Prof Malcom PPT

of 54
-
Upload
onon-essayed -
Category
Documents
-
view
239 -
download
0
Transcript of Prof Malcom PPT
-
7/29/2019 Prof Malcom PPT
1/54
The modern role of beta-blockers inthe treatment of cardiovascular
disease; focus on hypertension
JM Cruickshank
Saudi ArabiaNovember 2012
-
7/29/2019 Prof Malcom PPT
2/54
The Cardiovascular Continuum
-
7/29/2019 Prof Malcom PPT
3/54
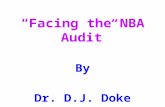
The Effect of Early Intervention with Atenolol in Reducing
Mortality in Acute Myocardial Infarction; ISIS-1
500
400
300
200
100
0
48
73
171
231
261
119
167
208
234
294
266
321
287
341
312
364
330
382
344
403
359
419
368
439
386
458
402
475
420
491
1 2 3 4 5 6 7 8 9 10 1112 13 14
Group allocated
control
Group allocatedatenolol
*** 2p < 0.002
** 2p < 0.04***
**
EarlyI.V. 5 + 5mg End of
oral dose
Days from randomisation
Oral 100mg/day
Numberof
vasculardeaths
-
7/29/2019 Prof Malcom PPT
4/54
COMMIT Trial AMI cases radomised
to metoprolol or placebo
N = 45,852 AMI cases who received thrombolytics
IV followed by oral metoprolol for 1 month
No reduction in death rate by metop
Re-infarction reduced by 18% (sig) by metop VF reduced by 17% (sig) by metop
Cardiogenic shock increased 30% (sig) by metopmainly 1st day
Give IV BB only when haemodynamics are stable
-
7/29/2019 Prof Malcom PPT
5/54
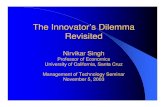
Secondary prevention of myocardial infarction with
different types ofb - blockers
b1 - selectivewithout ISA
b1 - selectivewith ISA
non-selective
without ISA
non-selective
with ISA
b- blockerswithout ISA
Reductionofm
ortality
b- blockerswith ISA
-30
-20
-10
-
Yusuf S et al. Progress Cardiovasc. Diseases 1985; 5: 335-371
-
7/29/2019 Prof Malcom PPT
6/54
b- blockers in MI
Kjekhus (1985)
Reduction in heart rate (min )-1
Reduction
inmortality
(%)
alprenolol
timolol
metoprolol
propranolol
practolol
sotalol
oxprenolol
pindolol
50
40
30
20
10
00 4 8 12 16 20
-
7/29/2019 Prof Malcom PPT
7/54
DECREASE-IV ; 1,066 medium-risk patients (mean age 64 y) for elective
non-cardiac surgery were randomised to control, bisoprolol (2.5 mg,
titrate to HR-50-70 bpm), fluvastatin or combination, 30 days pre-
surgery and 30 days post. Podermans et al Munich 2008.
-
7/29/2019 Prof Malcom PPT
8/54
TIBBS Study N=520 CAD Patients
Hard events (death, M.I. Hospitalisation) significantly lower on Bisoprolol than SR
Nifedipine
1.0
0.9
0.8
0.7
0.6
0.5
0 50 100 150
Days
Eventfree
survival
200 250 300 350 400
Bisoprolol
Nifedipine s.r.
p=0.03
von Arnim et al 1996
-
7/29/2019 Prof Malcom PPT
9/54
High heart-rates are harmful in patients with
stable CAD + DM. Anselmino M et al 2010
HR78
bpm
-
7/29/2019 Prof Malcom PPT
10/54
Framingham 26 y follow-up: low resting heart
rates protect from sudden death. Kannel 1985
-
7/29/2019 Prof Malcom PPT
11/54
Figure 30. Beta-blockers and hard end-point
placebo-controlled trials in systolic heart failure;
ISA reduces efficacy (all-cause death).
