
PREVIEW OF EMT/EMT NERVOUS SYSTEM TRAUMA POWERPOINT TRAINING PRESENTATION
16
PREVIEW OF EMT/EMR NERVOUS SYSTEM TRAUMA POWERPOINT TRAINING PRESENTATION
-
Upload
bruce-vincent -
Category
Education
-
view
60 -
download
1
Transcript of PREVIEW OF EMT/EMT NERVOUS SYSTEM TRAUMA POWERPOINT TRAINING PRESENTATION
PREVIEW OF
EMT/EMR NERVOUS SYSTEM TRAUMA
POWERPOINT TRAINING PRESENTATION
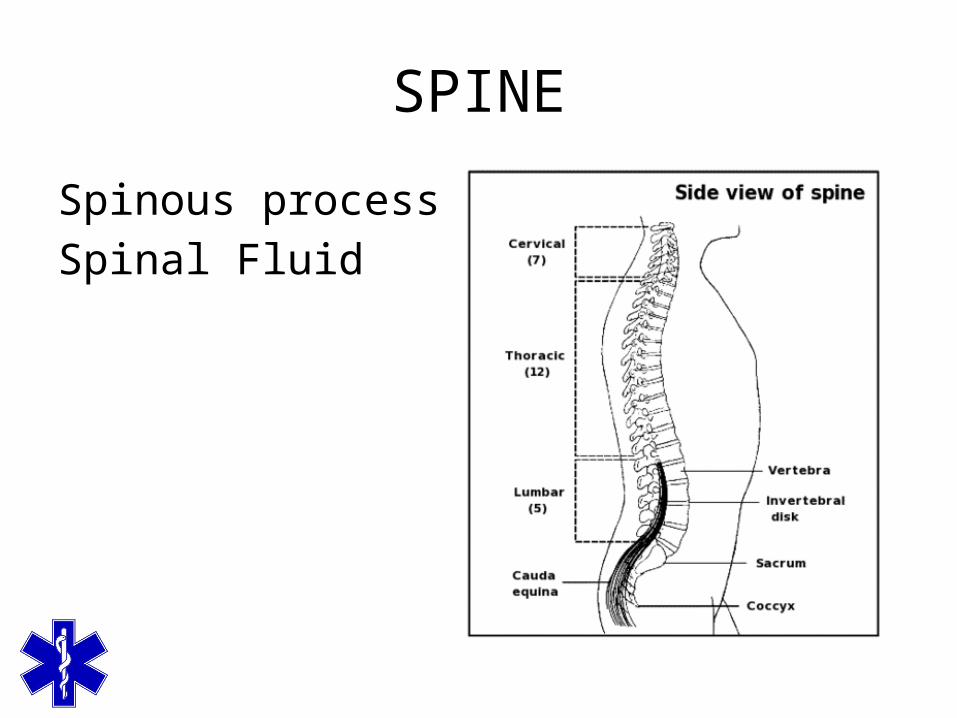
SPINE
Spinous processSpinal Fluid
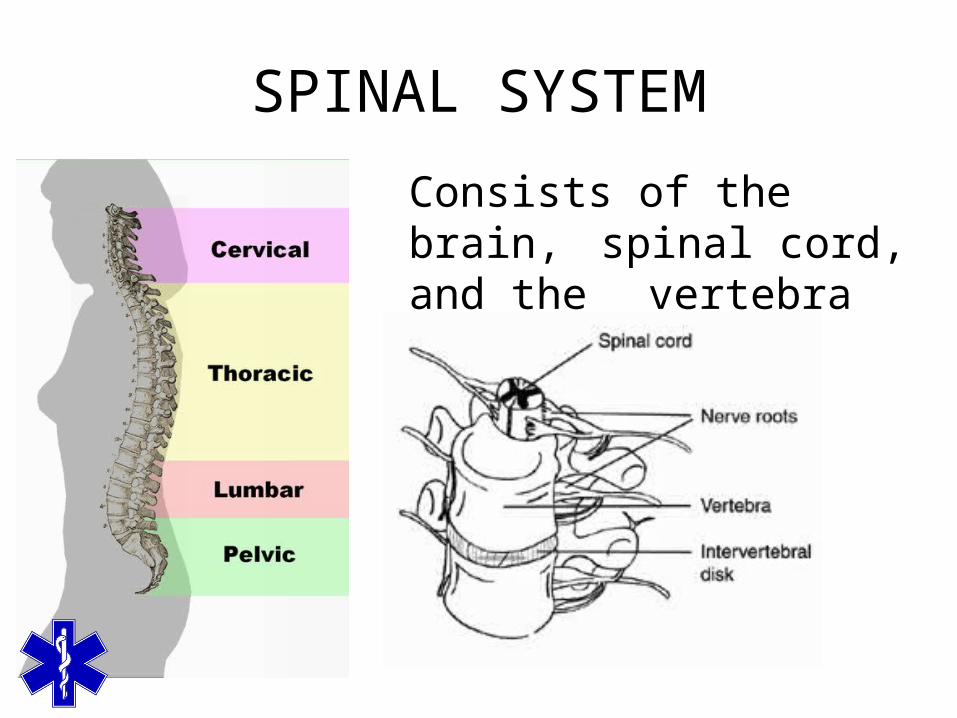
SPINAL SYSTEM
Consists of the brain, spinal cord, and the vertebra
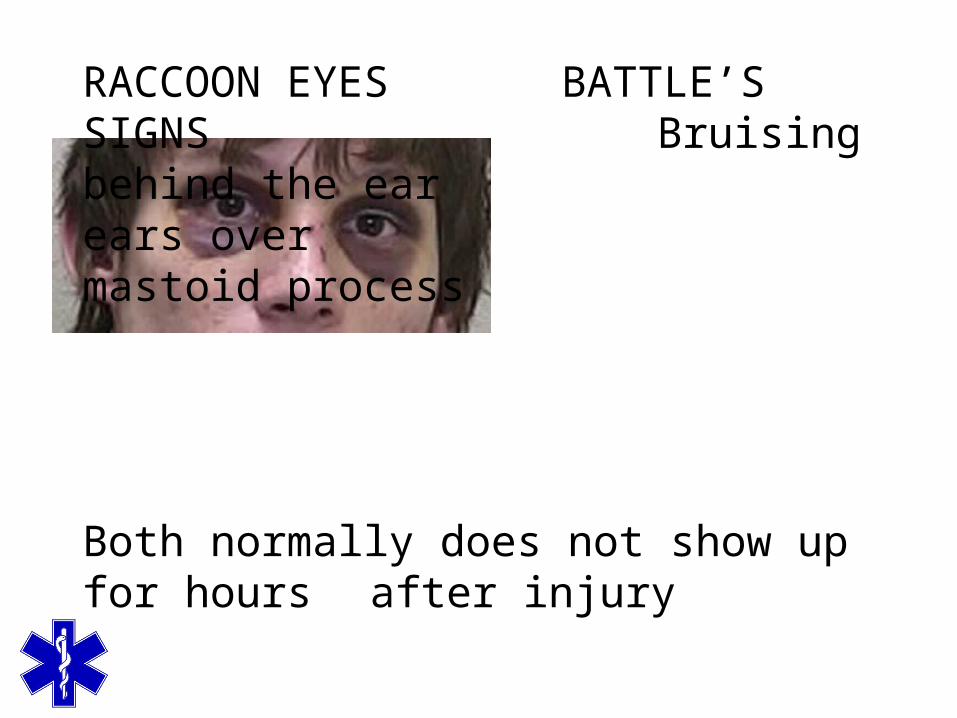
RACCOON EYES BATTLE’S SIGNS
Bruising behind the ear
ears over mastoid process
Both normally does not show up for hours after injury
CONCUSSION
AKA Minor head traumaThe most common traumatic brain injuryCaused by the jarring of the brain, resulting in
temporary signs & symptoms Repeated concussions may lead to permanent
brain damageCommonly seen in contact sports, car accidents,
falls & bicycle accidents
CEREBRAL LACERATION
Traumatic brain injury where the brain is torn Similar to a Contusion but more severe due to greater force Signs & symptoms
