Proposed policy priorities for preventing obesity and...
84
Proposed policy priorities for preventing obesity and diabetes in the Eastern Mediterranean Region EMRO Technical Publications Series 46
-
Upload
truongkien -
Category
Documents
-
view
212 -
download
0
Transcript of Proposed policy priorities for preventing obesity and...

Proposed policy priorities for preventing obesity and diabetes in the Eastern Mediterranean Region
EMRO Technical Publications Series 46


46EMRO Technical Publications Series
Proposed policy priorities for preventing obesity and diabetes in the Eastern Mediterranean Region

WHO Library Cataloguing in Publication Data
Proposed policy priorities for preventing obesity and diabetes in the Eastern Mediterranean Region / Ala Alwan, Karen McColl, Ayoub Al-Jawaldeh, Philip James
p. ISBN: 978-92-9022-200-2 ISBN: 978-92-9022-201-9 (online) 1. Diabetes Mellitus - prevention & control 2. Obesity - prevention & control 3. Diabetes Complications 4. Eastern
Mediterranean Region I. Alwan, Ala II. Title III. Regional Office for the Eastern Mediterranean (NLM Classification: WK 835)
Acknowledgements
This document was developed through a series of consultations held at the WHO Regional Office for the Eastern Mediterranean, with participation from representatives of academia and scientific researchers. The authors of this publication are:Dr Ala Alwan, former WHO Regional Director, WHO Regional Office for the Eastern Mediterranean, Cairo, EgyptMs Karen McColl, Policy Consultant, United KingdomDr Ayoub Al-Jawaldeh, Regional Adviser, Nutrition, WHO Regional Office for the Eastern Mediterranean, Cairo, EgyptPhilip James, Honorary Professor of Nutrition, London School of Hygiene and Tropical Medicine, London, United Kingdom, The Regional Office would like to acknowledge the technical input and support of Dr Maha El-Adawy, Director of Health Protection and Promotion, WHO Regional Office for the Eastern Mediterranean; Dr Francesco Branca, Director of Nutrition for Development, WHO headquarters; and Dr Fiona Bull, Programme Manager, Surveillance and Population-based Prevention, WHO Prevention of Noncommunicable Diseases Management Team, WHO headquarters.
© World Health Organization 2017
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. [Title]. Cairo: WHO Regional Office for the Eastern Mediterranean; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Design and layout by YAT Communication

Contents Executive summary .................................................................................................................. 5
1. Introduction: Obesity and diabetes in the Eastern Mediterranean Region ............. 9
1.1 Burden of obesity and diabetes .............................................................................................................................. 9
1.2 Dietary risk factors driving the burden of obesity and diabetes .......................................................... 11
1.3 Urgent action to tackle obesity and diabetes in the Region .................................................................. 12
2. Methodology for identifying priority actions for preventing obesity and diabetes in the Region ......................................................................................................................... 13
3. Proposed priority areas for action and strategic interventions ............................... 13
4. Implementation of the proposed priority areas for action ........................................ 24
4.1 Multisectoral action is essential ............................................................................................................................... 24
4.2 Clear commitments to action and monitoring of progress .................................................................... 25
4.3 Feasibility issues and phased implementation ................................................................................................. 25
Annex 1. Methodology for identifying priority actions for preventing obesity and diabetes in the Region ..................................................................................................... 40
Annex 2. Summary of strategic interventions in 10 priority areas for action for the prevention of obesity and diabetes in the Eastern Mediterranean Region ................. 42
Annex 3. Examples of country experience with implementation of the proposed strategic interventions ............................................................................................................ 64
Annex 4. Feasibility considerations for implementing strategic interventions in 10 priority areas for action to prevent obesity and diabetes in the Eastern Mediterranean Region ............................................................................................................. 72


5
Executive summary
Executive summaryThe Eastern Mediterranean Region of the World Health Organization (WHO) has an extremely high prevalence of overweight and obesity in both adults and children, precipitating the highest regional prevalence of diabetes in the world.
With regional obesity and overweight prevalence rates well above the global average, half the Region’s adult women (50.1%) and more than two in five men (43.8%) were overweight or obese in 2014 (1). In several countries two thirds or more of adults (especially women) are overweight or obese.
High rates of childhood overweight in the Region give particular cause for concern. On average, 6.9% of children under five years are already overweight – higher than the global average of 6.2% – and in some countries more than 15% of children are affected (2). In many countries of the Region more than half of adolescents are overweight or obese.
Around 43 million people in the Region live with diabetes, and its prevalence has risen from 6% in 1980 to 14% in 2014, affecting more than 20% of adults in some countries. The Region has the highest death rates from diabetes of all WHO regions (1). The prevalence of diabetes is higher than might be expected given the levels of obesity – diabetes prevalence rates are about twice the rates shown for equivalent obesity prevalence rates in, for example, European Union countries, potentially reflecting a greater sensitivity to diabetes in the Region.
The increasing prevalence of overweight, obesity and diabetes is closely linked to a dramatic reduction in physical activity accompanied by marked changes in dietary patterns in the Region. Average intakes of energy and fat are above WHO-recommended levels, with substantially higher fat intakes in
the Region’s high-income countries. More than three quarters of the Region’s countries consume substantially higher levels of sugars than WHO recommends.
Such high prevalence rates of these conditions and the heavy burden of morbidity, disability and death they can cause threaten to generate a devastating financial burden for countries of the Region, overwhelming health services and undermining their economic and social well-being. Urgent action is therefore needed to tackle this alarming and escalating problem. Yet the Eastern Mediterranean has the highest proportion of countries of any region without any policies to combat diabetes (1).
Taking the recommendations of several recent initiatives on the prevention of obesity and diabetes1 into account, the WHO Regional Office for the Eastern Mediterranean has identified priorities for an approach to reduce exposure to unhealthy dietary risk factors for obesity and diabetes (See Annex 1 for the methodology). This document presents an initial proposal for 10 priority areas for action, which cover 37 strategic interventions to help prevent overweight, obesity and diabetes in the whole population – children, adolescents and adults. These areas for action and interventions are set out in Table 1.
All the priority areas and interventions proposed have a sufficiently strong case-based on research evidence and expert analysis of the measures – to warrant recommending their adoption (See Annex 2 for a summary of the
1 Such as the United Nations Political Declaration of the High Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases (2011), the WHO Eastern Mediterranean Region Framework for action to implement the UN Political Declaration on Noncommunicable Diseases, including indicators to assess country progress by 2018, the Commission on Ending Childhood Obesity (2016), the political declaration and Framework for Action from the Second International Conference on Nutrition (2014) and WHO’s first Global Report on Diabetes (2016).

6
Proposed policy priorities for preventing obesity and diabetes
evidence). In addition, most of the interventions have been tried and tested in other countries or localities or adopted by innovative policy-makers, and growing country experience has bolstered the evidence base (See Annex 3 for examples of country implementation). Some of the proposed strategic interventions will be easier to implement than others and the challenges of their application, the financial implications, public acceptance and political feasibility very much depend on the particular country context (See Annex 4 for a summary of feasibility issues).
A phased approach may, therefore, be needed in some countries. The strongest candidate interventions for the first phase of action are indicated in Table 1, along with those that it may be more appropriate to implement in a second phase. Countries that are less affected by these feasibility constraints, however, are encouraged to implement all of the strategic interventions as soon as possible.
Detailed analysis of the effective measures and the responsibilities for implementing them has revealed that almost all the proposed interventions require simultaneous action by several government departments, in addition to the Ministry of Health, which should have an important coordination and monitoring role (3). The exact configuration of a cross-government approach will vary, but it is important to establish the highest level of political commitment and leadership and to ensure coordinated action across government with mechanisms to evaluate and drive progress by each government department.
This highlights more than ever the need for a whole-of-government and whole-of-society approach – backed by strong political commitment at the highest level – to tackling these major public health problems, which have multiple and inter-related risk factors and determinants.
Table 1. Summary of proposed priority areas of action and strategic interventions for preventing obesity and diabetes in the Eastern Mediterranean and their implementation phaseArea for action Interventions most suitable for first phase
implementation Interventions for which there is evidence of impact, but which it may be more appropriate to implement in a second phase
1 Fiscal measures 1.1 Progressively eliminate national subsidies for all types of fats/oils and sugar.
1.2 Implement an effective tax on sugar-sweetened beverages.
1.3 Consider an effective progressive tax on high fat foods and on high sugar foods.
2 Public procurement 2.1 Implement mandatory nutrition standards across all public institutions through (a) application of the regional nutrient profile model to assess the nutritional quality of different foods, (b) introduction of meal standards and (c) measures to eliminate the sale of foods or drinks high in fat, sugar or salt.
2.2 Issue mandatory guidelines for the revision of procurement to provide healthy food, including limiting the volume of fats/oils, sugar and salt entering public sector catering facilities in order to facilitate the necessary menu changes (e.g. so that meals provide not more than 25% energy from fats and less than 5% from free sugars).
2.3 Develop guidance and provide training to catering companies on appropriate catering methods in public institutions to reduce the use of frying and sweetening of foods and help with menu design.
2.4 Continue implementing these measures, scaling up coverage and monitoring impact.

7
Executive summary
Table 1. Summary of proposed priority areas of action and strategic interventions for preventing obesity and diabetes in the Eastern Mediterranean and their implementation phaseArea for action Interventions most suitable for first phase
implementation Interventions for which there is evidence of impact, but which it may be more appropriate to implement in a second phase
3 Physical activity interventions
3.1 Promote healthy physical activity through mass media campaigns (see priority area 9) and ensure adequate legislation supporting delivery of daily physical activity for students in schools and universities.
3.2 Ensure comprehensive delivery of regular, quality physical education to all children, as a key component of education in schools.
3.3 Develop a set of standards/guidelines promoting physical activity in the workplace, including facility/building design, availability of sports facilities and programmes enabling access to facilities away from the workplace.
3.4 Increase availability of and accessibility for participation in formal and informal recreational and sporting activities, particularly providing opportunities for participation in programmes such as “Sports-for-All”, with emphasis on ensuring equality of access and opportunity for participation.
3.5 Develop and implement an urban planning policy to ensure that urban environments encourage people to rely less on personal motorized vehicles and support access to safe, gender-sensitive and age-friendly public transport, cycling and walking, including by provision of facilities, equipment, open and green public space and shared use of school facilities (both indoor and outdoor).
3.6 Continue implementing these measures, scaling up coverage and monitoring impact.
4 Food supply and trade
4.1 Conduct a situation analysis of the national and/or local food supply, including establishing the proportions of fats/oils and sugar used in the diet that are derived from imports and domestic production, along with the extent of food manufacture and processing within the country and the supply of fruit, vegetables and whole grains.
4.2 Facilitate the development of local food policies and encourage city authorities to sign the Milan Urban Food Policy Pact and implement its Framework for Action to develop, where possible, sustainable urban food systems.
4.3 Consider introducing standards or other legal instruments (e.g. compositional standards, tariffs, import restrictions, sales bans, planning laws, zoning policies) to reduce the volume and improve the quality of fats/oils and reduce sugars in the national and local food supply.
4.4 Consider removing agricultural subsidies for producers of sugars and oils (especially those oils high in saturated fatty acids), replacing them, where necessary, with other mechanisms to support farmers and growers.
5 Reformulation 5.1 Cooperate with other Member States to adopt a regional approach for engaging with food producers to drive food reformulation to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size in a substantial proportion of processed foods.
5.2 Engage with private sector providers of food in catering/food service outlets (including takeaways and street food traders) to establish a programme to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size, with defined quantified reductions in use of these ingredients.

8
Proposed policy priorities for preventing obesity and diabetes
Table 1. Summary of proposed priority areas of action and strategic interventions for preventing obesity and diabetes in the Eastern Mediterranean and their implementation phaseArea for action Interventions most suitable for first phase
implementation Interventions for which there is evidence of impact, but which it may be more appropriate to implement in a second phase
6 Marketing 6.1 Work with other countries in the Region to establish a coordinated approach, including appropriate legal advice, to reduce the impact of cross-border marketing.
6.2 Implement the WHO Set of Recommendations on Marketing of Foods and Non-alcoholic Beverages to Children and consider mandatory restrictions to eliminate all forms of marketing of foods high in fat, sugar and salt to children and adolescents (up to age 18) across all media, according to the Regional Action Plan to Address Unopposed Marketing of Unhealthy Food and Beverages.
6.3 Use the regional nutrient profile model, which categorizes the appropriate level of nutrients in foods, to identify foods to which the marketing restrictions should apply.
6.4 Conduct an assessment (preferably as part of a regional collaboration) of the impact of marketing of foods high in fat, sugar or salt to adults to illuminate the magnitude of marketing and define how best to restrict inappropriate practices.
6.5 Consider extending mandatory restrictions on marketing of unhealthy foods to whole population.
6.6 Legislate to allow retail promotion only of healthy foods.
7 Labelling 7.1 Implement a mandatory front-of-pack labelling scheme with elements to enable consumers to interpret information easily (such as colour coding or the use of terms such as “high”, “medium”, ”low”).
7.2 Enforce the labelling scheme and monitor its impact with the potential to strengthen the labelling with suitable health warnings.
8 Breastfeeding 8.1 Promote breastfeeding through mandatory baby-friendly health systems and effective community-based strategies.
8.2 Fully implement the International Code of Marketing of Breast-milk Substitutes and the WHO Guidance on ending inappropriate promotion of foods for infants and young children.
8.3 Empower women to exclusively breastfeed, by enacting progressively increasing remunerated time off work up to a goal of 6 months’ mandatory paid maternity leave, as well as policies that encourage women to breastfeed in the workplace including breastfeeding breaks and provision of suitable facilities.
9 Mass media campaigns
9.1 Implement appropriate social marketing campaigns, led by the public sector, on healthy diet and physical activity in order to build consensus, complement the other interventions in the package and encourage behaviour change.
9.2 Ensure sustained implementation of campaigns and monitor their impact.
10. Health sector interventions
10.1 Ensure provision of dietary counselling on nutrition, physical activity and healthy weight gain before and during pregnancy for prospective mothers and fathers.
10.2 integrate screening for overweight and other diabetes risk factors into primary health care and provide primary-care based counselling for high-risk individuals.
10.3 Establish or strengthen, as appropriate, a high-level multisectoral mechanism to define and oversee the implementation of food and physical activity policies for the prevention of obesity and diabetes.
10.4 Establish national targets for obesity and diabetes, along with SMART commitments for action, and work with WHO to develop and implement a monitoring framework for reporting on progress.
10.5 Implement evidence-based community-based interventions, addressing both healthy eating and physical activity, comprising different activities and targeting high-risk groups, to promote and facilitate behaviour change and prevent obesity and diabetes.

9
Introduction
1. Introduction: Obesity and diabetes in the Eastern Mediterranean RegionThere is an alarming and escalating burden of overweight, obesity and diabetes in the Eastern Mediterranean Region, closely linked to changing dietary patterns. Obesity and the most common type of diabetes are largely preventable and urgent action is needed to reduce exposure to their causal factors, such as unhealthy diet and physical inactivity.
1.1 Burden of obesity and diabetes
The prevalence of obesity and overweight is worryingly high in the Region – at 46.8%,
well above the global average. In 2014, half the Region’s adult women (50.1%) and more than two in five men (43.8%) were overweight or obese (1). In some countries of the Region two thirds or more of adults are overweight or obese, while other countries, in an earlier stage of the nutrition transition that often accompanies economic development, have moderate levels of overweight/obesity or have emerging overweight/obesity only in certain socioeconomic groups (Fig. 1 and 2).
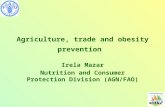
High rates of childhood overweight give particular cause for concern. On average, 6.9% of children under five years are already overweight – higher than the global average of 6.2% – and in some countries more than 15% of children are affected. In many countries of the Region more than half of adolescents (13–18 years) are overweight or obese (2) (Fig. 3).
Fig. 1. Prevalence of female overweight and obesity in Eastern Mediterranean countries (latest integrated 2014 prevalence data for adult women)
Source: Data from NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016; 387:1377-96.
0
10
20
30
40
50
60
70
80
Afghan
istan
Jorda
n
Kuwait
Leba
non
Libya
Moroc
co
Pales
tine
Oman
Pakis
tanQ
atar
Saud
i Ara
bia
Somali
aSu
dan
Syria
n Ara
b Rep
ublic
Tunisi
a
United
Ara
b Emira
tes
Yemen
BMIs25-<30 Obesity BMIs 30+
Islam
ic Rep
ublic
of Ir
anIraq
Bahr
ain
Djibou
tiEg
ypt

10
Proposed policy priorities for preventing obesity and diabetes
Young women who are overweight or obese before pregnancy are now having children who are immediately disadvantaged for life as they are at greater risk of later health problems,
including obesity (4). Diabetes during pregnancy not only exposes a mother to much greater risk, but also markedly increases her child’s chances of ill health in the future (5).
0
10
20
30
40
50
60
70
80
Afghan
istan
Jorda
n
Kuwait
Leba
non
Libya
Moroc
co
Pales
tine
Oman
Pakis
tanQ
atar
Saud
i Ara
bia
Somali
aSu
dan
Syria
n Ara
b Rep
ublic
Tunisi
a
United
Ara
b Emira
tes
Yemen
BMIs25-<30 Obesity BMIs 30+
Islam
ic Rep
ublic
of Ir
anIraq
Bahr
ain
Djibou
tiEg
ypt
%
Fig. 2. Prevalence of male overweight and obesity in Eastern Mediterranean countries (latest 2014 integrated prevalence data for adult men)
Source: Data from NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016; 387:1377-96.
Fig. 3. Prevalence of adolescent overweight and obesity in Eastern Mediterranean countries (13–18 years, average for boys and girls, 2014)
Source: Recalculated from WHO Eastern Mediterranean Framework for health information systems and core indicators for monitoring health situtation and health system performance, 2015
Afghan
istan
Jorda
n
Kuwait
Leba
non
Libya
Moroc
co
Pales
tine
Oman
Pakis
tanQ
atar
Saud
i Ara
bia
Somali
aSu
dan
Syria
n Ara
b Rep
ublic
Tunisi
a
United
Ara
b Emira
tes
Yemen
Islam
ic Rep
ublic
of Ir
anIraq
Bahr
ain
Djibou
tiEg
ypt
0102030405060708090
Moderate overweight Obesity

11
The Eastern Mediterranean Region has the highest prevalence of diabetes in the world (Fig. 4) (1). Around 43 million people in the Region live with this chronic disease, which, if not properly controlled, puts them at increased risk of serious complications, such as cardiovascular disease, vision loss, nerve damage, leg amputation or kidney failure, and of early death. More than 10% of deaths in adult women and 9% of deaths in adult men in the Region are attributable to high blood glucose (1). The prevalence of diabetes in the Region rose from 6% in 1980 to 14% in 2014 and now affects more than 20% of adults in some countries. In addition, there are many millions more with pre-diabetes,2 who are at increased risk of developing clinically evident
2 Impaired glucose intolerance and impaired fasting glycaemia are intermediate conditions in the transition between normal blood glucose levels and diabetes, although the transition is not inevitable.
diabetes within the next 5–10 years and who already have a greater risk of heart disease.
The risk of diabetes is recognized to increase as children and adults in particular gain weight. So the longer an adult has been overweight/obese and the more extreme their obesity, the greater their risk of diabetes. Yet in the Eastern Mediterranean Region, the prevalence of diabetes is about twice the rates found for equivalent prevalence rates of obesity in, for example, European Union countries (1) (Fig. 5), potentially reflecting a greater sensitivity of the population in the Region to diabetes if they gain weight.
Both obesity and diabetes were rare in the 1950s in most countries of the Region until the activity patterns and diet of the communities changed from the 1960s onwards with a
Introduction
1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Prev
alen
ce o
f dia
bete
s
12%
14%
10%
8%
6%
4%
2%
0%
African Region European Region
South-East Asia Region
Western Pacific Region
WorldRegion of the Americas
Eastern Mediterranean
Region
Fig. 4. Trends in the prevalence of diabetes, 1980–2014, by WHO Region
Source: (1).

12
Proposed policy priorities for preventing obesity and diabetes
subsequent increase in body weight and increasing prevalence of diabetes.
The greater sensitivity to diabetes when adults gain weight may relate to the greater genetic sensitivity of the population but it is also recognized that early nutritional deficiencies affecting mothers in early pregnancy and children in early childhood can potentially increase the sensitivity of the community to the development of obesity and diabetes, as recently emphasized by the Commission on Ending Childhood Obesity (6). These effects seem to relate to the impact of a poor environment on the responsiveness of normal genes through so-called “epigenetic changes” that are only just becoming understood. It is also being emphasized that a woman needs be nutritionally well fed and of normal weight before conception to promote the well-
being of her child and avoid the problems of an increased risk of childhood obesity. The Region is, therefore, facing a huge challenge as future generations are increasingly affected by obesity and diabetes at a much earlier age. No country can afford the financial and social costs these changes will bring.
This alarming and escalating burden of obesity and diabetes in the Region is closely linked to the dietary changes of recent decades. The good news is that both obesity and type 2 diabetes are largely preventable – but multisectoral, population-based initiatives are needed to reduce exposure to the major causes, namely unhealthy diet and physical inactivity. The high levels of obesity and diabetes in the Region also suggest that substantial measures need to be taken soon to alleviate and reverse the current escalating burden of disease.
EU Males
EU Females
0
5
10
15
20
25
0 10 20 30 40 50 60
National age standardized obesity prevalence %
EMR Females
EMR Males
Diabetes prevalence rates %
Fig. 5. National diabetes prevalence rates in countries of the Eastern Mediterranean Region (EMR) and European Union (EU) country equivalent obesity rates
Source: Based on WHO STEPS data

13
1.2 Dietary risk factors driving the burden of obesity and diabetes
Dietary factors causing unhealthy body weight gain and type 2 diabetes include high intakes of total fat and free sugars, excessive saturated fatty acid consumption and an inadequate intake of fibre-rich foods (1). In addition, high intake of sugary drinks, not just overall sugar intake, increases the likelihood of being overweight or obese, particularly among children, and is also associated with an increased risk of type 2 diabetes (1). WHO dietary recommendations for the prevention of type 2 diabetes include limiting saturated fatty acid intake to less than 10% of total energy intake (and for high-risk groups, less than 7%) and achieving adequate intake of dietary fibre (minimum daily intake of 20 g) through regular consumption of wholegrain cereals, legumes, fruits and vegetables (7). WHO is currently updating its guidelines on fat intake and carbohydrate intake, which will include recommendations on dietary fibre as well as fruits and vegetables. WHO strongly recommends that all individuals should reduce their intake of free sugars3 to less than 10% of total energy intake and suggests that “further reduction to 5% could have additional health benefits” (8). Given the heavy burden of disease in the Region and WHO evidence that both weight gain and dental disease seem to be progressively lower when intakes are further reduced, free sugar intake of less than 5% of total energy intake for every individual is considered the goal in order to achieve the dramatic improvement needed in children’s and adults’ health in countries of the Region.
Remarkable increases in total energy, fat and sugar intakes in countries throughout 3 This includes “all monosaccharides and disaccharides
added to foods by the manufacturer, cook, or consumer, plus sugars naturally present in honey, syrups, and fruit juices”.
the Eastern Mediterranean in recent decades mean that diets in the Region have gone in the opposite direction to all the national and WHO recommendations. Average intakes of energy and fat are above the WHO-recommended levels, with substantially higher fat intakes in the Region’s high-income countries. Thus, for example, in the 1950s and early 1960s the fat intake of the Bedouin in the Negev desert was 13% and their diet was rich in high fibre carbohydrate but low in sugar, and obesity and diabetes prevalence rates were very low (9), whereas now fat intakes are up to three times higher with much increased sugar intake. More than three quarters of the Region’s countries now consume substantially higher levels of sugar than the WHO-recommended daily intake of less than 5% from free sugars (10,11). This recommended level means that women should, on average, consume less than 25 g of free sugars per day and men less than 35 g per day. Average intakes in many countries already exceed 80 g per person daily (8).
Since excess body fat is a risk factor for type 2 diabetes, there is clearly benefit to be derived – with lower overweight and obesity rates – if coherent dietary measures are taken. In 2010, WHO proposed a series of evidence-based “best buy” interventions for tackling noncommunicable diseases (NCDs) and these were endorsed by the United Nations General Assembly’s political declaration on NCDs (12,13). The best buys for addressing unhealthy diet and physical inactivity were: reduced salt intake in food, replacement of trans fat with polyunsaturated fat, and raising public awareness on diet and physical activity through mass media. For cardiovascular diseases and diabetes, the best buys were counselling and multidrug therapy for people with a high risk of developing heart attacks and strokes, and treatment of heart attacks with aspirin (12). WHO’s first Global Diabetes Report, published in 2016, recommends
Introduction

14
Proposed policy priorities for preventing obesity and diabetes
prioritizing actions to prevent people becoming overweight and obese, implementing policies and programmes to promote breastfeeding and to increase the consumption of healthy foods, together with measures to discourage the consumption of unhealthy foods (1). The creation of supportive built and social environments is also recommended, in order to allow spontaneous as well as deliberate physical activity to improve health. These priorities can best be achieved through a combination of fiscal policies, legislation and regulations leading to environmental changes, as well as making the population aware of the changes and remedies needed.
1.3 Urgent action to tackle obesity and diabetes in the Region
Globally, countries are already working towards agreed global goals on maternal and infant nutrition and on the prevention of NCDs, and both these include halting the increase in overweight and obesity.4 The United Nations General Assembly convened a high-level meeting on NCDs in September 2011 attended by Heads of State and Government in which a political declaration was endorsed urging Member States to implement a comprehensive agenda to prevent and control the four major groups of NCDs, namely cardiovascular diseases, diabetes, cancer and chronic lung disease (13). The United Nations agenda covers high-impact, evidence-based and cost-effective measures (NCD best buys) to reduce risk factors including obesity and to create health-promoting environments through a whole-of-government and a whole-of-society effort. Subsequently, in 2012, the 4 The WHA global nutrition goals include a goal to halt the
increase in childhood overweight by 2025. The global NCD goals include a 25% relative reduction in overall mortality from NCDs (including diabetes) and halting the increase in obesity prevalence in adolescents and adults by 2025.
WHO Regional Committee for the Eastern Mediterranean endorsed a regional framework for action to translate the recommendations of the United Nations political declaration into a set of concrete population- and individual-based measures that Member States need to implement (14).
In November 2014, the Second International Conference on Nutrition (ICN2) adopted the Rome Declaration on Nutrition and its Framework for Action, which presented a set of 60 recommended actions, across sectors, to prevent malnutrition in all its forms, including overweight, obesity and diet-related NCDs (15,16). In early 2016, WHO’s Commission on Ending Childhood Obesity also made a series of recommendations to respond to the global crisis in childhood overweight (6).
Taking these recent recommendations and the regional framework for action into account, the WHO Regional Office for the Eastern Mediterranean has identified priorities for dietary change on a broad population-wide and regional basis to prevent obesity and diabetes in children, adolescents and adults. In that regard, this document presents 10 proposed priority areas for action involving 37 interventions.
With a focus on obesity and diabetes, these interventions have been selected to prioritize reducing the total amount of energy consumed from fat and sugar intakes, while recognizing that a shift from trans or saturated fats to unsaturated fats, reductions in salt intake and increases in fruit and vegetable consumption are also needed. These interventions should be seen as part of broader efforts to improve nutrition – especially since undernutrition is still prevalent in some countries of the Region – and to prevent other NCDs, including cardiovascular disease and cancer. Many of the priority interventions identified here would help prevent these other diseases by, for

15
3. Proposed priority areas for action and strategic interventions
Ten priority areas for action are proposed for the population-wide prevention of obesity and diabetes in the Eastern Mediterranean Region. Under these 10 areas, 37 strategic interventions are proposed for Member States’ consideration. These interventions focus mainly on a population-wide approach to address these major public health challenges, with a particular emphasis on food systems.
These recommendations are consistent with the WHO regional Framework for action to implement the United Nations Political Declaration on Noncommunicable Diseases and the 10 priority legal interventions for preventing NCDs identified for the Region (17). They also reflect the recommendations of the Commission on Ending Childhood Obesity and the ICN2 Framework for Action (6,16).
There are strong health and economic rationales for using fiscal measures, such as taxes and subsidies, which can both create incentives to reduce dietary risk factors for NCDs and generate government revenue, which could potentially be ring-fenced for health budgets (18). There is convincing evidence from modelling, experimental studies and from a growing body of country experiences that fiscal measures such as taxes and subsidies are very effective in shifting purchasing habits and thereby promoting dietary change (18–20).
Evidence is strongest and most consistent for the effectiveness of taxes on sugar-sweetened drinks, which are important contributors to calorie and free sugars intake (18). More than 10 countries (in addition to some sub-national or local jurisdictions) have introduced taxes on sugar-sweetened beverages. There is convincing and growing evidence that these
example, leading to reductions in intakes of salt and saturated fat or increases in fruit and vegetable consumption.
Priority area for action 1: Fiscal measures – Use judicious taxes and subsidies to promote healthier diets
Strategic interventions
1.1. Progressively eliminate all national subsidies for all types of fats/oils and sugar.
1.2. Implement an effective tax on sugar-sweetened beverages.
1.3. Consider an effective progressive tax on high fat foods and on high sugar foods.
2. Methodology for identifying priority actions for preventing obesity and diabetes in the Region
Starting with an informal regional meeting convened by the Regional Office in Geneva in May 2016, a process of identifying and defining effective, cost-effective and feasible interventions to address obesity and diabetes in the Eastern Mediterranean Region took place over the following eight months. The process involved consultation with policy experts and a review of the evidence on the key policy areas identified at the initial meeting. It culminated in the selection of 10 priority areas for action and 37 strategic interventions. This list was further developed, along with a summary of the evidence, case studies of implementation and feasibility considerations, into the current report. (The process is described in more detail in Annex 1).
Methodology for identifying priority actions for preventing obesity and diabetes in the Region

16
Proposed policy priorities for preventing obesity and diabetes
taxes are effective in reducing purchases, in the range of 20–50% (18,20–25). There is also a demonstrable impact of nutrient-focused taxes, such as those on high fat and/or sugar foods, which may reduce consumption of the target foods but may also increase intakes of foods not targeted by the tax (18–20,26–30). Subsidies on healthy foods have also been shown to increase intakes, with evidence strongest for subsidies on fruits and vegetables (18).
Priority area for action 2: Public procurement – Implement policies for the procurement and provision of healthy food in public institutions
Strategic interventions
2.4. Implement mandatory nutrition standards across all public institutions through (a) application of the regional nutrient profile model to assess the nutritional quality of foods, (b) introduction of meal standards and (c) measures to eliminate the sale of foods or drinks high in fat, sugar or salt.
2.5. Issue mandatory guidelines for the revision of procurement to provide healthy food, including limiting the volume of fats/oils, sugar and salt entering public sector catering facilities in order to facilitate the necessary menu changes (e.g. so that meals provide not more than 25% energy from fats and less than 5% from free sugars).
2.6. Develop guidance and provide training to catering companies on appropriate catering methods in public institutions to reduce the use of frying and sweetening of foods and help with menu design.
2.7. Continue implementing these measures, scaling up coverage and monitoring impact.
WHO has issued a technical report on the design and implementation of fiscal policies that should help policy-makers ensure that these are designed carefully in order to avoid unintended consequences, particularly on poorer groups who may then purchase other untaxed or cheaper foods (18). It has been suggested that taxes are more effective when applied to foods for which there are close healthy alternatives and that a targeted tax may be even more effective when combined with a subsidy on fruits and vegetables (19,20).
With the potential to save between 139 and 1696 disability-adjusted life-years (DALYs) per million population after 20 years in six low- or middle-income countries, a package of fiscal measures is predicted to be cost saving, i.e. the country not only saves expenditure on treating obesity and diabetes and their complications, but these saved costs are greater than the costs of implementing the measures (31–34).
Food subsidies, often on high fat or sugar commodities, are common throughout the Region – existing in three quarters of countries and amounting, on average, to just less than 1% of gross domestic product in 2011 (35).
Priority area for action 3: Physical activity interventions – Implement policies, legislation and interventions to promote and facilitate health-enhancing physical activity
Strategic interventions
3.8. Promote healthy physical activity through mass media campaigns (see priority area 9) and ensure adequate legislation supporting delivery of daily physical activity for students in schools and universities.
3.9. Ensure comprehensive delivery of regular, quality physical education to all children as a key component of education in schools.
3.10. Develop a set of standards/guidelines promoting physical activity in the workplace, including facility/building design, availability of sports facilities and programmes enabling access to facilities away from the workplace.
3.11. Increase availability of and accessibility for participation in formal and informal recreational and sporting activities, particularly providing opportunities for participation in programmes such as “Sports-for-All”, with emphasis on ensuring equality of access and opportunity for participation.
3.12. Develop and implement an urban planning policy to ensure that urban environments encourage people to rely less on personal motorized vehicles, and support access to safe, gender-sensitive and age-friendly public transport, cycling and walking, including by provision of facilities, equipment, open and green public space and shared use of school facilities (both indoor and outdoor).
3.13. Continue implementing these measures, scaling up coverage and monitoring impact.

