Prognosis of malignant lymphoma in dogs and correlation to ... · There are many similarities...
39
Faculty of Veterinary Medicine and Animal Science Department of Clinical Sciences Prognosis of malignant lymphoma in dogs and correlation to thymidine kinase (TK1) - a retrospective study Elin Falk Uppsala 2018 Degree Project 30 credits within the Veterinary Medicine Programme ISSN 1652-8697 Examensarbete 2018:14
Transcript of Prognosis of malignant lymphoma in dogs and correlation to ... · There are many similarities...

Faculty of Veterinary Medicine
and Animal Science
Department of Clinical Sciences
Prognosis of malignant lymphoma in dogs and correlation to thymidine kinase (TK1) - a
retrospective study
Elin Falk
Uppsala 2018
Degree Project 30 credits within the Veterinary Medicine Programme
ISSN 1652-8697 Examensarbete 2018:14

Prognosis of malignant lymphoma in dogs and correlation to thymidine kinase (TK1) - a retrospective study Prognos vid malignt lymfom hos hund och korrelation till thymidinkinas (TK1) - en retrospektiv studie
Elin Falk Supervisor: Henrik Rönnberg, Department of Clinical Sciences
Assistant Supervisor: Sara Saellström, University Animal Hospital in Sweden, Small animal clinic
Examiner: Jens Häggström, Department of Clinical Sciences
Degree Project in Veterinary Medicine Credits: 30 Level: Second cycle, A2E Course code: EX0830 Place of publication: Uppsala Year of publication: 2018 Number of part of series: Examensarbete 2018:14 ISSN: 1652-8697 Online publication: http://stud.epsilon.slu.se Key words: lymphoma, malignant lymphoma, thymidine kinase, TK1, canine, dog, prognosis Nyckelord: lymfom, malignt lymfom, thymidinkinas, TK1, hund, prognos (key words in Swedish)
Sveriges lantbruksuniversitet
Swedish University of Agricultural Sciences
Faculty of Veterinary Medicine and Animal Science
Department of Clinical Sciences


SUMMARY
Malignant lymphoma is the most common canine hematopoetic neoplasm, with an estimated
incidence rate of 20-100 cases per 100,000 dogs. Malignant lymphoma can arise in any organ
containing lymphoid tissue and is characterized by malignant proliferation of lymphoid cells.
Lymphomas most commonly occur in middle-age to older dogs, where the age category six to
ten years seems to be predisposed. Although any dog breed can be affected, middle-sized to
large dog breeds are overrepresented.
There are many similarities between canine lymphoma and human non-Hodgkin lymphoma
(NHL) and the canine lymphoma serves as a good large-animal model for the human NHL.
Thymidine kinase is a cellular enzyme involved in the salvage pathway of DNA-synthesis.
Thymidine kinase 1 (TK1) is regulated by the cell cycle and is located in the cytoplasm.
Moreover, TK1 is converting thymidine to thymidine monophosphate, and is related to DNA
replication and cell proliferation, which makes it possible to use as a proliferation marker in
malignant tumors. Thymidine kinase 1 activity is present in the early S-phase of cell division
in normal cells. However, in abnormal cells the activity of TK1 is often much higher. Previous
studies have shown that TK1 is useful in diagnosis and prognosis in humans and dogs with
malignant lymphoma.
The challenging area with canine lymphoma is rarely to set the diagnosis, but to predict the
prognosis and monitor the remission status in an objective way. Moreover, it is a challenge to
detect relapse in treated patients. The purpose of the study was to compare initial blood
parameters, for example TK and CRP, with clinical symptoms, clinical stage and prognosis.
The aim was to improve the prognostication and thereby be able to select the right patients for
further treatment.
The results of the study showed that there were no significant correlation between a higher
initial TK value and a shorter survival time and poorer prognosis. Neither could a high CRP
level, hypercalcemia, anemia, a high clinical stage, a T-cell lymphoma, B symptoms nor a high
grade tumor be correlated to a shorter survival time. The most important thing for a longer
survival time was, according to this study, treatment with the ADRIA-plus protocol. This
treatment resulted in a significantly longer survival time than the treatment with prednisolone
or doxorubicin alone. Further studies are needed to investigate if the above mentioned
parameters are useful in prognostication in dogs with malignant lymphoma.

SAMMANFATTNING
Malignt lymfom är den vanligaste hematopoetiska neoplasin som drabbar hundar, med en
incidensrat på 20-100 fall per 100 000 hundar. Malignt lymfom kan uppstå i alla organ som
innehåller lymfoid vävnad, och karaktäriseras av malign proliferation av lymfoida celler.
Lymfom drabbar framför allt medelålders och äldre hundar, med störst risk för hundar i
åldersgruppen 6-10 år. Alla raser kan drabbas av lymfom, men medelstora och stora hundraser
är klart överrepresenterade.
Det finns många likheter mellan malignt lymfom hos hund och humant non-Hodgkins lymfom
(NHL) och hunden fungerar i detta fall som en bra stordjursmodell för humana NHL.
Thymidinkinas är ett cellulärt enzym som är involverat i "salvage pathway" i DNA-syntesen.
Thymidinkinas 1 (TK1) regleras av cellcykeln och finns lokaliserat i cytoplasman. TK1
omvandlar thymidin till thymidinmonofosfat, och kopplas till DNA-replikation och
cellproliferation, vilket möjliggör användandet av TK1 som en proliferationsmarkör hos
maligna tumörer. TK1-aktivitet förekommer i tidig S-fas vid celldelning i normala celler. I
onormala celler är däremot TK1-aktiviteten ofta mycket högre. Tidigare studier har visat att
TK1 är användbar vid diagnostisering och prognostisering av malignt lymfom hos både
människor och hundar.
Utmaningen med malignt lymfom hos hundar är sällan att ställa diagnosen, utan att förutspå
prognos och monitorera remissionsstatus på ett objektivt sätt. Det är dessutom en utmaning att
upptäcka sjukdomsåterfall hos redan behandlade patienter. Syftet med denna studie var att
jämföra initiala blodparametrar, såsom TK och CRP, med kliniska symtom, klinisk gradering
och prognos. Målet var att förbättra prognostiseringen och därmed möjligheten att välja ut rätt
patienter som ska kunna genomgå behandling.
Resultaten i denna studie visade att det inte fanns någon signifikant korrelation mellan ett högre
initialt TK-värde och en kortare överlevnadstid eller sämre prognos. Det fanns inte heller någon
korrelation mellan en kortare överlevnadstid och ett högt CRP, hyperkalcemi, anemi, ett högt
kliniskt stadium, T-cellslymfom, B-symtom eller en histologiskt höggradig tumör. I denna
studie var den viktigaste faktorn för en längre överlevnadstid att hunden genomgick en
behandling med ADRIA-plus-protokollet. Denna behandling ledde till en signifikant längre
överlevnadstid jämfört med endast kortison- eller doxorubicinbehandling. Fler studier krävs för
att vidare undersöka om ovan nämnda parametrar är värdefulla i prognostisering hos hundar
med malignt lymfom.

CONTENT
INTRODUCTION ................................................................................................................................. 1
LITERATURE REVIEW ..................................................................................................................... 2
Anatomy of the lymphatic system ...................................................................................................... 2
Classification ...................................................................................................................................... 3
Diagnosis ............................................................................................................................................ 5
Clinical pathology ......................................................................................................................... 5
Diagnostic imaging ....................................................................................................................... 5
Cytology and histology ................................................................................................................. 5
Treatment ........................................................................................................................................... 6
Singel agent (mono) therapy ......................................................................................................... 6
Multidrug chemotherapy ............................................................................................................... 7
Side effects .................................................................................................................................... 8
Acute Tumor Lysis Syndrome (ATLS) .............................................................................................. 9
Drug resistance ................................................................................................................................... 9
Enzymatic function of thymidine kinase 1 ......................................................................................... 9
C-reactive protein and lymphoma .................................................................................................... 10
MATERIAL AND METHODS .......................................................................................................... 10
Background data ............................................................................................................................... 12
Breed ........................................................................................................................................... 12
Sex, weight and age ..................................................................................................................... 13
Blood analyzes ............................................................................................................................ 14
Immunophenotype ....................................................................................................................... 14
Tumor grade ................................................................................................................................ 14
Clinical stage ............................................................................................................................... 15
Treatment method ....................................................................................................................... 15
RESULTS ............................................................................................................................................. 15
TK levels in serum ........................................................................................................................... 15
CRP levels in serum ......................................................................................................................... 16
Calcium levels in serum ................................................................................................................... 17
Hematocrit level ............................................................................................................................... 17
Clinical stage .................................................................................................................................... 18
Immunophenotype ............................................................................................................................ 19
Tumor grade ..................................................................................................................................... 19
Symptoms ......................................................................................................................................... 20
Treatment method ............................................................................................................................ 20
DISCUSSION ...................................................................................................................................... 21
Age, weight, breed and sex .............................................................................................................. 21
Thymidine kinase ............................................................................................................................. 22
Tumor grade and immunophenotype ............................................................................................... 23
Anemia, hypercalcemia and clinical symptoms ............................................................................... 24
Limitations of the study .................................................................................................................... 24
CONCLUSION .................................................................................................................................... 25
REFERENCES .................................................................................................................................... 26


1
INTRODUCTION
Malignant lymphoma (also known as lymphoma or lymphosarcoma) is the most common
canine hematopoetic neoplasm, with an estimated incidence rate of 20-100 cases per 100,000
dogs (Zandvliet, 2016). Malignant lymphoma can arise in any organ containing lymphoid
tissue, and is characterized by malignant proliferation of lymphoid cells (Argyle et al., 2009).
Lymphomas most commonly occur in middle-age to older dogs. Dogs below four years of age
are less likely to develop lymphoma, and the age category six to ten years seems to be
predisposed (Simon et al., 2008; Villamil et al., 2009; Mirkes et al., 2014). Although malignant
lymphoma can affect any dog breed, middle-sized to large dog breeds are overrepresented.
Some of the predisposed breeds are Bullmastiff, Boxer, Bernese mountain dog, Dogo de
Bordeaux, Golden Retriever, German Shepherd, Labrador retriever and Scottish terrier
(Villamil et al., 2009; Vezzali et al., 2010; Elliott et al., 2013). Heritable factors may contribute
to the increased frequency in these breeds (Elvers et al., 2015; Tonomura et al., 2015).
Moreover, intact female dogs seem to have a decreased risk in developing malignant
lymphoma. However, the risk does not differ between neutered female dogs and male dogs
(Villamil et al., 2009).
There are many similarities between canine lymphoma and human non-Hodgkin lymphoma
(NHL), including clinical symptoms, molecular biology, treatment and treatment results. The
dog's genome has been sequenced and the dog breeds represent closed gene pools (Berlin et al.,
2005). Furthermore, many dog owners want to treat their dogs diagnosed with malignant
lymphoma. This makes the canine lymphoma a good large-animal model for the human NHL
(Zandvliet, 2016).
There is no established cause for canine lymphoma to this day. Several predisposing factors
have been suggested, for example living near industrial areas, exposure to chemicals, living
near waste incinerators, radioactive or polluted sites and exposure to magnetic fields. Many
other animal species have a species-specific leukemia virus, which makes it possible to believe
that a canine "lymphoma virus" may exist. However, a viral etiology is still not generally
accepted (Zandvliet, 2016).
Thymidine kinase (TK) is a cellular enzyme involved in the salvage pathway of DNA-synthesis.
There are two different forms of TK; TK1 and TK2. Thymidine kinase 1 is regulated by the cell
cycle and is located in the cytoplasm. Thymidine kinase 2 is located in the mitochondria and is
expressed in all cells, without influence of the stage in the cell cycle (Arnér & Eriksson, 1995).
Thymidine kinase 1 is converting thymidine to thymidine monophosphate, and is related to
DNA replication and cell proliferation, which makes it possible to use as a proliferation marker
in malignant tumors (He et al., 2010). The TK1 activity is present in the early S-phase of cell
division in normal cells. However, in abnormal cells the activity of TK1 is often much higher
(Hengstschläger et al., 1994).
Previous studies have shown that TK1 (TK onwards) is useful in diagnosis and prognosis in
humans and dogs with malignant lymphoma. Furthermore, TK can be used in
immunohistochemistry for RNA/protein expression in tissue specimens and for activity or

