Principle MANAGEMEN ACS-Upload
57
Principle Management of Acute Coronary Syndrome Nahar Taufiq Bagian Kardiologi dan Kedokteran Vaskuler FK UGM Yogyakarta
-
Upload
intan-farida-yasmin -
Category
Documents
-
view
225 -
download
0
Transcript of Principle MANAGEMEN ACS-Upload

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 1/57
Principle Managementof
Acute Coronary Syndrome
Nahar Taufiq
Bagian Kardiologi dan Kedokteran Vaskuler FK UGM
Yogyakarta

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 2/57
Atherothrombosis* is theLeading Cause of Death Worldwide1
*Atherothrombosis defined as ischemic heart disease and cerebrovascular disease.1The World Health Report 2001. Geneva: WHO; 2001.Reprod.with permission from Cannon CP. Atherothrombosis slide compendium. Available at:
22.3
19.3
12.6
9.7
9
6.3
0 5 10 15 20 25 30
Atherothrombosis*
Infectious Disease
Cancer
Injuries
Pulmonary Disease
AIDS
Causes of Mortality (%)
8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 3/57
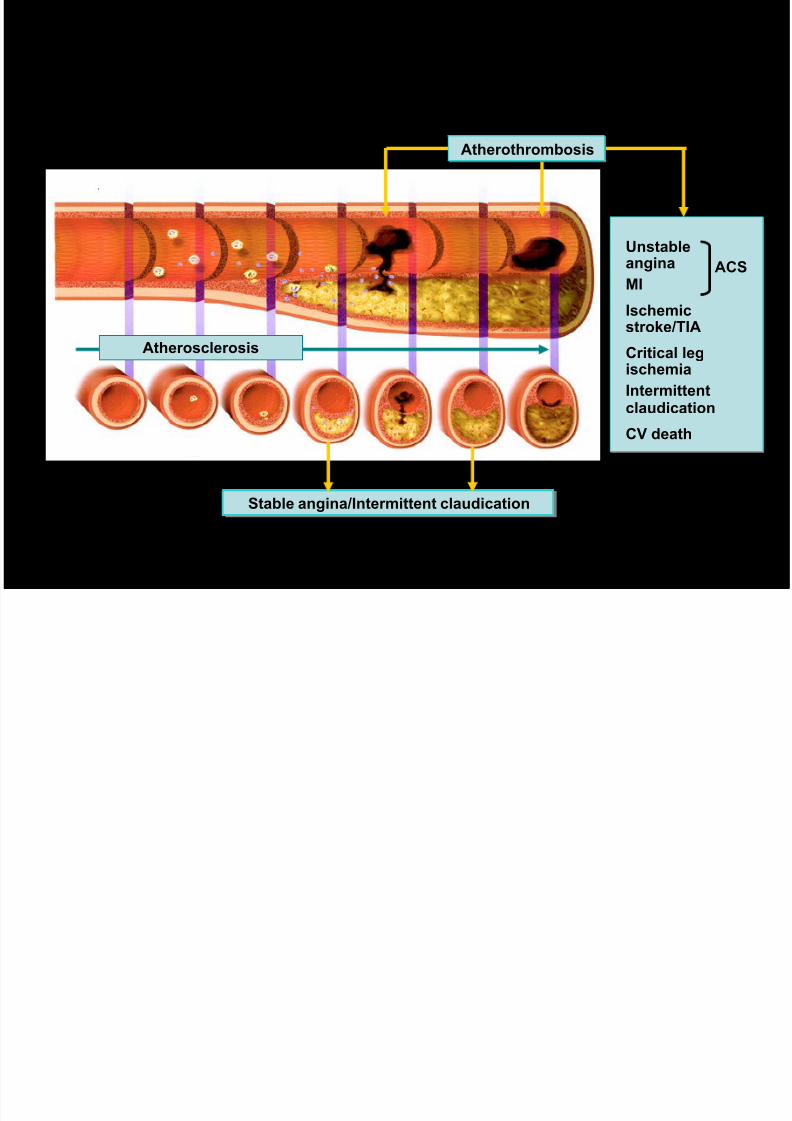
Atherothrombosis: A Generalized andProgressive Disease
Unstableangina
MI
Ischemicstroke/TIA
Critical legischemia
Intermittent
claudicationCV death
ACS
Atherosclerosis
Stable angina/Intermittent claudication
Stable angina/Intermittent claudication
Atherothrombosis
Atherothrombosis
MI = Myocardial infarction
ACS = Acute coronary syndromes
CV = CardiovascularAdapted from Libby P. Circulation 2001; 104: 365–372

