
prognosis question hrm 777
6
Carlos A. Cuello Garcia MD, PhD candidate Student No. 1352724 Health Research Methodology Program Department of Clinical Epidemiology and Biostatistics HRM 777 Methods for Diagnostic and Prognostic Research URINARY TRACT INFECTIONS AND VESICOURETERAL REFLUX DURING INFANCY AND THEIR ROLE IN THE PROGNOSIS OF RENAL DAMAGE AND END-STAGE RENAL DISEASE DERIVATION OF A PROGNOSTIC MODEL Prognosis research question Hamilton, Ontario June 18, 2015
-
Upload
carlos-cuello -
Category
Health & Medicine
-
view
121 -
download
0
Transcript of prognosis question hrm 777

Carlos A. Cuello GarciaMD, PhD candidateStudent No. 1352724 Health Research Methodology ProgramDepartment of Clinical Epidemiology and Biostatistics
HRM 777 Methods for Diagnostic and Prognostic Research
URINARY TRACT INFECTIONS AND VESICOURETERAL REFLUX DURING INFANCY AND THEIR ROLE IN THE PROGNOSIS OF RENAL DAMAGE AND END-STAGE RENAL DISEASE
DERIVATION OF A PROGNOSTIC MODEL
Prognosis research question
Hamilton, OntarioJune 18, 2015
• Among otherwise healthy infants (<36 months of age)
with a first febrile urinary tract infection (UTI), does
the use of several prognostic factors built into a
prognostic model, help predict the probability of renal
damage and end-stage renal disease (ESRD) during
childhood and adolescence?
Research question
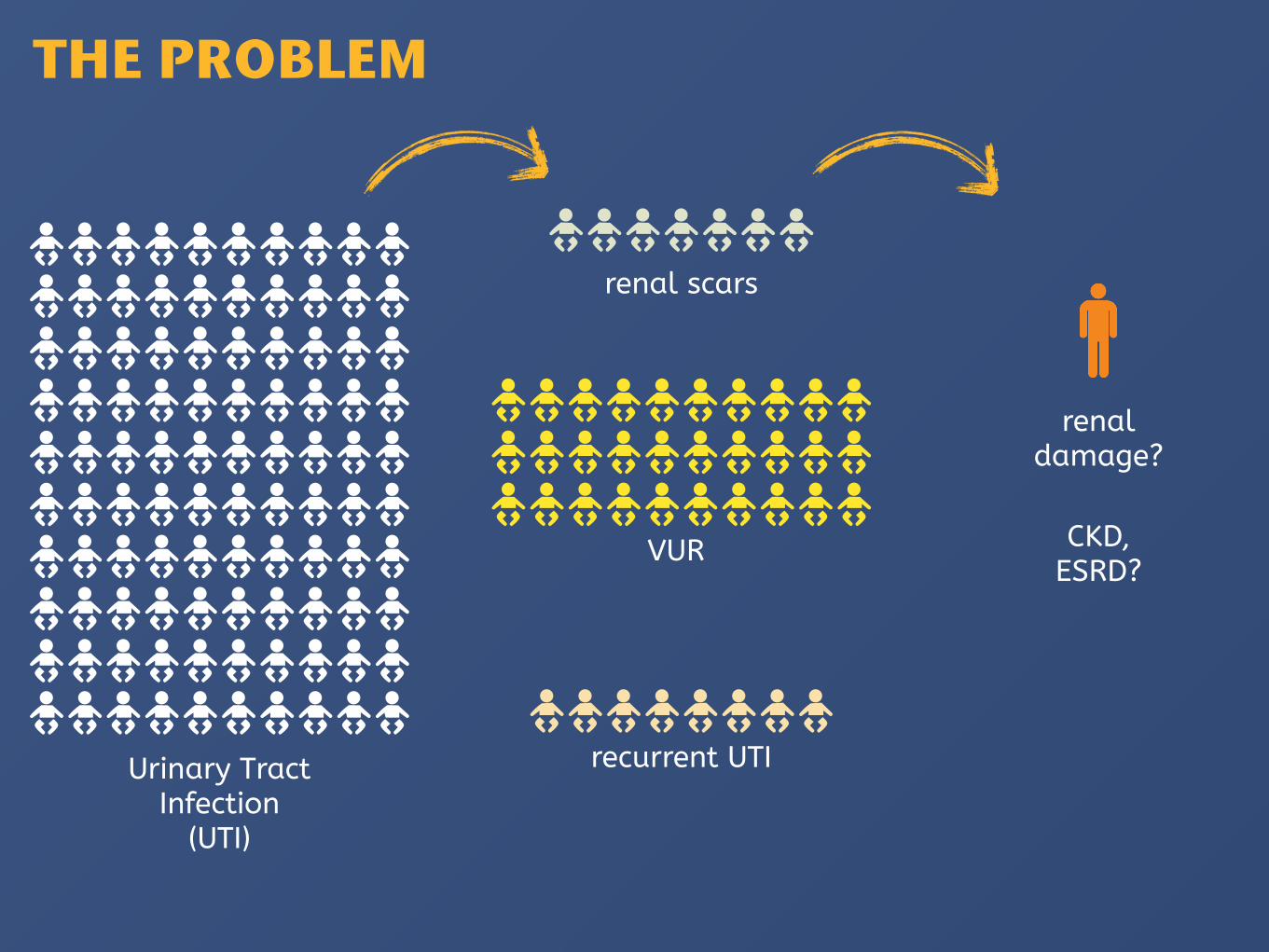
renal scars
VUR
recurrent UTI
renal damage?
CKD, ESRD?
Urinary Tract Infection
(UTI)
THE PROBLEM
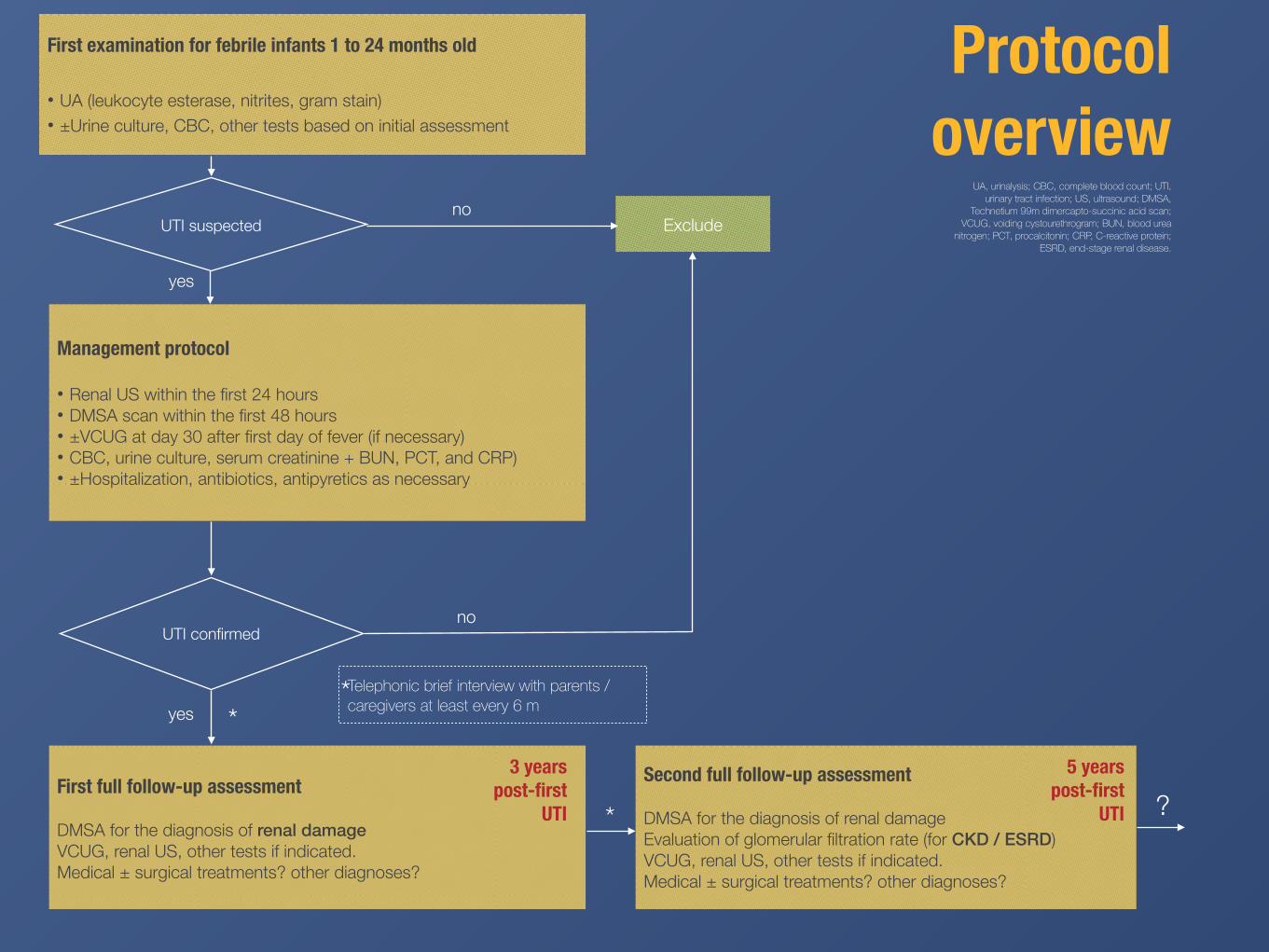
Exclude
First examination for febrile infants 1 to 24 months old
• UA (leukocyte esterase, nitrites, gram stain) • ±Urine culture, CBC, other tests based on initial assessment
Management protocol
• Renal US within the first 24 hours • DMSA scan within the first 48 hours • ±VCUG at day 30 after first day of fever (if necessary) • CBC, urine culture, serum creatinine + BUN, PCT, and CRP) • ±Hospitalization, antibiotics, antipyretics as necessary
UTI suspected
UTI confirmed
First full follow-up assessment
DMSA for the diagnosis of renal damage VCUG, renal US, other tests if indicated. Medical ± surgical treatments? other diagnoses?
Second full follow-up assessment
DMSA for the diagnosis of renal damage Evaluation of glomerular filtration rate (for CKD / ESRD) VCUG, renal US, other tests if indicated. Medical ± surgical treatments? other diagnoses?
Protocol overview
no
yes
3 years post-first
UTI
*
UA, urinalysis; CBC, complete blood count; UTI, urinary tract infection; US, ultrasound; DMSA,
Technetium 99m dimercapto-succinic acid scan; VCUG, voiding cystourethrogram; BUN, blood urea
nitrogen; PCT, procalcitonin; CRP, C-reactive protein; ESRD, end-stage renal disease.
no
yes
5 years post-first
UTI * ?
