
Prevention of Renal Diseases in the Emerging World: Toward Global Health Equity Bellagio, Italy...
37
Prevention of Renal Diseases in the Emerging World: Toward Global Health Equity Bellagio, Italy March 2004 Diabetic Nephropathy Epidemiological challenge in Mexico An educational program for prevention directed to primary physicians
-
date post
22-Dec-2015 -
Category
Documents
-
view
215 -
download
0
Transcript of Prevention of Renal Diseases in the Emerging World: Toward Global Health Equity Bellagio, Italy...

Prevention of Renal Diseases in the Emerging World: Toward
Global Health Equity
Bellagio, Italy March 2004
Diabetic NephropathyEpidemiological challenge in Mexico
An educational program for prevention directed to primary
physicians
Ricardo Correa-Rotter

Diabetes Mellitus in the World: A Pandemic
WHO. The World Health Report 1997.
Africa Americas Oriental Mediterraneum
Europe SoutheastAsia
Occidental Pacific
Prevalence estimated(millions)
0
10
20
30
40
50
60
70
80Year 1995 2000 2025

4.9 7.712
16.920.4
46.1
8.6
10.8
12.2
5.2
7
8.7
10.88.8
05
1015202530354045
20-29 30-39 40-49 50-59 60-69
Age (years)Known DM > 126 mg/dl 110-125 mg/dl
Prevalence of Diabetes by Age Groups Prevalence of Diabetes by Age Groups
National Chronic Diseases Survey (ENEC), 2002
14.1
20.8
29.3
38.546.7
Overall: 12 %
TodaysMinority
TomorrowsMajority

Mortality 1930-2000
11.5 10.1
23.3
26.7
16.2
6.54.45.1
4
7
10
13
16
19
22
25
28
1930 1940 1950 1960 1970 1980 1990 2000
M
Fuente: INEGI. Indicadores Sociodemgráficos de México, 1930-2000
Population Growth in Mexico1960-2000
3.4
2.6
2.0
1.61.51.71.92.12.32.52.72.93.13.33.5
1960-1970 1970-1990 1990-1995 1995-2000
TM
AC
Demographic Transition in MEXICO
Reduction in Population Growth
Reduction in Mortality
Informatics and GeographyInstitute, MEXICO(INEGI)

100959085807570656055504540353025201510
50
0.00.20.40.60.81.01.2 0.0 0.2 0.4 0.6 0.8 1.0 1.2
Population Pyramid of Mexico: Censed in 2000 and Projected in 2050
2000 Projected 2050
Millions of inhabitants
AGE Male Female
National Population Council, MEXICO, (CONAPO)

Diabetes Related Mortality in Mexico: Historic EvolutionDiabetes Related Mortality in Mexico: Historic Evolution
O. Velázquez M, A. Lara E., A. Peña C. La Diabetes en México, 2001
0
5
10
15
20
25
30
35
40
1922 1930 1940 1950 1960 1970 1980 1990 1995 2000
X 1
000
inha
bita
nts

34 %
Rank CIE 10a. Rev. Descrption Deaths Rate %
Total 441,004 100
1 E10-E14 Diabetes mellitus 49,855 48.96 11.3
2 I20-I25 Ischemic heart disease 45,421 44.61 10.3
3 K70, K72.1, Liver diseases and cancer 25,704 25.24 5.8
4 I60-I69 Cerebrovascular diseases 25,657 25.20 5.8
5 P00-P96 Neonatal period related problems 18,192 17.87 4.1
6 J40-J44, J67 Pulmonary obstructive disease 15,944 15.66 3.6
7 2/ Motor vehicle accidents 13,761 13.51 3.1
8 J10-J18, Acute pulmonary diseases 13,101 12.87 3.0
9 N00-N19 Nephritis and Nephrosis 10,477 10.29 2.4
10 I10-I15 Hypertension related diseases 10,170 9.99 2.3
General Mortality in Mexico in 2001General Mortality in Mexico in 2001
Secretaria de Salud, MEXICO 2002

Growth of ESRD on Renal Replacement Therapy (2001)
Comparison with population rate growth
1.3
10
7
5
7
0
2
4
6
8
10
12
Pop.Growth
ESRD HD PD TX

