Procedures for measuring and verifying gastric tube ... · Rev. Latino-Am. Enfermagem Review...
13
Review Article Rev. Latino-Am. Enfermagem 2017;25:e2908 DOI: 10.1590/1518-8345.1841.2908 www.eerp.usp.br/rlae Procedures for measuring and verifying gastric tube placement in newborns: an integrative review Flávia de Souza Barbosa Dias 1 Suellen Cristina Dias Emidio 2 Maria Helena Baena de Moraes Lopes 3 Antonieta Keiko Kakuda Shimo 4 Ana Raquel Medeiros Beck 4 Elenice Valentim Carmona 4 Objective: to investigate evidence in the literature on procedures for measuring gastric tube insertion in newborns and verifying its placement, using alternative procedures to radiological examination. Method: an integrative review of the literature carried out in the Cochrane, LILACS, CINAHL, EMBASE, MEDLINE and Scopus databases using the descriptors “Intubation, gastrointestinal” and “newborns” in original articles. Results: seventeen publications were included and categorized as “measuring method” or “technique for verifying placement”. Regarding measuring methods, the measurements of two morphological distances and the application of two formulas, one based on weight and another based on height, were found. Regarding the techniques for assessing placement, the following were found: electromagnetic tracing, diaphragm electrical activity, CO 2 detection, indigo carmine solution, epigastrium auscultation, gastric secretion aspiration, color inspection, and evaluation of pH, enzymes and bilirubin. Conclusion: the measuring method using nose to earlobe to a point midway between the xiphoid process and the umbilicus measurement presents the best evidence. Equations based on weight and height need to be experimentally tested. The return of secretion into the tube aspiration, color assessment and secretion pH are reliable indicators to identify gastric tube placement, and are the currently indicated techniques. Descriptors: Intubation, Gastrointestinal; Infant, Newborn; Nursing. 1 Doctoral student, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil. 2 Doctoral student, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil. Scholarship holder at Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil. 3 PhD, Full Professor, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil. 4 PhD, Professor, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil. How to cite this article Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV. Procedures for measuring and verifying gastric tube placement in newborns: an integrative review. Rev. Latino-Am. Enfermagem. 2017;25:e2908. [Access ___ __ ____]; Available in: ____________________. DOI: http://dx.doi.org/10.1590/1518-8345.1841.2908. URL day month year
Transcript of Procedures for measuring and verifying gastric tube ... · Rev. Latino-Am. Enfermagem Review...

Review ArticleRev. Latino-Am. Enfermagem2017;25:e2908DOI: 10.1590/1518-8345.1841.2908
www.eerp.usp.br/rlae
Procedures for measuring and verifying gastric tube placement in
newborns: an integrative review
Flávia de Souza Barbosa Dias1
Suellen Cristina Dias Emidio2
Maria Helena Baena de Moraes Lopes3
Antonieta Keiko Kakuda Shimo4
Ana Raquel Medeiros Beck4
Elenice Valentim Carmona4
Objective: to investigate evidence in the literature on procedures for measuring gastric tube insertion
in newborns and verifying its placement, using alternative procedures to radiological examination.
Method: an integrative review of the literature carried out in the Cochrane, LILACS, CINAHL,
EMBASE, MEDLINE and Scopus databases using the descriptors “Intubation, gastrointestinal” and
“newborns” in original articles. Results: seventeen publications were included and categorized as
“measuring method” or “technique for verifying placement”. Regarding measuring methods, the
measurements of two morphological distances and the application of two formulas, one based
on weight and another based on height, were found. Regarding the techniques for assessing
placement, the following were found: electromagnetic tracing, diaphragm electrical activity, CO2
detection, indigo carmine solution, epigastrium auscultation, gastric secretion aspiration, color
inspection, and evaluation of pH, enzymes and bilirubin. Conclusion: the measuring method using
nose to earlobe to a point midway between the xiphoid process and the umbilicus measurement
presents the best evidence. Equations based on weight and height need to be experimentally
tested. The return of secretion into the tube aspiration, color assessment and secretion pH are
reliable indicators to identify gastric tube placement, and are the currently indicated techniques.
Descriptors: Intubation, Gastrointestinal; Infant, Newborn; Nursing.
1 Doctoral student, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil.2 Doctoral student, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil. Scholarship holder at Coordenação de
Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil.3 PhD, Full Professor, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil.4 PhD, Professor, Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, SP, Brazil.
How to cite this article
Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV. Procedures for measuring and verifying gastric
tube placement in newborns: an integrative review. Rev. Latino-Am. Enfermagem. 2017;25:e2908. [Access ___ __ ____];
Available in: ____________________. DOI: http://dx.doi.org/10.1590/1518-8345.1841.2908.
URL
daymonth year

www.eerp.usp.br/rlae
2 Rev. Latino-Am. Enfermagem 2017;25:e2908.
Introduction
Insertion of Gastric Tube (GT) in Newborns (NB)
hospitalized in the Neonatal Intensive Care Unit (NICU)
is one of the most commonly performed nursing
procedures. It is indicated for gastric decompression,
administration of medications, and mainly for feeding
the gastric tube process, and despite being a standard
procedure for nurses working in the NICU, it is not
risk free and involves decisions that may compromise
patient safety(1).
Some of the important aspects to increase safety
in using GT in newborns involve care in measuring the
insertion length, assessing placement/positioning of the
distal end of the tube, and in maintaining its correct
positioning(1). Serious respiratory complications may
occur due to bronchopulmonary aspiration of gastric
contents or inadequate tube placement reaching the
respiratory tract. Intestinal absorption problems and
alimentary intolerance related to GT positioning in the
pylorus or duodenum can also occur. Moreover, difficulties
encountered in the trajectory can cause puncture injuries
to the esophagus or respiratory tract(2). The occurrence
of errors in GT placement is very frequent: studies
show proportions of 47.5 to 59% inadequate placement
between neonatal and pediatric patients(3-4).
The nurse’s decision-making process during gastric
tube procedure begins with the choice of an effective
method that has a strong association with measuring
the actual tube route from the nostril or oral cavity to
the body of the stomach, passing through the entire
length of the esophagus(1).
After choosing the measuring method and
performing the insertion, it is necessary to verify that
the distal end of the tube has reached the body of the
stomach, as well as whether all the distal orifices are
within the gastric cavity in order to prevent fluid leakage
into the esophagus or duodenum(1).
Radiological examination of the chest and abdomen
is considered the gold standard verification technique,
since it allows visualization of the GT route and the
positioning of its distal end. Despite presenting the
most reliable result, this technique is costly and is
not commonly used in neonatal clinical practice for
this reason, as the GT is often replaced, and repeated
exposure to radiation can be dangerous(2). Another
limitation is the fact that this test is only effective at the
moment it is performed, since tube displacement can
happen immediately after(2,5), thus requiring the use of
other techniques to assess tube placement other than
radiological examination.
