Principles of Oncology
164
Principles of Oncology 1
-
Upload
meducationdotnet -
Category
Documents
-
view
480 -
download
0
Transcript of Principles of Oncology

Principles of Oncology
1

2
CELL NUMBER CONTROL
Cell number is the
balance of:
• cell production (due to proliferation via the cell cycle)
and
• cell loss via a number of means including cell death by the process of apoptosis

Figure 23-8 Molecular Biology of the Cell (© Garland Science 2008)
Small number of stem cells Hard to identify Actually slowly turning over
Give rise to other cells which can proliferate extensively (transit amplifying cells) Allows amplification and increase in number of cells Allows for rapid response to changing demands And creation of cells with different phenotypes

4
GROWTH DISORDERS
• Hypertrophy
• Hyperplasia
• Atrophy
• Hypoplasia
• Metaplasia
• Dysplasia
• Neoplasia

5
Perspective
• About 250,000 people every year are diagnosed with cancer in the UK: – about 120,000 die every year
– about 1 in 3 of all deaths.
• The annual cost of diagnosing and treating cancer is about £1.5 billion for the NHS every year.

6
Basic definitions
Rupert Willis 1930s A neoplasm
• is an abnormal mass of tissue, • the growth of which is uncoordinated with that of
normal tissues, • and that persists in the same excessive manner after
the cessation of the stimulus which evoked the change“
An important additional component is • "the presence of genetic alterations that alter cell
growth"

7
Basic definition
An alternative OPERATIONAL definition
of neoplasia is;
"a growth disorder characterised by
genetic alterations that lead to loss of
the normal control mechanisms that
regulate cell growth, morphogenesis and
differentiation"

8
DYSPLASIA
• A spectrum of abnormal growth conditions with many of the morphological and genetic changes of neoplasia BUT without any invasion of spread
• Half way to neoplasia

9
DYSPLASIA IN THE COLON Associated sometimes with the formation of polyps Can be flat Pre malignant Associated with some familial types of colon cancer FAP or Familial Adenomatous Polyposis Also associated with inflammatory bowel disease

10
DYSPLASIA IN THE CERVIX Abnormal maturation of squamous epithelial cells Associated with HPV infection Varying degrees of abnormality . . . . . . . . . ultimately can become invasive and become a frank CARCINOMA

11
The purpose of classification
• is to provide an aid to diagnosis
• to allow the accurate exchange of information
• to define clinical sub-groups who have different biological or clinical features
– will benefit from particular types of treatment – have different outcomes (prognosis) – to facilitate epidemiological analysis

12
Why is classification important?
PRECISE CLASSIFICATION
OF A NEOPLASM FROM A PATIENT
IS ESSENTIAL FOR THE
CORRECT AND APPROPRIATE
PLANNING OF TREATMENT

13
Two key elements of classification of a neoplasm
Behavioural
classification
• based upon the
probable behaviour
of a tumour – E.g. benign or
malignant
Histogenetic
classification
• based upon the
presumed cell of
origin a tumour – E.g. epithelium or
connective tissue

14
Behavioural classification
• Spectrum of behaviour
e.g. benign or malignant
• Essentially a prediction of likely natural history
• Pathologists use a range of morphological features in an attempt to categorise a tumour as benign or malignant

15
Benign Malignant Slow growing Variable and may be rapid
Few mitoses Variable but may be many mitoses
Usually resemble tissue of origin Variable, but may only poorly
resemble tissue of origin
Nuclear morphology is usually normal
Nuclear morphology may be variable and can be very abnormal with
hyperchromasia, pleomorphism and nucleolomegaly
Usually have a well circumscribed or encapsulated
Often poorly defined or irregular
Necrosis is rare Necrosis is common
Ulceration is rare Ulceration is common
Never invade May invade surrounding tissues
Never metastasise May metastasise

16
Histogenetic classification
• Histogenesis refers to the presumed cell of origin of a tumour
• Tumours from a specific histological tissue often
have microscopic features similar too that tissue • The basis of this aspect of classification is
HISTOLOGY.
• Thus – tumours arising in squamous epithelia have a squamous pattern – tumours arising from the glandular epithelium of the gastro-
intestinal tract have a glandular pattern.

17
Two main histogenetic sub groups of malignant tumours
CARCINOMA SARCOMA
Derived from epithelium Derived from connective tissue
Always malignant Always malignant
Common Rare
Spread by lymphatics Spread by blood
May have a pre-malignant phase (or in situ phase)
Not believed to have a pre-malignant phase
Older patients Younger patients

18
PREFIXES
Prefix Tissue of origin
Adeno- Glandular
epithelium
Pappilo- Non-glandular
epithelium
Lipo- Fat
Osteo- Bone
Chondro- Cartilage
Angio- Blood vessel
Rhabdo- Skeletal muscle
Leiomyo- Smooth muscle

19
SUFFIXES
Suffix Meaning
-oma Tumour (benign
or malignant)
-carcinoma Epithelial
malignancy
-sarcoma Connective
tissue malignancy
-aemia
malignancy of bone marrow derived cells (exceptions exist eg. anaemia)

20
Grade • the degree of differentiation of a tumour.
• It is the degree to which a tumour cell resembles its presumed
normal counterpart as assessed by its morphological appearances by a pathologist.
• In general
– a low grade [or well differentiated] tumour has a less aggressive course
– than a high grade [or poorly differentiated] tumour.
• ANAPLASTIC – – This word implies that histological examination shows a very poorly
differentiated neoplasm that does not resemble any normal tissue. – These tumours are always malignant and usually behave very
aggressively.