17
Proposed priority areas for action and strategic interventions
expenditure means that procurement policies also have the potential to affect markets and bring about changes further up the supply chain.
There is international evidence that healthy food procurement policies can improve diets and health outcomes, particularly in studies done in schools (37–40), and experience shows that nutrition standards can be implemented across a wide range of public institutions. Many countries have introduced mandatory school food standards including bans on vending machines on school premises (41). Some countries have gone beyond nutrition standards to implement wider school procurement policies, linked to sustainability and boosting local markets (42,43). There are also examples of action at regional, national or local levels to improve public food beyond the school settings (44,45). See Annex 3 for examples of implementation.
Implementing healthy food procurement or nutrition standards could have cost implications for public food, but various strategies are available to keep costs down (42,46,47). There are, however, potentially high levels of return on investment in terms of health gains and the potential to bring about changes beyond health if social, environmental or economic objectives are also incorporated.
Physical inactivity is a risk factor for weight gain, type 2 diabetes and other NCDs, yet one third of men and half of the women in the Region do not undertake the minimum recommended levels of physical activity (48). Prevalence of physical inactivity ranges from about 30% to as high as 70% in some countries. Compared with other regions, women and younger adults in the Eastern Mediterranean Region are the least physically active in the world (48), but very few countries in the Region have programmes in place to increase physical activity. A high-level regional forum in 2014 agreed on a road map for promoting physical activity in the countries
These subsidies, often introduced to ensure food security, are in fact not particularly well targeted as a social protection measure and wealthier sectors of the population accrue a significant proportion of the benefits (35).In addition, such subsidies readily promote consumption of sugar or oils and can also encourage food manufacturers to use subsidized sugars or fats or ingredients derived from these commodities (e.g. high-fructose corn syrup or partially hydrogenated vegetable oils). The poorest groups are, therefore, particularly likely to suffer from the disease consequences of these measures.
Country experience in the Region shows that subsidies can be removed.5 It may be important to phase in the implementation to minimize public opposition, accompany it with explicit information campaigns that highlight the health benefits of such measures, and mitigate the impact on lower socioeconomic groups by replacing the subsidy with appropriate, nutrition-sensitive social protection measures, such as cash or food transfers, as advocated by the African Development Bank for at least one country in the Region (36).
Given the major dietary contribution of food eaten in schools, hospitals, residential care homes, universities, prisons, armed forces catering, government buildings and other publicly-funded venues or events, there is a strong case for ensuring that food served in these public institutions is always healthy.
“Healthy food procurement”6 can include application of nutritional standards/guidelines and may also – by changing what is served or sold – aim to promote healthy habits and preferences. The scale of government
5 Egypt, for example, has started to reform its food price subsidies (153).
6 The processes of procuring, distributing, selling and/or serving food in these institutions or distributing through social protection or welfare programmes, and ensuring it is healthy.

18
Proposed policy priorities for preventing obesity and diabetes
involvement of both boys and girls in daily physical activity as part of a comprehensive education with a whole-school approach to activity before, during and after school hours with measures to reduce time in sedentary activities. For many children, particularly from disadvantaged backgrounds, physical education classes are their only regular physical activity, yet provision of physical education has been in decline globally (50). The right to quality physical education as an essential element of lifelong education is enshrined in UNESCO’s 1978 International Charter of Physical Education and Sport (50).
For adults, there is a need to develop practical guidelines from international experience to improve activity in the workplace, as well as linking these with other preventive health measures. It also recommended that “Sport for all” programmes be promoted and delivered, with a focus on outreach to vulnerable and disadvantaged groups, and should also be based on international experience.
Special arrangements may need to be made for women and new approaches are required so that adults, including older adults, of both sexes recognize the immense benefits of physical activity and meet the current recommended physical activity guidelines.
Urban design is one of the important areas for action. There has been rapid urbanization, dramatic changes in urban design and escalating car use in the often very hot climates of countries of the Region in the last 30–40 years (49).
It is now becoming clear from new analyses of urban design (51) that urban communities, currently expanding throughout the Region, need to incorporate appropriate, shaded walking spaces, preferably with trees, suitable parks and open spaces with congenial settings for walking which promote physical activity (52). There also needs to be a preferential
of the Region (49) and a regional Call to Action was issued, urging high-level decision-makers to implement multisectoral national plans of action (48).
The high prevalence of physical inactivity should not be seen to be an issue solely of individual responsibility, rather the environment in many countries has been designed, in effect, to minimize activity. Thus, governments should recognize their responsibility to change societal arrangements so that physical activity is promoted and not inhibited, through policy actions in the fields of health, education, workplace, sport, communication, urban design and transport.
Priority area for action 4: Food supply and trade – Use food standards, legal instruments and other approaches to improve the national and/or local food supply in this Region of net food-importing countries
Strategic interventions
4.14. Conduct a situation analysis of the national and/or local food supply, including establishing the proportions of fats/oils and sugar used in the diet that are derived from imports and domestic production, along with the extent of food manufacture and processing within the country and the supply of fruit, vegetables and whole grains.
4.15. Facilitate the development of local food policies and encourage city authorities to sign the Milan Urban Food Policy Pact and implement its Framework for Action to develop, where possible, sustainable urban food systems.
4.16. Consider introducing standards or other legal instruments (e.g. compositional standards, tariffs, import restrictions, sales bans, planning laws, zoning policies) to reduce the volume and improve the quality of fats/oils and reduce sugars in the national and local food supply.
4.17. Consider removing agricultural subsidies for producers of sugars and oils (especially those oils high in saturated fatty acids), replacing them, where necessary, with other mechanisms to support farmers and growers.
The high-level forum recommended legislative and implementation measures to ensure the

19
investment in safe, gender-sensitive and age-friendly public transport and the restriction of private car use, as these measures are all associated with greater rates of walking and physical activity (53,54). High residential density in cities and diverse built environments promote widespread physical activity, particularly if public transport surpasses private car use. There is a need to consider specific environmental interventions targeting the built environment, with suitable policies that reduce barriers to physical activity and public transport and other policies to increase space for recreational activity.
Priority area for action 5: Reformulation – Implement a government-led programme of progressive reformulation, adapted to the national context, to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size
Strategic interventions
5.18. Cooperate with other Member States to adopt a regional approach for engaging with food producers to drive food reformulation to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size in a substantial proportion of processed foods.
5.19. Engage with private sector providers of food in catering/food service outlets (including takeaways and street food traders) to establish a programme to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size, with defined quantified reductions in use of these ingredients.
To be able to take action to improve the food supply, policy-makers need first to understand the food system (both at national and local levels) in order to understand where fats and sugars enter the food supply and how access to healthier foods can be improved. Major policy drivers, such as international trade agreements or agricultural policy, greatly influence what food is produced or imported and these policies have not always been consistent with nutrition objectives.
While, in theory, trade policies should support nutrition, in reality such policies may also sometimes undermine healthy diets by, for example, making foods high in fat, salt or sugar (HFSS) more accessible, reducing access to locally-produced nutritious foods or, by encouraging inward foreign direct investment by multinational food companies, facilitating greater exposure to soft drinks and processed foods (55,56). Trade agreements may hinder efforts to tackle obesogenic food environments (those promoting obesity) by constraining governments’ autonomy and the “policy space” available for implementing strong public health nutrition policies (57). Mechanisms are needed to ensure that nutrition concerns are taken into account in trade negotiations (55).
Policy-makers have access to a variety of policy or legal instruments to improve the nutritional quality of the food supply. Depending on the specific context, measures such as tariffs, import quotas, compositional standards or sales bans might be appropriate. Some countries, including some Pacific island states and Ghana, have used such instruments to reduce the availability or increase the price of fats and sugars in the food supply (58–61). International trade and legal expertise is important for the design of appropriate tools within the constraints of current World Trade Organization and other trade agreements. The magnitude of the obesity and diabetes problem in the Region, however, justifies such actions on public health grounds.
Agricultural subsidies, which have usually been designed to support agricultural producers and rarely take nutrition considerations into account, can also have an impact on the food supply and may influence rates of nutrition-related NCDs (62).
Although international trade and national policies are important drivers of the food supply, local policy-makers also have considerable scope to influence food systems
Proposed priority areas for action and strategic interventions

20
Proposed policy priorities for preventing obesity and diabetes
at the city or regional level. Globally, more than 130 cities, including a handful from the Eastern Mediterranean have signed up to the Milan Urban Food Policy Pact, committing to developing sustainable food systems that, among other things, provide healthy and affordable food to all (63). To this end, a Framework for Action sets out nearly 40 strategic options as a starting point for cities to address the development of their own urban food systems.
The ICN2 Framework for Action recommends that countries encourage a progressive reduction of saturated fats, sugars, salt/sodium and trans fats from foods and beverages (16) and WHO identified reformulation as important for the prevention of NCDs (64).
Priority area for action 6: Marketing – Implement appropriate restrictions on marketing (including price promotions) of foods high in fat, sugar and salt
Strategic interventions
6.20. Work with other countries in the Region to establish a coordinated approach, including appropriate legal advice, to reduce the impact of cross-border marketing.
6.21. Implement the WHO Set of Recommendations on Marketing of Foods and Non-alcoholic Beverages to Children and consider mandatory restrictions to eliminate all forms of marketing of foods high in fat, sugar and salt to children and adolescents (up to age 18) across all media, according to the Regional Action Plan to Address Unopposed Marketing of Unhealthy Food and Beverages.
6.22. Use the regional nutrient profile model, which categorizes the appropriate level of nutrients in foods, to identify foods to which the marketing restrictions should apply.
6.23. Conduct an assessment (preferably as part of a regional collaboration) of the impact of marketing of foods high in fat, sugar or salt to adults to illuminate the magnitude of marketing and define how best to restrict inappropriate practices.
6.24. Consider extending mandatory restrictions on marketing of unhealthy foods to the whole population.
6.25. Legislate to allow retail promotion only of healthy foods.
Specifically for the prevention of obesity and diabetes, the process of reformulation to reduce dietary energy density by reducing the fat and sugar content of foods is a particular priority. There is very strong and extensive evidence from many salt reduction programmes that progressive reformulation to lower the concentration of a specific nutrient can reduce the levels in available foods and thereby lower population intakes (65). This experience with salt should be readily transferrable to other nutrients or ingredients. Country experience also shows that trans fats can be virtually removed from foods by effective national or local policy interventions (66).
Progressive reformulation is well tolerated by consumers and can gradually alter consumer preferences (67–69). There is also evidence that a mandatory approach to food reformulation is more cost effective than a voluntary approach (70), and that this is also effective in creating a level playing field for the food industry. Specifying and requiring progressive reductions of the selected nutrients (e.g. salt, fats and sugars) with government-set limits using a combined multinutrient approach, together with comprehensive stakeholder engagement and a commitment to transparent monitoring and evaluation, are all key components of successful reformulation programmes (70). In addition, reformulation programmes should be accompanied by front-of-pack labelling and consumer awareness campaigns.
The potential impact and cost–effectiveness of reformulation programmes will depend on the specific eating patterns in the national context, including aspects such as where and how fats and sugars are added to foods and the scale of the measures implemented. In order to have a meaningful impact, programmes need to cover a significant proportion of processed foods and strive for substantive reductions. Impact could be maximized by reformulating processed foods, cooking ingredients and food provided

21
industry (6). This implies that in many countries mandatory changes are now required.
Country experience shows that measures to restrict marketing of HFSS foods to children and adolescents can reduce children’s exposure to such marketing, but the overall effectiveness depends on which foods are restricted, which age groups are protected, how audiences are targeted and what media and marketing techniques are covered (82–85). Research shows that mandatory restrictions on a national basis are more effective than the voluntary or self-regulatory approaches that have been adopted in many countries (86,87).
Priority area for action 8: Breastfeeding – Implement a package of policies and interventions to promote, protect and support breastfeeding
Strategic interventions
8.28. Promote breastfeeding through mandatory baby-friendly health systems and effective community-based strategies.
8.29. Fully implement the International Code of Marketing of Breast-milk Substitutes and the WHO Guidance on ending inappropriate promotion of foods for infants and young children.
8.30. Empower women to exclusively breastfeed, by enacting progressively increasing remunerated time off work up to a goal of 6 months’ mandatory paid maternity leave, as well as policies that encourage women to breastfeed in the workplace including breastfeeding breaks and provision of suitable facilities.
Modelling studies suggest that marketing restrictions would have a substantial health impact (especially in the longer term since most of the current measures target children). From a cost-benefit point of view, tackling adult obesity can bring much earlier financial benefits. Such measures have very low implementation costs and would be cost effective or cost saving (33,34).
To address these issues the WHO Regional Office for the Eastern Mediterranean has developed a regional action plan to address
in the food services sector (including takeaways which are a growing contributor to the diet in many countries in the Region). Analyses in high-income countries predict considerable population health benefits and estimate that reformulation (mainly salt) would be net cost-saving or very cost effective (70–75).
Populations of all ages are exposed to marketing of HFSS foods through a variety of different channels (e.g. print, broadcast, Internet, social media and others) and using a vast array of marketing techniques.7 There is convincing research that exposure to marketing for HFSS foods influences what and how much children eat (76–80).
Priority area for action 7: Labelling – Implement or revise standards for nutrition labelling to include front-of-pack labelling for all pre-packaged foods
Strategic interventions
7.26. Implement a mandatory front-of-pack nutrition labelling scheme with elements to enable consumers to interpret information easily (e.g. multiple colour-coded traffic lights, use of terms such as “high”, “medium”, “low”).
7.27. Enforce the labelling scheme and monitor its impact, with the potential to strengthen the labelling with suitable health warnings
Concern about the potential negative impact of such marketing led WHO to issue a Set of Recommendations on the Marketing of Foods and Non-Alcoholic Beverages to Children (81). The Commission on Ending Childhood Obesity noted that exposure to marketing of unhealthy foods is still a major issue despite the increasing number of voluntary efforts by
7 Marketing techniques include, for example, advertising, sponsorship, product placement, sales promotion, cross-promotions using celebrities, brand mascots or characters popular with children, web sites, packaging, labelling and point-of-purchase displays, e-mails and text messages, philanthropic activities tied to branding opportunities, and communication through “viral marketing” and by word-of-mouth (154).
Proposed priority areas for action and strategic interventions

22
Proposed policy priorities for preventing obesity and diabetes
where children and adolescents comprise more than half of the population.
Some health advocates and government public health institutions have called for mandatory or voluntary restriction of price promotions on HFSS foods to bring about dietary improvements (75,88,89). Retail price promotions on HFSS foods are increasingly common throughout the Region, including in fast food chains (90). Analyses from high-income countries show that price promotions – such as temporary price reductions, ”multibuy” offers and “extra free” offers – selectively promote HFSS foods and drinks (88,91,92). No examples have been identified yet of regulatory implementation, but some United Kingdom (UK) retailers, for example, have voluntarily restricted price promotions on HFSS foods (88). Given the Region’s extraordinarily high rates of obesity and diabetes, consideration should be given to developing a coherent policy to restrict marketing inducements to eat unhealthy foods.
Three quarters of the world’s population is estimated to live in countries that legally require pre-packaged food labels which provide a breakdown of the nutrient content, and this nutrition information panel is usually on the back (or side) of the package (93). There is growing interest in making nutrition information more accessible, understandable and meaningful for all consumers, since research shows that women, people with higher levels of education and those on particular diets are more likely to use labels (22). Options that have been explored include various forms of front-of-pack labelling for pre-packaged foods, menu and display board labelling for food sold in restaurants/food service outlets, shelf labelling in shops, and specific warning labels on pre-packaged and/or restaurant food.
Many authoritative bodies have called for the introduction of rules on front-of-pack labelling, menu labelling and/or other interpretative labelling schemes (6,94,95). There is evidence
unopposed marketing of unhealthy food and beverages (unpublished) and a nutrient profile model to help Member States define foods for which marketing is to be restricted.8 Region-wide cooperation will be important because cross-border broadcast media dominate the Region, and a human rights-based approach and relevant international law should be applied. Any regional or national measures should incorporate clauses, first, to enable court action to be taken against companies based or incorporated under its jurisdiction but operating across borders and, second, to curtail the right of foreign companies to sue for loss of revenue under international investment law.9
Some countries have been sufficiently concerned about the impact of marketing of HFSS foods on the whole population (not just children) that they have introduced broader limitations on marketing of these foods.10 Restricting all marketing of HFSS foods is a way to protect adult health and to protect adolescents and children from exposure to marketing that is supposedly targeted only at adults. Given that no country has completely eliminated children’s exposure to marketing of HFSS foods by defining child audiences, a whole population approach might well be particularly relevant to the Eastern Mediterranean Region,
8 Nutrient profile model for the marketing of food and non-alcoholic beverages to children in the WHO Eastern Mediterranean Region. Cairo: WHO Regional Office for the Eastern Mediterranean; 2017 (http://applications.emro.who.int/dsaf/EMROPUB_2017_en_19632.pdf?ua=1, accessed 17 July 2017).
9 The United Nations Guiding principles on business and human rights and the Maastricht principles on the extraterritorial obligations of states in the area of economic, social and cultural rights apply here.
10 The Islamic Republic of Iran has prohibited all broadcast advertising of soft drinks and other food items; Ireland has a Code limiting the amount of broadcast advertising of HFSS foods to no more than 25% of advertising time; France requires advertisements for certain foods to carry a healthy diet message.

23
that consumers like simple, interpretive, front-of-pack labels and that this can help them to make healthier choices (93,96,97). Evidence from several high-income countries suggests that interpretive front-of-pack labelling can drive food manufacturers to reformulate their products to make them healthier (40,98–100).
The government costs of introducing, explaining and enforcing compulsory food labelling – although the type of labelling is not specified – are generally estimated to be very low or low (33,34). It is predicted to be cost effective after 20 years and cost-saving after 50 years in low- and middle-income settings (34). It is estimated that the introduction of mandatory front-of-pack, menu and shelf labelling in the UK would be cost effective and would save 575 000 DALYs across the whole of the UK population (75).
It is estimated that universal breastfeeding would avert the deaths of 823 000 children under five years and 20 000 mothers every year (101). In addition to providing protection from respiratory infections, diarrhoeal disease and other common childhood illnesses, breastfeeding11 protects against overweight and obesity in children and adults (102,103). There is also some statistically significant evidence of protection for both the mother and her children against later diabetes (102,104). Some evidence that very early introduction of solid foods is associated with childhood overweight also exists (105,106).
There is highly significant evidence of the substantial positive impact of interventions on exclusive breastfeeding rates in various settings – including health systems and services, home
11 WHO recommends that infants should be exclusively breastfed (giving an infant only breastmilk and no other foods or liquids) for the first six months of life and that, thereafter, infants should receive nutritionally adequate and safe complementary foods, while continuing to breastfeed for up to two years or beyond. Optimal breastfeeding also comprises initiation of breastfeeding within one hour of life.
Priority area for action 9: Mass media campaigns – Conduct mass media campaigns on healthy diet and physical activity
Strategic interventions
9.31. Implement appropriate social marketing campaigns, led by the public sector, on healthy diet and physical activity in order to build consensus, complement the other interventions in the package and encourage behaviour change.
9.32. Ensure sustained implementation of campaigns and monitor their impact.
and family, community, and combinations of settings (107). There is modest evidence of workplace interventions that support, promote or protect breastfeeding on breastfeeding outcomes (107), and guaranteeing paid daily breastfeeding breaks for at least six months is associated with higher breastfeeding rates (108).
Marketing of breast-milk substitutes undermines breastfeeding (109) and national legislation to implement the International Code of Marketing of Breast-milk Substitutes has been shown to diminish the influence of marketing (110). Inappropriate promotion of baby foods also undermines optimal infant and young child feeding (111).
Countries should already be working towards the globally agreed target to increase the rate of breastfeeding in the first six months up to at least 50% by 2025 (Resolution WHA 65.6, 2012). WHO has set out the required actions:
1. Revitalize, expand and institutionalize the Baby-friendly Hospital Initiative in health systems.
2. Provide community-based strategies to support exclusive breastfeeding (e.g. tailored communication campaigns, home visits, support groups and counselling).
3. Implement, monitor and enforce legislation to implement the International Code of Marketing of Breast-milk
Proposed priority areas for action and strategic interventions

24
Proposed policy priorities for preventing obesity and diabetes
maternity protection legislation and regulatory action to counter the marketing of breast-milk substitutes and inappropriate promotion of baby foods (114).
Mass media campaigns to raise public awareness on diet and physical activity are proposed as a WHO “best buy” for tackling unhealthy diet and physical inactivity (12). They also have a role to play in enhancing the public’s understanding of the need for other interventions in order to create a positive climate for policy action.
Long-term, intensive mass media campaigns can change health behaviour (115) and, more specifically, have been shown to be effective for promoting physical activity and moderately effective for promoting healthy diet (116). Intensive campaigns promoting one simple message are also moderately effective (116). Evidence shows that it is challenging to sustain effects after campaigns finish in the face of competing factors, such as pervasive food marketing across many forms of media, so long-term campaigns are more successful (115).
Health education and the use of so-called “nudge” techniques (positive reinforcement and indirect suggestions to try to achieve non-forced compliance) are far more effective if used in conjunction with other measures, such as those in the other priority areas for action (117). Experts advocating for the implementation of interventions such as reformulation, taxation or front-of-pack labelling also argue that accompanying education and information campaigns are required (31,97). Media and education have been used as part of successful multicomponent approaches at national and community levels, but it is difficult to assess the relative contribution of health education to the overall success (22).
Assessments of cost–effectiveness estimate that, after 20 years, such campaigns would be
Substitutes and subsequent relevant World Health Assembly resolutions and WHO’s Guidance on ending the inappropriate promotion of foods for infants and young children (112).
4. Enact mandatory paid maternity leave, ideally for 6 months, as well as policies that encourage women to breastfeed in the workplace and in public.
5. Invest in training and capacity-building in breastfeeding protection, promotion and support.
Priority area for action 10: Health sector interventions – Harness the health sector to enable change and to provide leadership on governance and accountability
Strategic interventions
10.6. Ensure provision of dietary counselling on nutrition, physical activity and healthy weight gain before and during pregnancy for prospective mothers and fathers.
10.7. Integrate screening for overweight and other diabetes risk factors into primary health care and provide primary care-based couselling for high-risk individuals.
10.8. Establish or strengthen, as appropriate, a high-level multisectoral mechanism to define and oversee the implementation of food and physical activity policies for the prevention of obesity and diabetes.
10.9. Establish national targets for obesity and diabetes, along with SMART commitments for action, and work with WHO to develop and implement a monitoring framework for reporting on progress.
10.10. Implement evidence-based community-based interventions, addressing both healthy eating and physical activity, comprising different activities and targeting high-risk groups, to promote and facilitate behaviour change and prevent obesity and diabetes.
Despite the existence of clear guidance and tools, the implementation of laws to protect and promote breastfeeding remains inadequate in most countries (113). There are, nonetheless, examples of countries that have achieved remarkable results through a range of health and community interventions,

25
cost-effective in three of six low- or middle-income countries assessed. After 50 years, costs per DALY saved would drop to between US$ 1994 and US$ 15 211 and the intervention was estimated to be cost effective in four of the six low- or middle-income countries (34).
While most of the proposed priority areas for action depend largely on action from those outside the health sector, there remains a fundamentally important role for the health sector itself. It is important to harness the knowledge and skills of the health workforce – along with the respect and authority often accorded to health professionals – in order to promote, facilitate and support behaviour change.
Good nutrition and a healthy diet before and during pregnancy are important for the health of the mother and her child, and pregnancy may be an optimal time for behaviour change. Excessive weight gain during pregnancy is associated with many adverse short-term and long-term health outcomes for mother, including a higher risk of later obesity and gestational diabetes, and child. Propensity to obesity and diabetes appears to be, at least partially, programmed during early life – especially during the 1000-day period from conception to the child’s second birthday – and can be influenced by a mother’s nutritional status before and during pregnancy (4). Interventions on diet and/or exercise reduce the risk of excessive weight gain during pregnancy by around 20% (118) and WHO recommends counselling about healthy eating and keeping physically active during pregnancy (119). Interventions should be woman-centred, delivered in a non-judgemental manner and developed to ensure appropriate
weight gain.12 Cost implications of diet and exercise interventions are highly variable and, while diet and exercise counselling might have relatively low costs, available health service resources are critical for implementation.
In addition, physician counselling for at-risk groups has been shown to be effective (116) and cost effective (34) and is one of WHO’s “best buys” for preventing diabetes. Primary care-based counselling works best when the information is targeted and there is follow-up from trained personnel, while minimal contact interventions (such as health checks, single-visit counselling or distribution of information) are less effective (116). Primary care interventions are also effective when linked with other stakeholders, such as community groups or ongoing mass media campaigns.
Community-based interventions which comprise many different activities and address both diet and physical activity can be effective (116). Such interventions usually include a strong educational component and may target high-risk groups, such as those who are at a high risk of developing diabetes (116).
The health sector also has a vital – much broader – role to play in providing leadership, engaging other sectors and monitoring progress. While a cross-governmental approach is absolutely essential, the particular perspective and priorities of the Ministry of Health, and all those working in the health sector, will provide key incentives to drive progress in this area. The health sector will also be required to take a leading role in monitoring progress (see section 4 for more on these issues).
12 The definition of “normal” gestational weight gain is subject to regional variations, but should take into consideration pre-pregnant body mass index. According to the Institute of Medicine, women who are underweight at the start of pregnancy (i.e. BMI < 18.5 kg/m2) should aim to gain 12.5–18 kg, women who are normal weight at the start of pregnancy (i.e. BMI 18.5–24.9 kg/m2) should aim to gain 11.5–16 kg, women who are overweight (BMI 25–29.9 kg/m2) should aim to gain 7–11.5 kg and obese women (BMI ≥ 30 kg/m2) should aim to gain 5–9 kg.
Proposed priority areas for action and strategic interventions

26
Proposed policy priorities for preventing obesity and diabetes
4. Implementation of the proposed priority areas for action
Ten priority areas and 37 interventions have been proposed as options for Eastern Mediterranean countries to take action on the growing burden of obesity and diabetes. All of these proposed interventions have a sufficiently strong case to warrant recommending their adoption and are considered to be proportionate responses to the major health and economic burden from these conditions in the Region. This case is based on consideration of the evidence for the effectiveness of these measures (see Annex 2) and practical experience of their implementation (see Annex 3). In a few cases where prior experience of country implementation does not exist, or where there are some evidence gaps, a strong logical basis for action together with international expert support are taken into account. Consideration has been given to implementation costs, along with feasibility issues and political acceptability of the proposed interventions (see Annex 4).
4.1 Multisectoral action is essential
It is very clear from the proposed interventions that action is also required outside the health sector. Health ministers will not be able to act alone. In all of the priority areas for action, the commitment and engagement of other ministries and government bodies will be essential. Fig. 6 illustrates the different sectors that may need to be involved (3). The exact configuration of ministries and other institutions – and their respective roles and responsibilities – will vary from one country to another, but the figure clearly shows the importance of multisectoral collaboration.
This highlights more than ever the need for a whole-of-government and whole-of-society approach to tackling these major public health
problems, which have multiple and inter-related risk factors and determinants.
Political commitment at the highest level is important and political dialogue and advocacy will be important for building that political commitment and enhancing social participation. Effective mechanisms for governance and multisectoral collaboration and coordination are essential. As recommended by the ICN2 Framework for Action, countries should strengthen or establish national cross-government, intersector, multi-stakeholder mechanisms at various levels (including robust safeguards against abuse and conflicts of interest). In order to be most effective, such mechanisms should involve collaboration at a very high level (e.g. ministerial, cabinet-level) and leadership at the highest political level is essential.
4.2 Clear commitments to action and monitoring of progress
Countries are encouraged to make clear commitments to take action on these priority areas and to report on their progress. Member States are urged to make country-specific commitments that are SMART – specific, measurable, achievable, relevant and time-bound – on the 10 areas for action proposed here.
These commitments should also feed into country commitments for action under the United Nations Decade of Action on Nutrition (2016–2025) (Resolution WHA 69.8, 2016) declared to help realize the commitments of the Rome Declaration of Nutrition (15). Countries making commitments for the Decade of Action will be able to showcase their role as nutrition champions taking urgent action for better diet and health–through inclusion of their written commitments in a public repository of international commitments–and will have access to technical support from WHO and the Food and Agriculture Organization of the United Nations.