In this integrative review, we sought evidence
that may assist nursing assistants in the decision-
making process regarding gastric tubes in newborns
in the NICU, given the importance of always choosing
the best health practices aiming at patient safety. Thus,
this study aimed to investigate evidence in the literature
on procedures for measuring gastric tube insertion in
newborns and verifying its placement, using alternative
procedures to radiological examination.
Method
This is an integrative review of the literature which
seeks to synthesize results from previous studies on
the proposed subject(6). Integrative reviews have the
potential to evidence comprehensive understanding of
specific issues and to identify gaps in knowledge. This
is a very useful method for nurses who are in clinical
practice and wish to perform nursing assistance based
on scientific evidence(7-9).
The steps followed in elaborating this review
were: establishing the research question, conducting
a literature search, evaluating data, analysing the
included studies, interpreting the results and presenting
the review(8).
The guiding question of this study was “What are
the procedures for measuring gastric tubes in newborns
and for assessing its placement, other than radiological
examination?”
The search was performed in January 2017 in
the following databases: Cochrane Library, Cumulative
Index to Nursing and Allied Health Literature (CINAHL),
Excerpta Medica dataBase (EMBASE), Literature of
Latin American and the Caribbean on Health Sciences
(LILACS), Medical Literature Analysis and Retrieval
System Online (MEDLINE) and Scopus. No time frame
for inclusion of articles was established.
The terms used in the searches were extracted
from the Health Sciences Descriptors (DeCS) and
from the Medical Subject Headings (MeSH), and
included: Intubation, Gastrointestinal and Newborns,
as well as their respective versions in Portuguese and
Spanish. Synonymous terms suggested by EMBASE at
the time of the search were also searched. In order
to delimit the search, publications with the terms
gastrostomy, pain, surgery and intubation intratracheal
were excluded for not addressing the subject of this
review. Publications contained in the references of the

www.eerp.usp.br/rlae
3Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV.
selected studies whose titles addressed the research
subject were also investigated.
Article selection was carried out by two researchers
independently, and inclusion criteria were: original
studies published in-full that address, in the title or
abstract, gastric tube measurement procedures and/
or techniques for assessing its placement, and which
included newborns in the studied sample; studies
published in Portuguese, English or Spanish. Theses
and dissertations, pilot studies, review articles, case or
experience reports, letters, editorials and publications
where the method was not clearly described were
excluded. PRISMA recommendations(10) were followed
for the study selection, as shown in Figure 1.
A form with the following items was elaborated by
the authors for developing the analysis: bibliographic
reference, level of evidence, language, country of origin,
main researcher’s training, database, objective, study
design, ethical considerations, subjects, main results,
conclusion and limitations.
Seven (7) levels of classification were considered
to categorize the level of evidence: level 1 - systematic
review or meta-analysis of controlled clinical trials; level
2 - well-delineated randomized controlled clinical trial;
level 3 - controlled clinical trial without randomization;
level 4 - well-delineated cohort or case-control studies;
level 5 - systematic review of qualitative and descriptive
studies; level 6 - descriptive or qualitative studies; and
level 7 - opinion of authorities or experts(11). The results
were analyzed and presented in a descriptive way.
As this is an integrative review, it was not necessary
to request approval from the Ethics Committee to carry
out the study. We declare no conflicts of interest.
Records identified throughsearching the databases
(n=785)
Iden
tifica
tion
Sele
ctio
nEl
igib
ility
Incl
usio
n
Records identifiedfrom other sources
(n=3)
Records after excluding duplicates(n=612)
Tracked reports(n=52)
Excluded reports(n=560)
Full articlesexcluded
(n=35)
Qualitative studies includedin the review
(n=0)
Quantitative studies includedin the review
(n=17)
Full articles evaluated foreligibility
(n=17)
Figure 1 - Flowchart of the identification, selection and inclusion process of the studies, elaborated based on the
PRISMA recommendation(10).
Results
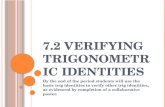
The number of publications found in the investigated
databases, as well as other sources included in this
review are presented in Figure 2.
The 17 articles included in the review were all
published in English between 1987 and 2016. The
majority of the studies were carried out in the United
States (n = 13), the main authors had training in nursing
(n = 11) and medicine (n = 6). The included studies were
classified into two categories for data analysis: “Methods
for measuring gastric tube” and “techniques for assessing
gastric tube placement”. Characterization of the articles
considering the level of evidence is presented in Figure 3.
www.eerp.usp.br/rlae
4 Rev. Latino-Am. Enfermagem 2017;25:e2908.
Database Interface Retrieved* Included*
LILACS Biblioteca virtual de Saúde – BVS Bvsalud.com
11 0
MEDLINE National Center for Biotechnology Informationncbi.nlm.nih.gov/pubmed
462 11
CINAHL EbscoHostweb.a.ebscohost.com
77 9
EMBASE Embase.com 9 0
Scopus Scopus.com 226 7
Cochrane Onlinelibrary.wiley.com/cochranelibrary 0 0
Other sources List of references from the articles 3 3
* Some publications were repeated in more than one database
Figure 2 – Number of publications found in the databases and included in the study.
N Title Authors Year Journal Country Level of evidence
1(12) Gavage tube insertion in the premature infant
Weibley TT, Adamson M, Clinkscales N, Curran J, Bramson R
1987 MCN - The American Journal of Maternal Child Nursing
United States 3
2(13) Orogastric tube insertion length in very low birth weight infants
Gallaher KJ, Cashwell S, Hall V, Lowe W, Ciszek T
1993 Journal of perinatology: official journal of the California Perinatal Association
United States 6
3(14) Indicators of feeding-tube placement in Neonates
Metheny NA, Eikov R, Rountree V, Lengettie E.
1999 Nutrition in Clinical Practice United States 6
4(15) Methods to test feeding tube placement in children
Westhus N 2004 MCN – The American Journal of Maternal Child Nursing
United States 6
5(16) Gastric tube placement in young children
Ellett ML, Croffie JM, Cohen MD, Perkins SM
2005 Clinical Nursing Research United States 6
6(17) Litmus tests for verification of feeding tube location in infants: evaluation of their clinical use
Nyqvist KH, Sorell A, Ewald U
2005 Journal of Clinical Nursing Sweden 6
7(18) Predicting internal distance to the stomach for positioning nasogastric and orogastric feeding tubes in children
Beckstrand J, Ellett MLC, McDaniel A
2007 Journal of Advanced Nursing
United States 6
8(19) Electrocardiographic guidance for the placement of gastric feeding tubes: a pediatric case series
Green ML, Walsh BK, Wolf GK, Arnold JH
2011 Respiratory Care United States 6
9(20) Predicting the insertion length for gastric tube placement in neonates
Ellett MLC, Cohen MD, Perkins SM, Smith CE, Lane KA, Austin JK
2011 JOGNN – Journal of Obstetric, Gynecologic and Neonatal Nursing
United States 2
10(21) Verification of an electromagnetic placement device compared with abdominal radiograph to predict accuracy of feeding tube placement
Powers J, Luebbehusen M, Spitzer T, Coddington A, Beeson T, Brown J, Jones D
2011 JPEN – Journal of Parenteral and Enteral Nutrition
United States 6
11(22) A weight-based formula for the estimation of gastric tube insertion length in newborns
Freeman D, Saxton V, Holberton J
2012 Advances in Neonatal Care Australia 6
12(23) Increasing the safety of blind gastric tube placement in pediatric patients: the design and testing of a procedure using a carbon dioxide detection device
Gilbert RT, Burns SM 2012 Journal of Pediatric Nursing United States 3
13(24) Comparing bedside methods of determining placement of gastric tubes in children
Ellett MLC, Cohen MD, Croffie JMB, Lane KA, Austin JK, Perkins SM
2014 Journal for Specialists in Pediatric Nursing
United States 6
14(25) Confirmation of gastric tube bedside placement with the sky blue method
Imamura T, Maeda H, Kinoshita H, Shibukawa Y, Suda K, Fukuda Y, Goto A, Nagasawa K
2014 Nutrition in Clinical Practice Japan 6
15(26) The pH of feeding tube aspirates from critically ill infants
Meert KL, Caverly M, Kelm LM, Metheny NA.
