Program Report - Cabrini Ministries Swaziland
64
Program Report 2012-2013 (01 October 2012 – 30 September 2013)
Transcript of Program Report - Cabrini Ministries Swaziland

Program Report
2012-2013
(01 October 2012 – 30 September 2013)

A special thanks to our funders:
Anonymous Donors, Bonino Foundation, Bristol-Myers Squibb Foundation, Cabrini
College, Cabrini Health Australia, Cabrini Mission Foundation, Centers for Disease
Control and Prevention, ELMA Foundation, ICAP (Columbia University),
Missionary Sisters of the Sacred Heart, PACT, PEPFAR (US Government),
SAFAIDS, Sahee Foundation, Solon Foundation, United States Agency for
International Development, and individual donors worldwide.

Cabrini Ministries Program Report // 2012-2013
3
TABLE OF CONTENTS
1. Letter from Executive Director .......................................................................................... 4
2. Letter from Deputy Executive Director ............................................................................. 5
3. Executive Summary ........................................................................................................... 6
4. Organization information ................................................................................................... 7
History.................................................................................................................................... 7
Vision / Mission / Values ....................................................................................................... 9
Staff and Leadership .............................................................................................................. 9
5. Situation in Swaziland ..................................................................................................... 11
6. Programmatic Overview .................................................................................................. 13
Health Care .......................................................................................................................... 14
Service Delivery............................................................................................................... 14
Program Impact ................................................................................................................ 22
Key Accomplishments .................................................................................................... 23
Strategic Partnerships....................................................................................................... 25
Child Care ............................................................................................................................ 27
Assessments ..................................................................................................................... 27
Service Delivery............................................................................................................... 27
Program Impact ................................................................................................................ 32
Key Accomplishments ..................................................................................................... 33
Strategic Partnerships....................................................................................................... 36
Social Services ..................................................................................................................... 36
Program Development ..................................................................................................... 37
Service Delivery............................................................................................................... 38
Impact and Expansion ...................................................................................................... 39
Agriculture ........................................................................................................................... 40
Food Security Programming ............................................................................................ 40
Program Transition .......................................................................................................... 40
7. Monitoring and Evaluation systems................................................................................. 41
8. Organizational Development ........................................................................................... 43
Identified Emerging Issues .................................................................................................. 43
Strategic Priorities ................................................................................................................ 46
Becoming a “Social Service Organization” ......................................................................... 47
Future Projects ..................................................................................................................... 48
9. Get involved ..................................................................................................................... 50
10. Appendices .................................................................................................................... 51
Cabrini Health Care Analysis of Services ........................................................................... 52
Clinical Cascade Results and Exits ...................................................................................... 56
Cabrini Impact Mitigation Analysis of Services .................................................................. 57
Cabrini Ministries Program Report // 2012-2013
4
1. LETTER FROM EXECUTIVE DIRECTOR
Dear Friends of Cabrini Ministries,
I greet you with joy from the Lubombo Lowveld of Swaziland.
It is truly a year of joy for the people of this region because this
summer we are experiencing rain – lots of life giving rain. For
those of you who are familiar with the 20 year drought this area
has endured, you know how important this is. The changes here
go deeper than the weather. Everywhere I look, I see the new
joy that accompanies lives being restored!
I also greet each of you with thanksgiving and gratitude for your prayers, interest and support
for the people of this area. As you read this report I am sure you will also give thanks with
me for the enormous work being done by this small faith-based and community-based
organization. You will see what your support, interest and prayer have wrought and where
you have brought this area over the last 10 years: from grave sickness, death, poverty and
abandonment, to life and hope for today and for the future.
In this last year, Cabrini Ministries has continued its work with the HIV/AIDS and TB
afflicted people of the area, as well as the orphaned and vulnerable children whom this great
pandemic has produced. Despite the daily struggles and real risks, we are moving from acute
care to chronic care as more people are alive and working. We are moving to more children
being able to live with their families and guardians due to the increasing stability of some
homesteads. We are moving from emergency support to once again dreaming about what the
future can hold. Your support this year has also allowed us to make a dream come true...a
new Social Service Department is now serving homesteads facing situations which Health
Care and Child Care have observed and reported, but have not been able to adequately
address. The family unit has truly become the center of our work.
God’s great love is poured out like a river in the desert and the desert has become a place of
life.
Many blessings to each of you.
Sr. Diane DalleMolle, MSC

Cabrini Ministries Program Report // 2012-2013
5
2. LETTER FROM DEPUTY EXECUTIVE DIRECTOR
My Dear Friends,
It’s been a great year of us working together to fulfill the mission of
Restoring Life and Rekindling Hope. It takes so many people to
make our work possible and we are deeply grateful to all of you for
your interest, prayers, donations and support. Without you our
Cabrini family here on the ground couldn’t continue this work of
love.
Cabrini Ministries in this past year realized our desire of opening a Social Service
Department. The impact of this movement is immense. As a Catholic faith-based
organization we continually think about how we can best serve and love the people in this
area with HIV/AIDS, TB and those impacted by these diseases. Our underlying framework
utilizing a psychosocial approach to care allows us to compliment the significant gains that
have been made in the scientific world regarding HIV. In Swaziland there has been a steady
upward trajectory in health care delivery. More people know their HIV status, more eligible
people are on treatment, and families and communities are starting to stabilize.
Despite all the scientific advances there are still a large number of families who lack the
necessary resources – physical, emotional, intellectual or spiritual – to adhere to treatment
regimens. Many factors converge to contribute to this challenge, including poverty,
education, and social beliefs. Our Social Service Department is able to assess the challenges
and barriers that families face in trying to manage adherence and the lack of governmental
social welfare supports. The interventions of the Social Service Department creates a safety
network to alleviate these struggles by providing food, health care, child protection, legal
assistance, and individualized human rights advocacy, to name just a few supports. As
families become stronger and more cohesive, they rely less on Cabrini Ministries’ help and
steadily move to a more independent functioning.
I am proud of the steady quality improvements in Cabrini Ministries over the years. The
most important factor in all of this is the staff at Cabrini Ministries, who each day grows in its
own capacity to love as Jesus loved and to know what it means to love.
United in this work of love,
Sr. Barbara Staley, MSC, LCSW

Cabrini Ministries Program Report // 2012-2013
6
3. EXECUTIVE SUMMARY
For over 40 years the Cabrini Sisters have been serving in Swaziland. During that time, their
work has always been driven by a connection to the community and a willingness to focus on
the most pressing needs. During the past decade, that work has been dedicated to helping
those people infected and affected by HIV/AIDS and Tuberculosis. This care delivery has
largely been carried out through Cabrini Ministries’ work in Health Care and Child Care.
The commitment to the community and its needs has never changed, yet this year represents a
significant period of transition for the organization. The work of Cabrini Ministries is
moving from crisis care to chronic care. The primary focus is still on keeping people alive
and ensuring that they are cared for, but now more people are able to think about
transitioning toward the future – a luxury many in the area haven’t had for over a decade.
The most concrete example of this transition is the recent formation of the Social Service
Department. Originally designed to address the community needs that exist between our
work in Health Care and Child Care, today the nascent department is providing a solid
framework for addressing the holistic needs of the community we serve.
In this report, you will read about the impact of the Social Service Department as well as the
on-going efforts of our existing departments. The programmatic year for Cabrini runs from
October 1st through September 30
th and this report seeks to draw together a detailed overview
of significant activity that has occurred in this period. It pulls from a variety of data sources
and reports to present a broad understanding of the organization and its impact.
While it is impossible to capture the breadth of what Cabrini does by simply looking at
statistics, the following figures provide a quick snapshot of what has happened this past year:
A total of 2,806 individuals received direct care from Cabrini
Our Health Care staff provided clinical services for 1,932 clients
o 872 HIV+ patients were given access to life-saving ARV medicine including
123 new initiations
o 89% of those initiated on ART were alive and on treatment one year later
874 Orphans and vulnerable children were served through Cabrini Child Care
o 151 of those received a full complement of comprehensive services
o 333 healthy child physicals were conducted at area schools
The Social Service Department assessed 1,067 individuals on 131 homesteads
o 177 interventions have already been initiated
In addition to the Social Service Department, several new initiatives have been
launched: a Medical Circumcision Clinic, on-site laboratory services, expanded
community health education, outreach academic enrichment, enhanced OVC
support groups and new strategic partnerships

Cabrini Ministries Program Report // 2012-2013
7
4. ORGANIZATION INFORMATION
Cabrini Ministries Swaziland is a Catholic
faith-based and community-based not-for-
profit organization (Section 21: R7/26820)
working in the Lubombo lowveld of Swaziland
to show God’s love in action through service.
Cabrini Ministries is based at St. Philip’s
Mission and operates for the good of the larger
community including the chiefdoms of Mamba,
Ngcamphalala, and Gamedze with recent
expansion into Shongwe, Mkweli and Nceka.
Our work is fundamentally about meeting the psychosocial needs of our community which
includes addressing issues of health, nutrition, education, and protection, as well as ensuring
mental and spiritual wellbeing. Service delivery is primarily achieved through three
integrated departments: Health Care, Child Care and Social Service. Individual interventions
are necessary, but can only be adequately assessed and understood in the context of family
and community. This contextual understanding of the people served by Cabrini is the core of
Cabrini Ministries’ effectiveness in responding to and providing for the many challenges
experienced by the people we serve.
History
Cabrini Ministries is founded on the work and principles of the Missionary Sisters of the
Sacred Heart (MSCs) and their founder, St. Francis Xavier Cabrini. The sisters have worked
in Swaziland for over 40 years after originally coming to the country at the request of King
Sobhuza II in 1971. For the first 25 years, the work at St. Philips Mission was focused on
education, basic health care, skills building and spiritual formation. By the early 1990s, the
Cabrini sisters were considering leaving the country because their work in community
development had yielded such positive results.
Unfortunately, as the millennium came to a close,
Swaziland was faced with a triple crisis of drought,
unemployment and – most damaging – the HIV
pandemic. In the span of less than a decade, an
entire generation of Swazis had been devastated and
the social fabric of the country began to unravel.
Bright young people who had been educated
through the hard work and sacrifice of their families
along with the support of the sisters were dying just
as their working lives were beginning. Families
were left without their children and consequently the
Sr. Anne Maria counsels a child
in the early 1980s

Cabrini Ministries Program Report // 2012-2013
8
social safety net they had expected to exist in their later years of life.
In 2002, in response to the crisis, a strategic decision was made to refocus the apostolic
mission of the Missionary Sisters of the Sacred Heart. All resources, human and financial,
were shifted to respond deliberately to the havoc caused by HIV and TB. With the support
and encouragement of the local leaders, a free hostel was established to care for orphans and
vulnerable children of the area. Initially, 50 children were enrolled, 98 showed up on the first
day and none were turned away. The work in health care moved from the clinic-based to
home care-based since most clients were simply too sick to travel. What started as
emergency palliative care eventually evolved into a systematic approach of educating,
testing, and linking to care. In 2006, Cabrini Ministries was officially incorporated as a
Swazi not-for-profit organization.
In recent years, the southern Lubombo region of Swaziland remains an area remarkably
underserved by care providers. The ongoing impact of HIV, along with the co-morbidity of
TB and the resulting number of parentless children is compounded by continued years of
drought and high unemployment. These realities intensify the problems already associated
with poverty, food insecurity, and low levels of education of the people living in these remote
rural chiefdoms.
Since its inception, Cabrini Ministries has established a strong track record demonstrating
creativity, determination and competency in responding to community needs. The
organization provides health care services of the highest quality to the people in the
catchment area and maintains on-going cooperative partnerships with families and neighbors
in the care and upbringing of children orphaned or vulnerable due to HIV/TB.
In the last decade, Cabrini has served over 6,000 people living with HIV and/or TB and
provided care to over 1,500 orphans and vulnerable children. What began as just a few
people doing what they could to help their neighbors has evolved into a full service
organization deeply rooted in the
community, providing
comprehensive integrated care as
well as targeted care to thousands
of others. In 2013, a Social
Service Department was launched
in order to better meet the multi-
faceted needs of the homesteads
receiving services from the
organization and to enhance the
quality of care provision.