27
To facilitate the process of measuring and reporting of progress, the WHO Regional Office for the Eastern Mediterranean will work with Member States to establish a monitoring framework and define indicators relevant to the SMART commitments.
4.3 Feasibility issues and phased implementation
All the priority areas and interventions proposed have a sufficiently strong case – based on research evidence and expert analysis of the measures – to warrant recommending their adoption (see Annex 2 for a summary of the evidence). In addition, most of the interventions have been tried and tested in other countries or localities or adopted by innovative policy-makers, and growing country experience has bolstered the evidence base (see Annex 3 for examples of country implementation). Some of the proposed strategic interventions will be easier to implement than others and the challenges of their application, the financial
implications, public acceptance and political feasibility very much depend on the particular country context (see Annex 4 for a summary of feasibility issues).
A phased approach may, therefore, be needed in some countries. The strongest candidate interventions for the first phase of action are shown in Section 5, along with those that it may be more appropriate to implement in a second phase. Countries that are less affected by these feasibility constraints – or which have already implemented many of the first phase interventions – are encouraged to move forward with implementation of all of the strategic interventions as quickly as possible. Importantly, countries should already be taking action and reporting on some of the interventions in both phases in order to meet existing global goals on nutrition and NCDs (e.g. all the breastfeeding interventions, including maternity protection legislation).
Fig. 6 Multisectoral action is needed to implement the proposed priority areas for action to prevent obesity and diabetes
Proposed WHO policies agreed at the UN General Assembly 2011.
President/Prime Minister
Coordinating Ministerial Mechanism/Council
Energy
Industry
Social Welfare
Justice/Security
Health
Regional and local
HEALTH POLICY GROUP
Nongovernmental organizations and
consumer representatives
Trade
Food
Education
Communication
Urban Planning
Housing
Environment
Transport
Sports
AgricultureTreasury
Foreign Affairs
The range of socio-economic/regional groups within the population
Health Services
government
Farming/food/retail/marketing/sports/ motor industry etc.
Private sector e.g.
WHO 2012: Options for strengthening and facilitating multisectoral action for the prevention and control of non- communicable diseases(NCD) through effective partnership. Transmitted by the UN Secretary General to all Member states following the UN General Assembly approval for an action plan on NCDs
Proposed WHO policies agreed at the UN General Assembly 2011.
President/Prime Minister
Coordinating Ministerial Mechanism/Council
Energy
Industry
Social Welfare
Justice/Security
Health
Regional and local
HEALTH POLICY GROUP
Nongovernmental organizations and
consumer representatives
Trade
Food
Education
Communication
Urban Planning
Housing
Environment
Transport
Sports
AgricultureTreasury
Foreign Affairs
The range of socio-economic/regional groups within the population
Health Services
government
Farming/food/retail/marketing/sports/ motor industry etc.
Private sector e.g.
WHO 2012: Options for strengthening and facilitating multisectoral action for the prevention and control of non- communicable diseases(NCD) through effective partnership. Transmitted by the UN Secretary General to all Member states following the UN General Assembly approval for an action plan on NCDs
Implementation of the proposed priority areas for action

28
Proposed policy priorities for preventing obesity and diabetes
Table 2. Summary of proposed priority areas of action and strategic interventions for preventing obesity and diabetes in the Eastern Mediterranean Region and their implementation phaseArea for action Interventions most suitable for first phase implementation Interventions for which there is
evidence of impact, but which it may be more appropriate to implement in a second phase
1 Fiscal measures 1.1 Progressively eliminate national subsidies for all types of fats/oils and sugar.
1.2 Implement an effective tax on sugar-sweetened beverages.
1.3 Consider an effective progressive tax on high fat foods and on high sugar foods.
2 Public procurement 2.1 Implement mandatory nutrition standards across all public institutions through (a) application of the regional nutrient profile model to assess the nutritional quality of different foods, (b) introduction of meal standards and (c) measures to eliminate the sale of foods or drinks high in fat, sugar or salt.
2.2 Issue mandatory guidelines for the revision of procurement to provide healthy food, including limiting the volume of fats/oils, sugar and salt entering public sector catering facilities in order to facilitate the necessary menu changes (e.g. so that meals provide not more than 25% energy from fats and less than 5% from free sugars).
2.3 Develop guidance and provide training to catering companies on appropriate catering methods in public institutions to reduce the use of frying and sweetening of foods and help with menu design.
2.4 Continue implementing these measures, scaling up coverage and monitoring impact.
3 Physical activity interventions
3.1 Promote healthy physical activity through mass media campaigns (see priority area 9) and ensure adequate legislation supporting delivery of daily physical activity for students in schools and universities.
3.2 Ensure comprehensive delivery of regular, quality physical education to all children, as a key component of education in schools.
3.3 Develop a set of standards/guidelines promoting physical activity in the workplace, including facility/building design, availability of sports facilities and programmes enabling access to facilities away from the workplace.
3.4 Increase availability of and accessibility for participation in formal and informal recreational and sporting activities, particularly providing opportunities for participation in programmes such as “Sports-for-All”, with emphasis on ensuring equality of access and opportunity for participation.
3.5 Develop and implement an urban planning policy to ensure that urban environments encourage people to rely less on personal motorized vehicles and support access to safe, gender-sensitive and age-friendly public transport, cycling and walking, including by provision of facilities, equipment, open and green public space and shared use of school facilities (both indoor and outdoor).
3.6 Continue implementing these measures, scaling up coverage and monitoring impact.

29
Table 2. Summary of proposed priority areas of action and strategic interventions for preventing obesity and diabetes in the Eastern Mediterranean Region and their implementation phaseArea for action Interventions most suitable for first phase implementation Interventions for which there is
evidence of impact, but which it may be more appropriate to implement in a second phase
4 Food supply and trade
4.1 Conduct a situation analysis of the national and/or local food supply, including establishing the proportions of fats/oils and sugar used in the diet that are derived from imports and domestic production, along with the extent of food manufacture and processing within the country and the supply of fruit, vegetables and whole grains.
4.2 Facilitate the development of local food policies and encourage city authorities to sign the Milan Urban Food Policy Pact and implement its Framework for Action to develop, where possible, sustainable urban food systems.
4.3 Consider introducing standards or other legal instruments (e.g. compositional standards, tariffs, import restrictions, sales bans, planning laws, zoning policies) to reduce the volume and improve the quality of fats/oils and reduce sugars in the national and local food supply.
4.4 Consider removing agricultural subsidies for producers of sugars and oils (especially those oils high in saturated fatty acids), replacing them, where necessary, with other mechanisms to support farmers and growers.
5 Reformulation 5.1 Cooperate with other Member States to adopt a regional approach for engaging with food producers to drive food reformulation to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size in a substantial proportion of processed foods.
5.2 Engage with private sector providers of food in catering/food service outlets (including takeaways and street food traders) to establish a programme to eliminate trans fats and reduce progressively total and saturated fat, salt, sugars, energy and portion size, with defined quantified reductions in use of these ingredients.
6 Marketing 6.1 Work with other countries in the Region to establish a coordinated approach, including appropriate legal advice, to reduce the impact of cross-border marketing.
6.2 Implement the WHO Set of Recommendations on Marketing of Foods and Non-alcoholic Beverages to Children and consider mandatory restrictions to eliminate all forms of marketing of foods high in fat, sugar and salt to children and adolescents (up to age 18) across all media, according to the Regional Action Plan to Address Unopposed Marketing of Unhealthy Food and Beverages.
6.3 Use the regional nutrient profile model, which categorizes the appropriate level of nutrients in foods, to identify foods to which the marketing restrictions should apply.
6.4 Conduct an assessment (preferably as part of a regional collaboration) of the impact of marketing of foods high in fat, sugar or salt to adults to illuminate the magnitude of marketing and define how best to restrict inappropriate practices.
6.5 Consider extending mandatory restrictions on marketing of unhealthy foods to whole population.
6.6 Legislate to allow retail promotion only of healthy foods.
7 Labelling 7.1 Implement a mandatory front-of-pack labelling scheme with elements to enable consumers to interpret information easily (such as colour coding or the use of terms such as “high”, “medium”, ”low”).
7.2 Enforce the labelling scheme and monitor its impact with the potential to strengthen the labelling with suitable health warnings.
(cont.)
Implementation of the proposed priority areas for action

30
Proposed policy priorities for preventing obesity and diabetes
Table 2. Summary of proposed priority areas of action and strategic interventions for preventing obesity and diabetes in the Eastern Mediterranean Region and their implementation phaseArea for action Interventions most suitable for first phase implementation Interventions for which there is
evidence of impact, but which it may be more appropriate to implement in a second phase
8 Breastfeeding 8.1 Promote breastfeeding through mandatory baby-friendly health systems and effective community-based strategies.
8.2 Fully implement the International Code of Marketing of Breast-milk Substitutes and the WHO Guidance on ending inappropriate promotion of foods for infants and young children.
8.3 Empower women to exclusively breastfeed, by enacting progressively increasing remunerated time off work up to a goal of 6 months’ mandatory paid maternity leave, as well as policies that encourage women to breastfeed in the workplace including breastfeeding breaks and provision of suitable facilities.
9 Mass media campaigns
9.1 Implement appropriate social marketing campaigns, led by the public sector, on healthy diet and physical activity in order to build consensus, complement the other interventions in the package and encourage behaviour change.
9.2 Ensure sustained implementation of campaigns and monitor their impact.
10. Health sector interventions
10.1 Ensure provision of dietary counselling on nutrition, physical activity and healthy weight gain before and during pregnancy for prospective mothers and fathers.
10.2 integrate screening for overweight and other diabetes risk factors into primary health care and provide primary-care based counselling for high-risk individuals.
10.3 Establish or strengthen, as appropriate, a high-level multisectoral mechanism to define and oversee the implementation of food and physical activity policies for the prevention of obesity and diabetes.
10.4 Establish national targets for obesity and diabetes, along with SMART commitments for action, and work with WHO to develop and implement a monitoring framework for reporting on progress.
10.5 Implement evidence-based community-based interventions, addressing both healthy eating and physical activity, comprising different activities and targeting high-risk groups, to promote and facilitate behaviour change and prevent obesity and diabetes.
(cont.)

31
References
References1. Global report on diabetes. Geneva: World Health Organization; 2016.2. World Health Statistics 2016. Monitoring health for the SDGs. Geneva: World Health
Organization; 2016.3. United Nations General Assembly. Note by the Secretary-General transmitting the
report of the Director-General of the World Health Organization on options for strengthening and facilitating multisectoral action for the prevention and control of non-communicable diseases through effective partnership (A/67/373 2012) (http://www.who.int/nmh/events/2012/20121128.pdf?ua=1, accessed 2 February 2017).
4. Good maternal nutrition; the best start in life. Copenhagen: World Health Organization Regional Office for Europe; 2016.
5. Poston L, Harthoorn LF, van der Beek EM. Obesity in pregnancy: implications for the mother and lifelong health of the child. A Consensus Statement. Pediatr Res. 2011;69(2):175-80.
6. Report of the Commission on Ending Childhood Obesity. Geneva: World Health Organization; 2016.
7. Diet, nutrition and the prevention of chronic diseases. Geneva: World Health Organization; 2003 (Technical report series, No. 916).
8. Guideline : Sugars intake for adults and children. Geneva: World Health Organization; 2015.
9. Abu-Rabia A. Indigenous medicine among the Bedouin in the Middle East. New York: Berghahn Books; 2015.
10. Food and Agriculture Organization of the United Nations. FAOSTAT. Supply Utilization Accounts and Food Balances Domain: Food Balance Sheets. 2014 (http://faostat3.fao.org/download/FB/FBS/E, accessed 19 February 2017).
11. Food and Nutrition in Numbers 2014. Rome: Food and Agriculture Organization of the United Nations (FAO-UN); 2014 (http://www.fao.org/publications/card/en/c/9f31999d-be2d-4f20-a645-a849dd84a03e/, accessed 19 February 2017).
12. Global status report on noncommunicable diseases. Geneva: World Health Organization; 2010.
13. Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases. Resolution A/RES/66/2, UN General Assembly, 19 September 2011.
14. Framework for action to implement the United Nations Political Declaration on Noncommunicable Diseases. Cairo: World Health Organization Regional Office for the Eastern Mediterranean; 2015.
15. Food and Agriculture Organization of the United Nations/World Health Organization. Second International Conference on Nutrition, Rome, 19-21 November 2014. Conference Outcome Document: Rome Declaration on Nutrition (http://www.fao.org/3/a-ml542e.pdf, accessed 1 February 2017).

32
Proposed policy priorities for preventing obesity and diabetes
16. Food and Agriculture Organization of the United Nations/World Health Organization. Second International Conference on Nutrition, Rome, 19–21 November 2014. Conference Outcome Document: Framework for Action (http://www.fao.org/3/a-mm215e.pdf, accessed 1 February 2017).
17. Gostin LO Abou-Taleb H, Roache SA, Alwan A.. Legal priorities for prevention of non-communicable diseases: innovations from WHO’s Eastern Mediterranean region. Public Health. 2017;144:4–12.
18. Fiscal policies for diet and the prevention of noncommunicable diseases. Technical Meeting Report 5–6 May 2015, Geneva, Switzerland. Geneva: World Health Organization Regional Office for Europe; 2016.
19. Using price policies to promote healthier diets. Copenhagen: World Health Organization Regional Office for Europe; 2015.
20. Thow AM, Downs S, Jan S. A systematic review of the effectiveness of food taxes and subsidies to improve diets: Understanding the recent evidence. Nutr Rev. 2014;72(9):551–65.
21. Powell LM, Chriqui JF, Khan T, Wada R, Chaloupka FJ. Assessing the potential effectiveness of food and beverage taxes and subsidies for improving public health: a systematic review of prices, demand and body weight outcomes. Obes Rev. 2013;14(2):110–28.
22. Mozaffarian D, Afshin A, Benowitz NL, Bittner V, Daniels SR, Franch HA, et al. Population Approaches to Improve Diet, Physical Activity, and Smoking Habits A Scientific Statement From the American Heart Association. Circulation. 2012 Sep 18;126(12):1514–63.
23. Sugar reduction : the evidence for action. Annexe 2: Review of behaviour changes resulting from experimental studies of fiscal methods. A mixed method review of behaviour changes resulting from experimental studies that examine the effect of fiscal measures targeted at high sugar food and non-alcoholic drink. London: Public Health England; 2015.
24. Colchero MA, Popkin BM, Rivera JA, Ng SW. Beverage purchases from stores in Mexico under the excise tax on sugar sweetened beverages: observational study. BMJ. 2016 Jan 6;352:h6704. doi: 10.1136/bmj.h6704
25. Taxes on sugar-sweetened beverages as a public health strategy: the experience of Mexico. Washington DC: Pan American Health Organization; 2015.
26. Popkin BM, Hawkes C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diabetes Endocrinol. 2016;4(2):174-86. 10.1016/S2213-8587(15)00419-2
27. Biro A. Did the junk food tax make the Hungarians eat healthier? Food Policy. 2015;54:107–15.
28. Jensen JD, Smed S. The Danish tax on saturated fat: Short run effects on consumption and consumer prices of fats. FOI Working Paper 2012/14. Copenhagen: Institute of Food and Resource Economics University of Copenhagen; 2014.

33
References
29. Smed S, Scarborough P, Rayner M, Jensen JD. The effects of the Danish saturated fat tax on food and nutrient intake and modelled health outcomes: an econometric and comparative risk assessment evaluation. Eur J Clin Nutr. 2015 April;2016:1–6.
30. Bodker M, Pisinger C, Toft U, Jørgensen T. The rise and fall of the world’s first fat tax. Health Policy. 2015 Jun;119(6):737–42.
31. Hawkes C, Smith TG, Jewell J, Wardle J, Hammond RA, Friel S, et al. Smart food policies for obesity prevention. Lancet. 2015 Jun 13;385(9985):2410–21.
32. Sassi F. Obesity and the economics of prevention - fit not fat. Paris: Organisation for Economic Co-operation and Development; 2010.
33. Vos T, Carter R, Barendregt J, Mihalopoulos C, Veerman L, Magnus, et al. Assessing cost-effectiveness in prevention (ACE-Prevention): Final Report. Brisbane, University of Queensland and Melbourne, Deakin University; 2010.
34. Cecchini M, Sassi F, Lauer JA, Lee YY, Guajardo-Barron V, et al. Tackling of unhealthy diets, physical inactivity, and obesity: Health effects and cost-effectiveness. Lancet. 2010 Nov 20;376(9754):1775–84.
35. Sdralevich C, Sab R, Zouhar Y, Albertin G. Subsidy reform in the Middle East and North Africa: recent progress and challenges ahead. Washinton DC: International Monetary Fund; 2014.
36. Ayadi M Ayadi M, Castel V, Lannes L, Abderrahim K, Mansour S, Jmal Y, et al. Food subsidies and direct social assistance: towards better targeting of monetary poverty and deprivations in Tunisia. African Development Bank, 2014 (https://www.afdb.org/fileadmin/uploads/afdb/Documents/Procurement/Project-related-Procurement/Food_Subsidies_and_Direct_Social_Assistance-_Towards_Better_Targeting_of_Monetary_Poverty_and_Deprivations_in_Tunisia.pdf, accessed 1 February 2017).
37. Niebylski ML, Lu T, Campbell NR, Arcand J, Schermel A, Hua D, et al. Healthy Food Procurement Policies and Their Impact. Int J Environ Res Public Health. 2014;11(3):2608–27.
38. Chriqui JF, Pickel M, Story M. Influence of school competitive food and beverage policies on obesity, consumption, and availability: a systematic review. JAMA Pediatr. 2014;168(3):279–86.
39. Power Up for Health. Impact of healthy food procurement policies/programs and nutrition standards on sales, intake and availability of healthier food, and body weight status overview. Evidence synthesis, July 2014 (https://powerupforhealth.files.wordpress.com/2015/03/food-procurement_power-up.pdf, accessed 1 February 2017).
40. Afshin A, Penalvo J, Del Gobbo L, Kashaf M, Micha R, Morrish K, et al. CVD prevention through policy: a review of mass media, food/menu labeling, taxation/subsidies, built environment, school procurement, worksite wellness, and marketing standards to improve diet. Curr Cardiol Rep. 2015;17(11).
41. Global nutrition policy review: what does it take to scale up nutrition action? Geneva: World Health Organization; 2013:122 (http://apps.who.int/iris/bitstream/10665/84408/1/9789241505529_eng.pdf, accessed 1 February 2017).

34
Proposed policy priorities for preventing obesity and diabetes
42. De Schutter O (United Nations special rapporteur on the right to food). The power of procurement: public purchasing in the service of realizing the right to food. Briefing Note 08 - April 2014 (http://reliefweb.int/sites/reliefweb.int/files/resources/20140514_procurement_en.pdf, accessed 1 February 2017).
43. Global Nutrition Report 2016: From promise to impact: ending malnutrition by 2030. Washington DC: International Food Policy Research Institute; 2016.
44. Noonan KG, Sell K, Miller D, Rubin D. Government purchasing to improve public health: theory practice and evidence (April 17, 2013). Public Health Law Research, March 13, 2013.
45. Lederer A, Curtis CJ, Silver LD, Angell SY, et al. Toward a healthier city: nutrition standards for New York City government. Am J Prev Med. 2014;46(4):423–8.
46. New York Academy of Medicine. Policy Brief : Healthy food procurement policy for New York State. March 2012 (http://www.dashny.org/wp-content/uploads/2016/01/HealthyFoodProcurementPolicy.pdf, accessed 2 February 2017).
47. Freudenberg N. Healthy-food procurement: using the public plate to reduce food insecurity and diet-related diseases. Lancet Diabetes Endocrinol. 2016;4(5):383–4.
48. Move for health: Promoting physical activity through the life course. Cairo: World Health Organization Regional Office for the Eastern Mediterranean; 2014.
49. Promoting physical activity: A regional call to action. East Mediterr Health J. 2014 Jul 8;20(7):469–71.
50. Quality physical education: guidelines for policy-makers. Paris: United Nations Educational, Scientific and Cultural Organization; 2015.
51. Sallis JF Bull F, Burdett R, Frank LD, Griffiths P, Giles-Corti B. Use of science to guide city planning policy and practice: how to achieve healthy and sustainable future cities. Lancet. 2016 Dec 10;388(10062):2936–47.
52. de Blasio B. Healthier neighbourhoods through healthier parks. Lancet. 2016 Dec 10;388(10062):2850-1.
53. Kleinert S, Horton R. Urban design: an important future force for health and wellbeing. Lancet. 2016 Dec 10;388(10062):2848–50.
54. Goenka S, Andersen LB. Urban design and transport to promote healthy lives. Lancet (London, England). 2016 Dec 10;388(10062):2851–3.
55. Hawkes C. Enhancing coherence between trade policy and nutrition action: implementing the framework for action of the Second International Conference on Nutrition. Discussion Paper 1. Geneva: United Nations System Standing Committee on Nutrition; 2016 (http://www.unscn.org/files/ICN2_TPM/UNSCN_ENGLISH_Trade_and_Nutrition_Dec_2015.pdf, accessed 1 February 2017).
56. Stuckler D, McKee M, Ebrahim S, Basu S, et al. Manufacturing epidemics: The role of global producers in increased consumption of unhealthy commodities including processed foods, alcohol, and tobacco. PLoS Med. 2012;9(6):10.
57. Thow AM, McGrady B. Protecting policy space for public health nutrition in an era of international investment agreements. Bull World Health Organ. 2014;92(2):139–45.

35
References
58. Snowdon W, Thow AM. Trade policy and obesity prevention: Challenges and innovation in the Pacific Islands. Obes Rev. 2013;14 S2:150–8.
59. Thow AM, Swinburn B, Colagiuric S, Diligolevud M, Questede C, Vivilif P, et al. Trade and food policy: Case studies from three Pacific Island countries. Food Policy. 2010;35(6):556–64.
60. Thow AM, Annan R, Mensah L, Chowdhury SN. Development, implementation and outcome of standards to restrict fatty meat in the food supply and prevent NCDs: learning from an innovative trade/food policy in Ghana. BMC Public Health. 2014;14(1):249.
61. Thow AM, Quested C, Juventin L, Kun R, Khan AN, Swinburn B. Taxing soft drinks in the Pacific: Implementation lessons for improving health. Health Promot Int. 2011;26(1):55–64.
62. Dangour AD, Hawkesworth S, Shankar B, Watson L, Srinivasan CS, Morgan EH, et al. Can nutrition be promoted through agriculture-led food price policies? A systematic review. BMJ open, 2013, 3(6):e002937.
63. Milan Urban Food Policy Pact [website] (http://www.milanurbanfoodpolicypact.org/, accessed 1 February 2017).
64. WHO Global Coordination Mechanism Working Groups. Policy brief: producing and promoting more food products consistent with a healthy diet. Geneva: World Health organization; 2014 (http://www.who.int/nmh/ncd-coordination-mechanism/Policybrief32.pdf, accessed 1 February 2017).
65. Trieu K, Neal B, Hawkes C, Dunford E, Campbell N, Rodriguez-Fernandez R, et al. Salt reduction initiatives around the world - a systematic review of progress towards the global target. PLoS One. 2015;10(7):e0130247.
66. Downs SM, Thow AM, Leeder SR. The effectiveness of policies for reducing dietary trans fat: a systematic review of the evidence. Bull World Health Organ. 2012 November;2013(91):262-9.
67. Jaenke R, Barzi F, McMahon E, Webster J, Brimblecombe J. Consumer acceptance of reformulated food products: a systematic review and meta-analysis of salt-reduced foods. Crit Rev Food Sci Nutr, 2016, 8398(January 2016):0.
68. Bertino M, Beauchamp GK, Engeiman K. Long term reduction in dietary sodium alters the taste of salt. Am J Clin Nutr. 1982;36:1134–44.
69. Blais CA, Pangborn RM, Borhani NO, Ferrell MF, Prineas RJ, Laing B. Effect of dietary sodium restriction on taste responses to sodium chloride: a longitudinal study14. Am J Clin Nutr. 1986 Aug;44(2):232–43.
70. Effectiveness of food reformulation as a strategy to improve population health. Canberra: National Heart Foundation of Australia; 2012.
71. Cobiac LJ, Magnus A, Lim S, Barendregt JJ, Carter R, Vos T. Which interventions offer best value for money in primary prevention of cardiovascular disease? PLoS One. 2012;7(7).

36
Proposed policy priorities for preventing obesity and diabetes
72. Barton P, Andronis L, Briggs A, McPherson K, Capewell S. Effectiveness and cost effectiveness of cardiovascular disease prevention in whole populations: modelling study. BMJ. 2011 Jul 28;343:d4044.
73. List G. Processing and reformulation for nutrition labelling of trans fatty acids. Lipid Technology. 2004;16:173–6.
74. Joffres MR, Campbell NR, Manns B, Tu K. Estimate of the benefits of a population-based reduction in dietary sodium additives on hypertension and its related health care costs in Canada. Can J Cardiol. 2007 May 1;23(6):437–43.
75. Overcoming obesity : An initial economic analysis. Discussion paper. McKinsey Global Institute; 2014:120.
76. Boyland EJ, Nolan S, Kelly B, Tudur-Smith C, Jones A, Halford JC, et al. Advertising as a cue to consume: a systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. Am J Clin Nutr. 2016 Feb;103(2):519–33.
77. Osei-Assibey G, Dick S, Macdiarmid J, Semple S, Reilly JJ, Ellaway A, et al. The influence of the food environment on overweight and obesity in young children: a systematic review. BMJ Open. 2012 Dec 18;2(6).
78. Harris JL, Speers SE, Schwartz MB, Brownell KD. US Food Company Branded Advergames on the Internet: Children’s exposure and effects on snack consumption. J Child Media. 2012;6(1):51–68.
79. Scully M, Wakefield M, Niven P, Chapman K, Crawford D, Pratt IS, et al. Association between food marketing exposure and adolescents’ food choices and eating behaviors. Appetite. 2012 Feb;58(1):1–5.
80. Sugar reduction : the evidence for action. Annexe 3 : Review of behaviour changes resulting from marketing strategies. A mixed method review of behaviour changes resulting from marketing strategies targeted at high sugar food and non-alcoholic drink. London: Public Health England; 2015.
81. Set of recommendations on the marketing of foods and non-alcoholic beverages to children. Geneva: World Health Organization; 2010 (http://apps.who.int/iris/bitstream/10665/44416/1/9789241500210_eng.pdf, accessed 1 February, 2017).
82. Smithers LG, Lynch JW, Merlin T. Industry self-regulation and TV advertising of foods to Australian children. J Paediatr Child Health. 2014;50(5):386–92.
83. HFSS advertising restrictions: Final Review. London: Ofcom; 2010.84. Scarborough P, Payne C, Agu CG, Kaur A, Mizdrak A, Rayner M, et al. How
important is the choice of the nutrient profile model used to regulate broadcast advertising of foods to children? A comparison using a targeted data set. Eur J Clin Nutr. 2013 Aug;67(8):815–20.
85. Brinsden H, Lobstein T. Comparison of nutrient profiling schemes for restricting the marketing of food and drink to children. Pediatr Obes. 2013;8(4):325–37.
86. Galbraith-Emami S, Lobstein T. The impact of initiatives to limit the advertising of food and beverage products to children: a systematic review. Obes Rev. 2013 Dec;14(12):960–74.

37
References
87. Chambers SA, Freeman R, Anderson AS, MacGillivray S. Reducing the volume, exposure and negative impacts of advertising for foods high in fat, sugar and salt to children: A systematic review of the evidence from statutory and self-regulatory actions and educational measures. Prev Med. 2015 Jun;75:32–43.
88. More supermarket promotions on less healthy food. Which? 4 August 2016 [Press release] (https://press.which.co.uk/whichpressreleases/more-supermarket-promotions-on-less-healthy-food/, accessed 1 February 2017).
89. Tedstone A, Targett V, Allen R. Sugar reduction: the evidence for action. London: Public Health England; 2015.
90. Bakr A, Tawii C, Jarmalaite D, Sherif F, Hanana H, Levi T. Major consumer foodservice trends in MEA, 2016 [web site] (http://blog.euromonitor.com/2016/02/major-consumer-foodservice-trends-in-mea.html, accessed 1 February 2017).
91. Sugar reduction: the evidence for action. Annexe 4 : An analysis of the role of price promotions on the household purchases of food and drinks high in sugar. London: Public Health England; 2015.
92. Nakamura R, Suhrcke M, Jebb SA, Pechey R, Almiron-Roig E, Marteau TM, et al. Price promotions on healthier compared with less healthy foods: A hierarchical regression analysis of the impact on sales and social patterning of responses to promotions in Great Britain. Am J Clin Nutr. 2015 Apr;101(4):808–16.
93. Mandle J, Tugendhaft A, Michalow J, Hofman K. Nutrition labelling: a review of research on consumer and industry response in the global South. Glob Health Action. 2015;8(1):1–10.
94. Committee on Accelerating Progress in Obesity Food and Nutrition Board. Glickman D, Parker L, Sim LJ, Del Valle Cook H,Miller EA, editors. Accelerating progress in obesity prevention: solving the weight of the nation. Washington DC: National Academies Press (US); 2012.
95. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016 Aug 1;37(29):2315–81.
96. Hersey JC, Wohlgenant KC, Arsenault JE, Kosa KM, Muth MK. Effects of front-of-package and shelf nutrition labeling systems on consumers. Nutr Rev. 2013 Jan;71(1):1–14.
97. Hawley KL, Roberto CA, Bragg MA, Liu PJ, Schwartz MB, Brownell KD. The science on front-of-package food labels. Public Health Nutr. 2013 Mar;16(3):430–9.
98. Vyth EL, Steenhuis IH, Roodenburg AJ, Brug J, Seidell JC. Front-of-pack nutrition label stimulates healthier product development: a quantitative analysis. Int J Behav Nutr Phys Act. 2010 Sep 8;7:65.
99. Young L, Swinburn B. Impact of the pick the tick food information programme on the salt content of food in New Zealand. Health Promot Int. 2002;17(1):13–9.

