
Procedures Basic Format Cesarean Section. Objectives Assess the anatomy, physiology, and...
53
Procedures Basic Format Cesarean Section
-
Upload
martin-valentine-doyle -
Category
Documents
-
view
231 -
download
10
Transcript of Procedures Basic Format Cesarean Section. Objectives Assess the anatomy, physiology, and...

Procedures
Basic Format
Cesarean Section

Objectives• Assess the anatomy, physiology, and
pathophysiology of the Cesarean Section.• Analyze the diagnostic and surgical interventions
for a patient undergoing a Cesarean Section.• Plan the intraoperative course for a patient
undergoing Cesarean Section.• Assemble supplies, equipment, and
instrumentation needed for the procedure.

Objectives
• Choose the appropriate patient position• Identify the incision used for the procedure• Analyze the procedural steps for Cesarean
Section.• Describe the care of the specimen• Discuss the postoperative considerations for a
patient undergoing Cesarean Section .

Terms and Definitions
• Obstetrics
• See Indications
• Same as for L & D Terms STST p. 486

Definition/Purpose of Procedure
• Surgical delivery of an infant through the abdominal and uterine wall. Often performed as an emergency for abruptio placentae, placenta previa, or cephalopelvic disproportion. May be scheduled for “previous c-section.”
• Performed when safe vaginal delivery is questionable or immediate delivery is crucial because the well-being of the mother or fetus is threatened

Indicationsa. Abnormal presentations (breech, transverse, etc.)
b. Abruptio Placenta
c. Carcinoma of the Cervix
d. Cephalopelvic Disporportion (CPD)
e. Cervix will not dilate
f. Fetal distress** Most common reason
g. Habitual death of the fetus during the course of labor
h. Placenta Previa
i. Preeclamptic toxemia in pts where difficult labor is anticipated
j. Presence of STDs such as genital herpes
k. Previous cesarean section
l. Prolapse of the umbilical cord

Relevant A & P
• Physiology of pregnancy
• Female anatomy (covered last week)

Blood supply to internal reproductive organs

Blood supply to vagina, ovary, uterus, & fallopian tube

Pelvic Bones

Midsagittal view in supine position with some ligaments

Pathophysiology
• Dependent on type of Indication

Female Pelvis: True Pelvis
Inlet, Cavity (midpelvis), and Outlet
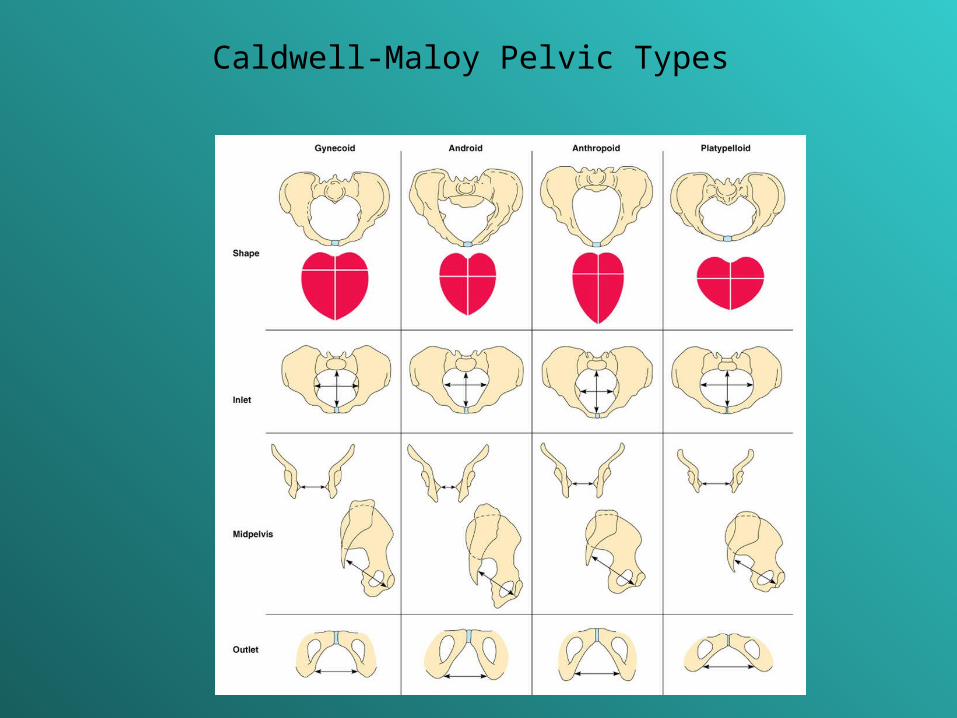
Caldwell-Maloy Pelvic Types