Cabrini Ministries Program Report // 2012-2013
9
Vision / Mission / Values
VISION:
Restoring life…..kubuyisela imphilo
MISSION:
Sharing the love of Jesus Christ through
Health Care Services for HIV, AIDS and TB at the homesteads and access to health
care and supportive services for HIV, AIDS, and TB
Care of orphans, vulnerable children and extended families/guardians
Economic strengthening and skills development of local people through employment
VALUES:
Hope Kwetsemba
Mercy Sihawu
Passion Kutinikela
Quality Care Kunakekela ngelizinga lelisetulu
Staff and Leadership
Cabrini currently has 55 staff members and operates with the following service departments:
Health Care Outreach, Child Care and Social Services. They are supported by work in
Administrative Services, Maintenance, and Transportation. Of the current staff members
who are employed, all but five are African, with the vast majority coming from the catchment
area served by the organization.
Executive Team
The Executive Team of Cabrini is comprised of five staff members who are responsible for
decisions related to the day-to-day operations of the organization. The members are:
Sr. Diane Dalle Molle – Executive Director
Sr. Barbara Staley – Deputy Executive Director
Mr. Pius Mamba – Cultural Liaison
Mr. Bongani Khumalo – Director of Health Care Outreach
Mr. Mzamo Sikhondze – Director of Human Resources
Board of Directors
The official board of Cabrini Ministries is comprised of members of the Provincial Council of
the Stella Maris Province of the Missionary Sisters of the Sacred Heart of Jesus. However,
the duties of advisement and oversight of the organization have been delegated to a local
Swazi Board comprised of the following members:
Nathi Gumede (Chairperson)
Executive Director, Conciliation Mediation and Arbitration Commission

Cabrini Ministries Program Report // 2012-2013
10
Mavis Dlamini (Vice Chair)
Head Teacher, Duze High School
Langalakhe Dlamini (Head of Finance Committee)
Finance Manager, Swaziland National Provident Fund
Khosi Mthethwa
Health Systems Advisor, WHO
Mary Da Silva
Coordinator, Swaziland Democracy Campaign
Zee Musuku, MSW
Social Welfare Advisor, Health Finance and Government
Cabrini Children perform traditional Swazi Dance.

Cabrini Ministries Program Report // 2012-2013
11
5. SITUATION IN SWAZILAND
Swaziland is a small land-locked country in Southern Africa extending roughly 175 by 135
kilometers (110 by 85 miles) and having a population of approximately 1.1 million. The
country is considered to be Africa’s last true monarchy with King Mswati III ruling the
country.
By technical definition, Swaziland is a middle-income country with a per capita income of
$5,246.1 However, 63% of the population lives on less than $2/day with 37% living on less
than $1/day.2 This illustrates the significant gap between the rich and poor in this small
country. The poorest 20% of the population account for only 1.4% of the national
consumption and Swaziland as a whole consistently ranks as one of the 25 worst countries in
the world for income inequality.3 The unemployment rate has risen in the last five years and
currently stands at 66.3% with even higher rates in the rural areas.4
The health situation in Swaziland is
even worse. The country holds the
unfortunate distinction of leading the
world in HIV rates as well as
incidence of Tuberculosis. According
to a recent national survey, 31% of
Swazis ages 18-49 are infected with
HIV and every year 2.38% of
previously uninfected people will
contract the disease.5 Swaziland
yearly has 1,350 new cases of TB for
every 100,000 people; compare that
to the world average of 122.6
While the deadly diseases of HIV and TB receive the most attention, Swaziland’s health and
sanitation systems face challenges as well. Even though basic health services are available
for most of the population, the country has an infant mortality rate of 7.9% and an under-five
mortality rate of 10.4%.7 One in ten children born in Swaziland won’t live to see their sixth
birthday. Only 53.8% of Swazis have access to adequate sanitation facilities and in the rural
areas of the country, 40% lack access to adequate drinking water sources.8
1 World Bank, 2012. Swaziland is ranked 112 out of 180 when adjusting for Purchasing Power Parity.
2 Swaziland MDG Progress Report, 2012.
3 Based on GINI coefficient.
4 Swaziland MDG Progress Report, 2012.
5 SHIMS Report, Columbia Univeristy.
6 WHO Global TB Report, 2013. Other rates for reference include: Africa as a whole – 220, Australia – 6,
United States – 4, Europe – 5. 7 Swaziland MDG Progress Report, 2012.
8 MICS Survey, 2011.

Cabrini Ministries Program Report // 2012-2013
12
Recent statistics paint a worrying social
picture as well. The HIV crisis has
overwhelmed the social safety net of the
country with a significant amount of children
becoming orphaned or vulnerable in a short
period of time. This, coupled with the lack of
wage earners, makes for a dangerous
situation. Currently, 45.1% of Swazi children
are officially classified as orphaned or
vulnerable. Of these children, 38% do not
have their basic needs met.9 Less than one in
four children live with both their biological parents. Protections that are considered basic in
many areas of the world are lacking from daily life for Swazi children: 42% of children ages
5-14 engage in child labor activities and 89% are regularly subjected to violent forms of
discipline.10
The combination of economic, social and health factors impacting the country of Swaziland
have produced a complicated situation, but it is not without hope. In the fight against HIV,
Swaziland has reached the tipping point – the rate of new initiations on life-saving drugs is
higher than the rate of new infections.11
In the economic arena, new opportunities are
emerging. For the lowveld in particular, sugar cane holds the potential to be an economic
engine. Even technology is changing for the better as more and more Swazis are connected
to the internet even in the most remote areas.
The next ten years promise to be pivotal in the history of Swaziland. Either the devastation
caused by the HIV crisis will prove too much to overcome, or the country will find its footing
and restore stability.
Despite the ongoing challenges, this country
certainly has reason to be hopeful. Cabrini
Ministries is committed to partnering with our
community, and country as a whole, to turn the
corner on this desperate situation.
9 Ibid. Defined as having a minimum of one meal a day, two pairs of clothing and one pair of shoes.
10 Ibid.
11 AVAC 2013 Annual Report.

Cabrini Ministries Program Report // 2012-2013
13
6. PROGRAMMATIC OVERVIEW
The goal of Cabrini Ministries, as a Catholic faith-based and community-based organization,
is to form a relationship with each family and individual it serves. Who are these family-ies?
What are the health problems, social problems, financial difficulties with which they struggle
daily? Over the years, Cabrini Ministries has come to know the strengths and challenges of
each of the families and individuals it serves, creating a covenant bond of faithful service.
Cabrini Ministries is committed to being faithful and persevering in helping these HIV, TB
and poverty stricken communities become healthier and stronger.
It is the great desire of Cabrini Ministries to love the people of this area with the same faithful
covenant love God has for each of us. We express this love during all our encounters through
a relationship based on respect and dignity – while encouraging those who have defaulted to
adhere to their medications; while teaching and supporting families about protecting the
rights of women and children; while reuniting and strengthening families who have been
overwhelmed by sickness, death and loss.
For the past decade Cabrini Ministries has focused its work on responding to the crisis caused
by HIV/AIDS and TB and the devastating corollaries of these illnesses. Historically, this has
taken the form of health care services for adults and children and impact mitigation measures
aimed primarily at orphans and vulnerable children.
The last year has brought a marked
transition from providing emergency
care to focusing on comprehensive
and integrated social, child care and
health services for families and
children in chronic conditions of
illness, abandonment, abuse, and
poverty. The communities we serve
are awakening from a dark night of
debilitating illness and death to new
beginning of working, caring for
their children and having hope for a
future.
This shift towards chronic care provision does not erase the very real day-to-day realities of
disease, death and poverty – these issues remain as devastating as ever. However, this
change in approach does point to something much greater: the communities we serve in
Swaziland once again have a hope for tomorrow.

Cabrini Ministries Program Report // 2012-2013
14
Cabrini Ministries has worked intensively in this last year to consider all of these changes as
we reshape our existing programs and develop new ones in order to meet the growing and
emerging needs of the communities we serve.
Health Care
The primary objective of the Health Care Program is: To provide a comprehensive,
community based, integrated health care to children and adults living with HIV/AIDS and
TB over their lifetimes.
Service Delivery
The Health Care program at Cabrini Ministries provides a full complement of services for
area clients who are affected by HIV/AIDS and Tuberculosis. The work of this department
occurs in three distinct arenas: Cabrini Drop-in Clinic, Community Health Outreach, and
Targeted Programs.
Drop-in Clinic
The primary point of service for Cabrini Health Care is the
Cabrini Drop-in Clinic located on St. Philips Mission. This
facility serves as the hub for HIV/TB work for the entire
catchment area.
Upon coming to the clinic, clients are checked in, their vital
signs are taken and they receive education and psychosocial
support which is offered by our trained staff. They then
meet with a treatment support counselor before visiting a
skilled nurse who specializes in HIV/TB care and
treatment. All clients, regardless of the purpose of their
visit, receive a TB screening. Basic medical care is also
provided for those who participate in the HIV Testing and Counseling program. For clients
that are in relatively good health, but for whom transportation is a problem, we provide
drivers to bring them to the clinic.
The following services are offered on-site:
HIV Test and Counseling
During an average month, 30-40 individuals come to Cabrini’s on-site facility to find out
their HIV status. If clients are negative for HIV and TB, they are counseled on strategies to
maintain their negative status and encouraged to come back for regular testing. If they are
positive, clients receive a full complement of support care services so they are prepared for
the treatment journey ahead. HIV Testing and Counseling is also regularly offered at
community events.

Cabrini Ministries Program Report // 2012-2013
15
Support Care (adherence counseling, support groups, health education, etc.)
Cabrini’s Health Care Services are not just focused on the medical aspects of care. Every
client, whether new or returning, is provided with psychosocial support and health education
activities.
Pre-ART / ART Initiation and Treatment
The center of Cabrini’s HIV program is treatment. Cabrini nurses are trained and equipped to
initiate clients on life-saving anti-retroviral treatment as well as pre-treatment antibiotic
prophylaxis (cotrimoxizole). Clients receive refills at regular intervals ranging from weekly
to quarterly, along with clinical assessments and personalized care.
Ongoing supportive Health Care
Because HIV suppresses the immune system, it often leads to a wide range of other health
issues. Cabrini integrates care for opportunistic infections and other complicating disorders,
into its regular continuum of care. Clients who are HIV or TB positive are guaranteed access
to the best comprehensive care possible.
Connection to Sexual and Reproductive Health Services
Cabrini works with other organizations to connect our clients with the services they need
including access to sexual and reproductive health interventions.
Basic Labs
As of this year, Cabrini has a small laboratory which provides its new clients with basic
laboratory results including CD4 counts (a basic measure of how advanced the HIV virus is
in a person). Other diagnostic services such as liver and kidney function tests are outsourced
to area laboratories.

Cabrini Ministries Program Report // 2012-2013
16
Food by Prescription
For clients who are clinically malnourished (as determined by body mass index), Cabrini
provides emergency food services as part of its comprehensive care provision.
Transportation to Other Services
Because Cabrini’s Health Care focus is on HIV and TB, not all treatment options are
available onsite. However, because of the covenantal relationship our organization has with
its clients, we are committed to connecting patients to other clinics that can provide the
services they need. On a weekly basis, clients are transported to other hospitals, and in
emergency situations, they are provided with transportation to the closest emergency care
facility.
The Drop-in Clinic also functions as the primary location for all missed appointment follow
up and Health Care data collection/analysis.
Community Health Outreach
In addition to extensive care and treatment for Cabrini
clients, several community health outreach activities
have been implemented:
Homestead Visits
Often, clients are too sick to make it into the clinic for their refills and appointments. In these
cases, Cabrini sends nurses into the catchment area to provide clinical support for the most
vulnerable. These sessions are designed to provide the same level of care offered at the
clinic, but are utilized in the most dire of situations. Nearly every day, a nurse is out doing
these visits. During homestead visits, patients are provided with treatment (pre-ART, ART,
TB, opportunistic infections etc.) as well as psychosocial support through nutritional
supplements, spiritual uplift and counseling.
Remote Refill Locations
Cabrini’s catchment area is approximately 50km in length and width and covers terrain with
only rudimentary dirt roads. Because of this, many clients find it difficult to come to the
In the last year, 1 in 3
Cabrini patients received
care away from the
clinic. This includes
remote refill locations
and home visits.
Patients line up outside a Remote Refill location awaiting care

Cabrini Ministries Program Report // 2012-2013
17
clinic for regular service. In order to alleviate this burden, Cabrini initially began offering a
shuttle service to clients in remote locations. However, as the number of clients served
steadily increased, it became essential to create a new solution. The result was mobile refill
stations. Every week, a nurse, counselor and support staff member head to a remote section
of the catchment area on a regular schedule to provide medication refills and on-site clinical
care. We currently have four refill locations throughout the region: Bhadlane, Mconcwane,
Ncandweni and Sinyamantulwa. These sites provide the same services as the drop-in clinic
(HIV testing and counseling, TB screening, treatment, care and support), but are mobile and
are designed to meet the needs of clients in the most effective way possible.
Missed Appointment Follow up (including partner clinics)
Cabrini recognizes that initiating a person on treatment is only effective if that person
remains on treatment. For this reason, the organization employs one of the most aggressive
missed appointment tracking protocols in the country:
Missed appointments are identified at the end of each day
Clients are contacted immediately to inform them of their appointment status
After 3 days of tracking, a register is opened for the client
If phone calls are not effective, a default tracker is sent to client’s home
If client has not returned in 7 days, they are classified as a defaulter
Follow up continues until client returns or refuses treatment
After 90 days, if client does not return, they are considered lost to follow up as per
national protocols; however, Cabrini continues to track them.
Tracking data is collected and analyzed on a quarterly basis
Cabrini has found that this level of client tracking
is very time and resource intensive, but has
resulted in return rates much better than the
national average. It also provides insights into our
clients’ needs and challenges that would not be
possible otherwise.
In addition to tracking regular Cabrini clients,
Cabrini has entered into partnership with two
government clinics (Sinceni and Siphofaneni) to
provide default tracking and community linkage support. These clinics lie on the outer edge
of the Cabrini catchment area and many of the households our organization serves have
clinical ties with the institutions. In the last year, Cabrini employees followed up with 342
unique clients from these government clinics.
Targeted Programming
In order to address specific health care needs, targeted programs have been established to
focus on the most significant barriers to a healthy community. Cabrini’s targeted programs