Adaptado de: Feidhlim Woods, 1998
Projected Need of Renal Replacement Therapy in the World
Published in the WWW
0
500
1000
1500
2000
2500
3000
Patients on dialysis (x1000)
1995 2000 2005 2010 2015 2020
Developed Nations
Developing Nations

Projected Growth of Dialysis Population in Mexico(Thousands of patients)
0
10
20
30
40
50
60
70
80
25,000
71,000
47,000
1,2502,500 5,000
92 98 00 0402 06 08 10
Year
Correa-Rotter et. al. National Health Planning Support Document 2001
dialysis
transplantation

27.625.5
22.219
26
16.3
49
0
20
40
60
Argentina Venezuela Colombia Brasil Panama Uruguay Mexico
Diabetes Mellitus as cause of ESRD on renal replacement therapy(Percentage).Adapted from: Kidney International: 57, 2000.
Diabetes as Cause of ESRF in Mexico Diabetes as Cause of ESRF in Mexico
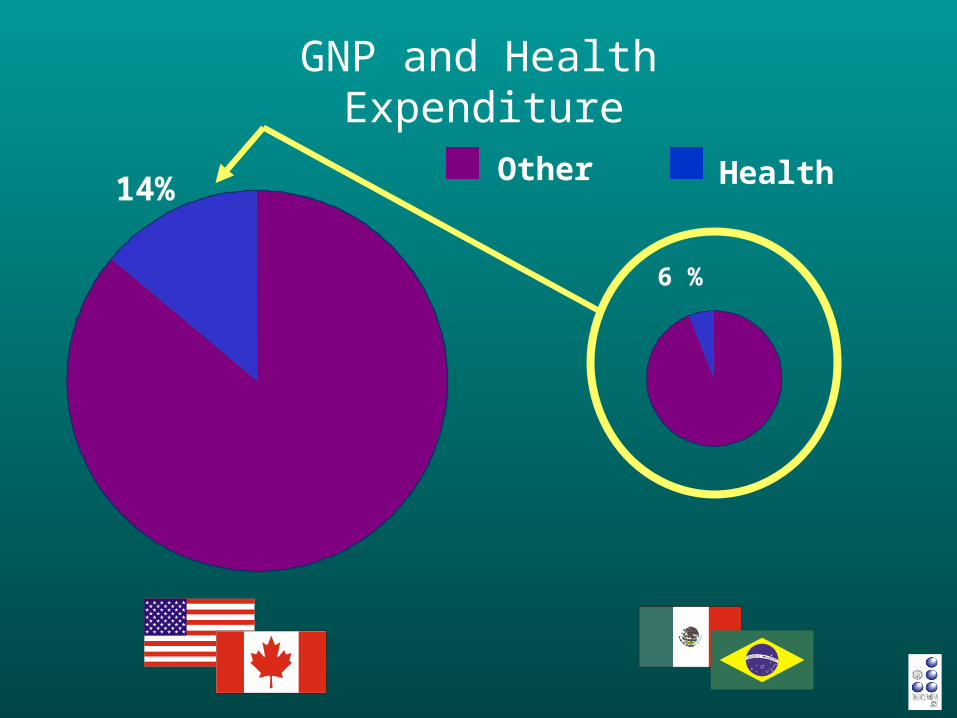
GNP and Health Expenditure
Other14%
6 %
Health

Growth of ESRD and Renal Replacement Therapy in Some Developing Nations
Uncontrolled !!
Unmanageable !!
Unaffordable !!
OPTIONS
Overlook the problem and leave to “natural history”
Patient Selection and Rationning of medical services
PREVENTION and RETARDATION of Vascular & Renal Disease

Strategies to Prevent Vascular and Progressive Renal Disease in Type 2 DM
• Changes in lifestyle Dietary issues
Obesity
Protein consumption
Salt intake
Cigarette smoking
Physical activity
Glycemic control
Blood pressure control Specific benefits induced by ACE inhibitors and/or AII blockers
Hiperlipidemia control

Strategies available in daily practice to reestablish
euglycemia are not efficient enough in order to
prevent later complications such as diabetic
nephropathy
• In our usual clinical environment, obtaining an VERY GOOD GLYCEMIC CONTROL can be extremely difficult.
• Physicians often lack commitment or time to reinforce consistently this practice and to follow closely patient´s performance.
• Patients underestimate consequences and comply poorly.
• Given these evidences, other modifiable variables should be treated in order to try to prevent or delay development of vascular damage and diabetic nephropathy.

