Principles of management and prevention of Odontogenic ...
85
Principles of management of Odontogenic Infections Dr Milad Parvin Oral and Maxillofacial Surgeon Assistant professor Boushehr University of Medical Sciences
Transcript of Principles of management and prevention of Odontogenic ...
Principles of managementof Odontogenic Infections
Dr Milad Parvin
Oral and Maxillofacial Surgeon
Assistant professor
Boushehr University of Medical Sciences
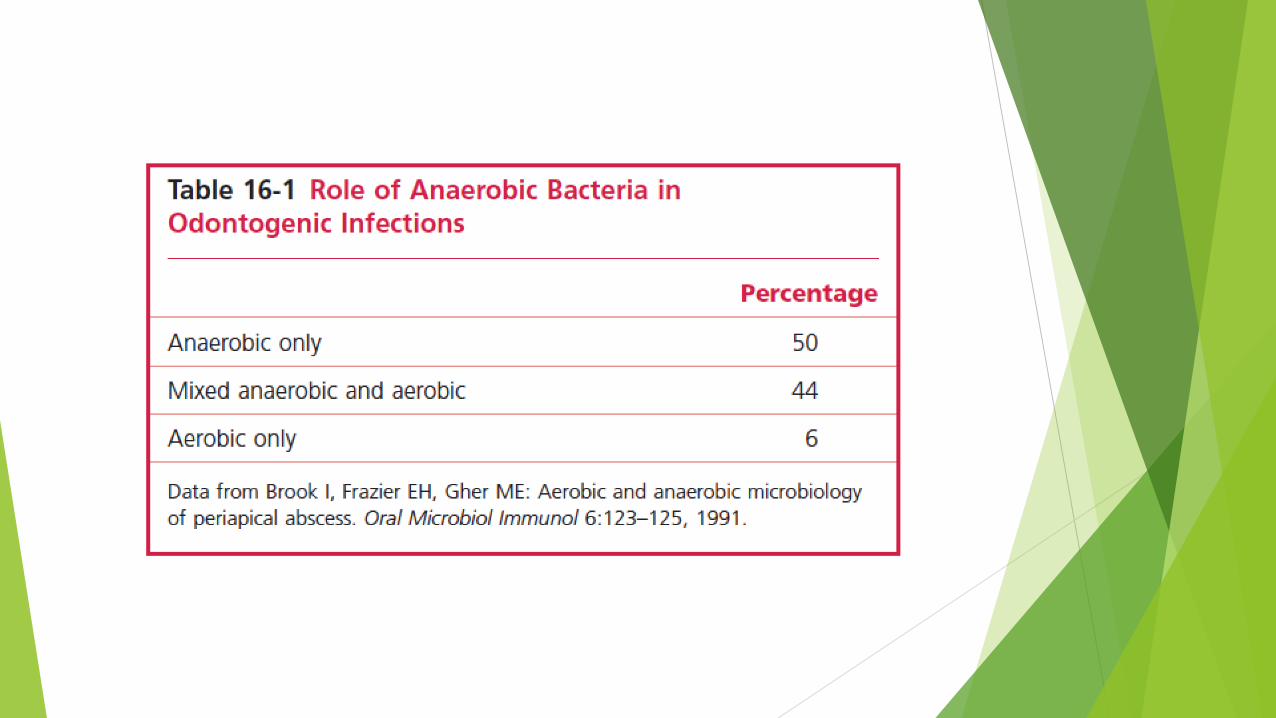
Microbiology of Odontogenic infections
• Bacteria that cause odontogenic infections are part of normal flora
• Aerobic gram positive cocci
• Anaerobic gram positive cocci
• Anaerobic gram negative rods
• They cause dental caries, gingivitis and periodentitis
• Almost all of of Odontogenic infections are caused by multiple bacteria
How an Aerobic bacteria cause OIs
• 1-intial inoculation in deeper tissues
• 2-synthesis of hyaluronidase by s.milleri group