2015 Nutrition in Critical Care United States 6
16(27) Accuracy of a weight-based formula for neonatal gastric tube insertion length
Nguyen S, Fang A, Saxton V, Holberton J
2016 Advances in Neonatal Care Australia 6
17(28) Use of temporary enteral access devices in hospitalized neonatal and pediatric patients in the United States
Lyman B, Kemper C, Northington L, Yaworski JA, Wilder K, Moore C, Duesing LA, Irving S
2016 JPEN – Journal of Parenteral and Enteral Nutrition
United States 6
Figure 3 - Characterization of publications and levels of evidence of the articles included in the review.

www.eerp.usp.br/rlae
5Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV.
Methods for measuring the gastric tube
Among the articles that addressed GT measurement,
four were observational studies(13,18,22,27) and two were
experimental studies(12,20), and were mostly published
in nursing journals. With regard to ethical aspects,
only one article(12) did not report having submitted the
study to ethical appreciation. Figure 4 briefly describes
each of these studies, addressing the design, objective,
population sample, main results and limitations.
The methods described in the literature for GT
measurement in NBs include the NEX and NEMU
morphological measures. NEX (Nose, Earlobe, Xiphoid)
corresponds to the distance measured from the tip of
the nose to the earlobe to the xiphoid appendix, while
NEMU (Nose, Earlobe, Mid-Umbilicus) corresponds to
the distance measured from the tip of the nose to the
earlobe to a point halfway between the xiphoid process
and the umbilicus(12).
A method that determines the minimum insertion
length of the tube has been specifically developed for
low birth weight newborns (<1500g)(13). Minimum
insertion measures proposed in this study are 13cm for
newborns weighing less than 750g, 15cm for newborns
weighing between 750 and 999g, 16cm for newborns
weighing between 1,000 and 1,249g, and 17cm for those
weighing between 1,250 and 1,499g. Application of this
minimum insertion length method to a sample of 27 NBs
weighing less than 1,500 g showed an increase in the
proportion of correct gastric tube positioning from 62 to
86%. This method makes it possible to avoid positioning
the end of the tube above the gastreophageal junction,
thus reducing the risk of aspiration and other respiratory
complications.
In addition to these measurements, two equations
are described to estimate the insertion length of the
tube: the height-based equation(18,20) and the weight-
based formula(22). According to one of the studies(18)
selected in this review, NEX and NEMU morphological
measures do not present good predictors of the internal
measurement due to their high variability when repeated
measures are taken.
In comparing several external measurements
with internal measurement verified by endoscopy
or esophageal manometry, the results showed that
height was the best predictor for measuring the gastric
tube. The relationship between height and internal
measurement of tube passage varied according to
age; therefore, specific equations at different age
intervals were developed for calculating the insertion
measurement of the naso-orogastric tube. When these
equations were projected onto the studied sample
through computational analysis, the performance was
very promising, with success rates between 96.5 and
98.8%, depending on the infant’s age(18). However, a
major limitation of this study considering the objective
of the present review was the small participation of NBs,
with only 1% in the studied sample.
A study comparing the accuracy/success rates of
the NEX, NEMU methods and the height-based equation
(ARHB - Age Related, Height Based) performed two
different analyzes(20). In the first analysis, the end of the
tube visualized in the stomach, pylorus or duodenum
was considered as correct positioning, and the accuracy
ratio was 60.6% for NEX, 92.4% for NEMU and 100%
for ARHB. NEMU and ARHB measurements were
significantly higher than NEX (p<0.001). In the second,
more restrictive analysis, only the tubes visualized
in the stomach were considered to be positioned
correctly. The results of the second analysis were:
60.6% accuracy for NEX, 90.9% for NEMU and 78% for
ARHB. Although no significant difference (p = 0.615)
between NEX and ARHB rates were found in the second
analysis, it can be noticed that all errors presented by
NEX measure occurred by placing the tube above the
gastroesophageal junction, while the errors presented
by the ARHB measure were always below the pylorus.
This difference is relevant with respect to the type of
error, its risks and complications. During this study, the
authors also developed a new ARHB equation adjusted
for use in newborns between 35 and 56.5cm in length for
measuring the nasogastric tube: 1.95 +0.372x[height in
cm]. It was not possible to develop a new equation for
orogastric route in newborns with the mentioned length
due to the small number tubes inserted by this route in
the sample (10.4%)(20).
Another method described in the literature is the
weight-based equation(22). The authors justify the need
to create this method based on the fact that height is not
an easily accessible measure in neonatal clinical practice,
while in contrast weight is a more viable predictor as it is
checked daily and used as a reference for several clinical
applications such as calculation of drug dosages, diets
and estimating catheter insertion, among others. In
this study, 218 radiological images were analyzed, and
by way of using a linear regression analysis, formulas
for orogastric (3x[weight in kg]+12) and nasogastric
tubes (3x[weight in kg]+13) were developed. When
designing such formulas in the studied sample based on
computational analysis, it was possible to predict 100%
of poorly placed nasogastric and 60% orogastric tubes.
The lower rates found in orogastric tubes may be related
to the fact that the tubes move more when positioned
in the oral cavity.
The use of the weight-based formula as an auxiliary
method to NEMU in GT insertion was described in another

www.eerp.usp.br/rlae
6 Rev. Latino-Am. Enfermagem 2017;25:e2908.
study(27), however, the result was lower than expected, with
16% of tubes being incorrectly positioned (above or near
the gastroesophageal junction). The authors suggest that
this result is justified by the fact that the formula was not
fully incorporated by the nursing team as a measurement
strategy. When individually analyzing the 31 cases of
incorrect positioning, 22 (71%) of them would have been
avoided if the formula had been calculated and used.