2
protein/peptide levels in serum from patients. In humans, TK is used in measuring several forms
of blood malignancies, as well as solid tumors, for example breast and lung cancer. However,
the results are poor on solid tumors in dogs. Canine solid tumors are hard to distinguish from
normal controls because they tend to induce much less of a response in terms of systemic
enzyme activity (von Euler & Eriksson, 2011; Leijon, 2013).
The challenging area of canine lymphoma is rarely to set the diagnosis, but to predict the
prognosis and monitor the remission status in an objective way. Moreover, it is a challenge to
detect relapse in treated patients. The purpose of the study is to compare initial blood
parameters, for example TK and CRP, with clinical symptoms, clinical stage and prognosis.
The aim is to improve the prognostication and thereby be able to select the right patients for
further treatment. The aim is also to find a better method to select patients who may need more
frequent monitoring after completed treatment.
The study will focus on the following set of questions:
Can the initial TK level in serum be used to predict the prognosis and survival time for
a patient diagnosed with malignant lymphoma?
Can the initial CRP level, together with clinical symptoms and stage be used for
prognostication?
Are the initial calcium and hematocrit levels, as well as the clinical stage,
immunophenotype, tumor grade and clinical symptoms correlated with prognosis and
survival time?
The hypothesis is that the initial TK level in serum can be used to predict the prognosis and
survival time of a dog with malignant lymphoma. Another hypothesis is that the CRP level may
be used for prognostication, but only together with the clinical stage and symptoms and not as
a single analysis. Furthermore, it is believed that hypercalcemia, T-cell lymphomas and a high
clinical stage are correlated to a shorter survival time.
LITERATURE REVIEW
Anatomy of the lymphatic system
The components of the lymphatic system are divided into two groups; the primary organs and
the secondary organs. The primary organs consist of the thymus gland and the bone marrow.
These organs regulate the production and differentiation of lymphocytes. Both T- lymphocytes
and B-lymphocytes are derived from stem cells in the bone marrow. The B-cells mature in the
bone marrow, while the immature T-cells are transported to the thymus for their final
development. Mature B- and T-lymphocytes are released into the circulation and transported to
the secondary lymphoid organs, where most of them will remain. The secondary organs include
the lymph nodes, lymphatic vessels, aggregated lymphoid tissue and the spleen.
Within the secondary organs, the lymphocytes undergo antigen-dependent proliferation and
differentiation into effector cells. The effector cells can either attend to the disposal of particular
antigens or provide the memory cells that become temporarily inactive. While the primary

3
lymphoid organs are only involved in the immune function, the secondary organs are involved
in the immunity, fat absorption and fluid regulation.
The lymphatic vessels link together the secondary lymphoid organs and makes a connection to
the cardiovascular system. They provide a route where the lymph can flow from the body tissues
to the heart. The lymph is a fluid collected from the interstitial spaces into lymphatic capillaries.
The lymph is transported in the lymphatic vessels through the lymph nodes, where a filtration
of the lymph takes place before it reaches the large ducts and enters the blood circulation in the
upper chest.
The lymph nodes are encapsulated structures distributed throughout the body. They are
comprised of several lymph nodules, which are compartments with several B-cells, T-cells and
macrophages. Unfiltered lymph is delivered through several afferent vessels. The lymph is then
filtered for antigens and particular matter, and an immune response may be generated if it is
necessary. The filtered lymph leaves the lymph node through one or two efferent vessels.
The spleen is composed of two types of tissue; the red and the white pulp. The red pulp is
mostly associated with blood storage and the destruction of old erythrocytes. The white pulp is
formed of lymph nodules, explaining why the tissue has lymphogenic and phagocytic
properties.
The aggregated lymphoid tissues are collections of non encapsulated lymphoid tissues of
various size and organization, for example the tonsils in the oral cavity and Peyer´s patches in
the lining of the small intestines. The main purpose of the aggregated lymphoid tissue is to
prevent infections from developing at the mucosal surfaces, where microorganisms easily can
enter the body (Dyce et al., 2010).
Classification
There are different types of lymphomas, which can be named by their anatomical localization.
These are listed in Table 1 (Argyle et al., 2009).
Table 1. Anatomic classification of lymphomas and some of the clinical symptoms they may cause
Type of lymphoma: Clinical presentation:
Multicentric lymphoma Localized or generalized lymphadenopathy with or without
hepatosplenomegaly. May cause respiratory distress and edema
formation if the lymph nodes are reducing the venous flow.
Thymic lymphoma Anterior mediastinal mass. May cause pleural effusion, leading to
respiratory signs.
Alimentary lymphoma With or without a palpable abdominal mass. May cause vomiting,
diarrhea and weight loss.
Cutaneous lymphoma Cutaneous tumors which rapidly progress to cause systemic disease.
Hepatosplenic
lymphoma
Causes hepatosplenomegaly. May cause vomiting, diarrhea and weight
loss.
Nasal lymphoma May cause nasal discharge, epistaxis, epiphora and facial deformity.
Ocular lymphoma May cause uveitis with or without hypema.

4
The most common anatomical form of lymphoma is the multicentric form, accounting for
approximately 75 % of all canine lymphomas (Argyle et al., 2009; Vezzali et al., 2010). The
diagnosis is often confirmed with a fine-needle aspirate (FNA) or a biopsy from an enlarged
lymph node. There is also a histopathological classification of the canine lymphomas, where
the tumors are divided into a low grade (also known as small-cell or lymphocytic lymphoma)
and a high grade (also known as large-cell or lymphoblastic lymphoma). High grade lymphoma
is the most common form in dogs and results in death within weeks from diagnosis, if
appropriate treatment is not initiated (Marconato et al., 2011). The low grade lymphoma is
characterized by an indolent clinical course and is correlated with an average survival time of
4.4 years after diagnosis. The low grade lymphomas represents 5.3-29 % of all canine
lymphomas (Flood-Knapik et al., 2013). Furthermore, it is possible to classify the tumors as T-
cell (CD3 positive) or B-cell (CD79 positive) lymphomas using immunophenotyping methods.
B-cell lymphomas accounts for approximately 80-85 % of the canine lymphomas (Vezzali et
al., 2010) and are associated with a better prognosis and a longer median survival time than T-
cell lymphomas (Argyle et al., 2009; Elliott et al., 2013).
Clinical staging enables a more accurate prognostication and can be done when the diagnosis
is stated. The World Health Organization (WHO) staging scheme is the most used scheme and
it is appropriate for dogs with multicentric lymphoma. This scheme takes into account the extent
of the peripheral lymph node involvement, involvement of liver, spleen, bone marrow and
nonlymphoid organs (table 2) (Owen et al., 1980).
Table 2. Clinical staging for multicentric lymphoma according to The World Health Organization
(WHO)
Stage
I A single lymph node affected, or lymphoid tissue in a single organ (excluding bone
marrow)
II Two or more lymph nodes affected in a regional area (i.e., cranial or caudal to the
diaphragm) ± tonsils
III Generalized lymph node involvement
IV Involvement of liver and/or spleen (± stage III)
V Manifestation in the blood and involvement of bone marrow and/or other organ systems
(± stages I-IV)
Substage
a Without clinical signs
b With clinical signs, i.e., fever, weight loss, hypercalcemia

5
Diagnosis
Clinical pathology
Most dogs diagnosed with malignant lymphoma show a wide range of non-specific
abnormalities on the hemathological and clinical chemistry profile. A mild to moderate non-
regenerative anemia is seen in many dogs. Both leukopenia and leukocytosis are described and
the latter is usually combined with neutrophilia representing an inflammatory response. A mild,
asymptomatic trombocytopenia is common (Gavazza et al., 2008). Hypercalcemia is seen in
10-15 % of the dogs and is often associated with T-cell lymphoma. The hypercalcemia results
from the parathyroid hormone-related peptide (PTH-rP) by CD4+ T-cell lymphoblasts
(Ruslander et al., 1997; Zandvliet, 2016). Hypercalcemia reduces the response to antidiuretic
hormone (ADH), leading to polyuria (Zandvliet, 2016).
Dogs with malignant lymphoma often have a higher TK value than healthy dogs. The TK value
also seems to correlate with stage and prognosis of the disease (von Euler et al., 2004; Elliott
et al., 2013). Measurements of C-reactive protein (CRP) levels has a low sensitivity and
specificity for diagnosing malignant lymphoma, and needs to be combined with clinical data to
be useful as a diagnostic test (Mirkes et al., 2014).
Elevated liver enzymes or kidney values may be due to the lymphoma affecting the liver or the
spleen, but more often it is caused by reactive hepatopathy and dehydration as a secondary
effect of the lymphoma. Proteinuria is a common finding in dogs with multicentric lymphoma,
even though urinanalysis is not routinely performed in the diagnostics. Bone marrow
involvement (leukemia) is reported in up to 55 % of the dogs (Raskin & Krehbiel, 1989).
However the bone marrow involvement cannot be detected accurately from peripheral blood
counts. The most commonly used method today is a cytologic examination of a single bone
marrow aspiration sample, which is proved sufficient for diagnosing bone marrow involvement
(Martini et al., 2015; Zandvliet, 2016).
Diagnostic imaging
Thoracic and abdominal radiographs often show unspecific findings which can be used to see
if lymphoma is a differential diagnosis rather than to set the diagnosis. Thoracic radiographs
can reveal thoracic lymphadenopathy, pulmonary infiltrates and a cranial mediastinal mass.
Ultrasonography of the abdomen and lymph nodes is a very useful diagnostic tool, where one
can assess lymph node size and architecture, as well as hepatic and/or spleen involvement
(Crabtree et al., 2010; Zandvliet, 2016). However, abdominal ultrasonography is not as useful
in the diagnostics of alimentary lymphoma, because they tend to have non-specific, or absent,
findings (Frances et al., 2013). A computed tomography (CT) scan may be useful to evaluate
the extent of a tumor but cannot be used to set a specific diagnose, for example differentiate a
thymoma from a mediastinal lymphoma (Yoon et al., 2004).
Cytology and histology
A cytological examination of a fine-needle aspirate from an enlarged lymph node is an easy,
cheap and minimally invasive method to diagnose high grade canine lymphomas. However,
cytology is sometimes insufficient for diagnosing low grade lymphomas or characterizing

6
atypical lymphoid proliferations (Sözmen et al., 2005; Zandvliet, 2016). A histological
examination of a biopsy may improve the diagnosis of a low-grade lymphoma. Furthermore,
the histological examination of a biopsy will allow further classification of the lymphoma.
Histological characterization of the lymphoma includes growth pattern, nuclear size and
morphology, mitotic index and immunophenotype (Zandvliet, 2016).
Treatment
Generally, the aim of the treatment is not to cure the patient, but to give the dog a good quality
of life striving to get the lymphoma in to remission for as long as possible. Without treatment,
most dogs with lymphoma die within 4-6 weeks from diagnosis (Zandvliet, 2016). A systematic
therapy is required to achieve the best possible outcome (Argyle et al., 2009; Marconato et al.,
2011). In general, dogs diagnosed with multicentric lymphoma have the best response to
treatment. However, only 10 % of the dogs with multicentric lymphoma who have been treated
with cytotoxic agents survive more than two years from diagnosis (Marconato et al., 2011).
Dogs with thymic lymphoma often have a good initial response to therapy, but the remission
period is often shorter than for the multicentric form. However, the alimentary form, as well as
the cutaneous form and the hepatosplenic form, are often difficult to treat (Argyle et al., 2009).
There is a significant difference in prognosis between a T-cell lymphoma and a B-cell
lymphoma, where the latter one is more susceptible to chemotherapy and is correlated to a better
prognosis than the former one (Ponce et al., 2004).
Singel agent (mono) therapy
Glucocorticoids - Prednisone
Glucocorticoids are routinely used as a palliative treatment in dogs suffering from malignant
lymphoma. The glucocorticoids induce apoptosis of lymphocytes and lymphoblasts (Smith &
Cidlowski, 2010). Most dogs will experience a partial to complete response, but the remission
duration is often short and lasts approximately two to four months (Squire et al., 1973; Bell et
al., 1984; Argyle et al., 2009). Moreover, dogs pretreated with glucocorticoids tend to have a
lower probability to enter complete remission after chemotherapy treatment (Gavazza et al.,
2008; Marconato et al., 2011).
Anthracyclines
The first anthracyclines were isolated from Streptomyces spp., explaining why they are
classified as antitumor antibiotics. Anthracyclines induce protein-linked breaks in the DNA and
inhibit re-ligation of DNA cleaved by topoisomerase type II. Furthermore, the anthracyclines
may also insert a part of their structure between two adjacent base pairs in the DNA strand. The
anthracyclines may also form free radicals that can cause oxidative damage to cellular proteins
by undergoing iron-catalyzed reduction. The anthracyclines are non-cell-cycle specific drugs
which are used extensively in veterinary medicine. Frequently used anthracyclines are
doxorubicin, dactinomycin and mitoxantrone (Argyle et al., 2009).
If doxorubicin is used as a single agent treatment, the drug is given as a slow intra venous
infusion every 21 days. Usually five doses are given over 15 weeks. The drug has a complete
remission rate of 59-85 % and the remission duration is up to seven months (Simon et al.,

