PRIMARY CARE COMMISSIONING COMMITTEE€¦ · Risk Register Enclosed ... justification for such a...
48
1 | Page HELD IN PUBLIC SESSION ON FRIDAY 26 MAY 2017 1:00pm – 3:00pm THE BOARD ROOM, 3 RD FLOOR, BRIERLEY HILL HEALTH AND SOCIAL CARE CENTRE, VENTURE WAY, BRIERLEY HILL, DY5 1RU QUORACY A meeting of the Committee will be quorate provided that at least 4 members are present of which: • one must be either the Chair or Vice-Chair of the Committee • one must be the Chief Finance Officer/Deputy Chief Finance Officer or Chief Nursing Officer AGENDA Time Item Attachment Presented by 1.00 pm 1 Apologies Mr S Wellings 1.00 pm 2 Declarations of Interest 2.1 To request members to disclose any interest they have, direct or indirect, in any items to be considered during the course of the meeting and to note that those members declaring an interest will not be allowed to take part in the consideration or discussion or vote on any questions relating to that item. 2.2 This meeting is being held in public and is being recorded purely to assist in the accurate production of minutes, decisions and actions. Once the minutes have been approved the recording will be destroyed. All care is taken to maintain your privacy; however, as a visitor in the public gallery, your presence may be recorded. Should you contribute to the meeting during questions from the public, you agree to being recorded. Mr S Wellings 1.00 pm 3 Questions from the Public Mr S Wellings 1.05 pm 4 Minutes of last meeting held on Friday 21 April 2016 Enclosed Mr S Wellings 1.05 pm 5 Matters Arising/Action Log Enclosed Mr S Wellings 1.10 pm 6 Contractual 6.1 Report from the Primary Care Operational Group Enclosed Mrs J Robinson 1.45 pm 7 Quality 7.1 Report from the Quality and Safety Team Enclosed Mrs C Brunt 2.05 pm 8 Finance 8.1 Finance Report Enclosed Mr P Cowley 2.25 pm 9 Performance 9.1 Performance Report Enclosed Mr R Franklin 2.45 pm 10 Risk Register Enclosed Mrs C Brunt 11 Date and Time of Next Meeting Friday 16 June 2017 1pm – 3pm The Board Room, Third Floor, Brierley Hill Health and Social Care Centre PRIMARY CARE COMMISSIONING COMMITTEE
Transcript of PRIMARY CARE COMMISSIONING COMMITTEE€¦ · Risk Register Enclosed ... justification for such a...

1 | P a g e
HELD IN PUBLIC SESSION ON FRIDAY 26 MAY 2017 1:00pm – 3:00pm THE BOARD ROOM, 3RD FLOOR, BRIERLEY HILL HEALTH AND SOCIAL CARE CENTRE,
VENTURE WAY, BRIERLEY HILL, DY5 1RU QUORACY A meeting of the Committee will be quorate provided that at least 4 members are present of which: • one must be either the Chair or Vice-Chair of the Committee • one must be the Chief Finance Officer/Deputy Chief Finance Officer or Chief Nursing Officer
AGENDA
Time Item Attachment Presented by
1.00 pm 1 Apologies Mr S Wellings 1.00 pm 2
Declarations of Interest 2.1 To request members to disclose any interest they have, direct or indirect, in any items to be considered during the course of the meeting and to note that those members declaring an interest will not be allowed to take part in the consideration or discussion or vote on any questions relating to that item. 2.2 This meeting is being held in public and is being recorded purely to assist in the accurate production of minutes, decisions and actions. Once the minutes have been approved the recording will be destroyed. All care is taken to maintain your privacy; however, as a visitor in the public gallery, your presence may be recorded. Should you contribute to the meeting during questions from the public, you agree to being recorded.
Mr S Wellings
1.00 pm 3 Questions from the Public Mr S Wellings
1.05 pm 4 Minutes of last meeting held on Friday 21 April 2016 Enclosed Mr S Wellings
1.05 pm 5 Matters Arising/Action Log Enclosed Mr S Wellings
1.10 pm 6 Contractual 6.1 Report from the Primary Care Operational Group
Enclosed
Mrs J Robinson
1.45 pm 7 Quality
7.1 Report from the Quality and Safety Team
Enclosed
Mrs C Brunt
2.05 pm 8
Finance 8.1 Finance Report
Enclosed
Mr P Cowley
2.25 pm 9
Performance 9.1 Performance Report
Enclosed
Mr R Franklin
2.45 pm
10
Risk Register
Enclosed
Mrs C Brunt
11
Date and Time of Next Meeting Friday 16 June 2017 1pm – 3pm The Board Room, Third Floor, Brierley Hill Health and Social Care Centre
PRIMARY CARE COMMISSIONING COMMITTEE

1 | P a g e
PRIMARY CARE COMMISSIONING COMMITTEE
MINUTES OF THE MEETING HELD IN PUBLIC ON FRIDAY 21 APRIL 2017 THE BOARD ROOM, 3RD FLOOR, BRIERLEY HILL HEALTH AND SOCIAL CARE CENTRE,
VENTURE WAY, BRIERLEY HILL, DY5 1RU
Quorum: A meeting of the Committee will be quorate provided that at least four members are present of which one must be either the Chair or Vice Chair of the Committee and one must be the Chief Finance Officer/Deputy Chief Finance or Chief Nursing Officer. ATTENDEES: Members Mr S Wellings Non-Executive Director for Governance, Dudley CCG (Chair) Ms S Johnson Deputy Chief Finance Officer, Dudley CCG Mrs C Brunt Chief Nurse, Dudley CCG Dr D Pitches Consultant in Public Health, Dudley MBC Dr C Handy Non-Executive Director for Quality & Safety In Attendance Mrs J Robinson Primary Care Contracts Manager, Dudley CCG Ms J Emery Chief Executive, Healthwatch Dudley Dr T Horsburgh Clinical Executive for Primary Care, Dudley CCG Mrs J Taylor Commissioning Manager for Primary Care, Dudley CCG Mr P Cowley Senior Finance Manager, Dudley CCG Mrs J Jasper Lay Member for Patient and Public Involvement, Dudley CCG Mr D Stenson Patient Opportunity Panel Representative Mr B Dhami Senior Contract Manager, NHS England (West Midlands) Mr T Thomik Dudley LPC Representative Ms K Hodgson Engagement Officer, Dudley CCG Minute Taker: Mrs R Gretton Personal Assistant, Dudley CCG 1. APOLOGIES FOR ABSENCE Apologies were received from: Mr M Hartland, Chief Operating and Finance Officer, Dudley CCG Mrs E Smith, Governance Support Manager, Dudley CCG Mr D King, Director of Membership Development and Primary Care, Dudley CCG Mrs L Broster, Director of Communications and Public Insight, Dudley CCG Mrs A Nicholls, Interim Deputy Head of Commissioning (Primary Care) NHS England (West Midlands) Dr V K Mittal, GP Representative Miss T Jeavons, Primary Care Contracts Support Officer, Dudley CCG 2. DECLARATIONS OF INTEREST To request members to disclose any interest they have, direct or indirect, in any items to be considered during the course of the meeting and to note that those members declaring an interest would not be allowed to take part in the consideration or discussion or vote on any questions relating to that item:

2 | P a g e
GP members declared a standing interest, particularly with regards to the contractual items, although they do not have a voting position on the Committee. Mrs Jasper declared her standing interest as NED for Sandwell and West Birmingham CCG. Mr Stenson declared his standing interest as an Associate Non-Executive Director for Black Country Partnership Foundation Trust. 3. QUESTIONS FROM THE PUBLIC Mr Wellings had received no questions from the public. 4. MINUTES FROM THE PREVIOUS MEETING HELD ON 17 MARCH 2017 The minutes of the Committee held on 17 March 2017 were accepted as a true and accurate record, subject to the following amendments on page 3, item 7; the word ‘victim’ is replaced with ‘risk factors’, paragraph 6 and 7 are moved under the heading of ‘CQC Inspections’. Page 4; the resolved item is amended to reflect ‘the Committee noted the report for assurance’. 5. MATTERS ARISING/ACTION LOG MATTER ARISING The action log was discussed and updated accordingly with the following points noted: PCCC/JAN/2017/10.0 This item was agreed to be deferred until August 2017 PCCC/MAR/2017/7.1 This item was noted to be on the agenda PCCC/MAR/2017/7.1(b) This item was agreed to be deferred to June 2017 PCCC/MAR/2017/10.0 Several conversations had taken place, where it was indicated that practices
had difficulty in articulating themselves in explaining and demonstrating achievement under the Dudley Quality Outcomes for Health Framework. Support is being given to those practices to help them to articulate how the framework actually replaces and contributes to improved outcomes for patients, in addition to a dashboard that practices can access to see benchmarks
PCCC/MAR/2017/11.0 Information had been requested and would be provided to the Committee in
May 2017 6. CONTRACTUAL 6.1 REPORT FROM THE PRIMARY CARE OPERATIONAL GROUP Mrs Robinson spoke to this item to update the Committee on the issues discussed at the Primary Care Operational Group (PCOG) held on 5 April 2017. The Committee was informed that no issues had arisen requiring any breach notifications. The main conversations to take place at PCOG was in regard to Bilston Street Surgery and the closure of the practice on 31 May 2017. It was reported that correspondence had been sent to all registered patients in addition to ‘drop in’ sessions at the practice to notify of the closure and provide details of how to re-register. It was noted that the CCG had done all possible at this stage to identify all vulnerable patients registered at the practice. A meeting is

3 | P a g e
due to take place next week at the practice, with attendance from CCG and NHS England representatives to reinforce the message that the practice need to identify those remaining vulnerable and at risk patients, which remains a main concern of the CCG. Four neighbouring practices were identified to have capacity to register new patients, but unfortunately it was reported that the one practice in particular that does not have the capacity had received a large number of patients requesting to register with them. Support had been requested by the practice and the CCG is keen to offer a similar package to all practices, along with the new registrations uplift. The Committee noted that the closure had increased the pressure on neighbouring practices, in addition to teams within the CCG in dealing with the process. The possibility of a request for a list closure was reported to be likely should the influx of new patients continue at the concerned practice. It was discussed for the practice to undertake a risk analysis, to include a threshold assessment to which a cap would need to be applied, but also to understand the practices justification for such a request. Resolved:
1) The Committee noted the actions of the Primary Care Operational Group for assurance 7. QUALITY 7.1 REPORT FROM THE QUALITY AND SAFETY TEAM Mrs Brunt spoke to this item to highlight key points within the report. Serious Incidents (SIs) The Committee was informed that two SI’s remain open in relation to information governance and secondly an unexpected death which is under investigation. The CCG offers support for those investigations and it is hoped that going into the MCP practices will have the skills and be able to undertake more independent Root Cause Analysis within their own resources. Resolved:
1) The Committee noted the report for assurance
8. FINANCE
8.1 FINANCE REPORT Mr Cowley spoke to this item to provide an overview of financial performance against budgets delegated to the Committee. The Committee was informed that the accounts and figures are not yet finalised due to the end of the financial year and these will be finalised next week. However, it was reported from the date of this report there had been no changes and no further changes were expected. The reported financial position is expected to be a break even position against co-commissioning aspects of the budget, with an underspend of £1,000 against the delegated primary care budget. An underspend of £40,000 is reported against the core CCG development budget for reasons outlined in previous months reports to the Committee. One change in budget was reported to the Committee from that reported at month 11, which noted a technical change to the allocation received for the GP Resilience Programme. This had been moved to another area following guidance from NHS England.
4 | P a g e
An error was stated within the report in the section ‘2017/18 Primary Care Budgets Overview’, Co-Commissioned Primary Care figure £39,863,000. The correct figure was noted to be within the table at £40,596,000, a 1.8% increase from 2016/17. The Committee was informed that the final page of the report contained the additional budgets that are expected to be allocated to the CCG by NHS England in line with the GP Forward View. Resolved:
1) The Committee noted the report for assurance 8.2 HEALTH INFRASTRUCTURE STRATEGY IMPLICATIONS FOR PRIMARY CARE Mr Cowley spoke to this item to outline the implications of the Health Infrastructure Strategy for the consideration of applications for premises development under the GMS Premises Costs Directions. The Committee was informed that the Health Infrastructure Strategy (HIS) was approved by the CCG Board in March 2016 and called for the future premises direction of the CCG for primary care and community services to be based around the provision of services at scale. Outlined within the report are a national approval framework and also a proposed additional local framework. It was clarified that any decisions following applications made by practices would be taken by the Committee, following discussion at the Primary Care Operational Group. In view of the potential implications to practices, a further consultation of the framework was recommended to be taken to fully enlighten of the specifics with the membership prior to approval by the Committee. A further report was requested following consultation in June 2017.
ACTION: MR COWLEY The Committee requested clarification around condition B, especially when published for wider consultation. It was reported back in 2014 only Lion Health was a condition A site, fulfilling all regulations. Most premises in Dudley are at condition B, which complies with statutory responsibility. Key sites were noted to have been identified as part of the Estates Strategy as sites that support the MCP model where long term financial commitments had been made. The Committee was informed that the figure of 15,000 within the report, again from the Estates Strategy, had been the level at which it is thought possible to wrap significant community services around single populations in a practice at a level that is cost effective for a community service provider. Resolved:
1) The Committee noted the report and considered the principles within the report, with a recommendation for further consultation
2) The Committee agreed that a further report following such consultation be brought back in June 2017
9. PRIMARY MEDICAL SERVICES – NEW CONTRACTUAL FRAMEWORK BUSINESS RULES Mrs Taylor spoke to this item to present to the Committee the final draft business rules for the ‘Dudley Quality Outcomes for Health’ (DQOFH) contract 2017/18 for ratification. The DQOFH was explained to be a local outcomes based framework, developed as an alternative to the national Quality Outcomes Framework (QoF). The Committee was informed that phase three had now been entered, with 42 of 46 practices signed up and delivering the DQOFH framework. Three additional practices had signed up this year and Bilston Street Surgery had not been offered the DQOFH or QOF framework due to the impending closure of the practice on 31 May 2017.
5 | P a g e
It was reported that a dashboard had been developed allowing practices to see their achievement against the DQOFH framework, which is updated on a monthly basis. The included business rules were reported to have been updated to reflect the changes to indicators, following a consultation process with the relevant clinical leads and are presented to the Committee for ratification and approval. It was reported that any feedback received by practice members is welcomed and fed back into the steering group but engagement with patients had proved difficult in the evaluation of the framework. Following question by the Committee, the three practices not signed up to the DQOFH framework were reported to be Crestfield Medical Practice, Central Clinic and Meadowbrook Medical Practice. Various reasons were explained to be the reasoning for non-sign up to the framework with the GP at Crestfield looking at retirement in the next twelve months, Meadowbrook Medical Practice having issues around access and wish to remain closed for one half day a week. Central Clinic had posed various questions to which responses had been supplied and continued engagement is taking place. Thanks and congratulations from the Committee were given to all involved in the DQOFH framework work. Resolved:
1) The Committee approved the final draft business rules for the DQOFH framework contract 2017/18
10. GP FORWARD VIEW STAGE 2 FEEDBACK Mrs Taylor spoke to this item to update the Committee on the GP Forward View Stage 2 Plan submission to NHS England. A small number of areas were noted to be rated amber/green and following a further discussion with NHS England on 11 March 2017 to discuss plans, the NHSE Local Area Team were not in agreement with the original assessment and thought that all sections should be rated green. Further clarification was requested in the area of leadership and governance and how this aligned to the STP. This had subsequently been clarified and reflected in the next item around primary care structure. Preliminary assurance had been received for this that the rating is now green overall though ratification was still awaited. Full assurance would be brought to the Committee in May. Resolved:
1) The Committee noted the report for assurance 11. PRACTICE ENGAGEMENT SCHEME Mrs Taylor spoke to this item to present to the Committee the final draft Practice Engagement Scheme 2017/18 for ratification. The Committee was informed that this scheme is offered to all practices to encourage their continued engagement with the commissioning processes. Part A was reported to be in regard to attendance at CCG Member and locality meetings, Part B in regard to the Prescribing Incentive Scheme, to which there had been some slight amendments made compared to last year’s scheme by the Prescribing Team. Part C relates to adherence to participation in different schemes, those of which are listed within the report. It was noted that part A should also require representatives to cascade learning back to the practices. Resolved:
1) The Committee noted the report and approved the draft Practice Engagement Scheme 2017/18 subject to the amendment above