Cabrini Ministries Program Report // 2012-2013
18
include: Tuberculosis Care, Prevention of Mother to Child Transmission, Medical
Circumcision, and Community Education.
Tuberculosis Care
While Tuberculosis Care is integrated into the comprehensive health approach Cabrini
implements, its impact necessitates a focused effort on prevention, case finding, diagnosis
and treatment. TB is one of the leading causes of death among HIV+ patients. In order to
decrease its effects, Cabrini has implemented the following systems:
Case Finding
The cornerstone of any TB program is case finding. Regular patients are screened for
symptoms of TB at every visit. Additionally, patients who are suspect for TB are encouraged
to have other members of their homesteads tested to identify if the disease has spread. TB
screening has also been incorporated into everyday aspects of Cabrini programming such as
homestead assessments and healthy child physicals.
If a patient is identified as being a TB suspect, they
are coached through giving a sputum sample for
testing. If other identification measures such as a
chest X-ray are needed, Cabrini arranges for those.
In FY13, roughly 10% of TB suspects were identified
as having the disease.
TB Prevention
Preventing the spread of Tuberculosis is always
preferable to treating the disease. Cabrini takes a
multi-pronged approach to prevention that includes
medical as well as behavioral interventions.
From a medical side, Cabrini offers its clients access
to TB prophylaxis (isoniazid). In the last year, 103
high-risk clients received this preventative care to
reduce their risk of contracting the disease.
In addition to medical interventions, Cabrini also provides existing clients with alternative
living arrangements to prevent the spread of the disease on their homestead. In instances
where a TB-positive client would have to live in the same dwelling as non-infected family
members, Cabrini provides alternative living arrangements so the individual can be cared for
while decreasing the risk of transmission.

Cabrini Ministries Program Report // 2012-2013
19
Treatment and Support
In Swaziland, it is estimated that 15,000 people each year will contract Tuberculosis. A
standard treatment regimen is six-months long, and Cabrini provides this service to over 130
individuals per year. Unlike with HIV on its own, treatment failure bears additional
significant risk – namely the development of Multi-Drug Resistant Tuberculosis (MDR-TB)
which can take up to three years of expensive treatment to cure and has a much higher
mortality rate. Therefore, Cabrini not only provides the treatment, but also focused support
for TB clients. This includes ongoing observation and intentional orientation to the treatment
process and the risks of non-adherence. In the last 3 years, Cabrini has not had any clients
default on TB treatment. This not only guarantees better outcomes for the clients, but also
reduces the risks of MDR-TB which can have devastating effects on the community as a
whole.
Transportation for MDR-TB Clients
Due to the high risk and intensive treatment regimen for MDR-TB clients, a government
hospital has been established to care for these patients. Clients of Cabrini who are suspect of
having MDR-TB are provided transport to the government hospital in order for them to
receive the best care possible. If appropriate, these clients can continue their treatment at
home with Cabrini nurses serving as treatment supporters.
Prevention of Mother to Child Transmission (PMTCT)
Cabrini has implemented a comprehensive education and support program to guide
prospective mothers in maximizing the potential for babies to be happy, healthy and HIV
negative. This requires a dedicated approach to care and support. Once an HIV positive
client in our catchment area is found to be pregnant or intending to become pregnant, a
Cabrini nurse consults with her to discuss options. She is encouraged to attend a support
group with other expectant and new mothers. These groups are led by nurses and include
lessons and open discussions about PMTCT issues. Food supplements and at-home care are
provided as needed. In addition to support care, participants receive ongoing clinical
assessment and support, nutritional support, treatment of opportunistic infections,

Cabrini Ministries Program Report // 2012-2013
20
prophylaxis, ART treatment for those with advanced HIV,
and ante-natal care in cooperation with partner
organizations.
In the last year, 49 new expectant mothers were reached
through our PMTCT program. These new clients joined
the nearly 100 other mothers who were already being
supported through PMTCT programming. Of those, 27
newborns from this year with known HIV statuses, only 2
became HIV positive representing a rate of 7.4%. While
any child becoming HIV positive at birth is tragic, it
should be noted that this rate is significantly lower than
average the mother to child transmission rate of 25%.
Medical Circumcision
Studies have shown that men who are circumcised have a 60% lower chance of contracting
HIV; this ultimately reduces the spread of the disease.12
These encouraging statistics have
prompted a nationwide effort to increase Medical Circumcision (MC). In partnership with
two other NGOs in the country, Cabrini opened a local MC clinic to meet the needs of men
who are willing to participate in this prevention strategy. In the last six months, over 500
school aged children have been encouraged to participate, and ongoing community dialogues
have occurred. Roughly 60 new clients have undergone the procedure at the Cabrini’s MC
Clinic
As the program establishes itself, Cabrini will continue to work with local service providers
to increase the uptake of this service.
Community Education
Cabrini firmly believes that successful prevention and treatment strategies must be built on
education and community engagement. In addition to the on-going education which occurs
during routine clinic sessions, Cabrini hosts regular community education sessions in a
variety of settings and targeting a diverse audience.
Homesteads
The core familial unit in Swaziland is the homestead. Most homesteads in the catchment area
are comprised of between 5 and 10 individuals and often include extended family. Because
of the close relationship Cabrini has with its clients, support often extends beyond the clinic
and into the communities. Several weekend education programs are regularly offered to
clients in order to reach those living with them. In the past year, this has included education
on HIV treatment, palliative care, TB infection control, and encouragement for TB screening
and HIV testing.
12
AVAC, VMMC Talking Points, 2011.

Cabrini Ministries Program Report // 2012-2013
21
Traditional Healers
The clients Cabrini serves are deeply enmeshed in the traditional belief systems of the area.
This includes the regular consultation of Traditional Healers for spiritual, social and health
related issues. An informal survey revealed that over 80% of Cabrini’s clients see a
Traditional Healer at least once before, during or after medical treatment. Despite potential
differences in values, beliefs and approaches to illness, we feel it is essential to work with
these Traditional Healers so that the clients can best be served.
Currently, regular meetings
occur in all three chiefdoms
with the Traditional Healers.
These are facilitated by a local
nurse who is also trained in the
traditional practices. The focus
of the meetings has been on
education. Cabrini has provided
training on how ARVs work and
the unique health concerns of
HIV positive patients. There has also been education on reducing risk in their own practices
and identifying warning signs of HIV and TB. Referrals and continuing education are always
encouraged.
Traditional Leaders
Because the work of Cabrini Ministries is within a setting of traditional chiefdoms, it is
essential that strong working relationships be maintained with the chief and the traditional
structures. Since 2012, Cabrini has offered quarterly education and dialogue sessions with
the traditional leaders of each chiefdom. Topics include HIV/AIDS and TB education,
Medical Circumcision, Treatment adherence and child protection. By reaching the people
who have the most influence in the community, we can ensure the issues are taken seriously.
The leaders are not expected to teach their people but to direct them towards healthy living
for the common good of their chiefdoms. Because traditional values and cultural norms are
involved, the process is always deliberate and respectful. Change does not come quickly and
will take years of building trust to see the full benefits of these efforts.
Healthy Living Advocacy Days
On a quarterly basis, the Health Care Department hosts an education day in different
communities in its catchment areas for current HIV+ patients. The clients invited to the day
are those who are most adherent in caring for themselves and have seen the value of entering
into treatment. They are encouraged to bring a relative or neighbor who has not yet tested.
The day consists of education on positive living, health related discussions, encouragement
for testing for newcomers. The day ends with a full meal and time for socializing. These
well attended events have sought to recognize and encourage those who have adopted a
healthy life style and also to education new community members about positive living.

Cabrini Ministries Program Report // 2012-2013
22
Program Impact
In FY13, the Cabrini Health Care Program served 1,932 unique clients. This includes 1,590
clients from Cabrini Clinic and outreach as well as 342 from the government clinics in
Siphofaneni and Sinceni. Over 20,000 services were provided to these patients. A full
overview of this service provision is available in the appendices, but the following figures
provide a glimpse at the overall impact of the program.
1,932 total clients served (1,399 of these were HIV+)
o 1,590 through Cabrini Clinic (Drop-in Clinic, Remote refill clinic and home
visits)
o 342 through Government Clinics
617 individuals received HIV Testing and Counseling
327 clients received Pre-ART services
872 received ART services
123 were initiated on ART
130 clients with tuberculosis received treatment
o 58 were newly initiated on treatment this year
o 6 new MDR-TB clients were identified
87 clinically malnourished patients received therapeutic food supplements through the
WHO’s Food by Prescription program
103 clients received TB prophylaxis (INH)
89% of clients initiated on ART are known to be alive and on treatment 12 months
after initiation
631 clients received CD4 results
969 missed appointments were followed up on
o 492 from Cabrini
o 477 from Government Clinics
80.5% of clients who missed appointments returned to care.
o 95.9% of Cabrini Clients returned to care13
Over 400 individuals engaged in community education events
o 130 individuals participated in events at the chiefdom level
o 131 participated in HIV testing events
o 91 Rural Health Motivators attended trainings
o Over 100 traditional healers participated in dialogues
49 new mothers were enrolled in programming designed to prevent mother to child
transmission of HIV
13
Lower rates for Government Clinics are due to employee transitions as well as difficulties experienced while
transitioning to a new data tracking system.

Cabrini Ministries Program Report // 2012-2013
23
Key Accomplishments
Alive and on Treatment Rates
The greatest measure of success in the Health Care Department is the number of patients who
remain healthy and productive. When working in the field of HIV, this success is most often
measured by looking at the proportion of clients who are alive and on treatment one year after
their initiation. In Swaziland, the alive and on treatment rate has historically been around
80% -- in other words, even when enrolled on life-saving anti-retroviral treatment, one in five
clients still either default on treatment or die. Over the last 3 years, Cabrini’s Alive and on
Treatment Rate has hovered around 90%. Many factors that influence this figure.
In 2011, Swaziland experienced a stock-out of CD4 reagent which is essential for monitoring
the advancement of HIV in the body. Without these test results, clients were unwilling to
initiate on treatment.14
This delay in initiation led to a decrease in new initiations, which in
turn meant that people started treatment later. All across the country, this decrease in
initiations was noted.
In response to this issue, Cabrini was proactive to ensure patients had the best chances for
survival. Health Care employees advocated at the highest levels of government for
restocking of the vital CD4 reagents. Nurses participated in a national program to allow them
to provide initiations (rather than having to wait on a doctor). Initiations were done when
14
In Swaziland, standard treatment is to start ART at a CD4 level of 350.