7
2008). The remission duration is shorter than after using a multidrug chemotherapy protocol
and doxorubicin as a single agent treatment should only be used as a palliative treatment. Dogs
with decreased heart contractility due to heart disease should not be treated with doxorubicin,
because of its potential cardiotoxicity. Furthermore, it is very important that doxorubicin is
given strictly intra venously. Extravascular injection causes severe tissue damage and necrosis
that may require amputation or euthanasia (Argyle et al., 2009).
Alkylating agents
The alkylating agents are the oldest group of antitumor drugs. These drugs consist of small
molecules that bind covalently to electron-rich parts on biological molecules. The binding of
the drugs to cellular DNA is believed to be the lethal event. Cell death may occur when the cell
tries to replicate the damaged DNA. Repair enzymes may worsen the damage process by
creating base deletions or misreplacements of single or double strand breaks. The alkalyting
agents are non-cell-cycle specific. Many alkylating agents are frequently used in veterinary
oncology, including mechlorethamine, melphalan, chlorambucil, cyclophosphamide and
lomustine (Morris & Dobson, 2008).
Lomustine is given per os every 21 days until progressive disease or hepatotoxicity develops.
Lomustine is more often used as a rescue treatment for relapsed multicentric lymphoma and for
cutaneous lymphoma (mycosis fungoides) (Argyle et al., 2009). Rescue protocols are used as
an attempt to rescue a patient back to remission, if they have failed to achieve remission as a
result of the first line therapy. The remission response rate of lomustine is 30-50 % and the
median response duration is one to three months from the therapy start (Sauerbrey et al., 2007;
Argyle et al., 2009). Most bioavailability data come from human studies and the oral
chemotherapy drugs, such as lomustine, are designed for the human gastrointestinal tract. There
is not much information about the absorption in veterinary patients to this day (Argyle et al.,
2009).
L-Asparaginase
L-asparaginase is an enzyme that inhibits the protein synthesis by the depletion of L-asparagine
sources, which is necessary for transformed lymphoid cells to proliferate (MacEwen et al.,
1992). Unlike lymphoma cells, normal cells synthesize their own asparagine which explains
why they do not get affected by the L-asparaginase (Argyle et al., 2009). The problem with L-
asparaginase treatment is the immunogenicity of the enzyme and the risk of developing
anaphylactic reactions. Fatal anaphylactic reactions have been reported after intravenous
injections. Hence, L-asparaginase is always given as an intramuscular or subcutaneous injection
(MacEwen et al., 1992; Argyle et al., 2009).
Multidrug chemotherapy
Multi-agent therapy protocols are often injection protocols that combine cyclophosphamide,
doxorubicin (Hydroxydaunorubicin), vincristine (Oncovin), prednisone (so-called CHOP
protocol), and sometimes L-asparaginase (so-called L-CHOP protocol). These protocols result
in a high response rate and long response duration and therefore form the basis for most of the
current protocols used for treating high grade malignant lymphomas (Zandvliet, 2016). The

8
most frequent used protocol at the University Animal Hospital in Sweden is the ADRIA-plus
protocol consisting of doxorubicin, L-asparaginase, cyclophosphamide, chlorambucil,
hydroxyurea and prednisone, as described by Piek et al. (1999). The reported remission rate is
65-84 % with the ADRIA-plus protocol and up to 22 % of the treated dogs survive more than
two years (Piek et al., 1999).
Table 3. An overview of the ADRIA-plus protocol used at the University Animal Hospital in Sweden.
The treatment is interrupted if the patient is at complete remission at week 19. Planned revisits week
24, 27, 30, 39 and 52
Week
Drug 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
L-asparaginase
Doxorubicin
Cyclophosphamide
Chlorambucil
Hydroxyurea
Prednisone
Dexamethasone
Side effects
It is well known that humans going through chemotherapy suffer from many side effects.
However, dogs are less sensible to these side effects than humans. Furthermore, a lower dose
of cytotoxic drugs is used in the veterinary medicine to reduce the risk of side effects.
Chemotherapy damages dividing cells. This means that both cancer cells and healthy cells are
affected, particularly fast dividing cells. Some organ systems are more likely to suffer from side
effects, due to their fast dividing cells. One of these organ systems is the bone marrow. If the
bone marrow suffers from too much chemotherapy, the patient may develop anemia and an
increased risk of developing infections and bleedings. Therefore, it is important to take a blood
sample and control the erythrocyte, leukocyte and platelet levels prior to each treatment.
Furthermore, another organ system often affected by side effects is the gastrointestinal tract,
due to the constant exchange of the intestinal mucosa. This may cause nausea, inappetence and
diarrhea.
Humans often suffer from hair loss as a side effect of the chemotherapy. Dogs rarely suffer
from this side effect, except for certain breeds such as poodles and schnauzers which may
develop focal hair loss. All breeds may experience a temporary increase in fur shedding during
the treatment (Piek et al., 1999; Nelson & Couto, 2008; Argyle et al., 2009; Zandvliet, 2016).
It is common to assess the hepatic and renal function before, during and after administration of
chemotherapy drugs that are either toxic to these organ systems or are excreted via these organs
(Morris & Dobson, 2008).
9
Acute Tumor Lysis Syndrome (ATLS)
Acute tumor lysis syndrome occurs in patients with lymphoproliferative malignancies, often
after initiation of treatment. The massive tumor cell lysis causes a release of large amounts of
potassium, phosphate, and uric acid. This may lead to acute renal failure due to deposition of
uric acid and calcium phosphate crystals in the renal tubules. Healthy kidneys normally excrete
these products, why a pre-existing renal failure makes the risk of ATLS higher. The treatment
aims to clear high plasma levels of potassium, uric acid, and phosphorus, to correct the acidosis,
and prevent acute renal failure by aggressive intravenous fluid therapy (Davidson et al., 2004).
Drug resistance
The cancer genome is unstable and may result in spontaneous mutations, making some cells
inherently resistant to chemotherapy. The heterogenous population of cells in a tumor varies in
their resistance to chemotherapy. This depends on many factors, including cell cycle-phase,
distance from vascular supply and genetically acquired properties.
The patient often shows a good initial response to chemotherapy. However, as soon as the
chemosensitive cells are killed, the chemoresistant cells have a selective advantage, leading to
progressive tumor growth despite of chemotherapy. Multi-agent therapy enables a maximal
amount of killed tumor cells within the range of toxicity tolerated by the patient for each drug.
The multidrug chemotherapy also provides a wider range of coverage of resistant cell lines.
Furthermore, the development of new resistant cell lines is prevented or slowed down when
using a multi-agent therapy protocol compared to a single-agent therapy (Morris & Dobson,
2008).
Tumor resistance to anthracyclines is primarily caused by overexpression of membrane P-
glycoprotein (P-gp). On the other hand, resistance to the alkylating agents is caused by changes
in the cellular metabolic systems. This mechanism makes the drug detoxification better and
results in a water soluble, less toxic product. Resistance to L-asparaginase comes from an
increased expression of the asparagine synthetase gene. Furthermore, formation of antibodies
against L-asparaginase may also decrease its efficacy (Morris & Dobson, 2008).
Enzymatic function of thymidine kinase 1
Thymidine kinase is a key enzyme in the salvage pathway of nucleotide metabolism. This
pathway recycles free deoxyribonucleosides originating from the DNA breakdown, and makes
new DNA precursor deoxyribonucleoside triphosphates. Thymidine kinase catalyses the initial
step of the salvage pathway, which is a transfer of γ-phosphoryl group from ATP to thymidine,
leading to the formation of thymidine monophosphate (TMP). The intracellular TMP is then
quickly phosphorylated into thymidine diphosphate (TDP) and further to thymidine
triphosphate (TTP). TTP can then be used as a substrate for the incorporation of pyrimidines in
the growing DNA-strand. It is not possible to form new DNA strands without TTP, meaning
that TTP is crucial for further replication and cell division (Berenstein, 2004). Studies have
shown that the serum TK1-activity is increased in dogs suffering from malignant lymphoma
(von Euler et al., 2004; Euler et al., 2009). Moreover, these studies showed that the TK activity

10
in serum was significantly higher three weeks before and at the time of relapse, than the activity
measured at complete remission (CR).
C-reactive protein and lymphoma
C-reactive protein (CRP) is an acute phase protein produced in the liver. The serum CRP is
typically increased in response to inflammation or infection (Merlo et al., 2007). Interleukin 6
(IL-6) is a cytokine that regulates acute phase proteins, and is the main inducer of the synthesis
of CRP. Furthermore, IL-6 plays a central role in normal B-cell maturation and in proliferation
of some B-cell malignancies, including human NHL. Studies have shown that the serum IL-6
levels correlates with B symptoms (fever, weight loss and night sweats) in human NHL.
Furthermore, these studies showed that the serum CRP levels correlated with the serum IL-6
levels (Legouffe et al., 1998). Therefore, the human medicine has been using serum CRP
concentrations as a prognostic factor for patients with lymphoid tumours, and as a marker for
remission and relapse (Legouffe et al., 1998; Elahi et al., 2005; Merlo et al., 2007).
When it comes to veterinary medicine, Merlo et al. (2007) found that the serum CRP
concentration is not a useful marker for relapse in dogs with multicentric lymphoma. However,
dogs often have high serum CRP concentrations at the time of diagnosis (Merlo et al., 2007;
Nielsen et al., 2007). Furthermore, Merlo et al. (2007) found that chemotherapy itself does not
affect serum CRP concentrations. Another study showed that the serum CRP concentration may
be useful to determine complete remission status after treatment with cytotoxic drugs. However,
the CRP concentration is not reliable to use in monitoring progression of the disease, due to the
big individual variation between dogs' mean CRP concentrations (Nielsen et al., 2007).
MATERIAL AND METHODS
A list of all dogs who had received the diagnosis malignant lymphoma in the last seven years
(2010-2017) at the University Animal Hospital in Sweden was created from medical records.
The study initially included 129 dogs with malignant lymphoma. However, due to inadequate
information in the medical record, 19 dogs were excluded from the study (two dogs due to a
prior diagnosis and treatment of the lymphoma at another animal hospital with no copy of the
initial medical record, seven dogs due to the lack of a definitive diagnosis and ten dogs due to
no record of the euthanasia or death date). To obtain missing information about the date of
euthanasia or death, 42 owners were phone called. Those who not answered the phone call
received both a text message and a phone message. Complementary information was obtained
from 32 of these owners. The remaining ten owners either did not answer or declined the
participation in the study. To be included in the study, the date for diagnosis and euthanasia or
death were required.
Each one of the 110 dogs was evaluated on the basis of the information collected at the first
examination including history, physical examination, diagnostic imaging and laboratory
examinations: complete blood count, serum biochemical profile, FNA and
immunophenotyping. All information was collected from the medical records. The collected
information were: breed, sex, age at diagnosis, weight, body condition score (BCS), symptoms
(polyuria/polydipsia, fatigue and inappetence), blood analyzes (hemoglobin [Hb], hematocrit