6 | P a g e
12. PRIMARY CARE ORGANISATIONAL STRUCTURE Mrs Taylor spoke to this item to update the Committee on the proposed organisational structure that reflects the separation of primary care commissioning and development and primary care development of the MCP. The Primary Care Development Group (PCDG) will report to the Primary Care Strategy Group (PCSG) that will see the overarching assurance around the GPFV. It was reported that the PCDG would concentrate on development schemes for primary care and the PCSG would look at the overarching items, which would include reporting of the workforce, IT Strategy and estates work. Both groups will feed into the Committee. In addition, across the Black Country STP, primary care leads are now meeting to explore opportunities for collaboration across the STP. Next steps were reported to be development of Terms of Reference for the PCDG and PCSG for presentation to the Committee in May.
ACTION: MRS TAYLOR It was noted that the line between the GP Collaborative and Finance & Performance Committee should be that of a ‘formally reports to’ one. Resolved:
1) The Committee noted the report for assurance 2) The Committee approved the proposed structure subject to the Terms of Reference for the
PCDG and PCSG being presented to the Committee for approval 13. SUPPORTING PROFESSIONAL DECISIONS Dr Horsburgh spoke to this item to present a proposal to the Committee on the development of a support mechanism for clinicians facing challenging patients and complex scenarios. The Committee was informed that there is an intention to establish a panel as a conduit for clinicians who have difficult situations that arise with a patient. The Committee supported the idea in principle but would like to see further detail of the membership and how that would work.
ACTION: DR HORSBURGH Resolved:
1) The Committee received the report and supported the idea in principle
14 PATIENT PARTICIPATION GROUP UPDATE Ms Hodsgon spoke to this item to update the Committee on the current situation and future plans regarding Patient Participation Groups (PPGs). The Committee was informed that participants from 18 practices attended a PPG event on 1 March 2017, which was noted to be a high proportion and a successful event. Subsequently a further event was agreed and would take place in 6 months’ time. The Committee noted the importance of PPGs and the involvement of patients in their care being critical with the expectation that there is a fully functioning PPG that is supported by their practice. It was requested that in two months’ time, a list of practices where there is concern in regard to their PPG is presented to the Committee
ACTION: MS HODGSON
7 | P a g e
Resolved: 1) The Committee requested a list of practices where there is concern in regard to their PPG 2) The Committee agreed the recommendation that the Communications & Public Insight team
continue to support PPGs and practices 15. DATE AND TIME OF NEXT MEETING Friday 26 May 2017 1 – 3pm The Board Room, Third Floor, Brierley Hill Health & Social Care Centre MINUTES ACCEPTED AS A TRUE AND CORRECT RECORD Name Title
Signed Date
1 | P a g e
PRIMARY CARE COMMISSIONING COMMITTEE
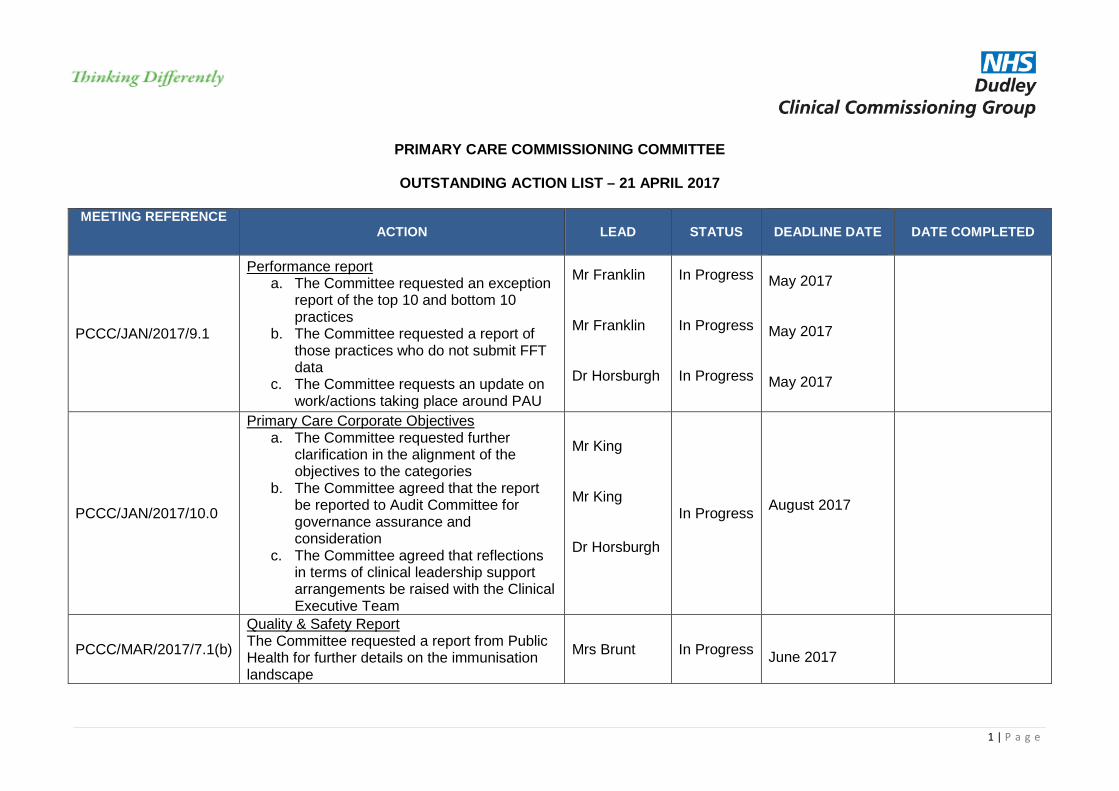
OUTSTANDING ACTION LIST – 21 APRIL 2017
MEETING REFERENCE
ACTION LEAD STATUS
DEADLINE DATE
DATE COMPLETED
PCCC/JAN/2017/9.1
Performance report a. The Committee requested an exception
report of the top 10 and bottom 10 practices
b. The Committee requested a report of those practices who do not submit FFT data
c. The Committee requests an update on work/actions taking place around PAU
Mr Franklin Mr Franklin Dr Horsburgh
In Progress In Progress In Progress
May 2017 May 2017 May 2017
PCCC/JAN/2017/10.0
Primary Care Corporate Objectives a. The Committee requested further
clarification in the alignment of the objectives to the categories
b. The Committee agreed that the report be reported to Audit Committee for governance assurance and consideration
c. The Committee agreed that reflections in terms of clinical leadership support arrangements be raised with the Clinical Executive Team
Mr King Mr King Dr Horsburgh
In Progress
August 2017
PCCC/MAR/2017/7.1(b)
Quality & Safety Report The Committee requested a report from Public Health for further details on the immunisation landscape
Mrs Brunt In Progress
June 2017
2 | P a g e
MEETING REFERENCE ACTION LEAD STATUS
DEADLINE DATE
DATE COMPLETED
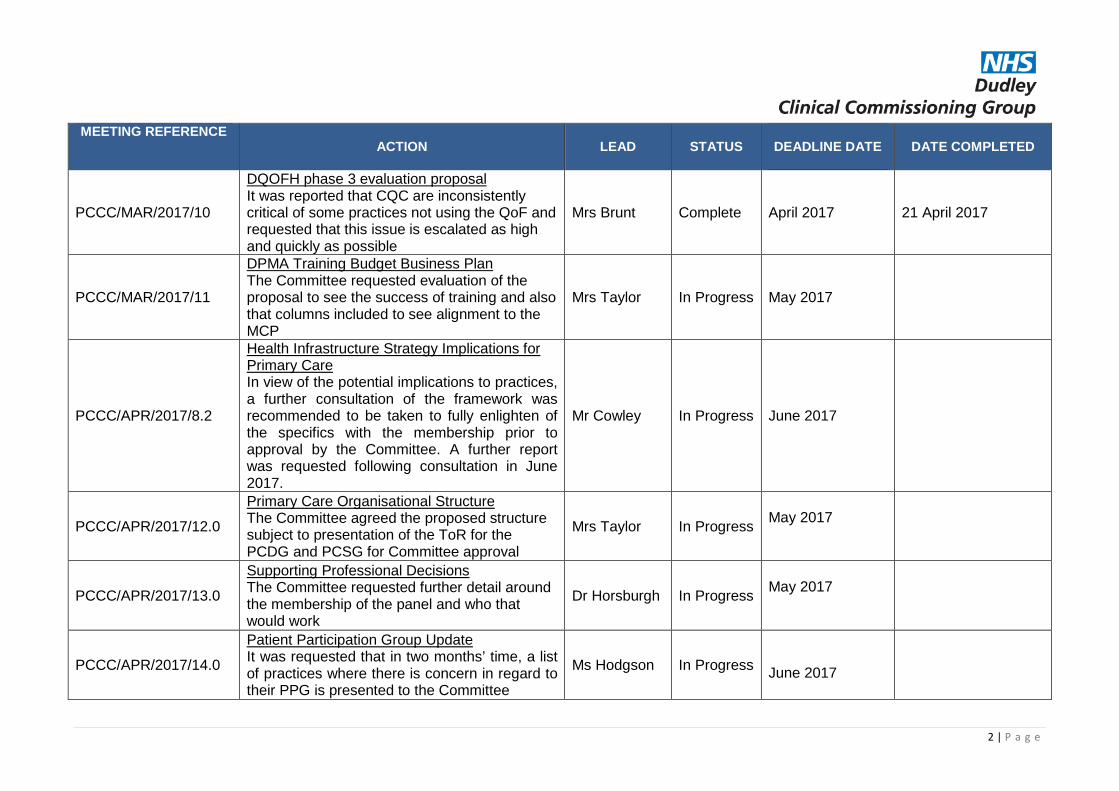
PCCC/MAR/2017/10
DQOFH phase 3 evaluation proposal It was reported that CQC are inconsistently critical of some practices not using the QoF and requested that this issue is escalated as high and quickly as possible
Mrs Brunt Complete
April 2017 21 April 2017
PCCC/MAR/2017/11
DPMA Training Budget Business Plan The Committee requested evaluation of the proposal to see the success of training and also that columns included to see alignment to the MCP
Mrs Taylor In Progress
May 2017
PCCC/APR/2017/8.2
Health Infrastructure Strategy Implications for Primary Care In view of the potential implications to practices, a further consultation of the framework was recommended to be taken to fully enlighten of the specifics with the membership prior to approval by the Committee. A further report was requested following consultation in June 2017.
Mr Cowley In Progress
June 2017
PCCC/APR/2017/12.0
Primary Care Organisational Structure The Committee agreed the proposed structure subject to presentation of the ToR for the PCDG and PCSG for Committee approval
Mrs Taylor In Progress
May 2017
PCCC/APR/2017/13.0
Supporting Professional Decisions The Committee requested further detail around the membership of the panel and who that would work
Dr Horsburgh In Progress
May 2017
PCCC/APR/2017/14.0
Patient Participation Group Update It was requested that in two months’ time, a list of practices where there is concern in regard to their PPG is presented to the Committee
Ms Hodgson In Progress
June 2017

