefense.419
420
ConflictofInterest:Dr.SteinhasinthepastthreeyearsbeenaconsultantforActelion,Dart421
Neuroscience,HealthcareManagementTechnologies,Janssen,OxeiaBiopharmaceuticals,Pfizer,422
ResilienceTherapeutics,andTonixPharmaceuticals.Inthepast3years,Dr.Kesslerreceivedsupportfor423
hisepidemiologicalstudiesfromSanofiAventis;wasaconsultantforJohnson&JohnsonWellnessand424
Prevention,Shire,Takeda;andservedonanadvisoryboardfortheJohnson&JohnsonServicesInc.Lake425
NonaLifeProject.Kesslerisaco-ownerofDataStat,Inc.,amarketresearchfirmthatcarriesout426
healthcareresearch.Theremainingauthorshavenofinancialdisclosures.427
428
Ethicalstandards:Theauthorsassertthatallprocedurescontributingtothisworkcomplywiththe429
ethicalstandardsoftherelevantnationalandinstitutionalcommitteesonhumanexperimentationand430
withtheHelsinkiDeclarationof1975,asrevisedin2008.431
432

20
References433434
Boulos,D.&Zamorski,M.A.(2016).ContributionofthemissioninAfghanistantotheburdenofpast-435
yearmentaldisordersinCanadianArmedForcespersonnel,2013.CanadianJournalofPsychiatry61,436
64S-76S.437
Bray,R.M.,Brown,J.M.&Williams,J.(2013).Trendsinbingeandheavydrinking,alcohol-related438
problems,andcombatexposureintheU.S.military.SubstanceUse&Misuse48,799-810.439
Cerda,M.,Richards,C.,Cohen,G.H.,Calabrese,J.R.,Liberzon,I.,Tamburrino,M.,Galea,S.&Koenen,440
K.C.(2014).CivilianstressorsassociatedwithalcoholusedisordersintheNationalGuard.American441
JournalofPreventiveMedicine47,461-6.442
Fink,D.S.,Calabrese,J.R.,Liberzon,I.,Tamburrino,M.B.,Chan,P.,Cohen,G.H.,Sampson,L.,Reed,443
P.L.,Shirley,E.,Goto,T.,D'Arcangelo,N.,Fine,T.&Galea,S.(2016).Retrospectiveage-of-onsetand444
projectedlifetimeprevalenceofpsychiatricdisordersamongU.S.ArmyNationalGuardsoldiers.Journal445
ofAffectiveDisorders202,171-7.446
Grant,B.F.,Goldstein,R.B.,Saha,T.D.,Chou,S.P.,Jung,J.,Zhang,H.,Pickering,R.P.,Ruan,W.J.,447
Smith,S.M.,Huang,B.&Hasin,D.S.(2015).EpidemiologyofDSM-5AlcoholUseDisorder:Results448
FromtheNationalEpidemiologicSurveyonAlcoholandRelatedConditionsIII.JAMAPsychiatry72,757-449
66.450
Harbertson,J.,Hale,B.R.,Watkins,E.Y.,Michael,N.L.&Scott,P.T.(2016).Pre-deploymentalcohol451
misuseamongshipboardactive-dutyU.S.militarypersonnel.AmericanJournalofPreventiveMedicine452
51,185-94.453
21
Heeringa,S.G.,West,B.T.&Berglund,P.A.(2010).Appliedsurveydataanalysis.ChapmanandHall:454
BocaRaton,FL.455
Hurt,L.(2015).Post-deploymentscreeningandreferralforriskyalcoholuseandsubsequentalcohol-456
relatedandinjurydiagnoses,activecomponent,U.S.ArmedForces,2008-2014.MedicalSurveillance457
MonthlyReport22,7-13.458
Jacobson,I.G.,Ryan,M.A.,Hooper,T.I.,Smith,T.C.,Amoroso,P.J.,Boyko,E.J.,Gackstetter,G.D.,459
Wells,T.S.&Bell,N.S.(2008).Alcoholuseandalcohol-relatedproblemsbeforeandaftermilitary460
combatdeployment.JournaloftheAmericanMedicalAssociation300,663-75.461
Kehle,S.M.,Ferrier-Auerbach,A.G.,Meis,L.A.,Arbisi,P.A.,Erbes,C.R.&Polusny,M.A.(2012).462
PredictorsofpostdeploymentalcoholusedisordersinNationalGuardsoldiersdeployedtoOperation463
IraqiFreedom.PsychologyofAddictiveBehaviors26,42-50.464
Kessler,R.C.,Colpe,L.J.,Fullerton,C.S.,Gebler,N.,Naifeh,J.A.,Nock,M.K.,Sampson,N.A.,465
Schoenbaum,M.,Zaslavsky,A.M.,Stein,M.B.,Ursano,R.J.&Heeringa,S.G.(2013a).Designofthe466
ArmyStudytoAssessRiskandResilienceinServicemembers(ArmySTARRS).InternationalJournalof467
MethodsinPsychiatricResearch22,267-75.468
Kessler,R.C.,Heeringa,S.G.,Colpe,L.J.,Fullerton,C.S.,Gebler,N.,Hwang,I.,Naifeh,J.A.,Nock,M.469
K.,Sampson,N.A.,Schoenbaum,M.,Zaslavsky,A.M.,Stein,M.B.,&Ursano,R.J.(2013b).Response470
bias,weightingadjustments,anddesigneffectsintheArmyStudytoAssessRiskandResiliencein471
Servicemembers(ArmySTARRS).InternationalJournalofMethodsinPsychiatricResearch22,288-302.472
Kessler,R.C.,Santiago,P.N.,Colpe,L.J.,Dempsey,C.L.,First,M.B.,Heeringa,S.G.,Stein,M.B.,473
Fullerton,C.S.,Gruber,M.J.,Naifeh,J.A.,Nock,M.K.,Sampson,N.A.,Schoenbaum,M.,Zaslavsky,474