11
[Hct], TK, CRP and calcium), information about the tumor (clinical stage, immunophenotype,
diagnostic method and malignancy grade) and information about the treatment (type of
treatment/protocol, pre-treatment with prednisolone or not, time to progression and overall
survival time from first day of treatment).
The serum TK levels were analyzed by the use of two different methods, either the radio enzyme
assay (TK-REA) or the TK-activity assay described by Stålhandske et al. (2013).
Staging was not complete in all cases. Patients with multicentric lymphoma who did not
undergo any diagnostic imaging were classified as stage 3, if no splenomegaly or hepatomegaly
were suspected during abdominal palpation.
The breed distribution was calculated and compared to the Swedish dog register from the
Swedish Board of Agriculture, to see if any breed seemed to be predisposed in developing
malignant lymphoma. Furthermore, the dogs were categorized in four different groups
depending on their sex and the distribution of males, neutered males, females and neutered
females was calculated. Mean values and median values were calculated for the weight and age
of the dogs. The Hct values were categorized in 4 different groups; within reference value
(>0.37 L/L), mild anemia (0.30-0.37 L/L), moderate anemia (0.20-0.29 L/L) and severe anemia
(<0.19 L/L). The Hb values were categorized into two groups; within the reference value and
below the reference value, after which the distribution was calculated. Moreover, the
distribution of dogs suffering from hypercalcemia was calculated as well as the distribution of
B- and T-cell lymphomas.
The dogs were categorized into two groups with different cut-off values on their initial TK
levels in serum. The cut-off values follows, for the respective groups; 0-11.0, 11.1-20.0, 20.1-
40.0 and 40.1-100 and 0-15.0, 15.1-40.0 and 40.1-100. Dogs pretreated with prednisolone
before the blood sample were excluded from the TK groups. Furthermore, the dogs were
categorized into different groups depending on their initial treatment method. The groups were;
no treatment, ADRIA-plus protocol, prednisolone ± L-asparaginase, CCNU (lomustine),
doxorubicin and other treatment.
The TK, CRP, calcium and Hct levels, as well as the clinical stage, immunophenotype, tumor
grade and clinical symptoms, were evaluated to see if they correlated with prognosis and overall
survival time in days from treatment. Dogs that did not receive any treatment were excluded
from the survival analyzis, due to not having any date of euthanasia or death. Dogs that lacked
certain test results were only excluded from that specific calculation concerning the missing
data. The survival distributions were estimated nonparametrically using the Kaplan-Meier
method. Furthermore, the significance was evaluated using the log rank test. A p-value < 0.05
was regarded as significant and a p-value < 0.01 was regarded as highly significant. All
numerical calculations were performed in Excel with an add-in called ExcelSurvival to draw
the Kaplan-Meier curves.
At the end of the study, six dogs were still alive at day 129, 130, 175, 204 and 468 from the
first day of treatment. One dog with an indolent lymphoma did not receive any treatment under

12
the duration of the study. Five dogs in the study were euthanized of other reasons than the
lymphoma.
Background data
Breed
Fifty different breeds were represented in the study (table 4). Out of these, 25.5 % (28/110)
were mixed breeds. The most frequent pure breed was Golden Retriever (8/110), followed by
Rottweiler (6/110) and Border Collie, Flat Coated Retriever, Nova Scotia Duck Tolling
Retriever and Bernese Mountain Dog (4/110). When compared to the total population of dogs
in each breed in Sweden (Jordbruksverket, 2016), the breeds Nova Scotia Duck Tolling
Retriever, Bernese Mountain Dog, Doberman and Great Dane seems to be overrepresented in
the study.
Table 4. Table showing all breeds that are represented in the study and the number of dogs in each
breed. The Columns show the percentage of each breed in the study (a) and the percentage of each
breed in Sweden (b), together with the ratio between them (a/b)
Breed Number of
dogs
Percentage
in study
(a)
Percentage
in Sweden
(b)
Ratio
(a/b)
Mixed breed 28 25.5 26.58 0.96
Golden Retriever 8 7.3 2.67 2.72
Rottweiler 6 5.5 1.74 3.13
Border Collie 4 3.6 1.29 2.81
Flat Coated Retriever 4 3.6 0.85 4.28
Nova Scotia Duck Tolling Retriever 4 3.6 0.45 8.02
Bernese Mountain Dog 4 3.6 0.54 6.74
Miniature Schnauzer 3 2.7 1.43 1.91
Finnish Hound 2 1.8 0.42 4.42
German Shepherd Dog 2 1.8 3.31 0.55
Great Dane 2 1.8 0.31 5.83
Doberman 2 1.8 0.32 5.75
Rhodesian Ridgeback 2 1.8 0.44 4.13
English Springer Spaniel 2 1.8 0.87 2.10
West Highland White Terrier 2 1.8 0.35 5.23
American Staffordshire Terrier 1 0.9 0.92 0.99
Staffordshire Bull Terrier 1 0.9 0.66 1.37
Labrador Retriever 1 0.9 3.08 0.30
Boxer 1 0.9 0.55 1.65
Miniature Pinscher 1 0.9 0.46 2.0
Border Terrier 1 0.9 0.64 1.43
Bouvier des flandres 1 0.9 0.06 15.16

13
Rough Collie 1 0.9 0.51 1.79
Norwegian Elkhound 1 0.9 0.84 1.09
Miniature Poodle 1 0.9 1.06 0.86
Standard Poodle 1 0.9 0.55 1.65
Whippet 1 0.9 0.39 2.33
Catalan Sheepdog 1 0.9 0.02 53.96
Saint Bernard Dog 1 0.9 0.14 6.38
Phalène 1 0.9 0.12 7.37
Bloodhound 1 0.9 0.01 79.36
German Spaniel 1 0.9 0.58 1.57
Beagle 1 0.9 0.38 2.40
Cavalier King Charles Spaniel 1 0.9 1.23 0.74
Polish Lowland Sheepdog 1 0.9 0.04 24.53
Gordon Setter 1 0.9 0.11 8.65
Briard 1 0.9 0.14 6.70
Irish Glen of Imaal Terrier 1 0.9 0.01 106.51
Dachshund 1 0.9 0.90 1.01
Clumber Spaniel 1 0.9 0.02 37.83
Dandie Dinmont Terrier 1 0.9 0.03 34.89
Miniature Bull Terrier 1 0.9 0.04 23.74
Norfolk Terrier 1 0.9 0.11 8.45
Scottish terrier 1 0.9 0.05 19.89
Irish Setter 1 0.9 0.35 2.58
Fox Terrier, smooth 1 0.9 0.16 5.84
Australian Shepherd 1 0.9 0.35 2.61
Curly Coated Retriever 1 0.9 0.04 22.55
Giant Schnauzer 1 0.9 0.20 4.48
Coton de tuléar 1 0.9 0.17 5.28
Total number of breeds: 50 Total number of dogs: 110
Sex, weight and age
The sex distribution of the study follow as, 30.9 % (34/110) male dogs, 20 % (22/110) neutered
male dogs, 36.4 % (40/110) female dogs and 13.6 % (15/110) neutered female dogs. The mean
age was 7.5 years (90.25 months) and the median age was 7.3 years (87.5 months, range 10-
162 months). The mean weight was 28.2 kg and the median weight was 27.2 kg (range 2.3-80
kg).

14
Blood analyzes
Hypercalcemia was seen in 6.67 % of the dogs (6/90). The initial calcium value was not
analyzed in 30 dogs. The TK values were categorized in two different ways, either in three or
four groups, with the distribution shown in figure 1. The initial TK value was only analyzed in
40 dogs. When it comes to CRP, 37 % of the dogs (17/46) had values below 30 mg/L and 63 %
(29/46) had values above 30 mg/L. The group of dogs with a Hct within the reference value
(>0.37 L/L) accounted for 69.3 % (70/101) of all the dogs that had an initial Hct value and the
dogs with mild anemia (0.30-0.37 L/L) accounted for 22.8 % (23/101), while 7.9 % (8/101) of
the dogs had a moderate anemia (0.20-0.29 L/L). No dogs suffered from severe anemia (<0.19
L/L) in this study. When focusing on the Hb value, 70 % (70/100) of the dogs had values within
reference, while 30 % (30/100) of the dogs had values below reference.
Distribution of TK values
Figure 1a & b. Distribution of dogs when categorizing their TK values into two groups with three
(a) or four (b) cut-off values. There were, in total, 40 dogs with an initial TK value in the study.
Immunophenotype
Immunophenotyping was performed in 30 of the 110 dogs. The remaining 80 dogs had an
unknown immunophenotype. Out of these 30 tumors, 53.3 % (16/30) were B-cell lymphomas,
36.7 % (11/30) were T-cell lymphomas, 6.7 % (2/30) were mixed B- and T-cell lymphomas
and 3.3 % (1/30) were nullcell (non-B-non-T-cell) lymphomas.
Tumor grade
The histological grade of the tumor was known in 97 dogs, showing that 10.3 % (10/97) of the
dogs had a low grade lymphoma, while 89.7 % (87/97) of the dogs had a high grade lymphoma.
0-15.0
U/L
40%
15.1-
40.0
U/L
32%
40.0-
100
U/L
28%
0-11.0
U/L
22%
11.1-
20.0
U/L
20%
20.1-
40.0
U/L
30%
> 40.0
U/L
28%
(a) (b)
15
Clinical stage
No dogs in the study were at stage 1, 7.3 % (8/110) of the dogs were at stage 2, 34.5 % (38/110)
of the dogs were at stage 3, 31.8 % (35/110) of the dogs were at stage 4 and 26.4 % (29/110)
dogs were at stage 5 at the time of diagnosis.
Treatment method
In the study, 30 % of the dogs (33/110) did not receive any kind of treatment, whilst 70 % of
the dogs were treated in different ways. Out of these, 31.8 % (35/110) were treated with the
ADRIA-plus protocol (consisted of doxorubicin, L-asparaginase, cyclophosphamide,
chlorambucil, hydroxyurea, and prednisone) and 15.5 % (17/100) were treated with
prednisolone, with or without L-asparaginase injections. On the other hand, 9.1 % (10/110) of
the dogs were treated with CCNU (lomustine) and 8.2 % (9/100) of the dogs were treated with
doxorubicin as a single agent treatment. Five dogs, 4.5 %, received another treatment.
RESULTS
TK levels in serum
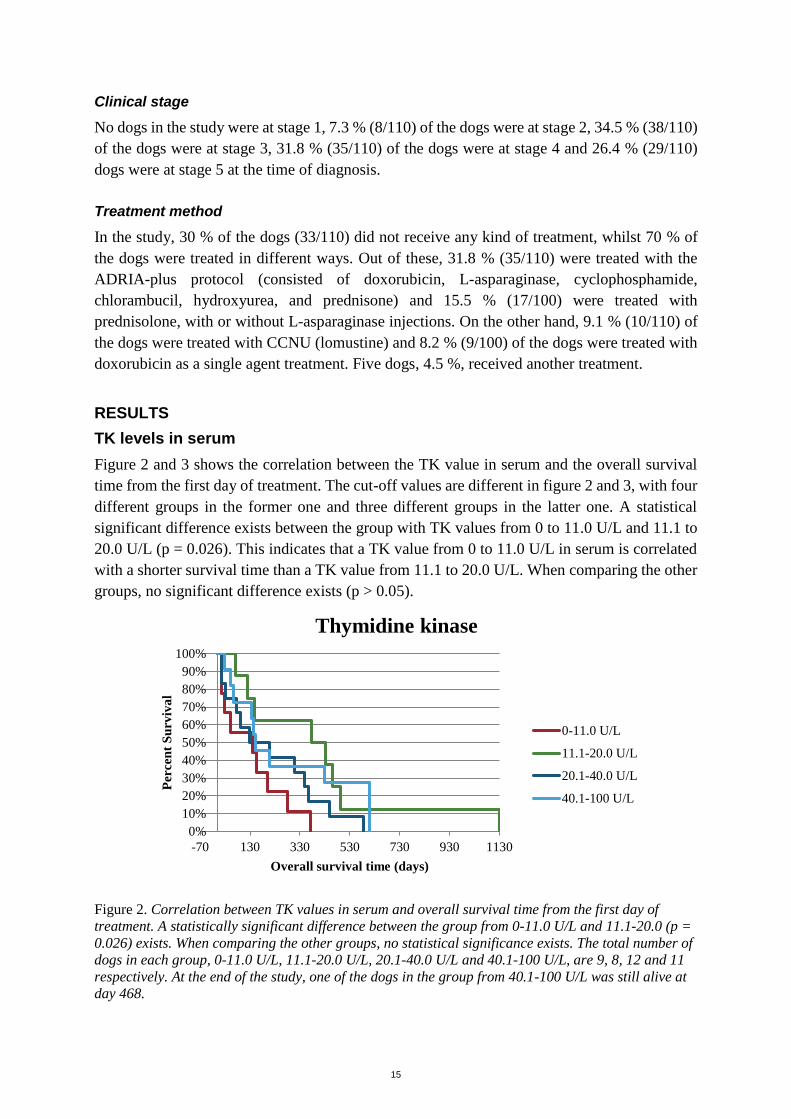
Figure 2 and 3 shows the correlation between the TK value in serum and the overall survival
time from the first day of treatment. The cut-off values are different in figure 2 and 3, with four
different groups in the former one and three different groups in the latter one. A statistical
significant difference exists between the group with TK values from 0 to 11.0 U/L and 11.1 to
20.0 U/L (p = 0.026). This indicates that a TK value from 0 to 11.0 U/L in serum is correlated
with a shorter survival time than a TK value from 11.1 to 20.0 U/L. When comparing the other
groups, no significant difference exists (p > 0.05).
Figure 2. Correlation between TK values in serum and overall survival time from the first day of
treatment. A statistically significant difference between the group from 0-11.0 U/L and 11.1-20.0 (p =
0.026) exists. When comparing the other groups, no statistical significance exists. The total number of
dogs in each group, 0-11.0 U/L, 11.1-20.0 U/L, 20.1-40.0 U/L and 40.1-100 U/L, are 9, 8, 12 and 11
respectively. At the end of the study, one of the dogs in the group from 40.1-100 U/L was still alive at
day 468.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Thymidine kinase
0-11.0 U/L
11.1-20.0 U/L
20.1-40.0 U/L
40.1-100 U/L
16
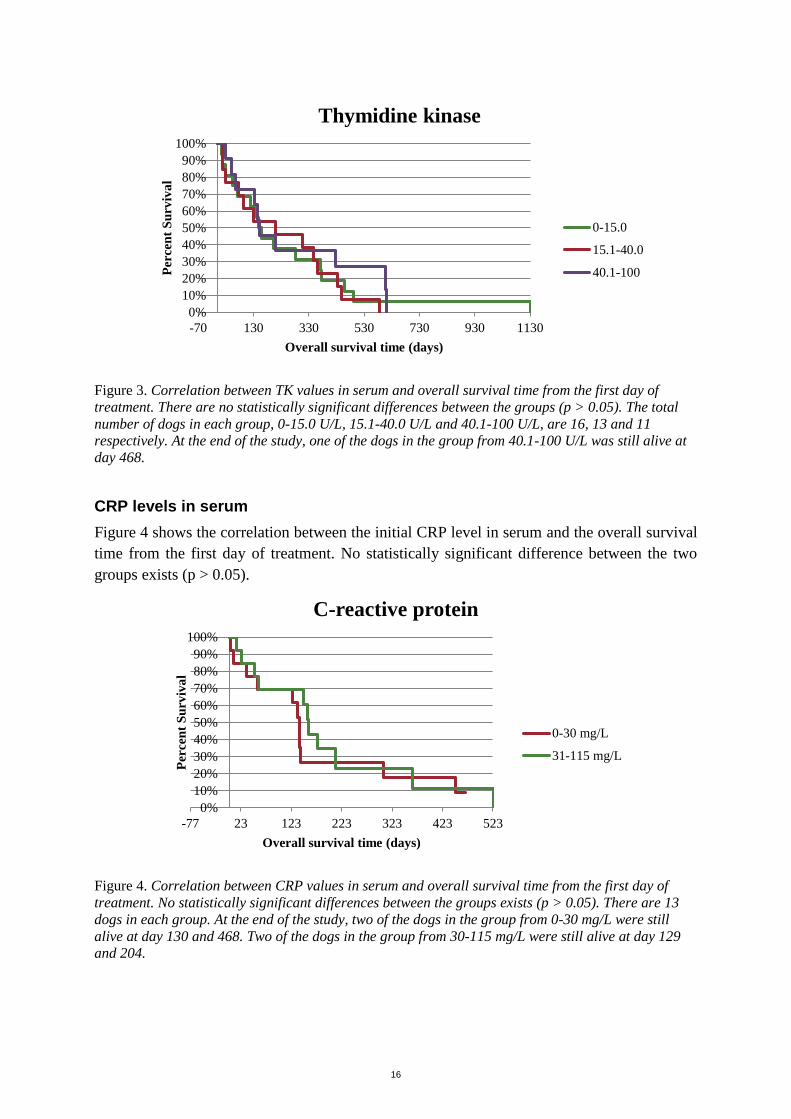
Figure 3. Correlation between TK values in serum and overall survival time from the first day of
treatment. There are no statistically significant differences between the groups (p > 0.05). The total
number of dogs in each group, 0-15.0 U/L, 15.1-40.0 U/L and 40.1-100 U/L, are 16, 13 and 11
respectively. At the end of the study, one of the dogs in the group from 40.1-100 U/L was still alive at
day 468.
CRP levels in serum
Figure 4 shows the correlation between the initial CRP level in serum and the overall survival
time from the first day of treatment. No statistically significant difference between the two
groups exists (p > 0.05).
Figure 4. Correlation between CRP values in serum and overall survival time from the first day of
treatment. No statistically significant differences between the groups exists (p > 0.05). There are 13
dogs in each group. At the end of the study, two of the dogs in the group from 0-30 mg/L were still
alive at day 130 and 468. Two of the dogs in the group from 30-115 mg/L were still alive at day 129
and 204.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Thymidine kinase
0-15.0
15.1-40.0
40.1-100
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-77 23 123 223 323 423 523
Per
cen
t S
urv
iva
l
Overall survival time (days)
C-reactive protein
0-30 mg/L
31-115 mg/L