3 | P a g e

1 | P a g e
PRIMARY CARE COMMISSIONING COMMITTEE
Date of Committee: 26 May 2017 Report: Update from the Primary Care Operational Group
Agenda Item: 6.1
TITLE OF REPORT: Update from the Primary Care Operational Group
PURPOSE OF REPORT: To update the Committee following the Primary Care Operational Group meeting held on 3 May 2017
AUTHOR OF REPORT: Mrs J Robinson, Primary Care Contracts Manager
MANAGEMENT LEAD: Mrs C Brunt, Chief Nurse CLINICAL LEAD: Dr T Horsburgh, Clinical Executive for Primary Care
KEY POINTS:
• The group provides assurance that there are no contractual
breaches to be issued for any Dudley practice • The group considered and recommends the contractual changes
set out below in the recommendations • The group considered the quality and safety issues that are set
out in the quality and safety report • The group received an update in respect of the Bilston Street
Surgery Closure
RECOMMENDATION:
The Committee is asked to:
• Note the actions of the primary care operational group for assurance
• Approve the contractual changes recommended by the group as follows:
• 24 hour retirement of one partner from Lower Gornal Medical Practice with effect from 1 September 2017
FINANCIAL IMPLICATIONS: Not applicable
WHAT ENGAGEMENT HAS TAKEN PLACE: Not applicable
ACTION REQUIRED: Decision Approval Assurance
2 | P a g e
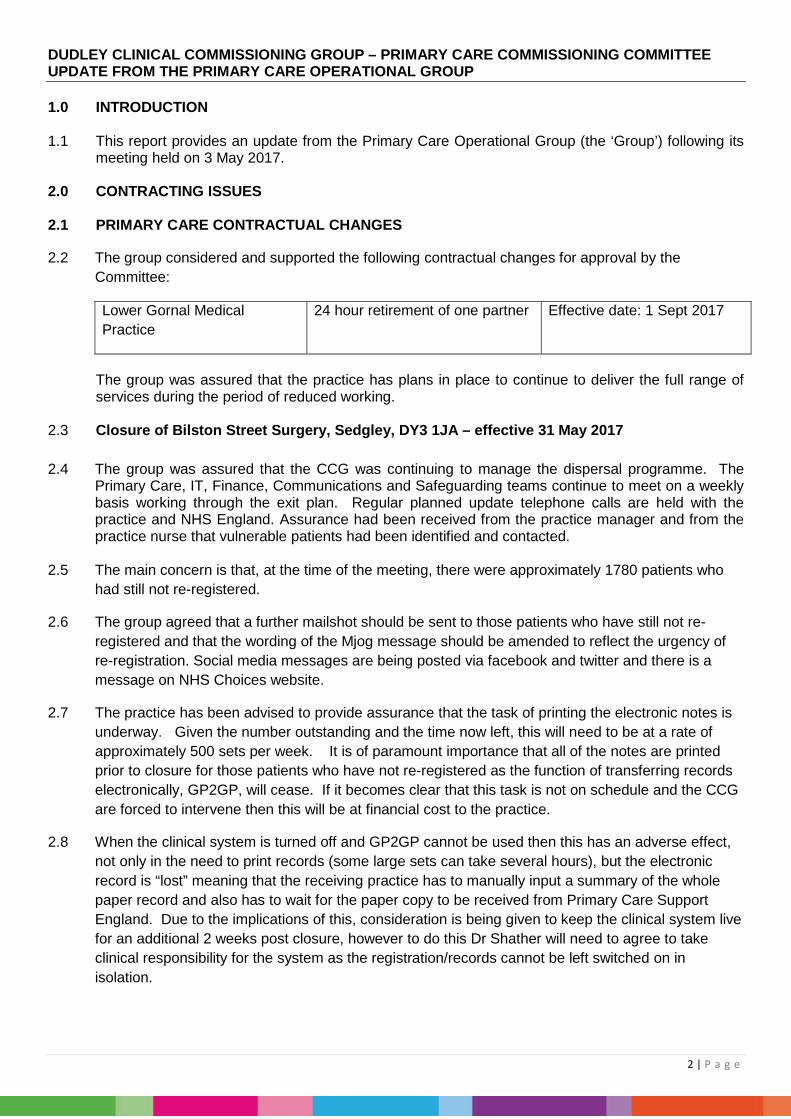
DUDLEY CLINICAL COMMISSIONING GROUP – PRIMARY CARE COMMISSIONING COMMITTEE UPDATE FROM THE PRIMARY CARE OPERATIONAL GROUP 1.0 INTRODUCTION
1.1 This report provides an update from the Primary Care Operational Group (the ‘Group’) following its
meeting held on 3 May 2017.
2.0 CONTRACTING ISSUES
2.1 PRIMARY CARE CONTRACTUAL CHANGES
2.2 The group considered and supported the following contractual changes for approval by the Committee:
Lower Gornal Medical Practice
24 hour retirement of one partner Effective date: 1 Sept 2017
The group was assured that the practice has plans in place to continue to deliver the full range of services during the period of reduced working.
2.3 Closure of Bilston Street Surgery, Sedgley, DY3 1JA – effective 31 May 2017 2.4 The group was assured that the CCG was continuing to manage the dispersal programme. The
Primary Care, IT, Finance, Communications and Safeguarding teams continue to meet on a weekly basis working through the exit plan. Regular planned update telephone calls are held with the practice and NHS England. Assurance had been received from the practice manager and from the practice nurse that vulnerable patients had been identified and contacted.
2.5 The main concern is that, at the time of the meeting, there were approximately 1780 patients who
had still not re-registered.
2.6 The group agreed that a further mailshot should be sent to those patients who have still not re-registered and that the wording of the Mjog message should be amended to reflect the urgency of re-registration. Social media messages are being posted via facebook and twitter and there is a message on NHS Choices website.
2.7 The practice has been advised to provide assurance that the task of printing the electronic notes is underway. Given the number outstanding and the time now left, this will need to be at a rate of approximately 500 sets per week. It is of paramount importance that all of the notes are printed prior to closure for those patients who have not re-registered as the function of transferring records electronically, GP2GP, will cease. If it becomes clear that this task is not on schedule and the CCG are forced to intervene then this will be at financial cost to the practice.
2.8 When the clinical system is turned off and GP2GP cannot be used then this has an adverse effect, not only in the need to print records (some large sets can take several hours), but the electronic record is “lost” meaning that the receiving practice has to manually input a summary of the whole paper record and also has to wait for the paper copy to be received from Primary Care Support England. Due to the implications of this, consideration is being given to keep the clinical system live for an additional 2 weeks post closure, however to do this Dr Shather will need to agree to take clinical responsibility for the system as the registration/records cannot be left switched on in isolation.
3 | P a g e
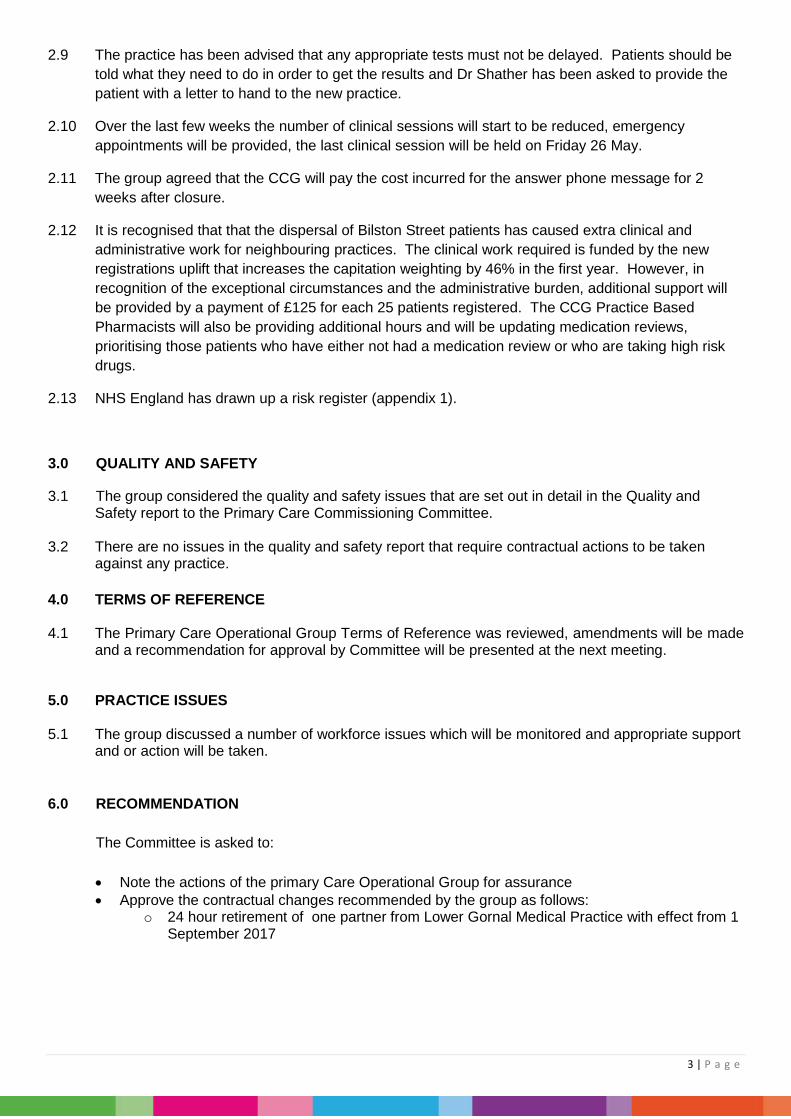
2.9 The practice has been advised that any appropriate tests must not be delayed. Patients should be told what they need to do in order to get the results and Dr Shather has been asked to provide the patient with a letter to hand to the new practice.
2.10 Over the last few weeks the number of clinical sessions will start to be reduced, emergency appointments will be provided, the last clinical session will be held on Friday 26 May.
2.11 The group agreed that the CCG will pay the cost incurred for the answer phone message for 2 weeks after closure.
2.12 It is recognised that that the dispersal of Bilston Street patients has caused extra clinical and administrative work for neighbouring practices. The clinical work required is funded by the new registrations uplift that increases the capitation weighting by 46% in the first year. However, in recognition of the exceptional circumstances and the administrative burden, additional support will be provided by a payment of £125 for each 25 patients registered. The CCG Practice Based Pharmacists will also be providing additional hours and will be updating medication reviews, prioritising those patients who have either not had a medication review or who are taking high risk drugs.
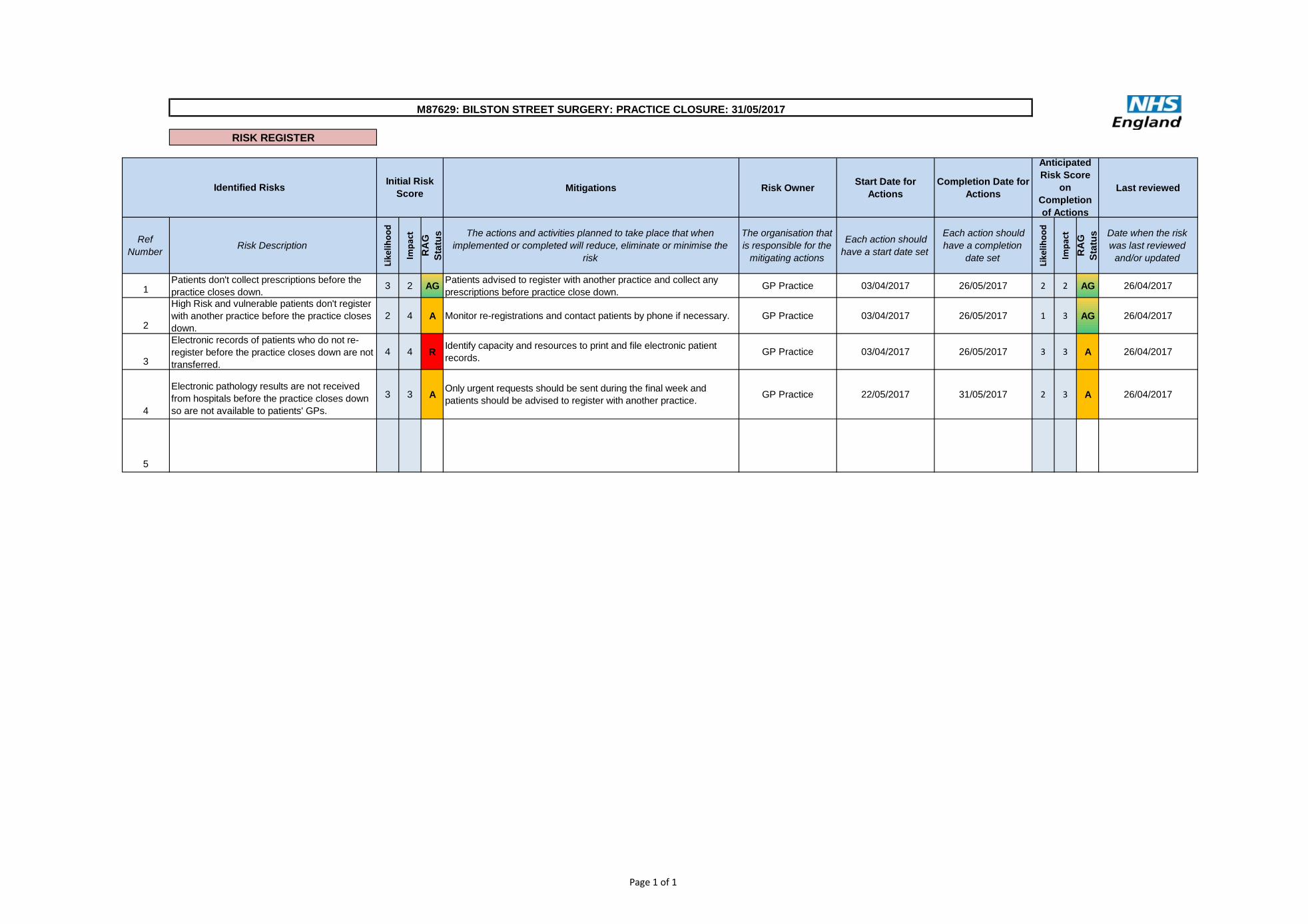
2.13 NHS England has drawn up a risk register (appendix 1).
3.0 QUALITY AND SAFETY
3.1 The group considered the quality and safety issues that are set out in detail in the Quality and Safety report to the Primary Care Commissioning Committee.
3.2 There are no issues in the quality and safety report that require contractual actions to be taken
against any practice. 4.0 TERMS OF REFERENCE
4.1 The Primary Care Operational Group Terms of Reference was reviewed, amendments will be made
and a recommendation for approval by Committee will be presented at the next meeting.
5.0 PRACTICE ISSUES 5.1 The group discussed a number of workforce issues which will be monitored and appropriate support
and or action will be taken.
6.0 RECOMMENDATION
The Committee is asked to: • Note the actions of the primary Care Operational Group for assurance • Approve the contractual changes recommended by the group as follows:
o 24 hour retirement of one partner from Lower Gornal Medical Practice with effect from 1 September 2017
Page 1 of 1
RISK REGISTER
Mitigations Risk Owner Start Date for Actions
Completion Date for Actions Last reviewed
Ref Number Risk Description
Like
lihoo
d
Impa
ct
RA
G
Stat
us The actions and activities planned to take place that when
implemented or completed will reduce, eliminate or minimise the risk
The organisation that is responsible for the
mitigating actions
Each action should have a start date set
Each action should have a completion
date set Like
lihoo
d
Impa
ct
RA
G
Stat
us Date when the risk
was last reviewed and/or updated
1Patients don't collect prescriptions before the practice closes down. 3 2 AG Patients advised to register with another practice and collect any
prescriptions before practice close down. GP Practice 03/04/2017 26/05/2017 2 2 AG 26/04/2017
2
High Risk and vulnerable patients don't register with another practice before the practice closes down.
2 4 A Monitor re-registrations and contact patients by phone if necessary. GP Practice 03/04/2017 26/05/2017 1 3 AG 26/04/2017
3
Electronic records of patients who do not re-register before the practice closes down are not transferred.
4 4 R Identify capacity and resources to print and file electronic patient records. GP Practice 03/04/2017 26/05/2017 3 3 A 26/04/2017
4
Electronic pathology results are not received from hospitals before the practice closes down so are not available to patients' GPs.
3 3 A Only urgent requests should be sent during the final week and patients should be advised to register with another practice. GP Practice 22/05/2017 31/05/2017 2 3 A 26/04/2017
5
M87629: BILSTON STREET SURGERY: PRACTICE CLOSURE: 31/05/2017
Identified Risks Initial Risk Score
Anticipated Risk Score
on Completion of Actions
Page 1 of 5
DUDLEY CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE
Date of Meeting: 26 May 2017 Report: Quality & Safety Report
Agenda Item No: 7.1
TITLE OF REPORT: Quality and Safety Report
PURPOSE OF REPORT: To provide on-going assurance to the Primary Care Commissioning Committee (PCCC) regarding quality and safety in accordance with the CCG’s statutory duties
AUTHOR(s) OF REPORT: Mr J Young, Quality and Patient Safety Manager
MANAGEMENT LEAD: Mrs C Brunt, Chief Nurse
CLINICAL LEAD: Dr Ruth Edwards, Clinical Lead, Quality & Safety
KEY POINTS:
• Four CQC reports have been published since the last report
• One practice has been rated as inadequate after a follow-up inspection
• One follow-up desktop CQC inspection has been completed
RECOMMENDATION:
The Primary Care Commissioning Committee is asked to:
• Note this report for assurance
FINANCIAL IMPLICATIONS:
None to report
WHAT ENGAGEMENT HAS TAKEN PLACE: N/A
ACTION REQUIRED: Assurance
Page 2 of 5
DUDLEY CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE – 26 MAY 2017 QUALITY & SAFETY REPORT
1 Introduction
1.1 A primary care quality and safety report is provided to the CCG Quality and Safety Committee (QSC) and CCG Primary Care Operational Group (PCOG) monthly. This report is a material summation of the report submitted to the latest QSC plus any additional information identified after the QSC report was finalised.
1.2 The PCCC will be briefed on any contemporaneous matters of consequence arising after submission of this report.
2 CQC Inspections
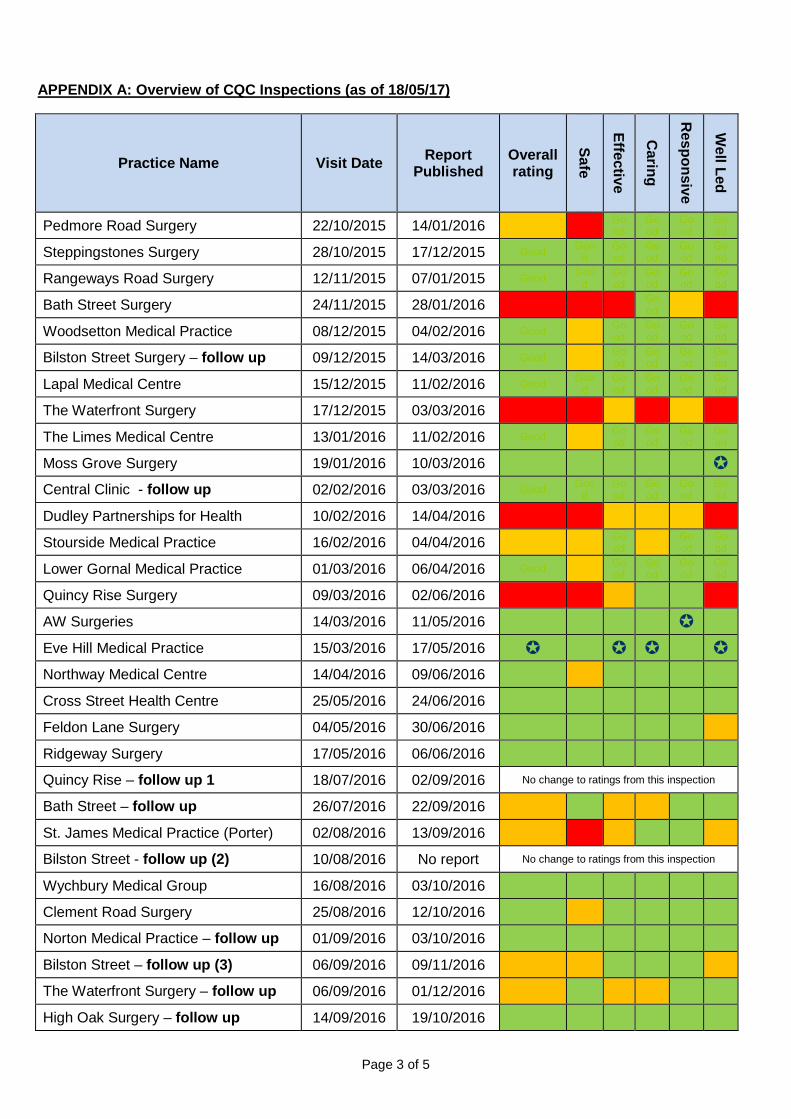
2.1 Appendix A shows the latest status of CQC inspections across Dudley.
2.2 Clement Road Surgery has been subject to a desktop follow-up review following their previous requires improvement rating for the safe domain.
2.3 Northway Medical Centre has been rated as good overall and for all domains following their previous requires improvement rating for the safe domain.
2.4 Feldon Lane Surgery has been rated as good overall and for all domains following a previous requires improvement rating for the well-led domain.
2.5 Three Villages Surgery has been rated as good overall and for all domains except safe which has been rated as requires improvement.
2.6 Stourside Medical Practice (reported as Halesowen Health Centre) has been rated as inadequate overall and for the safe and well-led domains, and requires improvement for the effective domain. The CCG are meeting with the practice w/b 22/05/17 to discuss the report and provide support for addressing the areas of concern raised.
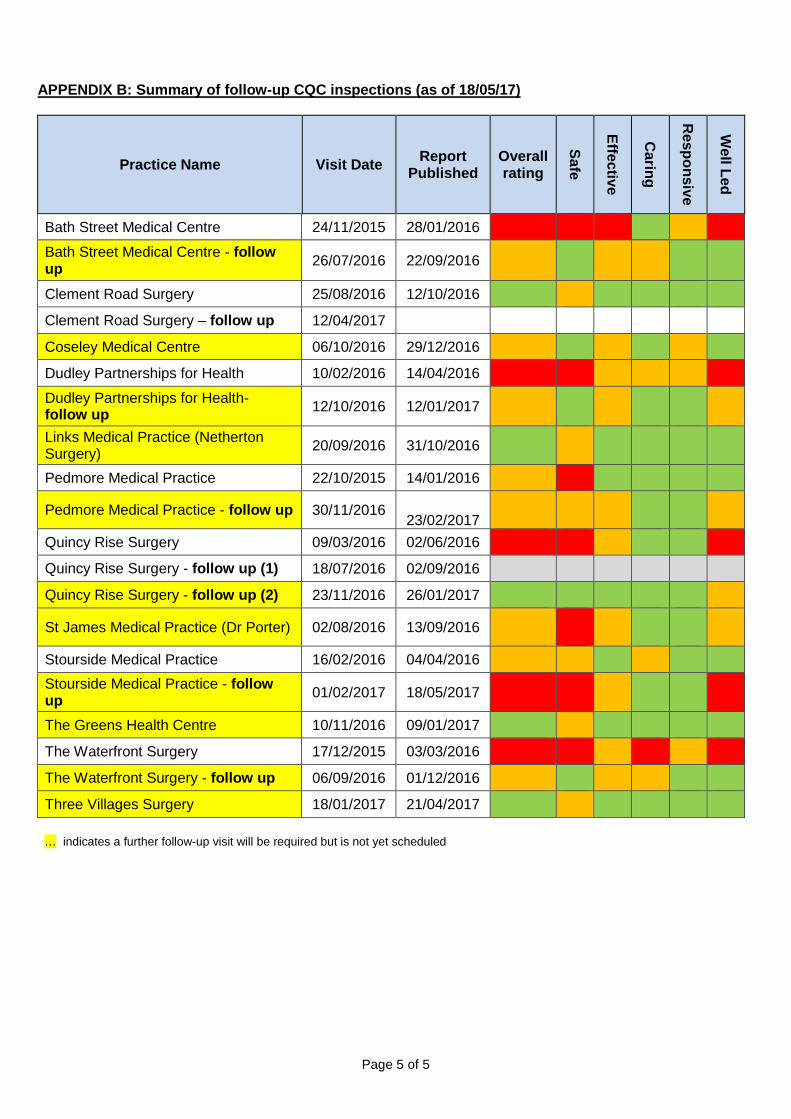
2.7 Appendix B shows all 12 practices who will require follow up visits from CQC i.e. where they have not been rated as good for all domains.
3 Serious Incidents (SIs)
3.1 Currently, there is one open SI. Support is continuing to be provided by the Q&S team to ensure robust RCAs are carried out and documented.
4 Infection Prevention & Control (IPC)
4.1 Dates for five of the IPC audits scheduled for 2017/18 have been confirmed with the first one due to take place w/b 22/05/17. Dates are currently being agreed for the remaining practices.
5 Service Developments
5.1 Datix – Datix is now being used within the CCG Quality & Safety team, in parallel with current systems to iron out any final issues. A follow-up meeting with one practice has been arranged with a view to using the live system. Meetings are being arranged with other practices to discuss wider use and gain further feedback on improving the system.
5.2 Primary Care Assurance Tool (PCAT) – further discussions have been held to define the reporting
format with the aim that future PCCC Q&S reporting will be based on PCAT data.
Page 3 of 5
APPENDIX A: Overview of CQC Inspections (as of 18/05/17)
Practice Name Visit Date Report Published
Overall rating
Safe
Effective
Caring
Responsive
Well Led
Pedmore Road Surgery 22/10/2015 14/01/2016 RI Inad Good
Good
Good
Good
Steppingstones Surgery 28/10/2015 17/12/2015 Good Good
Good
Good
Good
Good
Rangeways Road Surgery 12/11/2015 07/01/2015 Good Good
Good
Good
Good
Good
Bath Street Surgery 24/11/2015 28/01/2016 Inad Inad Inad
Good RI Ina
d
Woodsetton Medical Practice 08/12/2015 04/02/2016 Good RI Good
Good
Good
Good
Bilston Street Surgery – follow up 09/12/2015 14/03/2016 Good RI Good
Good
Good
Good
Lapal Medical Centre 15/12/2015 11/02/2016 Good Good
Good
Good
Good
Good
The Waterfront Surgery 17/12/2015 03/03/2016 Inad Inad RI Inad RI Ina
d
The Limes Medical Centre 13/01/2016 11/02/2016 Good RI Good
Good
Good
Good
Moss Grove Surgery 19/01/2016 10/03/2016 Central Clinic - follow up 02/02/2016 03/03/2016 Good Goo
d Good
Good
Good
Good
Dudley Partnerships for Health 10/02/2016 14/04/2016 Inad Inad RI RI RI Inad
Stourside Medical Practice 16/02/2016 04/04/2016 RI RI Good RI Go
od Good
Lower Gornal Medical Practice 01/03/2016 06/04/2016 Good RI Good
Good
Good
Good
Quincy Rise Surgery 09/03/2016 02/06/2016
AW Surgeries 14/03/2016 11/05/2016 Eve Hill Medical Practice 15/03/2016 17/05/2016 Northway Medical Centre 14/04/2016 09/06/2016 Cross Street Health Centre 25/05/2016 24/06/2016 Feldon Lane Surgery 04/05/2016 30/06/2016
Ridgeway Surgery 17/05/2016 06/06/2016
Quincy Rise – follow up 1 18/07/2016 02/09/2016 No change to ratings from this inspection
Bath Street – follow up 26/07/2016 22/09/2016
St. James Medical Practice (Porter) 02/08/2016 13/09/2016
Bilston Street - follow up (2) 10/08/2016 No report No change to ratings from this inspection
Wychbury Medical Group 16/08/2016 03/10/2016
Clement Road Surgery 25/08/2016 12/10/2016
Norton Medical Practice – follow up 01/09/2016 03/10/2016
Bilston Street – follow up (3) 06/09/2016 09/11/2016
The Waterfront Surgery – follow up 06/09/2016 01/12/2016
High Oak Surgery – follow up 14/09/2016 19/10/2016