• Issue remains controversial given the fact that the effects of protein restriction are far from spectacular and there is an important risk of malnutrition, particularly with very low protein diets.
• Situation in Mexico and other developing nations differs completely from Europe and USA, regions that usually have high protein diets.
• Present evidence does not support an intense protein restriction, yet it seems reasonable to limit intake to around 0.8 g/ kg/ day
Protein Intake Restriction in Diabetic Nephropathy

Cigarrette Smoking and Diabetic Nephropathy
• It has been demonstrated that cigarette smoking may increase the risk
of developing type 2 DM as well as associated microvascular
complicationes, including microalbuminuria
Remuzzi G et al, Am J Kidney Dis 33: 807, 1999
• Other authors have shown that smoking can be deletereous for diabetic
patients in terms of increasing incidence and/or severity of diabetic renal
disease
Orth SR et al, Kidney int 54: 926, 1998
Biesenbach G et al: Clin Nephrol. 48(3):146-50 1997
Sawicki P et al, Diabetes Care 17: 126, 1994

Prognostic Importance of Microalbuminuria in DM2Prognostic Importance of Microalbuminuria in DM2
Eastman RC, Keen H. Lancet 1997;350(Suppl 1):29–32.
M. Alb Tobacco Diast BP
CV Mortality
(OR)
Cholesterol
10.02
6.52
2.323.20
10
8
6
4
2
0

Reduction in albuminuria predicts a retardation of loss of
glomerular filtration rate in the diabetic patient
Useful and reasonably cheap marker for therapeutic
response
MICROALBUMINURIA

• Some ethnic groups have a higher risk of developing
diabetic nephropathy. Mexicans and mexico-americans are
among these high risk groups (Pugh et al, Diabetes 44: 1375, 1995).
• Prevention is MORE EFFICIENT if it starts in early stages
(even before appearance of microalbuminuria)
NEVERTHELESS: There is a clear opportunity for
intervention almost at any stage of the disease.
PREVENTION IN DIABETIC NEPHROPATHY
When to start and how to determine who is in higher risk ?


Education program for diagnosis and prevention of diabetic nephropathy in Mexico
Research Project:Research Project:
“ “Development and validation of an Development and validation of an
educational program for diagnosis and educational program for diagnosis and
prevention of diabetic nephropathy directed prevention of diabetic nephropathy directed
to general and family practitioners working in to general and family practitioners working in
the Public Health System”.the Public Health System”.

FACTSFACTS• In Mexico nationwide, there is no primary or secondary strategy for In Mexico nationwide, there is no primary or secondary strategy for
prevention of DN.prevention of DN.
• First contact physicians, First contact physicians, who actually are in chargewho actually are in charge of most patients of most patients
with DM, do not have adequate knowledge for an updated diagnostic with DM, do not have adequate knowledge for an updated diagnostic
and therapeutic aproach.and therapeutic aproach.
• In addition, first contact physicians do not have the In addition, first contact physicians do not have the MOTIVATIONMOTIVATION
required to implement measures directed towards prevention and required to implement measures directed towards prevention and
treatment of early phases of DN.treatment of early phases of DN.
Education program for diagnosis and prevention of diabetic nephropathy in Mexico

Education program for diagnosis and prevention of diabetic nephropathy in Mexico
JustificationJustification
• The establishment of an educational program for first The establishment of an educational program for first contact physicians may allow us to modify knowledge contact physicians may allow us to modify knowledge and practices directed to primary and secondary and practices directed to primary and secondary prevention of diabetic prevention of diabetic cardiovascular andcardiovascular and kidney kidney diseasedisease
– First contact physicians who are actually in charge of First contact physicians who are actually in charge of patients patients
– At a limited national level (pilot)At a limited national level (pilot)
• An efficient program may An efficient program may DELAYDELAY development or development or progression of Diabetic Nephropathyprogression of Diabetic Nephropathy