• 3-allowing other organisms to initiate cellulitis stage
How an Aerobic bacteria cause OIs
•Streptococci create a favorable environment for anaerobs by:
1-release essential nutrients
2-lowering PH
3-consumption of O2
• Than anaerobic bacteria become predominant and cause liquefaction necrosis by collagenase
liquefaction necrosis become:
Microabcess
Than clinically recognizable abscess
anaerobes become predominate
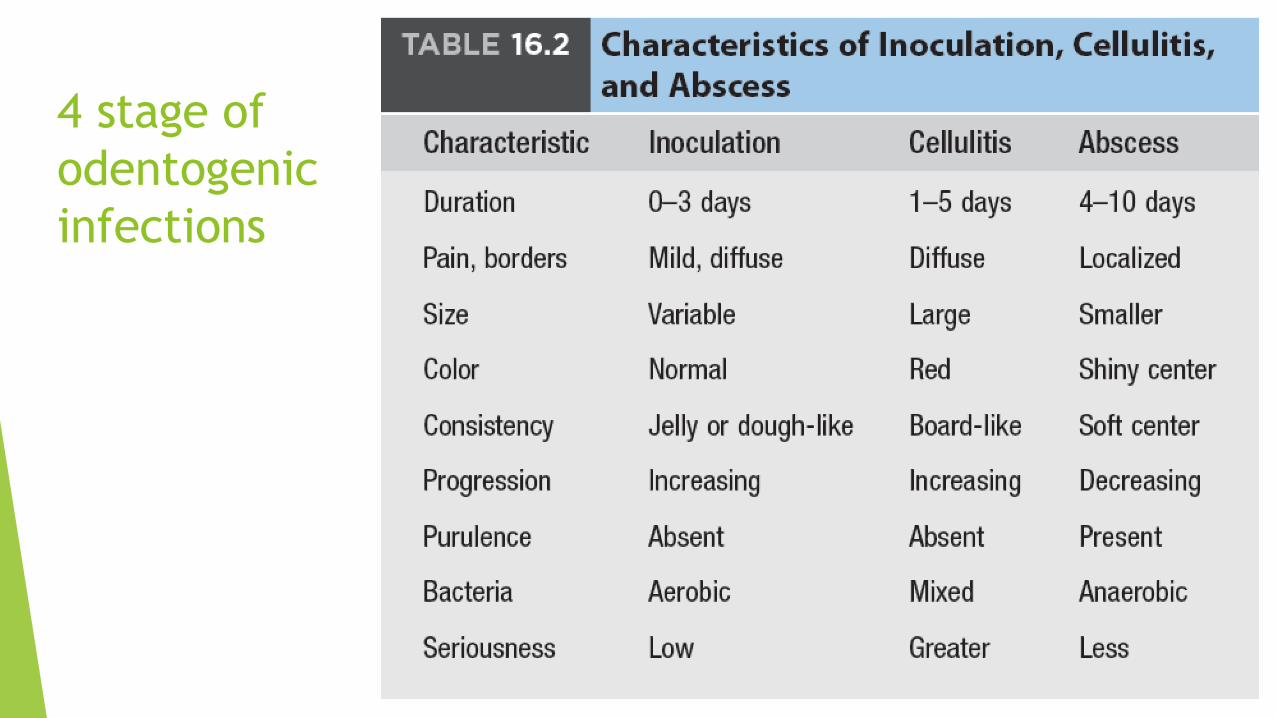
4 stage of
odentogenic
infections

odontogenic infections origins
1-periapical (palpal necrosis): most common
2- periodental(deep pocket)
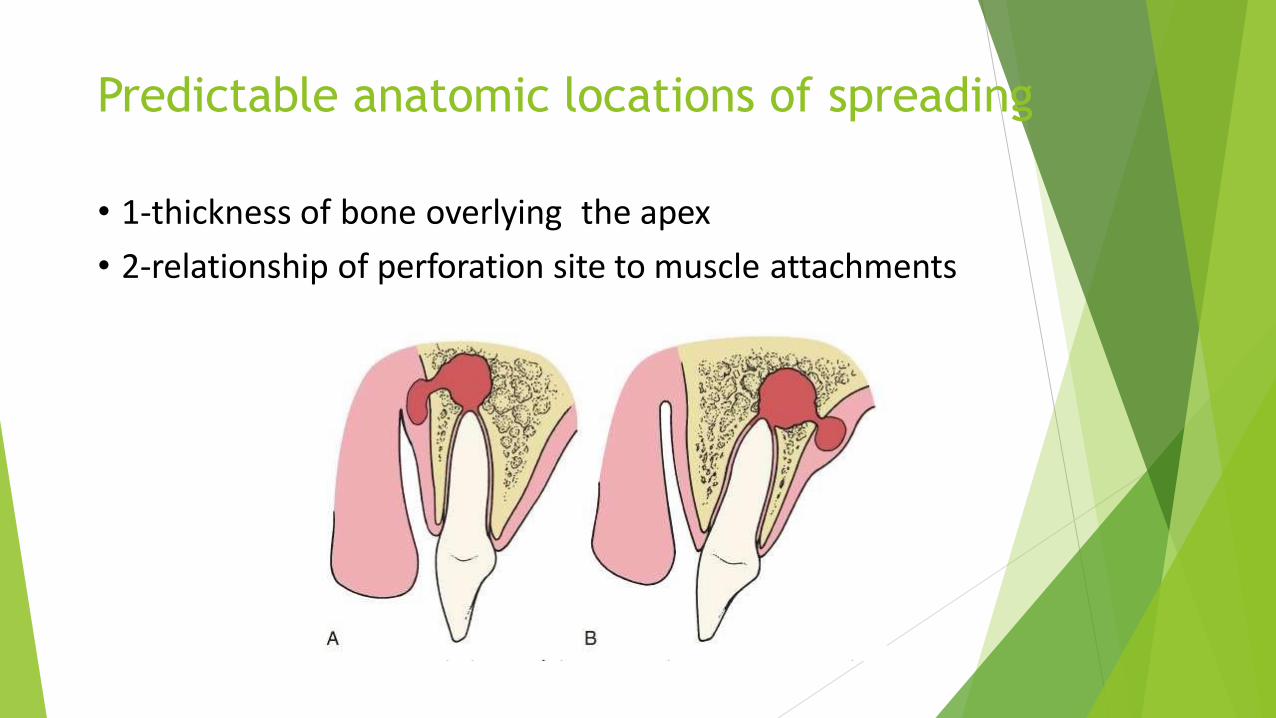
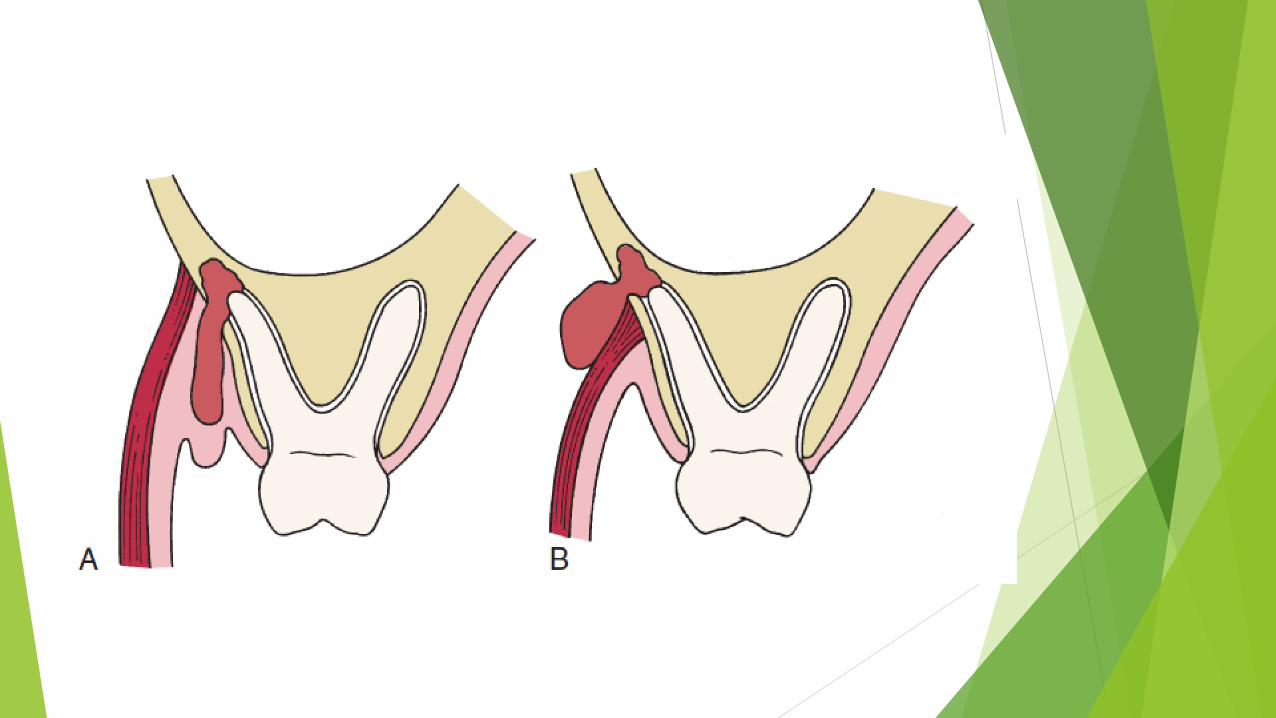
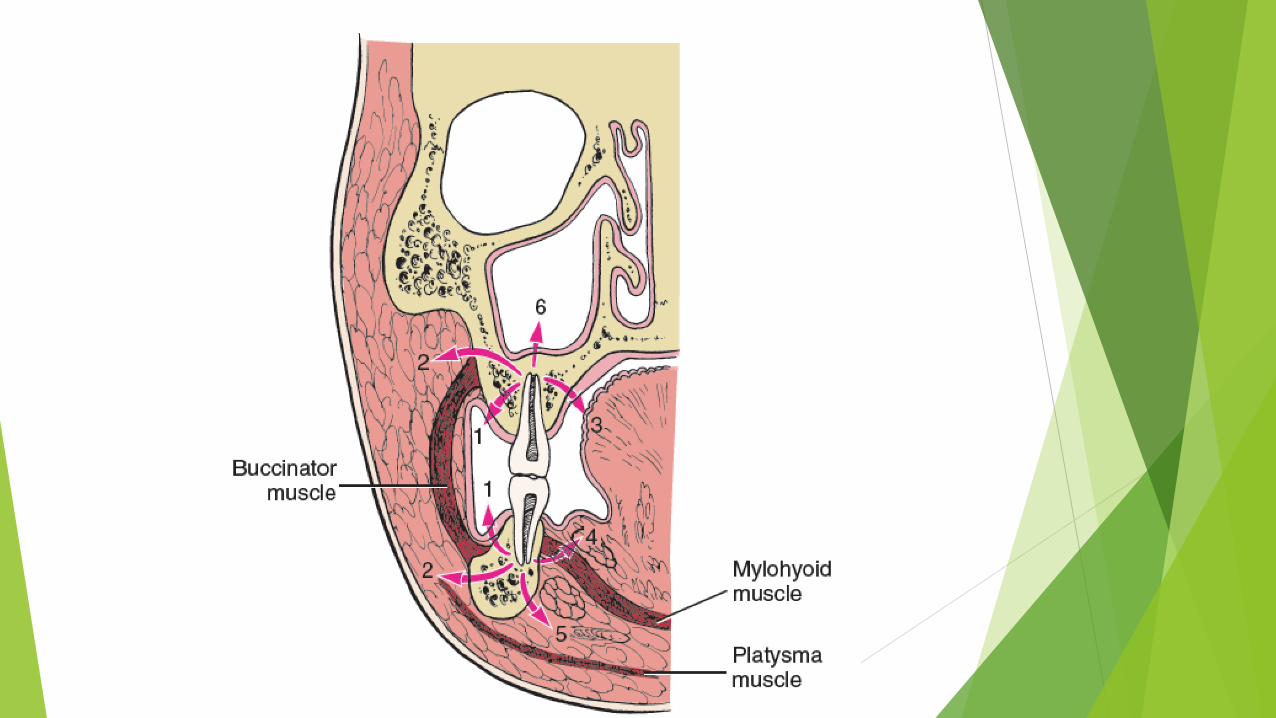
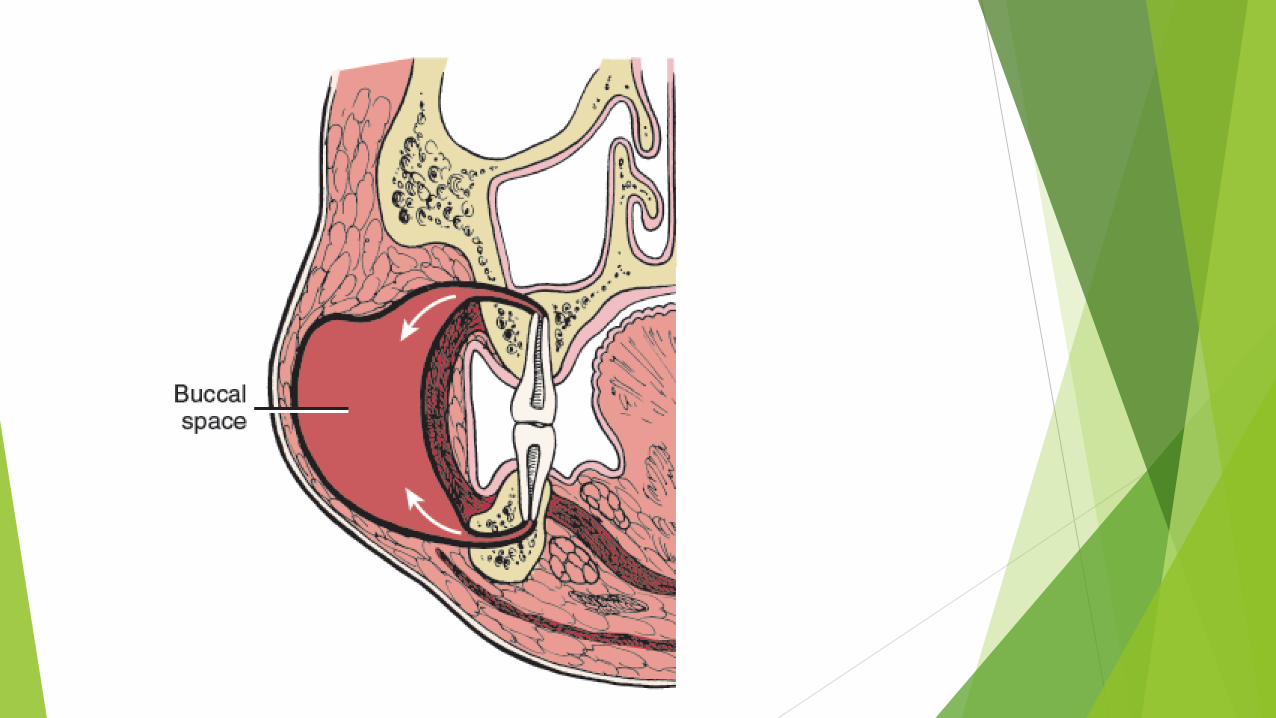
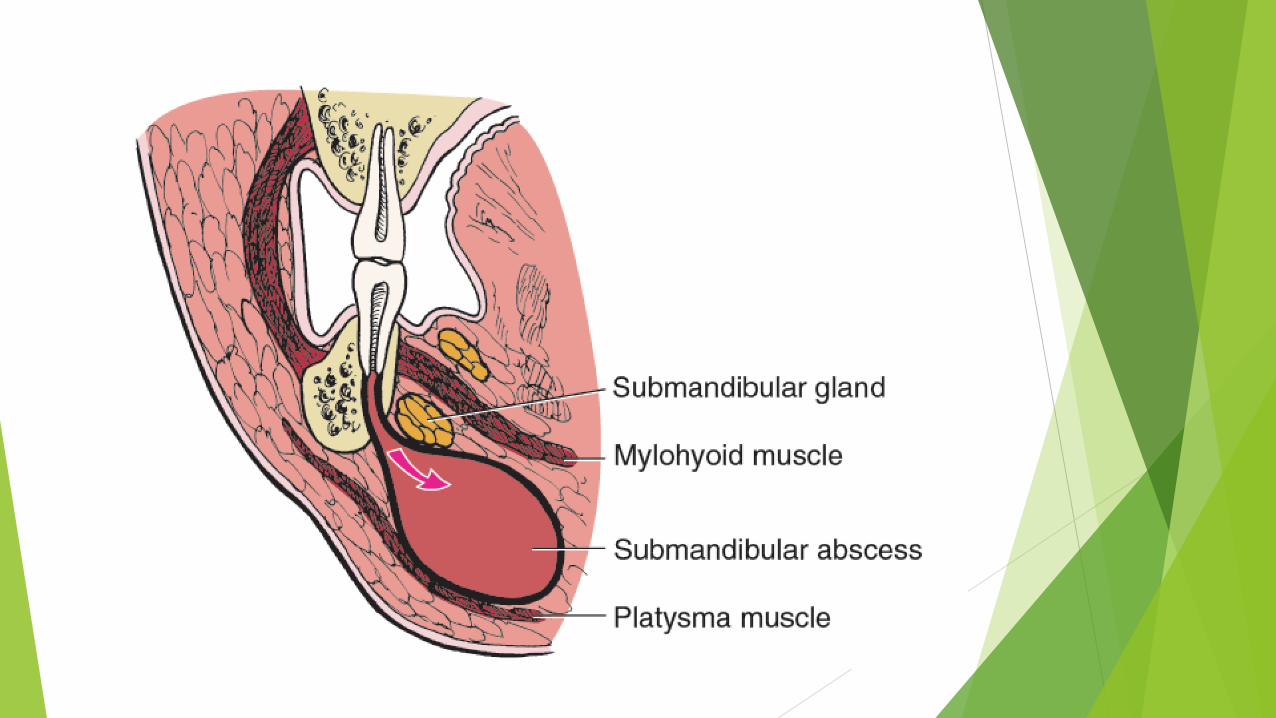
Predictable anatomic locations of spreading
• 1-thickness of bone overlying the apex
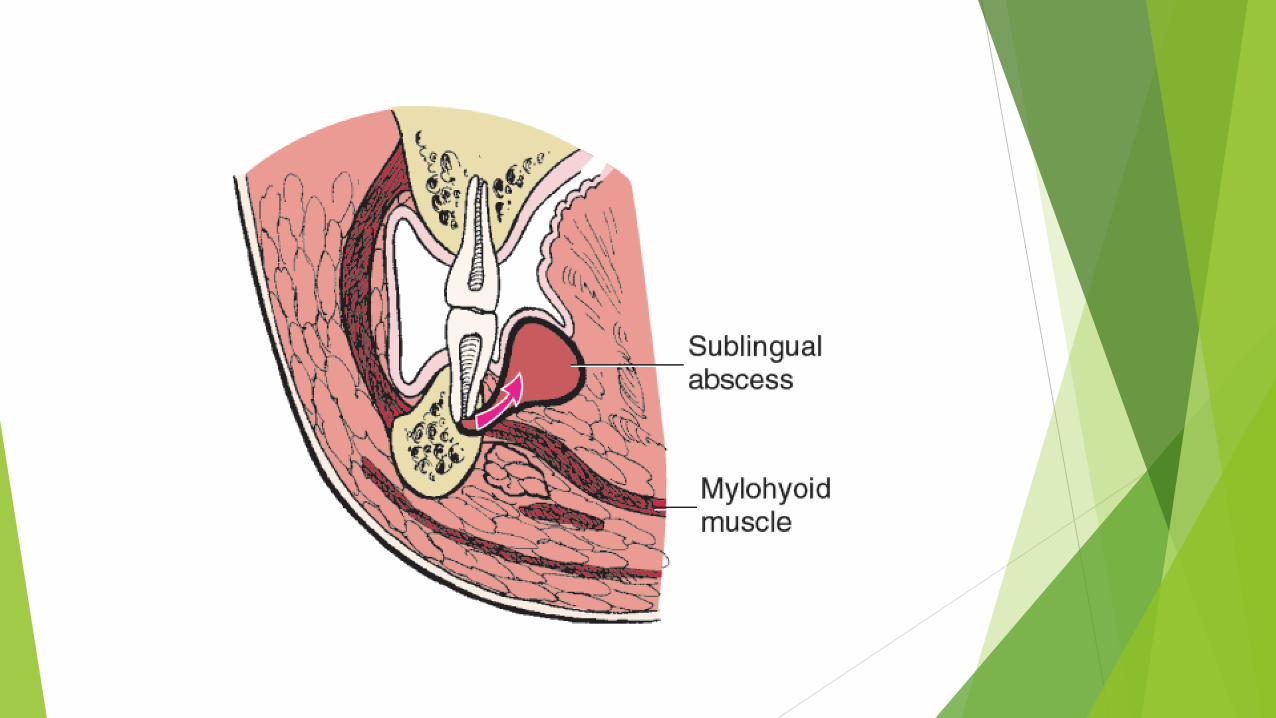
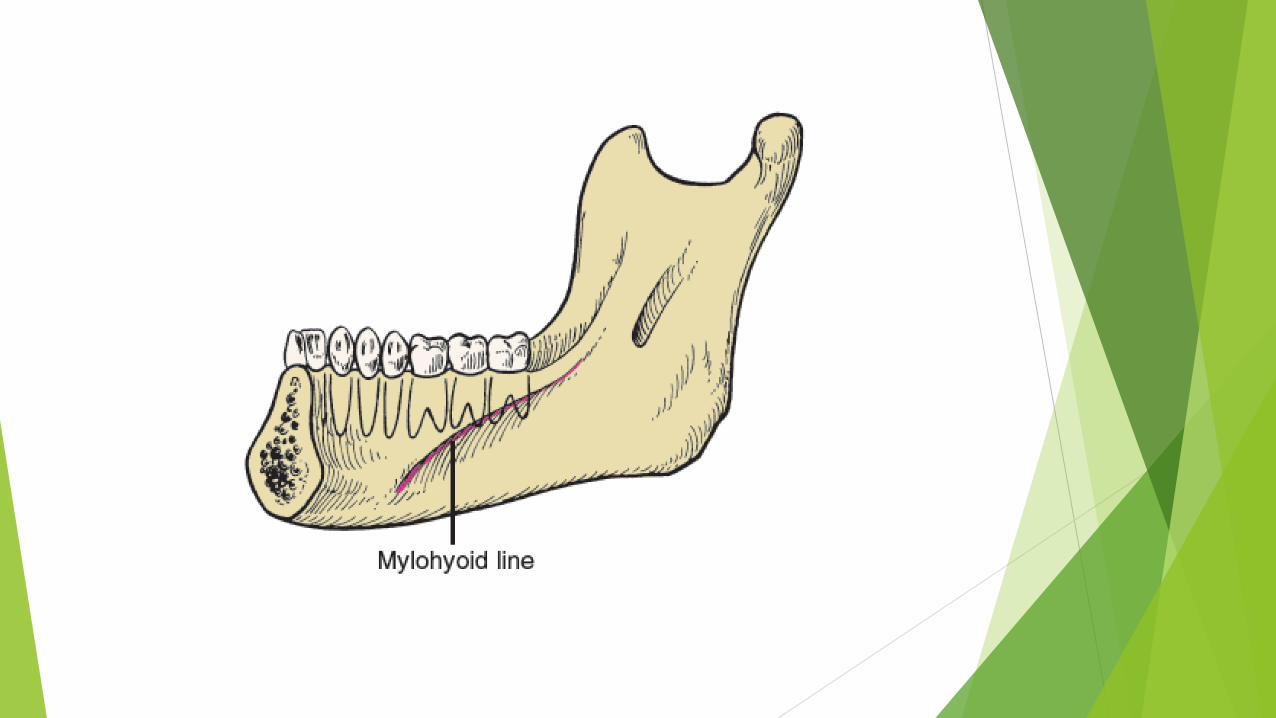