22
A.M.&Ursano,R.J.(2013c).ClinicalreappraisaloftheCompositeInternationalDiagnosticInterview475
ScreeningScales(CIDI-SC)intheArmyStudytoAssessRiskandResilienceinServicemembers(Army476
STARRS).InternationalJournalofMethodsinPsychiatricResearch22,303-21.477
Kessler,R.C.&Ustun,T.B.(2004).TheWorldMentalHealth(WMH)SurveyInitiativeVersionofthe478
WorldHealthOrganization(WHO)CompositeInternationalDiagnosticInterview(CIDI).International479
JournalofMethodsinPsychiatricResearch13,93-121.480
LeardMann,C.A.,Powell,T.M.,Smith,T.C.,Bell,M.R.,Smith,B.,Boyko,E.J.,Hooper,T.I.,481
Gackstetter,G.D.,Ghamsary,M.&Hoge,C.W.(2013).Riskfactorsassociatedwithsuicideincurrent482
andformerUSmilitarypersonnel.JournaloftheAmericanMedicalAssociation310,496-506.483
Mash,H.B.,Fullerton,C.S.,Ramsawh,H.J.,Ng,T.H.,Wang,L.,Kessler,R.C.,Stein,M.B.&Ursano,R.484
J.(2014).RiskforsuicidalbehaviorsassociatedwithalcoholandenergydrinkuseintheUSArmy.Social485
PsychiatryandPsychiatricEpidemiology49,1379-87.486
Mattiko,M.J.,Olmsted,K.L.,Brown,J.M.&Bray,R.M.(2011).Alcoholuseandnegative487
consequencesamongactivedutymilitarypersonnel.AddictiveBehaviors36,608-14.488
Okoro,C.A.,Brewer,R.D.,Naimi,T.S.,Moriarty,D.G.,Giles,W.H.&Mokdad,A.H.(2004).Binge489
drinkingandhealth-relatedqualityoflife:Dopopularperceptionsmatchreality?AmericanJournalof490
PreventiveMedicine26,230-3.491
Posner,K.,Brown,G.K.,Stanley,B.,Brent,D.A.,Yershova,K.V.,Oquendo,M.A.,Currier,G.W.,492
Melvin,G.A.,Greenhill,L.,Shen,S.&Mann,J.J.(2011).TheColumbia-SuicideSeverityRatingScale:493
initialvalidityandinternalconsistencyfindingsfromthreemultisitestudieswithadolescentsandadults.494
AmericanJournalofPsychiatry168,1266-77.495

23
RCoreTeam(2013).R:Alanguageandenvironmentforstatisticalcomputing.RFoundationfor496
StatisticalComputing:Vienna,Austria.497
Sacks,J.J.,Gonzales,K.R.,Bouchery,E.E.,Tomedi,L.E.&Brewer,R.D.(2015).2010nationaland498
statecostsofexcessivealcoholconsumption.AmericanJournalofPreventiveMedicine49,e73-9.499
Sampson,L.,Cohen,G.H.,Calabrese,J.R.,Fink,D.S.,Tamburrino,M.,Liberzon,I.,Chan,P.&Galea,S.500
(2015).Mentalhealthovertimeinamilitarysample:theimpactofalcoholusedisorderontrajectories501
ofpsychopathologyafterdeployment.JournalofTraumaticStress28,547-55.502
Stein,M.B.,Campbell-Sills,L.,Gelernter,J.,He,F.,Heeringa,S.G.,Nock,M.K.,Sampson,N.A.,Sun,503
X.,Jain,S.,Kessler,R.C.,Ursano,R.J.&Army,S.C.(2017).Alcoholmisuseandco-occurringmental504
disordersamongnewsoldiersintheU.S.Army.Alcoholism:ClinicalandExperimentalResearch41,139-505
148.506
Stein,M.B.,Kessler,R.C.,Heeringa,S.G.,Jain,S.,Campbell-Sills,L.,Colpe,L.J.,Fullerton,C.S.,Nock,507
M.K.,Sampson,N.A.,Schoenbaum,M.,Sun,X.,Thomas,M.L.,Ursano,R.J.&Army,S.c.(2015).508
Prospectivelongitudinalevaluationoftheeffectofdeployment-acquiredtraumaticbraininjuryon509
posttraumaticstressandrelateddisorders:resultsfromtheArmyStudytoAssessRiskandResiliencein510
Servicemembers(ArmySTARRS).AmericanJournalofPsychiatry172,1101-11.511
Thandi,G.,Sundin,J.,Ng-Knight,T.,Jones,M.,Hull,L.,Jones,N.,Greenberg,N.,Rona,R.J.,Wessely,512
S.&Fear,N.T.(2015).AlcoholmisuseintheUnitedKingdomArmedForces:Alongitudinalstudy.Drug513
andAlcoholDependence156,78-83.514