Cabrini Ministries Program Report // 2012-2013
24
possible on clinical staging rather than CD4 count. Eventually a point of care CD4 machine
was acquired in order to perform the labs on-site.
As the chart above illustrates, the lack of lab work resulted in decreased initiations and
consequently decreased rates of clients being alive and on treatment. However, once
corrective measures were put into place, the rate rose higher than ever before. It is currently
projected to end the year at nearly 95%!
Keeping people on treatment is not only essential for the health of individuals, but also for
the health of the country as a whole. Clients on treatment are less likely to transmit the
disease and individuals who remain healthy are better able to support their family and their
community.
Launch of MC Clinic and Laboratory
Cabrini realizes that quality health care services must also be accessible in order to be
effective. This approach has resulted in numberous partnerships regular expansion of point-
of-care services. This ensures our clients are as close as possible to the care that they need. In
the last programming year, two such expansions have occurred: the launch of an on-site
laboratory and the launch of a Medical Circumcision Clinic.
Laboratory
Cabrini has always partnered with government clinics to provide laboratory services to our
clients. However, the faster laboratory results can be obtained, the faster proper treatment
can be initiated. Therefore, this year, Cabrini launched its own mini-laboratory. For now its
primary function is providing rapid CD4 counts for clients while they wait. This allows
Cabrini Ministries Program Report // 2012-2013
25
clinicians to quickly pursue the best treatment course of action. In coming months, the
services offered are expected to expand.
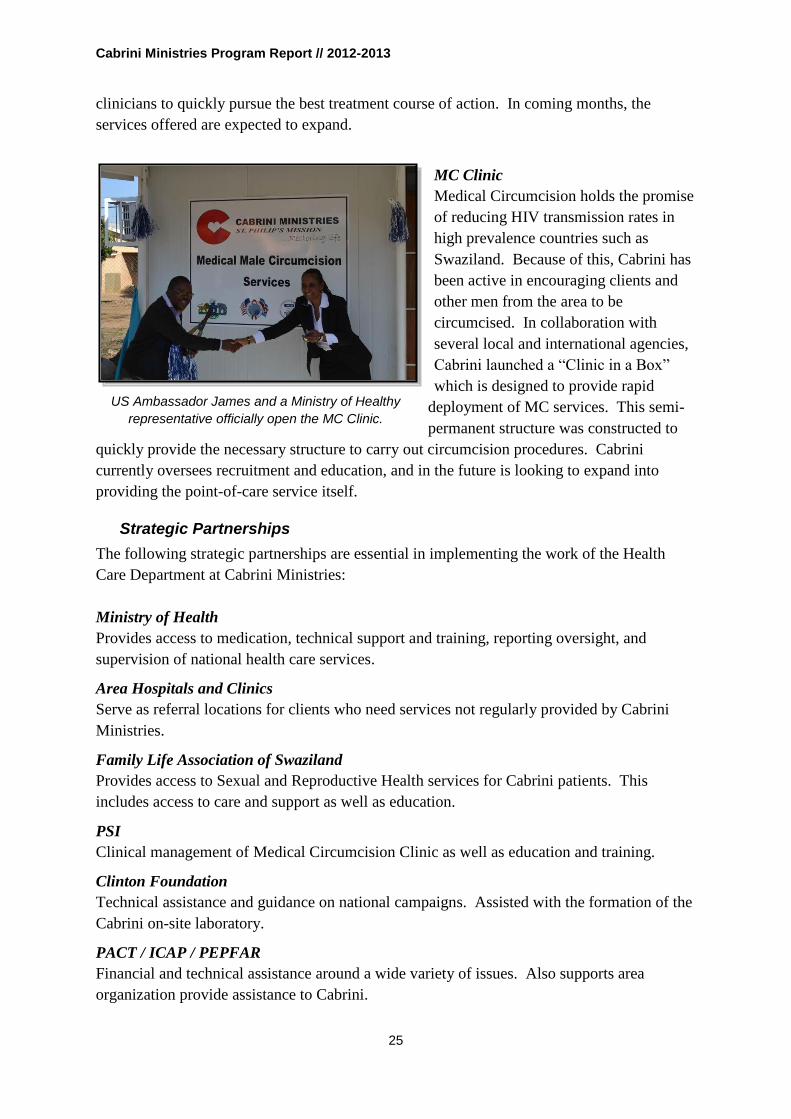
MC Clinic
Medical Circumcision holds the promise
of reducing HIV transmission rates in
high prevalence countries such as
Swaziland. Because of this, Cabrini has
been active in encouraging clients and
other men from the area to be
circumcised. In collaboration with
several local and international agencies,
Cabrini launched a “Clinic in a Box”
which is designed to provide rapid
deployment of MC services. This semi-
permanent structure was constructed to
quickly provide the necessary structure to carry out circumcision procedures. Cabrini
currently oversees recruitment and education, and in the future is looking to expand into
providing the point-of-care service itself.
Strategic Partnerships
The following strategic partnerships are essential in implementing the work of the Health
Care Department at Cabrini Ministries:
Ministry of Health
Provides access to medication, technical support and training, reporting oversight, and
supervision of national health care services.
Area Hospitals and Clinics
Serve as referral locations for clients who need services not regularly provided by Cabrini
Ministries.
Family Life Association of Swaziland
Provides access to Sexual and Reproductive Health services for Cabrini patients. This
includes access to care and support as well as education.
PSI
Clinical management of Medical Circumcision Clinic as well as education and training.
Clinton Foundation
Technical assistance and guidance on national campaigns. Assisted with the formation of the
Cabrini on-site laboratory.
PACT / ICAP / PEPFAR
Financial and technical assistance around a wide variety of issues. Also supports area
organization provide assistance to Cabrini.
US Ambassador James and a Ministry of Healthy
representative officially open the MC Clinic.

Cabrini Ministries Program Report // 2012-2013
26
URC
Training and technical assistance.
Community Health Motivators
Connect clients with local services and also assist with missed appointment follow up and
defaulter tracking.
Cabrini Health Australia
Provide financial and technical assistance. Coordinate with area staff to host extensive
healthy child physicals and work with clinicians to improve quality of care.
SAFAIDS
Partners in work aimed at community leaders and increasing uptake of ART treatment.
TASC
Training for HIV Testing and Counseling.
Mothers to Mothers
Support group facilitation for HIV+ mothers and their babies.
Baylor Clinic
Assistance with pediatric HIV cases.

Cabrini Ministries Program Report // 2012-2013
27
Child Care
The primary objective of the Child Care program is: To Raise orphans and Vulnerable
Children in partnership with their guardians in local communities to help them develop
into happy, healthy, and independent Swazis.
Cabrini Ministries provides
comprehensive care for those in the most
desperate situations as well as targeted
support for individuals and families only
requiring specific assistance. Service
delivery is based upon on-going
assessments of a client’s situation and all
interventions are designed with the larger
family and community in mind.
Assessments
Cabrini’s work with Orphans and Vulnerable children takes into account a person’s needs
and strengths when designing an appropriate intervention. All clients who receive services
through the department undergo an assessment process to ensure the services provided are
tailored to their situation. We believe that the best care comes from a person’s own
community and family and therefore, an emphasis is always placed on utilizing all resources
available.
Needy families are identified through local community
leaders and self-referral. The assessment evaluates not
only the financial situation, but also issues of health,
protection, education and access to non-material
resources and services. These evaluations provide the
basis for future interventions and take into account the
situation of the entire family. Because these assessments
are with high risk and high need individuals and families
and address sensitive issues, the work often takes several
hours as staff members engage in psychosocial care and
support throughout the assessment process.
On-going assessments for current comprehensive care
clients are being performed to determine if, and when, it
is possible to transition these children into a care
situation that is supported on their own homesteads.
Service Delivery
The Child Care program at Cabrini provides services across six domains of care: Shelter,
Nutrition, Health, Education, Legal / Protection, Economic Strengthening and

Cabrini Ministries Program Report // 2012-2013
28
Psychosocial Support. These domains are based on the national Quality Service Standards
for Child care and are integrated into Programs, Events and One-Time Services which are
delivered through the department. As a result of the organization embracing an approach to
service where caring for the whole family unit is understood as the best way to assist the
individuals in that family, the work of Child Care is increasingly being done in collaboration
with Health Care and Social Service.
Service areas
The following service areas are available to children as part of regular programming and as
required in need-specific situations:
Shelter
Provision of shelter is reserved for clients in the most desperate situations; this includes
individuals coming from child-headed homesteads or instances where the safety of a child is
at risk. Shelter services are provided as both long-term and short-term arrangements.
Nutrition
In addition to nutritional support for children
enrolled in comprehensive care, emergency
food provisions are available for families who
need short-term support. Growth monitoring
and appropriate follow up is also included in
the provision of nutritional care for those
served by Cabrini.
Health
The Cabrini Clinic provides access to health care services for children with chronic
conditions. Additional health services are available for community children through regular
physicals and referral to care and treatment, either through Cabrini or in collaboration with
another service provider.
Education
The Child Care Department provides access to education both as a direct provider and as a
liaison with traditional educational structures. As a direct provider, Cabrini offers a Bridge
School as well as after-school tutoring services and special events. In connection with the
national education system, Cabrini helps students overcome issues related to access by
assisting with schools fees, uniforms, boarding costs, etc. We advocate on educational rights
and act as parentis in locus.
Legal / Protection
Cabrini’s work in Legal and Protection is carried out in partnership with the Social Service
Department and commonly includes assisting children in obtaining legal documents such as
birth certificates, parent’s death certificates, identity cards, etc. Cabrini also regularly works
with area entities in issues of child protection. This includes responding to reports of rape or
abuse and helping victims navigate the way forward. Cabrini also provides training and

Cabrini Ministries Program Report // 2012-2013
29
sensitization on child protection issues to staff, children’s guardians and the community at
large.
Economic Strengthening
Various programs in the Child Care department connect children with opportunities to
increase their skills and provide the ability to live a sustainable life on their own. This
includes access to education and trade programs, hands-on job training, and technical skills
development in areas such as agriculture and handicraft.
Psychosocial Support (PSS)
Psychosocial support is care designed to influence the
individual and social environment of a person and
includes social, spiritual, emotional and psychological
elements. For Cabrini, this work is at the heart of all
activities and interventions. PSS is not an activity in
and of itself – rather, it is a methodology that Cabrini
embraces on all levels.
Comprehensive Care Programs
Individuals with the greatest level of need and least availability to services and support may
qualify for comprehensive care services. In the last year, over 150 children received this type
of care. Even when comprehensive services are offered by Cabrini, a partnership with the
client’s homestead is critical to our collaborative model of care. Cabrini staff may have a
parental role with these children, but it is only part of the co-parenting relationship as the
person’s homestead is expected to also provide leadership and support. This is monitored
and encouraged through regular meetings with the guardians.
Hostel
The free on-site hostel for orphans and
vulnerable children is the most intensive
program of care. Participants receive
support in a co-guardian structure wherein
children spend the school year in the Cabrini
hostel with 24 hour care, and then during
school breaks they return to their families
and/or homesteads. Shelter is provided 9+
months a year along with daily meals. All
participants receive regular primary health
care, including checkups and screenings and
additional health referrals are made when
necessary. All children participate in education enhancement activities outside of school four
days per week. Additionally, if necessary, school fees, uniforms, etc. are provided. Each
child receives legal and/or protection services through assessment for and assistance with
essential documents (birth certificates, parents’ death certificates, IDs, etc.). Through the

Cabrini Ministries Program Report // 2012-2013
30
residential childcare staff and case management workers, all children receive ongoing
emotional and social support. This is delivered through prayer, counseling, support groups
and ongoing love; this aspect of our psychosocial approach is deeply integrated into all
aspects of the program. Some students in this group are offered economic strengthening
opportunities through the skills training programs. In the last year, 107 students were stayed
at the hostel.
Aftercare / Supported Independent Living
Not all children who receive comprehensive care live on-site. Cabrini also cares for students
in a variety of off-site living situations. Cabrini pays for many of these students to attend
boarding or trade schools as they continue their education. Additionally, older students may
participate in life transition activities that provide them with safety net of care while still
adjusting to life on their own. All services offered to the Hostel participants are also offered
to these Aftercare participants. Last year, 41 students received Aftercare support.
Respite Care
Cabrini’s respite care program is essentially a short-term enrollment in the hostel. All
services are provided as described above, but participation is not anticipated to be long-term.
Respite care is often offered in cases of abuse while the formal process to find a safe
placement is handled through the appropriate channels. Individuals with short-term, yet
intense, health care needs have also received this service. Services in this area are expected
to expand as the Social Service Department extends its reach in the community.
Targeted Support Programs
The vast majority of children served by Cabrini fall into the category “Targeted Support.”
These children have specific needs as identified in the assessment process and thus are
enrolled in programs and activities that adequately address their situation. Even if a program
does not regularly include some service areas, if they are needed by the children, it is offered
on an individual basis. So, if a student is receiving support for education costs, but also has
health issues that need to be addressed, Cabrini will assist in that area as well.
Academic Support & Sponsorship
Students who are enrolled in our Academic
Support program are usually children who have
their basic needs met, but require support for
things like school fees and uniforms. Even with
expanding assistance from the Swaziland
government, many families simply cannot
afford to send their kids to school since regular
tuition costs can easily be several month’s
salary for a general laborer. Because most
children in our catchment area struggle with

Cabrini Ministries Program Report // 2012-2013
31
more than just academic problems, these children are also assessed for nutritional, health and
protection needs. Students’ progress is regularly monitored by the Education staff. Last year
121 students received this support.
Bridge School
The Cabrini Bridge School was created to facilitate accelerated learning for students who
showed great academic potential, but whose age was not appropriate for their grade level.
Older students who began school later than normal are given the opportunity to work through
multiple years of school in the course of one academic year so they can catch up to their
peers. Originally only offered to existing comprehensive care clients, in the last year, we
expanded this program to include students from neighboring communities as well. Currently
eleven students are enrolled in this program.
Life Skills Camps
Cabrini’s work with orphans and vulnerable children is not just about delivering services, but
also about providing positive environments where youth can learn, experience love, be safe
and ultimately thrive. This atmosphere is encouraged and facilitated through Cabrini’s inter-
term camps. We have observed that the most significant issues our children face present
when they are away from school, including teen pregnancy and abuse. For the past three
years Cabrini has offered these short-term camps during the four annual school term breaks.
This year, the camps’ content included career planning, emotional literacy and developing a
positive outlook on life. By providing a safe environment, the risks to children during these
breaks are reduced. These camps are offered to both students regularly in Cabrini
programming as well as area children who are interested. This also serves as a way for us to
expand our reach into the community. During the most recent camp, over 140 students
participated.
Healthy Child Physicals
For the past three years, Cabrini’s Health Care
and Child Care Departments have partnered
with nurses and doctors from Cabrini Health
Australia to provide physicals for children at
area schools. These health outreach activities
provide the only connection with medical care
some of these students ever receive. The
health checkups include assessments for
malnutrition and common conditions, as well
as TB screening and the opportunity for HIV
testing. Basic clinical care is offered when
possible; for clients with more complicated
issues, a referral and access to care is provided. We make sure to follow up with all at-risk
clients. Nearly 700 unique children have received this access to care in the last two years.