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 4/57
Thrombus Formation and ACS
UAP NQMI STE-MI
Plaque Disruption/Fissure/Erosion
Thrombus Formation
Non-ST-SegmentElevation
Acute Coronary
Syndrome (NSTE-ACS)
ST-SegmentElevation
Acute
Coronary
Syndrome
(STE-ACS)
OldTerminology:
NewTerminology:
UAP

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 5/57
Pathophysiology
Ruptured Plaque with Occlusive Thrombus Formation
UAP orNON STEMI-ACS
STEMI-ACS

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 6/57
Initial RecognitionInitial Recognition
in the Emergencyin the EmergencyDepartmentDepartment

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 7/57
ED Evaluation of PatientsED Evaluation of Patients
1. Airway, Breathing, Circulation (ABC)
2. Vital signs, general observation
3. Presence or absence of jugular venous distension
4. Pulmonary auscultation for rales
5. Cardiac auscultation for murmurs and gallops
6. Presence or absence of stroke
7. Presence or absence of pulses
8. Presence or absence of systemic hypoperfusion (cool,clammy, pale, ashen)
Brief Physical Examination in the ED
P ExP Ex

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 8/57
ED Evaluation of PatientsED Evaluation of Patients
Aortic dissection
Pulmonary Emboli
Perforating ulcer
Differential Diagnosis of STEMI: Life-Threatening
Tension pneumothorax
Boerhaave syndrome
(esophageal rupture with
mediastinitis)
P ExP Ex

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 9/57
ED Evaluation of PatientsED Evaluation of Patients
Pericarditis
Atypical anginaEarly repolarizationWolff-Parkinson-White
syndromeDeeply inverted T-
waves suggestive of a central nervoussystem lesion orapical hypertrophiccardiomyopathy
LV hypertrophy with
strainBrugada syndrome
Myocarditis
Hyperkalemia
Bundle-branch blocks
Vasospastic angina
Hypertrophiccardiomyopathy
Differential Diagnosis of STEMI:Other Cardiovascular and Nonischemic
P ExP Ex

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 10/57
Gastroesophagealreflux (GERD) and
spasmChest-wall pain
Pleurisy
Peptic ulcer disease
Panic attack
Cervical disc orneuropathic pain
Biliary or pancreatic pain
Somatization andpsychogenic paindisorder
ED Evaluation of PatientsED Evaluation of Patients
Differential Diagnosis of STEMI: Other Noncardiac
P ExP Ex