• 2-relationship of perforation site to muscle attachments












Principles of therapy of OdontogenicInfections
Principle 1:
determine severity of infection
• Complete history of current infection
• and physical examination
Complete history
• Chief compliant (patient own words)
• History of chief compliant of OI
1-how long OI been present
2-time of onset
3-how long from first symptoms (pain-swelling-drainage)
4-change of severity in time
Clinical sign of infections
• Infections are actually a severe inflammation
Redness
Pain
Swelling
Warmth
loss of function
pain
• Most common compliant
• Where it started
• How it spread since first noted

• Trismus• Dyspnea• dysphagia
Finally:
Ask how patient feel in general:Fatigue ,weak , sick, feverish
Previous Treatment
• Professional treatment
• Self treatment
• leftover antibiotics
• herbal remedies
• Completing the last treatment
Physical examination
• Vital signs
• Temperature
• Blood pressure
• pulse rate
• respiratory rate: 14-16 in a min
• Pain and anxiety
• septic shock results in Hypotension
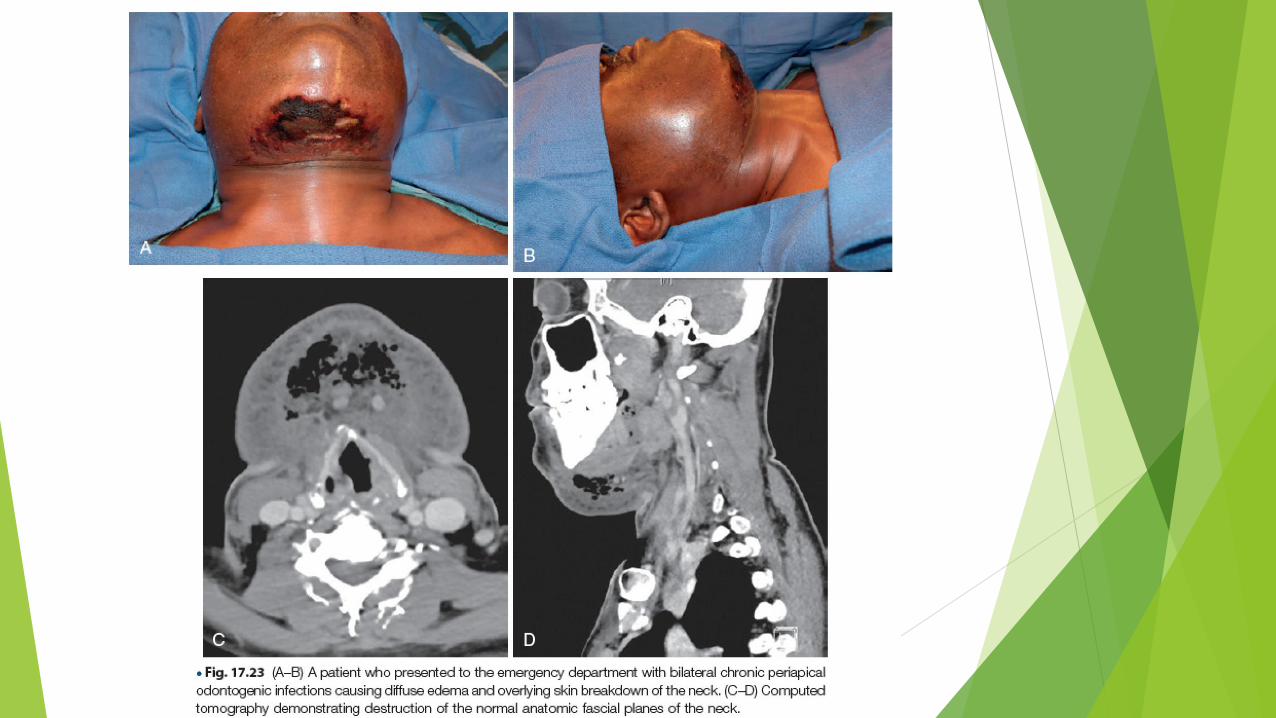
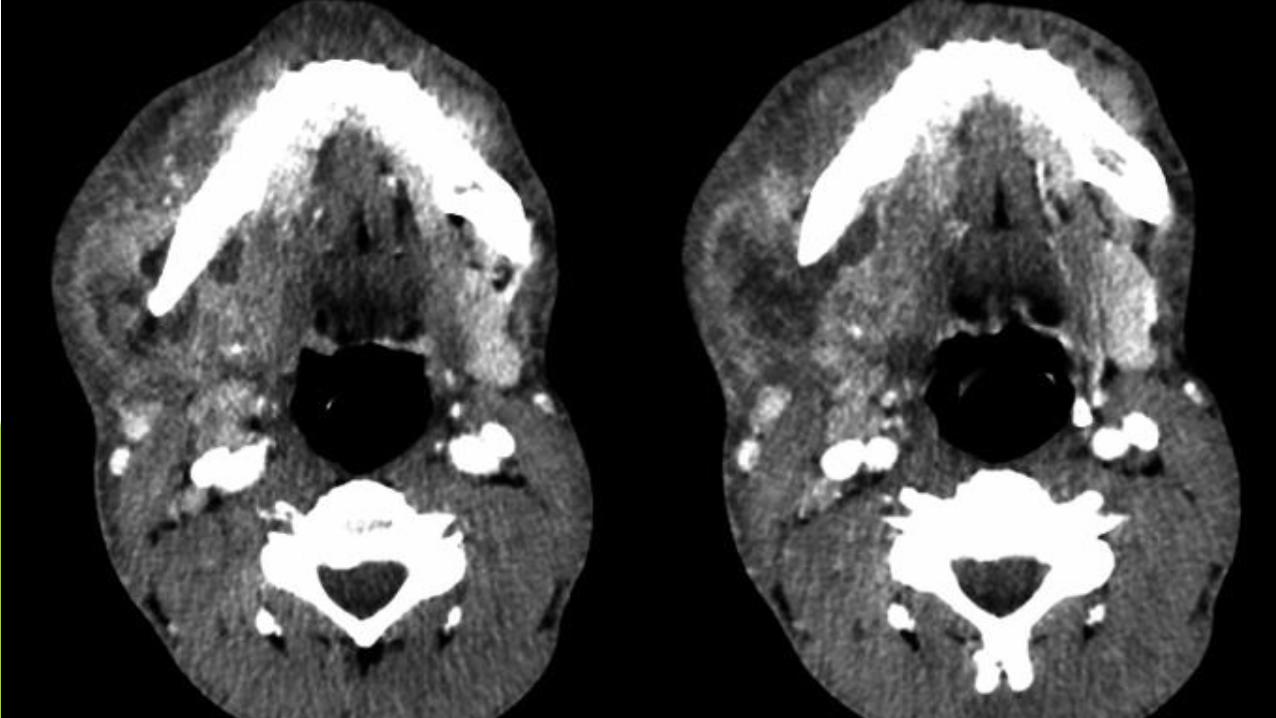
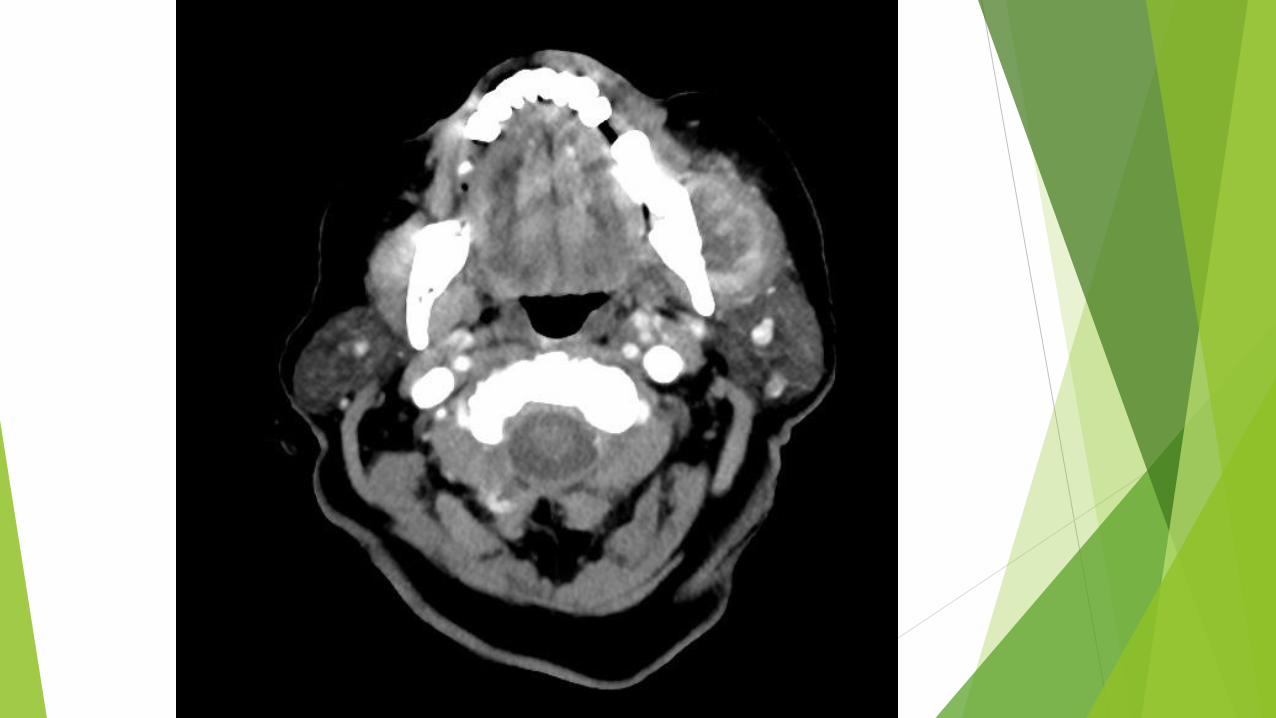
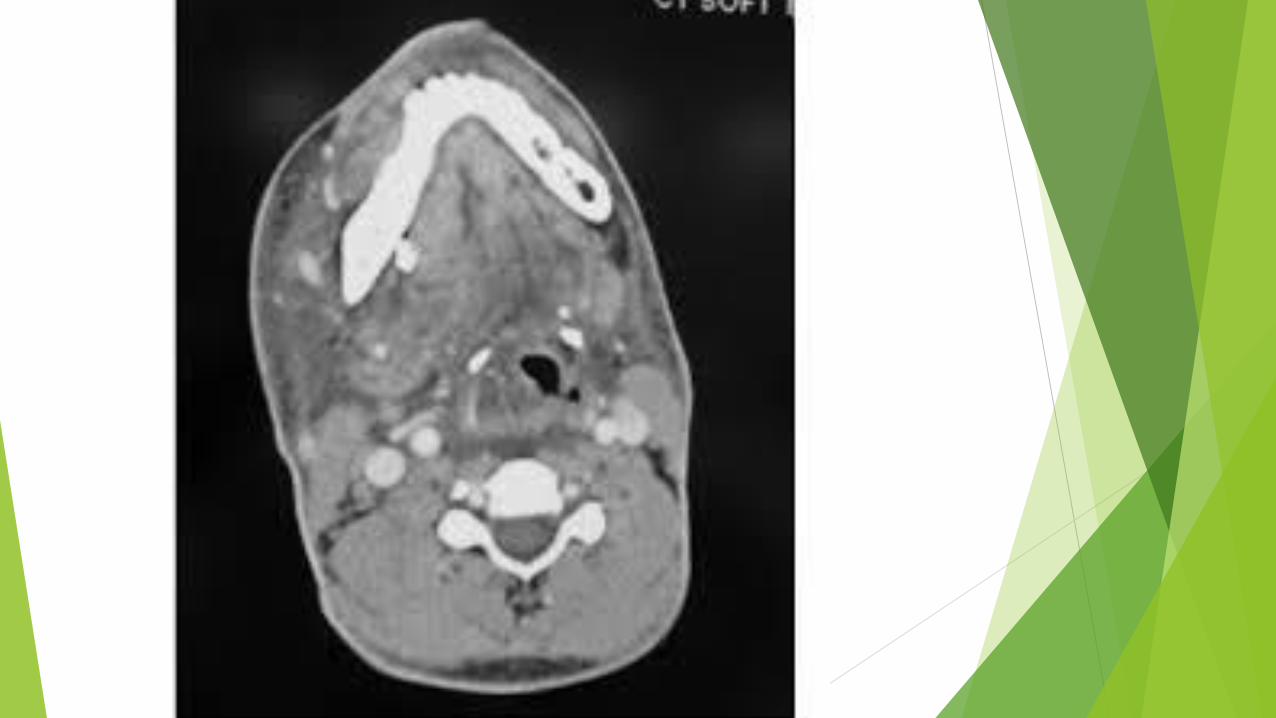
• Extention of Infection in fascial spaces of neck = partial or complete upper airway obstruction
Physical examination
• Inspection of patients general appearancetoxic appearancemalaisefatiguefeverishness
• Sign of infection
• Opening mouth
• Swallowing
• breathing
palpation
• In the area of swelling
• Tenderness
• Local warmth
• Consistency of swelling(soft-doughy-indurated-fluctuance)
• Fluctuance =a fluid filled balloon in the center of indurated tissue
Intra oral examination
• To find specific cause of infection
• Like severely carious teeth, periodontal abscess, periodontal disease ,
• Infected fracture of a tooth or entire of the jaw
• Should look for
• Area of gingivitis , swelling , draining sinus tracts