17
Calcium levels in serum
Figure 5 shows the correlation between the initial calcium level in serum and the overall
survival time from the first day of treatment. No statistically significant difference between the
two groups exists (p > 0.05).
Figure 5. Correlation between calcium levels in serum and overall survival time from the first day of
treatment. No statistically significant differences between the groups exists (p > 0.05). The total
number of dogs in each group, hypercalcemia and normal, are 5 and 55 respectively. At the end of the
study, five of the dogs in the group with normal calcium levels were still alive at day 129, 130, 175,
204 and 468. Hematocrit level
Figure 6 shows the correlation between the initial hematocrit level and the overall survival time
from the first day of treatment. No statistically significant difference between the two groups
exists (p > 0.05).
Figure 6. Correlation between the Hct level (anemia) and overall survival time from the first day of
treatment. No statistically significant difference between the two groups exists (p > 0.05). The total
number of dogs in each group, within reference and anemia, are 54 and 17 respectively. At the end of
the study, four of the dogs in the group with a normal Hct level were still alive at day 130, 175, 204
and 468, and one of the dogs in the anemia group was alive at day 129.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Calcium
Hyper Ca
Normal Ca
0%
20%
40%
60%
80%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Hematocrit
Within reference (>0.37 L/L)
Anemia (≤0.37 L/L)

18
Clinical stage
Figure 7 and 8 shows the correlation between the clinical stage at the time of diagnosis and the
overall survival time from the first day of treatment. In figure 8, stage 3 and 4 are combined to
one single group. No statistically significant differences between the groups exists (p > 0.05).
Figure 7. Correlation between the clinical stage and overall survival time from the first day of
treatment. There are no statistically significant differences between the groups (p > 0.05). The total
number of dogs in each group, stage 2, stage 3, stage 4 and stage 5, are 8, 33, 26 and 10 respectively.
At the end of the study, five dogs were still alive; one in stage 2 at day 175, two in stage 3 at day 204
and 468, one in stage 4 at day 129 and one in stage 5 at day 130.
Figure 8. Correlation between the clinical stage and overall survival time from the first day of
treatment. There are no statistically significant differences between the groups (p > 0.05). The total
number of dogs in each group, stage 2, stage 3+4 and stage 5, are 8, 59 and 10 respectively. At the
end of the study, five dogs were still alive; one in stage 2 at day 175, three in stage 3+4 at day 129,
204 and 468 and one in stage 5 at day 130.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Clinical stage
Stage 2
Stage 3
Stage 4
Stage 5
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Clinical stage
Stage 2
Stage 3+4
Stage 5

19
Immunophenotype
Figure 9 shows the correlation between the immunophenotype of the tumor and the overall
survival time from the first day of treatment. No statistically significant difference between the
two groups exists (p > 0.05).
Figure 9. Correlation between the immunophenotype of the tumor and the overall survival time from
the first day of treatment. No statistically significant difference between the two groups exists (p >
0.05). The total number of dogs in each group, B-cell lymphoma and T-cell lymphoma, are 14 and 10
respectively.
Tumor grade
Figure 10 shows the correlation between the histological tumor grade (low/high) and the overall
survival time from the first day of treatment. No statistically significant difference between the
two groups exists (p > 0.05).
Figure 10. Correlation between tumor grade (low/high) and overall survival time from the first day of
treatment. No statistically significant difference between the groups exists (p > 0.05). The total
number of dogs in each group, low and high, are 8 and 57 respectively. At the end of the study, five of
the dogs in the group with high grade lymphomas were still alive at day 129, 130, 175, 204 and 468.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Immunophenotype
T-cell lymphoma
B-cell lymphoma
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Tumor grade
Low
High