Cabrini Ministries Program Report // 2012-2013
32
CARE Tutoring & Outreach Education
As part of its comprehensive care package, Cabrini provides educational enrichment
opportunities for students living on-site. This program is known as CARE: Cabrini
Arithmetic and Reading Enhancement. Math and language skills have consistently been
identified as areas where students struggle, thus the intentional focus of the program. In
order to deliver high-quality educational services, several educators and tutors are employed.
While initially these teachers worked exclusively with the students at the hostel, in the last
fewyears this program has been expanded to children from area communities as well.
Through partnerships with local schools, Cabrini’s Arithmetic and Reading Enhancement
program was attended by over 200 students. These students have their basic needs met on
their homesteads, but needed some additional instruction outside the regular school day. By
focusing services towards those who need them the most, the impact of Cabrini’s existing
work has expanded.
Therapy and Support Groups
In addition to academic enrichment groups, Cabrini also regularly offers theraputic and
psychoeducation support groups. These groups provide a safe environment for peers to learn
and engage on important issues. In the past year, groups have been created around art-
therapy and life transition support. These groups are led by trained staff and volunteers in the
areas of their expertise.
One Time Services
Not all needs encountered by Cabrini need to be addressed through programmatic
interventions. Sometimes, a one-time service is all that is necessary to allow a family to get
through a difficult situation. Therefore in addition to the programs outlined above, Cabrini
regularly offers short-term care provisions in all domains: Shelter, Nutrition, Health,
Education, Legal / Protection, Economic Strengthening and Psychosocial Support.

Cabrini Ministries Program Report // 2012-2013
33
Program Impact
This year, the Cabrini Child Care Program served 874 unique clients. This includes 151 who
received comprehensive care. A full overview of service provision is available in the
appendices, but these statistics give a glimpse at the overall program impact:
110 children received care at Cabrini Hostel
o The respite program brought in 3 emergency cases included above
41 students participate in the aftercare program
The Academic Support program reached 121 students and is being expanded this year
330 students received Healthy Child Physicals in October
90 new students were enrolled in outreach education
140 students participated in inter-term camps
46 individuals were provided with one-time services
Key Accomplishments
Planned Transitions
The work of Cabrini Ministries in Child Care is largely comprised of long-term care
provision where success is measured over years rather than days or months. Many of the
children who receive care at the hostel have been enrolled in the program for close to a
decade. Because the goal of the department is to help develop orphans and vulnerable
children into happy, healthy and productive members of their community, transitions out of
comprehensive care are always watershed moments for the organization and the individuals.
This year, Cabrini staff has identified 18 students ready to transition from full on-site care
into a supported care situation. For many of these students, their homesteads have achieved a

Cabrini Ministries Program Report // 2012-2013
34
new level of stability as a result of on-going treatment for previously debilitating illness and
new income from expanded economic opportunities, most notably the introduction of sugar
cane. Other students have shown such promise and maturity, that they are ready to transition
into life on their own homesteads.
Some of these students will transition into other targeted care programs at Cabrini, and all
will receive ongoing psychosocial support and transition assistance. For many, the prospect
of a stable life outside of Cabrini was only a distant dream, but now it is a reality.
Student Cultural Exchange Program
Cabrini Ministries has a long-standing relationship with Cabrini College in the United States.
Over the past several years, many collaborations and exchange opportunities have been
created. Cabrini Education staff members have received training at the college, while faculty
and staff from the college have traveled to Swaziland to assist with our program
development.
This year, that cultural exchange was significantly expanded as three of Cabrini Ministries’
brightest students traveled to the United States to participate in an immersion and education
experience through Cabrini College. These students explored academic and career
opportunities and were able to learn from and share with their peers from theUnited States.
Students from the college benefitted from the life perspective these Swazis could offer, while
the Swazi students were given the opportunity to examine a way of life very different than
what they experienced growing up in Swaziland.
Opportunities such as this not only provide avenues for expanding understanding and
compassion on both sides of the ocean, but also serve as a reminder for local students and
staff of how valuable and empowering education can be. In January 2014, the trip will be
reversed as students from the college come to Swaziland for a similar immersion experience.
Khatsiwe, Fanana, Celemusa and Nonhlanhla

Cabrini Ministries Program Report // 2012-2013
35
Expansion of Camps
Cabrini’s inter-term camps have
continued to expand this year.
Originally conceived as a way of
providing a safe environment for
students during the school breaks,
this year has seen significant growth
in terms of content and participants.
In addition to guest speakers and
sessions geared towards life skills
and other psychosocial topics, these
camps have included group
activities, art projects, cooking
lessons and more. Each camp has introduced students to new people within their community
as well as new experiences. In addition to students already enrolled in Cabrini programming,
72 new students also participated.
Open Enrollment for Bridge School
As outlined above, the Cabrini Bridge School was designed to help accelerate the learning
process for students whose age is not appropriate for their academic grade. Whereas the
program was originally only offered to Cabrini hostel students, this year nine new students
from the community were enrolled. All of the students are in grade 7 and were targeted
because of their potential for success despite previous academic hurdles. The smaller class
size allows for more one-on-one attention in hopes that these students will be able to pass
external examinations and succeed in high school. In addition to a dedicated teacher, several
special instructors have been brought in throughout the year to assist.
New Psycoeducation Groups
Psychosocial support is always integrated into Cabrini’s care models. However, some
activities are specifically designed to address the emotional, spiritual and psychological needs
of individuals in our programs. An example of intentional programming has been the launch
of psychoeducation groups for children staying at the hostel. Groups are formed based on
peer groups and common challenges. Over the last year, various issues have been explored
including: self-esteem, body image, identity, good touch/bad touch and preparing for the
future. Currently there are seven groups meeting weekly that incorporatevarious interactive
activities, discussions, visual art, dance, and music. This psychoeducational approach to
group facilitation has also crossed over to the guardians meetings held at the beginning of
each term. The guardians were asked to participate in similar kinds of art and movement-
based activities along with the children. Additionally, many students are participating in one-
on-one care to increase the effectiveness and depth of this approach.

Cabrini Ministries Program Report // 2012-2013
36
Strategic Partnerships
The following strategic partnerships are essential in implementing the work of the Child Care
Department at Cabrini Ministries:
SOLON Foundation
Partners in Academic Support programming
Swazi Government Agencies
The Child Care staff work with various government agencies to address issues of abuse and
protection. This includes the local Police Departments, the Department of Social Welfare,
the National Children’s Coordination Unit, Rural Health Motivators, Lihlombe Lekukhalela
and SWAGAA.
PACT / ICAP / PEPFAR
Financial and technical assistance, especially around psychosocial support models and
connection to external care services. Also supports national initiatives in which Cabrini
participates.
Cabrini College
Continued education and pedagogical instruction for staff. Partners in cultural exchange
program.
Cabrini Health Australia
Financial and programmatic support, especially around areas of palliative care and academic
reporting. Also partners in implementation of Healthy Child Physicals.

Cabrini Ministries Program Report // 2012-2013
37
Social Services
The primary objective of the Social Service program is: To help families meet their
emotional, spiritual, physical and material needs through timely, expert and ongoing
support.
The department bridges the gaps outside the normal
scope of work of Child Care and Healthcare, and
navigates internal and external resources to address
challenges related to a range of issues, including child
abuse, mental and physical illness, food insecurity,
family reunification, and legal documentation.
Program Development
As part of an on-going evolution of program activities,
Cabrini Ministries formalized the establishment of a
Social Service Department in July 2013 after several
years of needs assessment and a full year of planning.
The department was developed in response to significant
gaps in service that exist for some of the most vulnerable
children and families in Cabrini’s catchment area. As a
result of the trusting relationship Cabrini Ministries has
developed with the community over the years, area stake holders -- including staff, current
clients, community leaders, and other service providers -- have increasingly been reporting
homesteads in desperate and dangerous conditions, necessitating the timely expert assistance
of a trained Social Worker and dedicated case managers. For example, Cabrini’s outreach
nurses often find cases of infants and toddlers unsupervised or otherwise neglected on their
homestead as a result of death, disease, poverty, or alcoholism.
The Health Care and Child Care staff have
always worked together to meet the needs in its
communities but these growing needs are
outside their capacity and scope of work. Cabrini
needed a way to provide a dedicated and focused
response with adequate infrastructure and staff
with specific training, tools and supervision to
meet the immediate and longer term needs of the
children and families in the catchment area.
Such a response was also necessary because of a critical lack of government resources
directed at meeting social and child welfare needs in Swaziland. The governmental systems
that are in place are limited to reporting and lack the ability to enforce child protection laws
or provide for extended care in cases of abuse or severe neglect. Sometimes the lack of
Understanding the challenges
that families face, and helping
them to find their own solutions
is most effectively accomplished
through a psychosocial, holistic,
community-based, and
culturally relevant approach.

Cabrini Ministries Program Report // 2012-2013
38
resources of the relevant government agencies is as basic as a vehicle to arrest an alleged
child abuser, leaving the child at continued risk of harm until transport can be organized. .
In addition to filling the gaps in services, the Social Service Department’s development is
also related to an evolution in how Cabrini views the people it serves, moving from a focus
on individual patients and children to a focus on the family or homestead as the client. This is
fundamental to Cabrini’s psychosocial approach and understanding that individuals function
in families within communities. Understanding the challenges that families face, and helping
them to find their own solutions are most effectively accomplished through a psychosocial-
holistic, community-based, and culturally relevant- approach.
Service Delivery
Even before the Social Service Department was formally launched, Cabrini Ministries was
responding to the diverse needs of community members as they emerged. However, without
the formal structures and expertise it was difficult to ensure effective and efficient service
provision.
In order to develop the department, a
Masters Level Social Worker was brought
in to design a system of assessments,
interventions and follows ups tailored to
the local situation. Two case managers,
including a dedicated liaison between
Health Care and Child Care, as well as the
services of other support staff ensure the
department has the capacity to respond.
Currently, in addition to regular
assessments and case management, targeted interventions exist in the follow areas:
Nutrition, Health, Education, Protection, Psychosocial Support and Economic
Strengthening.
The first step to expanding service delivery was to broaden the annual assessment process.
Historically, this was a process to identify children who qualified for Cabrini Ministries’
educational support program. The goal of the annual assessments in 2013 was to complete a
comprehensive evaluation of the entire family and identify the challenges they face in
meeting their own educational, material, physical, and emotional needs. This involved
creating a more time-intensive and detailed assessment form and process, as well as training
staff. In addition to assessing social service needs, assessors incorporated TB screenings into
the process, resulting in over 60 positive screens which were then referred to our Health Care
Department for follow up and treatment if needed.
This improved assessment process has provided an avenue for improving the comprehensive
integrated service delivery that is based on a homestead’s strengths and challenges. Currently,

Cabrini Ministries Program Report // 2012-2013
39
the Social Service Department is providing the following services to families in our
catchment area:
Educate and assist families in advocating for their rights when they are being abused
or when they have a disability.
Locate family members and obtain legal documents (for example, birth and death
certificates), especially when doing so has proved difficult for individuals whose
mothers have abandoned them or are otherwise unavailable to accompany them as is
required.
Confront short-term food emergencies.
Make referrals to Cabrini Health Care and/or other health facilities, and assure follow
through by arranging transport, advocacy and financial assistance where necessary.
Disclosure counseling for families with children who are HIV positive.
Psychoeducational and therapeutic support groups for children, pre-adolescents and
teens in our hostel program.
The assessment process has also resulted in an improved
referral system; this includes connecting clients with
services Cabrini already provides as well as linking them
to outside organizations who can better meet their
individual needs. The department has also made stronger
linkages with the Social Welfare and Child Protection
Departments in our catchment area as well as the national
referral agencies that support children who have been
physically or sexually abused for counseling and other
support services.
Impact and Expansion
Between August and October 2013, the Social Service department led the assessment process
of 131 homesteads resulting in 1,067 individual contacts. Ninety-two children were
recommended for educational assistance and 40 individuals were connected with health care
services. Forty-five additional homesteads received services in the realms of psychosocial
support, legal/protection, shelter and nutrition. Ongoing assessments, interventions and
referrals are occurring weekly along with regular case management of our clients.
Programs that are in process or are under consideration through the Social Service
Department include:
Forming a “teen club” in collaboration with Baylor Clinic to serve the 35 teens who
receive ART through our Health Care department.
Developing a 24 hour, 365 days a year short-term respite program for children who in
abusive or otherwise unsafe environments until a long-term safety plan can be put in
place in conjunction with community members, governmental resources and other
NGOs.
Working in collaboration with Child Care to create more formalized and structured
after-care services for our teens aging out of the hostel and moving on to independent
living.

