Product Level Information (PLI) - aras.com · ... DHF FDA - DMR FDA - DHR FDA - QS G e n e r a l f...
32
Public © 2012, Carestream Health Product Level Information (PLI) The PLM Journey
Transcript of Product Level Information (PLI) - aras.com · ... DHF FDA - DMR FDA - DHR FDA - QS G e n e r a l f...

Public
© 2012, Carestream Health
Product Level
Information
(PLI)
The PLM Journey

2
Public
© 2012, Carestream Health
2
Public
© 2012, Carestream Health
Abstract
This presentation outlines the implementation of Product Level Information
(PLI) utilizing Aras Innovator at Carestream Health, Inc.
Topics include:
• Snapshot of Carestream Health
• Why implement now? Current state drivers…
• Timelines
• Deployment Strategy
• Challenges
• New Development Plan

3
Public
© 2012, Carestream Health
David Sherburne Director
R&D Effectiveness, Engineering IT
Eli Tuber Process Re-Engineering
R&D Effectiveness
Rich Graham Platform Architecture
R&D Effectiveness
Chris Kapell Hardware Commercialization Process Platform Manager
R&D Effectiveness
ACE Attendees from Carestream Health, Inc.

4
Public
© 2012, Carestream Health
4
Public
© 2012, Carestream Health
An independent company with a proven track record and $2.5 billion in revenue
A world leader in:
• Medical imaging … digital and film
• Healthcare information solutions
• Dental imaging and dental practice
management software
• Molecular imaging
• Non-destructive testing
Carestream Health – Who We Are

5
Public
© 2012, Carestream Health
5
Public
© 2012, Carestream Health
Who We Are
Approximately 7,300 employees serve customers in more than 150 countries worldwide
We hold more than 1,000 patent for technology and intellectual property
Our products are at work in 90 percent of hospitals worldwide

6
Public
© 2012, Carestream Health
Where We Are
An independent, global company with 17 manufacturing and R&D locations, including three Technology & Innovation Centers…
…supporting sales and service teams in 150 countries
Technology &
Innovation Centers
Rochester, New York
Genoa, Italy
Shanghai, China
R&D and
Manufacturing Sites
Paris, France
Rochester, New York
Ronkonkoma, New York
Shanghai, China
Yokneam, Israel
R&D Sites
Atlanta, Georgia
Baltimore, Maryland
London, England
Oakdale, Minnesota
Ra’anana, Israel
Woodbridge, Connecticut
Manufacturing Sites
Berlin, Germany
Guadalajara, Mexico
White City, Oregon
Windsor, Colorado
Xiamen, China

7
Public
© 2012, Carestream Health
7
Public
© 2012, Carestream Health
Globalization was required to meet the business needs of our
company
• Desired access to global talent
• Needed a balanced cost structure
• Presence in emerging markets
Impact of Globalization
• Collaboration became more time consuming via email; uncontrolled
data sharing with partners
• Complexity in the organization increased as projects globalized
• Knowledge-workers’ time was drained, impacting innovation
• Productivity of NPD remained roughly flat
Business Challenges

8
Public
© 2012, Carestream Health
8
Public
© 2012, Carestream Health
• Quality and Compliance must be maintained in our business
• Project teams are split across several locations
• Platform development adds complexity
• Iterative methods require faster information transfer
• Faster prototyping cycles are needed for hardware
• Design for manufacturability and supplier IP capture are critical as ties
to the supplier base weaken
• Access to historical data is needed to improve planning, compare
reliability, and drive improvements to the development cycles
• Engineers are required to do deeper analysis to ensure product quality
• Requests for metrics are ever increasing and are difficult to produce
• Disjointed IT and non-standard process environment kills collaboration
Demands on Staff are Ever Increasing

9
Public
© 2012, Carestream Health
9
Public
© 2012, Carestream Health 5/17/2012
Product Service Information –
Processes and Tools
Product Manufacturing Information –
Processes and Tools
Product Design Information –
Processes and Tools
Project Information –
Processes and Tools
Site A
Site B
Site C
FDA - DHF
FDA - DMR
FDA - DHR
FDA - QS
Ge
ne
ral f
low
of p
rod
uct
info
rma
tion
“AIR GAPS”
between blocks
represent
inefficient
manual sharing
of information.
Innovative people innovate
many local processes.
Local
resources
focus on
product
families.
Complexity
increased as
work required
flow between
sites.
Non-Standard Commercialization Process