38
Proposed policy priorities for preventing obesity and diabetes
100. Eckel RH, Borra S, Lichtenstein AH, Yin-Piazza SY; Trans Fat Conference Planning Group. Understanding the complexity of trans fatty acid reduction in the American diet: American Heart Association Trans Fat Conference 2006: report of the Trans Fat Conference Planning Group. Circulation. 2007;115(16):2231–46.
101. Victora CG, Rollins NC, Murch S, Krasevec J, Bahl R. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016 May 21;387(10033):2089–90.
102. Horta BL, de Mola CL, Victora CG. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure, and type-2 diabetes: systematic review and meta-analysis. Acta Paediatr. 2015 Dec;104(467):30–7.
103. Yan J, Liu L, Zhu Y, Huang G, Wang PP. The association between breastfeeding and childhood obesity: a meta-analysis. BMC Public Health. 2014 Dec 13;14:1267. doi: 10.1186/1471-2458-14-1267.
104. Chowdhury R, Sinha B, Sankar MJ, Taneja S, Bhandari N, Rollins N, et al. Breastfeeding and maternal health outcomes: a systematic review and meta-analysis. Acta Paediatr. 2015 Dec;104(467):96–113.
105. Weng SF, Redsell SA, Swift JA, Yang M, Glazebrook CP. Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Child. 2012;97(12):1019–26.
106. Pearce J, Taylor MA, Langley-Evans SC. Timing of the introduction of complementary feeding and risk of childhood obesity: a systematic review. Int J Obes (Lond). 2013 Oct;37(10):1295–306.
107. Sinha B, Chowdhury R, Sankar MJ, Martines J, Taneja S, Mazumder S, et al. Interventions to improve breastfeeding outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015;104 Suppl 467:114–34.
108. Heymann J, Raub A, Earle A. Breastfeeding policy: a globally comparative analysis. Bull World Health Organ. 2013 Jun 1;91(6):398–406.
109. Piwoz EG, Huffman SL. The impact of marketing of breast-milk substitutes on WHO-Recommended breastfeeding practices. Food Nutr Bull. 2015;36(4):1–14.
110. Infant and Young Child Feeding Programme Review - Consolidated report of six country programme review. New York: United Nations Children’s Fund; 2010.
111. Resolution WHA63.23. Infant and young child nutrition. In: Sixty-Third World Health Assembly, Geneva, 17-21 May 2010. Resolutions and Decisions Annexes.
112. Maternal, infant and young child nutrition. Guidance on ending the inappropriate promotion of foods for infants and young children. Report by the Secretariat. Geneva: World Health Organization; 2016 (A69/7 Add.1) (http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_7Add1-en.pdf?ua=1, accessed 1 February 2017).
113. World Health Organization, United Nations Children’s Fund and International Baby Food Action Network. Marketing of breast-milk substitutes: national implementation of the International Code. Status Report 2016. Geneva: World Health Organization; 2016.

39
References
114. World Health Organization and United Nations Children’s Fund. Global nutrition targets 2025. Breastfeeding Policy Brief (WHO/MNH/NHD 14.7). Geneva: World Health Organization; 2014.
115. Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet. 2010;376(9748):1261–71.
116. Interventions on diet and physical activity: What works summary report. Geneva: World Health Organization; 2009:48.
117. House of Lords. Science and Technology Select Committee. 2nd Report of Session 2010-12. Behaviour Change. London: The Stationery Office Limited; 2011 (https://www.publications.parliament.uk/pa/ld201012/ldselect/ldsctech/179/179.pdf, accessed 1 February 2017).
118. Muktabhant B, Lawrie TA, Lumbiganon P, Laopaiboon M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst Rev. 2015; (6):CD007145.
119. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization; 2016.
120. Summary report on developing an action plan for preventing obesity and diabetes in the Eastern Mediterranean Region, Geneva, 31 May–1 June 2016. Cairo: WHO Regional Office for the Eastern Mediterranean; 2017 (http://applications.emro.who.int/docs/IC_Meet_Rep_2017_EN_19541.pdf?ua=1, accessed 1 February 2017).
121. Laine J, Kuvaja-Köllner V, Pietilä E, Koivuneva M, Valtonen H, Kankaanpää E. Cost-effectiveness of population-level physical activity interventions: a systematic review. Am J Health Promot. 2014;29(2):71-80.
122. Scaling up action against noncommunicable diseases: How much will it cost? Geneva: World Health Organization; 2011:51.
123. Centers for Disease Control and Prevention. Strategies to prevent obesity and other chronic diseases: The CDC Guide to Strategies to Increase Physical Activity in the Community. Atlanta, GA: U.S. Department of Health and Human Services; 2011.
124. Proper K, Van Mechelen W. Effectiveness and economic impact of worksite interventions to promote physical activity and healthy diet. Background paper prepared for the WHO/WEF Joint Event on Preventing Noncommunicable Diseases in the Workplace (Dalian/China, September 2007). Geneva: World Health Organization; 2007:1-63.
125. Roux L, Pratt M, Tengs TO, Yore MM, Yanagawa TL, Van Den Bos J, et al. Cost effectiveness of community-based physical activity interventions. Am J Prev Med. 2008;35(6):578-88.
126. Holla-Bhar R, Iellamo A, Gupta A, Smith JP, Dadhich JP. Investing in breastfeeding - the world breastfeeding costing initiative. Int Breastfeed J. 2015;10(1):1–12. 10.1186/s13006-015-0032-y.
127. Dodd JM, Ahmed S, Karnon J, Umberger W, Deussen AR, Tran T, et al. The cost-effectiveness of providing antenatal lifestyle advice for women who are overweight or obese: the LIMIT randomised trial. BMC Obesity. 2015;2(1):14.

40
Proposed policy priorities for preventing obesity and diabetes
128. Breisinger IC, Al-Riffai P, Ecker O; Abuismail R, Waite J, Abdelwahab N, et al. Tackling Egypt’s rising food insecurity in a time of transition. Cairo: International Food Policy Research Institute and World Food Programme; 2013 (Joint IFPRI-WFP Country Policy Note) (http://documents.wfp.org/stellent/groups/public/documents/ena/wfp257519.pdf, accessed 1 February 2017).
129. Hyde M. Morsy issues broad tax increases, including energy, soft drinks, cigarettes, alcohol. Egypt Independent, 9 December 2012 http://www.egyptindependent.com//news/morsy-issues-broad-tax-increases-including-energy-soft-drinks-cigarettes-alcohol-0, accessed 1 February 2017).
130. Review of NCDs and Mental Health Programme in the Islamic Republic of Iran. Mission report. Cairo: World Health Organization Regional Office for the Eastern Mediterranean; 2016.
131. GCC to impose heavy tax on tobacco, soft drinks. Middle East Monitor, 9 January 2017 (https://www.middleeastmonitor.com/20170109-gcc-to-impose-heavy-tax-on-tobacco-soft-drinks/, accessed 2 February 2017).
132. World Cancer Research Fund International. NOURISHING Framework [web page] (http://www.wcrf.org/int/policy/nourishing-framework, accessed 1 February 2017).
133. Improving the food environment through nutrition standards: a guide for government procurement. Atlanta GA: Centers for Disease Control and Prevention, Division for Heart Disease and Stroke; 2010.
134. Programme of the Maltese Presidency of the Council of the European Union (1 January 2017–30 June 2017) (https://www.eu2017.mt/en/Documents/NationalProgramme_EN.pdf, accessed 1 February 2017).
135. Factsheets on health-enhancing physical activity in the 28 European Union Member States of the WHO European Region. Copenhagen: WHO Regional Office for Europe; 2015.
136. Promoting physical activity in the workplace. London: National Institute for Health and Care Excellence; 2008 (Public health guideline [PH13].
137. National Institute for Health and Care Excellence. Physical activity and the environment. NICE public health guideline: 28 January 2008 (https://www.nice.org.uk/guidance/ph8/resources/physical-activity-and-the-environment-55460874949, accessed 1 February 2017).
138. Creating Healthy NHS Workplaces: A toolkit to support the implementation of the NICE workplace guidance. London: NHS Employers; September 2015. (http://www.nhsemployers.org/~/media/Employers/Documents/Retain and improve/Health and wellbeing/Creating healthy workplaces toolkit.pdf, accessed 1 February 2017).
139. A guide for population-based approaches to increasing levels of physical activity: implementation of the WHO Global Strategy on Diet, Physical Activity and Health. Geneva: World Health Organization; 2007.
140. Hourani HM Al, Naffa S, Fardous T. National commitment to action on social determinants of health in Jordan: Addressing obesity. Background paper 18 for the World Conference on Social Determinants of Health. Rio de Janeiro, 19–21 October

41
References
2011 (http://www.who.int/sdhconference/resources/draft_background_paper18_jordan.pdf, accessed 11 February 2017).
141. National Nutrition Strategy - Strategic Study 2014-2050. Muscat: Ministry of Health, Sultanate of Oman; 2014.
142. Sharp fall in palm oil imports. Financial Tribune - First Iranian English Economic Daily, 2 July 2016. (https://financialtribune.com/articles/economy-domestic-economy/44673/sharp-fall-in-palm-oil-imports, accessed 1 February 2017).
143. Zatonski W, Campos H, Willett W. Rapid declines in coronary heart disease mortality in Eastern Europe are associated with increased consumption of oils rich in alpha-linolenic acid. Eur J Epidemiol. 2008;23(1):3–10.
144. HM Government. Childhood Obesity: A Plan for Action, 2016 (https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/546588/Childhood_obesity_2016__2__acc.pdf, accessed 1 Febuary 2017).
145. Global nutrition report 2015: Actions and accountability to advance nutrition and sustainable development. Washington DC: International Food Policy Research Institute; 2015.
146. European Union. EU Pledge [website] (http://www.eu-pledge.eu/, accessed 1 February 2017).
147. Assessing national capacity for the prevention and control of noncommunicable diseases: report of the 2015 global survey. Geneva: World Health Organization; 2016:30.
148. Hungry for Change? Which? healthier choices progress report 2009. London: Which?; 2009 (http://www.which.co.uk/static/html/pdfs/hungry_for_change.pdf, accessed 11 February 2017).
149. International Labour Organization. C183 - Maternity Protection Convention, 2000 (No. 183) [web page] (http://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:55:0::NO::P55_TYPE,P55_LANG,P55_DOCUMENT,P55_NODE:REV,en,C183,/Document, accessed 1 February 2017).
150. World Health Organization. Global database on implementation of nutrition actions (GINA) [web site] (http://www.who.int/nutrition/gina/en/, accessed 1 February 2017).
151. Stratégie de Prévention et de lutte contre l’obésité 2013-2017 Programmation des Actions [Prevention strategy to tackle obesity 2013-2017. Plan of action]. Tunis: Ministry of Health; 2014.
152. Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343–50.
153. 2016 Global food policy report survey. Washington DC, International Food Policy Research Institute (IFPRI); 2016.
154. Persson M, Soroko S, Musicus A, Lobstein T. A junk-free childhood 2012: the 2012 report of the StanMark project on standards for marketing food and beverages to children in Europe. London: International Association for the Study of Obesity, 2012:1–29.

42
Proposed policy priorities for preventing obesity and diabetes
Annex 1. Methodology for identifying priority actions for preventing obesity and diabetes in the RegionThe proposed interventions have been identified through a number of steps outlined below.
Informal regional meeting on developing an action plan for preventing obesity and diabetes in the Eastern Mediterranean Region An informal regional meeting was organized by the Regional Office and held in Geneva in May 2016 to discuss the feasibility of different evidence-based interventions to prevent obesity and diabetes (120). Participants benefited from extensive analysis of the effectiveness and the costs of different interventions, with WHO and many other institutions having undertaken systematic reviews and assembled evidence from many different sectors.
Senior policy officials and experts assessed these interventions in different sectors. These included the scale of change required, costs of implementation, cost–effectiveness of measures, government departments involved, industrial sectors affected, potential implementation problems, robustness of evidence for the measure and the political challenges involved.
A series of recommendations emerged from the meeting.
1. Enforce the legal strategies and policies that regulate the marketing of breast-milk substitutes and unhealthy complementary foods to eliminate the conflict of interest
and control the misconduct related to national food procurements and supplies.
2. Develop/reinforce coherent policies between trade, industry and health to ensure healthy food supply partnership with private sectors to support implementation of WHO’s agenda on diabetes and obesity without conflict of interest.
3. Strengthen regional and national multistakeholder and multisectoral committees to harmonize the monitoring processes and implementation of the WHO strategies.
4. Restrict marketing, advertising and sponsorship across all media (including digital) platforms for all fat/sugar rich foods and drinks to children.
5. Progressively eliminate any subsidies by national governments for certain food items, i.e. sugar, fat.
6. Encourage companies to progressively reformulate sugar-rich drinks to lower sugar content.
7. Conduct vibrant media campaigns and explanations linked to health benefit aiming to change the political acceptance of the need for radical policies.
From these recommendations nine policy areas were identified and recommended for further exploration.
Evidence summary
In response to the recommendations of the Geneva meeting, a review was commissioned to summarize the evidence of the effectiveness, cost–effectiveness and country experience for nine specific policy areas identified (Table A1.).

43
Annex 1
Table A1. Potential priority areas for action requiring a summary of evidence
Priority area Potential interventions on which evidence to be summarized
1. Breastfeeding Protection, promotion and support of breastfeeding and regulatory control of breast-milk substitutes and complementary foods.
2. Regulating marketing a) Restrictions on marketing, advertising and sponsorship across all media (including digital) platforms for all fat/sugar-rich foods and drinks to children.
b) Restrictions on marketing, advertising and sponsorship across all media (including digital) platforms for all fat/sugar-rich foods and drinks to adults.
3. Fiscal measures a) Progressive elimination of any subsidies by national governments for certain food items, i.e. sugar, fat.
b) Tax(es) to raise the price of sweetened soft drinks and beverages. c) Tax(es) on fat(s).
4. Price promotions Action to limit price promotions on foods high in fat, sugar or salt (HFSS) in supermarkets, catering or street markets.
5. Public procurement Action on publicly-funded food – standards for foods in public institutions and improving public procurement.
6. Reformulation a) Progressive reformulation of sugar-rich drinks to lower sugar intakes.b) Progressive reformulation of HFSS foods.
7. Mass media Mass media campaigns to increase political/public acceptance of these initiatives.
8. Labelling Introduction of new standards for nutrition labelling (front-of-pack labelling, colour-coded schemes, menu labelling, warning labels), including:(1) examination of evidence on whether front-of-pack nutrition labels
attract attention more readily than more complete, mandated nutrition information (the Nutrition Facts Panel) and
(2) determination of whether label design characteristics, specifically colour-coding and/or coding with facial icons, increase attention to the front-of-pack label.
9. Trade Development of trade-related policy approaches to create a less obesogenic food environment.
The review generally focused on key systematic reviews (published in English after 2010) and reported pooled results from recent meta-analyses where possible.
Evidence review meeting
A further meeting was held in Cairo in August 2016 to review the findings of the rapid summary of evidence, while also taking account of the particular context of the Eastern Mediterranean Region. With input from external advisors, the meeting considered the potential specific impact in the regional context and questions of feasibility.
A list of priority areas for action and strategic interventions was then identified. This list was further developed, along with a summary of the evidence, case studies of implementation and feasibility considerations into the current report.

44
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Fisc
al m
easu
res
Car
eful
use
of t
axes
an
d su
bsid
ies
to
prom
ote
heal
thie
r di
ets
Exte
nsiv
e ev
iden
ce
that
food
pri
ce p
olic
ies
influ
ence
con
sum
er
purc
hase
s, t
here
by
affe
ctin
g he
alth
(i
nclu
ding
ris
k of
obe
sity
an
d di
abet
es)
139
to 1
696
DA
LYs
save
d pe
r m
illio
n po
pula
tion
af
ter
20 y
ears
in
6 LM
ICs:
Aft
er
50 y
ears
: 355
to
5 89
8 D
ALY
s pe
r m
illio
n14
Aus
tral
ia: 1
70 0
00
DA
LYs
aver
ted
over
life
tim
e of
20
03 p
opul
atio
n13
Cos
t sa
ving
aft
er
20 o
r 50
yea
rs
in 6
LM
ICs
and
cost
effe
ctiv
e in
2
HIC
s13
Ver
y lo
w
impl
emen
tati
on c
osts
(F
rom
US$
0.0
1 to
0.
02 p
er c
apit
a in
6
LMIC
s, r
isin
g to
U
S$ 0
.11
in 1
HIC
as
sess
ed)
Lead
: Pri
me
Min
iste
r’s
Offi
ce/
Min
istr
y of
Fi
nanc
eO
ther
s: T
rade
/In
dust
ry/S
uppl
y In
dust
ry
Prog
ress
ivel
y el
imin
ate
all
natio
nal s
ubsid
ies
for
all
type
s of
fats
/oils
and
sug
ar
Subs
idie
s on
hig
h fa
t or
sug
ar
com
mod
ities
are
pre
vale
nt
thro
ugh
the
Reg
ion
Cle
ar e
vide
nce
that
sel
ectiv
e su
bsid
izat
ion
incr
ease
s co
nsum
ptio
n of
sub
sidize
d co
mm
oditi
esC
ount
ry e
xper
ienc
e sh
ows
that
sub
sidie
s ca
n be
re
mov
ed. S
hifti
ng s
ubsid
ies
to
unsa
tura
ted
fats
, per
se,
is n
ot
effe
ctiv
e fo
r ob
esity
/dia
bete
s pr
even
tion
Lead
: Prim
e M
inist
er’s
Offi
ce/M
inist
ry o
f Fi
nanc
eO
ther
s: Tr
ade/
Indu
stry
/Sup
ply
Indu
stry
13 H
ighl
y co
st-e
ffect
ive
is le
ss th
an p
er c
apita
GD
P pe
r DA
LY sa
ved;
cos
t-ef
fect
ive
is 1-
3 tim
es p
er c
apita
GD
P pe
r DA
LY; m
ore
than
3 ti
mes
per
cap
ita G
DP
is no
t cos
t-ef
fect
ive.
14 A
ll fig
ures
rel
atin
g to
6 L
MIC
s (w
ith E
ngla
nd a
s com
para
tor)
are
from
an
anal
ysis
by O
rgan
isatio
n fo
r Ec
onom
ic C
oope
ratio
n an
d D
evel
opm
ent (
31).
Unl
ess o
ther
wise
cite
d, fi
gure
s for
A
ustr
alia
are
from
the
AC
E Pr
even
tion
Proj
ect (
30) a
nd fi
gure
s for
the
UK
are
from
an
anal
ysis
by M
cKin
sey
Gro
up In
tern
atio
nal (
73).

45
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Impl
emen
t an
effe
ctiv
e ta
x on
sug
ar-s
wee
tene
d be
vera
ges
Con
vinc
ing
evid
ence
from
m
odel
ling
and
coun
try
expe
rienc
e th
at p
urch
ases
are
re
duce
d by
tax
es
Lead
: Prim
e M
inist
er’s
Offi
ce/M
inist
ry o
f Fi
nanc
eO
ther
s: Tr
ade/
Indu
stry
/Sup
ply
Indu
stry
Con
sider
an
effe
ctiv
e pr
ogre
ssiv
e ta
x on
hig
h fa
t fo
ods
and
on h
igh
suga
r fo
ods
Con
sider
able
evi
denc
e fr
om
mod
ellin
g an
d de
mon
stra
ble
impa
ct fr
om e
xper
ienc
e in
in
divi
dual
cou
ntrie
s
UK:
203
000
DA
LYs
over
life
time
of 2
004
pop
for
10%
tax
on
HFS
S fo
ods
Cos
t-ef
fect
ive:
U
S$ 1
800
per
DA
LY
save
d in
UK
for
10%
ta
x on
HFS
S fo
ods
Lead
: Prim
e M
inist
er’s
Offi
ce/M
inist
ry o
f Fi
nanc
eO
ther
s: Tr
ade/
Indu
stry
/Sup
ply
Indu
stry
Publ
ic
proc
urem
ent
Proc
urem
ent
and
prov
isio
n of
hea
lthy
fo
od in
pub
lic
inst
itut
ions
(e.
g.
scho
ols,
hos
pita
ls,
mili
tary
, pri
sons
, ot
her
gove
rnm
ent
inst
itut
ions
)
Food
ser
ved
in p
ublic
in
stit
utio
ns is
a s
izea
ble
cont
ribu
tor
to d
iet
for
man
y gr
oups
in
coun
trie
s ac
ross
the
R
egio
n.
Inte
rnat
iona
l evi
denc
e sh
ows
that
hea
lthy
food
pr
ocur
emen
t po
licie
s ca
n im
prov
e di
ets
and
heal
th o
utco
mes
, pa
rtic
ular
ly a
mon
g st
udie
s do
ne in
sch
ools
No
esti
mat
es
avai
labl
eN
o co
st–
effe
ctiv
enes
s an
alys
es a
vaila
ble
No
gene
ric
esti
mat
es
of im
plem
enta
tion
co
sts.
Inve
stm
ent
will
be
req
uire
d, b
ut s
cale
of
gov
ernm
ent
buyi
ng
can
be h
arne
ssed
to
keep
cos
ts d
own
Lead
: Min
istr
y of
Fin
ance
/Pr
ocur
emen
t/Su
pplie
sO
ther
: All
gove
rnm
ent
depa
rtm
ents

46
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Impl
emen
t m
anda
tory
nu
triti
on s
tand
ards
acr
oss
all p
ublic
inst
itutio
ns,
thro
ugh
(a)
appl
icat
ion
of t
he R
egio
nal n
utrie
nt
profi
le m
odel
to
asse
ss
the
nutr
ition
al q
ualit
y of
diff
eren
t fo
ods
(b)
intr
oduc
tion
of m
eal
stan
dard
s, an
d (c
) m
easu
res
to e
limin
ate
the
sale
of
food
s or
drin
ks h
igh
in fa
t, su
gar
or s
alt
Cou
ntry
exp
erie
nce
show
s th
at n
utrit
ion
stan
dard
s ca
n be
im
plem
ente
d ac
ross
a w
ide
rang
e of
pub
lic in
stitu
tions
to
brin
g nu
triti
onal
impr
ovem
ents
Lead
: Foo
d st
anda
rds
auth
ority
O
ther
: Hea
lth,
Trad
e/In
dust
ry/
Supp
ly, C
ham
ber
of
Com
mer
ce, F
ood
insp
ectio
n au
thor
ities
Issue
man
dato
ry g
uide
lines
fo
r th
e re
visio
n of
pr
ocur
emen
t to
pro
vide
he
alth
y fo
od, in
clud
ing
limiti
ng t
he v
olum
e of
fats
/oi
ls, s
ugar
and
sal
t en
terin
g pu
blic
sec
tor
cate
ring
faci
litie
s in
ord
er t
o fa
cilit
ate
the
nece
ssar
y m
enu
chan
ges
(e.g
. so
that
mea
ls pr
ovid
e no
t m
ore
than
25%
en
ergy
from
fats
and
less
th
an 5
% fr
om fr
ee s
ugar
s)
Lead
: Min
istry
of
Fina
nce/
Proc
urem
ent/
Supp
lies
Oth
er: A
ll go
vern
men
t de
part
men
ts

47
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Dev
elop
gui
danc
e an
d pr
ovid
e tr
aini
ng t
o ca
terin
g co
mpa
nies
on
appr
opria
te
cate
ring
met
hods
in p
ublic
in
stitu
tions
to
redu
ce
the
use
of fr
ying
and
sw
eete
ning
of f
oods
and
he
lp w
ith m
enu
desig
n
Lead
: Min
istry
of
Hea
lth a
nd
mun
icip
aliti
esO
ther
: All
gove
rnm
ent
depa
rtm
ents
Con
tinue
impl
emen
ting
thes
e m
easu
res,
scal
ing
up
cove
rage
and
mon
itorin
g im
pact
Phys
ical
act
ivit
y in
terv
enti
ons
Impl
emen
t po
licie
s,
legi
slat
ion
and
inte
rven
tion
s to
pr
omot
e an
d fa
cilit
ate
heal
th-e
nhan
cing
ph
ysic
al a
ctiv
ity
Prom
otin
g ph
ysic
al a
ctiv
ity
and
heal
thy
diet
is o
ne o
f W
HO
’s “
best
buy
s” fo
r N
CD
pre
vent
ion
No
esti
mat
es
iden
tifie
dT
here
is a
n em
ergi
ng
body
of e
vide
nce
sugg
esti
ng t
hat
phys
ical
act
ivit
y in
terv
enti
ons
may
be
cost
-effe
ctiv
e (1
2),
alth
ough
the
num
ber
of s
tudi
es r
emai
ns
limit
ed (1
21)
WH
O e
stim
ated
tha
t th
e an
nual
cos
t pe
r pe
rson
of p
rom
otin
g pu
blic
aw
aren
ess
abou
t di
et a
nd p
hysi
cal a
ctiv
ity
wou
ld b
e U
S$ 0
.038
(on
th
e ba
sis
of U
S$ 2
008)
(1
22)
Lead
: Pre
side
nt/
Prim
e M
inis
ter’
s O
ffice
wit
h M
inis
try
of H
ealt
hO
ther
: Tre
asur
y/Fi
nanc
e, In
dust
ry,
Educ
atio
n,
Com
mun
icat
ion,
U
rban
Pla
nnin
g,
Hou
sing
, En
viro
nmen
t,
Tran
spor
t an
d Sp
ort

48
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Prom
ote
heal
thy
phys
ical
ac
tivity
thr
ough
mas
s m
edia
cam
paig
ns (
see
actio
n 9
belo
w)
and
ensu
re a
dequ
ate
legi
slatio
n su
ppor
ting
deliv
ery
of d
aily
ph
ysic
al a
ctiv
ity fo
r st
uden
ts
in s
choo
ls an
d un
iver
sitie
s
Mas
s m
edia
cam
paig
ns t
o pr
omot
e ph
ysic
al a
ctiv
ity
and
heal
thy
diet
are
co
nsid
ered
a “
best
buy
” by
W
HO
(12
). Sc
hool
-bas
ed
inte
rven
tions
sho
w c
onsis
tent
im
prov
emen
ts in
kno
wle
dge,
at
titud
es a
nd b
ehav
iour
and
, in
som
e ca
ses,
phys
ical
and
cl
inic
al o
utco
mes
(12
)
Mas
s m
edia
cam
paig
ns
on p
hysic
al a
ctiv
ity
are
estim
ated
to
be
very
cos
t-ef
fect
ive
(122
). Sc
hool
hea
lth
educ
atio
n pr
ogra
mm
es
to p
rom
ote
phys
ical
ac
tivity
hav
e be
en
foun
d to
be
cost
-ef
fect
ive
(121
), w
hile
W
HO
est
imat
ed
prom
otin
g ph
ysic
al
activ
ity in
sch
ools
wou
ld c
ost
>3
times
G
DP
per
pers
on
(cla
ssifi
ed a
s “le
ss c
ost-
effe
ctiv
e”)
(122
).
Prom
otin
g ph
ysic
al a
ctiv
ity
thro
ugh
mas
s m
edia
is
estim
ated
to
have
a v
ery
low
cos
t (<
US$
0.5
0 pe
r ca
pita
), w
hile
pro
mot
ing
phys
ical
act
ivity
in s
choo
ls w
ould
hav
e a
high
er c
ost
(> U
S$ 1
per
cap
ita o
n th
e ba
sis o
f US$
200
8) (
122)
Lead
: Pre
siden
t/Pr
ime
Min
ister
’s O
ffice
with
M
inist
ry o
f Edu
catio
n;
Com
mun
icat
ion
Ensu
re c
ompr
ehen
sive
deliv
ery
of r
egul
ar, q
ualit
y ph
ysic
al e
duca
tion
to
all c
hild
ren,
as
a ke
y co
mpo
nent
of e
duca
tion
in
scho
ols
Enha
nced
phy
sical
edu
catio
n (P
E) in
terv
entio
ns (
incr
ease
d tim
e du
ring
PE c
lass
es w
here
st
uden
ts a
re a
ctiv
e, a
dditi
onal
PE
cla
sses
in t
he s
choo
l tim
etab
le o
f lon
ger
PE c
lass
es)
are
effe
ctiv
e (1
23)
A s
yste
mat
ic r
evie
w
of s
choo
l-bas
ed
inte
rven
tions
(in
clud
ing
PE)
have
bee
n fo
und
to
be v
ery
cost
-effe
ctiv
e,
at a
cos
t ra
ngin
g fr
om
US$
0.0
6 to
0.7
9 pe
r M
ET-h
our
(a w
ay o
f es
timat
ing
phys
ical
ac
tivity
) ga
ined
per
pe
rson
per
day
(12
1)
Lead
: Min
istry
of
Educ
atio
n

49
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Dev
elop
a s
et o
f sta
ndar
ds/
guid
elin
es p
rom
otin
g ph
ysic
al a
ctiv
ity in
the
w
orkp
lace
, incl
udin
g fa
cilit
y/bu
ildin
g de
sign,
ava
ilabi
lity
of s
port
s fa
cilit
ies
and
prog
ram
mes
ena
blin
g ac
cess
to
faci
litie
s aw
ay
from
the
wor
kpla
ce
Evid
ence
tha
t m
ulti-
com
pone
nt p
rogr
amm
es t
o pr
omot
e ph
ysic
al a
ctiv
ity in
th
e w
orkp
lace
are
effe
ctiv
e in
impr
ovin
g he
alth
-rel
ated
ou
tcom
es (
12,1
24)
Prom
otin
g ph
ysic
al
activ
ity in
wor
ksite
s is
estim
ated
to
be q
uite
co
st e
ffect
ive
(<3
times
GD
P pe
r ca
pita
pe
r D
ALY
pre
vent
ed)
(122
)
Prom
otin
g ph
ysic
al a
ctiv
ity
in w
orks
ites
is es
timat
ed
to c
ost
>U
S$ 1
per
cap
ita
(on
the
basis
of U
S$ 2
008)
(1
22)
Lead
: Pre
siden
t/Pr
ime
Min
ister
’s O
ffice
with
M
inist
ry o
f Hea
lth;
Min
istry
of I
ndus
try
Incr
ease
ava
ilabi
lity
of a
nd
acce
ssib
ility
for
part
icip
atio
n in
form
al a
nd in
form
al
recr
eatio
nal a
nd s
port
ing
activ
ities
, par
ticul
arly
pr
ovid
ing
oppo
rtun
ities
fo
r pa
rtic
ipat
ion
in
prog
ram
mes
suc
h as
“S
port
s-fo
r-All”
, with
em
phas
is on
ens
urin
g eq
ualit
y of
acc
ess
and
oppo
rtun
ity fo
r pa
rtic
ipat
ion
Evid
ence
tha
t cr
eatin
g or
en
hanc
ing
acce
ss t
o pl
aces
for
phys
ical
act
ivity
is e
ffect
ive
in
raisi
ng t
he p
ropo
rtio
n of
the
po
pula
tion
who
are
phy
sical
ly
activ
e (1
23)
The
rel
ativ
e co
st a
nd c
ost-
effe
ctiv
enes
s w
ill de
pend
on
the
pre
cise
mea
sure
s, bu
t a
US
stud
y fo
und
that
“e
nhan
ced
acce
ss t
o ph
ysic
al a
ctiv
ity in
form
atio
n an
d op
port
uniti
es”
to b
e co
st-e
ffect
ive
and
to o
ffer
good
va
lue
for
mon
ey (
125)
Lead
: Min
istry
of
Spor
t w
ith M
inist
ry o
f H
ealth
Oth
er: T
reas
ury/
Min
istry
of F
inan
ce