Xam-
ISA
(ns)% change
Bucind-ISA
10%(ns)
Nebiv-ISA
12% (ns)
Bisop
34%(sig)Metop
35%(sig)
Carv
35%(sig)
HR 13-14 bpmHR 8-9 bpm
-
7/29/2019 Prof Malcom PPT
12/54
Figure 31. CIBIS III prevention of sudden
death with bisoprolol vs ACEI. 2005
Results of the CIBIS III study: Circulation, 2005; 112:121
10
8
6
4
2
0
0 6 12
Months
%
P = 0.049
46% Riskreduction in
Sudden CardiacDeath
Enalapril - first
Bisoprolol - first
-
7/29/2019 Prof Malcom PPT
13/54
The Cardiovascular Continuum
-
7/29/2019 Prof Malcom PPT
14/54
Mortality due to leading global risk
factors. Lopez AD et al Lancet 2006
-
7/29/2019 Prof Malcom PPT
15/54
Dr. Wilfried Meyer, IMM Paris31 Aug 2011
15
Current UK NICE Committee recommendations
for the treatment of hypertension
BBs = 4th or 5th line !!
Or only among the also-runs!
-
7/29/2019 Prof Malcom PPT
16/54
Different Predictors of Diastolic Hypertension (DH) ( raised
systolic SDH) and Isolated Systolic Hypertension (ISH)
FRAMINGHAM StudyFranklin et al, Circulat 2005
Predictors of Diastolic Hypertension (
Systolic Hypertension) = DBP 90mmHg
( SBP 140 mmHg)Predictors of Isolated Systolic
Hypertension = SBP 140 mmHg +DBP < 90 mmHg
1. Young age
2. Male sex
3. High BMI at baseline
4. Increased BMI during follow-up
5. Main mechanism of DH and SDH is
raised peripheral resistance
1. Older age
2. Female sex
3. Increased BMI during follow-up (weak)
4. ISH arises more commonly from normaland high normal BP, than burned out
diastolic hypertension
5. Only 18% with newonset ISH had a
previous DBP 95 mmHg6. Main mechanism of ISH is increased
arterial stiffness = aging of arteries
-
7/29/2019 Prof Malcom PPT
17/54
Table 3. First-line beta-blockers (atenolol) perform poorly in elderly
hypertension (wide pulse-pressure)
Trial Beta-blockerMean-age
(y)
Initial BP
(mm Hg)
Pulse-
Pressure
(mm Hg)
Result
MRC ElderlyAtenolol (vs
placebo vs
diuretic)
70 185/91 94
Only 1st line diuretics differed
from placebo in stroke
prevention; diuretic superior to 1st
line atenolol in reducing coronaryevents
HEPAtenolol (vs non-
treatment)69 196/99 97
Significant reduction in stroke but
no effect on coronary events by
atenolol
LIFE
Atenolol (vs
losartan) 67 174/98 76
Losartan superior to atenolol in
reducing cardiovascular mortality
and non-fatal and fatal stroke
ASCOT
Atenolol
diuretic (vs
amlodipine
perindopril)
63 164/94 70
Amlodipine perindopril was
superior to atenolol diuretic in
reducing all-cause mortality and
all coronary and stroke end-points
-
7/29/2019 Prof Malcom PPT
18/54
Effect of different antihypertensive agents (v placebo) on
brachial (B) and aortic (A) pulse-pressure in 52 elderly
(mean age 77y) systolic hypertensives (random, DB,
crossover x 1 month). Morgan T et al 2004
0
5
10
15
B A
ACE 1 b Blockers CaB DiurB A B A B A
ACE= perindopril; BB = atenolol (25-50mg); CaB = felodipine; diur = hydrochlorth.
Fall inPulse
Pressure
(mm Hg)
*
*
-
7/29/2019 Prof Malcom PPT
19/54
Figure 23. The INVEST Study :- n=22,576 hypertensives with CHD, mean age 66y,
randomised to Verapamil / ACE inhibitor or Atenolol / Thiazide based treatment.
Equal effects on primary and secondary end points (but Verap / ACE combination
less effective in subjects with CCF). Pepine CJ et al 2003.