Cabrini Ministries Program Report // 2012-2013
40
Agriculture
Agricultural work has been a part of programming at St. Philips Mission since the 1970s with
the early work of the Missionary Sisters of the Sacred Heart. It has taken many forms and
has always symbolized the coming of new life inherent in the work of Cabrini as a whole.
This year the Agriculture Department has seen some significant changes as a Food Security
program concluded and the department transitioned to more integrated programming.
Food Security Programming
In 2013, Cabrini Ministries successfully completed an
agricultural education and food security training program. The
program, which ran from January 2012 to July 2013, included
the creation of a locally relevant permanent agriculture
curriculum which was then utilized to train 147 children and
health care patients. Cabrini staff worked with families on their
homesteads to design and create permanent garden spaces.
These individuals were provided with the necessary inputs
(tools, seedlings, technical support) to improve their ability to
grow nutrient-rich fruits and vegetables for their families.
Key Indicators
Completed development of Agricultural Education Curriculum
147 people trained on farming techniques, nutritional practices and the establishment
of door-sized gardens.
o Including orphans and vulnerable children and 55 area families
98% of the children and families trained went on to establish productive gardens
Program Transition
After a year of implementing the food security program, Cabrini Ministries decided to
reorient its agriculture work. Up to 2013, Cabrini operated a small commercial agriculture
department. The department provided both food for our hostel and health-care patients and
crops for market. However, the operation was resource-intensive, dealing with local markets
was difficult, and production did not always meet expectations. Because the department was
not an integral part of the mission of Cabrini Ministries, the decision was made to shift focus
from internal food production towards community education and training.
By scaling down the program, we are also able to offer more effective agricultural education
to children and teenagers. Using the knowledge and skills gained, we are continuing to
mentor those in our care on best practices in individual food security. These mentorships are
important for improving the capacity of our children and teenagers to provide for themselves
and their families later in life. Finally, Cabrini is also cultivating bananas and has already
enjoyed the first crop. Bananas are a low-cost, low-maintenance fruit to cultivate and provide
our patients and children a significant amount of fresh fruit each year.

Cabrini Ministries Program Report // 2012-2013
41
7. MONITORING AND EVALUATION SYSTEMS
The Monitoring and Evaluation systems employed by Cabrini Ministries has been designed to
provide rapid programmatic feedback while also tracking relevant information needed for
grants management and collaboration with key stakeholders. It is built around a shared
database structure that utilizes appropriate primary source documentation for data entry and
quality assurance auditing. The overall M&E systems are then used on a regular basis to
review and improve program delivery and to provide accurate reports to donors and other key
stakeholders.
Every employee who assists with service delivery is aware of the importance of proper
indicator tracking; staff implementing programming play a vital role in providing accurate
and precise data about organizational impact. Cabrini currently employs a full time M&E
officer as well as a full time Health Care Data Officer. Two other Health Care employees are
cross-trained on data entry and basic reporting and support the operations. In Child Care,
primary source documentation is managed part-time by an administrative staff member with
the assistance of a Child Care focal person. The Social Service Department handles data
input on the case-management level. Regular reports can be compiled by all M&E staff,
while the Grants Manager is responsible for major report aggregation as well the
development of data tools and the compilation of trends and projections.
The current system is primarily based on three linked databases to track program enrollment
and service delivery. Work is currently underway to unify these into a single system. The
Health Care database is designed around tracking clinical services and appointment follow
up. The Child Care database focuses on program enrollment and event tracking. The Social
Service database links homestead assessments with interventions. All of these systems are
run in Microsoft Access with network capabilities that allow for multi-user sharing and easy
digital backups.
On a quarterly basis, the program enrollment in Child Care is reviewed and a full data audit
on one week’s worth of services is performed at Health Care. These reviews have resulted in
improved data quality, as corrective measures are constantly being implemented, particularly
as it relates to data flow and collection.
These M&E systems are used to collect over 400 unique indicators for various stakeholders
connected to Cabrini Ministries. Recent improvements in the systems have allowed the
organization to move from simply tracking program outputs to tracking the impact the work
has for those it serves
In order to improve the precision of the reporting, the Data Officers are primarily responsible
for maintaining data quality, while the M&E Officer oversees report generation. This ensures
continuity across all the statistics generated. An indicator aggregation tool has been
developed that converts a query of services offered into age and gender delineated results for

Cabrini Ministries Program Report // 2012-2013
42
a wide variety of indicators. This approach reduces human error and increases the reliability
of results.
Over the past two years, Cabrini’s approach to data management has been to focus on the
creation of precise results (replicable figures based on primary source documents) and then to
expand the scope of data collection. This strategy has resulted in consistent figures that
improve in quality each quarter.
Two major transitions are underway in the M&E department at Cabrini. The first is the
integration of all data systems into a unified database. This will improve Cabrini’s ability to
deduplicate impact results for people who receive services from multiple departments. It will
also improve service delivery as relevant staff will have a broad dataset to work from. If an
adolescent Health Care client is consistently missing refill appointments, the default trackers
will be able to access information from the homestead assessments to ascertain if outside
factors may contribute to the non-adherent behavior.
The second major transition involves shifting the system to track all clients in relation to the
homesteads they belong to. This will not only provide a better understanding of the
interconnectedness of Cabrini’s service delivery across multiple departments, but it will also
provide new information on how best to address issues at the homestead level as Cabrini
seeks to continually improve its service delivery to the family as a unit.
The Monitoring and Evaluation systems at Cabrini continue to evolve with the ultimate goal
of using information to provide the best delivery of care possible.

Cabrini Ministries Program Report // 2012-2013
43
8. ORGANIZATIONAL DEVELOPMENT
The ability of Cabrini Ministries to continue to offer high-quality, high-impact programming
is dependent on maintaining the support structures needed for implementation. The role of
Organizational Development is inseparable from
program delivery. Over the last two years, Cabrini
has been intentional about planning for the future
by looking at current and expected needs in relation
to the capacity of the organization and overall
expected internal and external transitions.
Concerted effort is being directed at continuing
development in the areas of: staff, programming,
funding and transitional planning.
Identified Emerging Issues
In the last decade, Cabrini Ministries has developed health care and child care programming
to address issues related to those infected and affected by HIV/AIDS and TB in its lowveld
catchment area. While significant immediate needs still exist, nearly everyone who wants
access to HIV/TB care is receiving it and the life threatening issues for orphans and
vulnerable children are being addressed. This movement from emergency care to chronic
care has resulted in a relative stability that now allows Cabrini Ministries to begin identifying
and responding to emerging issues.
The issues outlined below have been directly observed in Cabrini’s care context, yet are also
foreseen to have effects in the larger Southern African and Global context. Cabrini
Ministries is uniquely positioned as an “on-the ground implementer” while maintaining
significant connections with the larger structures in global health. This context can and
should be leveraged to impact future policy and funding movement.
Tuberculosis
TB is the leading cause of death among HIV+ positive clients. While a strong treatment
infrastructure and national protocols exist for TB and MDR-TB, implementation of national
public health policies regarding infection control are dangerously lagging behind. Rural
areas where eating utensils and sleeping arrangements are often shared are among the hardest
hit. Case finding in the rural areas is also more difficult due to poor infrastructure and lack of
regular clinical care. Treatment protocols are intensive and adherence often requires use of
public transportation which can be expensive and exposes more people to the disease as care
is given in the midst of other sick individuals. Additionally, monies dedicated to stopping the
spread of the disease have proven to be difficult to access, especially for civil society
organizations often tasked with orchestrating the community-based work.

Cabrini Ministries Program Report // 2012-2013
44
Addressing this issue will require the following activities:
Increase in implementing staff to address issues of education and more intense case
finding on the homestead-level.
Development of a Monitoring and Evaluation plan to track process and ensure
connection to relevant services.
Increased training for all staff – not just nurses, especially around MDR-TB, case
finding and infection control.
Ongoing discussion with national and international stakeholders concerning resource
allocation. Structural issues must be addressed in order to ensure this work is done
effectively and efficiently.
Stay on the cutting edge of TB work through ongoing training and innovative
program development.
Sustaining Treatment
In the catchment area served (approximately 350
square miles or 5% of Swaziland), well over 2,000
clients are enrolled on life-saving ARV treatment.
This number is bound to increase as discussion of
Treatment as Prevention is becoming more
commonplace. Cabrini has been pro-active is making
on-going treatment as easy as possible for clients with
outreach nursing services and remote refill clinics.
However, even with the significant headway being
made in treatment availability, the effectiveness of
this work relies on sustained treatment. Currently,
10% of appointments are missed, and without time
and resource intense follow up, many of these clients
would default. Addressing this is a primary concern.
In the context of Cabrini’s current work, this means
an increased focus on consistent treatment for current
patients, that include improved pre-initiation
counseling and sustained follow up and counseling for those with chronic missed
appointments. Additionally, as clients become more mobile, it will be essential to improve
transfer and patient follow up procedures.
Cabrini currently is leading the way in Swaziland when it comes to patient tracking and
follow-up, but needs to emphasize the importance of treatment support on a larger scale so
this need is not overshadowed by the push for increased initiations. Additionally, as HIV+
clients are initiated on ART at earlier stages before they have experienced the devastating
effects of the later stages of the disease, it is likely that sustaining treatment will become
more difficult.

Cabrini Ministries Program Report // 2012-2013
45
To further prepare to meet these needs, Cabrini needs to:
Research and provide training on Treatment as Prevention since this will complicate
and enhance work in this area
Improve intake processes (including interviews) so that clients are ready for ART and
its impacts
Expand connection with clients to their homesteads so we are better equipped to
address the issues that impact treatment
Identify and respond to factors influencing treatment default
Life Transition Programs
With the increased roll out of ARVs in the country and expanding Child Care services from
Cabrini, the urgency to simply keep people alive has evolved into a need to improve the
quality of life. Orphans and vulnerable children who would be dead are now alive; yet, many
have experienced the disintegration of family structures as multiple primary care providers
have died or abandoned them. These youth are now aging into adulthood with major issues
related to anger, depression and self-esteem. This, coupled with an intentional focus on
impact mitigation for only those under 18 has created a generation without the proper skills to
transition into a meaningful life experience. There is a high incidence rate of pregnancy and
increased risky behaviors that is being observed especially among those classified as Orphans
and Vulnerable Children.
Whereas meeting the basic needs (health, shelter, food, etc.) of at risk populations have been
relatively straightforward. These emerging psychosocial issues will require innovative
approaches and long term commitment. This will likely include:
life-skill development
relevant income generating opportunities
counseling and mental health care
mentoring and/or support groups
Responding to this emerging issue will require:
Increased staffing, especially amongst professionals and para-professionals.
Improved M+E procedures and systems to be able to track beyond “services
provided” and including future transitions and outcomes
(Re)Establish connections with children who have left the program to compile
“Lessons Learned”
Increased staff training and flexibility around broader life issues.
Expanded need for Social Service Provision
The issues mentioned above address emerging issues that are or will face the existing
departments at Cabrini. However, as the country of Swaziland moves to stabilizing in the
“new normal” of ARVs and broken families, a whole new category of need emerges: those
issues requiring Social Service intervention.