10
Public
© 2012, Carestream Health
10
Public
© 2012, Carestream Health
Enterprise PDM Authoring
Point Solutions worked but lacked proper architecture to enable global productivity
MCAD Tools
NX
Pro/E
SolidWorks
AutoCAD
ECAD Tools
Mentor DX
Cadence
OrCAD
Altium
Software
Authoring
Desktop Tools
(Browser,
MSOffice, etc)
EE File
Shares,
library
cache
MQDS
SAP
Lotus Notes DB
CAPA
SOP
DA MMR
Lotus Domino
DocManager
Version Control Tools
DOORS Requirements
Management Tools
Clearcase
Subversion PVCS
StarTeam
ClearQuest Defects
Enhancement
Requests
BOM
Electrical Part
Data, RoHS
Part
Data
CAD Files PDF’s
Quality Center
External
Systems
Standalone
Systems
Manual
Integration
Automated
Integration
Information
Flow
No Integration
No
Integration
No
Integration
No Integration
MS Project
Team Room
CAPA CAPA
Confluence
Excel
Sys 9K RoHS,
DoC,
MSDS
(no
home)
CAD Files PDFs
CIDx
Intralinks
Teamcenter
File Shares
EQDS
CQuest
No
Integration
No
Integration
No
Integration
Problem was
caused by an “IT
Cost Center”
mentality and
non- coordinated
local efforts .

MCAD Tools
Knowledge Sharing, Social Nets,
and Webchannel Desktop Enterprise Systems
Supplier 1
Supplier 3
ECAD Tools
ECAD 1
ECAD 2
ECAD 3
Integrated As Built
Master Data
Raw Material Master
SW Project Management,
Dashboards
(Rally)
KM
Platform
PLM Aras Innovator
Closed Loop Engineering Change
Management (HW/SW)
Event Tracking and Defect Mgmt
CAPA Management
Audit Management
Supplier Access/ DFM Input
Supplier Quote
ECAD, MCAD PDM Integrations
EBOM, MBOM Management
Costing
Commercial Parts Library
RoHS
Requirements Change Control
ISDE Integration for SW events
SW CM –
SVN
Build Tools and Services
Test Scripting
Build Configuration
Management
RQMTS
PDM Upgrade
End of
Life
Established
Standard
LN DBs
MS Visual Studio
XCODE, Other
Key IDEs
SW Authoring
Office,
Project
Auth
ori
ng S
yst
em
s
New
Platform
No
Standard
PDM
SAP
Some
Integration
Quality
Platform
(HPQC)
Dashboards –
Metrics
Manufacturing Transfer
Testing
HW
Emerging
Standard
2012
Proposal
Purchase
Portals –
ECoutlook
Smart source-Ebid
ISDE
Core
New
Modeling
Integrated SW Development Environment- SW Environment)
Supplier 2
Webchannel/
Social
Development
2010-13 New Product Development Foundation
11

Enterprise Systems
PLM Aras Innovator
Closed-Loop Engineering Change
Management (HW/SW)
Event Tracking and Defect Mgmt
CAPA Management
Audit Management
Supplier Access/ DFM Input
Supplier Quote
ECAD, MCAD PDM Integrations
EBOM, MBOM Management
Costing
Commercial Parts Library
RoHS
Requirements Change Control
ISDE Integration for SW events
12
2010-12 New Product Development Foundation

13
Public
© 2012, Carestream Health
2009 – Implement a Globally Standard
Closed-Loop Change-Management System

14
Public
© 2012, Carestream Health
14
Public
© 2012, Carestream Health
2009 Technology Partner Selection Model
Give Yourself Time Business Objectives
Identify Missing Capabilities
ROI of New Capabilities
Strategies to Obtain Capabilities
Business Requirements
Write Key Use Cases
Final Selection of Partners
Request for Information Request for Quote
April 2009 Time ~ 9 months 1½ FTEs Dec 2009
Look for a strategic relationship
Share in risk
Offer flexible terms in line with
business ROI
Remain a partner during
implementation
Keep costs in line with benefits
Aras Identified as a potential
partner

15
Public
© 2012, Carestream Health
15
Public
© 2012, Carestream Health
APR MAY JUN JUL AUG SEP OCT NOV DEC JAN FEB MAR
Requirements Development
RFP Issued
RFP Review
First Cut Decision
ROI Analysis
Supplier Capability Analysis
Second Cut Decision &
RFQ Issued
RFQ Analysis
Vendor Selection
Project Start
Request for Proposal (RFP) issued for applications
and implementation sent to five (5) suppliers and
two (2) implementers
Potential suppliers reduced to two (2)
Potential implementers reduced to three (3)
Aras added as a potential supplier and implementer
Potential suppliers reduced to two (2)
Potential implementers reduced to three (3)
Request for Quote (RFQ) issued
Aras selected as supplier
Corporate funding secured
2009 2010
Third Party Analysis
Carestream Health Product-Level
Information Timeline

16
Public
© 2012, Carestream Health
16
Public
© 2012, Carestream Health
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
Framework Development
Change Management
Development
Platform Release Go/No Go
Event Tracking & SAP
Integration Development
Event Tracking & SAP
Integration Go/No Go
EHS CAPA and Supplier
Access Development
EHS CAPA and Supplier
Access Go/No Go
2010
Carestream Health Product Level Information
Initial Development and Deployment Timeline

17
Public
© 2012, Carestream Health
17
Public
© 2012, Carestream Health
ACE – Spring 2010
Feedback
• Are you nuts!!!
• That’s really aggressive!!
• Good Luck with that!!