JustificationJustification
• This program may favor, on the long term, a lesser This program may favor, on the long term, a lesser growth of the number of diabetic ESRD patients growth of the number of diabetic ESRD patients requiring renal replacement therapyrequiring renal replacement therapy
• In addition it may reduce mortality related to In addition it may reduce mortality related to Diabetes Mellitus and ESRDDiabetes Mellitus and ESRD
• Finally, it may allow significant savings in the Finally, it may allow significant savings in the treatment of ESRD patients and in general to our treatment of ESRD patients and in general to our strained health budgetstrained health budget
Education program for diagnosis and prevention of diabetic nephropathy in Mexico

• Implementation of this program will increase knowledge of Implementation of this program will increase knowledge of
general practitioners as well as general practitioners as well as motivation and understanding motivation and understanding
of the great importance of their participationof the great importance of their participation in this process. in this process.
• Diagnostic and therapeutic approaches will be modified and Diagnostic and therapeutic approaches will be modified and
directed towards a systematic primary and secondary directed towards a systematic primary and secondary
preventive approach.preventive approach.
HypothesisHypothesis
Education program for diagnosis and prevention of diabetic nephropathy in Mexico

ObjectiveObjective
• We will compare modification of diagnostic and We will compare modification of diagnostic and
therapeutic conducts between experimental and paired therapeutic conducts between experimental and paired
control centers.control centers.
• The educational program in DN will be validated at the The educational program in DN will be validated at the
national level, as it will be randomly implemented national level, as it will be randomly implemented
(experimental) or not (control) in Primary Care Health (experimental) or not (control) in Primary Care Health
Centers Centers
Education program for diagnosis and prevention of diabetic nephropathy in Mexico

• Participation of 27 nephrologists of different states of the Mexican Participation of 27 nephrologists of different states of the Mexican
Republic as educators and co-investigators (already recruited and a Republic as educators and co-investigators (already recruited and a
1st. working meeting has taken place 10 days ago, with ISN 1st. working meeting has taken place 10 days ago, with ISN
collaboration).collaboration).
• Nephrologist directly participate in the design and implementation of Nephrologist directly participate in the design and implementation of
the educational program and each one of them will have 1-2 primary the educational program and each one of them will have 1-2 primary
care centers and around 10 or more primary care physicians.care centers and around 10 or more primary care physicians.• Experimental: primary care physicians (n 400)
• Control: primary care physicians from “paired centers” (n 400)
Education program for diagnosis and prevention of diabetic nephropathy in Mexico
MethodsMethods

Education program for diagnosis and prevention of diabetic nephropathy in Mexico

MethodsMethods
• The educational program is being developed by a group The educational program is being developed by a group of nephrologists, in conjunction with other professionals of nephrologists, in conjunction with other professionals (epidemiologist, sociologist, psicologist and teaching (epidemiologist, sociologist, psicologist and teaching professionals)professionals)
• After developed, the program will be aplied and validated After developed, the program will be aplied and validated employing an experimental design.employing an experimental design.– Experimental Health Centers will be randomly Experimental Health Centers will be randomly
selected.selected.– Paired Health Centers will be also selected as Paired Health Centers will be also selected as
controls (no educational manouever).controls (no educational manouever).• Centers will be evaluated and monitores identically in Centers will be evaluated and monitores identically in
order to compare results.order to compare results.
Education program for diagnosis and prevention of diabetic nephropathy in Mexico

Education program for diagnosis and prevention of diabetic nephropathy in Mexico
Project phases:Project phases:
Phase IPhase I
• Writing of a proposal (preliminary working draft)Writing of a proposal (preliminary working draft)
• Preliminary budget and looking for funding (National Council of Science Preliminary budget and looking for funding (National Council of Science
and Technology Grant, Industry, Others to come…….)and Technology Grant, Industry, Others to come…….)
• Selection of collaborators (consulting committee (7), epidemiologist (1), Selection of collaborators (consulting committee (7), epidemiologist (1),
psicologist (1), sociologist (1), teaching expert (1), collaborating psicologist (1), sociologist (1), teaching expert (1), collaborating
nephrologists (28), health authorities, international ISN/SLANH nephrologists (28), health authorities, international ISN/SLANH
consultants )consultants )
• Presentation of the project in an investigators meeting for discussion, Presentation of the project in an investigators meeting for discussion,
necessary ammendment and motivation.necessary ammendment and motivation.
• Obtaining a FINAL ammended version of the Protocol.Obtaining a FINAL ammended version of the Protocol.