21
Stage
Stage refers to the extent of spread
of a tumour.
Stage is informed by both
• clinical and radiological assessment (clinical stage)
as well as
• pathological examination of surgical specimens (pathological stage)

22
Classification of epithelial tumours
• Benign tumours of epithelium – Adenoma benign tumour of
glandular epithelium
– Papillomas benign tumour of
non-glandular epithelium
• Malignant tumours of epithelium – These are always carcinomas.
– Qualifying terms needed like • Adeno-carcinoma
• Transitional cell carcinoma

23
Classification of connective tissue tumours
Connective tissue Benign tumour Malignant tumour
Cartilage Chondroma Chondrosarcoma
Bone Osteoma Osteosarcoma
Blood vessel Angioma Angiosarcoma
Skeletal muscle Rhabdomyoma Rhabdomyosarcoma
Smooth muscle Leiomyoma Leiomyosarcoma
Fat Lipoma Liposarcoma

24
THE PROBLEMS OF EXCEPTIONS . . . . . .
• For example – MELANOMA – MESOTHELIOMA – LYMPHOMA
• EPONYMS
– Hodgkin's disease (a kind of lymphoma) – Ewing's sarcoma (a malignant tumour of bone in children and
young people) – Burkitt's lymphoma (a kind of lymphoma)

25
Relevance
• Classification, grade and stage • are important as they enable the
clinician to make some prediction of the likely prognosis of a patient
AND • are essential information for the logical
planning of treatment.

26
A case history
• A 48 year old man presents with a history of blood in his stool.
• He has lost weight (2 stone over 8 months).
• His brother had colon cancer a the age of 35.

27
• On examination middle aged man with evidence of weight loss, pale skin.
• Abdominal examination: ? Irregular liver edge and suggestion of mass in lower abdomen
• Rectal examination: blood on finger but no mass
• Differential diagnosis: – Piles – Inflammatory bowel disease – Diverticular disease – Tumour
• Referred to Consultant Surgeon.
• Sigmoidoscopy shows a mass at 20 cm which is biopsied

28
• Flexible sigmoidoscopy: – mass in colon
– biopsy taken
• Histology of mass – Glandular neoplasm
– Pleomorphism
– Invasion
• Surgery planned – Resection of colon

29

30
Evidence of metastatic spread
Liver deposits

31
Why epidemiology is useful
• It allows you to gauge what is common and what is rare
• It can provide clues to aetiology • Can guide the provision of scarce resources • Can facilitate planning of preventative
measures • It underpins the development of screening
methods for early diagnosis

32
A range of factors can influence the epidemiology of a disease
• Age variation • Gender differences • Historical variation • Geographic variation • Social and economic factors • Occupational factors • Dietary factors • Genetic factors etc . . . . . . . .

33
EPIDEMIOLOGY examples
• Ultraviolet light and skin cancer • Asbestos and mesothelioma • Smoking and lung cancer • HPV, sexual activity and cervix cancer • Malaria and Burkitt’s lymphoma • Meat consumption and colon cancer • Radiation and thyroid cancer • Aniline dyes and bladder cancer • Family history and many cancers • Alcohol and cancer • Hepatitis virus, aflatoxins and liver cancer

34
Colorectal cancer as an example Age Incidence increases rapidly with increasing age
Gender Affects both men and women
Historical variation Is becoming more common
Geographic variation Associated with developed nations rather than developing nations
Social and economic factors
Can occur in all groups
Occupational factors None known
Dietary factors Associated with a low fibre, high fat, high red meat diet
Genetic factors
Familial forms well described including:- 1. Familial Adenomatous Polyposis or FAP (APC gene) 2. Hereditary non polyposis cancer (HNPCC) DNA repair genes BUT ALSO 3. Genes whose products are involved in metabolism of carcinogens can increase the risk of neoplasia

35
MIGRATION STUDIES CAN ILLUMINATE THE ROLE OF ENVIRONMENTAL AND GENETIC FACTORS

36
Mortality statistics the big 5 in men and women
Males Females
Lung Lung
Prostate Breast
Colorectal Colorectal
Stomach Ovary
Oesophagus Pancreas

37
CHANGING PATTERNS OF NEOPLASIA

38
Why tumours cause problems
• grow • press on structures • ulcerate • bleed • cause loss of organ function • invade locally • spread to distant sites (metastasise) • produce substances
– appropriate for the site – inappropriate for the site

39
• It is implicit from our definition of neoplasia that neoplastic (or tumour) cells have lost normal regulation of cell number control
• Tumours are usually clonal in origin
• From this single transformed cell tumours grow
• 1 cm3 of tumour = ~ 1 gram = ~ 109 cells

40
Clonality
• Tumours are usually clonal in origin (that is they arise from neoplastic change in a single initial cell),
• But there are exceptions
• BUT NOTE not all cell populations that are clonal are
tumours!