Calcium
Antagonist
Strategy
(CAS)
(n=11,267)
Non-Calcium
Antagonist
Strategy
(NCAS)
(n=11,309)
Rate per 1000Patient-Years
Rate per 1000Patient-Years
RR (95% CI) FavoursCAS
FavoursNCAS
First Event
Death
Non-fatal Myocardial Infarction
Non-fatal Stroke
Cardiovascular-Related Death
Cardiovascular-Related Hospitalization
36
28
5
4
14
24
37
29
5
5
14
23
0.98 (0.90-1.06)
0.98 (0.90-1.07)
0.99 (0.79-1.24)
0.89 (0.70-1.12)
1.00 (0.88-1.14)
1.03 (0.93-1.14)
0.6 0.8 1.0 1.2 1.4
RR (95% CI)
-
7/29/2019 Prof Malcom PPT
20/54
In 30 lean (L), 20 peripherally obese (PO) and 26 centrally obese
(CO) subjects (mean age 36y), muscle sympathetic nerve activity
(MSNA) was significantly higher in CO than PO and L subjects
70
55
40
25L PO CO
MSNA
***
*
(bs/100 hb)
Grassi et al, J.Hypertens 2004
S mpatho e itation in normal ei ht and obesit
-
7/29/2019 Prof Malcom PPT
21/54
Sympatho-excitation in normal-weight and obesity-
related hypertension (HT), vs normotensives (NT), in
middle-aged (37-50 y) subjects.
Lambert E et al 2007
-
7/29/2019 Prof Malcom PPT
22/54
Framingham: Effect of resting heart rate on all-cause death, CHD and
CVD events in untreated male hypertensives, followed-up for 36 years.
Gillman MW et al 1993.
Figure 28a R l ti hi b t ) hi h ( 4 l/L
-
7/29/2019 Prof Malcom PPT
23/54
Figure 28a. Relationship between a) high (> 4 nmol/L =dotted line) and low (< 4 nmol/L = continuous line) plasma
noradrenaline levels (independent of BP) and survival, and (b)
cardiovascular mortality, in middle-aged hypertensives.
Peng Y-X et al 2006.
-
7/29/2019 Prof Malcom PPT
24/54
Agonist Activity and the b1 ReceptorFullb1 agonist activity (efficacy)eg. Noradrenaline
Cellwall
Full coupling
Ca++Troponin
cAMP
Phosphorylation
Contraction
(Cardiac = +ve inotropism)
ATP
b1
Highaffinity
G
-
7/29/2019 Prof Malcom PPT
25/54
Risk
Ratio
Beta-receptor density (Bmax) and cAMP levels (in
lymphocytes) as predictors of MI and stroke in middle-aged
hypertensives followed for 7 years. Peng Y 2006.
1.851.9
1.17 1.18
-
7/29/2019 Prof Malcom PPT
26/54
Randomised, controlled hypertension ( diabetes) studiesof 1st line BBs in young/middle-aged diastolic hypertensives
Trial BBMean Age
(y)
Initial BP
(mm Hg)
PP
(mm Hg)
IPPPSHOxprenolol
(v diuretic) 52 173 / 108 65
MRC Mild
Hypertension
Propranolol
(v diuretic v
placebo)
51 161 / 98 63
MAPHY Metoprolol(v diuretic) 52 167 / 108 59
UK PDSAtenolol
(v Captopril) 56 159 / 94 65
di b /h i d d i i h
-
7/29/2019 Prof Malcom PPT
27/54
UKPDS 39 - diabetes/hypertension study end points in the
randomised Tight (1st line atenolol or captopril) and Less Tight BP
control groups (BP diff=10/5); 10 year follow-up(RR plus 95% confidence intervals)
UK Prospective Diabetes Study Group
Any diabetes related end point
Deaths related to diabetes
All cause mortality
Myocardial infarction
Stroke
Peripheral vascular disease
Microvascular disease (eye/kidney)
0.1 1 10
Favours tightcontrol
Favours less tightcontrol
Clinical end point
-
7/29/2019 Prof Malcom PPT
28/54
UKPDS all primary end-point trends favour atenolol
vs captopril when compared with less-tight BP control
(diff = 10/5 mm Hg) over 10 year follow-up
% decrease
vs less tight
BP-control
-
7/29/2019 Prof Malcom PPT
29/54
UKPDS Study Effect of BB or ACE inhibitor
on death from any cause after 20 years
follow-up. NEJM 08
Death from any cause
- 23% less on BB(*)
-
7/29/2019 Prof Malcom PPT
30/54
BB/Smoking interaction (MI)
in young/mid-age hypertensives
% reduct
in MI
IPPPSH
Ox vs D
MRC1
Pr vs P
MRC1
Pr vs D MAPHYMe vs D
-
7/29/2019 Prof Malcom PPT
31/54
BB/smoking interaction (CV events)
in the elderly hypertensive (MRCe)
% reduct
CV event
vs placebo
Aten 1st
Diu 2nd
Aten 2nd
Diu 1st
-
7/29/2019 Prof Malcom PPT
32/54
Effect of Smoking ( ) and Sham Smoking
( ) on Plasma Catecholamines
Norepinephine
(pg/ml)
Epinephrine(pg/ml)
350
300
250
150
100
50
200
150
0
-10 0 10
Minutes
20 30
Cryer et al. 1976
-
7/29/2019 Prof Malcom PPT
33/54
Peri-operative interaction between adrenaline
and beta-blockers. Tarnow J, Muller R 1991
Change in
Mean BP
-mm Hg
39.2
18.1
9.39.0
TIBBS S d N 520 P i i h ild
-
7/29/2019 Prof Malcom PPT
34/54
TIBBS Study N=520 Patients with mild
hypertension and CAD
1.0
0.9
0.8
0.7
0.6
0.5
0 50 100 150
Days
Eventfree
survival
200 250 300 350 400
Bisoprolol
Nifedipine s.r.