18
Public
© 2012, Carestream Health
18
Public
© 2012, Carestream Health
Project Realization – June 2010
• Requirements gathering and analysis is difficult
• Deployment planning across a global organization is complicated
− Some businesses asked us to avoid 4th quarter deployments of major changes
• Underestimated training
• Decided to re-plan project
− Deploy base functionality in early Q4 2010
• Retire legacy commercial parts database
• Socialize the environment
• Understand deployment issues
−Deploy core functionality in Q2 & Q3 of 2011

19
Public
© 2012, Carestream Health
19
Public
© 2012, Carestream Health
NOV DEC JAN FEB MAR APR MAY JUN JUL AUG SEP OCT
Deploy Basic
Functionality Process Verification& Re-development Ready to Deploy Began Deploying Business by Business
2010 2011
Resulting Timeline
OCT
Close the “Air Gaps”

20
Public
© 2012, Carestream Health
20
Public
© 2012, Carestream Health
Resulting Time Line
October 2010 – Released commercial parts requests & database including the Mentor Design Library
• Implemented integration to Mentor DX Designer
October 2010 – Sept 2011
• Process Verification & Re-development
– Defect Management
– Engineering Change
– Audit Management System (added module into scope)
• Removed Corrective Action (CAPA) Module
– CAPA Development was complete but gains did not outweigh the effort of getting people to switch off our Lotus Notes-based system

21
Public
© 2012, Carestream Health
21
Public
© 2012, Carestream Health
What Is Deployed
October 2011
• USA & China
– Full closed-loop change process; Defect Management -> Engineering Change
January 2012
• USA
– Audit Management System Pilot
February 2012
• USA & China
– Engineering Change
April 2012
• China
– Defect Management -> Engineering Change

22
Public
© 2012, Carestream Health
22
Public
© 2012, Carestream Health
What’s Left
May – June 2012 (Three more business unit deployments)
• USA & China
– Full closed-loop change process; Defect Management -> Engineering
Change
• Total users: Currently 450, Projected 750 -1000 by YE 2012

23
Public
© 2012, Carestream Health
What Went Right
• Documenting the processes & closing the “Air Gap”
• Sacrificed schedule for quality and completeness
– Limited impact to Product Development
• First deployed basic functionality
– Commercial Parts, Mentor Library Integration
– Allowed us to socialize the environment
– Resolve accounts, deployment, and workstation issues

24
Public
© 2012, Carestream Health
What Went Right
• Initially deployed Closed-Loop Change Management to a fairly self-contained group in Shanghai
– Allowed us to fix any major issues quickly and limited impact
•Concurrent Global deployment went smoothly
•Data migration out of:
– Mentor DMS (electrical symbols, cells, and commercial parts)
– ClearQuest (defects)
– Matrix One (engineering change)
•Training was developed internally and was focused on process

25
Public
© 2012, Carestream Health
What Went Right
All of the following were equal to or better than the average, as
identified by a PLM industry expert.
• Costs (implementation and on-going)
• Schedule
– We delayed our schedule but is was average for the industry
• Functionality
• Scale and Scope

26
Public
© 2012, Carestream Health
Public
© 2012, Carestream Health
What Went Wrong
Attempted to utilize Agile development methodology from our
consulting partner
• Functionality vs. Schedule was too aggressive
– Developed functionality faster than we could absorb it
– Resource conflicts between reviewing and testing development
code and developing requirements for other capabilities
– SMEs did not have enough time to look at iterations

27
Public
© 2012, Carestream Health
Public
© 2012, Carestream Health
What Went Wrong
• The project became a waterfall-type project, and the following
came to light
– Managing change across four development sites is time consuming
– Creating the details up front is too complex and was not effective
– Users not sure what they wanted
– Users cannot really tell you what they want until they touch and feel
something
• So we had to sacrifice schedule for quality and completeness