Radiographic examination
• Usually PA radiographs
• If there was any trismus and limited mouth opening or tenderness=panoramic view may be necessary
Mild infection
• Normal vital sign
• Only a mild temperature elevation
• Can be rapidly treated
Serious infection
• Abnormal vital signs
• Elevation in temperature ,blood pressure ,respiratory rate,
• Require more intensive therapy and evaluation by maxillofacial surgeon

Sense the stage of the infection and then ..
inoculation stage:
may be cured by removal of odontogenic cause
with or without supportive antibiotics
Cellulitis or abscess stages:
removal of dental cause
incision and drainage
antibiotics
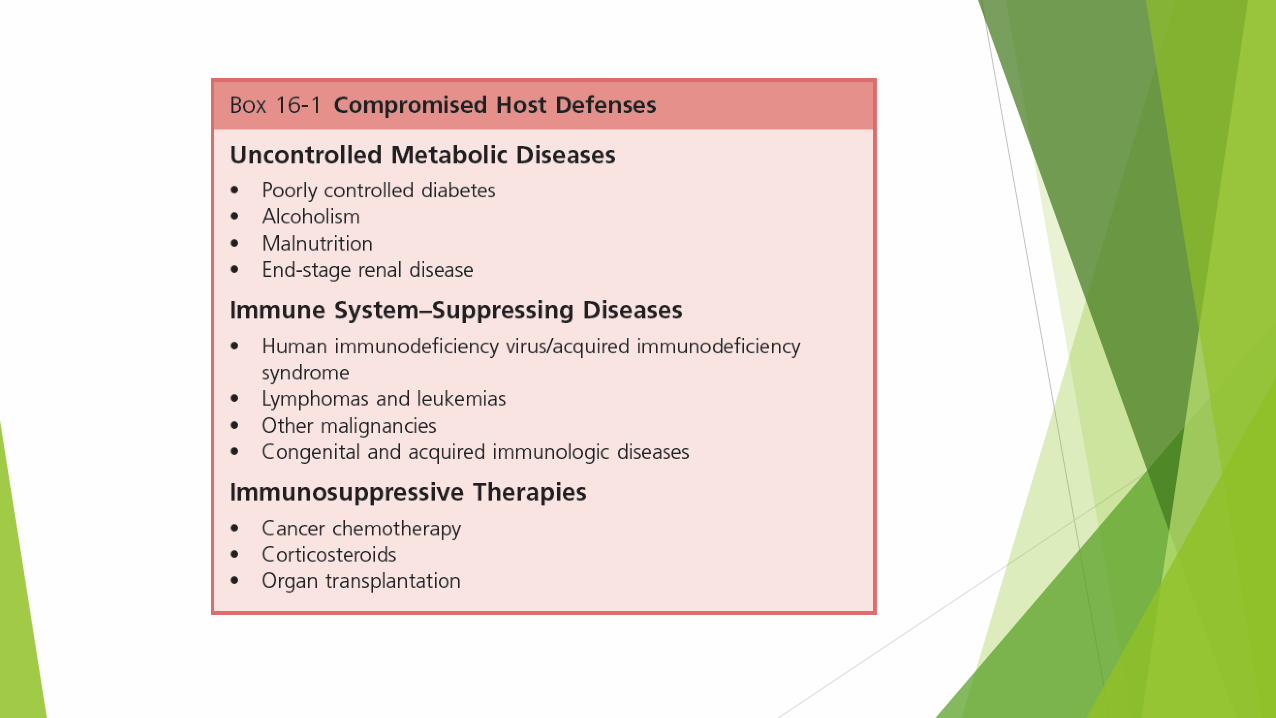
Principle 2 evaluate state of patients host
defense mechanisms
Principle 2 evaluate state of patients host
defense mechanisms
compromise host defense:
• infection may be spread more• treated more vigorously
• referral to MXF surgeon