24
Thomas,J.L.,Wilk,J.E.,Riviere,L.A.,McGurk,D.,Castro,C.A.&Hoge,C.W.(2010).Prevalenceof515
mentalhealthproblemsandfunctionalimpairmentamongactivecomponentandNationalGuard516
soldiers3and12monthsfollowingcombatinIraq.ArchivesofGeneralPsychiatry67,614-23.517
Ursano,R.J.,Colpe,L.J.,Heeringa,S.G.,Kessler,R.C.,Schoenbaum,M.,Stein,M.B.&Army,S.c.518
(2014).TheArmyStudytoAssessRiskandResilienceinServicemembers(ArmySTARRS).Psychiatry77,519
107-19.520
Warner,C.H.,Appenzeller,G.N.,Grieger,T.,Belenkiy,S.,Breitbach,J.,Parker,J.,Warner,C.M.&521
Hoge,C.(2011).Importanceofanonymitytoencouragehonestreportinginmentalhealthscreening522
aftercombatdeployment.ArchivesofGeneralPsychiatry68,1065-71.523
Weathers,F.,Litz,B.,Herman,D.,Huska,J.&Keane,T.(1993).ThePTSDChecklist(PCL):Reliability,524
Validity,andDiagnosticUtility.MeetingoftheInternationalSocietyforTraumaticStressStudies.San525
Antonio,TX.526
527

25
Table1
Weightedprevalenceofpast-monthbingedrinking,heavydrinking,andAUD/SUDamongU.S.Army
soldierspre-andpost-deployment(n=4645)
Pre-
deployment(T0)
3monthspost-
deployment(T2)
9monthspost-
deployment(T3)
BingeDrinking 52.5%(1.0%) 52.5%(1.0%) 41.3%(0.9%)
HeavyDrinking 23.3%(0.7%) 26.1%(0.8%) 22.3%(0.7%)
AUD/SUD - 6.8%(0.4%) 10.4%(0.5%)
Note.AUD/SUD=AlcoholorSubstanceUseDisorder.Valuesareweightedprevalence(standarderror).
AnalysissamplewascomprisedofPre/PostDeploymentStudyrespondentswhocompletedsurveysat
all4waves:pre-deployment(T0),within1monthofre-deploymenttotheU.S.(T1),3monthspost-
deployment(T2),and9monthspost-deployment(T3).NodataareshownforT1becauseneither
alcoholbingefrequencynorAUD/SUDwereassessedatthatwave.TheT0surveydidnotassesspast-
monthAUD/SUD;prevalenceoflifetimeAUD/SUDatT0was20.4%(0.7%).

26
Table2
Adjustedoddsofonsetandpersistenceofpost-deploymentHeavyDrinkingamongArmySTARRSPre/PostDeploymentSurveyrespondents
AdjustedOdds-Ratio(95%CI)
OnsetofHeavyDrinking
post-deployment(n=3575)
PersistenceofHeavyDrinking
frompre-topost-deployment(n=1070)
AnyHD ChronicHD1 AnyHD ChronicHD1
Soldiercharacteristics(assessedatT0)
Age,y 0.95(0.93-0.98) 0.94(0.91-0.98) 1.00(0.96-1.04) 1.01(0.98-1.05)
WaldΧ2(1) 10.82** 8.21** 0.00 0.49
Sex
Male 1.00 1.00 1.00 1.00
Female 0.62(0.41-0.94) 0.35(0.15-0.82) 1.57(0.76-3.23) 0.63(0.20-2.01)
WaldΧ2(1) 5.16* 5.76* 1.49 0.61
Race
White 1.00 1.00 1.00 1.00
Black 0.75(0.53-1.06) 0.84(0.51-1.40) 0.81(0.52-1.27) 0.76(0.47-1.23)
Asian 0.66(0.41-1.07) 0.90(0.47-1.73) 0.36(0.16-0.84) 0.49(0.23-1.01)