50
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Dev
elop
and
impl
emen
t an
urb
an p
lann
ing
polic
y to
ens
ure
that
urb
an
envi
ronm
ents
enc
oura
ge
peop
le t
o re
ly le
ss o
n pe
rson
al m
otor
ized
vehi
cles
an
d su
ppor
t ac
cess
to
safe
, ge
nder
-sen
sitiv
e an
d ag
e-fr
iend
ly p
ublic
tra
nspo
rt,
cycl
ing
and
wal
king
, in
clud
ing
by p
rovi
sion
of
faci
litie
s, eq
uipm
ent,
publ
ic
open
and
gre
en s
pace
an
d sh
ared
use
of s
choo
l fa
cilit
ies
(bot
h in
door
and
ou
tdoo
r)
City
pla
nnin
g ap
proa
ches
tha
t su
ppor
t w
alki
ng, c
yclin
g an
d pu
blic
tra
nspo
rt w
ith a
saf
e in
fras
truc
ture
and
prio
ritize
th
em o
ver
priv
ate
mot
orize
d tr
ansp
ort
are
mos
t ef
fect
ive
(51)
. Sm
all-s
cale
urb
an d
esig
n po
licie
s (in
clud
ing
impr
ovin
g st
reet
ligh
ting,
mak
ing
cros
sings
sa
fer,
traf
fic c
alm
ing,
impr
ovin
g th
e ap
pear
ance
of s
tree
ts
and
prov
idin
g co
ntin
uous
pe
dest
rian
pave
men
ts)
are
effe
ctiv
e in
faci
litat
ing
wal
king
(1
23).
Polic
ies
to c
hang
e th
e bu
ilt e
nviro
nmen
t ha
ve b
een
estim
ated
to
be t
he m
ost
cost
-effe
ctiv
e st
rate
gy fo
r in
crea
sing
phys
ical
act
ivity
am
ong
larg
e po
pula
tions
be
caus
e, a
lthou
gh t
hey
ofte
n re
quire
sub
stan
tial
inve
stm
ent,
thei
r be
nefit
s ar
e lo
ng-la
stin
g (1
21).
Cre
atio
n of
new
cyc
le o
r pe
dest
rian
trai
ls re
quire
s bu
dget
inve
stm
ent
but
prov
ides
goo
d va
lue
per
hour
of
phy
sical
act
ivity
gai
ned
(US$
0.2
43 p
er M
et-h
our
gain
ed)
(121
)
Lead
: Urb
an P
lann
ing,
H
ousin
g, En
viro
nmen
t, Tr
ansp
ort
and
Spor
t
Con
tinue
impl
emen
ting
thes
e m
easu
res,
scal
ing
up
cove
rage
and
mon
itorin
g im
pact
Food
sup
ply
and
trad
eU
se fo
od s
tand
ards
, leg
al
inst
rum
ents
and
oth
er
appr
oach
es t
o im
prov
e th
e na
tion
al a
nd/o
r lo
cal f
ood
supp
ly in
thi
s R
egio
n of
net
food
-im
port
ing
coun
trie
s
Evid
ence
from
sev
eral
co
untr
ies
show
s th
at
trad
e po
licy
tool
s an
d/or
st
anda
rds
can
be e
ffect
ive
in r
educ
ing
the
avai
labi
lity
or in
crea
sing
the
pri
ce o
f fa
ts a
nd s
ugar
s in
the
food
su
pply
No
esti
mat
es o
f im
pact
iden
tifie
dN
o co
st–e
ffect
ive
anal
yses
iden
tifin
ess
No
cost
est
imat
es
iden
tifie
dLe
ad: F
ood
stan
dard
s au
thor
ity
Oth
er: F
orei
gn
Affa
irs,
Hea
lth,
C
usto
ms,
Fin
ance
, Tr
ade/
Indu
stry
/Su
pply

51
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Faci
litat
e th
e de
velo
pmen
t of
loca
l foo
d po
licie
s an
d en
cour
age
city
aut
horit
ies
to s
ign
the
Mila
n U
rban
Fo
od P
olic
y Pa
ct a
nd
impl
emen
t its
Fra
mew
ork
for A
ctio
n to
dev
elop
, w
here
pos
sible
, sus
tain
able
ur
ban
food
sys
tem
s
Con
sider
intr
oduc
ing
stan
dard
s or
oth
er
lega
l ins
trum
ents
(e.
g.
com
posit
iona
l sta
ndar
ds,
tarif
fs, im
port
res
tric
tions
, sa
les
bans
, pla
nnin
g la
ws,
zoni
ng p
olic
ies)
to
redu
ce
the
volu
me
and
impr
ove
the
qual
ity o
f fat
s/oi
ls an
d re
duce
sug
ars
in t
he
natio
nal a
nd lo
cal f
ood
supp
ly
Con
sider
rem
ovin
g ag
ricul
tura
l sub
sidie
s fo
r pr
oduc
ers
of s
ugar
s an
d oi
ls (e
spec
ially
tho
se o
ils
high
in s
atur
ated
fatt
y ac
ids)
, rep
laci
ng t
hem
, w
here
nec
essa
ry, w
ith o
ther
m
echa
nism
s to
sup
port
fa
rmer
s an
d gr
ower
s

52
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Ref
orm
ulat
ion
Impl
emen
t a
gove
rnm
ent-
led
prog
ram
me
of
prog
ress
ive
refo
rmul
atio
n,
adap
ted
to t
he n
atio
nal
cont
ext,
to e
limin
ate
tran
s fa
ts a
nd r
educ
e pr
ogre
ssiv
ely
tota
l and
sa
tura
ted
fat,
salt,
sug
ars,
ener
gy a
nd p
ortio
n siz
e
The
re is
str
ong
and
exte
nsiv
e ev
iden
ce fr
om e
xper
ienc
e w
ith s
alt
redu
ctio
n th
at
prog
ress
ive
refo
rmul
atio
n ca
n re
duce
leve
ls of
spe
cific
in
gred
ient
s in
food
s an
d re
duce
pop
ulat
ion
inta
kes
of
thos
e in
gred
ient
s/nu
trie
nts
The
re is
evi
denc
e th
at
volu
ntar
y ef
fort
s ar
e le
ss
effe
ctiv
e th
an m
anda
tory
ap
proa
ches
. Evi
denc
e ha
s id
entifi
ed t
he k
ey c
ompo
nent
s of
suc
cess
ful r
efor
mul
atio
n pr
ogra
mm
es:
• Pr
ogre
ssiv
e re
duct
ions
•
Gov
ernm
ent-
set
targ
et
leve
ls ha
ve t
o be
set
by
food
ca
tego
ry
• M
ultin
utrie
nt r
educ
tions
(t
otal
fat,
suga
r, sa
lt)
• A
ccom
pani
ed b
y fr
ont-
of-
pack
labe
lling
and
cons
umer
aw
aren
ess
• G
over
nmen
t-le
d an
d co
mpr
ehen
sive
stak
ehol
der
enga
gem
ent
• C
omm
itmen
t to
mon
itorin
g an
d ev
alua
tion
UK
estim
ate:
1.7
m
illion
DA
LYs
over
lif
etim
e of
200
4 po
pula
tion
for
incr
emen
tal r
educ
tion
of e
nerg
y in
pac
kage
d fo
od, d
rink
and
rest
aura
nt fo
ods
Hig
hly
cost
effe
ctiv
e (U
K es
timat
e U
S$ 2
60
0 pe
r D
ALY
sav
ed)
Lead
: Min
istry
of
Trad
e/In
dust
ry/
Supp
ly, fo
od s
tand
ards
au
thor
ity a
nd M
inist
ry
of H
ealth

53
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Coo
pera
te w
ith o
ther
M
embe
r St
ates
to
adop
t a
regi
onal
app
roac
h fo
r en
gagi
ng w
ith fo
od
prod
ucer
s to
driv
e fo
od
refo
rmul
atio
n to
elim
inat
e tr
ans
fats
and
red
uce
prog
ress
ivel
y to
tal a
nd
satu
rate
d fa
t, sa
lt, s
ugar
s, en
ergy
and
por
tion
size
in
a su
bsta
ntia
l pro
port
ion
of
proc
esse
d fo
ods
Lead
: Min
istry
of
Trad
e/In
dust
ry/
Supp
ly, fo
od s
tand
ards
au
thor
ity a
nd M
inist
ry
of H
ealth
Enga
ge w
ith p
rivat
e se
ctor
pro
vide
rs o
f foo
d in
cat
erin
g/fo
od s
ervi
ce
outle
ts (
incl
udin
g ta
keaw
ays
and
stre
et fo
od t
rade
rs)
to e
stab
lish
a pr
ogra
mm
e to
elim
inat
e tr
ans
fats
and
re
duce
pro
gres
sivel
y to
tal
and
satu
rate
d fa
t, sa
lt,
suga
rs, e
nerg
y an
d po
rtio
n siz
e, w
ith d
efine
d qu
antifi
ed
redu
ctio
ns in
use
of t
hese
in
gred
ient
s
Lead
: Min
istry
of
Trad
e/In
dust
ry/S
uppl
y, M
inist
ry o
f Hea
lth a
nd
mun
icip
aliti
es (
food
in
spec
tors
)

54
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Mar
keti
ngIm
plem
ent
appr
opri
ate
rest
rict
ions
on
mar
keti
ng (
incl
udin
g pr
ice
prom
otio
ns)
of
food
s hi
gh in
fat,
sug
ar
and
salt
Con
vinc
ing
rese
arch
th
at e
xpos
ure
to
mar
keti
ng fo
r H
FSS
food
s in
fluen
ces
child
ren’
s di
ets.
Cou
ntry
ex
peri
ence
sho
ws
that
re
stri
ctio
ns c
an r
educ
e ch
ildre
n’s
expo
sure
to
suc
h m
arke
ting
. R
esea
rch
on c
ount
ry
impl
emen
tati
ons
show
s th
at m
anda
tory
re
stri
ctio
ns a
re m
ost
effe
ctiv
e R
etai
l pri
ce p
rom
otio
ns
on H
FSS
food
s ar
e in
crea
sing
ly c
omm
on
thro
ugho
ut t
he R
egio
n,
and
evid
ence
from
H
ICs
show
s th
at p
rice
pr
omot
ions
sel
ecti
vely
pr
omot
e H
FSS
food
s an
d ca
n in
crea
ses
suga
r in
take
See
belo
w fo
r es
tim
ates
for
som
e sp
ecifi
c in
terv
enti
ons
Cos
t-sa
ving
, hig
hly
cost
-effe
ctiv
e or
co
st-e
ffect
ive
(see
be
low
for
spec
ific
esti
mat
es)
Ver
y lo
w c
ost
impl
emen
tati
on (
see
belo
w)
Lead
: Tra
de/
Indu
stry
/Sup
ply/
Adv
erti
sing
re
gula
tory
bod
ies
and
mun
icip
alit
ies
Oth
er: H
ealt
h

55
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Wor
k w
ith o
ther
cou
ntrie
s in
the
Reg
ion
to e
stab
lish
a co
ordi
nate
d ap
proa
ch,
incl
udin
g ap
prop
riate
le
gal a
dvic
e, t
o re
duce
the
im
pact
of c
ross
-bor
der
mar
ketin
g
Cro
ss-b
orde
r br
oadc
ast
mar
ketin
g do
min
ates
Reg
iona
l m
edia
out
lets
. Adv
ertis
ing
expe
nditu
re a
naly
ses
show
th
at p
an-A
rab
med
ia
mar
ketin
g of
HFS
S fo
ods
is ex
tens
ive
and
esca
latin
g ra
pidl
y
Impl
emen
t th
e W
HO
Set
of
Rec
omm
enda
tions
on
Mar
ketin
g of
Foo
ds a
nd
Non
-alc
ohol
ic B
ever
ages
to
Chi
ldre
n an
d co
nsid
er
man
dato
ry r
estr
ictio
ns
to e
limin
ate
all f
orm
s of
m
arke
ting
of fo
ods
high
in
fat,
suga
r an
d sa
lt to
ch
ildre
n an
d ad
oles
cent
s (u
p to
age
18)
acr
oss
all m
edia
, acc
ordi
ng t
o th
e re
gion
al A
ctio
n Pl
an
to A
ddre
ss U
nopp
osed
M
arke
ting
of U
nhea
lthy
Food
and
Bev
erag
es
Cou
ntry
exp
erie
nce
show
s th
at r
estr
ictin
g ad
vert
ising
on
ly fo
r pa
rtic
ular
med
ia (
e.g.
te
levi
sion
and
radi
o) d
o no
t re
duce
ove
rall
expo
sure
to
mar
ketin
g. T
here
is e
vide
nce
that
chi
ldre
n ar
e in
crea
singl
y ex
pose
d to
HFS
S m
arke
ting
thro
ugh
digi
tal a
nd s
ocia
l m
edia
Ex
tens
ive
coun
try
expe
rienc
e sh
ows
that
lim
ited
defin
ition
s of
tar
get
audi
ence
s (e
.g. t
he
hour
s of
chi
ldre
n’s
tele
visio
n)
are
inef
fect
ive
38 t
o 28
8 D
ALY
s sa
ved
per
milli
on
popu
latio
n af
ter
20
year
s in
6 L
MIC
s; 65
8 to
5 8
23 D
ALY
s pe
r m
illion
afte
r 50
yea
rs
Cos
t sa
ving
, hig
hly
cost
-effe
ctiv
e or
cos
t-ef
fect
ive
in 6
LM
ICs
afte
r 20
and
50
year
s
Very
low
cos
t [U
S$ 0
.04
to
0.13
per
hea
d in
6 L
MIC
s fo
r ob
esity
pre
vent
ion.
In
1 h
igh
inco
me
coun
try
(Eng
land
) =
US$
0.3
0/he
ad]
Use
the
reg
iona
l nut
rient
pr
ofile
mod
el, w
hich
ca
tego
rizes
the
app
ropr
iate
le
vel o
f nut
rient
s in
food
s, to
iden
tify
food
s to
whi
ch
the
mar
ketin
g re
stric
tions
sh
ould
app
ly
Cou
ntry
exp
erie
nce
show
s th
at g
over
nmen
t-le
d nu
trie
nt
profi
les
are
mor
e ef
fect
ive
in
rest
rictin
g m
arke
ting
of H
FSS
food
s
Lead
: Min
istry
of H
ealth
w
ith a
dver
tisin
g re
gula
tory
bod
ies

56
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Con
duct
an
asse
ssm
ent
(pre
fera
bly
as p
art
of a
re
gion
al c
olla
bora
tion)
of
the
impa
ct o
f mar
ketin
g of
fo
ods
high
in fa
t, su
gar
or
salt
to a
dults
to
illum
inat
e th
e m
agni
tude
of m
arke
ting
and
defin
e ho
w b
est
to
rest
rict
inap
prop
riate
pr
actic
es.
Ove
r 50
% o
f the
Reg
ion’
s po
pula
tion
are
child
ren
or
adol
esce
nts.
No
coun
try
has
com
plet
ely
elim
inat
ed c
hild
ren’
s ex
posu
re
to m
arke
ting
of H
FSS
food
s by
impl
emen
ting
rest
rictio
ns
on m
arke
ting
to c
hild
ren,
sin
ce c
hild
ren
and
adol
esce
nts
rem
ain
expo
sed
to m
arke
ting
targ
eted
at
adul
ts
UK
estim
ate:
401
00
0 D
ALY
s ov
er
lifet
ime
of 2
004
popu
latio
n fr
om
rest
rictin
g hi
gh-c
alor
ie
food
adv
ertis
ing
to
redu
ce e
xpos
ure
to
mar
ketin
g
Hig
hly
cost
-effe
ctiv
eU
K es
timat
e: R
estr
ictin
g hi
gh-c
alor
ie fo
od
adve
rtisi
ng t
o re
duce
ex
posu
re t
o m
arke
ting
wou
ld c
ost
US$
50
per
DA
LY s
aved
.
Con
sider
ext
endi
ng
man
dato
ry r
estr
ictio
ns o
n m
arke
ting
of u
nhea
lthy
food
s to
who
le p
opul
atio
n
Legi
slate
to
allo
w r
etai
l pr
omot
ions
onl
y of
hea
lthy
food
s
Ret
ail p
rice
prom
otio
ns o
n H
FSS
food
s ar
e in
crea
singl
y co
mm
on t
hrou
ghou
t th
e R
egio
n.A
naly
ses
from
hig
h-in
com
e co
untr
ies
show
tha
t pr
ice
prom
otio
ns s
elec
tivel
y pr
omot
e H
FSS
food
s an
d af
fect
a h
igh
prop
ortio
n of
all
food
pur
chas
es, w
ith
iden
tified
incr
ease
s in
sug
ar
cons
umpt
ion
cons
isten
t w
ith
prom
otio
n of
obe
sity
and
diab
etes
UK
estim
ate:
561
000
D
ALY
s ov
er li
fetim
e of
200
4 po
pula
tion
from
reg
ulat
ing
pric
e pr
omot
ions
on
high
-ca
lorie
food
s
Hig
hly
cost
-effe
ctiv
eU
K es
timat
e: U
S$ 2
00
per
DA
LY s
aved
fr
om r
egul
atin
g pr
ice
prom
otio
ns o
n hi
gh-
calo
rie fo
ods
Lead
: Tra
de/
Indu
stry
/Sup
ply
and
mun
icip
aliti
esO
ther
: Hea
lth

57
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Labe
lling
Impl
emen
t or
rev
ise
stan
dard
s fo
r nu
trit
ion
labe
lling
to
incl
ude
fron
t-of
-pac
k la
belli
ng
for
all p
re-p
acka
ged
food
s
Evid
ence
tha
t co
nsum
ers
like
sim
ple,
inte
rpre
tive
, fr
ont-
of-p
ack
labe
ls
and
that
thi
s ca
n he
lp
them
to
mak
e he
alth
ier
choi
ces.
358
to 1
176
DA
LYs
per
mill
ion
popu
lati
on fo
r co
mpu
lsor
y fo
od
labe
lling
aft
er 2
0 ye
ars
in 6
LM
ICs;
A
fter
50
year
s:
1089
to
4099
D
ALY
s pe
r m
illio
n po
pula
tion
. U
K: 5
75 0
00
DA
LYs
over
lif
etim
e of
200
4 po
pula
tion
for
labe
lling
on
all
pack
aged
food
s,
men
us a
nd s
helf-
choi
ces
in fa
st
food
res
taur
ants
an
d w
ork
plac
e;A
ustr
alia
: 32
000
DA
LYs
over
lif
etim
e of
200
3 po
pula
tion
for
fron
t-of
-pac
k la
belli
ng
Hig
hly
cost
-ef
fect
ive
or
cost
-effe
ctiv
e af
ter
20 y
ears
in 6
LM
ICs;
Cos
t sa
ving
or
hig
hly
cost
-ef
fect
ive
afte
r 50
ye
ars.
Cos
t sa
ving
or
hig
hly
cost
-ef
fect
ive
in H
ICs
(UK
, Aus
tral
ia)
Ver
y lo
w: U
S$ 0
.05
to 0
.23
(200
5) in
6
LMIC
s; V
ery
low
(<
AS$
0.5
0 pe
r ca
pita
) in
Aus
tral
ia
Lead
: Foo
d st
anda
rds
auth
orit
y an
d M
inis
try
of H
ealt
hO
ther
: Tra
de/
Indu
stry
/Sup
ply,
C
usto
ms

58
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Impl
emen
t m
anda
tory
fr
ont-
of-p
ack
nutr
ition
la
bellin
g sc
hem
e w
ith
elem
ents
to
enab
le
cons
umer
s to
inte
rpre
t ea
sily
(e.g
. mul
tiple
col
our-
code
d tr
affic
ligh
ts, u
se o
f te
rms “
high
”, “m
ediu
m”,
“l
ow”)
Evid
ence
from
sev
eral
co
untr
ies
sugg
ests
tha
t in
terp
retiv
e fr
ont-
of-p
ack
labe
lling
can
driv
e fo
od
man
ufac
ture
rs t
o re
form
ulat
e th
eir
prod
ucts
to
mak
e th
em
heal
thie
r
Enfo
rce
the
labe
lling
sche
me
and
mon
itor
its
impa
ct w
ith t
he p
oten
tial t
o st
reng
then
the
labe
lling
with
su
itabl
e he
alth
war
ning
s

59
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Bre
astf
eedi
ngIm
plem
ent
a pa
ckag
e of
pol
icie
s an
d in
terv
enti
ons
to
prom
ote,
pro
tect
and
su
ppor
t br
east
feed
ing
Subs
tant
ial e
vide
nce
that
br
east
feed
ing
prot
ects
ag
ains
t ov
erw
eigh
t an
d ob
esit
y in
chi
ldre
n an
d ad
ults
and
som
e st
atis
tica
lly s
igni
fican
t ev
iden
ce o
f pro
tect
ion
for
both
mot
hers
and
ch
ildre
n ag
ains
t la
ter
diab
etes
.H
ighl
y si
gnifi
cant
ev
iden
ce o
f sub
stan
tial
im
pact
of i
nter
vent
ions
on
exc
lusi
ve
brea
stfe
edin
g ra
tes
823
000
deat
hs
per
year
ave
rted
in
75
high
-m
orta
lity
LMIC
s if
scal
ed u
p to
nea
r un
iver
sal l
evel
s;
plus
22
216
lives
pe
r ye
ar s
aved
by
incr
easi
ng
brea
stfe
edin
g du
rati
on t
o 12
m
onth
s in
HIC
s an
d 2
year
s pe
r ch
ild in
LM
ICs.
In
addi
tion
, 20
000
annu
al d
eath
s in
w
omen
(br
east
ca
ncer
) w
ould
be
avoi
ded
No
spec
ific
cost
-ef
fect
ive
anal
yses
of
pro
mot
ing
brea
stfe
edin
g fo
r pr
even
tion
of
obe
sity
an
d di
abet
es.
Con
side
rabl
e lit
erat
ure
exis
ts
on s
izea
ble
econ
omic
ben
efits
of
incr
easi
ng
brea
stfe
edin
g
Cos
t es
tim
ates
fo
r sc
alin
g up
in
terv
enti
ons
to p
rom
ote
brea
stfe
edin
g va
ry
imm
ense
ly. O
ne
glob
al e
stim
ate
for
a pa
ckag
e of
mea
sure
s is
US$
130
per
live
bi
rth
(126
)
Lead
: Min
istr
y of
H
ealt
h
Prom
ote
brea
stfe
edin
g th
roug
h m
anda
tory
bab
y-fr
iend
ly h
ealth
sys
tem
s an
d ef
fect
ive
com
mun
ity-b
ased
st
rate
gies
Con
vinc
ing
evid
ence
of
posit
ive
impa
ct o
n ex
clus
ive
brea
stfe
edin
g
Estim
ated
cos
ts o
f US$
28
per
live
birt
h fo
r ba
by-
frie
ndly
hos
pita
l ini
tiativ
e im
plem
enta
tion,
tra
inin
g he
alth
wor
kers
and
co
mm
unity
sup
port
(12
6)
Lead
: Min
istry
of
Hea
lth

60
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Fully
impl
emen
t th
e In
tern
atio
nal C
ode
of
Mar
ketin
g of
Bre
ast-
milk
Su
bstit
utes
and
WH
O
Gui
danc
e on
end
ing
inap
prop
riate
pro
mot
ion
of
food
s fo
r in
fant
s an
d yo
ung
child
ren
Exte
nsiv
e ev
iden
ce t
hat
mar
ketin
g of
bre
ast-
milk
su
bstit
utes
and
inap
prop
riate
pr
omot
ion
of fo
ods
for
infa
nts
and
youn
g ch
ildre
n un
derm
ines
opt
imal
infa
nt
and
youn
g ch
ild fe
edin
g, w
ith
pote
ntia
l neg
ativ
e im
pact
on
brea
stfe
edin
g, ob
esity
and
N
CD
s. C
ount
ry e
xper
ienc
e sh
ows
that
nat
iona
l leg
islat
ion
to r
egul
ate
such
mar
ketin
g ca
n be
effe
ctiv
e in
red
ucin
g m
arke
ting
influ
ence
.
Cos
ts o
f im
plem
entin
g th
e In
tern
atio
nal C
ode
estim
ated
at
US$
3.6
0 pe
r liv
e bi
rth
as a
one
-off
cost
an
d U
S$ 0
.70
per
live
birt
h an
nual
ly fo
r tr
aini
ng a
nd
mon
itorin
g (1
26)
Lead
: Min
istry
of
Trad
e/In
dust
ry w
ith
Min
istry
of H
ealth
an
d fo
od s
tand
ards
au
thor
ity
Empo
wer
wom
en t
o ex
clus
ivel
y br
east
feed
, by
ena
ctin
g pr
ogre
ssiv
ely
incr
easin
g re
mun
erat
ed
time
off w
ork
up t
o a
goal
of
6 m
onth
s’ m
anda
tory
pa
id m
ater
nity
leav
e, a
s w
ell
as p
olic
ies
that
enc
oura
ge
wom
en t
o br
east
feed
in
the
wor
kpla
ce in
clud
ing
brea
stfe
edin
g br
eaks
an
d pr
ovisi
on o
f sui
tabl
e fa
cilit
ies
Mod
est
evid
ence
of a
po
sitiv
e im
pact
on
excl
usiv
e br
east
feed
ing.
Posit
ive
coun
try
expe
rienc
e of
gua
rant
eein
g pa
id d
aily
bre
astfe
edin
g br
eaks
on
bre
astfe
edin
g ou
tcom
es
Estim
ated
gov
ernm
ent
cost
of
US$
94
per
live
birt
h pe
r ye
ar t
o en
act
mat
erni
ty
entit
lem
ents
for
6 m
onth
s (1
26).
Lead
: Min
istry
of
Labo
ur/W
ork
and
Pens
ions

61
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Mas
s m
edia
ca
mpa
igns
Con
duct
mas
s m
edia
ca
mpa
igns
on
heal
thy
diet
and
phy
sica
l ac
tivi
ty
Long
-ter
m, i
nten
sive
m
ass
med
ia c
ampa
igns
ha
ve b
een
show
n to
be
effe
ctiv
e fo
r pr
omot
ing
phys
ical
act
ivit
y an
d m
oder
atel
y ef
fect
ive
for
prom
otin
g he
alth
y di
et.
Inte
nsiv
e ca
mpa
igns
pr
omot
ing
one
sim
ple
mes
sage
are
als
o m
oder
atel
y ef
fect
ive.
246
to 1
361
DA
LYs
per
mill
ion
popu
lati
on in
6
LMIC
s;U
K: C
ould
sav
e 49
000
DA
LYs
over
life
tim
e of
20
04 p
opul
atio
n
Hig
hly
depe
nden
t on
con
text
: wou
ld
not
be c
ost-
effe
ctiv
e, c
ost-
effe
ctiv
e or
hig
hly
cost
-effe
ctiv
e in
6
LMIC
s af
ter
20 y
ears
; aft
er
50 y
ears
hig
hly
cost
effe
ctiv
e or
co
st-e
ffect
ive
in
4 co
untr
ies,
not
co
st-e
ffect
ive
in 2
co
untr
ies.
Mor
e lik
ely
to
be h
ighl
y co
st-
effe
ctiv
e In
HIC
s (U
K: U
S$ 2
00 p
er
DA
LY s
aved
)
Qui
te lo
w in
LM
ICs
(gen
eric
est
imat
e fo
r LM
ICs
cost
s U
S$ 0
.038
per
per
son
per
year
(122
); Es
tim
ates
in t
he 6
LM
ICs
rang
e fr
om
US$
0.2
7 to
0.8
0 pe
r he
adH
ighe
r co
sts
in a
hi
gh-in
com
e co
untr
y (E
ngla
nd =
US$
2.3
2 pe
r he
ad)
(34)
Lead
: Min
istr
y of
Info
rmat
ion,
M
inis
try
of
Hea
lth,
Min
istr
y of
Spo
rt a
nd
Min
istr
y of
Ed
ucat
ion
Impl
emen
t ap
prop
riate
so
cial
mar
ketin
g ca
mpa
igns
, le
d by
the
pub
lic s
ecto
r, on
he
alth
y di
et a
nd p
hysic
al
activ
ity in
ord
er t
o bu
ild
cons
ensu
s, co
mpl
emen
t th
e ot
her
inte
rven
tions
in
the
pack
age
and
enco
urag
e be
havi
our
chan
ge

62
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Ensu
re s
usta
ined
im
plem
enta
tion
of
cam
paig
ns a
nd m
onito
r th
eir
impa
ct
Evid
ence
sho
ws
that
it is
ch
alle
ngin
g to
sus
tain
effe
cts
afte
r ca
mpa
igns
fini
sh, in
the
fa
ce o
f com
petin
g fa
ctor
s, su
ch
as p
erva
sive
food
mar
ketin
g ac
ross
man
y fo
rms
of m
edia
Hea
lth
sect
or
inte
rven
tion
sH
arne
ss t
he h
ealt
h se
ctor
to
enab
le
chan
ge a
nd t
o pr
ovid
e le
ader
ship
on
gov
erna
nce
and
acco
unta
bilit
y
Evid
ence
tha
t he
alth
se
ctor
inte
rven
tion
s ca
n be
effe
ctiv
e, p
arti
cula
rly
nutr
itio
n co
unse
lling
du
ring
pre
gnan
cy a
nd
prim
ary-
care
bas
ed
coun
selli
ng fo
r at
ris
k gr
oups
(se
e be
low
)
No
over
all
esti
mat
es
iden
tifie
d, s
ee
belo
w fo
r so
me
spec
ific
esti
mat
es
No
over
all
esti
mat
es
avai
labl
e. S
ome
esti
mat
ed t
hat
diet
ary
advi
ce t
o pr
egna
nt w
omen
an
d pr
imar
y-ca
re
base
d co
unse
lling
fo
r at
-ris
k gr
oups
w
ould
be
cost
ef
fect
ive
No
over
all e
stim
ates
id
enti
fied,
see
bel
ow
for
som
e sp
ecifi
c es
tim
ates
Lead
: Pre
side
nt/
Prim
e M
inis
ter’
s O
ffice
wit
h M
inis
try
of H
ealt
hO
ther
: Tre
asur
y/Fi
nanc
e, T
rade
, Fo
reig
n A
ffair
s,
Indu
stry
, Ene
rgy,
So
cial
Wel
fare
, Ju
stic
e/Se
curi
ty,
Agr
icul
ture
, Fo
od, E
duca
tion
, C
omm
unic
atio
n,
Urb
an P
lann
ing,
H
ousi
ng,
Envi
ronm
ent,
Tr
ansp
ort
and
Spor
t