41
Growth of tumours

42
How tumours present
• A consequence of local disease – (eg. grow, compression, ulcerate, bleed, destroy adjacent
structures)
• A consequence of distant spread – (eg. grow, compression, ulcerate, bleed, destroy adjacent
structures)
• A non-metastatic manifestations of malignancy – (paraneoplastic effects) including anaemia, skin changes,
neurological effects, inappropriate hormone production, weight loss and fatigue.
- CACHEXIA or severe weight loss and debility.
• An incidental finding – (eg. on screening or on routine medical examination)

43
When thinking about a tumour at a given anatomical site, it might be
A primary tumour that can be either
benign or malignant
or be a
a secondary deposit (a metastasis)
from another site

44
Spread of tumours
• Metastasis is the process whereby malignant tumour cells spread from
• their site of origin – (known as the PRIMARY SITE or PRIMARY
TUMOUR) • to some other distant site in the body
– (known as the SECONDARY SITE or SECONDARY TUMOUR or SECONDARY DEPOSIT or METASTASIS or METASTATIC DEPOSIT)

45
INVASION and METASTASIS
• The two properties that accounts for most of the serious (and lethal) consequences of neoplasia.
• Associated with – increased cellular motility, – the production of enzymes with proteolytic
activity and – alterations in cell adhesion

46
ROUTES OF METASTASIS
1. BLOOD [ HAEMATOGENOUS] SPREAD
2. LYMPHATIC SPREAD
3. TRANSCOELOMIC SPREAD
4. PERINEURAL SPREAD
5. IMPLANTATION

47
SPREAD OF TUMOURS

48
The process of metastasis . . . . • Local growth
• Angiogenesis
• Further local growth
• Alteration in cell-cell and cell-matrix
adhesion and altered cell motility
• Remodelling and alteration of extra-cellular matrix
• Leading to invasion and detachment
• Entry into lymphatic and/or blood vessels
• Survival in the lymph and/or blood
• Arrest at some distant site
• Survival at the distant site . . . then repeat the whole sequence
• THE SPREAD OF TUMOURS IS NOT RANDOM
• DEPENDS ON FACTORS
RELATING TO BOTH
• SEED (THE TUMOUR CELLS)
AND
• SOIL (THE SITE OF SPREAD)

49
STAGE
Stage refers to the extent of spread of a tumour. TNM System • T How big the primary tumour is • N Whether nodes are involved • M Whether distant sites are involved
(eg. Liver or bone marrow)

50
WHY IS STAGE SO IMPORTANT?
• Key determinant of prognosis
• Key factor in determining type of treatment options available
– Surgery – Radiotherapy – Chemotherapy

51

52

OVERVIEW OF CARCINOGENESIS

54
The hallmarks of cancer Hanahan & Weinberg
Cell 2000; 100: 57-70

55
Properties of tumour cells
1. Self-sufficiency in growth signals
2. Insensitivity to anti-growth signals
3. Evasion of apoptosis
4. Unrestricted replicative potential
5. Sustained angiogenesis
6. Tissue invasion and metastasis
7. Genetic instability

56
Self-sufficiency in growth signals
• Normal cells depend on exogenous growth factors to stimulate growth and cell proliferation.
• Tumour cells grow and divide without these signals.
• Why? – because of mutations in genes that encode components of
the signalling pathways that normally regulate these processes.
– Such mutations lead to constitutively active signalling

57
Insensitivity to anti-growth signals
• Usually the growth and proliferation of cells is controlled by a balance of growth promoting signals and growth inhibitory (or anti-growth) signals.
• The loss of growth inhibitory signals or the loss of the ability to respond to these signals is typical of
tumour cells.

58
Evasion of apoptosis
• A critical component of normal cell number control is apoptosis (programmed cell death).
• Apoptosis is also a mechanisms for the removal of unwanted cells, for example those with significant damage, including genetic damage.
• Tumour cells have often developed mutations in key genes whose products are involved in apoptosis such that cell death is blocked.

59
Unrestricted replicative potential
• Normal cells can only divide a finite number of times.
• This was first shown by Hayflick in the 1960s – normal human fibroblasts will divide about 70 times if taken
from a neonate, – but 40 times from a middle aged person, – and barely divide at all from an elderly person.
• Normal cells thus have a restricted replicative potential as a
consequence of a number of mechanisms.
• Tumour cells have an unrestricted replicative potential and just carry on dividing!
• The role of telomerase

60

61
Sustained angiogenesis
• Tumours will stop growing when they outgrow their blood supply - without this they will have insufficient nutrients and oxygen to sustain themselves – and undergo ischaemia and infarction.
• Tumours overcome this problem by the production of various factors that stimulate the formation of new blood vessels.

62
Tissue invasion & metastasis
• Normal cells remain where they are supposed to be and normal tissue boundaries are maintained.
• Tumours are characterised by invasion into nearby tissues and structures (ie. normal boundaries are not maintained) and may spread to distant sites (metastasis).
• These properties are the main reason why tumours
are such a significant clinical problem.