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 11/57
ElectrocardiogramElectrocardiogram
If the initial ECG is not diagnostic of STEMI,
serial ECGs or continuous ST-segment
monitoring should be performed in the
patient who remains symptomatic or if there
is high clinical suspicion for STEMI.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
DxDx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 12/57
ElectrocardiogramElectrocardiogram
Show 12-lead ECG results to emergency
physician within 10 minutes of ED arrival in all
patients with chest discomfort (or anginal
equivalent) or other symptoms of STEMI.
In patients with inferior STEMI, ECG leads
should also be obtained to screen for right
ventricular infarction.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
DxDx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 13/57
Laboratory ExaminationsLaboratory Examinations
Laboratory examinations should be performed as partof the management of STEMI patients, but should not
delay the implementation of reperfusion therapy.
Serum biomarkers for cardiac damage
Complete blood count (CBC) with platelets International normalized ratio (INR)
Activated partial thromboplastin time (aPTT)
Electrolytes and magnesium
Blood urea nitrogen (BUN) Creatinine
Glucose
Complete lipid profile
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
DxDx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 14/57
Cardiac-specific troponins should be used as
the optimum biomarkers for the evaluation
of patients with STEMI who have coexistent
skeletal muscle injury.
For patients with ST elevation on the 12-lead
ECG and symptoms of STEMI, reperfusion
therapy should be initiated as soon aspossible and is not contingent on a
biomarker assay.
Biomarkers of Cardiac DamageBiomarkers of Cardiac Damage
III IIaIIaIIa IIbIIbIIb IIIIIIII IIII IIaIIaIIa IIbIIbIIb IIIIIIII IIII IIaIIaIIa IIbIIbIIb IIIIIIII IIIaIIaIIa IIbIIbIIb IIIIIIII I
III IIaIIaIIa IIbIIbIIb IIIIIIII IIII IIaIIaIIa IIbIIbIIb IIIIIIII IIII IIaIIaIIa IIbIIbIIb IIIIIIII IIIaIIaIIa IIbIIbIIb IIIIIIII I
DxDx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 15/57
InitialInitial ManagementManagement
in the Emergencyin the EmergencyDepartmentDepartment

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 16/57
Supplemental oxygen should be administered to
patients with arterial oxygen desaturation (SaO2
< 90%).
It is reasonable to administer supplemental
oxygen to all patients with uncomplicated STEMI
during the first 6 hours.
OxygenOxygen
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
TxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 17/57
Patients with ongoing ischemic discomfortshould receive sublingual NTG (0.4 mg) every 5minutes for a total of 3 doses, after which anassessment should be made about the need forintravenous NTG.
Intravenous NTG is indicated for relief of
ongoing ischemic discomfort that responds to
nitrate therapy, control of hypertension, or
management of pulmonary congestion.
NitroglycerinNitroglycerin
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
TxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 18/57
Nitrates should not be administered topatients with:
Nitrates should not be administered topatients who have received aphosphodiesterase inhibitor for erectiledysfunction within the last 24 hours (48 hoursfor tadalafil).
• systolic pressure < 90 mm Hg or ≥ to 30 mm Hg
below baseline
• severe bradycardia (< 50 bpm)• tachycardia (> 100 bpm) or • suspected RV infarction.
NitroglycerinNitroglycerin
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
TxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 19/57
AnalgesiaAnalgesia
Morphine sulfate (2 to 4 mg intravenously
with increments of 2 to 8 mg intravenously
repeated at 5 to 15 minute intervals) is theanalgesic of choice for management of pain
associated with STEMI.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
TxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 20/57
AspirinAspirin
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Aspirin should be chewed by patients who
have not taken aspirin before presentation
with STEMI. The initial dose should be 162
mg (Level of Evidence: A) to 325 mg (Level
of Evidence: C)
Although some trials have used enteric-coated aspirin for initial dosing, more rapid buccalabsorption occurs with non–enteric-coated formulations.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
TxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 21/57
0
5
10
15
0 5 10 20 25 30
Endp
oint*(%)
Days
Placebo
Clopidogrel
20%
P=0.03
* Cardiovascular death, recurrent MI, or recurrent ischemia
leading to the need for urgent revascularization
Sabatine MS et al for the CLARITY-TIMI 28 Investigators. N Engl J Med 2005;352:1179-89
CLARITY-TIMI 28
ClopidogrelClopidogrelTxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 22/57
1.9
1.6
3.4
1.7
0.9
2.7
0
1
2
3
4
P=0.80P=0.12
P=0.24
%
of
pati
en
ts
Major bleeding Minor bleeding Major or minor
bleeding
CLARITY-TIMI 28: Tingkat keamanan dalam 30hari
ASA + CLO
ASA