63
Annex 2
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Ensu
re p
rovi
sion
of d
ieta
ry
coun
sellin
g on
nut
ritio
n,
phys
ical
act
ivity
and
hea
lthy
wei
ght
gain
bef
ore
and
durin
g pr
egna
ncy
for
pros
pect
ive
mot
hers
and
fa
ther
s
Inte
rven
tions
on
diet
and
/or
exe
rcise
red
uce
the
risk
of
exce
ssiv
e w
eigh
t ga
in d
urin
g pr
egna
ncy
by a
roun
d 20
%
(118
) an
d W
HO
rec
omm
ends
co
unse
lling
abou
t he
alth
y ea
ting
and
keep
ing
phys
ical
ly
activ
e du
ring
preg
nanc
y (1
19). T
he C
omm
issio
n on
End
ing
Chi
ldho
od
Obe
sity
reco
mm
ende
d th
at
prec
once
ptio
n co
unse
lling
also
be
pro
vide
d to
pro
spec
tive
pare
nts
(6)
Econ
omic
ass
essm
ent
of a
n ra
ndom
ized
cont
rolle
d tr
ial i
n N
ew
Zea
land
foun
d it
high
ly
prob
able
tha
t an
tena
tal
diet
ary
advi
ce t
o ov
erw
eigh
t or
obe
se
wom
en w
ould
be
cost
-ef
fect
ive
(127
)
Lead
: Min
istry
of
Hea
lth
Inte
grat
e sc
reen
ing
for
over
wei
ght
and
othe
r di
abet
es r
isk fa
ctor
s in
to
prim
ary
heal
th c
are
and
prov
ide
prim
ary-
care
bas
ed
coun
sellin
g fo
r hi
gh r
isk
indi
vidu
als
Phys
icia
n co
unse
lling
for
at-r
isk
grou
ps is
one
of t
he m
ost
effe
ctiv
e in
terv
entio
ns (
116)
an
d is
one
of W
HO
’s “b
est
buys
” fo
r pr
even
ting
diab
etes
Phys
icia
n co
unse
lling
for
at r
isk g
roup
s is
estim
ated
to
save
up
to 6
988
DA
LYs
per
milli
on p
opul
atio
n af
ter
20 y
ears
, risi
ng
to 1
6 64
4 af
ter
50
year
s (3
4)
Cos
t-ef
fect
iven
ess
of
this
inte
rven
tion
is de
pend
ent
on m
ost
of t
he p
opul
atio
n ha
ving
reg
ular
acc
ess
to
prim
ary
care
(34
)
Cos
t pe
r he
ad v
arie
s fr
om
US$
0.2
0 to
4.4
0 pe
r he
ad
in s
ix L
MIC
s (3
4)
Lead
: Min
istry
of
Hea
lth

64
Proposed policy priorities for preventing obesity and diabetesA
nnex
2. S
umm
ary
of s
trat
egic
inte
rven
tion
s in
10
prio
rity
are
as fo
r ac
tion
for
the
prev
enti
on o
f obe
sity
and
dia
bete
s in
the
Eas
tern
Med
iter
rane
an R
egio
nA
rea
for
acti
onSt
rate
gic
inte
rven
tion
sEx
tent
and
str
engt
h of
ev
iden
cePo
tent
ial h
ealt
h im
pact
(D
ALY
s sa
ved)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Esta
blish
or
stre
ngth
en, a
s ap
prop
riate
, a h
igh-
leve
l m
ultis
ecto
ral m
echa
nism
to
defi
ne a
nd o
vers
ee t
he
impl
emen
tatio
n of
food
and
ph
ysic
al a
ctiv
ity p
olic
ies
for
the
prev
entio
n of
obe
sity
and
diab
etes
Glo
bally
, cou
ntrie
s ha
ve
inad
equa
te c
oord
inat
ion
mec
hani
sms,
and
coor
dina
tion
with
in a
nd b
etw
een
min
istrie
s an
d ot
her
part
ners
is
inad
equa
te o
r in
effe
ctiv
e (4
1). W
HO
has
long
re
com
men
ded
that
cou
ntrie
s im
plem
ent
cros
s-go
vern
men
t, m
ultis
ecto
ral g
over
nanc
e m
echa
nism
s to
ste
er a
ctio
n on
di
et a
nd n
utrit
ion
Lead
: Pre
siden
t/Pr
ime
Min
ister
’s O
ffice
with
M
inist
ry o
f Hea
lthO
ther
: Tre
asur
y/Fi
nanc
e, T
rade
, Fo
reig
n A
ffairs
, In
dust
ry, E
nerg
y, So
cial
W
elfa
re, J
ustic
e/Se
curit
y, A
gric
ultu
re,
Food
, Edu
catio
n,
Com
mun
icat
ion,
U
rban
Pla
nnin
g,
Hou
sing,
Envi
ronm
ent,
Tran
spor
t an
d Sp
ort
Esta
blish
nat
iona
l tar
gets
for
obes
ity a
nd d
iabe
tes,
alon
g w
ith S
MA
RT c
omm
itmen
ts
for
actio
n, a
nd w
ork
with
W
HO
to
deve
lop
and
impl
emen
t a
mon
itorin
g fr
amew
ork
for
repo
rtin
g on
pr
ogre
ss
Gov
ernm
ents
tha
t pr
iorit
ize
nutr
ition
in p
olic
y do
cum
ents
sp
end
mor
e m
oney
on
nutr
ition
, but
, by
2016
, on
ly 3
0% o
f cou
ntrie
s ha
d se
t ta
rget
s fo
r ob
esity
and
di
abet
es in
the
ir na
tiona
l NC
D
plan
s (4
3)
Lead
: Pre
siden
t/Pr
ime
Min
ister
’s O
ffice
with
M
inist
ry o
f Hea
lthO
ther
: As
abov
e
Impl
emen
t ev
iden
ce-
base
d co
mm
unity
-bas
ed
inte
rven
tions
, add
ress
ing
both
hea
lthy
eatin
g an
d ph
ysic
al a
ctiv
ity, c
ompr
ising
di
ffere
nt a
ctiv
ities
and
ta
rget
ing
high
-risk
gro
ups,
to p
rom
ote
and
faci
litat
e be
havi
our
chan
ge a
nd
prev
ent
obes
ity a
nd
diab
etes
Com
mun
ity-b
ased
in
terv
entio
ns w
hich
com
prise
m
any
diffe
rent
act
iviti
es a
nd
addr
ess
both
die
t an
d ph
ysic
al
activ
ity c
an b
e ef
fect
ive
(116
). Su
ch in
terv
entio
ns u
sual
ly
incl
ude
a st
rong
edu
catio
nal
com
pone
nt a
nd m
ay t
arge
t hi
gh-r
isk g
roup
s, su
ch a
s th
ose
who
are
at
a hi
gh r
isk o
f de
velo
ping
dia
bete
s (1
16)
DA
LYs:
Disa
bilit
y A
djus
ted
Life
Year
s; G
DP:
gro
ss d
omes
tic p
rodu
ct; H
FSS:
high
in fa
t, sa
lt or
sug
ar; H
ICs:
high
-inco
me
coun
trie
s; LM
ICs:
low
- or
mid
dle-
inco
me
coun
trie
s; M
ET: m
etab
olic
equ
ival
ent
of t
ask;
NC
D: n
onco
mm
unic
able
di
seas
e; U
K: U
nite
d Ki
ngdo
m.

65
Ann
ex 2
. Sum
mar
y of
str
ateg
ic in
terv
enti
ons
in 1
0 pr
iori
ty a
reas
for
acti
on fo
r th
e pr
even
tion
of o
besi
ty a
nd d
iabe
tes
in t
he E
aste
rn M
edit
erra
nean
Reg
ion
Are
a fo
r ac
tion
Stra
tegi
c in
terv
enti
ons
Exte
nt a
nd s
tren
gth
of
evid
ence
Pote
ntia
l hea
lth
impa
ct (
DA
LYs
save
d)
Cos
t–ef
fect
iven
ess
(U
S$ p
er D
ALY
sa
ved)
Affo
rdab
ility
(im
plem
enta
tion
cos
t in
U
S$ p
er c
apit
a: v
ery
low
=
<US$
0.5
0; q
uite
low
=
< U
S$ 1
; hig
her
= >
US$
1)
Gov
ernm
ent
inst
itut
ions
in
volv
ed (
lead
bod
y,
othe
r m
inis
trie
s/de
part
men
ts
invo
lved
)
Esta
blish
or
stre
ngth
en, a
s ap
prop
riate
, a h
igh-
leve
l m
ultis
ecto
ral m
echa
nism
to
defi
ne a
nd o
vers
ee t
he
impl
emen
tatio
n of
food
and
ph
ysic
al a
ctiv
ity p
olic
ies
for
the
prev
entio
n of
obe
sity
and
diab
etes
Glo
bally
, cou
ntrie
s ha
ve
inad
equa
te c
oord
inat
ion
mec
hani
sms,
and
coor
dina
tion
with
in a
nd b
etw
een
min
istrie
s an
d ot
her
part
ners
is
inad
equa
te o
r in
effe
ctiv
e (4
1). W
HO
has
long
re
com
men
ded
that
cou
ntrie
s im
plem
ent
cros
s-go
vern
men
t, m
ultis
ecto
ral g
over
nanc
e m
echa
nism
s to
ste
er a
ctio
n on
di
et a
nd n
utrit
ion
Lead
: Pre
siden
t/Pr
ime
Min
ister
’s O
ffice
with
M
inist
ry o
f Hea
lthO
ther
: Tre
asur
y/Fi
nanc
e, T
rade
, Fo
reig
n A
ffairs
, In
dust
ry, E
nerg
y, So
cial
W
elfa
re, J
ustic
e/Se
curit
y, A
gric
ultu
re,
Food
, Edu
catio
n,
Com
mun
icat
ion,
U
rban
Pla
nnin
g,
Hou
sing,
Envi
ronm
ent,
Tran
spor
t an
d Sp
ort
Esta
blish
nat
iona
l tar
gets
for
obes
ity a
nd d
iabe
tes,
alon
g w
ith S
MA
RT c
omm
itmen
ts
for
actio
n, a
nd w
ork
with
W
HO
to
deve
lop
and
impl
emen
t a
mon
itorin
g fr
amew
ork
for
repo
rtin
g on
pr
ogre
ss
Gov
ernm
ents
tha
t pr
iorit
ize
nutr
ition
in p
olic
y do
cum
ents
sp
end
mor
e m
oney
on
nutr
ition
, but
, by
2016
, on
ly 3
0% o
f cou
ntrie
s ha
d se
t ta
rget
s fo
r ob
esity
and
di
abet
es in
the
ir na
tiona
l NC
D
plan
s (4
3)
Lead
: Pre
siden
t/Pr
ime
Min
ister
’s O
ffice
with
M
inist
ry o
f Hea
lthO
ther
: As
abov
e
Impl
emen
t ev
iden
ce-
base
d co
mm
unity
-bas
ed
inte
rven
tions
, add
ress
ing
both
hea
lthy
eatin
g an
d ph
ysic
al a
ctiv
ity, c
ompr
ising
di
ffere
nt a
ctiv
ities
and
ta
rget
ing
high
-risk
gro
ups,
to p
rom
ote
and
faci
litat
e be
havi
our
chan
ge a
nd
prev
ent
obes
ity a
nd
diab
etes
Com
mun
ity-b
ased
in
terv
entio
ns w
hich
com
prise
m
any
diffe
rent
act
iviti
es a
nd
addr
ess
both
die
t an
d ph
ysic
al
activ
ity c
an b
e ef
fect
ive
(116
). Su
ch in
terv
entio
ns u
sual
ly
incl
ude
a st
rong
edu
catio
nal
com
pone
nt a
nd m
ay t
arge
t hi
gh-r
isk g
roup
s, su
ch a
s th
ose
who
are
at
a hi
gh r
isk o
f de
velo
ping
dia
bete
s (1
16)
DA
LYs:
Disa
bilit
y A
djus
ted
Life
Year
s; G
DP:
gro
ss d
omes
tic p
rodu
ct; H
FSS:
high
in fa
t, sa
lt or
sug
ar; H
ICs:
high
-inco
me
coun
trie
s; LM
ICs:
low
- or
mid
dle-
inco
me
coun
trie
s; M
ET: m
etab
olic
equ
ival
ent
of t
ask;
NC
D: n
onco
mm
unic
able
di
seas
e; U
K: U
nite
d Ki
ngdo
m.
Annex 3
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Fisc
al m
easu
res
1.1
Prog
ress
ivel
y el
imin
ate
all n
atio
nal s
ubsid
ies
for
all t
ypes
of f
ats/
oils
and
suga
r.T
hree
– q
uart
er o
f the
cou
ntrie
s in
the
Reg
ion
subs
idize
food
com
mod
ities
, ofte
n in
clud
ing
suga
r an
d oi
ls (3
5).
The
Isla
mic
Rep
ublic
of I
ran
and
Egyp
t ha
ve r
educ
ed o
r re
mov
ed s
uch
subs
idie
s an
d re
plac
ed t
hem
with
mea
sure
s, su
ch a
s ca
sh t
rans
fers
, tha
t ar
e kn
own
to p
rovi
de m
ore
effe
ctiv
e so
cial
pro
tect
ion
for
poor
er fa
milie
s (1
28).
1.2
Impl
emen
t an
effe
ctiv
e ta
x on
sug
ar-s
wee
tene
d be
vera
ges.
Glo
bally
, by
2016
, mor
e th
an 3
0 na
tiona
l or
sub-
natio
nal a
utho
ritie
s ha
d in
trod
uced
, or
wer
e pl
anni
ng, t
axes
on
suga
r-sw
eete
ned
drin
ks –
incl
udin
g Eg
ypt,
Islam
ic R
epub
lic o
f Ira
n an
d th
e G
ulf C
oope
ratio
n C
ounc
il St
ates
in t
he E
aste
rn M
edite
rran
ean
Reg
ion
(129
–131
). A
fter
one
year
of M
exic
o’s
tax
on s
ugar
-sw
eete
ned
drin
ks (
equi
vale
nt t
o ab
out
a 10
% p
rice
incr
ease
) pu
rcha
ses
wer
e do
wn
by 1
2% o
n av
erag
e (a
nd b
y as
muc
h as
17%
in p
oore
r ho
useh
olds
) an
d ov
er U
S$ 9
milli
on h
ad b
een
colle
cted
in e
xcise
dut
y, an
incr
ease
of 5
1%
(24)
.
1.3
Con
sider
an
effe
ctiv
e pr
ogre
ssiv
e ta
x on
hig
h fa
t fo
ods
and
high
sug
ar fo
ods.
The
re is
an
emer
ging
cou
ntry
exp
erie
nce,
alth
ough
not
as
wel
l dev
elop
ed a
s th
e ex
perie
nce
on t
axin
g su
gar-s
wee
tene
d dr
inks
.H
unga
ry’s
Publ
ic H
ealth
Tax
on
food
s hi
gh in
sug
ars
or s
alt
and
on s
ugar
-sw
eete
ned
and
ener
gy d
rinks
has
res
ulte
d in
a d
rop
in c
onsu
mpt
ion
of t
axed
pro
duct
s (b
y as
muc
h as
25–
30%
acc
ordi
ng t
o so
me
estim
ates
) (1
8,27
). The
Gov
ernm
ent
also
enc
oura
ged
man
ufac
ture
rs t
o re
form
ulat
e th
eir
prod
ucts
and
rai
sed
arou
nd €
60
milli
on in
201
3 fo
r go
vern
men
t he
alth
spe
ndin
g (6
).D
enm
ark’s
sat
urat
ed fa
t ta
x, a
lthou
gh s
hort
-live
d, r
educ
ed fa
t co
nsum
ptio
n by
10–
15%
and
ra
ised
€ 13
4 m
illion
in le
ss t
han
a ye
ar (
28,2
9). F
inla
nd’s
tax
on s
wee
ts, ic
e cr
eam
and
sof
t dr
inks
rai
sed
€ 20
4 m
illion
in 2
013
(19)
.

66
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Publ
ic p
rocu
rem
ent
2.1
Impl
emen
t m
anda
tory
nut
ritio
n st
anda
rds
acro
ss
all p
ublic
inst
itutio
ns t
hrou
gh (
a) a
pplic
atio
n of
the
reg
iona
l nut
rient
pro
file
mod
el, (
b)
intr
oduc
tion
of m
eal s
tand
ards
and
(c)
mea
sure
s to
elim
inat
e th
e sa
le o
f foo
ds o
r dr
inks
hig
h in
fa
t, su
gar
or s
alt.
Nat
iona
l act
ion
on p
ublic
ly-fu
nded
food
has
gen
eral
ly fo
cuse
d on
sch
ools.
By
2013
, 47
coun
trie
s gl
obal
ly r
epor
ted
natio
nal p
olic
ies
for
scho
ol m
eals
base
d on
nat
iona
l die
tary
gu
idel
ines
and
17
had
natio
nwid
e ba
ns o
n ve
ndin
g m
achi
nes
on s
choo
l pre
mise
s (4
1).
In t
he R
egio
n, t
he Is
lam
ic R
epub
lic o
f Ira
n, Jo
rdan
, Kuw
ait
and
the
Uni
ted
Ara
b Em
irate
s, fo
r ex
ampl
e, h
ave
intr
oduc
ed n
utrit
ion
stan
dard
s fo
r he
alth
y sc
hool
mea
ls an
d in
trod
uced
re
stric
tions
on
prov
ision
or
sale
of u
nhea
lthy
food
s in
sch
ools
(132
).T
he c
once
pt o
f int
rodu
cing
nut
ritio
n st
anda
rds
acro
ss a
ll pu
blic
ly-fu
nded
food
is a
ttra
ctin
g in
crea
sing
atte
ntio
n an
d th
ere
are
som
e pi
onee
ring
exam
ples
.N
ew Yo
rk C
ity, f
or e
xam
ple,
est
ablis
hed
nutr
ition
sta
ndar
ds fo
r al
l foo
ds p
urch
ased
or
serv
ed in
all
of t
he C
ity’s
3000
sch
ools,
hos
pita
ls, c
hild
care
or
resid
entia
l car
e fa
cilit
ies
and
priso
ns in
200
8. A
ll pr
ocur
emen
t co
ntra
cts
cont
ain
a m
anda
tory
cla
use
to s
ay t
hat
any
food
pr
ovid
ed m
ust
mee
t th
e st
anda
rds
(45)
.
2.2
Issue
man
dato
ry g
uide
lines
for
the
revi
sion
of
proc
urem
ent
to p
rovi
de h
ealth
y fo
od, in
clud
ing
limiti
ng t
he v
olum
e of
fats
/oils
, sug
ar a
nd s
alt
ente
ring
publ
ic s
ecto
r ca
terin
g fa
cilit
ies
in o
rder
to
faci
litat
e th
e ne
cess
ary
men
u ch
ange
s (e
.g. s
o th
at m
eals
prov
ide
not
mor
e th
an 2
5% e
nerg
y fr
om fa
ts a
nd le
ss t
han
5% fr
om fr
ee s
ugar
s).
Som
e na
tiona
l, or
subn
atio
nal, a
utho
ritie
s ar
e ta
king
act
ion
on t
he r
ules
and
gui
delin
es o
n pr
ocur
emen
t fo
r pu
blic
inst
itutio
ns t
o en
sure
tha
t th
e fo
ods
serv
ed in
the
se in
stitu
tions
are
he
alth
y.Br
azil’s
app
roac
h to
pro
cure
men
t of
sch
ool f
ood
com
bine
d nu
triti
on s
tand
ards
with
a
requ
irem
ent
for
30%
of s
choo
l foo
d bu
dget
s to
be
spen
t in
loca
l far
mer
s’ m
arke
ts (
43).
The
Sta
te o
f Mas
sach
uset
ts in
the
Uni
ted
Stat
es o
f Am
eric
a (U
SA)
set
nutr
ition
al s
tand
ards
fo
r al
l foo
d pu
rcha
sed
by s
tate
age
ncie
s (in
clud
ing
hosp
itals,
pris
ons
and
child
care
ser
vice
s)
and
thei
r co
ntra
ctor
s (4
4).
2.3
Dev
elop
gui
danc
e an
d pr
ovid
e tr
aini
ng t
o ca
terin
g co
mpa
nies
on
appr
opria
te c
ater
ing
met
hods
in p
ublic
inst
itutio
ns t
o re
duce
the
use
of
fryi
ng a
nd s
wee
teni
ng o
f foo
ds a
nd h
elp
with
m
enu
desig
n.
Publ
ic in
stitu
tions
are
like
ly t
o re
quire
sup
port
to
be a
ble
to m
ake
the
nece
ssar
y ch
ange
s to
co
mpl
y w
ith n
ew n
utrit
iona
l sta
ndar
ds a
nd/o
r pr
ocur
emen
t gu
idel
ines
.In
the
USA
, the
fede
ral g
over
nmen
t ha
s de
velo
ped
a na
tiona
l con
trac
t te
mpl
ate
for
heal
thy
food
pro
cure
men
t (1
33).
In E
urop
e, M
alta
is d
evel
opin
g so
me
volu
ntar
y gu
idin
g pr
inci
ples
fo
r fo
od p
rocu
rem
ent,
initi
ally
focu
sing
on s
choo
ls bu
t fo
r fu
ture
use
in o
ther
sec
tors
(13
4).
2.4
Con
tinue
impl
emen
ting
thes
e m
easu
res,
scal
ing
up c
over
age
and
mon
itorin
g im
pact
.
Phys
ical
act
ivity
3.1
Prom
ote
heal
thy
phys
ical
act
ivity
thr
ough
mas
s m
edia
cam
paig
ns (
see
prio
rity
area
9)
and
ensu
re a
dequ
ate
legi
slatio
n su
ppor
ting
deliv
ery
of d
aily
phy
sical
act
ivity
for
stud
ents
in s
choo
ls an
d un
iver
sitie
s.
Man
y co
untr
ies
have
legi
slatio
n re
quiri
ng a
cer
tain
num
ber
of h
ours
to
be d
edic
ated
to
phys
ical
act
ivity
in t
he s
choo
l cur
ricul
um.
In D
enm
ark,
for
exam
ple,
par
liam
ent
revi
sed
the
law
in 2
014
to m
ake
it co
mpu
lsory
for
scho
ols
to o
ffer
an a
vera
ge o
f 45
min
utes
of p
hysic
al a
ctiv
ity p
er s
choo
l day
in p
rimar
y an
d lo
wer
-sec
onda
ry e
duca
tion
and
to a
dd a
n ex
tra
phys
ical
edu
catio
n le
sson
per
sch
ool
wee
k in
gra
de 1
. Chi
ldca
re fa
cilit
ies
are
also
req
uire
d to
incl
ude
“bod
y an
d m
otio
n” in
the
ir cu
rric
ula
(135
).
3.2
Ensu
re c
ompr
ehen
sive
deliv
ery
of r
egul
ar,
qual
ity p
hysic
al e
duca
tion
to a
ll ch
ildre
n, a
s a
key
com
pone
nt o
f edu
catio
n in
sch
ools.

67
Annex 3
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Phys
ical
act
ivity
3.3
Dev
elop
a s
et o
f sta
ndar
ds/g
uide
lines
pro
mot
ing
phys
ical
act
ivity
in t
he w
orkp
lace
, incl
udin
g fa
cilit
y/bu
ildin
g de
sign,
ava
ilabi
lity
of s
port
s fa
cilit
ies
and
prog
ram
mes
ena
blin
g ac
cess
to
faci
litie
s aw
ay fr
om t
he w
orkp
lace
.
In t
he U
nite
d Ki
ngdo
m (
UK)
, the
Nat
iona
l Ins
titut
e fo
r H
ealth
and
Car
e Ex
celle
nce
(NIC
E)
issue
d gu
idel
ines
on
prom
otin
g ph
ysic
al a
ctiv
ity in
the
wor
kpla
ce fo
r N
atio
nal H
ealth
Se
rvic
e or
gani
zatio
ns in
Eng
land
, whi
ch e
mpl
oy m
ore
than
hal
f a m
illion
peo
ple
(136
,137
). In
201
5, t
his
guid
ance
was
tra
nsla
ted
into
pra
ctic
al a
dvic
e an
d re
com
men
datio
ns a
s pa
rt o
f a
tool
kit
on h
ealth
y w
orkp
lace
(13
8).
In a
gov
ernm
ent-
supp
orte
d in
itiat
ive
in T
haila
nd, p
rivat
e an
d pu
blic
sec
tor
empl
oyer
s pr
ovid
e th
eir
empl
oyee
s w
ith t
rain
ing
and
time
to e
ngag
e in
var
ious
typ
es o
f phy
sical
ac
tiviti
es (
139)
.
3.4
Incr
ease
ava
ilabi
lity
of a
nd a
cces
sibilit
y fo
r pa
rtic
ipat
ion
in fo
rmal
and
info
rmal
rec
reat
iona
l an
d sp
ortin
g ac
tiviti
es, p
artic
ular
ly p
rovi
ding
op
port
uniti
es fo
r pa
rtic
ipat
ion
in p
rogr
amm
es
such
as “
Spor
ts-fo
r-All”
, with
em
phas
is on
en
surin
g eq
ualit
y of
acc
ess
and
oppo
rtun
ity fo
r pa
rtic
ipat
ion.
In Jo
rdan
, as
part
of a
mul
tisec
tora
l par
tner
ship
, Gre
ater
Am
man
Mun
icip
ality
ope
ned
four
pu
blic
gar
dens
at
spec
ific
times
for
wom
en o
nly
so t
hat
they
can
wal
k an
d pa
rtic
ipat
e in
ex
erci
se (
140)
. In
Bah
rain
, the
re h
ave
been
effo
rts
to r
each
agr
eem
ents
bet
wee
n th
e M
inist
ry o
f Hea
lth
and
shop
ping
mal
ls to
pro
vide
mal
ls as
a p
ublic
ven
ue fo
r sp
orts
(48
).
3.5
Dev
elop
and
impl
emen
t an
urb
an p
lann
ing
polic
y to
ens
ure
that
urb
an e
nviro
nmen
ts e
ncou
rage
pe
ople
to
rely
less
on
pers
onal
mot
orize
d ve
hicl
es a
nd s
uppo
rt a
cces
s to
saf
e, g
ende
r-se
nsiti
ve a
nd a
ge-fr
iend
ly p
ublic
tra
nspo
rt, c
yclin
g an
d w
alki
ng, in
clud
ing
by p
rovi
sion
of fa
cilit
ies,
equi
pmen
t, pu
blic
ope
n an
d gr
een
spac
es a
nd
shar
ed u
se o
f sch
ool f
acilit
ies
(bot
h in
door
and
ou
tdoo
r).
Nat
iona
l and
loca
l aut
horit
ies
are
incr
easin
gly
reco
gnisi
ng t
he n
eed
to e
nact
pol
icie
s to
cr
eate
urb
an e
nviro
nmen
ts c
ondu
cive
to
phys
ical
act
ivity
.T
he Is
lam
ic R
epub
lic o
f Ira
n ha
s im
plem
ente
d a
pack
age
of a
ctiv
ities
to
prom
ote
phys
ical
ac
tivity
, incl
udin
g im
prov
emen
ts t
o pu
blic
ope
n sp
aces
, dev
elop
men
t of
cyc
le h
ire s
chem
es
in s
ome
citie
s an
d ex
pand
ing
cycl
e la
nes
(48)
.A
live
able
nei
ghbo
urho
ods
desig
n co
de w
as in
trod
uced
in t
he c
ity o
f Per
th, W
este
rn
Aus
tral
ia. A
stu
dy c
ompa
ring
impl
emen
tatio
n in
diff
eren
t ne
ighb
ourh
oods
foun
d th
at fo
r ev
ery
10%
incr
ease
in it
s im
plem
enta
tion,
the
odd
s of
wal
king
incr
ease
d by
50%
(51
).O
man
’s N
atio
nal N
utrit
ion
Stra
tegy
201
4–20
50 in
clud
es t
he a
im t
o cr
eate
urb
an g
reen
sp
aces
and
ped
estr
ian
tran
spor
t ro
utes
for
cycl
ing,
wal
king
and
jogg
ing
in a
ll ci
ties
that
are
pe
dest
rian-
frie
ndly
and
ope
n fo
r sa
fe e
xerc
ise a
nd t
rave
l day
and
nig
ht, in
clud
ing
“gre
en
tunn
els”
of t
rees
and
shr
ubs
to p
rovi
de s
hade
for
wal
king
(14
1).
3.6
Con
tinue
impl
emen
ting
thes
e m
easu
res,
scal
ing
up c
over
age
and
mon
itorin
g im
pact
.Su
stai
ned
effo
rts
are
requ
ired
to b
ring
abou
t th
e re
quire
d ch
ange
s in
urb
an a
nd r
ural
en
viro
nmen
ts a
nd v
ario
us s
ettin
gs a
nd fa
cilit
ate
grea
ter
part
icip
atio
n in
phy
sical
act
ivity
.Fi
nlan
d ha
s sh
own
com
mitm
ent
to in
crea
sing
phys
ical
act
ivity
sin
ce 1
980
thro
ugh
a va
riety
of
diff
eren
t ac
tions
, incl
udin
g le
gisla
tion,
gui
delin
e de
velo
pmen
t, re
com
men
datio
ns a
nd lo
cal
fund
ing
(46)
. It
has
succ
essf
ully
dev
elop
ed n
atio
nal p
rogr
amm
es fo
r ev
ery
phas
e of
the
life
-co
urse
(13
5).