p=0.03
von Arnim et al 1996
-
7/29/2019 Prof Malcom PPT
35/54
Figure 13. Decrease in coronary atheromatous volume
(mm3) by BBs over 1 year (independent of statins, ACE
inhibitors, other drugs, LDL Conc., HR). Sipahi I et al 2007
-0.4(ns)
-2.4
(p
-
7/29/2019 Prof Malcom PPT
36/54
Table 1. In 106 patients who had 2 coronary angiograms over6 months, plaque disruption was significantly less frequent with
beta-blocker usage and more common at high heart rates.
Heidland V and Strauer B 2001
A li Mild H i S d di i
-
7/29/2019 Prof Malcom PPT
37/54
Australian Mild Hypertension Study diuretic vs
placebo in 3427 hypertensives (mean age 50 y).
Lancet 1980
n/ocases
-
7/29/2019 Prof Malcom PPT
38/54
Change in muscle sympathetic nerve activity after 3 months
diuretic therapy in untreated hypertensives. Menon DV et al
2009
% change
in muscle
symp. n.activity
spironolact chlorthalidone
-
7/29/2019 Prof Malcom PPT
39/54
Figure 21. Olmesartan vs placebo (randomised) in 4447 DM2,
mean age 57, mean BMI 31, BP 136/81, over 3.2 years.Haller H et al NEJM 2011
0
2
4
6
8
10
12
14
16
CV
death
(all)
CV
death
(CHD
history)
Sudden
death
MI
death
placebo
Olmesartan
n/o
events
p=0.01
P=0.02
-
7/29/2019 Prof Malcom PPT
40/54
Figure 22. ARBs and sympathetic nerve activity;
double-blind, random, X-over, placebo-controlled study
in young, hypertensive males. Heusser K et al 2003
BP HR
Musc
Symp
Plasma
Noradren
% change
-
7/29/2019 Prof Malcom PPT
41/54
ABCD Study; in middle-aged hypertensives with
diabetes randomised to enalapril or nisoldipine
there was a significant increase in MI in the CB
group. Estacio RO et al 1998
n/o MI p
-
7/29/2019 Prof Malcom PPT
42/54
Dihydropyridine CBs and noradrenaline/resting heart-
rate levels after 24 weeks therapy. Fogari R et al 2000.
-
7/29/2019 Prof Malcom PPT
43/54
80
60
40
20
non-smokers (n = 69) smokers (n = 25)
64%58%
80%
52%
p
-
7/29/2019 Prof Malcom PPT
44/54
160
150
140
130
120
110
100
90
80
70
60
BP
(mmHg)
and
Heart Rate
In 34 young (28-55yrs) hypertensives, Bisoprolol 5mg was more
effective than Amlodipine 5mg, Doxazosin 104mg, Bendrofluazide
2.5mg, Lisinopril 2.5-10mg (double blind, crossover,
1 month each) incontrolling office and 24 hr BP
Deary; Brown et al J. Hypert. 2002
Anti hypertensive efficacy of bisoprolol(5mg)
-
7/29/2019 Prof Malcom PPT
45/54
Anti-hypertensive efficacy of bisoprolol(5mg),
losartan, amlodipine and diuretic in 187 middle-aged
men; random, D-B, placebo-controlled x 1 month.