27
Other 1.21(0.84-1.73) 1.44(0.91-2.28) 0.93(0.57-1.53) 0.63(0.37-1.08)
WaldΧ2(3) 9.43* 3.74 6.13 7.96*
Ethnicity
Non-Hispanic 1.00 1.00 1.00 1.00
Hispanic 0.88(0.64-1.22) 0.86(0.55-1.37) 0.70(0.45-1.08) 0.92(0.56-1.51)
WaldΧ2(1) 0.56 0.40 2.59 0.12
Education
Highschooldegree 1.00 1.00 1.00 1.00
Generalequivalencydiploma 0.69(0.42-1.15) 0.98(0.46-2.09) 0.82(0.50-1.37) 0.81(0.49-1.35)
Collegedegree 0.85(0.63-1.15) 1.10(0.79-1.53) 1.10(0.80-1.52) 0.78(0.50-1.22)
WaldΧ2(2) 2.51 0.41 1.05 2.17
Maritalstatus
Married 1.00 1.00 1.00 1.00
Divorced/separated/widowed 1.21(0.85-1.70) 1.02(0.53-1.96) 1.24(0.77-1.98) 0.92(0.61-1.39)
Nevermarried 1.44(1.12-1.85) 1.79(1.28-2.50) 1.51(1.07-2.12) 1.23(0.91-1.66)
WaldΧ2(2) 8.84* 12.42** 5.42 2.55
Pre-deploymentfactors(assessedatT0)

28
PriorDeployments
Zero 1.00 1.00 1.00 1.00
One 0.85(0.67-1.08) 0.77(0.49-1.20) 0.97(0.70-1.35) 1.12(0.75-1.68)
Twoormore 0.80(0.58-1.09) 1.00(0.59-1.68) 1.19(0.83-1.70) 1.08(0.64-1.80)
WaldΧ2(2) 2.56 1.75 1.24 0.33
Past-monthBingeDrinking 3.21(2.57-4.02) 2.69(1.89-3.82) - -
WaldΧ2(1) 104.68*** 30.52*** - -
Past-monthPTSD,MDE,GAD,orSI 0.78(0.52-1.17) 0.76(0.43-1.35) 0.97(0.58-1.63) 0.77(0.46-1.29)
WaldΧ2(1) 1.48 0.87 0.01 0.99
Peri-deploymentfactors(assessedatT1)
Combat/deploymentstress(standardized) 1.03(0.91-1.16) 1.03(0.89-1.20) 1.00(0.85-1.18) 1.11(0.95-1.30)
WaldΧ2(1) 0.16 0.14 0.00 1.73
Personallifestress(standardized) 1.20(1.06-1.35) 1.21(0.98-1.49) 0.99(0.86-1.14) 1.03(0.88-1.21)
WaldΧ2(1) 8.64** 3.08 0.04 0.14
Militarylifestress(standardized) 1.01(0.89-1.15) 0.94(0.77-1.13) 0.97(0.84-1.10) 0.94(0.81-1.10)
WaldΧ2(1) 0.01 0.48 0.28 0.60
PTSDsymptomseverity(standardized) 1.14(0.99-1.30) 1.10(0.91-1.33) 1.06(0.87-1.29) 0.95(0.79-1.16)

29
WaldΧ2(1) 3.43 0.96 0.36 0.22
MDE/GADsymptomseverity(standardized) 1.02(0.87-1.20) 1.03(0.81-1.32) 1.20(1.02-1.40) 1.21(0.95-1.55)
WaldΧ2(1) 0.08 0.07 5.09* 2.33
Note.CI=confidenceinterval;HD=heavydrinking;PTSD=posttraumaticstressdisorder;MDE=majordepressiveepisode;GAD=generalized
anxietydisorder;SI=suicidalideation.Eachcolumndisplaystheresultsforaseparateweights-adjustedlogisticregressionmodel.Modelsalso
adjustedforBrigadeCombatTeam.Significantadjustedoddsratios(wheretheoverallWaldΧ2testisalsostatisticallysignificant)arebolded.
*p<.05;**p<.005;***p<.0005.
1ChronicHDwasdefinedasheavydrinkingthatwaspresentatboth3monthsand9monthspost-deployment(i.e.,atbothT2andT3).