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 23/57
1 Dabaghi SF et al. Am J Cardiol 1994;74:720-3. 2. Savcic M et al. Semin Thromb Hemost 1999;25:15-19
3 Quinn MJ, Fitzgerald DJ. Circulation 1999;100:1667-72 4. Hochholzer W et al. Circulation
2005;111:2560-4 5. Lubbe DF, Berger PB. J Interv Cardiol
Agent Dose Onset
Aspirin Dosis 80 - 320 mg1 15 - 30 minutes
Clopidogrel 75 mg maintenance dose2
300 mg loading dose3
600 mg loading dose4
900 mg loading
dose3
Max at 3-7 days Max
at 24 to 48 h Max at
2 h same with
600 mg loading dose
Ticlopidine 250 mg 2x perhari5 50% pada 5 hari dan maksimum
8-11 hari
Onset of antiplateletTxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 24/57
Mona_Mona_
CoCo
InitialInitial ManagementManagement in the EDin the ED
1 2 3

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 25/57
Reperfusion Therapy and
RecommendationsSTEMI
11

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 26/57
ReperfusionReperfusion
The medical system goal is to facilitate rapid
recognition and treatment of patients with STEMI
such that door-to- needle (or medical contact–
to-needle) time for initiation of fibrinolytic
therapy can be achieved within 30 minutes or
that door-to-balloon (or medical contact–to-
balloon) time for PCI can be kept within 90
TxTx

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 27/57
Symptom
Recognition
Call to
Medical System
ED-Hospital Cath LabPreHospital
Delay in Initiation of Reperfusion Therapy
Increasing Loss of Myocytes
Treatment Delayed is Treatment DeniedTreatment Delayed is Treatment Denied

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 28/57
Fibrinolysis generally preferred Early presentation ( ≤ 3 hours from symptom
onset and delay to invasive strategy)
Invasive strategy not an option Cath lab occupied or not available
Vascular access difficulties
No access to skilled PCI lab
Delay to invasive strategy Prolonged transport
Door-to-balloon more than 90 minutes
> 1 hour vs fibrinolysis (fibrin-specific agent) now
Reperfusion Options for STEMI PatientsReperfusion Options for STEMI Patients Select Reperfusion Treatment.Select Reperfusion Treatment.
If presentation is < 3 hours and there is no delay to an invasive
strategy, there is no preference for either strategy.

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 29/57
Contraindications and CautionsContraindications and Cautions
for Fibrinolysis in STEMIfor Fibrinolysis in STEMI
Absolute
Contraindications
• Any prior intracranial hemorrhage
• Known structural cerebral vascular lesion
(e.g., arteriovenous malformation)
• Known malignant intracranial neoplasm(primary or metastatic)
• Ischemic stroke within 3 months EXCEPT
acute ischemic stroke within 3 hours
NOTE: Age restriction for fibrinolysis has been removed
compared with prior guidelines.

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 30/57
Contraindications and CautionsContraindications and Cautions
for Fibrinolysis in STEMIfor Fibrinolysis in STEMI
AbsoluteContraindications
• Suspected aortic dissection
• Active bleeding or bleeding diathesis
(excluding menses)
• Significant closed-head or facial traumawithin 3 months

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 31/57
Contraindications and CautionsContraindications and Cautions
for Fibrinolysis in STEMIfor Fibrinolysis in STEMI
• History of chronic, severe, poorly controlled
hypertension
• Severe uncontrolled hypertension on
presentation (SBP > 180 mm Hg or DBP >
110 mm Hg)
• History of prior ischemic stroke greater than
3 months, dementia, or known intracranial
pathology not covered in contraindications
• Traumatic or prolonged (> 10 minutes) CPR
or major surgery (< 3 weeks)
Relative
Contraindications