N Design Objective Population sample Main results and limitations
1(12) Experimental Compare error rates of NEX* and NEMU† measurements, visualized by x-ray
60 PTRNs‡ NEX*: 55.6% error;NEMU†: 39.3% error.NEMU† has greater reliability than NEX*, however with no statistical significance. 50% of the sample was excluded from the analysis due to the impossibility of data collection
2(13) Descriptive Determine the minimum insertion length of the GT§ in low birth weight NB||, after the analysis of 188 x-rays of GT§
27 NBs|| <1500g Presents a table with minimum insertion measures, according to NB|| weight.
Small sample, only orogastric positioning was evaluated
7(18) Descriptive Compare the anatomical-morphological distances with the inner distance of the esophagus and develop an equation based on height to estimate exterior insertion length of the GT§
498 children (5 NBs||) NEX* and NEMU† measurements were not shown to be good predictors of esophageal distance.The best predictor was height.Height-based and age-differentiated (ARHB¶) equations were developed to estimate GT length.
Negligible number of NB|| in the sample
9(20) Experimental Compare success/accuracy of gastric placement among NEX*, NEMU† and ARHB¶
methods.
173 NBs|| NEX*: 60.6% success; ARHB¶: 78% success; NEMU†: 90.9% success. Recommends that NEX* is no longer used. Introduces a new ARHB¶ equation adjusted to NB||.
ARHB¶ cannot be randomized in 34% of cases
11(22) Descriptive Develop an equation based on the weight of the NB|| to estimate exterior length of insertion of the GT§, after the analysis of 218 x-rays of GT§
87 NBs|| Introduce formulas for nasal and orogastric tubes, suggesting that this new method be used in combination with the current method.
Only one radiologist evaluated the images, and no prospective study was performed for the application of the formula
16(28) Descriptive Describe the correct positioning rate using the weight-based formula as an auxiliary method
107 NBs|| 84% of the tubes were correctly positioned, 12.5% were at the limit and 3.6% were high.Only one radiologist evaluated the images
*(Nose, Earlobe, Xiphoid): distance measured from the tip of the nose to the earlobe to the xiphoid process; †(Nose, Earlobe, Mid-Umbilicus): distance measured from the tip of the nose to the earlobe, a point halfway between the xiphoid process and the umbilicus; ‡pre-term newborns; §gastric tube; ||newborns; ¶(Age Related, Height Based): height-based equation classified by age.
Figure 4 - Studies on gastric tube measurement methods.
Techniques for assessing gastric tube placement
Of the 11 studies classified in this category, 10
were observational studies that investigated alternative
techniques to visualizing radiological imaging, established
as the gold standard to verify GT placement. Such
alternative techniques have the objective of improving
patient safety, achieving a reduction of radioactive
exposure without increasing the risk and complications
related to incorrect tube placement. The studies included
in this category are described in detail in Figure 5.
The techniques investigated to verify GT positioning
in NBs include: gastric secretion aspiration; epigastric
region auscultation; checking aspirated secretion’s pH,
pepsin, trypsin and bilirubin; secretion color; presence
of CO2 test; acid test with litmus paper, reading
diaphragm’s electrical activity; electromagnetic tracing
and the use of indigo carmine at 0.01%.
The diagnostic accuracy tests used in three
studies(15,16,24) included in this review were always
compared to radiological examination. However, one
study(15) evaluated the test accuracy in identifying
correctly positioned tubes, and two other studies(16,24)
evaluated the accuracy in identifying incorrectly
positioned tubes. This prevents the simple comparison
of the values between the three studies.

www.eerp.usp.br/rlae
7Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV.
The study that investigated the accuracy of correctly
positioned tubes found that the use of pH evaluation
along with color evaluation is the safest technique to
confirm correct positioning, considering pH <6.0 and
translucent greenish and brownish colors(15).
For studies that performed accuracy tests for
incorrect positioning of the tube(16,24), the most
important value to be considered is positive predictive
value, since the use of the investigated techniques
occurs at the bedside and represents the proportion
of tests that assertively indicate incorrect positioning
of the tube. The indicator with the highest positive
predictive value (66.7%) was absence of aspirated
secretion. The second most important indicator was
the pH test, which presented positive predictive values
ranging from 20 to 25%.
The accuracy of capnography in identifying incorrect
positioning of the GT cannot be confirmed as there were
no placements in the respiratory tract(16,24), and also
because it is possible to detect the presence of CO2 in
the oral cavity, oropharynx, esophagus and stomach(23).
The evaluation of bilirubin presence was not a
reliable indicator to identify incorrect positioning, since
N Designand population sample Investigated techniques Main results and limitations
3(14) Descriptive; 39 newborns pH, Pepsin, Trypsin, Bilirubin and color of the secretion of 88 tubes correctly positioned in the stomach
pH 4.32(±0.2); Pepsin 60.4(±6.3); Trypsin 6.8 (±1.4); Bilirubin 0.35 (±0.1). Col-or of the secretion: 68.2% off white; 22.7% greenish; 4.5% translucent; 2.3% brown. 2.3% yellowish.pH, trypsin and bilirubin values are similar to those described in the literature for the adult population, while the pepsin value found in newborns is much lower. Small sample
4(15) Descriptive; 56 children, between newborns and up to 14 years of age
pH (<6.0), Pepsin (>20), Trypsin (<50) and secretion color
Sens* Spec† PPV‡ NPV§
pH 77.6% 85.7% 97.4% 35.2%
Pepsin 69.4% 71.4% 94.4% 25%
Trypsin 90% 71% 96% 50%
Color 92.5% 71.4% 94.4% 62.5%
pH+Cor 70% 100% 100% 36.8%
pH 4.1(±3.2); Pepsin 215.4 (±32.0); Trypsin 10.6 (±2.9). The colors that were identified as gastric positioning were: whitish, translucent, greenish and brownish.It was not specified how many newborns participated in the sample. The value of Pepsin was high because it contained many children in the sample of 1 year (42%).
5(16)|| Descriptive; 72 children, between newborns and up to 7 years of age
pH (5.0 limit), Bilirubin (5mg/dl limit) and Capnography, compared to radiological examination
Sens* Spec† PPV‡ NPV§
pH 53.9% 61.8% 25% 85%
Bilirrubin 0% 96.6% 0% 96.6%No tubes were present in the respiratory tract (according to the radiological examination). The CO2 reading was 0mmHg in 71 samples, and it was 2mmHg in only one.The subjects had already used the tube when they were included in the study.
6(17) Descriptive; 60 newborns Acidity test using litmus paper
97% Positive tests, 3% Negative tests. No comparison was made with another method.Litmus paper is limited for pH assessment because it only classifies the secre-tion as acidic or alkaline.
8(19) Descriptive, with case se-ries; 20 children
Catheter with embedded electrodes (EAdi¶) to evaluate the electrical activity of the diaphragm
Gastric insertion of EAdi¶, connected to the Servo-i mechanical ventilation de-vice at its proximal end (Maquet Critical Care, Solna, Sweden) allows reading of the electrical activity of the diaphragm during insertion and positioning of the catheter. The EAdi¶ device allowed for correctly identifying the placement of all tubes, when compared to the radiological examination.Small sample. High catheter cost.
it did not predict tubes positioned in the duodenal
portion(16, 24).