63
Genetic instability
• Normal cells maintain the integrity of their genomes
• Mutation is a key feature of neoplasia • Genetic instability is common in neoplasms.
• A characteristic feature of tumours, particularly
aggressive tumours, is the unstable nature of their genomes. – They often develop aneuploidy (abnormal DNA content) with
abnormal chromosomes and mutation is also common – Hyperchromasia (densely staining) – Pleomorphism (variable size & shape)

64
Evidence that neoplasia is a genetic disease
1 Nuclear abnormalities are common in tumours – Hyperchromasia
– pleomorphism
2 Often see abnormal mitoses
3 Abnormal DNA content is common in tumours
4 Chromosomal abnormalities are common in tumours – Some are specific to particular
tumour types
– Some are non-specific

65
5 Nearly all carcinogens are mutagens
6 Specific mutations in growth control genes are common in tumours
7 Genetic instability is a characteristic feature of tumours
8 Tumour cells breed true
Evidence that neoplasia is a genetic disease
M FISH – GMP lecture 10

66
9 SOME CANCERS RUN IN FAMILIES There are a number of familial forms of neoplasia. That is genetic abnormalities in genes that predispose to neoplasia that can be inherited. Provide insights into the molecular events in neoplasia
Evidence that neoplasia is a genetic disease

67
TUMOUR PROGRESSION
• Clinical and experimental phenomenon • With time tumours grow and successive
populations become increasingly abnormal, accumulating more genetic abnormalities (mutations)
• Associated with increasingly abnormal appearance and behaviour
• Increasingly insensitive to growth inhibitory signals, more resistant to apoptosis, increasingly unstable etc.

68
Tumours: Multiple genetic events are needed Evidence: clinical examples eg. colorectal cancer

69
Tumours: Multiple genetic events are needed Evidence: clinical examples eg. tumour progression

70
Tumours: Multiple genetic events are needed Evidence: Experimental skin tumours in mice

71
Molecular events in neoplasia
Exactly what genes are involved in neoplasia? several hundred genes mutated in tumours have been identified usually encode proteins involved in the kinds of process as being typical
of tumours.
• Self-sufficiency in growth signals • Insensitivity to anti-growth signals • Evasion of apoptosis • Unrestricted replicative potential • Sustained angiogenesis • Tissue invasion and metastasis
We can call such genes 'CANCER CRITICAL GENES' : meaning all genes whose mutation contributes to the causation and
progression of cancer.

72

73
Cancer critical genes
There are two broad
categories of cancer
critical gene
• Oncogenes
• Tumour suppressor genes
ONCOGENES
+
Cell number [or other key cellular control]
-
TUMOUR SUPPRESSOR
GENES

74
Cancer critical genes
Cancer critical genes
generally are involved
in cell cycle or cell
death processes
[Some are involved in
DNA repair]
ONCOGENES
Stimulate cell division OR inhibit cell death
+
Cell number [or other Key cellular control]
-
Inhibit cell division or stimulate cell death
TUMOUR SUPPRESSOR GENES

75
Oncogenes
Involved in cancer by an increased activity of the (proto)oncogene stimulating an increase in cell number
Genetically dominant Function like an accelerator The gain of function of an oncogene product as a consequence • of more of the gene product being expressed, • or a mutation in the gene such that the resultant protein has increased
function, • or expression occurring in the wrong cell type, • or at the wrong time
leads to the stimulation of a critical cell process (such as the cell cycle). Examples include is the ras oncogene, myc oncogene, bcr-abl oncogene

76
Tumour suppressor genes
Involved in cancer by a decreased activity of the tumour suppressor gene leading to an increase in cell number Genetically recessive Functions like a brake The loss of function of a tumour suppressor gene product as a consequence • of less of the gene product being expressed, • or a mutation in the gene such that the resultant protein has reduced
or loss of function, • It is a genetically recessive event and requires the loss of both copies
of the tumour suppressor gene (as first proposed by Knudson in his 'two hit hypothesis').
• Examples include the p53 gene, the APC gene and the Rb gene

77
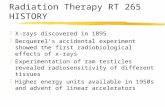
Understanding cancer critical genes: an analogy
One Accelerator Two brakes
A foot on the accelerator can make you go faster! Oncogenes encode potential accelerators of growth. A single event is enough - it is genetically dominant – and involves GAIN OF FUNCTION
You have two brakes If one stops working you can use the other. If both stop working you cannot stop and will accelerate. Tumour suppressor genes usually encode the brakes on cell growth – loss of their function can lead to accelerated growth - but it requires 2 events - loss of both brakes. You need LOSS OF FUNCTION of both alleles of a tumour suppressor gene (genetically recessive)!