Lucid interval with no change in level of consciousness
Level of consciousness will decrease as laceration bleeds & blood builds up into skull
PENETRATING WOUNDS
Common causes include gun shot, arrows, metal rods, & other high velocity projectiles
Often have exit woundHas high mortality rate (up to 92%)Signs & symptoms vary depending upon parts of
brain affected
SPINAL IMMOBILIZATION
In patients with head injuries with altered mental statusMechanism of injury that suggests the possibility
of trauma to the spine
COMPLETE NEUROLOGICAL EXAM
Vital signsBlood pressure
Systolic pressure increaseHypotension is associated with
poorer outcomes in head injured patients
Pulse rate – may be slower than normal if severe head injury
TRAUMATIC BRAIN INJURY FOUNDATION GUIDELINES
They have treatment guidelines for EMS for concussions as well as other traumatic brain
injurieswww.braintrauma.org
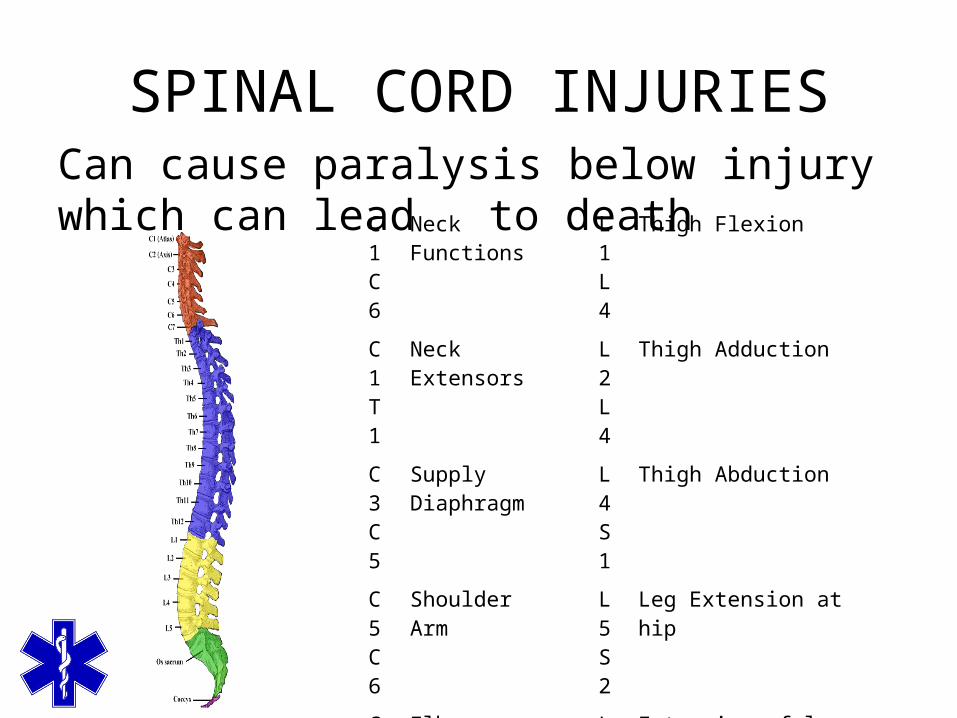
SPINAL CORD INJURIESCan cause paralysis below injury which can lead
to death C1C6
Neck Functions L1L4
Thigh Flexion
C1T1
Neck Extensors L2L4
Thigh Adduction
C3C5
Supply Diaphragm
L4S1