The use of the electromagnetic tracing device and
evaluating electrical activity in the diaphragm showed
good precision and accuracy. The major advantage of
these techniques is the possibility of real-time path
correction during tube passage, as well as avoiding
exposure to radiation, since these procedures are
presented as possible substitutes for abdominal
radiography. However, the sample of pediatric patients
was very reduced, thus making generalizations difficult;
also, both techniques are very expensive(19,21).
Administration of an indigo carmine solution (sky
blue) to check the positioning of the gastric tube is only
useful when it is possible to ensure correct positioning
of an anterior tube. In the study investigating this
method(25), the first passage of GT was always verified
by radiological imaging, and subsequent exchanges were
performed every three weeks. At the time of each change
before the tube was removed, the techniques for verifying
the presence of gastric secretion and pH were used to
confirm the positioning. The anterior tube measurement
was maintained for insertion of the new tube.
(the Figure 5 continue in the next page...)

www.eerp.usp.br/rlae
8 Rev. Latino-Am. Enfermagem 2017;25:e2908.
N Designand population sample Investigated techniques Main results and limitations
10(21) Descriptive; 194 individu-als, between newborns and up to 102 years of age (12 individuals less than 1 year of age)
Electromagnetic device (EMPD**)compared to two radiological examination images
Among the pediatric patients, the EMPD** presented 99.4% agreement with the first radiological examination (simple) and 100% with the second (con-trast). 19 incorrect positions in the respiratory tract were avoided in the total sample with the use of EMPD**, 4 of them in pediatric patients.Small sample of pediatric patients. Specific training is required to read the EMPD** result.
12(23) Experimental; 42 children, between newborns and up to 18 years of age
CO2 detector device 100% accuracy in detecting CO2, however CO2 can be detected outside the airway, for example if the child cries during tube introduction.Sample selected by convenience.
13||(24) Descriptive; 276 children, between newborns and up to 17 years old (173 new-borns)
pH (5.0 limit for fasted chil-dren and 6.0 for fed infants),Bilirubin,Capnography,Gastric secretion color, Gas-tric secretion consistency,Absence of gastric residue
Sens* Espec† VPP‡ VPN§
pH>5,0†† 8.7% 92.2% 20% 81.7%
pH>6,0†† 0% 89.5% 0% 89.5%
Sem resíduo 34.9% 94.8% 66.7% 83.1%
Cor 42.5% 60% 17.5% 83.9%White, green and bronze colors may indicate correct tube placement.Secretion consistency did not prove useful for the positioning assessment.It was not possible to evaluate Bilirubin and CO2, since they did not present variability.
14(25) Descriptive; 44 newborns Sky blue method for gastric tube exchange
Administration of 0.01% indigo carmine solution immediately prior to the ex-change procedure. Positioning is considered correct when it is possible to as-pirate bluish secretion through the new tube. 94.4% showed a blue solution result. No comparison was made with another method.The long-term effects of the use of indigo carmine are not known.
15(26) Descriptive; 54 newborns pH test in situations with and without the use of gastric secretion inhibitors, in fasting and fed newborns
Regardless of the use of gastric secretion inhibitors and whether newborns were fasting or not, pH was <5.5 in 90% of cases where the tube was correctly positioned in the radiological evaluation.Small sample selected by convenience.
17(28) Descriptive; 63 institutions (1,191 children using gas-tric or enteral tube,between newborns and up to 14 years)
Description of the technique used to verify tube place-ment, according to the team’s responses to the question-naire
First choice techniques in the investigated institutions: inspection of the secre-tion (n=21), auscultation of the epigastric region (n=18), measurement of the tube (n=8), pH (n=10), X-rays (n=6). Sample selected by convenience, low reliability of the data collected as they were self-reported by the institutions
*Sensitivity; †Specificity; ‡Positive predictive value; §Negative predictive value; ||Investigated the accuracy to determine incorrect positioning; ¶Electrical Activity of the Diaphragm; **Electromagnetic Placement Device; †† Only refers to NBs included in the sample.
Figure 5 - Studies on techniques for assessing gastric tube placement.
Discussion
The first description found in the literature on NEX and
NEMU methods dating from 1978 was not included in this
review, as it did not clearly present the method described.
In this study, the authors describe using the NEX measure
in clinical practice, however, they suspected that it was not
a long enough measure, as they were not always able to
aspire gastric contents. In order to validate their hypothesis,
the authors followed some necropsies (they do not describe
how many), and observed that with the NEX method, the
distal end of the tube was at the limit of the gastroesophageal
junction, and that it was necessary to add a few centimeters
to the measurement for the distal end of the tube to reach
the body of the stomach. Thus, the authors proposed the
NEMU method and observed that the tube was correctly
positioned in necropsies using this method(29).
After this one, other studies have showed the
inferiority of the NEX measure compared to the
NEMU(12,18,20). Although the latter also represents a
measure that has high variability, the present review
indicates that it is the best evidenced method to date to
be reproduced in clinical practice.
Equations that use height(18,20) and weight(22,27)
to calculate the gastric tube insertion measure seem
to reproduce reliable results; however, the absence
of experimental studies with such methods impedes
them being used as a single reference. Therefore, it
is suggested that these equations are only used as a
supporting measure in the decision on the tube length to
be introduced, at least until studies with new evidence
are available.
For the population of NBs below 1,500g, use of
the minimum length table of the tube to be introduced
can also be indicated as an auxiliary method to avoid
positioning above the gastroesophageal junction(13). It
should be noted that this table should only be used for
the oral route of insertion.

www.eerp.usp.br/rlae
9Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV.
Verifying GT positioning in NBs is a process that
requires nurses’ attention due to the unavailability of
precise techniques such as electromagnetic tracings or
diaphragm electrical activity evaluation, as well as the
impossibility of performing a radiological examination at
each tube exchange due to the costs and risks involved(1,2).
Thus (and the findings of this review confirm), nurses
must use several strategies simultaneously, with the
objective of increasing the safety of the procedure.
The most easily accessible indicator is gastric
secretion return to the tube aspiration, which
presented good results in the accuracy tests of one
of the reviewed studies(24). Recommendations from
international agencies(30-32) also indicate pH (<5.0)
evaluation of aspirated secretion as a technique for
verifying GT positioning. Other studies(15-16) suggest
that combining pH assessment with secretion coloration
(whitish, translucent, greenish or brownish) makes the
assessment even safer, since these are the indicators
with the best results among the accuracy tests.
The use of gastric shields (histamine-2 receptor
antagonists and proton pump inhibitors), as well as
continuous infusion of milk formula and the use of sterile
water to wash the catheter raise questions about the
safety of the aforementioned combined evaluation, since
they could increase gastric pH(2). However, the reviewed
studies comparing gastric pH in NBs and infants did not
find significant differences between those who received
and did not receive these medications, as well as those
who were fed continuous infusion, gavage, or those who
underwent fasting(2,16,24,26).