68
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Food
sup
ply
and
trad
e
4.1
Con
duct
a s
ituat
ion
anal
ysis
of t
he n
atio
nal a
nd/
or lo
cal f
ood
supp
ly, in
clud
ing
esta
blish
ing
the
prop
ortio
ns o
f fat
s/oi
ls an
d su
gar
used
in t
he
diet
tha
t ar
e de
rived
from
impo
rts
and
dom
estic
pr
oduc
tion,
alo
ng w
ith t
he e
xten
t of
food
m
anuf
actu
re a
nd p
roce
ssin
g w
ithin
the
cou
ntry
an
d th
e su
pply
of f
ruit,
veg
etab
les
and
who
le
grai
ns.
As
part
of d
evel
opm
ent
of a
nut
ritio
n st
rate
gy fo
r O
man
, a S
WO
T a
naly
sis w
as c
ondu
cted
, w
hich
iden
tified
a n
eed
to r
educ
e im
port
s of
hig
h-en
ergy
den
sity
food
pro
duct
s. T
he
nutr
ition
str
ateg
y in
clud
es t
he a
im o
f red
ucin
g im
port
atio
n of
hig
h-de
nsity
food
s to
< 3
0%
of a
ll in
take
s th
roug
h co
oper
ativ
e ag
reem
ents
with
reg
iona
l sup
plie
rs, in
crea
sed
regu
latio
n an
d im
port
tar
iffs
on u
nhea
lthy
food
s (1
41).
4.2
Faci
litat
e th
e de
velo
pmen
t of
loca
l foo
d po
licie
s an
d en
cour
age
city
aut
horit
ies
to s
ign
the
Mila
n U
rban
Foo
d Po
licy
Pact
and
impl
emen
t its
Fr
amew
ork
for A
ctio
n to
dev
elop
sus
tain
able
ur
ban
food
sys
tem
s.
By t
he e
nd o
f 201
6, 1
33 c
ities
glo
bally
, with
a t
otal
of m
ore
than
460
milli
on in
habi
tant
s, ha
d sig
ned
up t
o th
e M
ilan
Urb
an F
ood
Polic
y Pa
ct. I
n th
e Ea
ster
n M
edite
rran
ean,
a fe
w c
ities
, su
ch a
s Be
thle
hem
and
Heb
ron,
are
sig
nato
ries
(63)
.
4.3
Con
sider
intr
oduc
ing
stan
dard
s or
oth
er le
gal
inst
rum
ents
(e.
g. co
mpo
sitio
nal s
tand
ards
, tar
iffs,
impo
rt r
estr
ictio
ns, s
ales
ban
s, pl
anni
ng la
ws,
zoni
ng p
olic
ies)
to
redu
ce t
he v
olum
e an
d im
prov
e th
e qu
ality
of f
ats/
oils
and
redu
ce s
ugar
s in
the
nat
iona
l and
loca
l foo
d su
pply.
A n
umbe
r of
cou
ntrie
s ha
ve in
trod
uced
impo
rt d
utie
s on
pro
duct
s su
ch a
s so
ft dr
inks
, su
gar,
conf
ectio
nery
, ice
crea
m, f
atty
mea
ts a
nd s
peci
fic o
ils.
In r
espo
nse
to c
once
rns
abou
t hi
gh le
vels
of c
onsu
mpt
ion
of c
heap
mea
t pr
oduc
ts w
ith a
ve
ry h
igh
fat
cont
ent
– su
ch a
s tu
rkey
tai
ls –
, Sam
oa a
nd G
hana
, for
exa
mpl
e, in
trod
uced
le
gal m
easu
res
(a s
ales
ban
and
com
posit
iona
l sta
ndar
ds r
espe
ctiv
ely)
in o
rder
to
limit
avai
labi
lity
of t
hese
pro
duct
s (5
9,60
).T
he Is
lam
ic R
epub
lic o
f Ira
n in
trod
uced
mea
sure
s to
red
uce
impo
rts
of p
alm
oil,
with
the
ai
m o
f low
erin
g th
e sh
are
of p
alm
oil
in t
otal
veg
etab
le o
il co
nsum
ptio
n to
30%
(14
2).
Om
an’s
nutr
ition
str
ateg
y in
clud
es t
he a
im o
f red
ucin
g im
port
atio
n of
hig
h-de
nsity
food
s to
<30
% o
f all
inta
kes
thro
ugh
coop
erat
ive
agre
emen
ts w
ith r
egio
nal s
uppl
iers
, incr
ease
d re
gula
tion
and
impo
rt t
ariff
s on
unh
ealth
y fo
ods
(141
).
4.4
Con
sider
rem
ovin
g ag
ricul
tura
l sub
sidie
s fo
r pr
oduc
ers
of s
ugar
s an
d oi
ls (e
spec
ially
tho
se
oils
high
in s
atur
ated
fatt
y ac
ids)
, rep
laci
ng t
hem
, w
here
nec
essa
ry, w
ith o
ther
mec
hani
sms
to
supp
ort
farm
ers
and
grow
ers.
In E
aste
rn E
urop
ean
coun
trie
s, ch
ange
s to
nat
iona
l sub
sidie
s of
ani
mal
fats
afte
r th
e po
litic
al
chan
ges
of t
he e
arly
199
0s le
d to
muc
h hi
gher
con
sum
ptio
n of
veg
etab
le o
ils in
som
e co
untr
ies,
with
res
ulta
nt h
ealth
ben
efits
(14
3).

69
Annex 3
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Ref
orm
ulat
ion
5.1
Coo
pera
te w
ith o
ther
Mem
ber
Stat
es t
o ad
opt
a re
gion
al a
ppro
ach
for
enga
ging
with
fo
od p
rodu
cers
to
driv
e fo
od r
efor
mul
atio
n to
el
imin
ate
tran
s fa
ts a
nd r
educ
e pr
ogre
ssiv
ely
tota
l and
sat
urat
ed fa
t, sa
lt, s
ugar
s, en
ergy
and
po
rtio
n siz
e in
a s
ubst
antia
l pro
port
ion
of
proc
esse
d fo
ods.
Mos
t of
the
exp
erie
nce
of r
efor
mul
atio
n to
dat
a ha
s fo
cuse
d on
red
ucin
g sa
lt le
vels
in
proc
esse
d fo
ods.
A 2
015
revi
ew fo
und
that
61
coun
trie
s in
clud
ed r
efor
mul
atio
n in
the
ir na
tiona
l sal
t re
duct
ion
stra
tegi
es, 1
9 co
untr
ies
repo
rt r
educ
tions
in t
he s
alt
cont
ent
of fo
ods
and
12 c
ount
ries
repo
rt a
fall
in p
opul
atio
n sa
lt in
take
(65
).
Kuw
ait
has
intr
oduc
ed a
vol
unta
ry fo
od r
efor
mul
atio
n pr
ogra
mm
e to
red
uce
salt
and
fat
leve
ls, w
ith a
n in
itial
focu
s on
red
ucin
g sa
lt th
e sa
lt co
nten
t of
bre
ad a
nd c
hees
es (
132)
.M
ore
than
11
coun
trie
s ha
ve in
trod
uced
law
s to
lim
it th
e tr
ans
fatt
y ac
id c
onte
nt o
f foo
ds,
incl
udin
g, fr
om t
he R
egio
n, t
he Is
lam
ic R
epub
lic o
f Ira
n (1
32).
A n
umbe
r of
cou
ntrie
s ha
ve m
oved
bey
ond
salt,
to
impl
emen
t re
form
ulat
ion
mea
sure
s to
re
duce
the
leve
ls of
oth
er n
utrie
nts
or in
gred
ient
s.T
he N
ethe
rland
s ha
s im
plem
ente
d a
prog
ram
me
to r
educ
e sa
lt, s
atur
ated
fat
and
calo
ries
in s
ugar
pro
duct
s; In
the
UK,
a p
rogr
amm
e to
red
uce
suga
r le
vels
by 2
0% b
y 20
20 w
ill fo
cus
initi
ally
on
nine
typ
es o
f pro
duct
tha
t m
ake
the
bigg
est
cont
ribut
ion
to c
hild
ren’
s su
gar
inta
ke [
brea
kfas
t ce
real
s, yo
ghur
ts, b
iscui
ts, c
akes
, con
fect
ione
ry, m
orni
ng g
oods
(fo
r ex
ampl
e, p
astr
ies)
, pud
ding
s, ic
e cr
eam
and
sw
eet
spre
ads]
(14
4).
5.2
Enga
ge w
ith p
rivat
e se
ctor
pro
vide
rs o
f foo
d in
cat
erin
g/fo
od s
ervi
ce o
utle
ts (
incl
udin
g ta
keaw
ays
and
stre
et fo
od t
rade
rs)
to e
stab
lish
a pr
ogra
mm
e to
elim
inat
e tr
ans
fats
and
red
uce
prog
ress
ivel
y to
tal a
nd s
atur
ated
fat,
salt,
sug
ars,
ener
gy a
nd p
ortio
n siz
e, w
ith d
efine
d qu
antifi
ed
redu
ctio
ns in
use
of t
hese
ingr
edie
nts.
Sing
apor
e’s
Hea
lthie
r H
awke
r pr
ogra
mm
e en
cour
ages
str
eet
food
ven
dors
to
use
heal
thie
r in
gred
ient
s an
d in
volv
es t
he g
over
nmen
t ab
sorb
ing
som
e of
the
cos
ts a
ssoc
iate
d w
ith t
he
use
of t
he h
ealth
ier
ingr
edie
nts
(145
).T
he U
K’s
suga
r re
duct
ion
prog
ram
me
– to
red
uce
suga
r co
nten
ts b
y at
leas
t 20
% b
y 20
20
– w
ill al
so a
pply
to
the
out-
of-h
ome
sect
or, in
clud
ing
rest
aura
nts,
take
away
s an
d ca
fés
(144
)
Mar
ketin
g
6.1
Wor
k w
ith o
ther
cou
ntrie
s in
the
Reg
ion
to
esta
blish
a c
oord
inat
ed a
ppro
ach,
incl
udin
g ap
prop
riate
lega
l adv
ice,
to
redu
ce t
he im
pact
of
cros
s-bo
rder
mar
ketin
g.
In t
he E
aste
rn M
edite
rran
ean
Reg
ion,
whe
re c
ross
-bor
der
mar
ketin
g is
so p
reva
lent
, a
regi
onal
app
roac
h w
ill be
fund
amen
tal.
In t
he E
urop
ean
Uni
on fo
od m
anuf
actu
rers
hav
e th
emse
lves
rec
ogni
zed
the
valu
e of
th
e le
vel p
layi
ng fi
eld
crea
ted
by a
har
mon
ized
regi
onal
app
roac
h an
d ha
ve in
trod
uced
a
volu
ntar
y pl
edge
(th
e EU
Ple
dge)
to
rest
rict
broa
dcas
t m
arke
ting
of fo
ods
high
in fa
t or
sal
t or
sug
ar t
o ch
ildre
n (1
46).

70
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Mar
ketin
g
6.2
Impl
emen
t th
e W
HO
Set
of R
ecom
men
datio
ns
on M
arke
ting
of F
oods
and
Non
-alc
ohol
ic
Beve
rage
s to
Chi
ldre
n an
d co
nsid
er m
anda
tory
re
stric
tions
to
elim
inat
e al
l for
ms
of m
arke
ting
of fo
ods
high
in fa
t, su
gar
and
salt
to c
hild
ren
and
adol
esce
nts
(up
to a
ge 1
8) a
cros
s al
l med
ia,
acco
rdin
g to
the
Reg
iona
l Act
ion
Plan
to
Add
ress
U
nopp
osed
Mar
ketin
g of
Unh
ealth
y Fo
od a
nd
Beve
rage
s.
Six
year
s on
from
the
pub
licat
ion
of W
HO
’s Se
t of
Rec
omm
enda
tions
on
the
Mar
ketin
g of
Foo
ds a
nd N
on-A
lcoh
olic
Bev
erag
es t
o C
hild
ren,
aro
und
20%
of c
ount
ries
in t
he
East
ern
Med
iterr
anea
n (a
nd 2
8% o
f cou
ntrie
s gl
obal
ly)
have
intr
oduc
ed g
over
nmen
t le
gisla
tion
on t
his
issue
(14
7). A
lthou
gh n
o co
untr
y ha
s co
mpr
ehen
sivel
y im
plem
ente
d th
e R
ecom
men
datio
ns, t
here
are
ele
men
ts o
f goo
d pr
actic
e.R
estr
ictio
ns in
trod
uced
in S
outh
Kor
ea, I
rela
nd, B
razi
l and
Nor
way
con
cern
chi
ldre
n up
to
the
age
of 1
8 ye
ars
(132
). M
easu
res
in C
hile
and
Por
tuga
l inc
lude
aud
ienc
es w
ith 2
0% o
r m
ore
child
ren,
in c
ontr
ast
to
man
y sc
hem
es t
hat
only
cov
er a
udie
nces
com
prisi
ng a
t le
ast
35%
or
50%
chi
ldre
n (1
32).
Res
tric
tions
in P
eru
and
Braz
il ar
e ba
sed
on b
road
defi
nitio
ns o
f mar
ketin
g, co
verin
g di
ffere
nt m
edia
(e.
g. te
levi
sion,
rad
io, p
rint,
Inte
rnet
, app
s) a
nd m
arke
ting
met
hods
(13
2).
In t
he E
aste
rn M
edite
rran
ean
Reg
ion,
the
Isla
mic
Rep
ublic
of I
ran
has
intr
oduc
ed r
ules
to
rest
rict
radi
o an
d te
levi
sion
adve
rtisi
ng t
o ch
ildre
n an
d ad
oles
cent
s (u
p to
19
year
s of
age
) (u
npub
lishe
d re
port
).
6.3
Use
the
reg
iona
l nut
rient
pro
file
mod
el, w
hich
ca
tego
rizes
the
app
ropr
iate
leve
l of n
utrie
nts
in
food
s, to
iden
tify
food
s to
whi
ch t
he m
arke
ting
rest
rictio
ns s
houl
d ap
ply.
The
nut
rient
pro
file
mod
el d
evel
oped
for
the
Euro
pean
reg
ion
has
alre
ady
been
ado
pted
an
d ad
apte
d by
a n
umbe
r of
Eur
opea
n co
untr
ies
(e.g
. Slo
veni
a, Ire
land
) fo
r us
e in
res
tric
ting
mar
ketin
g to
chi
ldre
n.
6.4
Con
duct
an
asse
ssm
ent
(pre
fera
bly
as p
art
of a
reg
iona
l col
labo
ratio
n) o
f the
impa
ct o
f m
arke
ting
of fo
ods
high
in fa
t, su
gar
or s
alt
to
adul
ts.
Polic
y at
tent
ion,
to
date
, has
focu
sed
pred
omin
antly
on
mar
ketin
g to
chi
ldre
n an
d th
is is
an
unde
r-res
earc
hed
area
.
6.5
Con
sider
ext
endi
ng m
anda
tory
res
tric
tions
on
mar
ketin
g of
unh
ealth
y fo
ods
to w
hole
po
pula
tion.
Som
e co
untr
ies
have
tak
en s
teps
to
limit
the
effe
cts
of m
arke
ting
of fo
ods
high
in fa
t or
sal
t or
sug
ar t
o th
e w
hole
pop
ulat
ion.
The
Isla
mic
Rep
ublic
of I
ran
has
proh
ibite
d br
oadc
ast
adve
rtisi
ng o
f sof
t dr
inks
sin
ce 2
004
and,
in 2
014,
furt
her
rest
rictio
ns w
ere
prop
osed
on
an a
dditi
onal
24
food
item
s (1
32).
Irela
nd li
mits
bro
adca
st a
dver
tisin
g of
HFS
S fo
ods
to n
o m
ore
than
25%
of s
old
adve
rtisi
ng
time
(132
).
6.6
Legi
slate
to
allo
w r
etai
l pro
mot
ions
onl
y on
he
alth
y fo
ods.
Som
e U
K-ba
sed
supe
rmar
ket
chai
ns h
ave
volu
ntar
ily a
gree
d to
lim
it th
e pr
opor
tion
of
pric
e pr
omot
ions
on
HFS
S fo
ods
(148
).
Labe
lling
7.1
Impl
emen
t a
man
dato
ry fr
ont-
of-p
ack
labe
lling
sche
me
with
ele
men
ts t
o en
able
con
sum
ers
to
inte
rpre
t in
form
atio
n ea
sily
(e.g
. col
our
codi
ng o
r th
e us
e of
ter
ms
such
as “
high
” “m
ediu
m”,
“low
”).
Man
dato
ry fr
ont-
of-p
ack
nutr
ition
labe
lling
has
been
intr
oduc
ed in
, for
exa
mpl
e, E
cuad
or
and
Mex
ico
(132
), an
d tr
affic
-ligh
t la
bellin
g ha
s be
en in
trod
uced
in t
he Is
lam
ic R
epub
lic o
f Ira
n (1
33).
Gov
ernm
ent-
defin
ed v
olun
tary
tra
ffic-
light
sch
emes
are
in p
lace
in a
num
ber
of
othe
r co
untr
ies
such
as
Sout
h Ko
rea
and
the
UK
(132
).
7.2
Enfo
rce
the
labe
lling
sche
me
and
mon
itor
its
impa
ct.
It is
impo
rtan
t th
at t
he in
trod
uctio
n of
the
labe
lling
sche
me
is pr
oper
ly e
nfor
ced
and
mon
itore
d, p
artic
ular
ly t
o as
sess
the
impa
ct a
cros
s al
l soc
ioec
onom
ic g
roup
s.

71
Annex 3
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Brea
stfe
edin
g
8.1
Prom
ote
brea
stfe
edin
g th
roug
h m
anda
tory
ba
by-fr
iend
ly h
ealth
sys
tem
s an
d ef
fect
ive
com
mun
ity-b
ased
str
ateg
ies.
Cam
bodi
a in
crea
sed
brea
stfe
edin
g fr
om 1
1% in
200
0 to
74%
by
2010
thr
ough
vig
orou
s pr
omot
ion
of b
reas
tfeed
ing,
regu
latin
g th
e m
arke
ting
of b
reas
t-m
ilk s
ubst
itute
s an
d ba
by
food
s an
d a
wid
e-ra
ngin
g ba
by-fr
iend
ly in
itiat
ive
(114
).
8.2
Fully
impl
emen
t of
the
Inte
rnat
iona
l Cod
e of
M
arke
ting
of B
reas
t-m
ilk S
ubst
itute
s an
d th
e W
HO
Gui
danc
e on
end
ing
inap
prop
riate
pr
omot
ion
of fo
ods
for
infa
nts
and
youn
g ch
ildre
n.
In t
he R
egio
n, 8
5% o
f cou
ntrie
s ha
ve e
nact
ed le
gisla
tion
to im
plem
ent
the
Cod
e bu
t on
ly
30%
hav
e la
ws
with
all
or m
any
of t
he C
ode
prov
ision
s (1
13).
Keny
a an
d So
uth
Afr
ica
have
ado
pted
com
preh
ensiv
e C
ode-
rela
ted
legi
slatio
n, in
clud
ing
wid
e-ra
ngin
g pr
ohib
ition
s on
pro
mot
iona
l act
iviti
es a
nd m
easu
res
to e
nsur
e ef
fect
ive
enfo
rcem
ent
(113
). Ku
wai
t’s 2
014
Cod
e-im
plem
entin
g le
gisla
tion
feat
ures
a b
road
sco
pe, a
wid
e ra
nge
of
proh
ibiti
ons
and
deta
iled
requ
irem
ents
for
info
rmat
ion
and
educ
atio
n m
ater
ials
and
labe
lling
(113
).
8.3
Empo
wer
wom
en t
o ex
clus
ivel
y br
east
feed
by
enac
ting
prog
ress
ivel
y in
crea
sing
rem
uner
ated
tim
e of
f wor
k up
to
a go
al o
f 6 m
onth
s’ m
anda
tory
pai
d m
ater
nity
leav
e, a
s w
ell a
s po
licie
s th
at e
ncou
rage
wom
en t
o br
east
feed
in
the
wor
kpla
ce, in
clud
ing
brea
stfe
edin
g br
eaks
an
d pr
ovisi
on o
f sui
tabl
e fa
cilit
ies.
Glo
bally
, 32
coun
trie
s ha
ve r
atifi
ed t
he In
tern
atio
nal L
abou
r O
rgan
izat
ion
Mat
erni
ty
Prot
ectio
n C
onve
ntio
n (C
onve
ntio
n N
o. 1
83)
(149
). In
the
Eas
tern
Med
iterr
anea
n R
egio
n, M
oroc
co r
atifi
ed t
he C
onve
ntio
n in
201
1, p
rovi
ding
14
wee
ks o
f mat
erni
ty le
ave
(149
).
Mas
s m
edia
9.1
Impl
emen
t ap
prop
riate
soc
ial m
arke
ting
cam
paig
ns, le
d by
the
pub
lic s
ecto
r, on
hea
lthy
diet
and
phy
sical
act
ivity
in o
rder
to
build
co
nsen
sus,
com
plem
ent
the
othe
r in
terv
entio
ns
in t
he p
acka
ge a
nd e
ncou
rage
beh
avio
ur c
hang
e.
Man
y co
untr
ies
have
impl
emen
ted
publ
ic a
war
enes
s, m
ass
med
ia a
nd in
form
atio
nal
cam
paig
ns a
nd s
ocia
l mar
ketin
g on
hea
lthy
eatin
g. T
here
are
also
exa
mpl
es o
f cou
ntrie
s us
ing
mas
s m
edia
cam
paig
ns t
o re
info
rce
othe
r ac
tions
.M
exic
o la
unch
ed a
med
ia c
ampa
ign
aim
ed a
t ra
ising
aw
aren
ess
of o
besit
y at
the
sam
e tim
e as
intr
oduc
ing
the
suga
ry d
rink
tax
and
new
fron
t-of
-pac
k la
bellin
g re
quire
men
ts, a
s w
ell a
s an
initi
ativ
e on
food
in s
choo
ls an
d in
crea
sing
acce
ss t
o dr
inki
ng w
ater
(25
).T
he P
ourin
g on
the
Pou
nds
publ
ic in
form
atio
n ca
mpa
ign
in N
ew Yo
rk C
ity r
an a
t th
e sa
me
time
as t
he e
xcise
tax
was
intr
oduc
ed o
n su
gary
drin
ks. A
35%
and
27%
dro
p in
the
nu
mbe
r of
adu
lts a
nd p
ublic
hig
h sc
hool
stu
dent
s re
spec
tivel
y ha
ving
one
of m
ore
suga
ry
drin
ks a
day
was
rep
orte
d (2
6).
9.2
Ensu
re s
usta
ined
impl
emen
tatio
n of
cam
paig
ns
and
mon
itor
thei
r im
pact
.C
ampa
igns
nee
d to
be
sust
aine
d in
ord
er t
o ha
ve a
long
-ter
m im
pact
.
Hea
lth s
ecto
r10
.1 E
nsur
e pr
ovisi
on o
f die
tary
cou
nsel
ling
on n
utrit
ion,
phy
sical
act
ivity
and
hea
lthy
wei
ght
gain
bef
ore
and
durin
g pr
egna
ncy
for
pros
pect
ive
mot
hers
and
fath
ers.
Seve
ral c
ount
ries
prov
ide
nutr
ition
al c
ouns
ellin
g to
pre
gnan
t w
omen
. T
hese
incl
ude,
for
exam
ple,
Fin
land
, whe
re n
utrit
ion
guid
ance
is p
rovi
ded
by p
ublic
hea
lth
nurs
es a
s pa
rt o
f ant
enat
al a
nd p
ostn
atal
car
e, a
nd M
exic
o, w
here
indi
vidu
al c
ouns
ellin
g is
prov
ided
to
preg
nant
wom
en a
nd m
othe
rs o
f chi
ldre
n un
der
five
year
s (1
32).

72
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 3
. Exa
mpl
es o
f cou
ntry
exp
erie
nce
wit
h im
plem
enta
tion
of t
he p
ropo
sed
stra
tegi
c in
terv
enti
ons
Pri
orit
y ar
ea fo
r ac
tion
Prop
osed
str
ateg
ic in
terv
enti
ons
Exam
ples
of c
ount
ry e
xper
ienc
e of
impl
emen
tati
on
Hea
lth s
ecto
r
10.2
inte
grat
e sc
reen
ing
for
over
wei
ght
and
othe
r di
abet
es r
isk fa
ctor
s in
to p
rimar
y he
alth
car
e an
d pr
ovid
e pr
imar
y-ca
re b
ased
cou
nsel
ling
for
high
-risk
indi
vidu
als.
Cou
ntrie
s th
at h
ave
inte
grat
ed s
cree
ning
and
/or
coun
sellin
g fo
r hi
gh-r
isk in
divi
dual
s in
to
prim
ary
care
incl
ude
Braz
il, Fi
ji, So
uth
Afr
ica
and
Mal
aysia
(13
2).
Und
er B
razi
l’s U
nifie
d H
ealth
Sys
tem
hea
lth t
eam
s pr
omot
e he
alth
y ea
ting,
eval
uate
fo
od in
take
and
ant
hrop
omet
ry o
f ind
ivid
uals
and
prov
ide
nutr
ition
al c
ouns
ellin
g. T
he
gove
rnm
ent
prov
ides
man
uals
and
teac
hing
mat
eria
ls fo
r he
alth
pro
fess
iona
ls, a
s w
ell a
s pr
ovid
ing
fund
s fo
r th
is w
ork
(132
).U
nder
Qat
ar’s
natio
nal n
utrit
ion
and
phys
ical
act
ivity
act
ion
plan
, reg
ular
scr
eeni
ng o
f th
e po
pula
tion
in p
rimar
y he
alth
car
e ce
ntre
s w
as in
trod
uced
, alo
ng w
ith p
rovi
sion
of
coun
sellin
g fo
r hi
gh-r
isk g
roup
s (1
50).
10.3
Est
ablis
h or
str
engt
hen,
as
appr
opria
te, a
hi
gh-le
vel m
ultis
ecto
ral m
echa
nism
to
defin
e an
d ov
erse
e th
e im
plem
enta
tion
of fo
od a
nd
phys
ical
act
ivity
pol
icie
s fo
r th
e pr
even
tion
of
obes
ity a
nd d
iabe
tes.
Man
y co
untr
ies
have
est
ablis
hed
som
e ki
nd o
f cro
ss-g
over
nmen
t co
ordi
natio
n m
echa
nism
fo
r nu
triti
on a
nd/o
r no
ncom
mun
icab
le d
iseas
es (
NC
D)
prev
entio
n. L
eade
rshi
p at
the
hi
ghes
t le
vel i
s im
port
ant
to c
reat
e th
e ne
cess
ary
polit
ical
will.
In t
he P
acifi
c isl
and
stat
es, t
he P
acifi
c N
CD
Par
tner
ship
, whi
ch w
as s
et u
p to
enc
oura
ge a
m
ultis
ecto
ral a
ppro
ach,
has
hig
h le
vel p
oliti
cal p
artic
ipat
ion
with
the
invo
lvem
ent
of P
acifi
c Isl
and
Foru
m L
eade
rs a
nd M
inist
ers
of H
ealth
(13
2). B
razi
l’s N
atio
nal C
ounc
il of
Foo
d an
d N
utrit
ion
Secu
rity
(CO
NSE
A)
repo
rts
to t
he o
ffice
of t
he c
ount
ry’s
Pres
iden
t (1
32).
10.4
Est
ablis
h na
tiona
l tar
gets
for
obes
ity a
nd
diab
etes
, alo
ng w
ith S
MA
RT c
omm
itmen
ts
for
actio
n, a
nd w
ork
with
WH
O t
o de
velo
p an
d im
plem
ent
a m
onito
ring
fram
ewor
k fo
r re
port
ing
on p
rogr
ess.
The
Tun
isian
str
ateg
y fo
r pr
even
ting
and
tack
ling
obes
ity 2
013-
2017
set
s ou
t fiv
e pr
iorit
y ar
eas
and
88 s
peci
fic a
ctio
ns a
re d
etai
led.
For
eac
h ac
tion
the
body
res
pons
ible
(an
d pa
rtne
rs),
timet
able
, sou
rces
of i
nfor
mat
ion
and
mon
itorin
g in
dica
tors
are
defi
ned
(151
).
10.5
Impl
emen
t ev
iden
ce-b
ased
com
mun
ity-b
ased
in
terv
entio
ns, a
ddre
ssin
g bo
th h
ealth
y ea
ting
and
phys
ical
act
ivity
, com
prisi
ng d
iffer
ent
activ
ities
and
tar
getin
g hi
gh-r
isk g
roup
s, to
pr
omot
e an
d fa
cilit
ate
beha
viou
r ch
ange
and
pr
even
t ob
esity
and
dia
bete
s.
Som
e of
the
mos
t w
ell-k
now
n w
ork
in t
his
area
has
tak
en p
lace
in F
inla
nd, w
here
, fam
ously
, th
e N
orth
Kar
elia
pro
ject
red
uced
car
diov
ascu
lar
deat
hs. P
rogr
amm
es t
arge
ting
mid
dle-
aged
ove
rwei
ght
men
and
wom
en a
t hi
gher
risk
of d
iabe
tes
(ove
rwei
ght
with
impa
ired
gluc
ose
tole
ranc
e) p
rovi
ded
indi
vidu
al c
ouns
ellin
g an
d re
duce
d th
e ris
k of
dia
bete
s by
mor
e th
an 5
0% (
152)
.