Figure 15-1 Molecular Biology of the Cell (© Garland Science 2008)
Oncogene Pathways

79
Activating oncogenes
1 2 3

80
erbB2 in breast and
ovarian cancer
(Neoplasia 6)
1. GENE AMPLIFICATION
Positive growth
signal
Receptor amplification
HSR=homogeneously staining region

81
2. POINT MUTATIONS IN CODING SEQUENCE
Positive growth
signal
Receptor mutation
Mutations in oncogenes are termed ‘gain of function or activating mutations’
inappropriate expression of the
pathway eg. ras signalling

Many signalling proteins are molecular switches

Mutant ras is always switched on

84
Altered regulation: myc gene over-expressed in lymphoma
New gene formed: bcr-abl with altered/new properties
3. CHROMOSOMAL REARRANGEMENTS

85
Tumour suppressor genes The Knudson Hypothesis
Knudson studies children with an eye tumour called retinoblastoma
2 groups of patients:- • those with a family
history • and those without (the
majority)
Familial form • present earlier in
childhood • often had bilateral
disease • within an eye could be
multi-focal.
Sporadic • presented later • only had a single eye
involved.

86
Tumour suppressor genes The Knudson Hypothesis
For a tumour to develop Knudson proposed that:- • a gene was involved
• mutations were needed in this gene (called the retinoblastoma
gene)
• normal people have two copies of this gene
• one inherited from the father and one from the mother
• Needed to have loss of function mutations in BOTH maternal and paternal copies of the retinoblastoma gene

87
Knudson’s Two-Hit Hypothesis
Hereditary Sporadic
Multiple tumours, Single tumours, bilateral, early onset. unilateral, late onset

88
Tumour suppressor genes The Knudson Hypothesis
Sporadic form • a mutation has to occur in both
copies of the retinoblastoma gene. • If a single mutation could occur in
one in a 106 cells in a given period of time then the probability of a mutation occurring in both copies would be one in 1012.
• ie. very rare.
• the longer the period of time that elapses the more likely this is, but it is unlikely to occur more than in one cells. hence tumours occur late and are unilateral.
Familial form • the child inherits from one mutant
copy of the retinoblastoma gene.
• Since it still requires mutations in both copies for a tumour to develop then the probability of this is one in a 106.
• This is a million times more likely than in the sporadic form.
• the disease occurs earlier and also there is a high probability of it occurring in more than one cell, and thus tumours may be multi-focal and bilateral.

89
Familial
Sporadic
1 in 106
1 in 106 1 in 106
Overall
1 in 106
Overall
1 in 1012

PEDIGREE OF THE FAMILIAL FORM OF RETINOBLASTOMA
• Disease status of 24 children & grandchildren descended from a single male with retinoblastoma in childhood
• ~ 50% of his descendants developed disease (red)
• Proband did not develop disease but passed the susceptibility to 2 of his children
• Proband is one of the small fraction (10%) with incomplete penetrance
90

91

92
Ways of inactivating a TSG
92

93
p53 TSG
• Altered in more than 50% of human cancers
• Involved in a pathway that responds to DNA damage and allows repair or apoptotic cell death: – if it is not working damage accumulates and
tumours can arise.
• Is a transcription factor: regulates other genes

94

PREVALENCE
OF P53
MUTATIONS
IN HUMAN
CANCERS
95

PEDIGREE OF A FAMILY WITH LI-FRAUMENI
SYNDROME
96

The component cancers of Li-Fraumeni syndrome tend to show up at different stages of life:
Age of Onset
1. Infancy
2. Under 5 years of age
3. Childhood and young adulthood
4. Adolescence
5. Twenties to thirties
Type of Cancer
1. Development of adrenocortical carcinoma
2. Development of soft-tissue sarcomas
3. Acute leukaemias and brain tumors
4. Osteosarcomas 5. Premenopausal breast
cancer is common
Those who survive the first cancer are at higher risk for a second cancer. These
second cancers often occur in areas of the body previously treated with radiation. 97

Tumours: Multiple genetic events are needed Evidence: clinical examples eg. colorectal cancer
98

NORMAL
COLON
INNER SURFACE OF THE COLON OF A
PATIENT WITH FAMILIAL ADENOMATOUS
POLYPOSIS
99

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
CHRPE rare CHRPE frequent
EXON
AAPC LESS PROFUSE
POLYPOSIS PROFUSE POLYOSIS
EARLY ONSET
THE APC GENE- genotype/phenotype correlations
MUTATION CLUSTER
REGION
FAP
GARDNER’S SYNDROME
AAPC
MULTIPLE ADENOMAS
AS FOR FAP
VARIABLE NOS OF ADENOMAS
DUODENAL POLYPOSIS,
GASTRIC ADENOMAS, CHRPE
AS FOR FAP + EPIDERMOID CYSTS, DESMOID TUMOURS
GASTRIC POLYPS OF FUNDAL GLANDS
100

FOUR GENERATION FAMILY PEDIGREE WITH AN INHERITED PREDISPOSITION
TO BREAST & OVARIAN CANCER 101

BRCA1 Tumour Suppressor Gene
Isolated by positional cloning as one of the genes predisposing to early onset breast and ovarian cancer
Germline mutations of BRCA1 found in 50% inherited breast cancers 81% inherited breast-ovarian cancer)
Penetrance varies based on age and population 56-85% by age 70 for inherited breast cancer 16-60% by age 70 for inherited ovarian cancer
Sporadic disease - BRCA1 mutations detected in 10% of sporadic ovarian cancer - Reduced protein expression observed in the majority of sporadic breast cancers
102