In the absence of gastric secretion return, the
risk of improper placement increases. In this situation,
nurses may insist on obtaining a sample, performing
movement maneuvers with the newborns and injecting
air (not more than 2ml). Since it is possible that the tube
is in direct contact with the mucosa, these maneuvers
can favor its displacement and attainment of secretion.
If it is still not possible to aspirate secretion through
the catheter after such maneuvers, the possibility of
changing the catheter or performing a radiological
examination can be discussed to visualize the path and
positioning of the distal end(31).
The use of abdominal ultrasonography to verify
GT placement has been shown to be a useful and
effective technique in adults with high sensitivity and
specificity; attaining 98.3 and 100%, respectively, when
compared with the results of conventional radiological
examination(33). Its use in verifying the location of the
end of the GT has been recommended in adult patients
instead of radiological examination since it is a simple
and fast technique, in addition to the advantage of not
exposing the patient to radiation(34-35). A study carried out
in two intensive care units with 14 neonatal and pediatric
patients also demonstrated the efficacy of ultrasound to
evaluate jejunal tube placement in these patients(36).
A pilot study published as a letter(37), which was
not part of this review sample, reports that the use of
ultrasonography to verify GT positioning in NBs is not
a reliable technique, as it was only possible in one
of the 10 cases studied to visualize the distal end of
the tube in the stomach. However, all had the gastric
position confirmed by the pH test (<5.5)(37). Considering
the small sample size of the cited study and data that
contradict promising results in adults, it is necessary to
perform more research with ultrasound in NBs.
Despite care for tube maintenance not being
the subject of this review, it should be pointed out
that monitoring the external length can be used as a
supporting measure in maintenance of tube placement
and patient safety, especially when dealing with long-
term tubes. In the description of an implementation
protocol for tube maintenance in NBs(5) and in an
integrative review(38), the authors recommend that the
external length should be checked and recorded in the
medical record and/or recorded on the tube in a visible
manner, always confirming it before use. However,
it is relevant to consider that keeping the external
length stable does not eliminate the risk of internal
displacement.
In this review, it was identified that the procedure
of introducing air through the tube and auscultating
the epigastric region is the second chosen method of
American nurses to confirm gastric positioning(28), which
is also observed in the clinical practice of the authors
considering their action and teaching fields. However,
literature indicates that it is possible to listen to the air
bubbles in the epigastric region, regardless of whether
the end of the tube is located in the stomach, esophagus
or respiratory tract. Therefore, the use of this technique
is discouraged and should be banned(1,16,29-32,38).
As a contribution to clinical practice, the findings of
this integrative review support, recommending the use
of the NEMU method (with possible confirmation by the
use of formulas based on weight or height) in order to
reduce risks and complications related to the procedure
since it presents a smaller proportion of error, and
the combined performance of positioning verification

www.eerp.usp.br/rlae
10 Rev. Latino-Am. Enfermagem 2017;25:e2908.
techniques prior to each GT use (gastric secretion
aspiration with pH and color assessment).
Another integrative literature review(38) addressing
this subject was found, however, it also included pediatric
patients up to 18 years of age. We also found literature
reviews(1-2) that did not present a detailed description of
the method and included studies. Thus, the difference in
the present integrative literature review was to gather
evidence on the methods for measuring and confirming
GT placement in NBs. Among the 17 studies of this
integrative review, only one well-delineated randomized
controlled clinical trial, two randomized controlled trials
and 14 descriptive studies were found. No systematic
reviews or meta-analyses were found.
Given the specificities of the age group in question
and gaps in the literature, it is considered relevant to
emphasize that there is a need for experimental research
on the methods already described for measuring the
tube and verifying its positioning in order to offer
support and safety to neonatal clinical practice, as well
as for the technological development of devices with
affordable cost.
The results of the present study were limited by the
lack of research that specifically focused on neonates,
as well as by the predominant number of descriptive
studies which made it impossible to synthesize findings
with high levels of evidence to innovate clinical practice.
Conclusion
Regarding methods for measuring gastric tube
for insertion in newborns, implemented morphological
distances present high variability, which compromises
their reliability. The use of the NEX measurement greatly
increases the risk of positioning the tube tip above the
gastroesophageal junction, and should be replaced by
the NEMU measurement. New measurement methods
based on weight and height have been developed, but
clinical trials are still needed to test their efficacy.
Regarding the choice of technique for placement
verification after insertion, no other method is available
as safe as the radiological examination of the chest and
abdomen. The use of electromagnetic tracing seems
promising and deserves further investigation in newborn
subjects. However, it is still expensive and inaccessible
in the Brazilian context.
Evidence indicates that the absence of secretion
return to tube aspiration is a simple and sensitive
method, and therefore it should be seen as a strong
indicator of inadequate positioning. Moreover, pH
evaluation and secretion staining for verification of
gastric placement are the indicators that present the
best results in accuracy tests when compared with
radiological examinations.
Concerning implications for clinical practice, there
is still a lack of evidence to establish safe protocols,
as some current procedures should have already been
abandoned as pointed out in the literature, such as the
use of NEX for measuring the tube and epigastric region
auscultation to confirm its positioning.
References
1. Wallace T, Steward D. Gastric tube use and care in
the NICU. Newborn Infant Nurs Rev. [Internet] 2014
[cited April 1, 2015];14(3):103-8. Available from:
http://www.sciencedirect.com/science/article/pii/
S1527336914000610. doi 10.1053/j.nainr.2014.06.011.
2. Irving SY, Lyman B, Northington L, Bartlett JA,
Kemper C, Grp NPW. Nasogastric tube placement
and verification in children: review of the current
literature. Crit Care Nurse. [Internet] 2014 [cited
April 1, 2015];34(3):67-78. Available from: http://
ccn.aacnjournals.org/content/34/3/67.full.pdf+html.
doi:10.4037/ccn2014606.
3. de Boer JC, Smit BJ, Mainous RO. Nasogastric tube
position and intragastric air collection in a neonatal
intensive care population. Adv Neonatal Care. [Internet]
2009 [cited February 4, 2017];9(6):293-8. Available
from: http://journals.lww.com/advancesinneonatalcare/
pages/articleviewer.aspx?year=2009&issue=120
00&article=00009&type=abstract. doi: 10.1097/
ANC.0b013e3181c1fc2f.
4. Quandt D, Schraner T, Bucher HU, Mieth RA.
Malposition of feeding tubes in neonates: is it an issue? J
J Pediatr Gastroenterol Nutr. [Internet] 2009 [cited April
3, 2015];48(5):608-11. Available from: http://journals.
lww.com/jpgn/pages/articleviewer.aspx?year=2009&iss
ue=05000&article=00015&type=abstract. doi:10.1097/
MPG.0b013e31818c52a8.