30
Table3
Adjustedoddsofonsetandpersistenceofpost-deploymentAUD/SUDamongArmySTARRSPre/PostDeploymentSurveyrespondents
AdjustedOddsRatio(95%CI)
IncidenceofAUD/SUD
post-deployment(n=3729)
PersistenceofAUD/SUD
frompre-topost-deployment(n=916)
AnyAUD/SUD ChronicAUD/SUD1 AnyAUD/SUD ChronicAUD/SUD1
Pre-deploymentfactors(assessedatT0)
Numberofpriordeployments
Zero 1.00 1.00 1.00 1.00
One 0.57(0.30-1.05) 0.52(0.27-1.01) 0.94(0.64-1.40) 1.05(0.63-1.73)
Twoormore 0.81(0.40-1.65) 0.58(0.27-1.25) 0.72(0.50-1.04) 0.84(0.55-1.28)
WaldΧ2(2) 3.40 4.47 3.02 0.86
Past-monthbingedrinking 1.84(1.27-2.70) 1.93(1.26-2.95) - -
WaldΧ2(1) 10.30** 9.09** - -
Past-monthPTSD,MDE,GAD,orSI 0.77(0.38-1.58) 0.54(0.24-1.22) 0.84(0.44-1.62) 1.06(0.52-2.13)
WaldΧ2(1) 0.50 2.22 0.27 0.02
Peri-deploymentfactors(assessedatT1)

31
Combat/deploymentstress(standardized) 1.22(0.96-1.55) 1.29(0.97-1.70) 1.05(0.90-1.23) 1.12(0.96-1.30)
WaldΧ2(1) 2.61 3.07 0.34 1.96
Personallifestress(standardized) 1.54(1.25-1.89) 1.72(1.41-2.09) 1.19(0.99-1.44) 1.30(1.08-1.56)
WaldΧ2(1) 16.99*** 28.48*** 3.49 7.80**
Militarylifestress(standardized) 1.02(0.89-1.16) 1.06(0.83-1.35) 1.20(1.02-1.41) 1.07(0.89-1.27)
WaldΧ2(1) 0.08 0.22 5.04* 0.49
PTSDsymptoms(standardized) 1.04(0.77-1.40) 0.94(0.64-1.37) 0.93(0.72-1.20) 0.87(0.65-1.16)
WaldΧ2(1) 0.07 0.11 0.35 0.88
MDE/GADsymptoms(standardized) 1.01(0.72-1.42) 0.99(0.69-1.44) 1.23(0.90-1.70) 1.24(0.92-1.68)
WaldΧ2(1) 0.00 0.00 1.69 1.97
Note.AUD/SUD=AlcoholorSubstanceUseDisorder;CI=confidenceinterval;PTSD=posttraumaticstressdisorder;MDE=majordepressive
episode;GAD=generalizedanxietydisorder;SI=suicidalideation.Eachcolumndisplaystheresultsforaseparateweights-adjustedlogistic
regressionmodel.Tostreamlinethetable,soldiercharacteristicsincludedinthemodels(age,sex,race,ethnicity,education,andmaritalstatus)
areomitted;nonedisplayedsignificantassociationswithincidenceorpersistenceofAUD/SUD(ps>.10).ModelsalsoadjustedforBrigade
CombatTeam.Significantadjustedoddsratios(wheretheoverallWaldΧ2testisalsostatisticallysignificant)appearinbold.
*p<.05;**p<.005;***p<.0005.
1ChronicAUD/SUDwasdefinedasthedisorderbeingpresentatboth3monthsand9monthspost-deployment(i.e.,atbothT2andT3).

32
FigureCaptions
Figure1.Weightedprevalencebygenderofbingedrinkingandheavydrinkingatpre-deployment(T0),
3monthspost-deployment(T2),and9monthspost-deployment.Groupn’stotalslightlylessthan4645
duetoraremissinggenderdata.Prevalenceofbingedrinkingandheavydrinkingwasloweramong
womenthanmenatallwaves[Χ2(1)=21.98to63.42,ps<.001].
Figure2.Weightedprevalencebyagegroupofheavydrinkingatpre-deployment(T0),3monthspost-
deployment(T2),and9monthspost-deployment.Groupn’stotalslightlylessthan4645duetorare
missingagedata.Prevalenceofheavydrinkingdifferedbyagegroupatallwaves[Χ2(3)=85.01to92.02,
ps<.001].

33
0%
10%
20%
30%
40%
50%
60%
Males (n=4358) Females (n=276) Males (n=4358) Females (n=276)
Binge Drinking Heavy Drinking
Wei
ghte
d pr
eval
ence
Pre-deployment 3 months post-deployment 9 months post-deployment

34
0%
5%
10%
15%
20%
25%
30%
35%
40%
Pre-deployment 3 months post-deployment 9 months post-deployment
Weightedprevalen
ceofH
eavy
Drinking
18 to 20 (n=731) 21 to 25 (n=1796) 26 to 30 (n=1114) 31 and older (n=989)