22
(1) Regulation of transcription (2) DNA damage (3) Cell cycle
BRCA1 Function
103

XERODERMA PIGMENTOSUM
2 mutant copies of the same gene inherited – one from each parent
Very rare condition
Susceptibility to skin cancer
Inherited defect in DNA repair (excision repair)
Skin cancer rates 2000-fold > normal
Average age 8yrs cf 60yrs general population
20-fold > brain, lung, stomach, breast & leukaemias
Also a cancer critical gene!! 104

XERODERMA PIGMENTOSUM PEDIGREE
Both parents are ‘carriers’ with no disease symptoms
Child has 50% chance of inheriting mutant allele from each parent
Overall probability of developing XP is 50%x50%=25%
1st generation 2/8 children developed the disease
All of their children inherit a mutant allele so are carriers
Some in the 1st generation may be carriers but not evident from the pedigree
105

FOUR GENERATION FAMILY PEDIGREE WITH AN INHERITED PREDISPOSITION
TO BREAST & OVARIAN CANCER 106

30 50 70
AGE (YEARS)
PR
OB
AB
ILIT
Y O
F B
RE
AS
T O
R O
VA
RIA
N C
AN
CE
R (
%)
50
100
With BRCA1
mutation
With family
history
Without BRCA1
mutation
WHY BOTHER TO TEST FOR BRCA1 MUTATIONS?
107

RISKS/BENEFITS OF CANCER GENETIC TESTING
• Ambiguous results
• Results cause anxiety
• Lack of prevention strategies
• Discrimination
• Strain on family relationships
• Ends uncertainty
• Possible absence of mutation
• Improved medical care
• Clarifies risk for relatives
• Informed reproductive choices
RISKS BENEFITS
108

ETHICAL ISSUES
• Patient confidentiality - insurance - employment • Commercialism – Myriad Genetics
• Prenatal testing
Harris, Winship & Spriggs Lancet Oncology 2005; 6:
301-10 ‘Controversies and ethical issues in cancer-genetics clinics’.
To be continued PoDT year 2 – clinical genetics 109

A MULTIFACTORIAL DISEASE
• Having these mutant genes inherited from a parent is not enough: need other mutations
• Also the other genes in the genome contribute to overall risk – The deck of cards!
• Modifying loci
– Penetrance – The exact mutation
110

The causes of neoplasia
Carcinogenesis is the process by which a normal cell is converted into a neoplastic cell A carcinogen is an agent that can cause neoplasia • Most neoplasms occur as a consequence of environmental factors
• Epidemiological and experimental studies provide insight into
carcinogens
• It is rare for a carcinogen to act by itself - it usually requires co-factors
• Genetic variability in the population and other host factors contributes to carcinogenesis
• Carcinogens are almost invariably mutagens

The causes of neoplasia
• Toxins such as smoking
• Ionising radiation
• Non-ionising radiation
• Viruses
• Bacteria
• Fungi
• Parasites
• Hormones
• Diet
• Inherited genes
There is a complex interplay between environmental factors and host factors, including genetics susceptibility

How do we find carcinogens?
• Epidemiology – Geographical risk
– Historical changes
– Occupational risk
– Behavioural risk
• Experimental evidence – Cell culture
– Animal models

Genetic damage is the key to neoplasia
Chemical carcinogenesis
• History – Percival Pott 1776
• Identified skin cancer in chimney sweeps as being due to soot
– Aniline dyes and bladder cancer

Genetic damage is the key to neoplasia
Chemical carcinogenesis
• Diverse compounds – Direct acting
– Indirect acting: require metabolic activation
• Examples – Alkylating agents (direct)
– Polycyclin hyrdocarbons (indirect)

Genetic damage is the key to neoplasia
Chemical Carcinogenesis – Ames test
• Use bacteria that can only grow on particular media
– Treat with compound: do they mutate to grow on other media?
– Pre treat compound with metabolic enzymes (liver microsaomes) and repeat
– Animal studies • As good as it gets! . . . . but possibly not always
relevant to man

Figure 2.24 The Biology of Cancer (© Garland Science 2007)
THE AMES TEST

Genetic damage is the key to neoplasia
Chemical carcinogenesis – Human studies – Epidemiology
– Complex and difficult but lots of good
evidence for environmental chemical carcinogens • Asbestos • Aflatoxins • Aniline dyes

Genetic damage is the key to neoplasia
Chemical carcinogenesis – Smoking
– Huge number of chemicals involved
– Clear evidence for carcinogenic role of smoking
– “If everyone smoked then lung cancer would be a genetic disease”
– Emphasises the point that we are all genetically different
• Xenobiotic metabolism
• DNA repair
• Other

Genetic damage is the key to neoplasia
Radiation carcinogenesis
• Ionising radiation
• Hiroshima, Nagasaki, Chernobyl, Laboratory accidents
• Environmental radiation – Aberdeen, Cornwall,
– radon exposure
• Therapeutic & diagnostic radiation