73
Ann
ex 4
. Fe
asib
ility
con
side
rati
ons
for
impl
emen
ting
str
ateg
ic i
nter
vent
ions
in
10
prio
rity
are
as fo
r ac
tion
to
prev
ent
obes
ity
and
diab
etes
in t
he E
aste
rn
Med
iter
rane
an R
egio
n Pr
iori
ty a
rea
for
acti
onR
each
(ca
paci
ty t
o de
liver
an
inte
rven
tion
to
the
targ
et
popu
lati
on)
Tech
nica
l com
plex
ity
(e.g
. tec
hnol
ogie
s or
exp
erti
se n
eede
d)A
fford
abili
ty c
onsi
dera
tion
sC
ultu
ral a
ccep
tabi
lity
(soc
ial n
orm
s,
belie
fs)
Fisc
al m
easu
res:
Car
eful
us
e of
tax
es a
nd s
ubsid
ies
to p
rom
ote
heal
thie
r di
ets
Who
le p
opul
atio
n be
nefit
s fr
om a
ppro
pria
te fi
scal
pol
icie
s, w
ith a
gra
ded
soci
oeco
nom
ic
effe
ct (
bigg
er im
pact
on
poor
er
grou
ps).
Sele
ctiv
e ap
plic
atio
n of
fisc
al m
easu
res
to
help
the
poo
r re
quire
spe
cific
exp
ertis
e fr
om in
tern
atio
nal a
genc
ies,
e.g.
the
regi
onal
de
velo
pmen
t ba
nks.
Tech
nica
l sup
port
from
Reg
iona
l Offi
ce t
o he
lp c
ount
ries
impl
emen
t ta
xes.
For
taxe
s on
hig
h fa
t an
d/or
sug
ar fo
ods,
idea
lly c
ondu
ct m
odel
ling
exer
cise
s to
ca
refu
lly d
esig
n ap
prop
riate
tax
es t
o av
oid
unin
tend
ed e
ffect
s (e
.g. in
crea
sed
salt
inta
kes)
. Car
eful
ana
lyse
s ha
ve s
ugge
sted
a
simpl
er a
ppro
ach
is to
use
a c
omm
odity
ap
proa
ch, i.
e. o
n th
e ve
geta
ble
oils
and
fats
or
tot
al fr
ee s
ugar
inpu
t to
the
indu
stry
, ra
ther
tha
n a
reta
il pr
oduc
t ba
sis w
hich
is
mor
e co
mpl
icat
ed in
cou
ntrie
s w
ithou
t ex
istin
g sa
les
taxe
s.Te
chni
cal s
uppo
rt fr
om t
he R
egio
nal O
ffice
to
ada
pt t
he n
utrie
nt p
rofil
e m
odel
to
use
for
taxe
s.
App
ropr
iate
tax
es c
an g
ener
ate
reve
nue
and
prov
ide
grea
ter
flexi
bilit
y fo
r ot
her
gove
rnm
ent
spen
ding
.R
emov
ing
exist
ing
subs
idie
s on
fats
/oi
ls an
d su
gars
can
rem
ove
a m
ajor
bu
rden
on
natio
nal fi
nanc
es. S
ome
of t
he fi
nanc
ial g
ain
to g
over
nmen
t fin
ance
s ca
n be
sel
ectiv
ely
used
for
targ
etin
g th
roug
h ca
sh t
rans
fers
an
d ot
her
sche
mes
, e.g
. vou
cher
s fo
r po
orer
sec
tions
of t
he
com
mun
ity a
s al
read
y pr
opos
ed
by d
evel
opm
ent
bank
ana
lyse
s fo
r so
me
coun
trie
s in
the
Reg
ion.
Polit
ical
and
soc
ial a
ccep
tanc
e ca
n be
incr
ease
d by
pub
lic c
omm
itmen
t to
allo
cate
som
e of
the
tax
rev
enue
to
sup
port
hea
lth p
rom
otio
n/he
alth
se
rvic
es.
The
con
cept
of t
axat
ion
for
heal
th
purp
oses
is a
lread
y w
ell a
ccep
ted.
Som
e ta
xes
on s
ugar
-sw
eete
ned
beve
rage
ar
e al
read
y in
pla
ce, b
ut a
t lo
w le
vels.
C
onsid
er in
crea
sing
taxe
s pr
ogre
ssiv
ely
as
with
tob
acco
tax
.R
emov
al o
f foo
d su
bsid
ies
need
s ca
refu
l han
dlin
g po
litic
ally.
Pha
sed
impl
emen
tatio
n m
ay b
e ne
eded
and
m
easu
res
to m
itiga
te t
he im
pact
on
low
er
soci
oeco
nom
ic g
roup
s by
rep
laci
ng w
ith
appr
opria
te c
ash
tran
sfer
s.
Annex 4

74
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 4
. Fe
asib
ility
con
side
rati
ons
for
impl
emen
ting
str
ateg
ic i
nter
vent
ions
in
10
prio
rity
are
as fo
r ac
tion
to
prev
ent
obes
ity
and
diab
etes
in t
he E
aste
rn
Med
iter
rane
an R
egio
n Pr
iori
ty a
rea
for
acti
onR
each
(ca
paci
ty t
o de
liver
an
inte
rven
tion
to
the
targ
et
popu
lati
on)
Tech
nica
l com
plex
ity
(e.g
. tec
hnol
ogie
s or
exp
erti
se n
eede
d)A
fford
abili
ty c
onsi
dera
tion
sC
ultu
ral a
ccep
tabi
lity
(soc
ial n
orm
s,
belie
fs)
Publ
ic p
rocu
rem
ent:
Proc
urem
ent
and
prov
ision
of h
ealth
y fo
od
in p
ublic
inst
itutio
ns (
e.g.
sc
hool
s, un
iver
sitie
s, ho
spita
ls, m
ilitar
y, pr
isons
, ot
her
gove
rnm
ent
inst
itutio
ns)
Rea
ch is
con
sider
able
, but
will
depe
nd o
n pr
opor
tion
of m
eals
eate
n in
pub
lic s
ecto
r fa
cilit
ies.
Will
requ
ire c
apac
ity b
uild
ing
of t
hose
in
volv
ed in
pro
cure
men
t an
d ca
terin
g.
Ass
essm
ents
of b
udge
t im
plic
atio
ns w
ill be
req
uire
d, a
long
with
adv
ice
on t
he
prep
arat
ion
of n
utrit
iona
lly a
ppro
pria
te
mea
ls w
ithou
t su
bsta
ntia
l cos
t in
crea
ses.
The
re h
ave
been
con
cern
s th
at im
plem
entin
g he
alth
y fo
od
proc
urem
ent
or n
utrit
ion
stan
dard
s m
ight
incr
ease
the
cos
ts o
f pub
lic
sect
or fo
od, w
heth
er b
ecau
se
of h
ighe
r co
sts
of fr
esh
and/
or
who
le fo
ods
or a
nee
d fo
r m
ore
equi
pmen
t an
d/or
mor
e sk
illed
staf
f. Ef
fect
ive
stra
tegi
es t
o m
inim
ize
the
inve
stm
ent
need
ed in
clud
e (a
) co
llabo
ratio
n w
ith fo
od
who
lesa
lers
, man
ufac
ture
rs a
nd
cate
rers
to
impr
ove
the
nutr
ition
al
qual
ity o
f pro
duct
s, (b
) pa
rtne
rshi
ps
betw
een
publ
ic in
stitu
tions
to
harn
ess
thei
r co
llect
ive
barg
aini
ng
pow
er a
nd (
c) r
igor
ous
over
sight
of
con
trac
t ca
tere
rs’ c
harg
es
(42,
46,4
7).
Emph
asis
on r
educ
ing
the
use
of o
ils a
nd s
ugar
s (in
add
ition
to
switc
hing
typ
es o
f oil
used
) sh
ould
le
ad t
o co
st s
avin
gs.
The
se m
easu
res
will
crea
te n
ew
dem
and
for
heal
thy
food
s an
d w
ill,
with
the
ir in
crea
sed
scal
e, o
ften
resu
lt in
pric
e re
duct
ions
.
Dra
mat
ic c
hang
es in
soc
ieta
l foo
d pa
tter
ns h
ave
occu
rred
thr
ough
out
the
Reg
ion
over
the
pas
t 10
–20
year
s. Ye
t re
sista
nce
to t
hese
pro
pose
d ch
ange
s is
likel
y un
less
acc
ompa
nied
by
a cl
ear
publ
ic a
war
enes
s ca
mpa
ign
to e
xpla
in
the
impo
rtan
ce o
f the
se m
easu
res
for
redu
cing
the
risk
of d
iabe
tes
and
obes
ity.
The
re is
pot
entia
l for
coh
eren
ce w
ith
sust
aina
bilit
y an
d ec
onom
ic o
bjec
tives
. T
his
will
depe
nd o
n th
e pa
rtic
ular
food
en
viro
nmen
t/co
ntex
t.Pu
blic
-fund
ed fo
od is
ofte
n a
sour
ce o
f pr
ofit
for
cate
ring
cont
ract
ors,
who
may
sh
ow r
esist
ance
to
chan
ge e
spec
ially
if
ther
e is
a pe
rcei
ved
thre
at t
o pr
ofit
mar
gins
. How
ever
, alte
rnat
ive
cate
ring
sour
ces
shou
ld b
e co
nsid
ered
as
wel
l as
, in s
ome
coun
trie
s, th
e po
ssib
ility
of s
ettin
g up
sel
ectiv
e in
itiat
ives
to
purc
hase
food
s fr
om lo
cal f
arm
ers.
The
re
is su
bsta
ntia
l int
erna
tiona
l exp
erie
nce
that
thi
s ca
n be
ver
y ef
fect
ive
and
lead
to
com
mun
ity e
ngag
emen
t, w
ith
loca
l far
mer
s pr
ofitin
g fr
om t
hese
de
velo
pmen
ts.

75
Annex 4
Ann
ex 4
. Fe
asib
ility
con
side
rati
ons
for
impl
emen
ting
str
ateg
ic i
nter
vent
ions
in
10
prio
rity
are
as fo
r ac
tion
to
prev
ent
obes
ity
and
diab
etes
in t
he E
aste
rn
Med
iter
rane
an R
egio
n Pr
iori
ty a
rea
for
acti
onR
each
(ca
paci
ty t
o de
liver
an
inte
rven
tion
to
the
targ
et
popu
lati
on)
Tech
nica
l com
plex
ity
(e.g
. tec
hnol
ogie
s or
exp
erti
se n
eede
d)A
fford
abili
ty c
onsi
dera
tion
sC
ultu
ral a
ccep
tabi
lity
(soc
ial n
orm
s,
belie
fs)
Phys
ical
act
ivity
: Im
plem
ent
polic
ies,
legi
slatio
n an
d in
terv
entio
ns t
o pr
omot
e an
d fa
cilit
ate
heal
th
enha
ncin
g ph
ysic
al a
ctiv
ity
The
re is
pot
entia
l to
reac
h th
e w
hole
pop
ulat
ion,
par
ticul
arly
th
roug
h in
terv
entio
ns o
n ur
ban
plan
ning
and
impr
ovin
g ac
cess
to
phys
ical
act
ivity
opp
ortu
nitie
s.
Polic
y ex
pert
ise in
diff
eren
t ar
eas
will
be
need
ed, s
uch
as e
duca
tion,
urb
an p
lann
ing,
co
mm
unity
org
aniz
atio
n an
d sp
ort.
Som
e of
the
inte
rven
tions
m
ay r
equi
re c
apita
l inv
estm
ent
(par
ticul
arly
in r
elat
ion
to t
rans
port
an
d ur
ban
plan
ning
) an
d w
ill ta
ke
time
to e
nact
, but
the
res
ultin
g im
pact
sho
uld
be s
usta
inab
le
and
the
bene
fits
long
-last
ing.
In
addi
tion,
the
ben
efits
are
like
ly t
o ex
tend
wel
l bey
ond
obes
ity a
nd
diab
etes
pre
vent
ion.
Tra
nspo
rt a
nd
plan
ning
pol
icie
s m
ay g
ener
ate
envi
ronm
enta
l ben
efits
, incl
udin
g im
prov
ing
heal
th o
utco
mes
thr
ough
cl
eane
r ai
r. Ph
ysic
al e
duca
tion
and
scho
ol-b
ased
inte
rven
tions
may
re
ap b
road
er s
ocia
l and
aca
dem
ic
rew
ards
(50
).
Car
eful
des
ign
of in
terv
entio
ns is
nee
ded
to e
nsur
e th
at t
hey
faci
litat
e in
crea
sed
phys
ical
act
ivity
for
all. S
pace
s an
d fa
cilit
ies
that
are
saf
e an
d ap
prop
riate
for
wom
en
are
esse
ntia
l. Fac
ilitie
s an
d pr
ogra
mm
es
shou
ld a
lso a
ddre
ss t
he s
peci
fic n
eeds
of
peop
le w
ith d
isabi
litie
s.T
he p
oten
tial s
yner
gies
with
en
viro
nmen
tal a
nd s
usta
inab
ility
obje
ctiv
es s
houl
d be
em
phas
ised
in o
rder
to
bui
ld p
ublic
sup
port
.

76
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 4
. Fe
asib
ility
con
side
rati
ons
for
impl
emen
ting
str
ateg
ic i
nter
vent
ions
in
10
prio
rity
are
as fo
r ac
tion
to
prev
ent
obes
ity
and
diab
etes
in t
he E
aste
rn
Med
iter
rane
an R
egio
n Pr
iori
ty a
rea
for
acti
onR
each
(ca
paci
ty t
o de
liver
an
inte
rven
tion
to
the
targ
et
popu
lati
on)
Tech
nica
l com
plex
ity
(e.g
. tec
hnol
ogie
s or
exp
erti
se n
eede
d)A
fford
abili
ty c
onsi
dera
tion
sC
ultu
ral a
ccep
tabi
lity
(soc
ial n
orm
s,
belie
fs)
Food
sup
ply
and
trad
e:
Use
food
sta
ndar
ds, le
gal
inst
rum
ents
and
oth
er
appr
oach
es t
o im
prov
e th
e na
tiona
l and
/or
loca
l fo
od s
uppl
y in
thi
s R
egio
n of
net
food
-impo
rtin
g co
untr
ies
Any
tra
de m
easu
res
have
po
tent
ial f
or u
nive
rsal
rea
ch
if im
port
ed fo
ods
mak
e up
a
subs
tant
ial p
ropo
rtio
n of
the
na
tiona
l foo
d su
pply.
City
- or
mun
icip
ality
-bas
ed
inte
rven
tions
cou
ld r
each
a
subs
tant
ial p
ropo
rtio
n of
the
po
pula
tion
in t
hese
loca
litie
s.
Inte
rnat
iona
l tra
de a
nd le
gal e
xper
tise
is re
quire
d to
des
ign
appr
opria
te t
ools,
w
ithin
the
con
stra
ints
of c
urre
nt W
orld
Tr
ade
Org
aniz
atio
n (W
TO)
and
othe
r tr
ade
agre
emen
ts, t
o re
duce
the
vol
ume
of im
port
s of
fats
and
sug
ars.
The
det
aile
d ca
se o
f the
mag
nitu
de o
f the
obe
sity
and
diab
etes
pro
blem
in t
he R
egio
n m
ay n
eed
to b
e m
ade
for
a pu
blic
hea
lth e
xem
ptio
n to
just
ify t
hese
mea
sure
s w
ithin
WTO
rul
es
(invo
king
the
SPS
sub
-cla
uses
). H
owev
er if
re
stric
tions
are
not
disc
rimin
ator
y be
caus
e do
mes
tic s
uppl
y an
d im
port
s ar
e bo
th
rest
ricte
d, t
hen
appl
ying
con
siste
ncy
to
dom
estic
food
sup
ply
as w
ell a
s im
port
s is
legi
timat
e an
d m
inim
izes
disp
utes
with
in a
W
TO c
onte
xt.
As
part
of a
pac
kage
with
ref
orm
ulat
ion
effo
rts,
tech
nica
l exp
ertis
e w
ill be
pro
vide
d to
the
food
indu
stry
to
cut
the
leve
ls of
fa
ts/s
ugar
s an
d/or
rep
lace
with
hea
lthie
r in
gred
ient
s (f
ruit
and
vege
tabl
es, p
ulse
s, co
mpl
ex c
arbo
hydr
ates
).
Thi
s w
ill de
pend
on
the
prec
ise
inst
rum
ents
use
d. Im
port
dut
ies
will
gene
rate
pub
lic r
even
ue, w
hile
tr
ade
rest
rictio
ns w
ill no
t.
Phas
ed r
educ
tions
, sup
port
ed w
ith
advo
cacy
, will
help
with
pub
lic a
ccep
tanc
e an
d in
dust
rial a
dapt
atio
n. L
ocal
food
in
itiat
ives
can
com
bine
hea
lth, e
cono
mic
an
d su
stai
nabi
lity
obje
ctiv
es, w
hich
ca
n he
lp t
o ge
nera
te a
bro
ad b
ase
of
supp
ort.
Ref
orm
ulat
ion:
Impl
emen
t a
gove
rnm
ent-
led
prog
ram
me
of p
rogr
essiv
e re
form
ulat
ion,
ada
pted
to
the
nat
iona
l con
text
, to
elim
inat
e tr
ans
fats
an
d re
duce
pro
gres
sivel
y to
tal a
nd s
atur
ated
fat,
salt,
sug
ars,
ener
gy a
nd
port
ion
size.
Rea
ch d
epen
ds o
n th
e sp
ecifi
cs
of t
he n
atio
nal f
ood
supp
ly, i.
e.
how
and
whe
re t
he in
gred
ient
s/nu
trie
nts
ente
r fo
od (
impo
rts,
loca
l pro
duct
ion
or in
the
ho
me)
.
Tech
nica
l sup
port
/exp
ertis
e w
ill be
nee
ded
to c
ondu
ct in
itial
ana
lyse
s to
des
ign
a re
form
ulat
ion
prog
ram
me
appr
opria
te t
o th
e na
tiona
l foo
d en
viro
nmen
t. A
det
aile
d un
ders
tand
ing
of t
he n
atio
nal f
ood
chai
n is
requ
ired
to d
esig
n an
effe
ctiv
e pr
ogra
mm
e.Fo
od p
rodu
cers
/pro
vide
rs w
ill re
quire
te
chni
cal s
uppo
rt t
o m
ake
the
chan
ges.
Phas
ed a
nd p
rogr
essiv
e nu
trie
nt/
ingr
edie
nt c
hang
es a
re w
ell t
oler
ated
, pr
ovid
ed t
hat
they
are
uni
vers
ally
app
lied
acro
ss fo
od c
ateg
orie
s. N
on-
com
plia
nt
com
pani
es c
an li
mit
the
effe
ctiv
enes
s of
na
tiona
l mea
sure
s. T
hese
des
ired
chan
ges
are
ther
efor
e be
st m
anda
ted
as s
tand
ards
th
at a
re c
hang
ed e
very
1–2
yea
rs a
s th
e lim
its o
n th
e un
desir
able
nut
rient
s/in
gred
ient
s ar
e re
duce
d pr
ogre
ssiv
ely.

77
Annex 4
Ann
ex 4
. Fe
asib
ility
con
side
rati
ons
for
impl
emen
ting
str
ateg
ic i
nter
vent
ions
in
10
prio
rity
are
as fo
r ac
tion
to
prev
ent
obes
ity
and
diab
etes
in t
he E
aste
rn
Med
iter
rane
an R
egio
n Pr
iori
ty a
rea
for
acti
onR
each
(ca
paci
ty t
o de
liver
an
inte
rven
tion
to
the
targ
et
popu
lati
on)
Tech
nica
l com
plex
ity
(e.g
. tec
hnol
ogie
s or
exp
erti
se n
eede
d)A
fford
abili
ty c
onsi
dera
tion
sC
ultu
ral a
ccep
tabi
lity
(soc
ial n
orm
s,
belie
fs)
Mar
ketin
g: Im
plem
ent
appr
opria
te r
estr
ictio
ns
on m
arke
ting
(incl
udin
g pr
ice
prom
otio
ns)
of
food
s hi
gh in
fat,
suga
r an
d sa
lt.
A c
ompr
ehen
sive
appr
oach
(m
edia
, aud
ienc
e, t
ype
of
mar
ketin
g) is
req
uire
d to
hav
e su
bsta
ntia
l im
pact
.T
here
is p
oten
tial t
o re
ach
a la
rge
prop
ortio
n of
the
reg
iona
l po
pula
tion
give
n th
e do
min
ance
of
cro
ss-b
orde
r m
edia
.T
here
is p
oten
tial f
or t
otal
co
vera
ge if
res
tric
tions
are
ex
tend
ed t
o m
arke
ting
to t
he
who
le p
opul
atio
n (a
s is
curr
ently
do
ne in
one
cou
ntry
in t
he
Reg
ion)
. In
view
of t
he R
egio
n’s
youn
g po
pula
tion
and
the
maj
or
heal
th a
nd s
ocie
tal c
osts
of
obes
ity, d
iabe
tes
and
the
othe
r N
CD
s in
adu
lts, t
here
is m
erit
in r
estr
ictin
g m
arke
ting
of fo
ods
high
in fa
t or
sal
t or
sug
ar fo
r th
e w
hole
of s
ocie
ty.
Ado
ptio
n of
the
reg
iona
l nu
trie
nt p
rofil
e m
odel
ens
ures
w
ides
prea
d ap
plic
atio
n of
re
stric
tions
to
unhe
alth
y fo
ods.
Onl
y re
gula
tory
mea
sure
s to
re
stric
t pr
ice
prom
otio
ns o
n hi
gh fa
t/su
gar
food
s w
ill pe
rmit
com
plet
e co
vera
ge, p
artic
ular
ly
in p
oore
r ar
eas.
Mea
sure
s fo
r m
onito
ring
and
enfo
rcem
ent
are
an im
port
ant
chal
leng
e fo
r th
e R
egio
n.
Spec
ialis
t le
gal a
nd m
edia
exp
ertis
e is
requ
ired
from
the
beg
inni
ng o
f the
le
gisla
tive
proc
ess.
Giv
en t
he c
onsis
tent
Reg
ion-
wid
e co
nseq
uenc
es o
f the
se is
sues
, a h
uman
rig
hts-
base
d ap
proa
ch t
o re
gula
tion
in
this
area
sho
uld
be t
aken
, suc
h th
at a
ctio
n is
unde
rsto
od a
s ne
cess
ary
to p
rom
ote,
re
spec
t an
d fu
lfil t
he r
ight
to
heal
th in
the
R
egio
n, e
spec
ially
the
chi
ld’s
right
to
heal
th.
The
lega
l bas
is is
the
com
mon
obl
igat
ions
of
tho
se c
ount
ries
in t
he R
egio
n th
at a
re
stat
e pa
rtie
s to
the
Inte
rnat
iona
l Cov
enan
t on
Eco
nom
ic, S
ocia
l and
Cul
tura
l Rig
hts.
On
this
hum
an r
ight
s un
ders
tand
ing,
the
UN
Gui
ding
Prin
cipl
es o
n Bu
sines
s an
d H
uman
Rig
hts,
and
the
Maa
stric
ht P
rinci
ples
on
the
Ext
rate
rrito
rial O
blig
atio
ns o
f St
ates
in t
he A
rea
of E
cono
mic
, Soc
ial a
nd
Cul
tura
l Rig
hts
prov
ide
guid
elin
es o
n ho
w
to d
eal w
ith t
he c
ompl
ex c
ross
-bor
der
issue
s in
volv
ed in
suc
cess
fully
res
tric
ting
inap
prop
riate
mar
ketin
g ac
ross
the
Reg
ion.
Cou
ntry
-spe
cific
ana
lyse
s on
the
de
mog
raph
ic p
rofil
e an
d m
arke
ting
expo
sure
of c
hild
ren
and
adol
esce
nts
are
need
ed.
Tech
nica
l sup
port
from
the
Reg
iona
l Offi
ce
may
be
need
ed t
o im
plem
ent
the
nutr
ient
pr
ofile
mod
el a
nd t
o ad
apt
it fo
r va
rious
us
es.
Prim
ary
cost
s fo
r go
vern
men
t im
plem
enta
tion
are
mod
est.
The
re a
re m
ajor
impl
icat
ions
for
med
ia
and
othe
r or
gani
zatio
ns d
epen
dent
on
the
curr
ent
inte
nsiv
e m
arke
ting
of fo
ods
high
in fa
t or
sal
t or
sug
ar; t
his
requ
ires
maj
or h
igh-
leve
l pol
itica
l com
mitm
ent
and
sust
aine
d ad
voca
cy.
A p
relim
inar
y st
udy
to d
ocum
ent
the
exte
nt a
nd n
atur
e of
pric
e pr
omot
ions
in
the
Reg
ion
wou
ld b
e he
lpfu
l to
build
po
litic
al a
ccep
tabi
lity.
Prio
r aw
aren
ess-
raisi
ng c
ampa
igns
to
enh
ance
pub
lic u
nder
stan
ding
of
the
harm
ful e
ffect
s of
cur
rent
pric
e pr
omot
ions
on
food
s hi
gh in
fat
or s
alt
or
suga
r w
ill pr
obab
ly b
e ne
eded
to
impr
ove
the
publ
ic a
nd p
oliti
cal a
ccep
tabi
lity
of
thes
e ch
ange
s.

78
Proposed policy priorities for preventing obesity and diabetes
Ann
ex 4
. Fe
asib
ility
con
side
rati
ons
for
impl
emen
ting
str
ateg
ic i
nter
vent
ions
in
10
prio
rity
are
as fo
r ac
tion
to
prev
ent
obes
ity
and
diab
etes
in t
he E
aste
rn
Med
iter
rane
an R
egio
n Pr
iori
ty a
rea
for
acti
onR
each
(ca
paci
ty t
o de
liver
an
inte
rven
tion
to
the
targ
et
popu
lati
on)
Tech
nica
l com
plex
ity
(e.g
. tec
hnol
ogie
s or
exp
erti
se n
eede
d)A
fford
abili
ty c
onsi
dera
tion
sC
ultu
ral a
ccep
tabi
lity
(soc
ial n
orm
s,
belie
fs)
Labe
lling:
Impl
emen
t or
rev
ise s
tand
ards
for
nutr
ition
labe
lling
to
incl
ude
fron
t-of
-pac
k la
bellin
g fo
r al
l pre
-pa
ckag
ed fo
ods
The
rea
ch o
f the
pro
gram
me
will
be v
ery
depe
nden
t on
the
pr
opor
tion
of n
atio
nal d
iet
deriv
ed fr
om p
re-p
acka
ged
food
.
The
food
indu
stry
will
requ
ire t
echn
ical
su
ppor
t to
impl
emen
t th
e st
anda
rds.
Phas
ed im
plem
enta
tion
(e.g
. ove
r a
two-
year
per
iod)
to
min
imize
the
co
sts
to in
dust
ry w
ill be
impo
rtan
t.In
vest
men
t in
tra
inin
g of
sta
ff in
volv
ed in
reg
ulat
ion
and
insp
ectio
n of
food
s w
ill be
nee
ded.
The
gro
win
g ac
cept
ance
of h
ealth
m
essa
ges
and
rapi
d ex
pans
ion
of a
cces
s to
diff
eren
t fo
rms
of m
edia
pre
sent
an
oppo
rtun
ity t
o co
mm
unic
ate
mes
sage
s to
ac
com
pany
and
exp
lain
labe
lling.
Brea
stfe
edin
g: Im
plem
ent
a pa
ckag
e of
pol
icie
s an
d in
terv
entio
ns t
o pr
omot
e,
prot
ect
and
supp
ort
brea
stfe
edin
g
Full
capa
city
can
be
reac
hed
in
polit
ical
ly s
tabl
e co
ntex
ts.
(All
effo
rts
to p
rom
ote
prot
ect
and
supp
ort
brea
stfe
edin
g sh
ould
also
be
mad
e in
con
flict
sit
uatio
ns.)
Lega
l exp
ertis
e is
need
ed t
o im
plem
ent
the
Inte
rnat
iona
l Cod
e, t
he G
uida
nce
and
mat
erni
ty le
gisla
tion.
Cap
acity
to
mon
itor
and
enfo
rce
legi
slatio
n is
cruc
ial.
Publ
ic a
nd p
rivat
e se
ctor
(em
ploy
er)
enga
gem
ent
is re
quire
d to
intr
oduc
e m
ater
nity
pro
tect
ion
for
wom
en.
Subs
tant
ial i
nves
tmen
t is
requ
ired
part
icul
arly
for
mat
erni
ty
prot
ectio
n, d
epen
ding
on
the
prop
ortio
n of
wom
en w
orki
ng in
th
e fo
rmal
sec
tor.
Neg
ativ
e at
titud
es t
o br
east
feed
ing
amon
g yo
ung
wom
en, e
spec
ially
in
high
-inco
me
coun
trie
s, ne
ed t
o be
tr
ansf
orm
ed.
The
re is
gro
win
g cu
ltura
l acc
epta
nce
of t
he n
eed
for
paid
mat
erni
ty le
ave
alre
ady
in e
vide
nce
in t
he R
egio
n an
d on
e co
untr
y (M
oroc
co)
has
ratifi
ed t
he
rele
vant
ILO
Con
vent
ion
(ILO
Mat
erni
ty
Prot
ectio
n C
onve
ntio
n 20
00, N
o 18
3).
Mas
s M
edia
Cam
paig
n:
Mas
s m
edia
cam
paig
ns o
n he
alth
y di
et a
nd p
hysic
al
activ
ity.
The
ext
ent
of r
each
dep
ends
on
the
desig
n of
cam
paig
ns, w
hich
ne
ed t
o be
tar
gete
d an
d ad
apte
d fo
r di
ffere
nt a
udie
nces
.
Expe
rt u
nder
stan
ding
of s
ocie
tal a
ttitu
des
and
com
mun
icat
ion
tech
niqu
es is
req
uire
d.D
etai
led
eval
uatio
n an
d m
essa
ge a
dapt
atio
n ar
e fr
eque
ntly
req
uire
d to
sus
tain
cam
paig
ns
Maj
or r
epea
ted
annu
al
com
mitm
ent
is ne
cess
ary
to
coun
ter
perv
asiv
e in
dust
rial
mar
ketin
g in
the
Reg
ion.
Cam
paig
ns m
ust
be c
ultu
rally
app
ropr
iate
in
ord
er t
o be
effe
ctiv
e.
Hea
lth S
ecto
r Act
ion:
H
arne
ss t
he h
ealth
sec
tor
to e
nabl
e ch
ange
and
to
pro
vide
lead
ersh
ip
on g
over
nanc
e an
d ac
coun
tabi
lity
The
re is
pot
entia
l to
reac
h fu
ture
ge
nera
tions
thr
ough
cou
nsel
ling
to p
rosp
ectiv
e pa
rent
s; pr
imar
y-ca
re b
ased
cou
nsel
ling
and
com
mun
ity-b
ased
inte
rven
tions
w
ould
be
mor
e ta
rget
ed a
t hi
gh-
risk
grou
ps.
The
effe
ctiv
enes
s an
d th
e co
st–e
ffect
iven
ess
of t
he h
ealth
-ser
vice
bas
ed in
terv
entio
ns
(ant
enat
al c
ouns
ellin
g, pr
imar
y-ca
re b
ased
co
unse
lling
and
scre
enin
g) w
ill de
pend
on
exte
nt a
nd e
ase
of a
cces
s to
prim
ary
care
. Sp
ecifi
c tr
aini
ng o
f hea
lth p
rofe
ssio
nals
will
also
be
requ
ired.
The
affo
rdab
ility
of t
he h
ealth
-se
rvic
e re
late
d in
terv
entio
ns is
al
so r
elat
ed t
o th
e cu
rren
t st
ate
of
prim
ary
care
pro
visio
n an
d he
alth
sy
stem
fina
ncin
g.
Mul
tisec
tora
l coo
rdin
atio
n an
d ac
coun
tabi
lity
are
heav
ily d
epen
dent
on
succ
essf
ully
con
vinc
ing
polic
y-m
aker
s ou
tsid
e th
e he
alth
dom
ain
that
the
ir po
licy
area
s ar
e im
port
ant
for
heal
th a
nd
that
thi
s w
ill tr
ansla
te t
o br
oade
r so
cial
an
d ec
onom
ic g
ains
.




There is an alarming and escalating burden of overweight, obesity and diabetes in the Eastern Mediterranean Region, closely linked to changing dietary patterns. Obesity and the most common type of diabetes are largely preventable and urgent action is needed to reduce exposure to their causal factors, such as unhealthy diet and physical inactivity. This document takes into account the recommendations of several recent initiatives on the prevention of obesity and diabetes and identifies priorities for an approach to reduce exposure to unhealthy dietary risk factors. It presents an initial proposal for 10 priority areas for action, which cover 37 strategic interventions to help prevent overweight, obesity and diabetes in the whole population, including children, adolescents and adults.