35
SupplementaryTable1
Item-levelcodingforDeploymentStressScale
Combatpatrol/dangerousduty <10times=0points;10ormoretimes=1point
Firedroundsatenemy/Tookenemyfire <10times=0points;10ormoretimes=1point
Wounded 0times=0points;1ormoretimes=1point
Hadclosecall(e.g.,equipmentshotoff) 0or1time=0points;2ormoretimes=1point
Unitmemberseriouslywounded/killed 0=0points;1to4times=1point;5ormoretimes=2points
Responsibleforenemycombatantdeath 0times=0points;1ormoretimes=1point
Responsiblefornon-combatantdeath 0times=0points;1ormoretimes=1point
ResponsibleforU.S.orallydeath 0times=0points;1ormoretimes=1point
Witnessedhomes/villagesdestroyed 0times=0points;1ormoretimes=1point
Directlyexposedtodeath/violence 0to4times=0;5ormoretimes=1point
Seriousphysicalassaultorfight1,2 0times=0points;1ormoretimes=1point
Sexualassault2 0times=0points;1ormoretimes=1point
Bullied/hazedbyunitmembers2 0times=0points;1ormoretimes=1point
Anyotherhighlystressfulexperience2 0=0points;1time=1point;2ormoretimes=2points
Note.Codingschemawasderivedduringpreliminaryanalysisofdatafromarestrictedsampleof1,145
respondentswhocompletedthePPDST0,T1,andT2surveys.Scoringwasinformedbyexaminationof
thefunctionalformofrelationshipsofeachratingtoaclinicallysalientoutcome(new-onsetofPTSDor
majordepressionatT2).TheDeploymentStressScalescorewascomputedbysummingpointsassigned
foreachitem(theoreticalrange=0-16).
1Separateitemsassessedphysicalassaultandgettingintoafight,buttheywerecollapsedforscoring.