Cabrini Ministries Program Report // 2012-2013
46
Cabrini’s recent launch of the Social Service Department has been designed to respond more
efficiently and effectively to growing needs such as child protection, abuse, psychosocial
support, counseling, etc. The role and function of this department will continue to evolve and
expand.
In order to respond to this need, the following actions need to occur:
Continue to develop the Social Service department headed by professional staff and
capacitated to assess and respond to social needs of those currently receiving services
and to the families in the catchment area as a whole.
Further integrate these services with the existing departments of Child Care and
Health Care.
Upgrade M&E systems to track activities and identify progress and ways for
improvement.
Work with existing and interested parties to push for a national system which
effectively addresses the national issues.
Strategic Priorities
In light of the items considered above, the following strategic priorities have been set by the
organization:
Continue focus on providing cutting edge work with measurable results
Cabrini Ministries is already known for its high quality work in a resource limited setting.
The organization has designed and modeled “best practices” that are utilized on a local and
regional setting. It has a rapidly improving Monitoring and Evaluation structure that has the
emerging ability to provide significant data points for program evaluation and future
planning. On the whole, Cabrini Ministries’ track record of success and accountability makes
it attractive for funding organizations.
If Cabrini Ministries is going to succeed in the future, it must keep its focus on innovation
and superior service delivery. Future development cannot occur without an emphasis on
current implementation.
Additionally, the M+E systems in place must continue to expand to include improved data,
more relevant indicators, and future trends. It must also include significant qualitative data in
the form of success stories and lessons learned. This will make Cabrini more attractive while
also positioning the organization to respond to new issues faced in the catchment area.
Strengthen existing funding relationships
It is easier to keep existing funds than it is to raise new funds. With this in mind, Cabrini
Ministries will continue to strengthen its existing relationships. This includes improved
reporting, better donor follow up, and expanded relationships. It is not only relevant to keep

Cabrini Ministries Program Report // 2012-2013
47
the current funding sources, but to also explore expanded opportunities such as new grant
opportunities, increased funding and extended reach.
Position the organization to be ready to handle emerging issues
Cabrini Ministries has always “followed the need” and in doing so has positioned itself on the
cutting edge of many emerging global issues. Because of its structure and relationships, the
organization has been able to bridge the gap between high level policy makers and on the
ground needs. Cabrini is primarily an “implementer” but has the ability to make an influence
on a higher structural level. This unique status allows the organization to be an innovator and
the opportunities that arise from this should be optimized.
Moving forward, Cabrini will be attentive to
ways of positioning itself to receive funding for
emerging issues. This means that more attention
needs to be paid towards monitoring local needs
that are not being met and also the effectiveness
of interventions. This may require willingness
to “staff ahead of the need” and to invest in
work that is not yet funded.
As the organization expands to provide even more comprehensive and integrated services in
the area, new issues will be discovered. Cabrini is committed to continually evaluating the
assets and challenges in the community in order to be able to respond in the most appropriate
way possible.
Integrate development planning into organization's on-going life
As Cabrini grows, its programmatic footprint and financial needs also expand. As a result,
significant breakthroughs are being made in terms of community assistance and impact.
However, this also increases the burden of sustainability. More money is required every year
to provide existing and emerging services; additionally, there is more demand for
professional staff in a location that is not inherently attractive. Therefore, an intentional
focus needs to exist towards how the organization grows and develops. This includes the
need for
Further development of a long range succession plan for all key staff members as well
as training and staffing plans which are tied to organizational priorities
Movement towards multi-year budgets and funding forecasting
Strategic emphasis on developing new relationships with potential funders and policy
makers
Improved indicators which inform and shape the items described above.
Becoming a “Social Service Organization”
In 2013, Cabrini undertook a series of Strategic Development retreats to build an action plan
based on the realities outlined above. The apex of the dialogues revolved around a discussion

Cabrini Ministries Program Report // 2012-2013
48
about the core business of Cabrini Ministries in light of programmatic transitions and
emerging needs. By identifying the changing circumstances in our organization, our
community and our world, the following conclusion was formed:
Cabrini is at a critical transitional moment in its understanding of itself and needs to
evaluate its mission, vision, value and work as it moves into the future.
Specifically, the team that gathered recognized that it is Cabrini’s integrated psycosocial
methodology to its work in the community that makes it unique and effective. That,
combined with our Christian identity and mission, undergirds the programmatic approach in
all departments. While the development of the Social Service Department was originally
conceived as a way to expand care to those who fall between Health Care and Child Care
services, in reality, all of our work is based on Social Service – Health Care and Child Care
programming are simply expressions of that.
Rather than looking at ways to integrate Social Services into the current work, the Cabrini
leadership believes that the organization is moving to a place where a Social Service
framework will inform and direct the organization as a whole.
While this is a transition which is in-line with Cabrini’s ongoing history and implementation,
it is a significant evolution. Additional strategic development sessions have already been
planned for 2014 to further explore and develop the implications of this transition. In the
end, the vision of “Restoring Life” will not change; instead it will only develop and expand in
its scope.
Future Projects
In evaluating future organizational development, investment in the following has been
identified as priorities:
Maintenance / Expansion of Vehicle Fleet – On average, Cabrini needs one vehicle
per year to keep up with the wear and tear of community based projects.
Expanded Staffing – This primarily involves professional and para-professional staff
for all departments including a Clinical Social worker, additional nurses, and child
care professionals.
Expanded laboratory– This includes a point of care GeneXpert and viral load
machine. These machines hold the potential to increase our responsiveness to HIV
and TB in our area.
Staff trainings / development – As Cabrini grows, it becomes necessary to develop
the professional capacity of existing staff in key roles as a way of increasing
organizational capacity and individual potential. This will require ongoing training
and most likely the sponsorship of education fees in areas like Pharmacy, Social
Work, etc.
Improved Infrastructure for Child Care – The Child Care department is in need of
capital expenditure around things like beds, desks, building remodels, etc.
Cabrini Ministries Program Report // 2012-2013
49
Respite Care Facilities – In order to respond to emergency shelter needs for those in
Respite Care, a dedicated facility along with 24-hour staff is essential. This is
particularly true for care provision to those under 5 years of age.
Staff housing – As our staff increases, especially among professional staff, increasing
the availability of on-site housing will be essential.
Upgrading Remote Outreach – Our Remote refill and treatment sites have become a
large part of the work being done in the communities. Upgrades of the “borrowed”
facilities will improve the quality of work in these areas.
Expanded Health Services – Cabrini is investigating the possibility of integrated full
clinical care to meet the needs of those served in the catchment area. This would be
an expansion from our current focus on HIV and TB towards being a full service
clinic.
Scholarships for transitioning Cabrini Students – Students transitioning from high
school are often faced with the inability to attend tertiary education opportunities due
to a lack of funding. It is our desire to establish a scholarship program.
Energy Infrastructures – Cabrini’s work has been more sophisticated in the last 5
years while the infrastructure in the area, particularly electricity, has gotten worse.
Cabrini needs to install automated generators to ensure the highest level of care is
possible even during regular power outages. Additionally solar panels are being
investigated to achieve an overall cost reduction and improve environmental
sustainability.
Establishment of an Endowment Fund – In order to ensure the vital programming in
Swaziland is able to continue, the organization is looking to establish an endowment
fund that would support the work of the organization well into the future.

Cabrini Ministries Program Report // 2012-2013
50
9. GET INVOLVED
The work of Cabrini exists through the support of numerous foundations, organizations and
individuals across the globe. If you would like to get involved, please consider one of the
following.
Sponsor a Special Project
Our development team would love to work with you or your organization to sponsor one of
the special projects outlined above. To find out more, please contact the Cabrini staff at
Donate as an individual.
Regardless of your desired level of involvement, you can make a tangible impact in the lives
of people served by Cabrini Ministries in Swaziland. Consider the following:
Provide hope to marginalized youth by sponsoring a child
For $100 per month, you are able to provide for all the needs of one of Swaziland’s most at-
risk youth. This will cover food, shelter, clothing, education and healthcare for a child. You
will receive periodic photos and updates on your child.
Give life to the sick by supporting essential medical care
For $90 you can provide a year’s worth of comprehensive health care for someone suffering
from HIV or Tuberculosis. This includes testing, counseling, treatment, transportation and
follow up support.
Offer the promise of a better future through education
For $400 per year, you can sponsor the education of a child in Swaziland. This includes all
of the costs associated with schooling for a Swazi child including tuition, uniforms and exam
fees.
Donation Information
To support the work of Cabrini Ministries in the United States, please send your tax-
deductible payment and contact information to: Swaziland Donation, C/O Cabrini Mission
Foundation, 222 East 19th Street, Suite 5E, New York, NY 10003.
In Australia, staff at Cabrini Health Australia can work with their employer to make one-time
or ongoing contributions to the work in Swaziland. Please contact Kate Barker for more
information: [email protected]
For more donation options, please visit: www.cabriniministries.org/donate/

Cabrini Ministries Program Report // 2012-2013
51
10. APPENDICES
Cabrini Health Care Analysis of Services ........................................................................... 52
Clinical Cascade Results and Exits ...................................................................................... 56
Cabrini Impact Mitigation Analysis of Services .................................................................. 57

Cabrini Ministries Program Report // 2012-2013
52
Cabrini Health Care Analysis of Services
Report for the period of Oct 2012 - Sep 2013
TOTAL Clients Served (18)
Female Male
Grand Total
<18 201 168 369
18+ 862 492 1354
Grand Total 1063 660 1723
TOTAL HIV+ Clients Served (18)
Female Male
Grand Total
<18 60 54 114
18+ 620 352 972
Grand Total 680 406 1086
TOTAL Visits (18)
Female Male
Grand Total
<18 781 657 1438
18+ 4823 2541 7364
Grand Total 5604 3198 8802
TOTAL Services (18)
Female Male
Grand Total
<18 1641 1357 2998
18+ 12095 6270 18365
Grand Total 13736 7627 21363
ART Clients Served (18)
Female Male
Grand Total
<18 52 44 96
18+ 488 291 779
Grand Total 540 335 875
ART Initiations (18)
Female Male
Grand Total
<18 13 5 18
18+ 66 44 110
Grand Total 79 49 128
Pre-ART Clients Served (18)
Female Male
Grand Total
<18 24 18 42
18+ 192 95 287
Grand Total 216 113 329
CD4 Tests (18)
Female Male
Grand Total
<18 73 75 148
18+ 864 410 1274
Grand Total 937 485 1422
CD4 Individuals (18)
Female Male
Grand Total
<18 44 43 87
18+ 502 259 761
Grand Total 546 302 848
Visits with OI Treatment (18)
Female Male
Grand Total
<18 165 123 288
18+ 2262 949 3211
Grand Total 2427 1072 3499

Cabrini Ministries Program Report // 2012-2013
53
Clients with OI Treatment (18)
Female Male
Grand Total
<18 48 46 94
18+ 568 299 867
Grand Total 616 345 961
TB Clients Served (18)
Female Male
Grand Total
<18 12 9 21
18+ 66 59 125
Grand Total 78 68 146
TB Clients Served by Type (18)
Ordinary MDR/XDR
Grand Total
Female 75 3 78
<18 12 0 12
18+ 63 3 66
Male 67 1 68
<18 9 0 9
18+ 58 1 59
Grand Total 142 4 146
HIV + TB Clients Served (18)
Female Male
Grand Total
<18 7 7 14
18+ 47 45 92
Grand Total 54 52 106
TB Initiations (18)
Female Male
Grand Total
<18 3 4 7
18+ 25 28 53
Grand Total 28 32 60
TB Initiations by Type (18)
Ordinary MDR/XDR
Grand Total
Female 26 2 28
<18 3 0 3
18+ 23 2 25
Male 32 0 32
<18 4 0 4
18+ 28 0 28
Grand Total 58 2 60
TB Initiations of HIV+ clients (18)
Female Male
Grand Total
<18 2 3 5
18+ 21 19 40
Grand Total 23 22 45
INH Initiation (18)
Female Male
Grand Total
<18 1 2 3
18+ 27 13 40
Grand Total 28 15 43
INH Completion (18)
Female Male
Grand Total
<18 0 2 2
18+ 28 12 40
Grand Total 28 14 42
Total Clients on INH (18)
Female Male
Grand Total
<18 2 4 6
18+ 63 34 97
Grand Total 65 38 103