Page 4 of 5
Practice Name Visit Date Report Published
Overall rating
Safe
Effective
Caring
Responsive
Well Led
Links Medical Practice (Netherton) 20/09/2016 31/10/2016
Castle Meadows Surgery 04/10/2016 01/11/2016
Coseley Medical Centre 06/10/2016 29/12/2016
Dudley P’ships for Health – follow up 12/10/2016 12/01/2017
Thorns Road Surgery – follow up 21/10/2016 14/12/2016
The Limes Medical Centre – follow up 27/10/2016 16/12/2016
The Greens Health Centre 10/11/2016 09/01/2017
Summerhill Surgery – follow up 17/11/2016 16/12/2016
Quincy Rise Surgery – follow up (2) 23/11/2016 26/01/2017
Pedmore Medical Practice – follow up 30/11/2016 23/02/2017
Quarry Bank Medical Practice 06/12/2016 09/01/2017
Woodsetton Medical Practice - follow up 19/12/2016 18/01/2017
Lower Gornal Medical Practice - follow up 21/12/2016 18/01/2017
Wordsley Green Health Centre 10/01/2017 08/02/2017
Kingswinford Medical Practice 12/01/2017 07/02/2017
Three Villages Surgery 18/01/2017 21/04/2017
Halesowen Medical Practice 20/01/2017 20/03/2017
Stourside Medical Practice – follow up 01/02/2017 18/05/2017
Northway Medical Centre 09/03/2017 11/05/2017
Feldon Lane Surgery – follow up 16/03/2017 21/04/2017
Clement Road Surgery – follow up 12/04/2017
Key:
Good Inadequate Requires Improvement Outstanding
Page 5 of 5
APPENDIX B: Summary of follow-up CQC inspections (as of 18/05/17)
Practice Name Visit Date Report Published
Overall rating
Safe
Effective
Caring
Responsive
Well Led
Bath Street Medical Centre 24/11/2015 28/01/2016 Inad Inad Inad Good RI Inad
Bath Street Medical Centre - follow up 26/07/2016 22/09/2016
RI Good RI RI
Good
Good
Clement Road Surgery 25/08/2016 12/10/2016
Clement Road Surgery – follow up 12/04/2017
Coseley Medical Centre 06/10/2016 29/12/2016 RI Goo
d RI Goo
d RI Goo
d
Dudley Partnerships for Health 10/02/2016 14/04/2016 Inad Inad RI RI RI Inad
Dudley Partnerships for Health- follow up 12/10/2016 12/01/2017
RI Goo
d RI Goo
d Goo
d RI
Links Medical Practice (Netherton Surgery) 20/09/2016 31/10/2016
Good RI Goo
d Goo
d Goo
d Goo
d
Pedmore Medical Practice 22/10/2015 14/01/2016 RI Inad Good
Good
Good
Good
Pedmore Medical Practice - follow up 30/11/2016 23/02/2017 RI RI RI
Good
Good RI
Quincy Rise Surgery 09/03/2016 02/06/2016 Inad Inad RI Good
Good Inad
Quincy Rise Surgery - follow up (1) 18/07/2016 02/09/2016 Quincy Rise Surgery - follow up (2) 23/11/2016 26/01/2017 good RI
St James Medical Practice (Dr Porter) 02/08/2016 13/09/2016 RI Inad RI
Good
Good RI
Stourside Medical Practice 16/02/2016 04/04/2016 RI RI Good RI Goo
d Goo
d
Stourside Medical Practice - follow up 01/02/2017 18/05/2017
The Greens Health Centre 10/11/2016 09/01/2017 Good RI Goo
d Goo
d Goo
d Goo
d
The Waterfront Surgery 17/12/2015 03/03/2016 Inad Inad RI Inad RI Inad
The Waterfront Surgery - follow up 06/09/2016 01/12/2016 RI Goo
d RI RI Goo
d Goo
d
Three Villages Surgery 18/01/2017 21/04/2017 RI … indicates a further follow-up visit will be required but is not yet scheduled