Genetic damage is the key to neoplasia
Radiation carcinogenesis
• Non-ionising radiation
• UV causes skin cancer – Low risk in Negroes, high risk in Caucasians,
high risk in albinos
– Families with defective DNA repair (Xeroderma pigmentosa)

Genetic damage is the key to neoplasia SOME EXCEPTIONS
• Hormones – Act as promoters, stimulating cell proliferation
– Breast, endometrial and ovarian cancer are hormone dependent (used in treatment)
• Bacteria, fungi and parasites – Gastritis caused by Helicobacter pylori
– Aflatoxins (carcinogen) produced by Aspergillus flavus and liver cancer
– Bladder inflammation caused by Schistosomes (Eygpt) - bladder cancer

Genetic damage is the key to neoplasia
Viruses and cancer
• Good evidence in experimental models
• Good evidence that viruses cause human cancer – HPV and cervical cancer
– HBV and liver cancer
– EBV and lymphoma
• Viral genes functioning in human cells

Viral carcinogenesis I
• Viral genes can act as dominant transforming oncogenes like ras
• Viral genes can encode proteins that can inactivate cellular proteins – HPV encodes 2 proteins called E6 and E7
that bind to and inactivate p53 and Rb thus effectively inactivating these tumour suppressor proteins (genes)

125
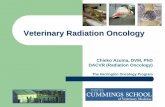
Human papillomavirus and the pathogenesis of cervical carcinomas
This histological section of a human papillomavirus (HPV)-infected cervical epithelium reveals, through immunostaining with an anti-HPV antibody stain (brown), clusters of HPV-infected cells in dysplastic areas of the epithelium, termed high-grade squamous intraepithelial lesions (HSILs). The dysplastic cells arise, in large part, from the ability of the HPV E7 oncoprotein to inactivate pRb and thus block entrance into a postmitotic state, and to suppress apoptosis, the latter being achieved through the actions of the viral E6 oncoprotein, which targets the host cell’s p53 protein for destruction. The resulting lesions progress with a low but significant frequency to cervical carcinomas.

Viral carcinogenesis II
• Viruses can also integrate into the genome of a cells and do one of two things
Activate the expression of a cellular gene (proto-oncogene)
OR Inactivate a gene by disrupting it
(inactivate a TSG)

Viral carcinogenesis III
• Viruses can also function in neoplasia by stimulating proliferation (HBV in liver; EBV in lymphocytes) and thus acting as a promoter
• Also some viruses can cause immunosuppression (EBV and HIV) and this may be associated with development of tumours

Genetic damage is the key to neoplasia
Host factors – Race,
– diet,
– gender,
– inherited factors, etc
• Familial cancers

Hereditary cancer • Some tumours run in families • We know the genes involved in some
cases – Familial polyposis coli
• (APC)
– Hereditary non polyposis colon cancer • (DNA repair enzymes)
– Breast cancer (+/- ovarian cancer) • BRCA1 and BRCA2
– Li Fraumeni syndrome • p53

Hereditary cancer
• Having these mutant genes inherited from a parent is not enough: need other mutations
• Also the other genes in the genome contribute to overall risk – The deck of cards!
• Modifying loci
– Penetrance – The exact mutation

Genetic damage is the key to neoplasia
• Abnormalities of DNA repair genes are common in cancer
• Can be inherited or be acquired – Mismatch repair
– Double strand repair
– Nueclotide excsion repair

Genetic damage is the key to neoplasia
• Familial cancers are relatively rare
• Genes involved in familial forms of cancer are (usually) also involved in the sporadic forms of cancer


Overview of treatment options
Accurate clinical diagnosis of patients with neoplastic disease requires a logical and careful application of
history taking clinical examination and appropriate special tests & investigations.
Ultimately the diagnosis of neoplasia requires histopathological assessment or a tissue diagnosis. This involves
cytology (eg. fine needle aspiration) needle or core biopsy incision biopsy or excision biopsy

Multi-disciplinary team approach
The diagnosis and treatment of cancer is increasingly complex Requires a multi-disciplinary team (MDT) of professionals including
– Surgical oncologists – Radiation oncologists – Medical oncologists – Pathologists – Radiologists – Geneticist – General practitioners – Palliative care specialists – Psychologists – Social workers – Nurses – Chaplains etc . . . . . . . . . .

New information helps diagnosis
• Molecular profiles
• Expression arrays
• Antibodies
• More robust and reproducible diagnoses and classification
• Identification of subgroups that need specific therapies
• Tailored treatments

Identifying prognostic factors
Things that predict survival
• Tumour type
• Stage and Grade
• Karnovsky status
• Tumour factors – Gene expression
– Proliferation

Identifying predictive factors
Things that predict response to therapy
• Sub types of tumour
• Expression of various genes
• Expression of p53
• Expression of other genes

Survival curves (Kaplan-Meier) TUMOUR TYPE
Mesothelioma Seminoma
Time
100%
1 yr 10 yr