20
Symptoms
Figure 11 shows the correlation between initial symptoms and the overall survival time from
the first day of treatment. No statistically significant difference between the two groups exists
(p > 0.05).
Figure 11. Correlation between symptoms and overall survival time from the first day of treatment.
The dogs are divided into two groups, "A symptoms", which means no clinical symptoms, and "B
symptoms" which means that the dogs have at least one of the following symptoms; polyuria,
polydipsia, fatigue, inappetence, vomiting, diarrhea, weight loss or anemia. No statistically significant
difference between the groups exists (p > 0.05). The total number of dogs in each group, A symptoms
and B symptoms, are 28 and 44 respectively. At the end of the study, three dogs in the group with A
symptoms were still alive at day 130, 175 and 468 and two dogs in the group with B symptoms were
alive at day 129 and 204.
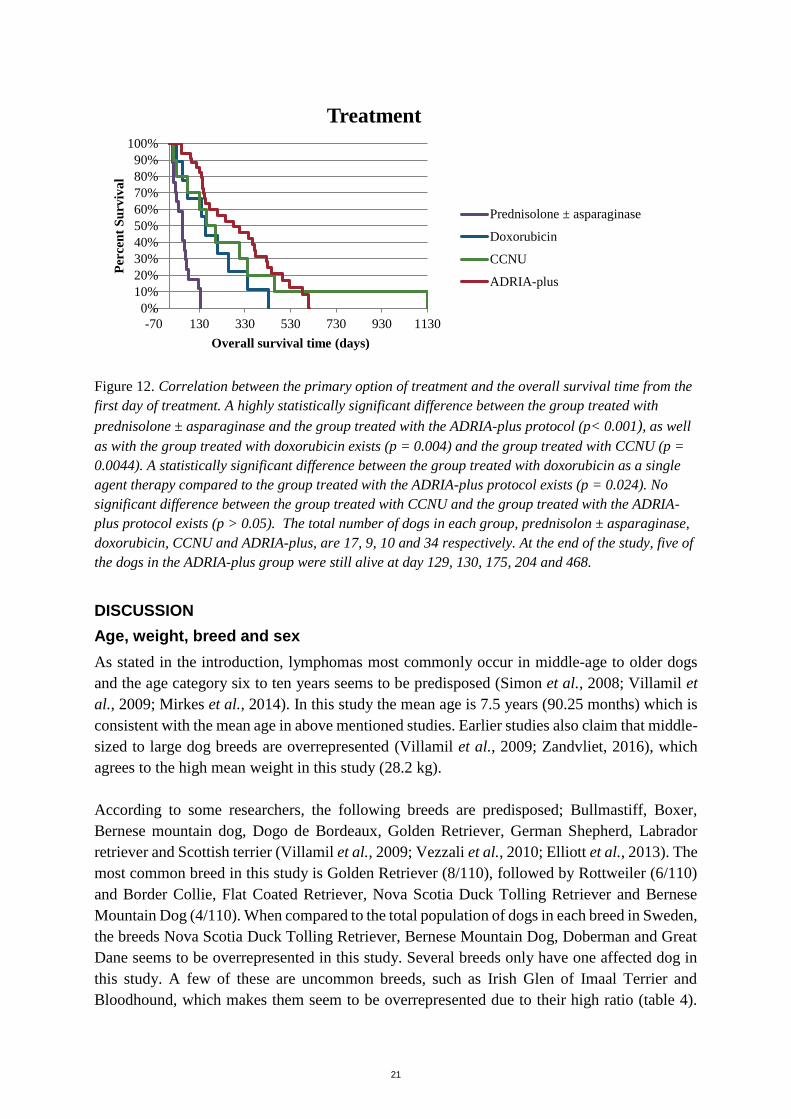
Treatment method
Figure 12 shows the correlation between the primary option of treatment and the overall
survival time from the first day of treatment. A highly statistically significant difference
between the group of dogs treated with prednisolone ± asparaginase compared to the group
treated with the ADRIA-plus protocol exists (p < 0.001), as well as the group treated with
doxorubicin (p = 0.004) and the group treated with CCNU (p = 0.0044). A statistically
significant difference between the group treated with doxorubicin as a single agent therapy
compared to the group treated with the ADRIA-plus protocol exists (p = 0.024). No statistically
significant difference between the group treated with CCNU and the group treated with the
ADRIA-plus protocol exists (p > 0.05).
0%
20%
40%
60%
80%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Symptoms
A symptoms
B symptoms
21
Figure 12. Correlation between the primary option of treatment and the overall survival time from the
first day of treatment. A highly statistically significant difference between the group treated with
prednisolone ± asparaginase and the group treated with the ADRIA-plus protocol (p< 0.001), as well
as with the group treated with doxorubicin exists (p = 0.004) and the group treated with CCNU (p =
0.0044). A statistically significant difference between the group treated with doxorubicin as a single
agent therapy compared to the group treated with the ADRIA-plus protocol exists (p = 0.024). No
significant difference between the group treated with CCNU and the group treated with the ADRIA-
plus protocol exists (p > 0.05). The total number of dogs in each group, prednisolon ± asparaginase,
doxorubicin, CCNU and ADRIA-plus, are 17, 9, 10 and 34 respectively. At the end of the study, five of
the dogs in the ADRIA-plus group were still alive at day 129, 130, 175, 204 and 468.
DISCUSSION
Age, weight, breed and sex
As stated in the introduction, lymphomas most commonly occur in middle-age to older dogs
and the age category six to ten years seems to be predisposed (Simon et al., 2008; Villamil et
al., 2009; Mirkes et al., 2014). In this study the mean age is 7.5 years (90.25 months) which is
consistent with the mean age in above mentioned studies. Earlier studies also claim that middle-
sized to large dog breeds are overrepresented (Villamil et al., 2009; Zandvliet, 2016), which
agrees to the high mean weight in this study (28.2 kg).
According to some researchers, the following breeds are predisposed; Bullmastiff, Boxer,
Bernese mountain dog, Dogo de Bordeaux, Golden Retriever, German Shepherd, Labrador
retriever and Scottish terrier (Villamil et al., 2009; Vezzali et al., 2010; Elliott et al., 2013). The
most common breed in this study is Golden Retriever (8/110), followed by Rottweiler (6/110)
and Border Collie, Flat Coated Retriever, Nova Scotia Duck Tolling Retriever and Bernese
Mountain Dog (4/110). When compared to the total population of dogs in each breed in Sweden,
the breeds Nova Scotia Duck Tolling Retriever, Bernese Mountain Dog, Doberman and Great
Dane seems to be overrepresented in this study. Several breeds only have one affected dog in
this study. A few of these are uncommon breeds, such as Irish Glen of Imaal Terrier and
Bloodhound, which makes them seem to be overrepresented due to their high ratio (table 4).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
-70 130 330 530 730 930 1130
Per
cen
t S
urv
iva
l
Overall survival time (days)
Treatment
Prednisolone ± asparaginase
Doxorubicin
CCNU
ADRIA-plus

22
However, they are not counted as overrepresented in this study because that one affected dog
may be caused by a statistical fluctuation.
Villamil et al. (2009) stated that intact female dogs seem to have a decreased risk in developing
malignant lymphoma compared to neutered females. However, in this study there are more
intact female dogs than neutered females, 36.4 % and 13.6 % respectively. This may be
explained by the high number of intact female dogs in Sweden. In 2012, the prevalence of
neutered dogs in Sweden was 22 % (Svenska Kennelklubben, 2012) compared to 64 % in the
United States in the year of 2007 (Trevejo et al., 2011). This may explain why the result in this
study does not agree with the result in the study made by Villamil et al. (2009).
Thymidine kinase
Previous studies have shown that TK is useful in diagnosis and prognosis in humans and dogs
suffering from malignant lymphoma (von Euler et al., 2004; von Euler & Eriksson, 2011;
Selting et al., 2016). Dogs with malignant lymphoma often have a higher TK value than healthy
dogs. The TK value also seems to correlate with stage and prognosis of the disease (von Euler
et al., 2004; Elliott et al., 2013). However, in this study, no correlation between a high initial
TK value in serum and a shorter overall survival time is shown. On the other hand, in figure 2
there is a significantly shorter survival time in the group with a lower TK value compared to a
group with a higher TK value. This result contradicts the results from the above mentioned
studies. The eight dogs in the group with an initial TK value from 0-11 U/L are shown in table
5. The results may be explained by the fact that two out of eight dogs in this group had a high
grade T-cell lymphoma. This type of tumor is correlated to a shorter survival time and a poorer
prognosis (Ponce et al., 2004; Calvalido et al., 2016). Moreover, T-cell lymphomas often have
lower TK values than B-cell lymphomas (Elliott et al., 2013). Furthermore, one of the dogs
only received prednisolone as treatment and the owners wanted to euthanize the dog before
becoming more affected by the disease, explaining the short survival time of only 14 days. One
dog with a high grade B-cell lymphoma has a survival time of 17 days. One explanation to this
short survival time could be that the dog suffered from a more aggressive form of B-cell
lymphoma called Burkitt's lymphoma, which is correlated to a poor prognosis and shorter
survival time (Ponce et al., 2004). However, in this case the mitotic activity was low. Another
explanation could be that the tumor had a low proliferation rate, why resistance may occur due
to the majority of cells being in G0 phase (Jerkeman et al., 2004). The small number of dogs (n
= 8) in this group may also contribute to the result.
Furthermore, the TK levels were analyzed by the use of two different methods, either the radio
enzyme assay (TK-REA) or the TK-activity assay described by Stålhandske et al. (2013). The
latter analyze method was stopped from use at the date of 2017-01-01. The results in this study
may have been affected by the fact that two different analyze methods were used and the results
were compared without taking account of the method.

23
Table 5. A summary of all dogs with initial TK values from 0-11 U/L. The table is showing breed, initial
TK value, clinical stage, tumor grade, immunophenotype, treatment and overall survival time in days
from start of treatment
Breed TK Stage Grade Immuno-
phenotype
Treatment OS
(days)
Golden Retriever <2.5 5 High Unknown ADRIA-plus 140
Giant Schnauzer 4.1 3 High T ADRIA-plus 53
Labrador Retriever <2.5 2 High Unknown CCNU 201
Flat Coated
Retriever 2.7 4 High T CCNU 28
West Highland
White Terrier <2.5 3 High B CCNU 17
Catalan Sheepdog 3 2 High Unknown Doxorubicin 158
German Shepherd
Dog 5.2 3 Unknown Unknown Pred only 14
Irish Setter 8.6 3 Low Unknown ADRIA 371
Another aspect that may affect the result is that all dogs that not received any kind of treatment
were excluded from the survival analyzes because they did not have an overall survival time
from first day of treatment. Dogs with indolent lymphomas often have low TK values and a
long survival time. If these dogs were included in the survival analyzes, the results could have
been different.
Furthermore, the difference between figure 2 and figure 3 shows that it is important to define
the cut-off values before the start of the study. In figure 2 a significant difference between two
of the groups exists, which is absent in figure 3 with different cut-off values.
Tumor grade and immunophenotype
Earlier studies show that the low grade lymphomas represents 5.3-29 % of all canine
lymphomas (Flood-Knapik et al., 2013). In this study, the prevalence of low grade lymphomas
is 10.3 % (10/97) which is consistent with literature. On the other hand, when it comes to the
survival analysis, no significant difference is seen between tumor grade and survival time in
this study. At first sight, it looks like the low grade tumors have a longer survival time but no
significant difference exists when calculating the p-value (p = 0.299). This may be affected if
more data is added. Another solution would be to categorize the tumors in three different groups
instead of two. In this way, all intermediate tumors will have their own group and may lead to
a bigger difference between the low and high grade tumors.
The immunophenotype was only recorded in 30 out of 110 dogs in this study and the results
shows that 53.3 % (16/30) of the dogs have a B-cell lymphoma. According to Vezzali et al.

24
(2010) B-cell lymphomas accounts for approximately 80-85 % of the canine lymphomas. It is
possible that the low percentage of B-cell lymhomas in this study is caused by the low number
of immunophenotyped tumors.
Anemia, hypercalcemia and clinical symptoms
According to Gavazza et al. (2008) a mild to moderate non-regenerative anemia is seen in many
dogs suffering from malignant lymphoma. In this study, 30.7 % (31/101) of the dogs have a
mild or moderate anemia, none of the dogs have a severe anemia. No correlation between
anemia and a shorter survival time is found.
Hypercalcemia is seen in 6.67 % (6/90) of the dogs. According to Ruslander et al. (1997) and
Zandvliet (2016), hypercalcemia is seen in 10-15 % of the dogs and is often associated with T-
cell lymphoma and thereby a poorer prognosis. No correlation between hypercalcemia and a
sorter survival time can be seen in this study.
Earlier studies states that dogs with B symptoms have a poorer prognosis and shorter survival
time than dogs with A symptoms (von Euler et al., 2004). In figure 11, there is a visual
difference between the curves. However, the p-value is not significant (p = 0.21). This may be
due to the number of dogs in each group (n = 44 and n = 28, respectively). A larger set of data
could possibly affect the result.
Limitations of the study
This study has several limitations. First of all, this is a retrospective study, which means that all
desired data is not always available. One of the advantages of a prospective study is that the
protocols can be made in advance and it is easier to obtain the right set of data. Another problem
linked to this study design is that no standardized staging was done. Some of the dogs went
through all diagnostic methods and others only confirmed the diagnosis through FNA or
biopsies, but no further staging was done. This makes it much more difficult to evaluate if the
dogs were at stage 3, 4 or 5 at the time of diagnosis. This is why figure 8 was drawn, where
stage 3 and 4 were put in the same group. Another negative aspect of a retrospective study is
that it is challenging to count the progression free survival time, which is a better measure of
time when evaluating the prognosis. In a retrospective study, the best way to find out the
prognosis is to count the overall survival time. The owners often remember when their dog
passed away if there is no information about it in the medical record. When choosing overall
survival time as a measure of time in the Kaplan-Meier plot, you have to take into account that
it is the owner's decision when the dog is going to die. Sometimes it depends on the owner's
economy, other times on ethical reasons or on logistic reasons, if the owner cannot take the dog
to the veterinary hospital as often as a treatment would require. It also depends on whether the
owner contacts the veterinarian as soon as the lymph nodes are slightly enlarged or if they wait
until the lymph nodes are very large and the dog finds difficulties breathing. In a prospective
study where progression free survival time is used as a measure of time in the Kaplan-Meier
plot, these factors will be eliminated. On the other hand, it requires a schedule with planned
revisits in advance at decided days. Furthermore, a problem with this study design is that no
standardized analyze methods were decided before the start of the study. This causes a difficulty