1 | P a g e
DUDLEY CLINICAL COMMISSIONING GROUP
PRIMARY CARE COMMISSIONING COMMITTEE
Date of Report: 26 May 2016 Report: Finance Report
Agenda item No: 8.1
TITLE OF REPORT: Primary Care Baseline Budgets 2017/18
PURPOSE OF REPORT: To present baseline budgets for the financial year 2017/18
AUTHOR OF REPORT: Mr P Cowley, Senior Finance Manager
MANAGEMENT LEAD: Mr M Hartland, Chief Operating and Finance Officer
CLINICAL LEAD: Dr T Horsburgh, Clinical Executive
KEY POINTS:
• Budgets delegated to this Committee by the CCG Board for the
financial year 2016/17 total £41.4m, with Primary Care Development budgets totalling £811,000 and Commissioning budgets £40,596,000
• This paper sets out the key areas of expenditure and the risks associated with each area.
• The overall level of risk associated with Primary Care budgets is low
• Uncommitted reserves total £253,000, with additional contingency and non-recurrent reserves also to be released.
• Additional allocations remain to be made to the CCG in respect of GP Forward View priorities.
RECOMMENDATION: Committee is requested to approve the baseline budgets as set out in the report.
FINANCIAL IMPLICATIONS: As above.
WHAT ENGAGEMENT HAS TAKEN PLACE: None
ACTION REQUIRED: Decision Approval √ Assurance
2 | P a g e
DUDLEY CLINCAL COMMISSIONING GROUP
PRIMARY CARE COMMISSIONING COMMITTEE – 26th MAY 2017 PRIMARY CARE COMMISSIONING FINANCE REPORT __________________________________________________________________________________ 1. INTRODUCTION
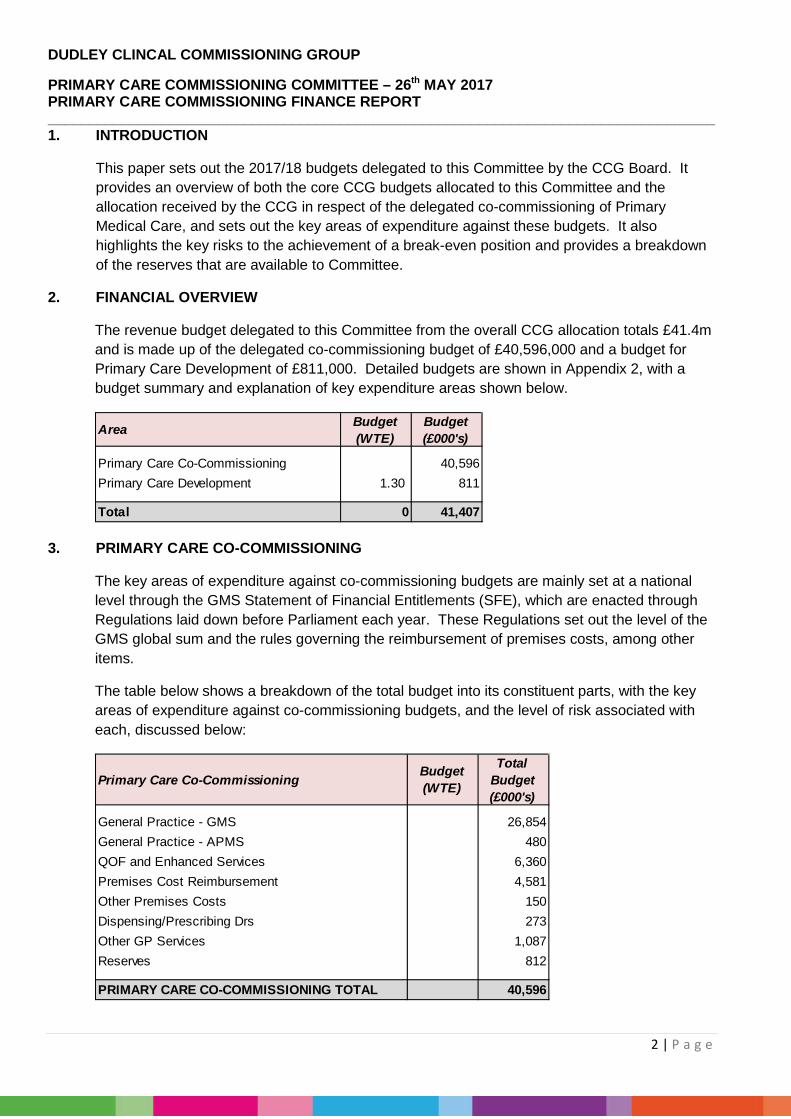
This paper sets out the 2017/18 budgets delegated to this Committee by the CCG Board. It provides an overview of both the core CCG budgets allocated to this Committee and the allocation received by the CCG in respect of the delegated co-commissioning of Primary Medical Care, and sets out the key areas of expenditure against these budgets. It also highlights the key risks to the achievement of a break-even position and provides a breakdown of the reserves that are available to Committee.
2. FINANCIAL OVERVIEW
The revenue budget delegated to this Committee from the overall CCG allocation totals £41.4m and is made up of the delegated co-commissioning budget of £40,596,000 and a budget for Primary Care Development of £811,000. Detailed budgets are shown in Appendix 2, with a budget summary and explanation of key expenditure areas shown below.
3. PRIMARY CARE CO-COMMISSIONING
The key areas of expenditure against co-commissioning budgets are mainly set at a national level through the GMS Statement of Financial Entitlements (SFE), which are enacted through Regulations laid down before Parliament each year. These Regulations set out the level of the GMS global sum and the rules governing the reimbursement of premises costs, among other items.
The table below shows a breakdown of the total budget into its constituent parts, with the key areas of expenditure against co-commissioning budgets, and the level of risk associated with each, discussed below:
Area Budget(WTE)
Budget(£000's)
Primary Care Co-Commissioning 40,596Primary Care Development 1.30 811
Total 0 41,407
Primary Care Co-Commissioning Budget(WTE)
Total Budget(£000's)
General Practice - GMS 26,854General Practice - APMS 480QOF and Enhanced Services 6,360Premises Cost Reimbursement 4,581Other Premises Costs 150Dispensing/Prescribing Drs 273Other GP Services 1,087Reserves 812
PRIMARY CARE CO-COMMISSIONING TOTAL 40,596
3 | P a g e
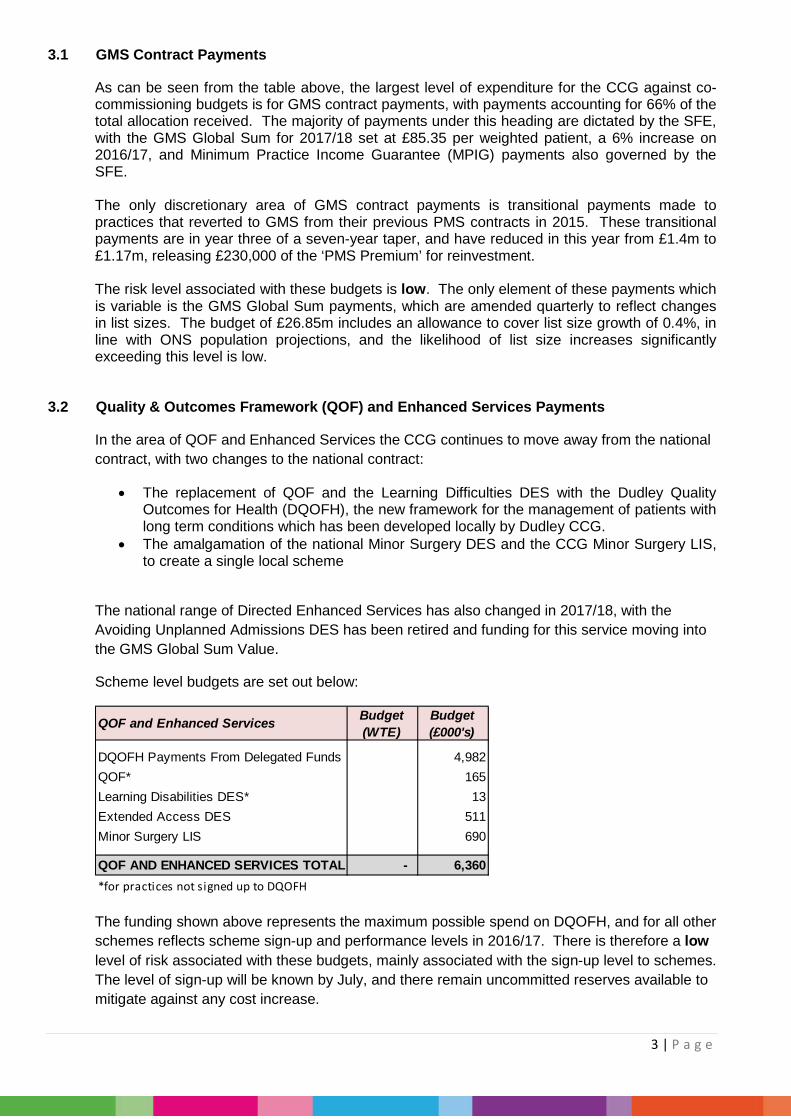
3.1 GMS Contract Payments
As can be seen from the table above, the largest level of expenditure for the CCG against co-commissioning budgets is for GMS contract payments, with payments accounting for 66% of the total allocation received. The majority of payments under this heading are dictated by the SFE, with the GMS Global Sum for 2017/18 set at £85.35 per weighted patient, a 6% increase on 2016/17, and Minimum Practice Income Guarantee (MPIG) payments also governed by the SFE. The only discretionary area of GMS contract payments is transitional payments made to practices that reverted to GMS from their previous PMS contracts in 2015. These transitional payments are in year three of a seven-year taper, and have reduced in this year from £1.4m to £1.17m, releasing £230,000 of the ‘PMS Premium’ for reinvestment. The risk level associated with these budgets is low. The only element of these payments which is variable is the GMS Global Sum payments, which are amended quarterly to reflect changes in list sizes. The budget of £26.85m includes an allowance to cover list size growth of 0.4%, in line with ONS population projections, and the likelihood of list size increases significantly exceeding this level is low.
3.2 Quality & Outcomes Framework (QOF) and Enhanced Services Payments
In the area of QOF and Enhanced Services the CCG continues to move away from the national contract, with two changes to the national contract:
• The replacement of QOF and the Learning Difficulties DES with the Dudley Quality Outcomes for Health (DQOFH), the new framework for the management of patients with long term conditions which has been developed locally by Dudley CCG.
• The amalgamation of the national Minor Surgery DES and the CCG Minor Surgery LIS, to create a single local scheme
The national range of Directed Enhanced Services has also changed in 2017/18, with the Avoiding Unplanned Admissions DES has been retired and funding for this service moving into the GMS Global Sum Value.
Scheme level budgets are set out below:
The funding shown above represents the maximum possible spend on DQOFH, and for all other schemes reflects scheme sign-up and performance levels in 2016/17. There is therefore a low level of risk associated with these budgets, mainly associated with the sign-up level to schemes. The level of sign-up will be known by July, and there remain uncommitted reserves available to mitigate against any cost increase.
QOF and Enhanced Services Budget(WTE)
Budget(£000's)
DQOFH Payments From Delegated Funds 4,982QOF* 165Learning Disabilities DES* 13Extended Access DES 511Minor Surgery LIS 690
QOF AND ENHANCED SERVICES TOTAL - 6,360*for practices not signed up to DQOFH