Telephonic brief interview with parents / caregivers at least every 6 m*
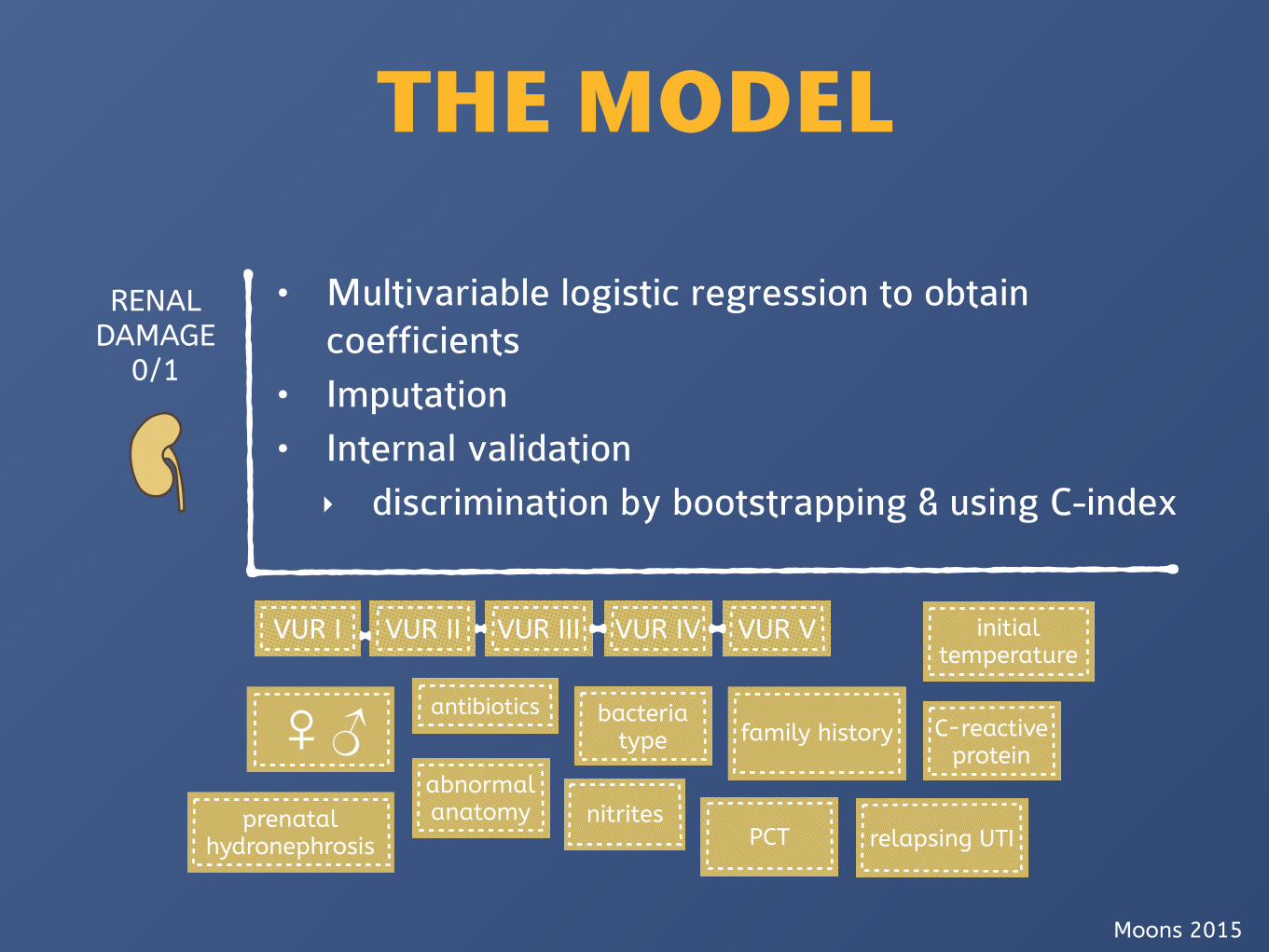
RENAL DAMAGE
0/1
bacteria type♀♂ antibiotics
VUR I VUR II VUR III VUR IV VUR V
family history
prenatal hydronephrosis
abnormal anatomy
PCT
C-reactive protein
nitrites
initial temperature
THE MODEL
relapsing UTI
• Multivariable logistic regression to obtain coefficients
• Imputation • Internal validation ‣ discrimination by bootstrapping & using C-index
Moons 2015

• We’re still uncertain if UTIs in infancy ± VUR ± renal scars cause CKD / ESRD, and how strong the association is.
• Limitations
‣ Physicians still have problems diagnosing CKD (overdiagnosis?)
‣ It might require a very long time, and lots of patients
COMMENTARY













![8 Eigenvectors and the Anisotropic Multivariate Gaussian …jrs/189s17/lec/08.pdf · 2017. 2. 14. · 777 777 777 777 777 5 [diagonal matrix of eigenvalues] Defn. of “eigenvector”:](https://static.fdocuments.us/doc/165x107/61216a6db677231115104a22/8-eigenvectors-and-the-anisotropic-multivariate-gaussian-jrs189s17lec08pdf.jpg)