• parenteral antibiotic therapy
Principle 3 determine whether patient should be treated by general dentist or oral-maxillofacial surgeon
Mostly: managed by DENTIST
Main criteria for Referring
1- rapidly progressive infection
2- dyspnea
3- dysphagia
4- drooling
threat to the airway


Other criteria
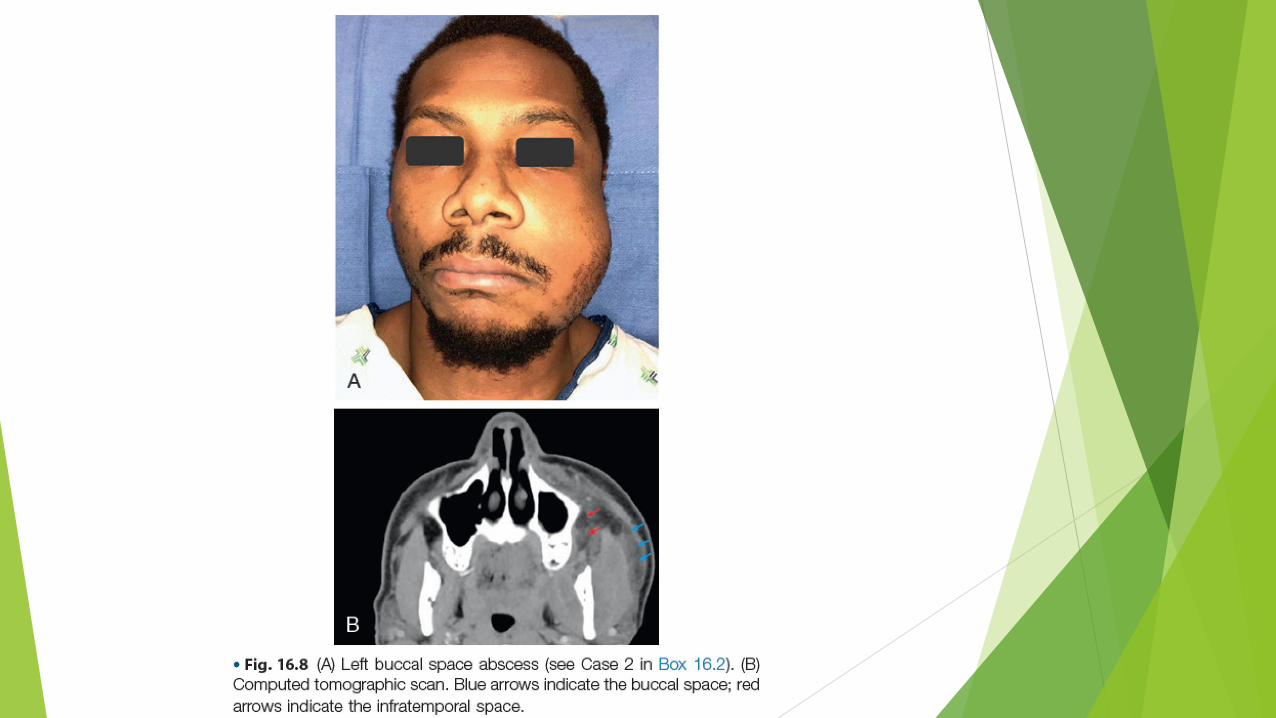
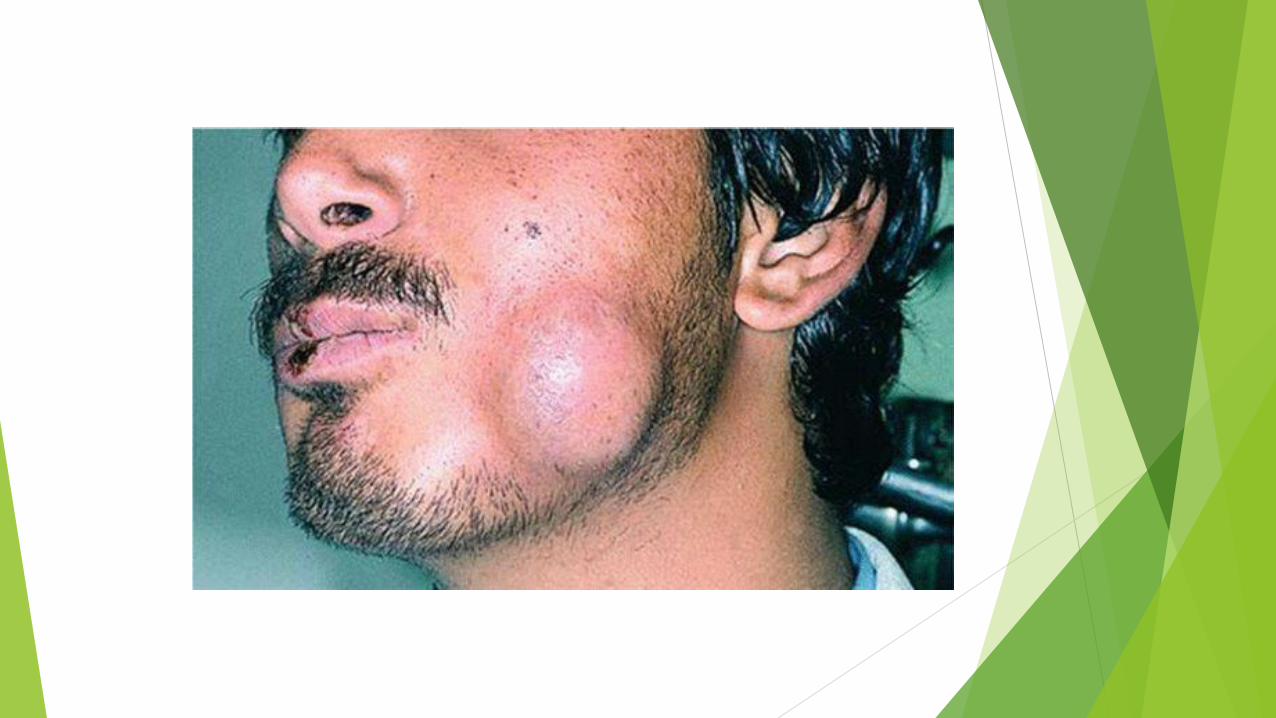
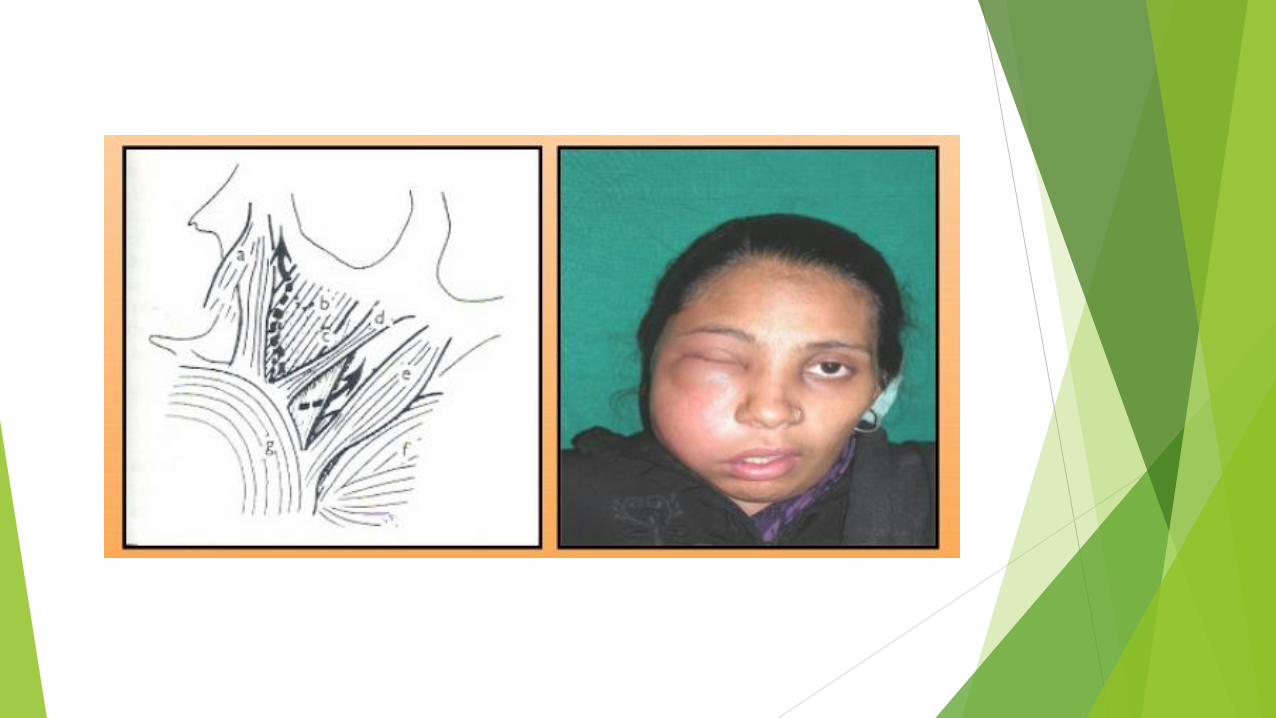
• 1-extraoral Swelling
• 2-High temperature
• 3-trismus
• MIO between:
• 20 and 30 =mild
• 10 and 20 =moderate
• less than 10 = severe
Other criteria
• Moderate or severe:
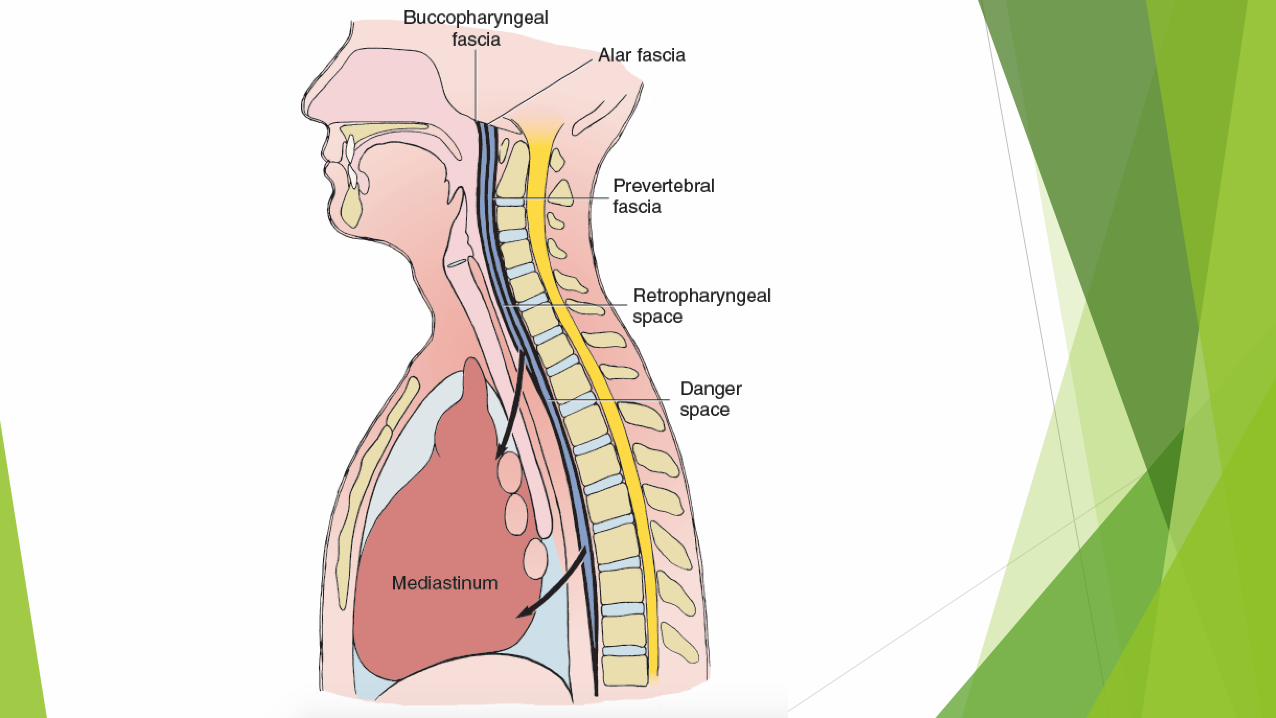
• infection in masticator spaces or worse both the lateral pharyngeal space and retropharyngeal space
• 4- systematic involvement (toxic appearance)
• 5- compromised host defense

Principle 4: treat infection surgically
odontogenic infections are a
surgicallymanaged disease process
antibiotics
Principle 4: treat infection surgically