5. Farrington M, Lang S, Cullen L, Stewart S. Nasogastric
tube placement verification in pediatric and neonatal
patients. Pediatr Nurs. [Internet] 2009 [cited June
1, 2016];35(1):17-24. Available from: http://go-
galegroup.ez88.periodicos.capes.gov.br/ps/i.do?id=GAL
E|A195322936&v=2.1&u=capes&it=r&p=AONE&sw=w
&asid=88cda8aeb1bd7a420d774272f02c6100.
6. Whittemore R, Knafl K. The integrative review:
updated methodology. J Adv Nurs. [Internet] 2005
[cited April 4, 2015];52(5):546-53. Available from:

www.eerp.usp.br/rlae
11Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV.
http://onlinelibrary.wiley.com/doi/10.1111/j.1365-
2648.2005.03621.x/abstract.
doi:10.1111/j.1365-2648.2005.03621.x.
7. Souza MTd, Silva MDd, Carvalho Rd. Integrative review:
what is it? How to do it? Einstein. (São Paulo) [Inter-
net] 2010 [cited February 4, 2017]; 8(1):102-6. Avail-
able from: http://www.scielo.br/scielo.php?script=sci_
arttext&pid=S1679-45082010000100102&lng=en. doi:
10.1590/S1679-45082010RW1134.
8. Crossetti MdGO. Integrative review of nursing research:
scientific rigor required. Rev. Gaúcha Enferm. [Inter-
net] 2012 [cited February 4, 2017];33( 2 ):8-9. Avail-
able from: http://www.scielo.br/scielo.php?script=sci_
arttext&pid=S1983-14472012000200001&lng=en. doi
10.1590/S1983-14472012000200001.
9. Soares CB, Hoga LAK, Peduzzi M, Sangaleti C, Yoneku-
ra T, Silva D. Integrative review: concepts and meth-
ods used in nursing. Rev Esc Enferm USP. [Internet]
2014 [cited February 4, 2017]; 48(2):335-45. Avail-
able from: http://www.scielo.br/scielo.php?script=sci_
arttext&pid=S0080-62342014000200335&lng=en. doi
10.1590/S0080-6234201400002000020.
10. Moher D, Liberati A, Tetzlaff J, Altman DG. Pre-
ferred reporting items for systematic reviews and meta-
analyses: the PRISMA statement. Int J Surg. [Internet]
2010 [cited February 4, 2001];8(5):336-41. Avail-
able from: https://www.ncbi.nlm.nih.gov/pmc/articles/
PMC2714657/. doi 10.1136/bmj.b2535.
11. Galvão CM. Níveis de evidência. Acta Paul Enferm. [In-
ternet] 2006 [cited April 4, 2015];19(2):5. Available from:
http://www.scielo.br/pdf/ape/v19n2/en_a01v19n2.pdf.
doi:10.1590/S0103-21002006000200001.
12. Weibley TT, Adamson M, Clinkscales N, Curran J,
Bramson R. Gavage tube insertion in the premature infant.
MCN Am J Matern Child Nurs. [Internet] 1987 [cited May
1, 2015];12(1):24-7.Available from: http://ovidsp.ovid.
com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltex
t&D=yrovft&AN=00005721-198701000-00009&PDF=y.
13. Gallaher KJ, Cashwell S, Hall V, Lowe W, Ciszek T.
Orogastric tube insertion length in very low birth weight
infants. J Perinatol. 1993;13(2):128-31.
14. Metheny NA, Eikov R, Rountree V, Lengettie E. Indicators
of feeding-tube placement in neonates. Nutrition Clin Prac-
tice. [Internet] 1999 [cited February 4, 2017];14(6):307-14.
Available from: http://journals.sagepub.com.ez88.periodi-
cos.capes.gov.br/doi/abs/10.1177/088453369901400606.
doi 10.1177/088453369901400606.
15. Westhus N. Methods to test feeding tube placement in
children. MCN Am J Matern Child Nurs. 2004;29(5):282-
7; quiz 90-1. doi: 10.1097/00005721-200409000-
00004
16. Ellett MLC, Croffie JMB, Cohen MD, Perkins SM. Gastric
tube placement in young children. Clin Nurs Res. [Internet]
2005 [cited May 1, 2015];14(3):238-52. Available from:
http://cnr.sagepub.com/content/14/3/238.abstract.
doi:10.1177/1054773805275121.
17. Nyqvist KH, Sorell A, Ewald U. Litmus tests for
verification of feeding tube location in infants: evaluation
of their clinical use. J Clin Nurs. [Internet] 2005 [cited
February 4, 2017];14(4):486-95. Available from:
http://onlinelibrary.wiley.com/doi/10.1111/j.1365-
2702.2004.01074.x/abstract. doi 10.1111/j.1365-
2702.2004.01074.x.
18. Beckstrand J, Ellett MLC, McDaniel A. Predicting
internal distance to the stomach for positioning
nasogastric and orogastric feeding tubes in children. J Adv
Nurs. [Internet] 2007 [cited May 1, 2015];59(3):274-
89. Available from: http://onlinelibrary.wiley.com/
wol1/doi/10.1111/j.1365-2648.2007.04296.x/full.
doi:10.1111/j.1365-2648.2007.04296.x.
19. Green ML, Walsh BK, Wolf GK, Arnold JH.
Electrocardiographic Guidance for the Placement
of Gastric Feeding Tubes: A Pediatric Case Series.
Respiratory Care. [Internet] 2011 [cited February
4, 2017];56(4):467-71. Available from: http://
rc.rcjournal.com/content/56/4/467.short. doi 10.4187/
respcare.00886.
20. Ellett MLC, Cohen MD, Perkins SM, Smith CE, Lane
KA, Austin JK. Predicting the insertion length for gastric
tube placement in neonates. J Obstet Gynecol Neonatal
Nurs. [Internet] 2011 [cited May 1, 2015];40(4):412-
21. Available from: http://www.sciencedirect.com/
science/article/pii/S0884217515305694. doi:10.1111/
j.1552-6909.2011.01255.x.
21. Powers J, Luebbehusen M, Spitzer T, Coddington A,
Beeson T, Brown J, et al. Verification of an electromagnetic
placement device compared with abdominal radiograph to
predict accuracy of feeding tube placement. J Parenter En-
teral Nutr. [Internet] 2011 [cited May 1, 2015];35(4):535-
9. Available from: http://pen.sagepub.com/con-
tent/35/4/535. doi:10.1177/0148607110387436.
22. Freeman D, Saxton V, Holberton J. A weight-based
formula for the estimation of gastric tube insertion
length in newborns. Adv Neonatal Care. [Internet] 2012
[cited May 1, 2015];12(3):179-82. Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NE
WS=N&PAGE=fulltext&D=&AN=00149525-201206000-
00010&PDF=y.

www.eerp.usp.br/rlae
12 Rev. Latino-Am. Enfermagem 2017;25:e2908.
23. Gilbert RT, Burns SM. Increasing the Safety of
Blind Gastric Tube Placement in Pediatric Patients:
The Design and Testing of a Procedure Using a Carbon
Dioxide Detection Device. J Pediatr Nurs. [Internet]
2012 [cited February 4, 2017];27(5):528-32. Available
from: http://www.sciencedirect.com/science/article/pii/
S088259631100580X. doi: 10.1016/j.pedn.2011.08.004.