Cabrini Ministries Program Report // 2012-2013
54
Sputum Tests (18)
Female Male
Grand Total
<18 0 0 0
18+ 77 57 134
Grand Total 77 57 134
Clients with Sputum Tests (18)
Female Male
Grand Total
<18 0 0 0
18+ 60 47 107
Grand Total 60 47 107
HIV+ Clients with Sputum Tests (18)
Female Male
Grand Total
<18 0 0 0
18+ 48 37 85
Grand Total 48 37 85
HIV Tests by Age / Gender (18)
Female Male
Grand Total
<18 140 120 260
18+ 307 180 487
Grand Total 447 300 747
Total HIV Tests by Result (18)
Negative Positive
Grand Total
Female 378 69 447
<18 133 7 140
18+ 245 62 307
Male 244 56 300
<18 112 8 120
18+ 132 48 180
Grand Total 622 125 747
HIV Re-Tests Only by Result (18)
Negative Positive
Grand Total
Female 122 5 127
<18 7 0 7
18+ 115 5 120
Male 39 0 39
<18 6 0 6
18+ 33 0 33
Grand Total 161 5 166
% of HIV Tests Positive (18)
Female Male Grand Total
<18 5.0% 6.7% 5.8%
18+ 20.2% 26.7% 22.6%
Grand Total 15.4% 18.7% 16.7%
% of People HIV Positive (18)
Female Male Grand Total
<18 5.3% 7.0% 6.1%
18+ 33.2% 32.7% 32.9%
Grand Total 21.6% 21.5% 21.5% *Note: The figures above are the percent of all tests that are positive including people who are retesting. The figures here are total percent of people who test positive.
Blood Sugar (18)
Female Male
Grand Total
<18 0 1 1
18+ 61 46 107
Grand Total 61 47 108
Blood Sugar Individuals (18)
Female Male
Grand Total
<18 0 1 1
18+ 59 46 105
Grand Total 59 47 106
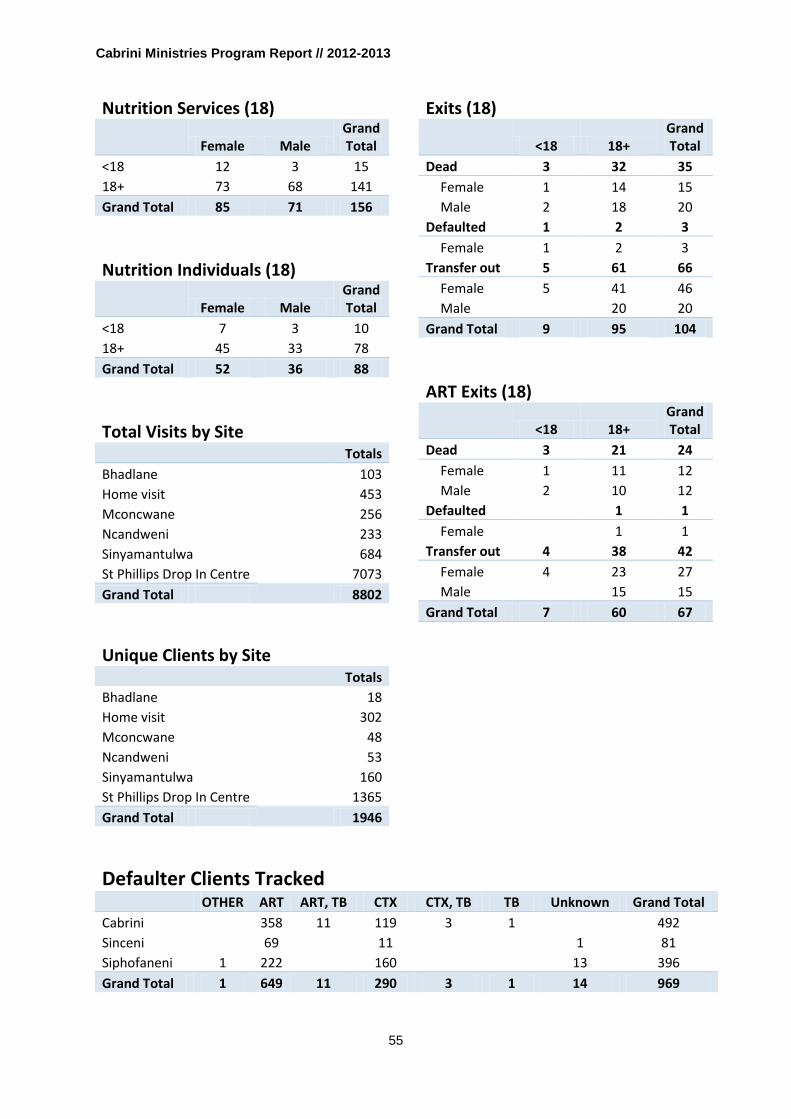
Cabrini Ministries Program Report // 2012-2013
55
Nutrition Services (18)
Female Male
Grand Total
<18 12 3 15
18+ 73 68 141
Grand Total 85 71 156
Nutrition Individuals (18)
Female Male
Grand Total
<18 7 3 10
18+ 45 33 78
Grand Total 52 36 88
Total Visits by Site Totals
Bhadlane 103
Home visit 453
Mconcwane 256
Ncandweni 233
Sinyamantulwa 684
St Phillips Drop In Centre 7073
Grand Total
8802
Unique Clients by Site
Totals
Bhadlane 18
Home visit 302
Mconcwane 48
Ncandweni 53
Sinyamantulwa 160
St Phillips Drop In Centre 1365
Grand Total
1946
Exits (18)
<18 18+
Grand Total
Dead 3 32 35
Female 1 14 15
Male 2 18 20
Defaulted 1 2 3
Female 1 2 3
Transfer out 5 61 66
Female 5 41 46
Male
20 20
Grand Total 9 95 104
ART Exits (18)
<18 18+
Grand Total
Dead 3 21 24
Female 1 11 12
Male 2 10 12
Defaulted
1 1
Female
1 1
Transfer out 4 38 42
Female 4 23 27
Male
15 15
Grand Total 7 60 67
Defaulter Clients Tracked
OTHER ART ART, TB CTX CTX, TB TB Unknown Grand Total
Cabrini
358 11 119 3 1
492
Sinceni
69
11
1 81
Siphofaneni 1 222
160
13 396
Grand Total 1 649 11 290 3 1 14 969

Cabrini Ministries Program Report // 2012-2013
56
Clinical Cascade Results and Exits
HIV Tests 716 100.0%
Negative 591 82.5%
Positive 125 17.5%
ART Eligible 83 66.4%
Initiated 68 81.9%
Via CD4 49 72.1%
Other 19 27.9%
Not Initiated 15 18.1%
Exit 14 93.3%
Dead 6 42.9%
Default / Refused 5 35.7%
Transfer 3 21.4%
Need Int 1 6.7%
Counseling 1 100.0%
Other 0 0.0%
ART Ineligible 42 33.6%
W/ CD4 28 66.7%
W/o CD4 14 33.3%
Exited 14 100.0%
Dead 0 0.0%
Default / Refused 3 21.4%
Transfer 11 78.6%
Need CD4 0 0.0%
Ongoing Client 0 -
HIV Test Only 0 -
Cabrini HIV Testing > CD4 > ART CascadeOctober 2012 - September 2013

Cabrini Ministries Program Report // 2012-2013
57
Cabrini Impact Mitigation Analysis of Services
Report for the period of Oct 2012 - Sep 2013
Child Care Enrollment
Hostel After Care
Respite Care
Acad. Support
One Time Bridge TOTAL
Male 18+ 13 16
12 8
49
Male <18 41 6 2 45 40 6 140
Female 18+ 9 14
7 13
43
Female <18 44 5 1 57 38 3 148
18+ 22 30 0 19 21 0 92
<18 85 11 3 102 78 9 288
Total 107 41 3 121 99 9 380
*Level 5 is included below in “One-Offs”
Child Care Enrollment Impact Nutrition Shelter Health Education Legal PSS Economic TOTAL
Male 18+ 29 29 29 41 29 49 16 49
Male <18 55 49 55 100 55 140 6 140
Female 18+ 23 23 23 30 23 43 14 43
Female <18 53 50 53 110 53 148 5 148
18+ 52 52 52 71 52 92 30 92
<18 108 99 108 210 108 288 11 288
Total 160 151 160 281 160 380 41 380
Child Care One-Offs
Nutrition Shelter Health Education Legal PSS Economic TOTAL
Male 18+ 6 0 5 2 2 10 0 10
Male <18 18 0 171 59 10 233 0 233
Female 18+ 39 0 2 8 0 11 0 11
Female <18 50 0 166 67 6 240 0 240
18+ 45 0 7 10 2 21 0 21
<18 68 0 337 126 16 473 0 473
Total 113 0 344 136 18 494 0 494
*”One-Offs” are services provided outside the levels of care. Details included below.

Cabrini Ministries Program Report // 2012-2013
58
Child Care Full Stats Nutrition Shelter Health Education Legal PSS Economic TOTAL
Male 18+ 35 29 34 43 31 59 16 59
Male <18 73 49 226 159 65 373 6 373
Female 18+ 62 23 25 38 23 54 14 54
Female <18 103 50 219 177 59 388 5 388
18+ 97 52 59 81 54 113 30 113
<18 176 99 445 336 124 761 11 761
Total 273 151 504 417 178 874 41 874
Health Care Stats
Nutrition Shelter Health Education Legal PSS Economic Total
Male 18+ 51 564 564 18 564
Male <18 8 141 141 5 141
Female 18+ 78 1058 1058 34 1058
Female <18 12 169 169 5 169
18+ 129 1622 1622 52 1622
<18 20 310 310 10 310
Total 149 1932 1932 62 1932
Total Impact Mitigation Stats
Nutrition Shelter Health Education Legal PSS Economic TOTAL
Male 18+ 86 29 598 43 31 623 34 623
Male <18 81 49 367 159 65 514 11 514
Female 18+ 140 23 1083 38 23 1112 48 1112
Female <18 115 50 388 177 59 557 10 557
18+ 226 52 1681 81 54 1735 82 1735
<18 196 99 755 336 124 1071 21 1071
Total 422 151 2436 417 178 2806 103 2806

Cabrini Ministries Program Report // 2012-2013
59
Oct 2012 Healthy Physicals Oct 2012 Assessments TOTALS TOTALS
Male 18+ 2 Male 18+ 8
Male <18 168 Male <18 40
Female 18+ 2 Female 18+ 13
Female <18 165 Female <18 38
18+ 4 18+ 21
<18 333 <18 78
Total 337 Total 99
*Full Dataset in Jan 2013 ME+R folder *Figures for Level 6 Care
Outreach Education TOTAL
Male 18+ 1
Male <18 42
Female 18+ 2
Female <18 45
18+ 3
<18 87
Total 90
*Estimated Age/Gender based on register
Camp Term 1 2013 TOTAL LVL 1-3 LVL 4 NEW
Male 18+ 16 12 4
Male <18 25 17 8
Female 18+ 13 7 4 2
Female <18 52 22 23 7
18+ 29 19 8 2
<18 77 39 31 7
Total 106 58 39 9
*Totals taken from 2013 Term 1 camp register

Cabrini Ministries Program Report // 2012-2013
60
Camp Term 2 2013 TOTAL LVL 1-3 LVL 4 Camp 1 NEW
Male 18+ 15 10 1 3 1
Male <18 21 12 0 3 6
Female 18+ 12 7 0 2 3
Female <18 44 14 6 18 6
18+ 27 17 1 5 4
<18 65 26 6 21 12
Total 92 43 7 26 16
*Totals taken from 2013 Term 2 camp register ***For assumptions based on level, refer to table above
Memory Box Camp, Q4 2013 TOTAL LVL 1-3 NEW
Male 18+ 0 0 0
Male <18 7 4 3
Female 18+ 0 0 0
Female <18 9 4 5
18+ 0 0 0
<18 16 8 8
Total 16 8 8
*Totals taken from 2013 Memory Box Camp Register
Stand Alone One Offs -- Q1-2 Stand Alone One Offs TOTAL Nutrition Shelter Health Education Legal PSS Economic
Male 18+ 0 Male <18 4 1
2 1
Female 18+ 0 Female <18 9 3
3 3
18+ 0
0 0 0 0 0 0
<18 13 4 0 0 0 5 4 0
Total 13 4 0 0 0 5 4 0

Cabrini Ministries Program Report // 2012-2013
61
Stand Alone One Offs -- Q3 TOTAL Nutrition Shelter Health Education Legal PSS Economic
Male 18+ 1
1 1 Male <18 9
3 6 6
Female 18+ 1
1 Female <18 3
1 2 3
18+ 2 0 0 0 0 1 2 0
<18 12 0 0 0 4 8 9 0
Total 14 0 0 0 4 9 11 0
*Compiled from Social Service case files -- includes unique services occurring in Q3
Stand Alone One Offs -- Q4 TOTAL Nutrition Shelter Health Education Legal PSS Economic
Male 18+ 5
3
1 5 Male <18 7
3 5 2 7
Female 18+ 1
1
1 Female <18 6
1 3 1 6
18+ 6
3 1 1 6 <18 13
4 8 3 13
Total 19
7 9 4 19 *Compiled from Social Service case files -- only includes interventions occurring in Q4
**Above tables reflect only individuals receiving unique services
Combined One Offs TOTAL Nutrition Shelter Health Education Legal PSS Economic
Male 18+ 10 6 0 5 2 2 10 0
Male <18 233 18 0 171 59 10 233 0
Female 18+ 11 39 0 2 8 0 11 0
Female <18 240 50 0 166 67 6 240 0
18+ 21 45 0 7 10 2 21 0
<18 473 68 0 337 126 16 473 0
Total 494 113 0 344 136 18 494 0
*Total Previously uncounted clients **Includes impact from events above.

Cabrini Ministries Program Report // 2012-2013
62

Cabrini Ministries would like to express their gratitude to all
who have made this program report possible:
All the staff who implement activities daily caring for and
loving their neighbors
To Phindile Tfwala and rest of the data management
team for their data compilation
To Joseph DalleMolle, Beth Kickert, and Katie McCaskie
for narrative composition and editing
Especially to Ben Kickert for coordinating the production
of this work; for his integrity and the generous,
passionate use of his intelligence and skill for the Mission
of Cabrini Ministries.

CABRINI MINISTRIES SWAZILAND
St. Philips Mission
Mhlatuze, Lubombo
Box 5183
Manzini, M200
Swaziland, Africa
(o) +268.2343.4944
(f): +268.2518.5598
www.cabriniministries.org
A ministry of the Missionary Sisters of the Sacred Heart