Survival curves (Kaplan-Meier)
STAGE

Survival curves (Kaplan-Meier)
GENE EXPRESSION

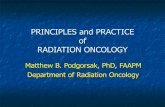
Figure 16.4a The Biology of Cancer (© Garland Science 2007)
Analysis of expression levels of 70 ‘prognosis genes’ in 295 primary breast cancers Stratification into 2 groups based on common patterns of expression
Kaplan-Meier plot following survival of 151 patients over 10 years shows they have a dramatically different clinical course
GENE EXPRESSION ARRAYS

Treatment goals
The goals of patient management:
• Cure
• Palliation – with the aim of improving lifespan and
quality of life

Treatment principles I
Are based upon: • Biological behaviour of the tumour
• Extent and bulk of disease
• Mortality and morbidity of any therapies
• The efficacy of the therapies
• The general well being of the patient including co-
existent (co-morbid) diseases

• Screening – Early Diagnosis is preferable (eg. Breast cancer)
– Diagnosis at a pre-malignant stage (eg. Cervical cytology)
• Prevention – Behaviour modification (eg. smoking, sun exposure)
– Risk avoidance (eg. occupational risks, dietary factors)
Treatment principles II

Cancer cure: difficult but not hopeless!
• SURGERY is very effective
• For some tumours chemotherapy and radiotherapy are very effective
• Over the last decade all sorts of new approaches and new drugs coming into the clinic.
• Lots of hope for the future . . . . . . .

How do current therapies work?
• Exploit properties of tumour cells – Proliferation & loss of cell cycle control
– Genetic instability
• Most drugs and radiation cause massive DNA damage and induce cell cycle arrest and cell death

Figure 16.7 The Biology of Cancer (© Garland Science 2007)
low doses of doxorubicin on hepatoma cells induce ‘mitotic catastrophe’ in tumour cells because they often lack G2/M checkpoint controls and so continue into mitosis without repairing the chromosomal damage. Normal cells with intact checkpoints arrest mitosis until damage is repaired.
Increasing aneuploidy, polyploidy and cell death with time

Figure 9.8 The Biology of Cancer (© Garland Science 2007)
THE CENTRAL ROLE OF P53
Various cellular stresses can upregulate p53 with a variety of downstream effects
IHC of an ovarian carcinoma stained for p53 protein.
Intense staining is that of mutant p53.

Cancers can evolve resistance to treatment
• Just like bacteria and antibiotics! • Mutation and natural selection for resistant
clones • If the apoptotic pathway is not working then
drugs will not work. – Therefore, Increased resistance when there is
mutant p53
• Increased expression of MDR1 in tumours: an efflux pump that exports exogenous compounds out of cells

Monitoring treatment I
• Clinical examination
• Radiology
• Tumour markers – Measure something produced by the tumour
cells as an index of tumour burden • AFP (alpha feto protein in liver cancer)
• AFP & HCG (human chorionic ganadotrophin in testicular cancer)

Monitoring treatment II

Monitoring treatment IIIa
Time
Clinical examination
Occult disease

Monitoring treatment IIIb
Time
Radiological examination
Occult disease

Monitoring treatment IIIc
Time
Biochemical examination Level of marker
Occult disease

Monitoring treatment IIIc
Time
Molecular marker MINIMAL RESIDUAL DISEASE

New treatments are based on new understanding of cancer biology: p53
• Drugs that reactivate mutant p53: restoring sensitivity to current drugs.
• Viruses that will only grow in cells with mutant p53 as biological therapy
• Side effects of current therapy include cell death in bone marrow due to p53 function in normal cells: use drugs that inactivate p53 in normal cells to reduce side effects of current therapies and increase therapeutic ratio

What about blocking blood vessels?
• Angiogenesis is key to tumour growth so is an obvious target
• Angiogenesis is induced by various factors such as VEGF: this acts on a receptor VEGF-R to induce new blood vessels to grow. Design drugs that block the receptor so that the tumour derived VEGF does not work?

Small molecules can be designed to target specific oncogenic proteins
• The example of HERCEPTIN – An antibody that blocks the erbB2
receptor (also called HER2) now used in breast cancer
• The example of GLEEVEC – A small molecule that blocks the active site
of the abnormal bcr-abl protein, now used in CML (chronic myeloid leukaemia)

INTRACELLULAR SIGNALLING VIA THE ERBB2 RECEPTOR
LIGAND
RECEPTOR mRNA
NUCLEUS
INTRACELLULAR
TRANSDUCER
ERBB2 RECEPTOR
INTRACELLULAR SIGNALLING VIA THE ERBB2 RECEPTOR
LIGAND

AMPLIFICATION OF THE ERBB2 PROTO-ONCOGENE
LIGAND
INTRACELLULAR TRANSDUCER
NUCLEUS
ERB B2
RECEPTOR

THERAPY VIA RECEPTOR BLOCKING BY ANTIBODY
LIGAND
INTRACELLULAR TRANSDUCER
NUCLEUS
RECEPTOR
ANTIBODY
Herceptin


Understanding cancer biology leads to rationale tailored treatments
• Next generation of treatments will be based on our new understanding
PLUS • Specific treatments for specific
patients based on genetic and molecular knowledge . . . . . .
Grounds for optimism