Diagnostics
• Exams
– Multiple methods depending on problem
– Standard Assessments: Client history, determining gestational age (EDB); uterine assessment, fetal development, pelvic adequacy
• Preoperative Testing: typical for any surgery (CBC, blood chemistries, U/A)

External Cephalic Version
Surgical Intervention:Special Considerations
• Patient Factors– Psychological status
– Significant other present or not
• Room Set-up: all preparations are made before the anesthetic is administered. If regional anesthesia is planned, the set-up, counts, and preliminary routines can be performed simultaneously w/anesthesia procedures. If general, the set-up, prep, catheterization, gowning & gloving of all personnel and draping are performed before anesthesia induction. Why?
Surgical Intervention: Anesthesia
• Method: Regional (Epidural preferred or Spinal) or Local or General
• Equipment: spinal or epidural tray
• Other meds: Oxytocin (Pitocin) 10-20 u per liter of IV fluids once infant is delivered to minimize blood loss
– Oxytocin may be used to induce or continue labor, contract the uterus post delivery; stimulate lactation
– Carbopost (Hemabate) parenteral oxytocic used to control uterine hemorrhage following childbirth
– Ergonovine, Methylergononvine (Ergotrate, Methergine) causes uterine muscle contraction


Surgical Intervention: Positioning
• Position during procedure– Supine with roll at Rt hip to displace the uterus
& prevent aortocaval compression• Supplies and equipment: rolled sheet for hip roll,
safety belt• Special considerations: high risk areas: bony
prominences; assistance PRN –awkward and in pain/between contractions

Surgical Intervention: Skin Prep
• Method of hair removal: wet prep or clippers• Anatomic perimeters: Similar to laparotomy—
table side to table side; to xiphoid process extending down to mid thigh: NO Vaginal prep
• Solution options: Betadine or Duraprep or Hibiclens
• Insert foley before prep

Surgical Intervention: Draping/Incision
• Types of drapes: C-Section pack includes laparotomy drape, which may sticky clear plastic around fenestration and fluid-catching channels
• Order of draping: 4 towels, abd drape
• Special considerations
• State/Describe incision
– Skin: Low transverse Pfannenstiel (Most common) or low midline vertical; length depends on estimated size of fetus
– Uterus: type depends on the need for the c-section

Uterine Incisions
Kerr Incision vs Sellheim Incision vs Classical
Surgical Intervention: Supplies
• General: prep set, C-Section pack, basin set, gloves
• Specific– Bulb syringe for infant suction
– Cord clamps, 2 per infant
– Delee suction device
– Cord blood tubes (2)
– Blood gas tubes on standby
– Suture/dressings of choice
– Medications on field (name & purpose)
– Catheters & Drains: Foley catheter is placed preoperatively

Surgical Intervention: Instruments
• General: those for a major GYN laparotomy plus (below) or C-Section tray (facility specific)
• Specific– Delivery forceps (in room), a cord clamp, mucus
aspiration bulb, possible Delee suction trap, Lister bandage scissors, Foerster ring forceps, Pennington forceps, Delee retractor, (2) lab tubes for cord blood

Surgical Intervention: Equipment
• General: ESU, Suction
• Specific:
– Infant radiant warmer mobile unit and possibly additional transport device depending on location of procedure (OR vs L & D)
– Fetal monitor