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 32/57
Contraindications and CautionsContraindications and Cautions
for Fibrinolysis in STEMIfor Fibrinolysis in STEMI
RelativeContraindications
• Recent (< 2 to 4 weeks) internal bleeding• Noncompressible vascular punctures
• For streptokinase/anistreplase: prior
exposure (> 5 days ago) or prior allergic
reaction to these agents
• Pregnancy
• Active peptic ulcer
• Current use of anticoagulants: the higher the
INR, the higher the risk of bleeding
f i i f i

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 33/57
Invasive strategy generally preferred Skilled PCI lab available with surgical backup
Door-to-balloon < 90 minutes
• High Risk from STEMI
Cardiogenic shock, Killip class ≥ 3
Contraindications to fibrinolysis, including
increased risk of bleeding and ICH
Late presentation
> 3 hours from symptom onset
Diagnosis of STEMI is in doubt
Reperfusion Options for STEMI PatientsReperfusion Options for STEMI Patients Select Reperfusion Treatment.Select Reperfusion Treatment.
If presentation is < 3 hours and there is no delay to an invasive strategy,
there is no preference for either strategy.

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 34/57
Antithrombin Therapyand Recommendations
Non-STEMI & UAP
2-32-3
ACC/AHA R d ti f

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 35/57
ACC/AHA Recommendations forAntithrombin Therapy in Patients with
NSTE-ACS
• Class I
– Anticoagulation with subcutaneous LMWH or intravenousUFH should be added to antiplatelet therapy
– Dose of UFH 60-70 U/kg (max 5000) IV followed byinfusion of 12-15 U/kg/hr (initial max 1000 U/hr) titratedto aPTT 1.5-2.5 times control
– Dose of enoxaparin 1 mg/kg subcutaneously q12 hr; thefirst dose may be preceded by a 30-mg IV bolus
– Fundaparinoux SC
• Class IIa– Enoxaparin is preferable to UFH as an anticoagulant
unless CABG is planned within 24 hours
Available at: www.acc.org/clinical/guidelines/unstable/unstable.pdf.
1 2 3

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 36/57
1 2 3

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 37/57
Secondary Prevention
andLong Term Management
S

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 38/57
Secondary Prevention and Long Term Management
• Assess tobacco use.
• Strongly encourage patient and familyto stop smoking and to avoid secondhand
smoke.
• Provide counseling, pharmacologicaltherapy (including nicotine replacement
and bupropion), and formal smokingcessation programs as appropriate.
SmokingGoal: Complete Cessation
Goals Recommendations
S d P ti d L T M t

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 39/57
Secondary Prevention and Long Term Management
If blood pressure is 120/80 mm Hg or greater:
• Initiate lifestyle modification (weight control,physical activity, alcohol moderation, moderatesodium restriction, and emphasis on fruits,
vegetables, and low-fat dairy products) in allpatients.
If blood pressure is 140/90 mm Hg or greater or130/80 mm Hg or greater for individuals with
chronic kidney disease or diabetes:
• Add blood pressure-reducing medications,emphasizing the use of beta-blockers and inhibitorsof the renin-angiotensin-aldosterone system.
Blood pressurecontrol:Goal: < 140/90 mm Hg or <130/80 mm Hg if chronic kidney disease or diabetes
Goals Recommendations
S d P ti d L T M t

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 40/57
Secondary Prevention and Long Term Management
• Assess risk, preferably with exercise test, to
guide prescription.
• Encourage minimum of 30 to 60 minutes ofactivity, preferably daily but at least 3 or 4 times
weekly (walking, jogging, cycling, or other aerobic
activity) supplemented by an increase in daily
lifestyle activities (e.g., walking breaks at work,gardening, household work).
• Cardiac rehabilitation programs are
recommended for patients with STEMI.
Physicalactivity:Minimum goal: 30 minutes 3 to
4 days per week; Optimal daily
Goals Recommendations
S d P ti d L T M t