25
to compare the test results between different patients in the study and may affect the results in
the survival analysis.
Another limitation in this study is the low number of dogs in each group. The problem in this
study is that 33 dogs out of 110 could not be counted in the Kaplan-Meier survival curves
because they did not receive any kind of treatment and therefore had no overall survival time
from the first day of treatment. If a similar study is done, a count of the overall survival time
from diagnosis would be preferable. Thereby it would be possible for these dogs to be included
in the Kaplan-Meier curves as well.
Furthermore, a limitation in this study is that there is no standardized treatment method. The
dogs are treated in several different ways, and the treatment methods have significant
differences in the survival time. This is thought to affect the results considerably. A dog with a
high grade T-cell lymphoma with clinical symptoms and a high initial TK value in serum,
treated with the ADRIA-plus protocol, may have a longer survival time than a dog with a B-
cell lymphoma without any clinical symptoms and a lower initial TK value due to treatment
with prednisolone or doxorubicin as a single agent therapy.
One thing that may have affected the results in this study is that the oncologists at the University
Animal Hospital in Sweden have a good knowledge of the latest research which states that for
example a high initial TK value, a high clinical stage and severe symptoms correlates with a
bad prognosis (Zandvliet, 2016). This may lead to the advice of euthanasia directly, without
trying to treat the lymphoma. Furthermore, this could mean that the patients who have the
poorest prognosis are not involved in the study data because they were euthanized right after
diagnosis.
No multivariate analyzes are performed in this study due to the lack of significant p-values in
the univariate analyzes.
One dog in the study has a survival time of 1130 days which deviates considerably from the
other dogs. This dog has a low grade small T-cell lymphoma. This can be explained by the fact
that the small clear-cell lymphoma is correlated to a good prognosis and a longer survival time.
Its clinical behaviour seems to be similar to that of the indolent human lymphomas, with
survival time measured in years (Ponce et al., 2004).
CONCLUSION
In conclusion, the results in this study are not consistent with the hypotheses. No correlation
between a higher TK or CRP value and survival is found. Neither could hypercalcemia, anemia,
a high clinical stage, a T-cell lymphoma, B symptoms nor a high grade tumor be correlated to
a shorter overall survival time. The most important thing for a longer survival time is, according
to this study, treatment with the ADRIA-plus protocol, which leads to a significantly longer
survival time than the treatment with prednisolone or doxorubicin. Further studies are needed
to investigate if the above mentioned parameters are useful in prognostication in dogs with

26
malignant lymphoma. In the future, prospective studies with progression free survival time as
a measure of time and standardized treatment protocols would be preferable.
REFERENCES
Argyle, D. J., Brearley, M. J. & Turek, M. M. (2009). Decision making in small animal oncology
[online]. John Wiley & Sons. Available from:
http://juliet84.free.fr/Cancerologie/Decision%20Making%20in%20Small%20Animal%20Oncolog
y.pdf. [Accessed 2017-10-23].
Arnér, E. S. J. & Eriksson, S. (1995). Mammalian deoxyribonucleoside kinases. Pharmacology &
Therapeutics [online], 67(2), pp 155–186. Available from:
http://www.sciencedirect.com/science/article/pii/0163725895000159. [Accessed 2017-09-26].
Bell, R., Cotter, S., Lillquist, A., Sallan, S. & McCaffrey, R. (1984). Characterization of
glucocorticoid receptors in animal lymphoblastic disease: correlation with response to single-agent
glucocorticoid treatment. Blood, 63(2), pp 380–383.
Berenstein, D. (2004). Structure-function studies of human cytosolic thymidine kinase. Diss. PhD
Thesis at the Department of Life Sciences and Chemistry, Roskilde University, Denmark.
Available from: http://forskning.ruc.dk/site/files/57418654/Structure-function_studies_of.pdf.
[Accessed 2017-11-02].
Berlin, A., Farina, A., Abebe, A., Brown, A., Navidi, A., Wilson, A., Dupes, A., Melnikov, A., Aslam,
A., Franke, A., Kieu, A. C., Collymore, A., Abouelleil, A., Horn, A., Heger, A., Barry, A.,
Zimmer, A., Vo, A., Lui, A., Rachupka, A., Cook, A., Kamat, A., Mihalev, A., Goyette, A.,
O’Neill, B., Kanga, B., Jester, B., Blitshteyn, B., Hagos, B., Boukhgalter, B., Members, B. S. P.,
Webber, C., Bardeleben, C., Stone, C., Rise, C., Matthews, C., Jones, C., Chin, C.-W., Foley, C.,
Smith, C., Norbu, C., Ponting, C. P., Raymond, C., Hitte, C., Patti, C., Nguyen, C., Healy, C.,
Wade, C. M., Bonnet, C., Antoine, C., Kells, C., Bessette, D., Hagopian, D., Perrin, D., Jaffe, D.
B., DeCaprio, D., Thoulutsang, D., Friedrich, D., Ferguson, D., Shih, D., Gage, D., Khazanovich,
D., Smith, D. R., Grandbois, E., Iii, E. J. K., Ostrander, E. A., Karlsson, E. K., Lander, E. S.,
Mauceli, E., Kirkness, E., Rege, F., Galibert, F., Pierre, F., Gearin, G., Young, G., Giannoukos, G.,
Munson, G., Arachchi, H., Parker, H. G., Vassiliev, H., Topping, I., Cuff, J., Meldrim, J.,
Macdonald, J., Wilkinson, J., Blye, J., Chang, J. L., Leger, J.-P., Chu, J., Baldwin, J., Hall, J.,
Naylor, J., Sloan, J., Shi, J., Falk, J., Liu, J., Zainoun, J., Camarata, J., Major, J., Pollinger, J. P.,
Stalker, J., Butler, J., Graham, J., Rogers, J., Sahalie, J., Foley, K., Miller, K., Decktor, K., Dooley,
K., Maru, K., O’Neill, K., Topham, K., Lindblad-Toh, K., Dooley, K., Koepfli, K.-P., Lance, K.,
Dorjee, K., Gyaltsen, K., Ayotte, L., Hughes, L., Hunnicutt, L., Goodstadt, L., Boguslavskiy, L.,
Mulrain, L., Dorris, L., Kim, L., Leuper, L., Zembek, L., Meneus, L., Oyono, L., Aftuck, L.,
Husby, M., Grabherr, M., Kellis, M., Garber, M., Lara, M., Priest, M., Daly, M. J., Breen, M.,
Kumar, M., Sheehan, M., Zody, M. C., Kamal, M., Kleber, M., Weiand, M., Clamp, M., Citroen,
M., FitzGerald, M., Ait-zahra, M., Benamara, M., Hafez, N., Calixte, N., Sutter, N. B., Houde, N.,
Novod, N., Nguyen, N., Sherpa, N., Lennon, N., Allen, N., Stange-Thomann, N., Duffey, N.,
Dhargay, N., Norbu, N., Egbiremolen, O., Alvarez, P., Bachantsang, P., Dorje, P., Ferreira, P.,
Cahill, P., Cooke, P., Phunkhang, P., Tenzing, P., An, P., Kisner, P., Olandt, P., Rogov, P.,
Tchuinga, P., deJong, P. J., Yu, Q., Thomas, R., Mittelman, R., Rameau, R., Elong, R., Marabella,
R., Daza, R., Wayne, R. K., Nicol, R., Hegarty, R., Stone, S., Osman, S., Settipalli, S., Gnerre, S.,
LeVine, S., Anderson, S., Sykes, S., Tesfaye, S., Yadav, S., Stavropoulos, S., Fisher, S., Yang, S.,
Searle, S. M. J., DeGray, S., Raghuraman, S., Faro, S., McDonough, S., Mihova, T., Biagi, T.,
Mikkelsen, T. S., Bayul, T., Lokyitsang, T., Mehta, T., Nyima, T., Dawoe, T., Shea, T., Sharpe, T.,
Landers, T., Nguyen, T., Goode, T., Bloom, T., Sparrow, T., Honan, T., Tsamla, T., Wangchuk,
T., Wangdi, T., Nguyen, T., Aldredge, T., Mlenga, V., Ray, V., Venkataraman, V., Brockman, W.,
Lee, W., Liu, X., Xie, X., Yang, X., Cheshatsang, Y., Thoulutsang, Y. & Lokyitsang, Y. (2005).
Genome sequence, comparative analysis and haplotype structure of the domestic dog. Nature
27
[online], 438(7069), p 803. Available from: https://www.nature.com/articles/nature04338.
[Accessed 2017-11-24].
Calvalido, J., Wood, G. A., Mutsaers, A. J., Wood, D., Sears, W. & Woods, J. P. (2016). Comparison
of serum cytokine levels between dogs with multicentric lymphoma and healthy dogs. Veterinary
Immunology and Immunopathology [online], 182(Supplement C), pp 106–114. Available from:
http://www.sciencedirect.com/science/article/pii/S0165242716302185. [Accessed 2017-12-11].
Crabtree, A. C., Spangler, E., Beard, D. & Smith, A. (2010). Diagnostic accuracy of gray-scale
ultrasonography for the detection of hepatic and splenic lymphoma in dogs. Veterinary Radiology
& Ultrasound [online], 51(6), pp 661–664. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1740-8261.2010.01725.x/abstract. [Accessed 2017-
11-01].
Davidson, M. B., Thakkar, S., Hix, J. K., Bhandarkar, N. D., Wong, A. & Schreiber, M. J. (2004).
Pathophysiology, clinical consequences, and treatment of tumor lysis syndrome. The American
Journal of Medicine [online], 116(8), pp 546–554. Available from:
http://www.sciencedirect.com/science/article/pii/S0002934303007253. [Accessed 2017-11-03].
Dyce, K. M., Sack, W. O. & Wensing, C. J. G. (2010). Textbook of veterinary anatomy. 4. ed
Saunders. ISBN 978-1-4160-6607-1.
Elahi, M. M., McMillan, D. C., McArdle, C. S., Angerson, W. J., Soukop, M., Johnstone, J. & Sattar,
N. (2005). The systemic inflammatory response predicts overall and cancer specific survival in
patients with malignant lymphoma. Medical Science Monitor: International Medical Journal of
Experimental and Clinical Research, 11(2), pp CR75-78.
Elliott, J. W., Cripps, P. & Blackwood, L. (2013). Thymidine kinase assay in canine lymphoma.
Veterinary and Comparative Oncology [online], 11(1), pp 1–13. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1476-5829.2011.00296.x/abstract. [Accessed 2017-
10-26].
Elvers, I., Turner-Maier, J., Swofford, R., Koltookian, M., Johnson, J., Stewart, C., Zhang, C.-Z.,
Schumacher, S. E., Beroukhim, R., Rosenberg, M., Thomas, R., Mauceli, E., Getz, G., Palma, F.
D., Modiano, J. F., Breen, M., Lindblad-Toh, K. & Alföldi, J. (2015). Exome sequencing of
lymphomas from three dog breeds reveals somatic mutation patterns reflecting genetic
background. Genome Research [online], 25(11), pp 1634–1645. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4617960/. [Accessed 2017-11-24].
von Euler, H., Einarsson, R., Olsson, U., Lagerstedt, A.-S. & Eriksson, S. (2004). Serum thymidine
kinase activity in dogs with malignant lymphoma: a potent marker for prognosis and monitoring
the disease. Journal of Veterinary Internal Medicine [online], 18(5), pp 696–702. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1939-1676.2004.tb02608.x/abstract. [Accessed 2017-
09-11].
von Euler, H. & Eriksson, S. (2011). Comparative aspects of the proliferation marker thymidine kinase
1 in human and canine tumour diseases. Veterinary and Comparative Oncology [online], 9(1), pp
1–15. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1476-
5829.2010.00238.x/abstract. [Accessed 2017-09-11].
Euler, V., P, H., Rivera, P., Aronsson, A.-C., Bengtsson, C., Hansson, L.-O. & Eriksson, S. K. (2009).
Monitoring therapy in canine malignant lymphoma and leukemia with serum thymidine kinase 1
activity - evaluation of a new, fully automated non-radiometric assay. International Journal of
Oncology [online], 34(2), pp 505–510. Available from: http://www.spandidos-
publications.com/ijo/34/2/505/abstract. [Accessed 2017-09-11].
Flood-Knapik, K. E., Durham, A. C., Gregor, T. P., Sánchez, M. D., Durney, M. E. & Sorenmo, K. U.
(2013). Clinical, histopathological and immunohistochemical characterization of canine indolent