Procedure Overview
• The pelvis & uterus are entered.
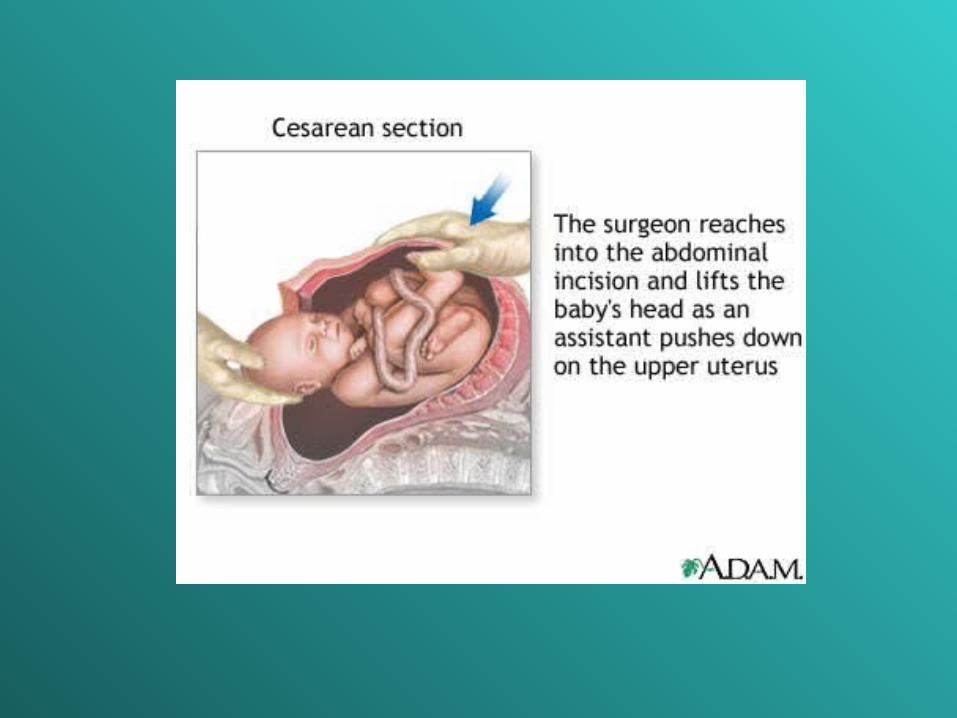
• The head of the infant is delivered & the infant’s airways are cleared
• The infant’s body is delivered
• The placenta is removed
• The uterus is closed.
• The abdomen is closed.

Surgical Intervention: Procedure Steps• Incision is made (#10 blade) and tissues of abdomen are
divided w/usual fashion: have goulet or army-navy ready for muscle separation at midline & fascial incision and dissection
• Peritoneal covering over bladder is palpated (to ensure no inclusion of bladder, bowel, or omentum) and incised (exposing distended uterus). 2 crile hemostats are used to elevate the peritoneum about 2 cm apart.
• Bleeding sites will be clamped but not ligated until later (typically)
• The uterus is quickly palpated to determine fetal placement & position
• STSR: Be ready with dry lap sponges, bulb syringe, and suction

Step 6: Creation of bladder flap at vesicouterine fold

Step 7: Bladder flap retracted & transverse incision made in lower uterine segment


Surgical Intervention: Procedure Steps
• Amniotic fluid is quickly evacuated from field
• Assistant retracts the bladder downward with the bladder blade or other similar retractor
• Surgeon nicks the uterus w/deep knife and extends the incision w/bandage scissors (blunt tips prevent injury to fetus)
• STSR may be asked to remove bladder retractor & simultaneously assistant pushes firmly on upper abd while surgeon grasps infant’s head & rotates upward
• Head is delivered from wound & airways immediately suctioned with bulb (poss Delee)

Step 10: Delivery of infant w/umbilical cord clamped

Surgical Intervention: Procedure Steps
• STSR: Once the head is controlled, all sharp and metal objects are removed prior to elevating the infant’s head
• The umbilical cord is clamped and cut. Cord blood sample is collected (surgeon may milk the cord)
• The infant is passed off to the pediatrician and into the warmed crib for assessment and possible emergency resuscitation measures
• STSR: Protect your sterile field
• The placenta is delivered, inspected, & removed to back table (usually in a basin)

Step 12: Dissection of the placenta from the uterine wall

Surgical Intervention: Procedure Steps
• The uterine interior may be cleaned w/a moist lap sponge. Oxytocin MAY be injected into the uterus to help with hemostasis
• The surgeon closes the uterus in 2 layers with 2-0 or 0 absorbable suture (chromic catgut, Vicryl, or Dexon)—running stitch

Step 14: Uterus is closed in 2 layers
Surgical Intervention: Procedure Steps
• The bladder flap may be approximated or not—if so, a 2-0 or 3-0 absorbable suture w/fine taper needle is often used
• The abdominal cavity is examined for bleeding, sponges, etc and is irrigated.
• Surgeon closes abd wall and skin for low transverse incision; subcuticular stitch or staples are used for closure.
• Blood clots are expressed from the uterus (STSR may be asked for basin at perineum).
• Wound and vaginal area are cleaned
• Dressing & perineal pad applied

Counts
• Initial: Before case begins: sponges, sharps, instruments, bovie tip cleaner
• First closing: Closure of uterus
• Second count: beginning closure of abd cavity
• Final closing
– Sponges
– Sharps & sm items
– Instruments

Dressing, Casting, Immobilizers, Etc.
• Types & sizes– Abdominal dressing and perineal pad
• Type of tape or method of securing– Silk, paper, foam tape. Elastoplast for
compression dressing as ordered.