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 41/57
Secondary Prevention and Long Term Management
• Start dietary therapy in all patients (< 7% of totalcalories as saturated fat and < 200 mg/dcholesterol). Promote physical activity and weightmanagement. Encourage increased consumption ofomega-3 fatty acids.
• Assess fasting lipid profile in all patients,preferably within 24 hours of STEMI. Add drugtherapy according to the following guide:
Lipidmanagement:(TG less than200 mg/dL)Primary goal: LDL-C << than 100 mg/dL
Goals Recommendations
LDL-C < 100 mg/dL (baseline or on
treatment):Statins should be used to lower LDL-C.
LDL-C ≥ 100 mg/dL (baseline or ontreatment):
Intensify LDL-C–lowering therapy with drugtreatment, giving preference to statins.
S d P ti d L T M t

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 42/57
Secondary Prevention and Long Term Management
If TGs are ≥ 150 mg/dL or HDL-C is < 40 mg/dL:Emphasize weight management and physical
activity. Advise smoking cessation.
If TG is 200 to 499 mg/dL:
After LDL-C–lowering therapy, consider addingfibrate or niacin.
If TG is ≥ 500 mg/dL:
Consider fibrate or niacin before LDL-C–lowering
therapy.
Consider omega-3 fatty acids as adjunct for high
TG.
Lipidmanagement:
(TG 200 mg/dL
or greater)
Primary goal:
Non–HDL-C <<130 mg/dL
Goals Recommendations

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 43/57
NCEP ATP III Guidelines
Patients withPatients withDrug therapyDrug therapy
considered if LDLconsidered if LDL
* TLC: therapeutic lifestyle changes* TLC: therapeutic lifestyle changesNational Cholesterol Education Program, Adult Treatment Panel III.National Cholesterol Education Program, Adult Treatment Panel III. JAMA JAMA 2001;2001;285285:2486–2497:2486–2497
Initiate TLC*Initiate TLC*if LDLif LDL
LDLLDLtreatmenttreatment
goalgoal
00 1 risk factors1 risk factors ≥160 mg/dL160 mg/dL†† ≥ 190 mg/dL190 mg/dL
(160(160–189 mg/dL:189 mg/dL:drug optional)drug optional)
<160 mg/dL<160 mg/dL††
2 risk factors2 risk factors(10(10 year riskyear risk 20%)20%)
≥130 mg/dL130 mg/dL††
1010 year risk 10year risk 10–
20%:20%: ≥ 130 mg/dL130 mg/dL10-year risk <10%:10-year risk <10%:
≥ 160 mg/dL160 mg/dL
<130 mg/dL<130 mg/dL††
CHD and CHD riskCHD and CHD risk
equivalentsequivalents
(10(10 year risk >20%)year risk >20%)
≥100 mg/dL100 mg/dL†† <100 mg/dL<100 mg/dL††
†† 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L
≥ 130 mg/dL130 mg/dL
drug optional)drug optional)
(100–129 mg/dL:(100–129 mg/dL:
Secondary Prevention and Long Term Management

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 44/57
Secondary Prevention and Long Term Management
Goals Recommendations
Calculate BMI and measure waistcircumference as part of evaluation. Monitorresponse of BMI and waist circumference totherapy.
Start weight management and physical activityas appropriate. Desirable BMI range is 18.5 to24.9 kg/m2.
If waist circumference is ≥ 35 inches in women
or ≥ 40 inches in men, initiate lifestyle changesand treatment strategies for metabolicsyndrome.
Weightmanagement:Goal: BMI 18.5 to 24.9 kg/m 2
Waist circumference: Women: < 35 in.Men: < 40 in.