4 | P a g e
3.2.1 Dudley Quality Outcomes for Health
In 2017/18 42 of the CCG’s 46 practices have signed up to DQOFH, with 3 practices not participating and Bilston Street Surgery not being offered the scheme due to their imminent closure. For those 42 practices, payments under DQOFH will be based upon their historic income under QOF, the LD DES and the CCG Local Improvement Schemes that have been replaced by the scheme, and payments will be made under a hybrid system with a proportion of the payment based upon achievement of specific indicators.
The breakdown of the payments to practices under the scheme is shown below:
As the payments above represent the maximum payment to practices there is no risk of overspend against this budget, although there is a risk of underperformance against the indicators causing an underspend against this budget. As such, the risk level associated with DQOFH is low.
3.2.2 Minor Surgery
As agreed by Committee in October 2016, the Minor Surgery DES and LIS schemes have been combined for 2017/18, reducing the administrative burden on practices and the CCG by allowing all payments to be made monthly through automatic extractions of EMIS data. This change has no financial implication, as the combined payment rates for Minor Surgery will remain unchanged.
3.3. Premises Cost Reimbursement
General Practices are reimbursed for a range of premises-related costs based upon the rules laid out in the GMS Premises Costs Directions 2013, with reimbursement being available for rent (either actual rent, where the practice lease their premises, or notional, where the practice own their own premises), Business and Water Rates, and Clinical waste.
3.3.1 Business Rates
There has been a significant reduction in Business Rates in 2017/18, due to national changes in business rates rules and the effect of the 2017 revaluation of premises, with costs reducing from approximately £850,000 in 2016/17 to £470,000 in 2017/18. It should be noted, however, that some of this reduction is temporary as practices seeing an increase have been able to access transitional relief, and that in the long term these costs will rise to approximately £650,000.
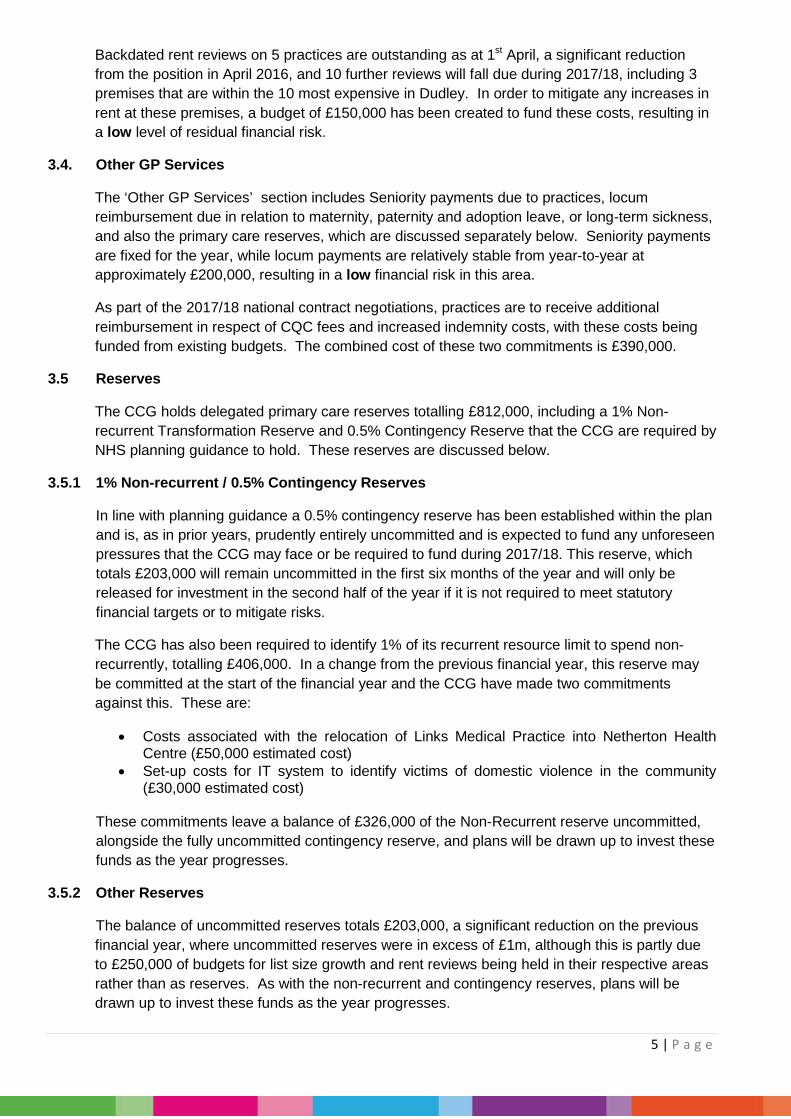
3.3.2 Outstanding Rent Reviews
Under the Premises Costs Directions practices are entitled to three-yearly reviews of their rent reimbursement levels, a process that can result in the level of reimbursement either increasing or decreasing and which in 2016/17 resulted in a net increase in reimbursement of £60,000.
Item Delegated Primary Care Core CCG Total
Access Standards 664 664Historic Payment - Block 2,137 650 2,787Historic Payments - Indicator Based 2,137 650 2,787Total 4,938 1,300 6,238
Budget (£000's)
5 | P a g e
Backdated rent reviews on 5 practices are outstanding as at 1st April, a significant reduction from the position in April 2016, and 10 further reviews will fall due during 2017/18, including 3 premises that are within the 10 most expensive in Dudley. In order to mitigate any increases in rent at these premises, a budget of £150,000 has been created to fund these costs, resulting in a low level of residual financial risk.
3.4. Other GP Services
The ‘Other GP Services’ section includes Seniority payments due to practices, locum reimbursement due in relation to maternity, paternity and adoption leave, or long-term sickness, and also the primary care reserves, which are discussed separately below. Seniority payments are fixed for the year, while locum payments are relatively stable from year-to-year at approximately £200,000, resulting in a low financial risk in this area.
As part of the 2017/18 national contract negotiations, practices are to receive additional reimbursement in respect of CQC fees and increased indemnity costs, with these costs being funded from existing budgets. The combined cost of these two commitments is £390,000.
3.5 Reserves
The CCG holds delegated primary care reserves totalling £812,000, including a 1% Non-recurrent Transformation Reserve and 0.5% Contingency Reserve that the CCG are required by NHS planning guidance to hold. These reserves are discussed below.
3.5.1 1% Non-recurrent / 0.5% Contingency Reserves
In line with planning guidance a 0.5% contingency reserve has been established within the plan and is, as in prior years, prudently entirely uncommitted and is expected to fund any unforeseen pressures that the CCG may face or be required to fund during 2017/18. This reserve, which totals £203,000 will remain uncommitted in the first six months of the year and will only be released for investment in the second half of the year if it is not required to meet statutory financial targets or to mitigate risks.
The CCG has also been required to identify 1% of its recurrent resource limit to spend non-recurrently, totalling £406,000. In a change from the previous financial year, this reserve may be committed at the start of the financial year and the CCG have made two commitments against this. These are:
• Costs associated with the relocation of Links Medical Practice into Netherton Health Centre (£50,000 estimated cost)
• Set-up costs for IT system to identify victims of domestic violence in the community (£30,000 estimated cost)
These commitments leave a balance of £326,000 of the Non-Recurrent reserve uncommitted, alongside the fully uncommitted contingency reserve, and plans will be drawn up to invest these funds as the year progresses.
3.5.2 Other Reserves
The balance of uncommitted reserves totals £203,000, a significant reduction on the previous financial year, where uncommitted reserves were in excess of £1m, although this is partly due to £250,000 of budgets for list size growth and rent reviews being held in their respective areas rather than as reserves. As with the non-recurrent and contingency reserves, plans will be drawn up to invest these funds as the year progresses.
6 | P a g e
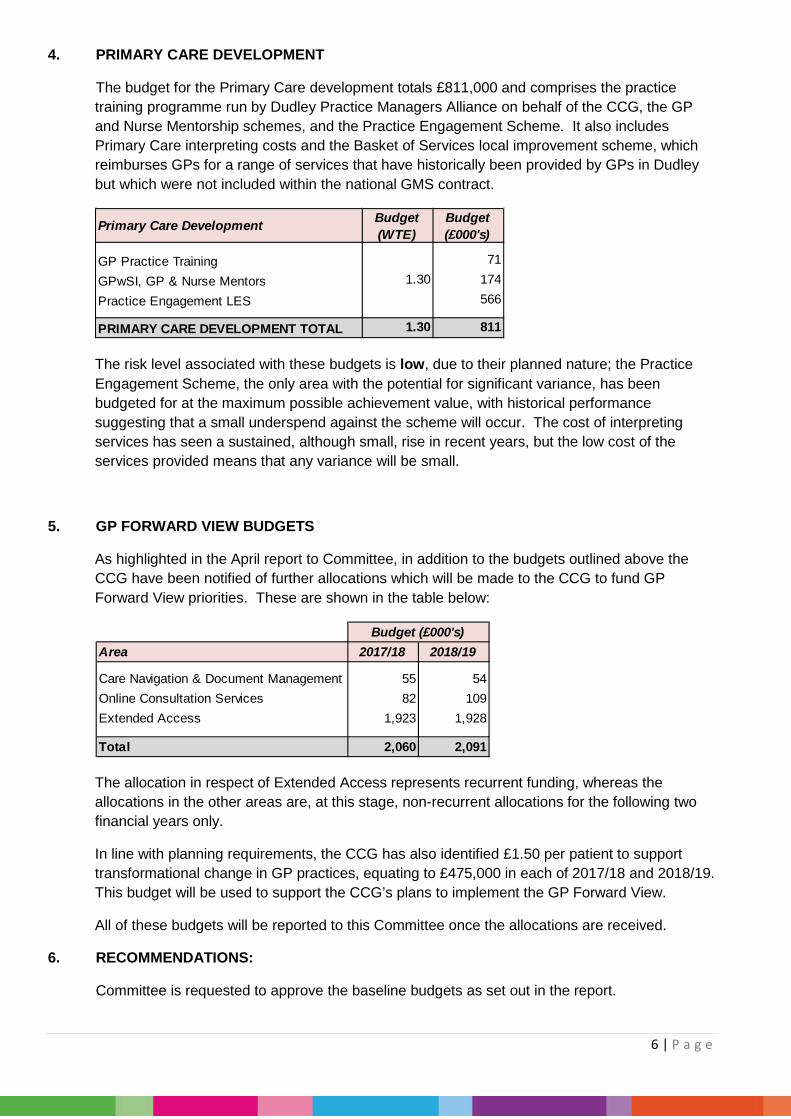
4. PRIMARY CARE DEVELOPMENT
The budget for the Primary Care development totals £811,000 and comprises the practice training programme run by Dudley Practice Managers Alliance on behalf of the CCG, the GP and Nurse Mentorship schemes, and the Practice Engagement Scheme. It also includes Primary Care interpreting costs and the Basket of Services local improvement scheme, which reimburses GPs for a range of services that have historically been provided by GPs in Dudley but which were not included within the national GMS contract.
The risk level associated with these budgets is low, due to their planned nature; the Practice Engagement Scheme, the only area with the potential for significant variance, has been budgeted for at the maximum possible achievement value, with historical performance suggesting that a small underspend against the scheme will occur. The cost of interpreting services has seen a sustained, although small, rise in recent years, but the low cost of the services provided means that any variance will be small.
5. GP FORWARD VIEW BUDGETS
As highlighted in the April report to Committee, in addition to the budgets outlined above the CCG have been notified of further allocations which will be made to the CCG to fund GP Forward View priorities. These are shown in the table below:
The allocation in respect of Extended Access represents recurrent funding, whereas the allocations in the other areas are, at this stage, non-recurrent allocations for the following two financial years only.
In line with planning requirements, the CCG has also identified £1.50 per patient to support transformational change in GP practices, equating to £475,000 in each of 2017/18 and 2018/19. This budget will be used to support the CCG’s plans to implement the GP Forward View.
All of these budgets will be reported to this Committee once the allocations are received.
6. RECOMMENDATIONS:
Committee is requested to approve the baseline budgets as set out in the report.
Primary Care Development Budget(WTE)
Budget(£000's)
GP Practice Training 71
GPwSI, GP & Nurse Mentors 1.30 174
Practice Engagement LES 566
PRIMARY CARE DEVELOPMENT TOTAL 1.30 811
Area 2017/18 2018/19
Care Navigation & Document Management 55 54Online Consultation Services 82 109Extended Access 1,923 1,928
Total 2,060 2,091
Budget (£000's)
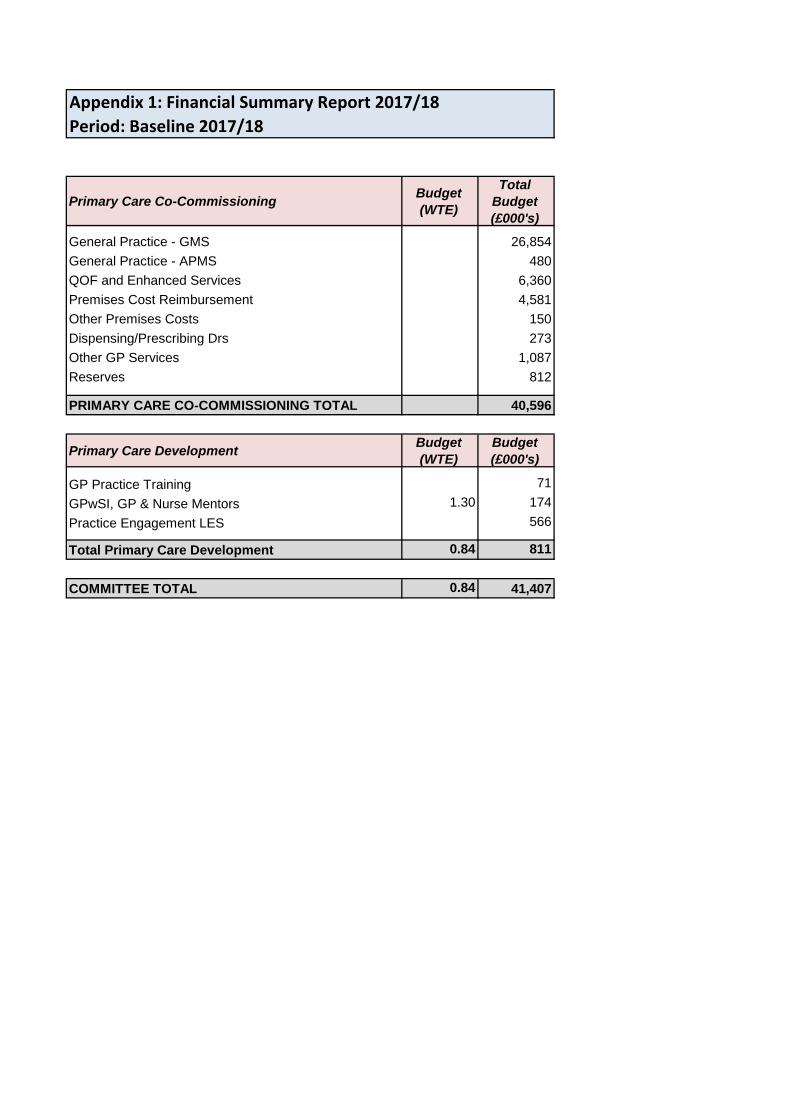
Appendix 1: Financial Summary Report 2017/18Period: Baseline 2017/18
Primary Care Co-Commissioning Budget(WTE)
Total Budget(£000's)
General Practice - GMS 26,854General Practice - APMS 480QOF and Enhanced Services 6,360Premises Cost Reimbursement 4,581Other Premises Costs 150Dispensing/Prescribing Drs 273Other GP Services 1,087Reserves 812
PRIMARY CARE CO-COMMISSIONING TOTAL 40,596
Primary Care Development Budget(WTE)
Budget(£000's)
GP Practice Training 71GPwSI, GP & Nurse Mentors 1.30 174Practice Engagement LES 566
Total Primary Care Development 0.84 811
COMMITTEE TOTAL 0.84 41,407
1 | P a g e
PRIMARY CARE COMMISSIONING COMMITTEE
Date of Committee: 26 May 2017 Report: Primary Care Analysis Tool (PCAT) Report and Update
Agenda Item: 9.1
TITLE OF REPORT: Primary Care Analysis Tool (PCAT) Report and Update
PURPOSE OF REPORT: Update the Primary Care Development Committee on the PCAT and further developments of the tool
AUTHOR OF REPORT: Mr R Franklin (BI Developer & Analyst)
MANAGEMENT LEAD: Mr M Hartland (Chief Operating & Finance Officer)
CLINICAL LEAD: Dr J Darby
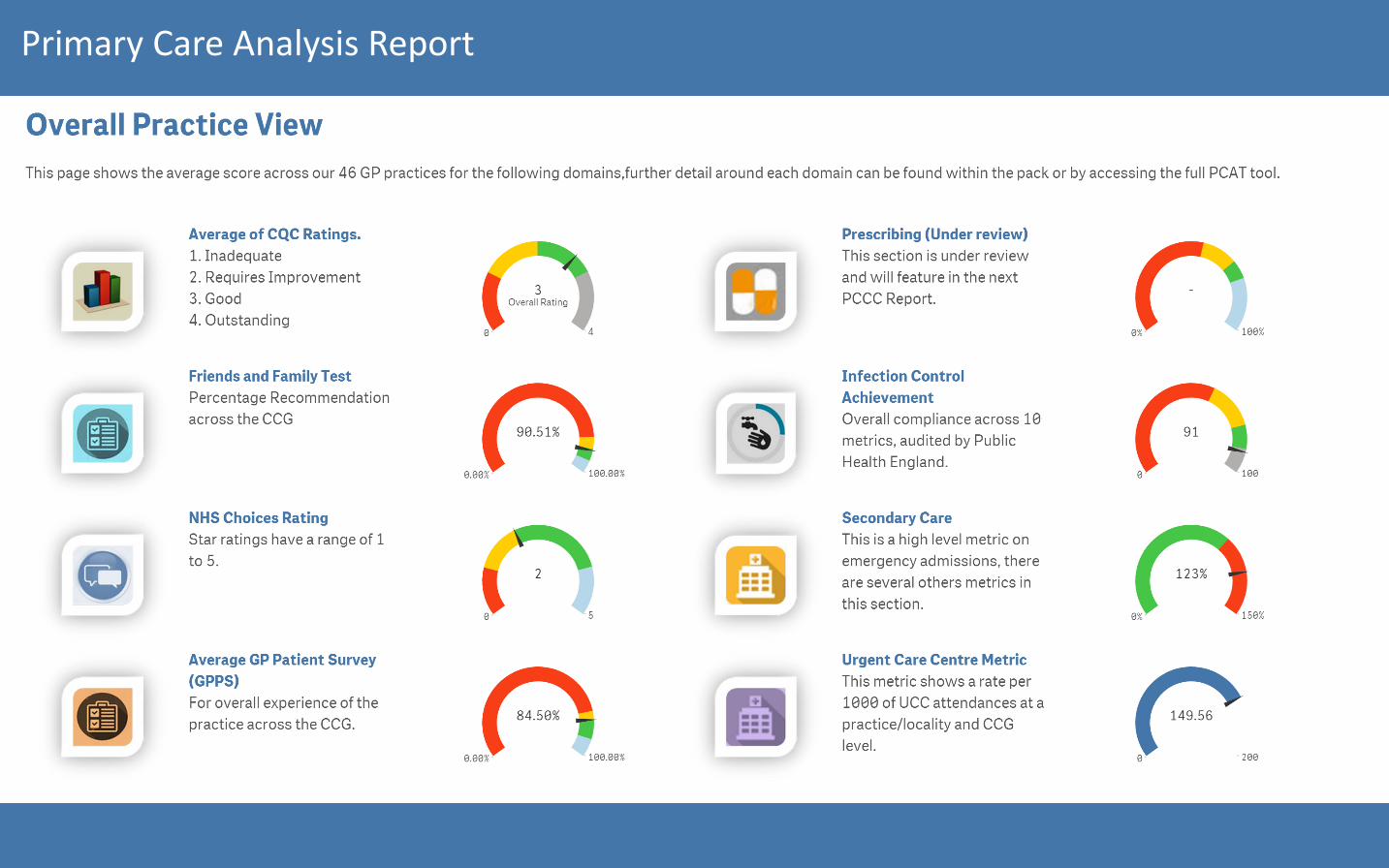
KEY POINTS:
• A solution has now been agreed with TerraFirma (Dudley IT
services) on 10.05.17 for Qliksense to be available in GP practices. A rollout will begin W/C 5th June.
• The prescribing element of the PCAT is currently under development, this revised section will provide practices with their own prescribing dashboard broken down to drug level.
• Further datasets will be added to the PCAT to better triangulate performance and quality datasets, some elements of this report will be presented at the Primary Care Operational Group (PCOG).
RECOMMENDATION:
• The PCAT will provide a central platform for performance and quality datasets.
• The PCAT was designed to be a flexible and responsive analysis tool. Therefore development will in a sense be on-going through the request for change process
FINANCIAL IMPLICATIONS: None
WHAT ENGAGEMENT HAS TAKEN PLACE:
Extensive clinical and management engagement has previously taken place on the development of the PCAT metrics in various forums both formal and informal.
ACTION REQUIRED: Approval Assurance

2 | P a g e

Primary Care Analysis Report
Primary Care Analysis Report
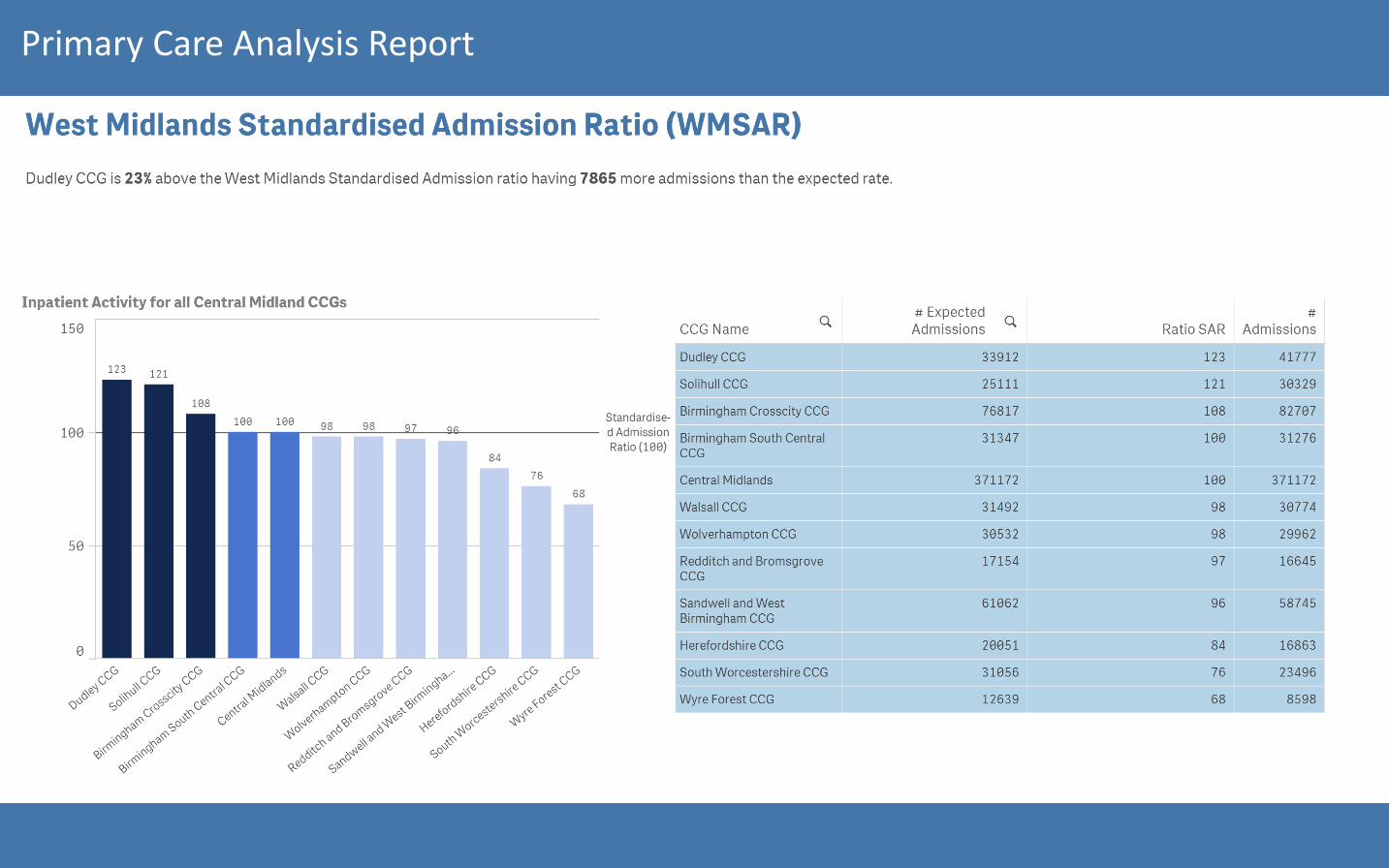
Primary Care Analysis Report