Specimen & Care
• Identified as: Placenta is sent per surgeon request for evaluation– Cord blood tubes x 2 filled– Blood gasses of cord may be ordered and
drawn by circulator or peds from the artery within the umbilical cord
• Handled: Placenta is usually sent in formalin, if sent

Postoperative Care
• Destination– Allow for bonding time with infant if possible– PACU
• Expected prognosis (Good, Depends on Indication and any anesthetic complications) * mortality is 4-6 times that assoc w/vaginal delivery– Maternal: healing & care of surgical wound
increased risk of future C-sectionInfant: prognosis depends on reason for C-section and extent of oxygen deprivation


Postoperative Care
• Potential complications– Hemorrhage: Fundus must be massaged just
after delivery and become firm to help stop bleeding
– Infection– Other: Injury to surrounding structures
• Surgical wound classification: II
References
• Alexander Ch 14, pp. 513-517
• www.Allrefer.com
• Berry & Kohn Ch 34, pp. 694-697
• Fuller pp. 362-363
• MAVCC Unit 5

Vaginal Delivery
Procedure 15-1
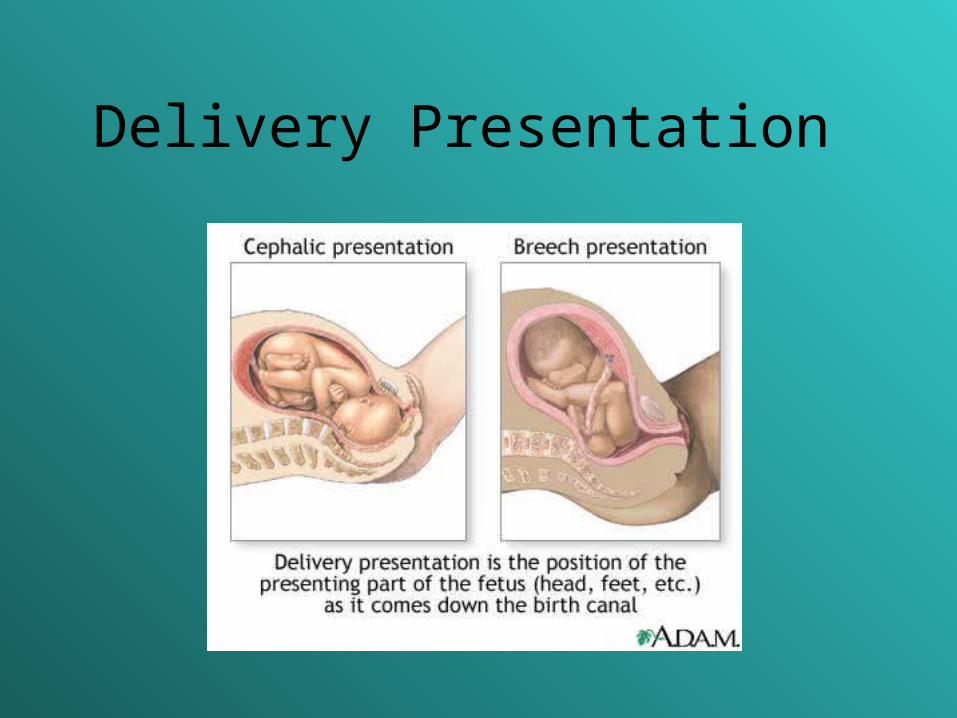
Delivery Presentation

Labor & Delivery Terminology
• Stage one: onset of labor
• Stage two: complete dilatation of cervix
• Stage three: birth of the infant
• Stage four: after placenta is delivered

What is an episiotomy?
Intentional incision at perineum to ease birth process or to protect mother from
uncontrolled perineal lacerations.

Perineal Lacerations & Incisions
• First degree
• Second degree
• Third degree
• Fourth degree

Episiotomies: Midline & Rt Mediolateral


