Porthan K et al 2009
Bisoprolol vs losartan: effects (rand/DB) on
-
7/29/2019 Prof Malcom PPT
46/54
Bisoprolol vs losartan: effects (rand/DB) on
BP/renal function over 1 year in 72
hypertensives (mean age 50 y). Parrinello G et al 2009
% change
DBPCreat
Clear
X (sig)
SBP
-
7/29/2019 Prof Malcom PPT
47/54
Effect of bisoprolol and enalapril on LVH in 56
randomised hypertensives, mean age 50y, over a 6
month periodGosse et al 1990
10
5
15
5
10
15
5
10
%
reduction
LVM
PWT
Septal T
Bisoprolol Enalapril
7
13
11
4
3
7
-
7/29/2019 Prof Malcom PPT
48/54
Fogarl et al 1980
Effect of various Beta Blockers on HDL
**
****
**
**
**
**
**
**
** *
+10
0
-10
-20
-30
-40 6 12 18 24 30 36 months
* p < 0.05
** p < 0.01vs. baseline}
%
HDL-
cholesterol
MepindololBisoprolol
PropranololAtenolol
-
7/29/2019 Prof Malcom PPT
49/54
Bisoprolol: b1-selectivity and glucose metabolism in hypertensives
with type II diabetes mellitus (2 hr after administration)
170 10
9
8
7
6
160
150
140
130
120
110
100
A B C A B C(p >0.05)C-B (p >0.05)C-B
glucose(mg/dl)
HbA(%)
1
A: initial value B:after 2 weeks
of bisoprolol
C:after 2 weeks
of placebon = 20x + SEM
Janka HU et al. J Cardiovasc Pharmacol 1986: 8 (Suppl.11): 961 99
Eff t f Bi l l d At l l Ai R i t
-
7/29/2019 Prof Malcom PPT
50/54
90
9
8
7
70
50
b1 3 6 12
Placebo Bisoprolol Atenolol
1 3 6 12 1 3 6 122 4 6 24 b 2 4 6 24 b 2 4 6 24
AWR
(cm HO/l/s)2
HR
(beats/min)
Effect of Bisoprolol and Atenolol on Airway Resistance
in patients with Reversal Obstruction Airways Disease
Dorow et al 1986
-
7/29/2019 Prof Malcom PPT
51/54
Beta-blockers and sexual
dysfunction vs placebo
Beta-blocker Sexual dysfunction
- % increase vs
placebo
Reference
Carvedilol 13.5 Fogari R et al 2001
Propranolol 5.0 MRC-Mild Hypert
1985
Atenolol 3.0 Silvestri A et al
2003
Bisoprolol 0.0 Broekman CP et al
1992
-
7/29/2019 Prof Malcom PPT
52/54
100
75
50
25
0
ICI 118,551
B1/B2
Selectivity
Ratios
PropranololMetoprolol
AtenololBetaxolol
Bisoprolol
1/25
20 /1
35 /135 /1
75 /1
1/50
1/300
1/300
12/
Wellstein et al Europ Heart J 1987
Beta1 and Beta2 Selectivity Ratios
-
7/29/2019 Prof Malcom PPT
53/54
Conclusion
Beta-blockers are highly effective across the whole CV spectrum The active ingredient is beta-1 blockade
Thus highly beta-1 selective bisoprolol is the most effective way tolower BP in young/middle-aged, reverse LVH, preserve renal function,reverse/stablise atheroma, avoid metabolic disturbance and the vitalsmoking/adrenaline/hypertension interaction (seen withnon/moderately selective BBs),and avoid impotence (worst with carv)
In the young/middle-aged hypertensive beta-1 blockade is highlyeffective in preventing stroke/MI/CCF vs placebo/diuretics; in theelderly BBs belong second-line to diuretics or CBs (1st line if CAD )
Beta-1 selective bisoprolol is a highly effective anti-ischaemic, anti-
arrhythmic and anti-heart failure agent
Longditudinal observational cohort studies
-
7/29/2019 Prof Malcom PPT
54/54
Longditudinal, observational cohort studies
draw wrong conclusions on beta-blockers.
Bangalore S et al JAMA 2012