Education program for diagnosis and prevention of diabetic nephropathy in Mexico
Project phases:Project phases:
Phase IIPhase II
• Preparation of Standardized Educational Material Preparation of Standardized Educational Material (“Time to Act”)(“Time to Act”)
• Preparation of “measurement instruments” to quantitate and Preparation of “measurement instruments” to quantitate and
validate results of educational effortsvalidate results of educational efforts
• Logistics, selection of participating Primary Care Health Centers Logistics, selection of participating Primary Care Health Centers
and final decisions on how to apply the educational programand final decisions on how to apply the educational program
±
±
Phase IIIPhase III
• Second investigators meeting for specific review of educational Second investigators meeting for specific review of educational
material and training for standardized uniform teaching practices material and training for standardized uniform teaching practices
(including theoretical aspects, motivational and others)(including theoretical aspects, motivational and others)
• Comprehensive review and practice of the use and application of Comprehensive review and practice of the use and application of
the “measurement instruments” specifically designed.the “measurement instruments” specifically designed.

Education program for diagnosis and prevention of diabetic nephropathy in Mexico
Project phases:Project phases:
Phase IVPhase IV
• Experimental protocol implementationExperimental protocol implementation
– Educational activitiesEducational activities
– Monitoring of educational activitiesMonitoring of educational activities
– Application of “measurement instrument” in an anonymous pattern using an “alias” for each general Application of “measurement instrument” in an anonymous pattern using an “alias” for each general
practitioner (control and experimental)practitioner (control and experimental)
– Patient selection and questionnaire application to explore potential impact of medical education on Patient selection and questionnaire application to explore potential impact of medical education on
information provided (or not) to patients (control vs experimental centers)information provided (or not) to patients (control vs experimental centers)
– Random patient chart selection to explore diagnostic and prescription changes (experimenta Vs. control Random patient chart selection to explore diagnostic and prescription changes (experimenta Vs. control
centers)centers)
Phase VPhase V
• Analysis of dataAnalysis of data

Quantitation of ResultsQuantitation of ResultsComparative evaluations of experimental group (before Comparative evaluations of experimental group (before
and after) and of experimental with control centersand after) and of experimental with control centers
• Knowledge, attitude and motivation related to diagnostic and Knowledge, attitude and motivation related to diagnostic and therapeutic conducts before and after (15 days, 1,3 and 6 mo.) therapeutic conducts before and after (15 days, 1,3 and 6 mo.) exposure to education.exposure to education.
• Comparison with control centers in these same issues (before Comparison with control centers in these same issues (before education and at 6 months).education and at 6 months).
• Patient questionnaire about medical indications and physicians Patient questionnaire about medical indications and physicians recommendations (6 months, experimental vs. control). recommendations (6 months, experimental vs. control). (sample)(sample)
• Patient chart comparisons on indications and prescriptions Patient chart comparisons on indications and prescriptions after educational manouever (6 months, experimental vs. after educational manouever (6 months, experimental vs. control). control). (sample)(sample)
Education program for diagnosis and prevention of diabetic nephropathy in Mexico

Presentation and Initial Project DiscussionPresentation and Initial Project Discussion
Presentation and Training of Nephrologist on the Educational Project
Health Centers: General PractitionersHealth Centers: General Practitioners
Random Selection of HCRandom Selection of HC
Exposure to the educational manouever
ControlControl
Evaluation of knowledge
Evaluation of the educational manouever
Education program for diagnosis and prevention of diabetic nephropathy in Mexico
Evaluation of knowledge,
before
15 days, 1, 3 y 6 months after: Knowledge evaluation
Practice change evaluation (6 months)

What can a succesful project do for ISN/COMGAN?
What can ISN/COMGAN do to support the project?

Prevention May Give us an Opportunity to Improve Global
Health Equity
One small ecosystem = Planet Earth
One small world in which we all should fit and have an opportunity to develop
One small planet full of inequities and underdevelopment that need to be overcome


