Primary Care Analysis Report
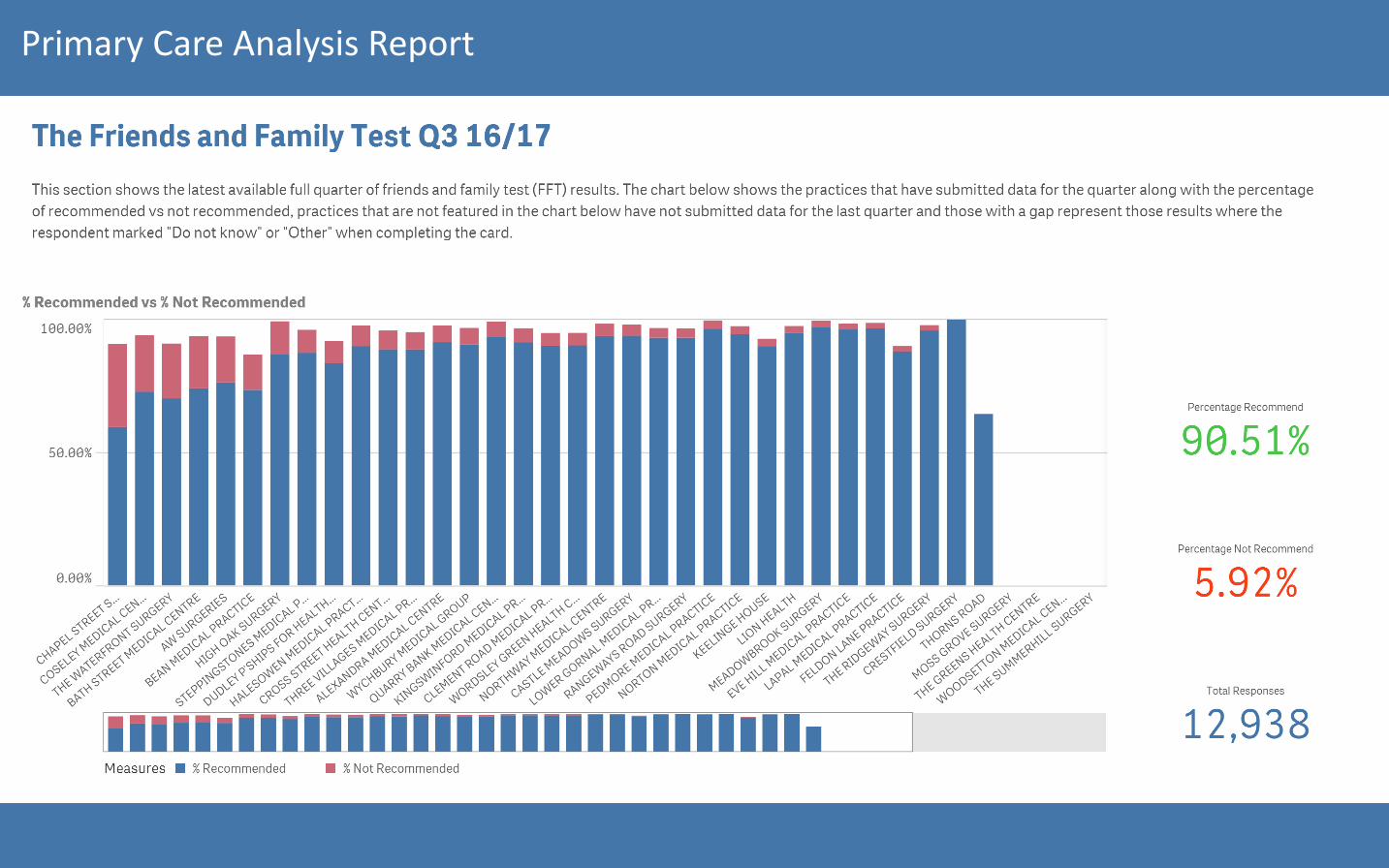
Primary Care Analysis Report
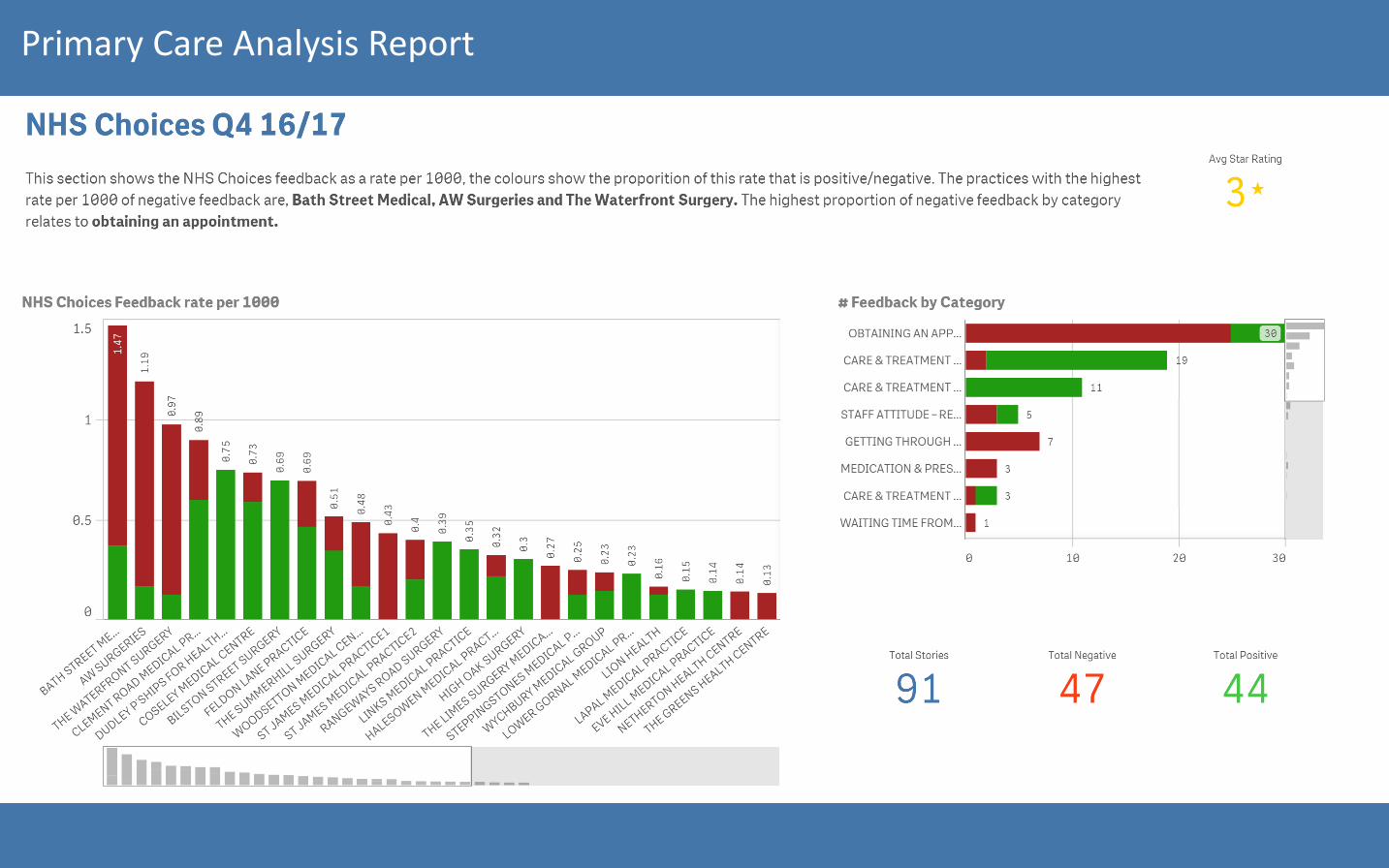
Primary Care Analysis Report
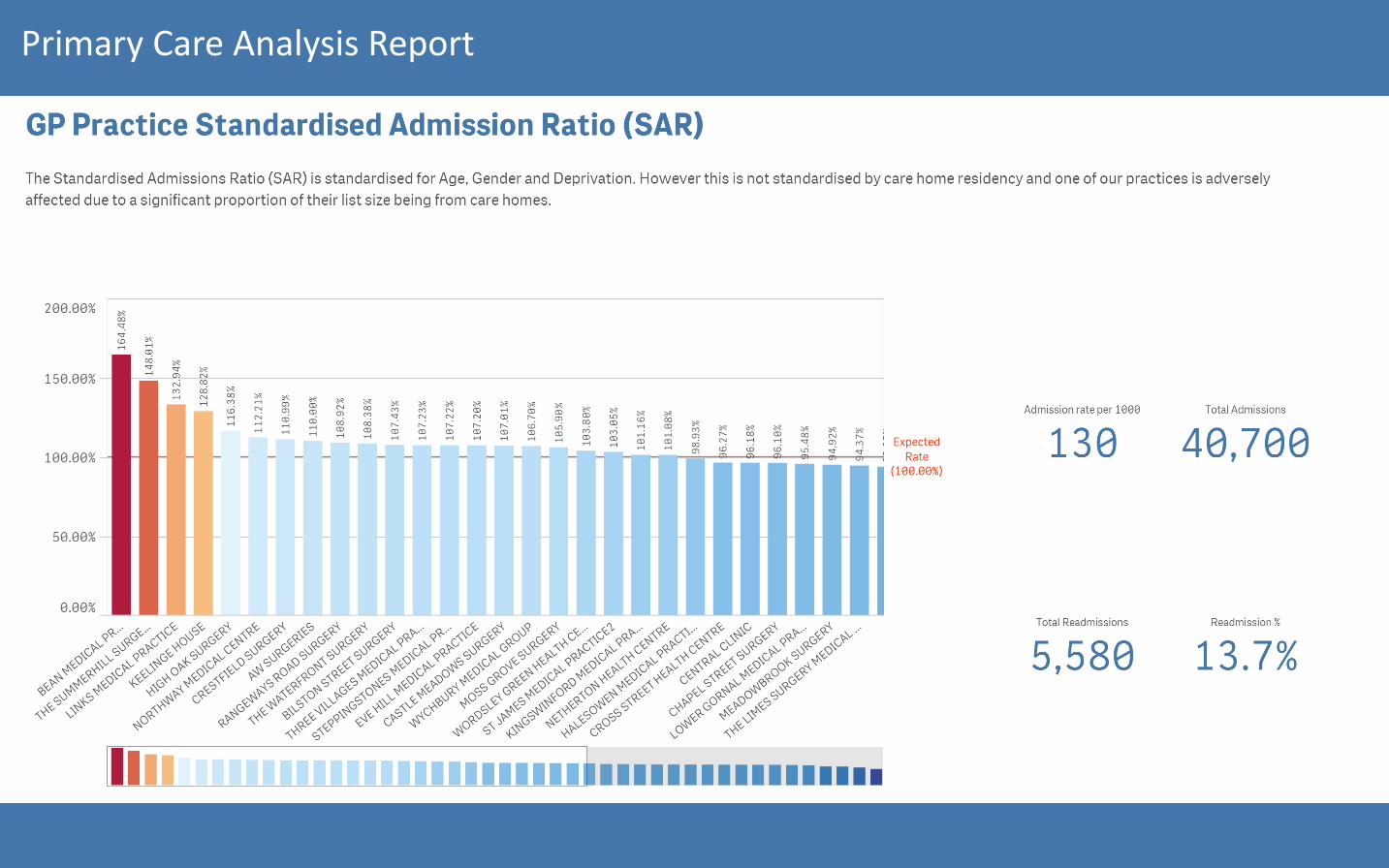
Primary Care Analysis Report