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 45/57
Secondary Prevention and Long Term Management
Goals Recommendations
Appropriate hypoglycemic therapy to
achieve near-normal fasting plasma
glucose, as indicated by HbA1c.
Treatment of other risk factors (e.g.,
physical activity, weight management,
blood pressure, and cholesterol
management).
Diabetes
management:
Goal:
HbA1c < 7%

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 46/57

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 47/57
Guidelines for the Use of Enoxaparin in Patientswith NSTE-ACS
• 1 mg/kg SQ q12 hours (actual body weight)
– An initial 30 mg IV dose can be considered
• Adjust dosing if CrCl <30 cc/min
– 1 mg/kg SQ q24 hours
•Do not follow PTT; do not adjust based on PTT
• Stop if platelets ↓ by 50% or below 100,000/mm3
• If patient to undergo PCI:
– 0-8 hours since last SQ dose: no additional antithrombin therapy
– 8-12 hours since last SQ dose: 0.3 mg/kg IV immediately prior to PCI
Applying Classification ofApplying Classification of

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 48/57
Class I Benefit >>> Risk
Procedure/ TreatmentSHOULD be performed/administered
Class IIa Benefit >> Risk
Additional studies withfocused objectives needed
IT IS REASONABLE toperformprocedure/administer treatment
Class IIb Benefit ≥ Risk
Additional studies withbroad objectives needed;
Additional registry datawould be helpful
Procedure/TreatmentMAY BE CONSIDERED
Class III Risk ≥ Benefit No additional studiesneeded
Procedure/Treatment should NOT beperformed/administered SINCE IT IS NOT HELPFUL
AND MAY BE HARMFUL
shouldis recommendedis indicatedis useful/effective/ beneficial
is reasonablecan be useful/effective/
beneficialis probably recommended or
indicated
may/might be consideredmay/might be reasonableusefulness/effectiveness is
unknown /unclear/uncertain or not well established
is not recommendedis not indicatedshould notis not useful/effective/beneficialmay be harmful
Applying Classification of Applying Classification of
Recommendations and Level of EvidenceRecommendations and Level of Evidence
Applying Classification of

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 49/57
Level A
Multiple (3-5) population risk strata evaluated
General consistency of
direction and magnitude of effect
Class I
• Recommen-dation thatprocedure or treatment isuseful/ effective
• Sufficient
evidence frommultiplerandomizedtrials or meta-analyses
Class IIa
• Recommen-dation in favor of treatment or procedure beinguseful/ effective
• Some conflicting
evidence frommultiplerandomized trialsor meta-analyses
Class IIb
• Recommen-dation’susefulness/efficacy less wellestablished
• Greater
conflictingevidence frommultiplerandomized trialsor meta-analyses
Class III
• Recommen-dation thatprocedure or treatment notuseful/effectiveand may be
harmful• Sufficient
evidence frommultiplerandomized trialsor meta-analyses
Applying Classification of
Recommendations and Level of Evidence
Applying Classification of Applying Classification of

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 50/57
Level B
Limited (2-3) population risk strata evaluated
Class I
• Recommen-dation thatprocedure or treatment isuseful/effective
• Limited evidence
from singlerandomized trialor non-randomizedstudies
Class IIa
• Recommen-dation in favor of treatment or procedure beinguseful/ effective
• Some conflicting
evidence fromsinglerandomized trialor non-randomizedstudies
Class IIb
• Recommen-dation’susefulness/efficacy less wellestablished
• Greater
conflictingevidence fromsinglerandomized trialor non-randomizedstudies
Class III
• Recommen-dation thatprocedure or treatment notuseful/effectiveand may be
harmful• Limited evidencefrom singlerandomized trialor non-randomizedstudies
pp y gpp y g
Recommendations and Level of EvidenceRecommendations and Level of Evidence
Applying Classification ofApplying Classification of

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 51/57
Applying Classification of Applying Classification of
Recommendations and Level of EvidenceRecommendations and Level of Evidence
Level C
Very limited (1-2) population risk strata evaluated
Class I
• Recommen-dation thatprocedure or treatment isuseful/ effective
• Only expert
opinion, casestudies, or standard-of-care
Class IIa
• Recommen-dation in favor of treatment or procedure beinguseful/effective
• Only diverging
expert opinion,case studies, or standard-of-care
Class IIb
• Recommen-dation’susefulness/efficacy less wellestablished
• Only diverging
expert opinion,case studies, or standard-of-care
Class III
• Recommend-ation thatprocedure or treatment notuseful/effectiveand may be
harmful• Only expertopinion, casestudies, or standard-of-care
P th t Th b i