24. Ellett MLC, Cohen MD, Croffie JMB, Lane KA,
Austin JK, Perkins SM. Comparing bedside methods
of determining placement of gastric tubes in children.
J Spec Pediatr Nurs. [Internet] 2014 [cited May 1,
2015];19(1):68-79. Available from: http://onlinelibrary.
wiley.com/doi/10.1111/jspn.12054/pdf. doi:10.1111/
jspn.12054.
25. Imamura T, Maeda H, Kinoshita H, Shibukawa Y,
Suda K, Fukuda Y, et al. confirmation of gastric tube
bedside placement with the sky blue method. Nutr Clin
Pract. [Internet] 2014 [cited May 1, 2015];29(1):125-30.
Available from: http://ncp.sagepub.com/content/29/1/125.
doi:10.1177/0884533613515932.
26. Meert KL, Caverly M, Kelm LM, Metheny NA.
The pH of Feeding Tube Aspirates From Critically Ill
Infants. Am J Crit Care. [Internet] 2015 [cited June
1, 2016];24(5):e72-7. Available from: http://ajcc.
aacnjournals.org/content/24/5/e72. doi:10.4037/
ajcc2015971.
27. Nguyen S, Fang A, Saxton V, Holberton J. Accuracy
of a Weight-Based Formula for Neonatal Gastric Tube
Insertion Length. Adv Neonatal Care. [Internet] 2016
[cited February 4, 2017];16(2):158-61. Available from:
http://journals.lww.com/advancesinneonatalcare/
pages/articleviewer.aspx?year=2016&issue=040
00&article=00011&type=abstract. doi 10.1097/
ANC.0000000000000261.
28. Lyman B, Kemper C, Northington L, Yaworski JA,
Wilder K, Moore C, et al. Use of Temporary Enteral cited
Devices in Hospitalized Neonatal and Pediatric Patients
in the United States. JPEN J Parenter Enteral Nutr.
[Internet] 2016 [cited February 4, 2017] ;40(4):574-80.
Available from: http://journals.sagepub.com/doi/abs/10
.1177/0148607114567712?url_ver=Z39.88-2003&rfr_
id=ori:rid:crossref.org&rfr_dat=cr_pub=pubmed. doi
10.1177/0148607114567712.
29. Ziemer M, Carroll JS. Infant gavage reconsidered. Am
J Nurs. [Internet] 1978 [cited June 1, 2016];78(9):1543-
4. Available from: http://ovidsp.ovid.com/ovidweb.
cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=ovft&
AN=00000446-197809000-00037&PDF=y.
30. NSW Government Health. Infants and Children
Insertion and Confirmation of Placement of Nasogastric
and Orogastric Tubes [Internet]. Sydney; 2016 [cited
June 1, 2016]. Available from: http://www0.health.nsw.
gov.au/policies/gl/2016/pdf/GL2016_006.pdf.
31. NHS National Patient Safety Agency. Reducing the
harm caused by misplaced naso and orogastric feeding
tubes inbabies under the care of neonatal units. [Internet]
2005 [cited June 1, 2016]. Available from: http://www.
nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetI
D=60018&type=full&servicetype=Attachment.
32. American Association of Critical-Care Nurses
(AACN). AACN practice alert: initial and ongoing
verification of feeding tube placement in adults.
Crit Care Nurse. [Internet] 2016 [cited June 1,
2016];36:e8-e13. Available from: http://www.aacn.
org/wd/practice/content/feeding-tube-practice-alert.
pcms?menu=practice.
33. Chenaitia H, Brun P-M, Querellou E, Leyral J, Bessereau
J, Aime C, et al. Ultrasound to confirm gastric tube
placement in prehospital management. Resuscitation.
[Internet] 2012 [cited June 1, 2016];83(4):447-51.
Available from: http://www.sciencedirect.com/science/
article/pii/S0300957211007404. doi:10.1016/j.
resuscitation.2011.11.035.
34. Vigneau C, Baudel JL, Guidet B, Offenstadt G, Maury
E. Sonography as an alternative to radiography for
nasogastric feeding tube location. Intensive Care Med.
[Internet] 2005 [cited June 1, 2016];31(11):1570-2.
Available from: http://link.springer.com/article/10.1007/
s00134-005-2791-1. doi:10.1007/s00134-005-2791-1.
35. Kim HM, So BH, Jeong WJ, Choi SM, Park KN.
The effectiveness of ultrasonography in verifying
the placement of a nasogastric tube in patients with
low consciousness at an emergency center. Scand
J Trauma Resusc Emerg Med. [Internet] 2012 [cited
June 1, 2016];20:38. Available from: http://sjtrem.
biomedcentral.com/articles/10.1186/1757-7241-20-38.
doi: 10.1186/1757-7241-20-38.
36. Greenberg M, Bejar R, Asser S. Confirmation of
transpyloric feeding tube placement by ultrasonography. J
Pediatr. [Internet] 1993 [cited June 1, 2016];122(3):413-
5. Available from: http://www.sciencedirect.com/
science/article/pii/S0022347605834298.
37. Tamhne S, Tuthill D, Evans A. Should ultrasound
be routinely used to confirm correct positioning
of nasogastric tubes in neonates? Arch Dis Child
Fetal Neonatal Ed. [Internet] 2006 [cited June 1,

www.eerp.usp.br/rlae
13Dias FSB, Emidio SCD, Lopes MHBM, Shimo AKK, Beck ARM, Carmona EV.
Received: Sept. 4th 2016
Accepted: Apr. 6th 2017
Copyright © 2017 Revista Latino-Americana de EnfermagemThis is an Open Access article distributed under the terms of the Creative Commons (CC BY).This license lets others distribute, remix, tweak, and build upon your work, even commercially, as long as they credit you for the original creation. This is the most accommodating of licenses offered. Recommended for maximum dissemination and use of licensed materials.
Corresponding Author:Flávia de Souza Barbosa DiasUniversidade Estadual de Campinas. Faculdade de EnfermagemRua Tessália Vieira de Camargo, 126Cidade Universitária Zeferino VazCEP: 13083-887, Campinas, SP, BrasilE-mail: [email protected]
2016];91(5):F388-F. Available from: http://fn.bmj.com/
content/91/5/F388.2. doi:10.1136/adc.2005.088476.
38. Clifford P, Heimall L, Brittingham L, Finn Davis
K. Following the evidence: enteral tube placement
and verification in neonates and young children. J
Perinat Neonatal Nurs. [Internet] 2015 [cited June 1,
2016];29(2):149-61. Available from: http://journals.
lww.com/jpnnjournal/pages/articleviewer.aspx?year
=2015&issue=04000&article=00013&type=abstract.
doi:10.1097/JPN.0000000000000104.