36
2Toisolatecombatstress,ashorterformoftheDeploymentStressScalewasderivedafterexcluding4
items.Noneofthereportedresultschangedwhentheshortformwasusedinplaceofthefull
DeploymentStressScale.
37
SupplementaryTable2
Latentstructureof7surveyitemsassessingstressindifferentlifedomains:2-factormodel
Promax-rotatedfactorloadings
Personallifestress Armylifestress
Financialsituation 0.51 0.05
Lovelife 0.70 -0.02
Legalproblems 0.36 0.05
Relationshipwithfamily 0.76 -0.03
Problemsexperiencedbylovedones 0.75 -0.01
Problemswithchainofcommand -0.06 0.82
Problemswithunitmembers 0.02 0.73
Note.Exploratoryfactoranalysiswasconductedwithminimumresidualestimationandpromax
rotation.Arangeof1-to3-factorsolutionswasattempted;however,aninvalidsolutionwasobtained
when3factorswerespecified.The1-factormodelwasrejectedduetopooroverallfit(RMR=.10;
TLI=.68;RMSEA=.16).Theoverallfitofthe2-factorsolutionwasgood(RMR=.03;TLI=.95;RMSEA=.06);
eachitemdisplayedasalient(>.32)loadingononeofthetwofactors;cross-loadingswereabsent,and
thetwofactorswerereadilyinterpretable.
38
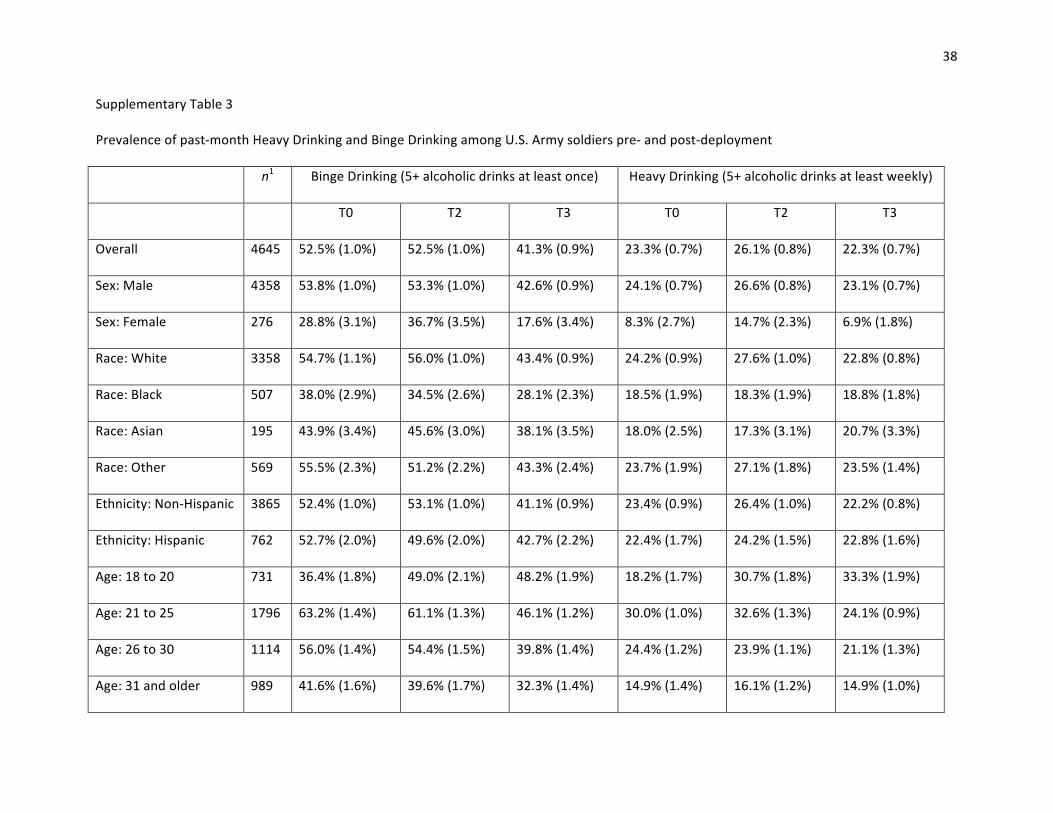
SupplementaryTable3
Prevalenceofpast-monthHeavyDrinkingandBingeDrinkingamongU.S.Armysoldierspre-andpost-deployment
n1 BingeDrinking(5+alcoholicdrinksatleastonce) HeavyDrinking(5+alcoholicdrinksatleastweekly)
T0 T2 T3 T0 T2 T3
Overall 4645 52.5%(1.0%) 52.5%(1.0%) 41.3%(0.9%) 23.3%(0.7%) 26.1%(0.8%) 22.3%(0.7%)
Sex:Male 4358 53.8%(1.0%) 53.3%(1.0%) 42.6%(0.9%) 24.1%(0.7%) 26.6%(0.8%) 23.1%(0.7%)
Sex:Female 276 28.8%(3.1%) 36.7%(3.5%) 17.6%(3.4%) 8.3%(2.7%) 14.7%(2.3%) 6.9%(1.8%)
Race:White 3358 54.7%(1.1%) 56.0%(1.0%) 43.4%(0.9%) 24.2%(0.9%) 27.6%(1.0%) 22.8%(0.8%)
Race:Black 507 38.0%(2.9%) 34.5%(2.6%) 28.1%(2.3%) 18.5%(1.9%) 18.3%(1.9%) 18.8%(1.8%)
Race:Asian 195 43.9%(3.4%) 45.6%(3.0%) 38.1%(3.5%) 18.0%(2.5%) 17.3%(3.1%) 20.7%(3.3%)
Race:Other 569 55.5%(2.3%) 51.2%(2.2%) 43.3%(2.4%) 23.7%(1.9%) 27.1%(1.8%) 23.5%(1.4%)
Ethnicity:Non-Hispanic 3865 52.4%(1.0%) 53.1%(1.0%) 41.1%(0.9%) 23.4%(0.9%) 26.4%(1.0%) 22.2%(0.8%)
Ethnicity:Hispanic 762 52.7%(2.0%) 49.6%(2.0%) 42.7%(2.2%) 22.4%(1.7%) 24.2%(1.5%) 22.8%(1.6%)
Age:18to20 731 36.4%(1.8%) 49.0%(2.1%) 48.2%(1.9%) 18.2%(1.7%) 30.7%(1.8%) 33.3%(1.9%)
Age:21to25 1796 63.2%(1.4%) 61.1%(1.3%) 46.1%(1.2%) 30.0%(1.0%) 32.6%(1.3%) 24.1%(0.9%)
Age:26to30 1114 56.0%(1.4%) 54.4%(1.5%) 39.8%(1.4%) 24.4%(1.2%) 23.9%(1.1%) 21.1%(1.3%)
Age:31andolder 989 41.6%(1.6%) 39.6%(1.7%) 32.3%(1.4%) 14.9%(1.4%) 16.1%(1.2%) 14.9%(1.0%)