elimination of the cause
source control
endodontic or periodontal
primary principle
Principle 4: treat infection surgically
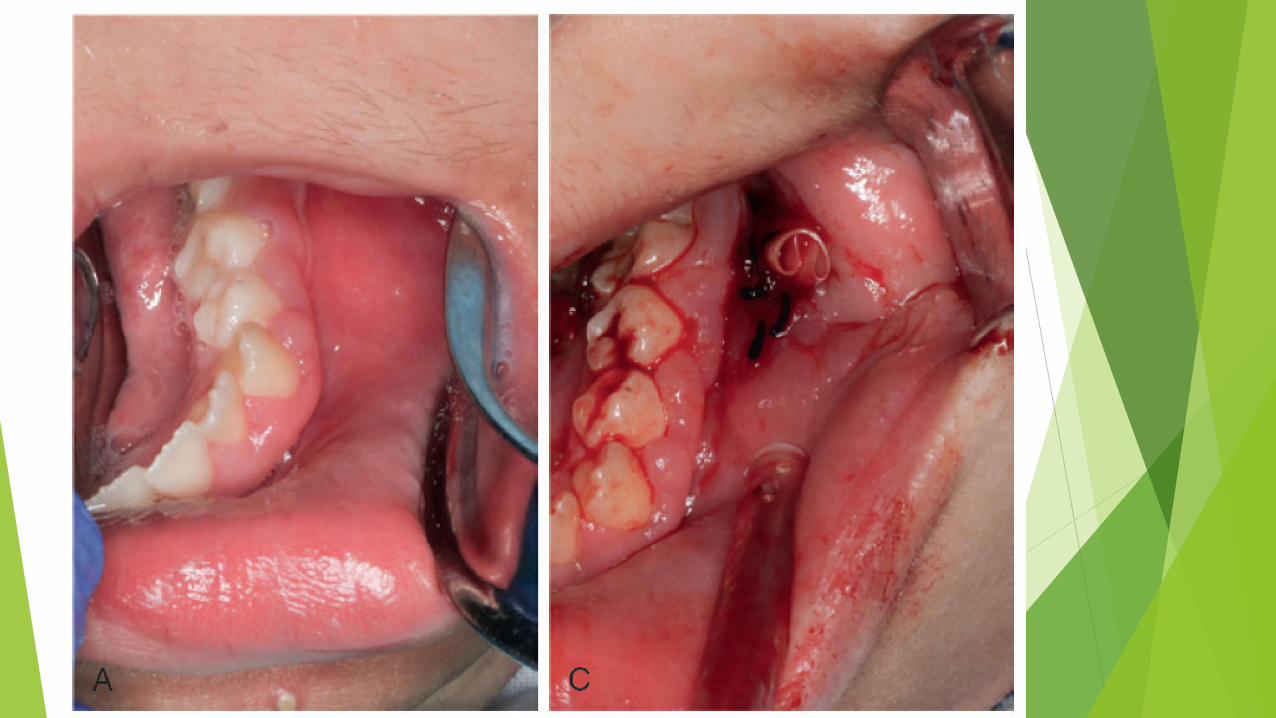
Secondary goal is to provide drainage
Incision & Drainage
1-decrease the load of bacteria and necrotic debries
2-Reduce the hydrostatic pressure in the region. which improve blood supply and delivery of host defense and antibiotic
3-stop cellulitis to spread deeper



•Whenever an abscess or cellulitis is diagnosed the surgeon must drain it.
• even if tooth cant be opened or extracted immedietly
• Antibiotic should be used if complete dranage cannot be achieved

Principle 5 support patient medically

Medications
• Coumadin (warfarin)-require reversal of anticoagulation before surgery
Dehydration
• Fever increase fluid requirement
• Inadequate fluid intake –because of the swelling –pain and…
• They should be encouraged to drink water and to take high –nutritional supplements
• -should be taking analgesics for pain
Principle 6 : choose and prescribe
appropriate antibiotic
• 1- seriousness of infection
• 2-whether adequate surgical treatment can be achieved
• 3- patients host defense


AB used in OI
For anaerobic bacteria = metronidazole and should be used in combination to others
Fewest times daily to improve compliance
C&S test should be considered

Use a bactericidal AB if possible
• Host defense play a less important role
• Specially in medically compromised patient
Penicillin

Principle 7 : administer antibiotic properly
• For odontogenic infection a 3or 4 day course of penicillin with appropriate surgery is effective as a 7 day course
• entire prescription must be taken

Principle 8: evaluate frequently
2 to 3 days after therapy
Check the site of I&D to remove the drain
Recurrence of infection
• Early removal of the drain
• Patient may stoped taking the drug too early
• Surgical intervention and antibiotic therapy should be considered