28
lymphoma. Veterinary and Comparative Oncology [online], 11(4), pp 272–286. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1476-5829.2011.00317.x/abstract. [Accessed 2017-
10-26].
Frances, M., Lane, A. E. & Lenard, Z. M. (2013). Sonographic features of gastrointestinal lymphoma
in 15 dogs. Journal of Small Animal Practice [online], 54(9), pp 468–474. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/jsap.12117/abstract. [Accessed 2017-11-01].
Gavazza, A., Lubas, G., Valori, E. & Gugliucci, B. (2008). Retrospective survey of malignant
lymphoma cases in the dog: clinical, therapeutical and prognostic features. Veterinary Research
Communications [online], 32(S1), pp 291–293. Available from:
http://www.academia.edu/19007203/Retrospective_survey_of_malignant_lymphoma_cases_in_th
e_dog_clinical_therapeutical_and_prognostic_features. [Accessed 2017-10-26].
He, E., Xu, X. H., Guan, H., Chen, Y., Chen, Z. H., Pan, Z. L., Tang, L. L., Hu, G. Z., Li, Y., Zhang,
M., Zhou, J., Eriksson, S., Fornander, T. & Skog, S. (2010). Thymidine kinase 1 is a potential
marker for prognosis and monitoring the response to treatment of patients with breast, lung, and
esophageal cancer and non-Hodgkin’s lymphoma. Nucleosides, Nucleotides and Nucleic Acids
[online], 29(4–6), pp 352–358. Available from: http://dx.doi.org/10.1080/15257771003738535.
[Accessed 2017-09-18].
Hengstschläger, M., Knöfler, M., Müllner, E. W., Ogris, E., Wintersberger, E. & Wawra, E. (1994).
Different regulation of thymidine kinase during the cell cycle of normal versus DNA tumor virus-
transformed cells. The Journal of Biological Chemistry, 269(19), pp 13836–13842.
Jerkeman, M., Anderson, H., Dictor, M., Kvaløy, S., Åkerman, M. & Cavallin-Ståhl, E. (2004).
Assessment of biological prognostic factors provides clinically relevant information in patients
with diffuse large B-cell lymphoma—a Nordic Lymphoma Group study. Annals of Hematology
[online], 83(7), pp 414–419. Available from: https://link.springer.com/article/10.1007/s00277-004-
0855-x. [Accessed 2017-12-11].
Jordbruksverket. Statistik hundregistret 2016 - Antal hundar per ras. [online] (2016-12-31). Available
from:
https://www.jordbruksverket.se/download/18.4ed35dff1597acb955888099/1483957215820/Antal
+hundar+per+ras.pdf. [Accessed 2017-12-08].
Legouffe, E., Rodriguez, C., Picgt, M. C., Richard, B., Klein, B., Rossi, J. F. & Commes, T. (1998). C-
reactive protein serum level is a valuable and simple prognostic marker in non Hodgkin’s
lymphoma. Leukemia & Lymphoma [online], 31(3–4), pp 351–357. Available from:
http://dx.doi.org/10.3109/10428199809059228. [Accessed 2017-11-06].
Leijon, A. (2013). Immunohistochemical detection of thymidine kinase 1 in canine mammary tumors
and lymphomas. Swedish University of Agricultural Sciences. Department Of Clinical
Sciences/Veterinary Medicine. (Degree project 2013:71). Available from:
http://stud.epsilon.slu.se/6268/7/leijon_a_131113.pdf. [Accessed 2017-09-08].
MacEwen, E. G., Rosenthal, R. C., Fox, L. E., Loar, A. S. & Kurzman, I. D. (1992). Evaluation of L-
asparaginase: polyethylene glycol conjugate versus native L-asparaginase combined with
chemotherapy: a randomized double-blind study in canine lymphoma. Journal of Veterinary
Internal Medicine [online], 6(4), pp 230–234. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1939-1676.1992.tb00344.x/abstract. [Accessed 2017-
11-01].
Marconato, L., Stefanello, D., Valenti, P., Bonfanti, U., Comazzi, S., Roccabianca, P., Caniatti, M.,
Romanelli, G., Massari, F. & Zini, E. (2011). Predictors of long-term survival in dogs with high-
grade multicentric lymphoma. Journal of the American Veterinary Medical Association [online],
238(4), pp 480–485. Available from:
http://avmajournals.avma.org/doi/full/10.2460/javma.238.4.480. [Accessed 2017-10-26].

29
Martini, V., Melzi, E., Comazzi, S. & Gelain, M. E. (2015). Peripheral blood abnormalities and bone
marrow infiltration in canine large B-cell lymphoma: is there a link? Veterinary and Comparative
Oncology [online], 13(2), pp 117–123. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/vco.12024/abstract. [Accessed 2017-11-01].
Merlo, A., Rezende, B. C. G., Franchini, M. L., Simões, D. M. N. & Lucas, S. R. R. (2007). Serum C-
reactive protein concentrations in dogs with multicentric lymphoma undergoing chemotherapy.
Journal of the American Veterinary Medical Association [online], 230(4), pp 522–526. Available
from: http://avmajournals.avma.org/doi/abs/10.2460/javma.230.4.522. [Accessed 2017-11-06].
Mirkes, E. M., Alexandrakis, I., Slater, K., Tuli, R. & Gorban, A. N. (2014). Computational diagnosis
and risk evaluation for canine lymphoma. Computers in Biology and Medicine [online],
53(Supplement C), pp 279–290. Available from:
http://www.sciencedirect.com/science/article/pii/S001048251400208X. [Accessed 2017-10-26].
Morris, J. & Dobson, J. (2008). Small animal oncology. John Wiley & Sons. ISBN 978-0-470-68013-
1.
Nelson, R. W. & Couto, C. G. (2008). Small animal internal medicine - E-Book. 4. ed Elsevier Health
Sciences. ISBN 978-0-323-06512-2.
Nielsen, L., Toft, N., Eckersall, P. D., Mellor, D. J. & Morris, J. S. (2007). Serum C-reactive protein
concentration as an indicator of remission status in dogs with multicentric lymphoma. Journal of
Veterinary Internal Medicine [online], 21(6), pp 1231–1236. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1939-1676.2007.tb01943.x/abstract. [Accessed 2017-
11-06].
Owen, L. N., Unit, W. H. O. V. P. H. & Oncology, W. C. C. for C. (1980). TNM classification of
tumours in domestic animal. [online],. Available from:
http://www.who.int/iris/handle/10665/68618. [Accessed 2017-10-24].
Piek, C. J., Rutteman, G. R. & Teske, E. (1999). Evaluation of the results of a L-asparaginase-based
continuous chemotherapy protocol versus a short doxorubicin-based induction chemotherapy
protocol in dogs with malignant lymphoma. The Veterinary Quarterly, 21(2), pp 44–49.
Ponce, F., Magnol, J.-P., Ledieu, D., Marchal, T., Turinelli, V., Chalvet-Monfray, K. & Fournel-
Fleury, C. (2004). Prognostic significance of morphological subtypes in canine malignant
lymphomas during chemotherapy. Veterinary Journal (London, England: 1997), 167(2), pp 158–
166.
Raskin, R. E. & Krehbiel, J. D. (1989). Prevalence of leukemic blood and bone marrow in dogs with
multicentric lymphoma. Journal of the American Veterinary Medical Association, 194(10), pp
1427–1429.
Ruslander, D. A., Gebhard, D. H., Tompkins, M. B., Grindem, C. B. & Page, R. L. (1997).
Immunophenotypic characterization of canine lymphoproliferative disorders. In Vivo (Athens,
Greece), 11(2), pp 169–172.
Sauerbrey, M. L., Mullins, M. N., Bannink, E. O., Van Dorp, T. E. R., Kaneene, J. B. & Obradovich,
J. E. (2007). Lomustine and prednisone as a first-line treatment for dogs with multicentric
lymphoma: 17 cases (2004–2005). Journal of the American Veterinary Medical Association
[online], 230(12), pp 1866–1869. Available from:
http://avmajournals.avma.org/doi/abs/10.2460/javma.230.12.1866. [Accessed 2017-11-03].
Selting, K. a., Ringold, R., Husbands, B. & Pithua, P. o. (2016). Thymidine kinase type 1 and C-
reactive protein concentrations in dogs with spontaneously occurring cancer. Journal of Veterinary
Internal Medicine [online], 30(4), pp 1159–1166. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/jvim.13954/abstract. [Accessed 2017-12-11].

30
Simon, D., Moreno, S. N., Hirschberger, J., Moritz, A., Kohn, B., Neumann, S., Jurina, K.,
Scharvogel, S., Schwedes, C., Reinacher, M., Beyerbach, M. & Nolte, I. (2008). Efficacy of a
continuous, multiagent chemotherapeutic protocol versus a short-term single-agent protocol in
dogs with lymphoma. Journal of the American Veterinary Medical Association [online], 232(6),
pp 879–885. Available from: http://avmajournals.avma.org/doi/full/10.2460/javma.232.6.879.
[Accessed 2017-11-03].
Smith, L. K. & Cidlowski, J. A. (2010). Chapter 1 - Glucocorticoid-induced apoptosis of healthy and
malignant lymphocytes. In: Martini, L. (Ed) Progress in Brain Research. pp 1–30. Elsevier.
Squire, R. A., Bush, M., Melby, E. C., Neeley, L. M. & Yarbrough, B. (1973). Clinical and pathologic
study of canine lymphoma: clinical staging, cell classification, and therapy. Journal of the
National Cancer Institute, 51(2), pp 565–574.
Stålhandske, P., Wang, L., Westberg, S., von Euler, H., Groth, E., Gustafsson, S. A., Eriksson, S. &
Lennerstrand, J. (2013). Homogeneous assay for real-time and simultaneous detection of
thymidine kinase 1 and deoxycytidine kinase activities. Analytical Biochemistry [online], 432(2),
pp 155–164. Available from:
http://www.sciencedirect.com/science/article/pii/S0003269712004022. [Accessed 2018-01-02].
Svenska Kennelklubben. Hundar, katter och andra sällskapsdjur 2012. [online] (2012). Available
from: https://www.skk.se/globalassets/dokument/om-skk/scb-undersokning-hundar-katter-och-
andra-sallskapsdjur-2012.pdf. [Accessed 2017-12-10].
Sözmen, M., Tasca, S., Carli, E., Lorenzi, D. D., Furlanello, T. & Caldin, M. (2005). Use of fine
needle aspirates and flow cytometry for the diagnosis, classification, and immunophenotyping of
canine lymphomas. Journal of Veterinary Diagnostic Investigation [online], 17(4), pp 323–329.
Available from: https://doi.org/10.1177/104063870501700404. [Accessed 2017-11-01].
Tonomura, N., Elvers, I., Thomas, R., Megquier, K., Turner-Maier, J., Howald, C., Sarver, A. L.,
Swofford, R., Frantz, A. M., Ito, D., Mauceli, E., Arendt, M., Noh, H. J., Koltookian, M., Biagi,
T., Fryc, S., Williams, C., Avery, A. C., Kim, J.-H., Barber, L., Burgess, K., Lander, E. S.,
Karlsson, E. K., Azuma, C., Modiano, J. F., Breen, M. & Lindblad-Toh, K. (2015). Genome-wide
association study identifies shared risk loci common to two malignancies in golden retrievers.
PLOS Genetics [online], 11(2), p e1004922. Available from:
http://journals.plos.org/plosgenetics/article?id=10.1371/journal.pgen.1004922. [Accessed 2017-
11-24].
Trevejo, R., Yang, M. & Lund, E. M. (2011). Epidemiology of surgical castration of dogs and cats in
the United States. Journal of the American Veterinary Medical Association [online], 238(7), pp
898–904. Available from: https://avmajournals.avma.org/doi/full/10.2460/javma.238.7.898.
[Accessed 2017-12-10].
Vezzali, E., Parodi, A. L., Marcato, P. S. & Bettini, G. (2010). Histopathologic classification of 171
cases of canine and feline non-Hodgkin lymphoma according to the WHO. Veterinary and
Comparative Oncology [online], 8(1), pp 38–49. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1476-5829.2009.00201.x/abstract. [Accessed 2017-
10-26].
Villamil, J. A., Henry, C. J., Hahn, A. W., Bryan, J. N., Tyler, J. W. & Caldwell, C. W. (2009).
Hormonal and sex impact on the epidemiology of canine lymphoma. Journal of Cancer
Epidemiology [online]. Available from: https://www.hindawi.com/journals/jce/2009/591753/.
[Accessed 2017-10-24].
Yoon, J., Feeney, D. A., Cronk, D. E., Anderson, K. L. & Ziegler, L. E. (2004). Computed
tomographic evaluation of canine and feline mediastinal masses in 14 patients. Veterinary
Radiology & Ultrasound [online], 45(6), pp 542–546. Available from:

31
http://onlinelibrary.wiley.com/doi/10.1111/j.1740-8261.2004.04093.x/abstract. [Accessed 2017-
11-01].
Zandvliet, M. (2016). Canine lymphoma: a review. Veterinary Quarterly [online], 36(2), pp 76–104.
Available from: http://dx.doi.org/10.1080/01652176.2016.1152633. [Accessed 2017-10-24].


