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 52/57
Pathway to Thrombosis
B t Bl kB t Bl k

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 53/57
Oral beta-blocker therapy should beadministered promptly to those patients without
a contraindication, irrespective of concomitant
fibrinolytic therapy or performance of primary
PCI.
It is reasonable to administer intravenous beta-
blockers promptly to STEMI patients without
contraindications, especially if a
tachyarrhythmia or hypertension is present.
Beta-BlockersBeta-Blockers
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
TxTx
S f T i l f B t Bl k ThS mmar of Trials of Beta Blocker Therap

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 54/57
Phase of
Treatment
Acute
treatment
Secondary
prevention
Overall
Total No.
Patients
28,970
24,298
53,268
0.5 1 2
Relative risk (RR) of death
Beta blocker
better
RR (95% CI)
Placebobetter
0.87 (0.77-0.98)
0.77 (0.70-0.84)
0.81 (0.75-0.87)
Summary of Trials of Beta-Blocker TherapySummary of Trials of Beta-Blocker Therapy
Antman E, Braunwald E. Acute Myocardial Infarction. In:
Braunwald E, Zipes DP, Libby P, eds. Heart Disease: A
textbook of Cardiovascular Medicine, 6th ed.,Philadelphia, PA: W.B. Sanders, 2001, 1168.
C i f H i + ASA ASA Al

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 55/57
RR:Death/MI
ASA Alone68/655=10.4%
Heparin + ASA55/698=7.9%
0.1 1 10
Summary Relative Risk
0.67 (0.44-0.1.02)
Theroux
RISC
Cohen 1990
ATACS
Holdright
Gurfinkel
Comparison of Heparin + ASA vs ASA Alone
ASA indicates acetylsalicylic acid; RISC, Research on InStability in Coronary artery disease; ATACS, Antithrombotic Therapy in Acute
Company Syndromes; RR, relative risk; and MI, myocardial infarction.
Data from Oler A, Whooley MA, Oler J, et al. Adding heparin to aspirin reduces the incidence of myocardial infarction and death in
patients with unstable angina: a meta-analysis. JAMA. 1996;276:811-815. Slide reproduced with permission from Cannon CP.
Atherothrombosis slide compendium. Available at: www.theheart.org.
ESSENCE Results

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 56/57
ESSENCE Results
30%
25%
20%
15%
10%
09 13
Days After Randomization
17 215
5%
25 29
Unfractionated Heparin
Enoxaparin (Lovenox)
Death,MI
or
Recu
rren
tAngina
P = 0.02
Risk Reduction 16.2%
Adapted with permission from Cohen M, Demers C, Gurfinkel EP, et al. A comparison of low-molecular-weight
heparin with unfractionated heparin for unstable coronary artery disease. Efficacy and Safety of Subcutaneous
Enoxaparin in Non-Q-Wave Coronary Events Study Group. N Engl J Med. 1997;337:447-452. Copyright © 1997,Massachusetts Medical Society. All rights reserved.
TxTx
TIMI 11B Eno aparin sTIMI 11B Enoxaparin vs

8/8/2019 Principle MANAGEMEN ACS-Upload
http://slidepdf.com/reader/full/principle-managemen-acs-upload 57/57
D e a t h
, M I
o r
U r g
e n
t R
e v a
s c
u l
a r i z
a t i
o n
Unfractionated Heparin
Enoxaparin (Lovenox)
Days
20
16
12
8
4
2 4 6 8 10 12 140
16.7%
14.2 %
p = 0.03
Relative Risk Reduction = 15%
TIMI 11B: Enoxaparin vs.Heparin in NSTE-ACS
TIMI 11B: Enoxaparin vs.Heparin in NSTE-ACS