Thigh Abduction
C5C6
Shoulder Arm
L5S2
Leg Extension at hip
C6C7
ElbowWrist
L2L4
Extension of leg at knee
C7T1
Wrist flex L4S2
Flexion of leg at knee
T1T6
Intercostal & Trunk
L4S1
Flexion of foot
T7L1
Abdominal Muscles L4S1
Extension of toes
OPEN SPINE WOUND
Often caused by projectilesHas high susceptibility for paralysis & infection
NEUROLOGICAL EXAMINATION CONSIDERATIONS
Movement of extremitiesAbsent or weakNote level of impairment
Respiratory abilityChest wall movementAbdominal Excursion
SensationPresent throughout bodyAbsent – note the specific level of impairment
Altered sensation distal to injury – jingling, numbness,“electric shocks”
GENERAL MANAGEMENT CONSIDERATIONS WITH SPINAL TRUAMA
Manual immobilization of spine when airway openedImmobilization principlesLog-roll patient with suspected spinal trauma to move or examine backCervical collars
RigidProper size
VARIATIONS FOR GERIATRIC ASSESSMENT AND MANAGEMENT OF SPINAL INJURY
Unusual spinal anatomy due to agingSpecial modifications of spinal immobilization
techniques

To purchase this presentation go to www.bravetraining.com
Or tap the above link


