Primary Care Analysis Report

Primary Care Analysis Report

Primary Care Analysis Report

Dudley CCG Combined Board Assurance Framework and Corporate Risk Register 2017/18
09-May-17 Updates from Committees in April 2017
1A Primary care and Multi Speciality Community Provider (MCP) development
NOTE: TREND IN RESIDUAL RISK AGAINST PREVIOUS MONTH IS SHOWN //=
ID Original Date Last Review (Committee
Date)
Last Update (Risk
Amended)
LIN
K T
O
CO
RPO
RA
TE
OB
JEC
TIVE
(SEE
K
EY A
BO
VE)
Risk Description Accountable Committee
Accountability Sponsor & Owner
Management Lead
P I
Initial Risk Score (PxI)Score
before any controls are
in place.
Key ControlsWhat controls/systems are in place to assist in securing delivery of ourobjective. Such as strategies, policies and procedures
Gaps in ControlWhere are we failing to put controls/ systems in place. / Where are we failing in making them effective. For example lack of training or no regular review of performance
Gaps in Assurance Where are we failing to gain evidence that our controls/ systems, on which we place reliance, are effective. Such as no assurance a strategy or policy is effective
(R) P (R) I
Residual Risk Score
(PxI)Score
following controls put
in place
Risk Trend Internal AssurancesBoard Reports, Minutes of meetings
External AssurancesInternal and External Audit Reports, CQC Reports
ActionsTo improve control, ensure delivery ofprincipal objectives, gain assurance
TimescalesDate action will be completed
COMMENTS
34 22/04/2013 17/03/2017 17/02/2017 2
The impact of significant individual performance issues in relation to primary medical services that could result in removal of GP member from the Performers' List
PCC Steve Wellings Caroline Brunt 4 4 16
GP Contracts / AppraisalsPeer Review AuditTraining and EducationGMC RegistrationGP under performance referred to the NHS England Professional & Practice Information Gathering Group (PIGG)
None identified. None identified 3 4 12 =
Primary Care Operational Group reporting into Primary Care Commissioning Committee and Quality and Safety Committee
GMC RegistrationTwo way communication between the CCG PCOG and the PIGG at NHS England
GP / Nurse MentoringCommissioning of Services for Primary CareGP Education, training and Development
On-going
Recent allegations and charges against a GP has increased this residual risk score from 2 to 12 (3x4).
50 04/08/2014 17/03/2017 17/02/2017 2
Failure of member practices to meet the standards of the Care Quality Commission risks continuity of service provision in member practices.
PCC Steve Wellings Caroline Brunt 4 4 16
Relationship with the Link Inspector at the CQC who is invited to attend the Primary Care Operational Group (PCOG).Training and Development with Practices to help them manage inspections.Blue Stream online academy. Quality Assurance Manager for Primary Care appointed and in post. PCOG and PCC following NHS England "Framework for responding to CQC inspections of GP practices". CCG has support process and package in place for all practices.
Further develop the working arrangements with NHS England Professional & Practice Information Gathering Group.
None identified 3 3 9 =
All CQC inspection reports considered in the Primary Care Operational Group and coordinated actions in place between CCG, NHS England and CQC.
CQC Reports and associated action plans from GP Practices.
Develop a quality framework and Care Quality Review Meeting (CQRM) for Primary Care
On-Going
Residual risk score decreased from 12 to 9 as a practice was classed as inadequate and in special measures but has now turned round to score Good. The report is however draft and not yet published.
59 29/10/2014 17/03/2017 17/02/2017 3
The ability of member practices to fulfil their contractual obligations and provide primary medical services as a result of difficulties recruiting substantive GPs
PCC Steve Wellings Caroline Brunt 3 4 12
Developing and implementing the new model of care - Dudley Multispecialty Community Provider (MCP). As part of the new model, developing and investing in the clinical and non clinical infrastructure and estate to deliver the model.
N/A 3 3 9 =
Engagement visits with all GP practices. Workforce data collection. Developing and investing in the clinical and non clinical infrastructure and professional development to implement the new model of care.
NHS England and Health Education England commitment to training and professional development. New models of care team supporting the Dudley Vanguard MCP model of care and development.
Successful bids to the new models of care team for additional investment and support to enable the implementation of the new model of care.
On-Going
69 22/05/2015 17/03/2017 17/02/2017 2
Loss of Primary Care Medical Services as a result of increasing overheads and financial pressure on member practices beyond their control i.e. increasing cost of medical indemnity insurance, rent increases and financial sustainability of operating branch surgery sites.
PCC Steve Wellings Caroline Brunt 2 3 6
Developing and implementing the new model of care - Dudley Multispecialty Community Provider (MCP). As part of the new model, developing and investing in the clinical and non clinical infrastructure and estate to deliver the model.
None identified. N/A 1 3 3 =
Engagement visits with all GP practices. Workforce data collection. Developing and investing in the clinical and non clinical infrastructure and professional development to implement the new model of care. Successful bids to the new models of care team for additional investment and support to enable the implementation of the new model of care.
New models of care team supporting the Dudley Vanguard MCP model of care and development.
Education, training and support. Providing access to specialist advice and support. Coordinating and supporting practices liaising with NHS property services regarding rent increases. Investing in systems and creating processes that enable improvements in practise efficiency i.e. practice development programmes. Implementation of the new model of care including successful bid to the new model of care team for additional investment, and the development and implementation of the estates strategy.
Publication of the GP Forward View
Apr-17Action PCOG to reconsider this risk in its entirety and advise the Committee accordingly
81 05/10/2015 17/03/2017 17/02/2017 1The risk to provision of primary medical services arising from unforeseen branch surgery closures.
PCC Steve Wellings Caroline Brunt 4 4 16
GP Practices need to undertake statutory Consultation and apply to CCG, which has full authority to decide on an application
None None 3 3 9 = Application considered by PCOG decision by PCCC
NHS England Policy which CCG adopted under delegated primary care commissioning
Support GP Practices in the consultation process.Primary Care contracts manager meeting practices to take through contractual process in terms on branch closures.Finance & IT provide advice on financial advice and IT infrastructure advice.
Mar-17 Changes made to Risk Description for clarity of purpose
96 17/06/2016 17/03/2017 17/02/2017 4
That increases in the cost of facilities management and service charges of buildings owned by NHS Property Services (NHSPS) may destabilise the finances of General Practices, leading to loss of services.
PCC Steve Wellings Caroline Brunt 2 3 6
The CCG has set up a working group of affected practices to ensure visibility of issues and co-ordinate practice responses, and has offered to act on practices’ behalf in dealing with NHSPS to resolve existing disputes.
Further development of CCG and practice relationships with NHS Property Services is required.
2 3 6 =Liaise with NHS Property Services on behalf of General Practices and use tenants’ forum to identify common issues and approaches to resolution
Jun-17
118 08/06/2016 17/03/2017 17/02/2017 1A
Lack of clinical and managerial capacity and capability for primary care to deliver the required transformation and operate primary care at scale
PCC Steve Wellings Caroline Brunt 4 3 12
Primary Care Development Steering Group established and co-ordinating and developing plans to enable practices to improve and change.
None identified. None identified 3 3 9 =Primary Care Development Steering Group reports to the Primary Care Commissioning Committee
Primary Care Commissioning Committee reports to NHS England
None identified Mar-17This Risk was approved by the Committee subject the sponsor being changed to Steve Wellings
119 08/06/2016 17/03/2017 17/02/2017 4B
Where there is poor quality estate that compromises the ability of practices to deliver General Medical Service contracts
PCC Steve Wellings Caroline Brunt 4 3 12
Primary Care Estates Strategy and participation and support of CCG to enable access to National funding streams.
None identified. None identified 3 3 9 =
The CCG agreed its Estates Strategy. Practical support available to practices to prepare and access National funding streams.
None identified None identified On-goingThis Risk was approved by the Committee with the alterations as outlined.
124 18/11/2016 17/03/2017 17/02/2017 4B
The impact of contractors (single handed or partnership) not performing against their GMS/APMS contract which may result in remedial/breach notices and possible termination of contract by provider or commissioner
PCC Steve Wellings Caroline Brunt 3 3 9Support provided to contract holder to remedy the breach. Support provided by NHS England, West Midlands
None N/A 3 3 9 = N/A N/AMonitored through Primary Care Commissioning Committee.Legal advice will be taken
Jan-17 Committee approved
2C Develop the CCG: Fit for purpose for the future2D Performance management of the system and Value Proposition (VP) implementation
3. Improving quality and safety 3A Ensure on-going safety and performance of the system4. System effectiveness 4A Procure the MCP
4B Primary Care contract4C Actively participate in the Black Country Sustainability Transformation Plan (STP)
2B Public engagement on model and procurement
STRATEGIC AIMS OBJECTIVES 2016/17 & 2017/181. Reducing health inequalities2. Delivering best possible outcomes 2A Ensure appropriate procurement of secondary care services

1
GLOSSARY
ABBREVIATIONS Abbreviation Meaning #NOF Fractured Neck of Femur
£K £1,000 equivalent
A&E Accident and Emergency
ABC / ABCD Above and Beyond the Call of Duty (Local surveys which include praise for
nominated staff members as well as assessment of services)
ACRA Advisory Committee on Resource Allocation
ACS Acute Coronary Syndrome
AD Assistant Director
AfC Agenda for Change
AHSN Academic Health Science Networks
ALE Auditors Local Evaluation
ALOS Average Length of Stay (in hospital)
AMI Acute Myocardial Infarction
AMMC Area Medicines Management Committee
Anti-D An antibody occurring in pregnancy
Anti-TNF Drugs used in the treatment of rheumatoid arthritis and Crohn’s disease
ARIF Aggressive Research Intelligence Facility
ASAP As soon as possible
AVE Advertising Value equivalent
BACs Bank Automated Credit
BCC Black Country Cluster
BCG Bacillus Calmette-Guerin
BCPFT Black Country Partnership NHS Foundation Trust
BCUCG Black Country Urgent Care Group
BFT Behavioural Family Therapy
BLCCB Black Country Local Collaborative Commissioning Board
BME Black Minority Ethnic
BMJ British Medical Journal
BPAS British Pregnancy Advisory Board
BSCCP British Society of Colposcopy and Cervical Pathology
CAB Citizens Advise Bureau
2
CABG Coronary Artery Bypass Graft
CAO Chief Accountable Officer
CAMHS Children and Adolescent Mental Health Service
CASH Contraception and Sexual Health
CAT Change Agent Team
CBSA Commissioning Business Support Agency
CCBT (CBT) Computerised Cognitive Behavioural Therapy
CCF Capable Care Forum
CCG Clinical Commissioning Group
CCRN Comprehensive Clinical Research Networks
CDC Clinical Development Committee
CEO Chief Executive Officer
CFO Chief Finance Officer
CHADD The Churches Housing Association of Dudley & District Ltd
CHC Continuing Healthcare
CHD Coronary Heart Disease
CIS Community Investment Strategy
CMO Chief Medical Officer
CNST Clinical Negligence Scheme for Trusts
CNT Community Nursing Team
CONNECT Mental Health information website for staff
COSHH Control of Substances Hazardous to Health Regulations 2002
CPA Care Programme Approach
CPN Community Psychiatric Nurse
CRL Capital Resource Limit
CRRT Community Rapid Response Team
CSSD Central Sterile Services Department
CT scan Computer Topography
CQNO Chief Quality and Nursing Officer
CQUIN Commissioning for Quality and Innovation
CQRM Clinical Quality Review Meeting
CVD Cardio Vascular Disease
CWAS Coventry and Warwickshire Audit Services
DACHS Directorate of Adult Children and Housing Services
DCS Dudley Community Services
DCVS Dudley Community Voluntary Service
DES Directed Enhanced Service
DfES Department for Education and Skills
DGFT Dudley Group Foundation Trust
DNA Did not attend

3
DoH Department of Health
DoLS Deprivation of Liberty Safeguards
DoS Directory of Service
DTC Diagnostic and Treatment Centre
DWMHPT Dudley and Walsall Mental Health Partnership Trust
DXA Dual X-ray Absorptiometry (measures bone density).
E&D Equality and Diversity
EAU Emergency Assessment Unit
EBME Electro Bio-Mechanical Engineer
ECA Extra Care Area
ECM Every Child Matters
ECT Electroconvulsive Therapy
ED Emergency Department
EI Early Implementer
EI Early Intervention
EMI Older People with Mental Illness (Elderly Mentally Ill)
EPP Expert Patients Programme
EPR Electronic Patient Record
ERMA Emergency Response & Management Arrangements
ERT Enzyme Replacement Therapy
ESR Electronic Staff Record
FCEs Finished Consultant Episodes
FED Forum for Education and Development
FHS Family Health Services
FIP Computerised data collection facility used by community health teams.
FMC Facility Management Centre
FOI Freedom of Information
FYE Full Year Effect
GMS General Medical Services
GOWM Government Office for the West Midlands
GP General Practitioner
GPAQ General Practice Assessment of Quality
GPwSI GPs with Special Interest
GU Genito-urinary
GUM Genito-urinary Medicine
HCAI Healthcare Associated Infections
HEE Health Education England
HENIG Health Economy NICE Implementation Group
HF Heart Failure
HIC Health Improvement Centre
4
HIV Human Immunodeficiency Virus
HPA Health Protection Agency
HPS/S Health Promoting Schools / Service
HPU Health Protection Unit
HR Human Resources
HSC Health and Safety Commission
HSCQC Health and Social Care Quality Centre
HSE Health and Safety Executive
HT Home Treatment
HV Health Visitor
IAPT Improved Access to Psychological Therapies
IC Infection Control
ICAS Independent Complaints Advocacy Service
ICNA Infection Control Nurses Association
ICP Integrated Care Pathway
ICSM Interim Customer Services Manager
IFR Individual Funding Request
IG Information Governance
IOSH Institute of Occupational Safety and Health
IT Information Technology
IUCD Intrauterine Contraceptive Device
JCAB Joint Clinical Advisory Board
JCC Joint Consultative Committee
JD Job Description
JE Job Evaluators
JM Job Matching
KLOE Key lines of enquiry
KSF Knowledge and Skills Framework
KPI Key Performance Indicators
LAA Local Area Agreement
LAC Looked After Children
LAT Local Area Team
LBC Liquid Based Cytology
LD Learning Disability
LDP Local Delivery Plan
LEA Local Education Authority
LIFT Local Improvement Finance Trust
LIG Local Implementation Group
LIT Local Implementation Team
LMC Local Medical Committee

5
LNG Local Negotiating Committee
LPS Local Pharmaceutical Scheme
LRF Local Resilience Forum
LTC Long Term Conditions
LVD Left Ventricular Dysfunction
LVSD Left Ventricular Systolic Dysfunction
MAPA Management of Actual and Potential Aggression
MAU Medical Assessment Unit
MBC Metropolitan Borough Council
MDT Multi Disciplinary Team
MIMT Major Incident Management Team
MIRE Major Incident Response Executive
MLSOs Medical Laboratory Scientific Officers
MRSA Methicillin Resistant Staphylococcus Aureus
MSS Medium Secure Service
NCA Non contract activity
NCB National Commissioning Board
NCRS National Care Record System
NELHI National Electronic Library for Health Information
NICE National Institute for Clinical Excellence
NGMS New General Medical Services
NHS National Health Service
NHSCPT NHS Community Practice Teacher
NHSCSP NHS Cancer Screening Programme
NHSE NHS England
NHSLA NHS Litigation Authority
NHSP National Healthy Schools Programme
NICE National Institute for Clinical Excellence
NOF New Opportunities Fund
NPfIT National Programme for IT
NPSA National Patient Safety Agency
NRF Neighbourhood Renewal Fund
NRLS National Reporting and Learning System
NRT Nicotine Replacement Products
NSF National Service Framework
OAT Out of Area Treatment
OBD Occupied Bed Day
OD Organisational Development
ODM Oesophageal Doppler Monitoring
OOH Out of Hours

6
OSC Overview and Scrutiny Committee
OT Occupational Therapist
PALS Patient Advice and Liaison Service
PAF Positive Assurance Framework
PAS Patient Administration System
PAU Paediatric Assessment Unit
PbR Payment by Results
PC Personal Computer
PCDB Primary Care Delivery Board
PCCC Primary Care Commissioning Committee
PCDC Primary Care Development Committee
PCOG Primary Care Operational Group
PCT Primary Care Trust
PDF Portable Document Format
PDP Personal Development Plan
PDS Personal Dental Services
PDSA Plan, Do, Study, Act
PDU Professional Development Unit
PE Pulmonary Embolism
PEAK Database holding the main registered details of patients and associated referral,
contact, caseload, outpatient, inpatient, MH Act and clinic information.
PEAT Patient Environment Action Team
PEC Professional Executive Committee
PEPP Pooled Budget External Placement Panel
PFI Private Finance Initiative
PGD Patient Group Directives
PICU Psychiatric Intensive Care Unit
PID Project Initiation Document
PIN Personal Identification Number
PMLD Profound and Multiple Learning Difficulties
PMS Primary Medical Services
PPA Prescription Pricing Authority
PPG Patient Participation Group
PPIF Patient and Public Involvement Forum
PSA Public Service Agreement
PSHE Personal and Social Health Education
PTCA Percutaneous Transluminary Coronary Angioplasty
Q&A Questions and Answers
Q&S Quality & Safety
QA Quality Assurance
7
QIPP Quality, Innovation, Productivity and Prevention
QMAS Quality Management and Analysis System
QOF Quality and Outcome Framework
QPDT Quality and Practice Development Teams
RACPC Rapid Access Chest Pain Clinic
RAS Respiratory Assessment Service
RCA Root Cause Analysis
RES Race Equality Scheme
RHH Russells Hall Hospital
RIDDOR Reporting of Injuries, Diseases and Dangerous Occurrences Regulations
RMO Responsible Medical Officer
RRL Revenue Resource Limit
RSL Register Social Landlords
RTT Referral to Treatment Target
SAP Single Assessment Process
SEPIA Mental health computer system
SFBH Standards for Better Health
SFI Standing Financial Instructions
SIC Statement of Internal Control
SLA Service Level Agreement
SRE Sex and Relationship Education
SSD Social Services Department
SSDP Strategic Services Development Plan
STI Sexually Transmitted Disease
STRW Support, Time & Recovery Worker
TB Tuberculosis
TIA Transient Ischaemic Attack
TP Teenage Pregnancy
TPT Teenage Pregnancy Team
TTO To Take Out
UCC Urgent Care Centre
UHBT University Hospital Birmingham Trust
Vaccs & Imms Vaccinations and Immunisations
WAN Wide Area Network
WCC World Class Commissioning
WIC Walk in Centre
WMAS West Midlands Ambulance Service
WMCSU West Midlands Commissioning Support Unit
WMHTAC West Midlands Health Technology Advisory Committee
WMSCG West Midlands Strategic Commissioning Group
8
WMSSA West Midlands Specialised Services Agency
WTE Whole Time Equivalent