39
Note.Valuesareweightedprevalence(standarderror).Atallwaves,prevalenceofBDandHDdifferedsignificantlybysex[Χ2(1)=21.98to63.42,
allps<.001]andagegroup[Χ2(3)=63.19to193.46,allps<.001].PrevalenceofBDdifferedbyraceatallwaves[Χ2(3)=42.63to88.40,ps<.001],
andprevalenceofHDdifferedbyraceatT0[Χ2(3)=13.99,p=.003]andT2[Χ2(3)=28.62,p<.001].Nodifferenceswereobservedbasedon
ethnicity(ps>.14).1Somesubgroupsamplesizestotalslightly<4645duetorarecasesofmissingdemographicdata.
40
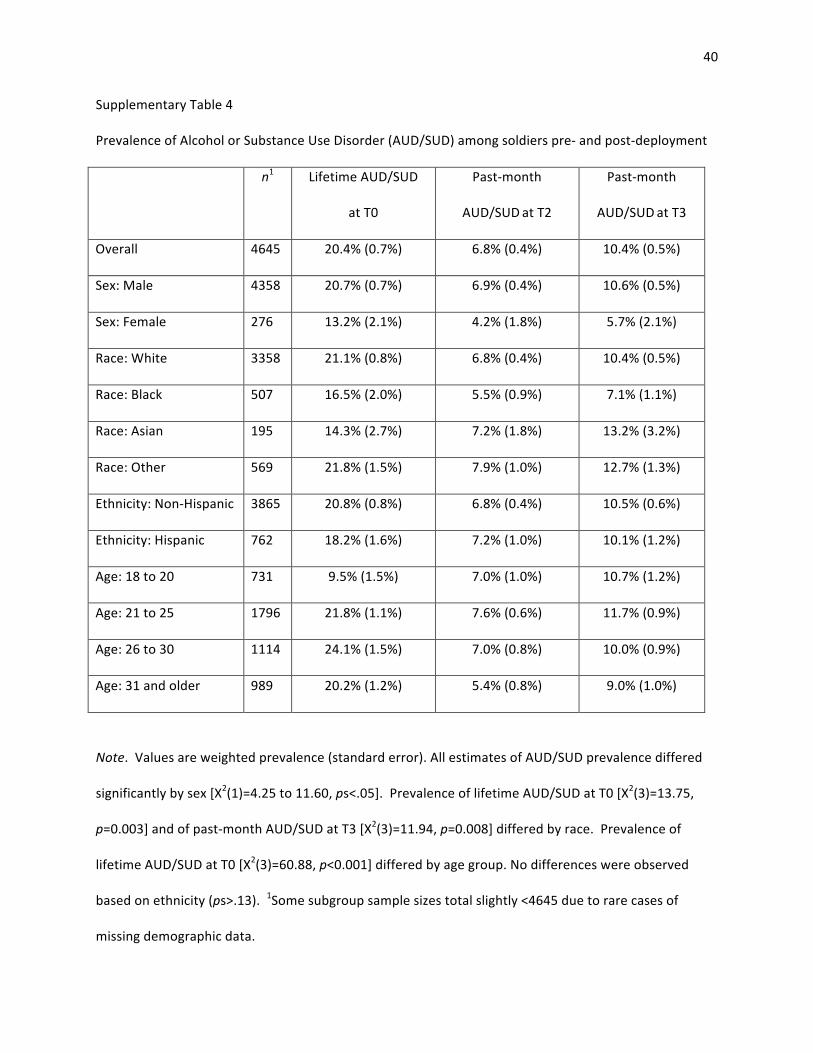
SupplementaryTable4
PrevalenceofAlcoholorSubstanceUseDisorder(AUD/SUD)amongsoldierspre-andpost-deployment
n1 LifetimeAUD/SUD
atT0
Past-month
AUD/SUDatT2
Past-month
AUD/SUDatT3
Overall 4645 20.4%(0.7%) 6.8%(0.4%) 10.4%(0.5%)
Sex:Male 4358 20.7%(0.7%) 6.9%(0.4%) 10.6%(0.5%)
Sex:Female 276 13.2%(2.1%) 4.2%(1.8%) 5.7%(2.1%)
Race:White 3358 21.1%(0.8%) 6.8%(0.4%) 10.4%(0.5%)
Race:Black 507 16.5%(2.0%) 5.5%(0.9%) 7.1%(1.1%)
Race:Asian 195 14.3%(2.7%) 7.2%(1.8%) 13.2%(3.2%)
Race:Other 569 21.8%(1.5%) 7.9%(1.0%) 12.7%(1.3%)
Ethnicity:Non-Hispanic 3865 20.8%(0.8%) 6.8%(0.4%) 10.5%(0.6%)
Ethnicity:Hispanic 762 18.2%(1.6%) 7.2%(1.0%) 10.1%(1.2%)
Age:18to20 731 9.5%(1.5%) 7.0%(1.0%) 10.7%(1.2%)
Age:21to25 1796 21.8%(1.1%) 7.6%(0.6%) 11.7%(0.9%)
Age:26to30 1114 24.1%(1.5%) 7.0%(0.8%) 10.0%(0.9%)
Age:31andolder 989 20.2%(1.2%) 5.4%(0.8%) 9.0%(1.0%)
Note.Valuesareweightedprevalence(standarderror).AllestimatesofAUD/SUDprevalencediffered
significantlybysex[Χ2(1)=4.25to11.60,ps<.05].PrevalenceoflifetimeAUD/SUDatT0[Χ2(3)=13.75,
p=0.003]andofpast-monthAUD/SUDatT3[Χ2(3)=11.94,p=0.008]differedbyrace.Prevalenceof
lifetimeAUD/SUDatT0[Χ2(3)=60.88,p<0.001]differedbyagegroup.Nodifferenceswereobserved
basedonethnicity(ps>.13).1Somesubgroupsamplesizestotalslightly<4645duetorarecasesof
missingdemographicdata.


