28
Public
© 2012, Carestream Health
28
Public
© 2012, Carestream Health
What’s Changed
Created our own development team
• 4 FTEs in Shanghai; 0.5 FTE in USA
– Still challenges our ability to keep up with testing, utilizing
deployment, and supporting resources
• Switched the program management to an Agile and Iterative
development methodology
– Continuing to mature
29
Public
© 2012, Carestream Health
© 2012, Carestream Health
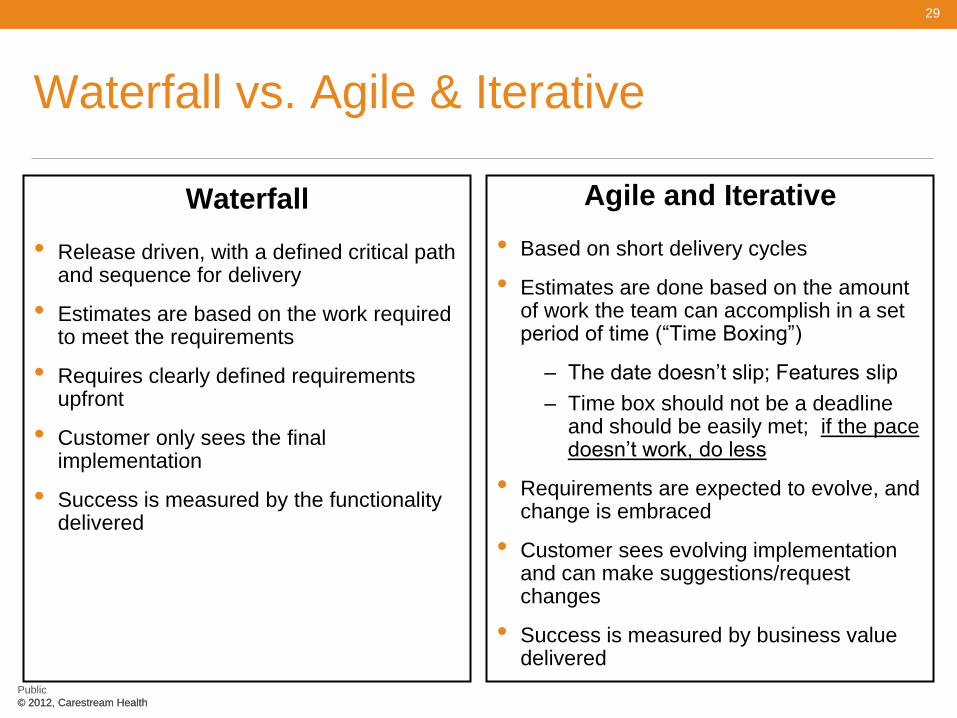
Waterfall vs. Agile & Iterative
Waterfall
• Release driven, with a defined critical path and sequence for delivery
• Estimates are based on the work required to meet the requirements
• Requires clearly defined requirements upfront
• Customer only sees the final implementation
• Success is measured by the functionality delivered
Agile and Iterative
• Based on short delivery cycles
• Estimates are done based on the amount of work the team can accomplish in a set period of time (“Time Boxing”)
– The date doesn’t slip; Features slip
– Time box should not be a deadline and should be easily met; if the pace doesn’t work, do less
• Requirements are expected to evolve, and change is embraced
• Customer sees evolving implementation and can make suggestions/request changes
• Success is measured by business value delivered

30
Public
© 2012, Carestream Health
Public
© 2012, Carestream Health
Current Development
Six to eight-week release made up of 4 - 2 week iterations (Sprints). • Maintain a constant pace • 1-2 weeks planning iteration
– If a user story is not defined thoroughly, it does not get put into the release
• 2 weeks development iteration • 2 weeks development/QA iteration • 1-2 weeks validation testing iteration
Up to now, most of our development has been fixes and point enhancements • So we release to production at the end of the release
• We still tend to put too much into the box
• It’s hard to strip functionality out if it is not ready, without negatively impacting code quality
New functionality, such as the revamped Engineering Change Implementation (ECI) and Supplier Integration, will have multiple time box development iterations before being released into production.

31
Public
© 2012, Carestream Health
31
Public
© 2012, Carestream Health
What’s Next
Short term
• Enhancement of the Engineering Change Implementation (ECI) with integration with SAP
• Software Development Environment Integration
• Brush off CAPA and add additional features
• Supplier Integration
• Visualization
Long term
• Requirements Management
• Project Management and Design History File (DHF) incorporation
• Standard Operating Procedures
• Manufacturing Work Instructions

32
Public
© 2012, Carestream Health
Carestream Health, Inc.
Questions?














![v ] ] u l v o f v f v µ À f ] v f } R µ V › storage › app › public › unalk... · D } o ] Ì u W ] v u o ] v ] v } l µ o l f o f f v v f f Ç f o u Ç Z Ì f f l º º](https://static.fdocuments.us/doc/165x107/5f189f94edad7c27c0292753/v-u-l-v-o-f-v-f-v-f-v-f-r-v-a-storage-a-app-a-public-a.jpg)