Focus on Falls The importance of vision in preventing falls.

Preventing Falls by Providing a Good
Night’s Sleep
Sue Ann Guildermann RN, BA, MADirector of Education, Empira

How’d we get here?• We completed a three year PIPP Fall Prevention
program in 2011 to investigate and identify the roo t causes of resident falls in 16 skilled nursing faci lities
• From the Fall Prevention Program, we identified that sleep fragmentation at night and the lack of activity during the day were significant conditions that contributed to residents falling
• We spring boarded off of our previous PIPP Fall Prevention Program into Restorative Sleep
• We needed to become knowledgeable in the etiology of sleep and wake

Using root cause analysis to determine reasons for residents’ falls:
RCA is a process to find out what happened, why it happened, and to determine what can be done to prevent it from happening again.

Tools to determine RCA
• RCA: Check, Call, Care• “10 RCA Questions”• Post Fall Huddle• Staff Interviews
• FSI Report• Rounding Needs for 4Ps• MDS, QM/QI Report
Fall Scene Investigation (FSI) Report
IDT Falls Committee Meeting

When you (all staff) see a resident who has fallen, do the following:
1. Immediately go to the resident, stay with the resid ent
2. If you are not a nurse, call for a nurse
3. Encourage the resident not to move
4. Ask them, “What were you doing just before you fell ?” or “What were you trying to do just before you fel l?”
5. Begin getting answers to the “10 Questions”
6. Stay for the fall huddle, assist in getting a fall huddle started

10 Questions at the time a resident falls. Stay with resident, call nurse.
1. Ask resident: Are you ok?2. Ask resident: What were you trying to do?3. Ask resident or determine: What was different thi s time?4. Position of Resident?
a. Did they fall near a bed, toilet or chair? How far away?b. On their back, front, L side, or R side?c. Position of their arms & legs?
5. What was the surrounding area like? a. Noisy? Busy? Cluttered?b. If in bathroom, contents of toilet?c. Poor lighting – visibility?d. Position of furniture & equipment? Bed height c orrect?
6. What was the floor like? a. Wet floor? Urine on floor? Uneven floor? Shiny floor?b. Carpet or tile?
7. What was the resident’s apparel?a. Shoes, socks (non-skid?) slippers, bare feet?b. Poorly fitting clothes?
8. Was the resident using an assistive device?a. Walker, cane, wheelchair, merry walker, othe r
9. Did the resident have glasses and/or hearing aid es on ?10. Who was in the area when the resident fell?

Fall Huddle(ground zero)
• Performed immediately after resident is stabilized
• Charge nurse has all staff, working in the area of the fall, meet together to determine RCA
•
• Review “10 Questions” with staff• Also ask staff:
• “Who has seen or has had contact with this resident within the last few hours?”
• “What was the resident doing?” • “How did they appear? How did they behave?”
Fall Scene Investigation (FSI) Report
• Post fall investigation form
• Data collection tool used to assess clues and evidence to determine RCA
• Completed soon after the fall occurs and/or during the fall huddle
• Completed by nurse in charge on duty at time of the fall
• Sent electronically to Empira where the software program collates, aggregates and determines trends and patterns

Assessing for the Needs of 4 Ps• Position:
• Does the resident look comfortable? • Does the resident look bored, restless and/or agita ted?• Ask the resident, “Would you like to move or be repo sitioned?”• Ask the resident, “Are you where you want to be?” Re port to the nurse.
• Personal (Potty) Needs:• Ask the resident, “Do you need to use the bathroom?” • Ask if they’d like help to the toilet or commode. Report to the nurse.
• Pain:• Does the resident appear in to be uncomfortable or in pain? • Ask the resident, “Are you uncomfortable, ache or ar e in pain?”• Ask them what you can do to make them comfortable. • Report to the nurse.
• Placement:• Is the phone, call light, remote control, tissue s, walker, trash can,
water, urinal, all near the resident? Can they e asily see them?• Place them all within easy reach. Are they in cont rast to background?• Is the bed at the correct height?

• External causes: busy activity, la ck of environment contrasts, placement of furniture, equipment & personal items, floor surfaces
• Internal causes: Poor balance, sleep deprivation/ sleep fragmentation, need for the 4Ps, medications (type & amt), orthostatic B/P, lack of endurance
• Systemic causes: Time of day, shift change/times, break times, day of week, location of fall, type o f fall, routine staff assignments, staffing levels
Noise,

External lesson learned:if we can stop the noise,
then we can reduce the falls.

Noise – Where is it? What’s causing it?
Who’s causing it?

Internal lesson learned:
if we can stop disturbing sleepthen we can reduce the falls.
RSVP: Sleep and WakeChallenges & Interventions
• CMS and LTC providers have never considered sleep as an integral part of the plan of care and services provided for the resident.
• MDS 3.0: “Over the last 2 weeks, did the resident have any of the following problems: trouble falling or staying asleep, or sleeping too much?” and “How important is to you to go to bed when you want?”

Empira’s RSVP:Restorative Sleep Vitality Program
• This program is a combination of nationally recognized evidence-based, sleep hygiene research studies and the application of cutting edge practices to enhance residents’ sleep & wake
• Empira is challenging some of the standards of practice and operational procedures for providing cares and services in skilled nursing facilities
• Empira staff and corporate representatives attend national & international sleep conferences and conventions to learn and educate membership

Background & Process• Empira awarded 3-year MN DHS PIPP grant, began 10/1 /11
~ A project implementing best practices from eviden ce based studies
~ Reduction Goal: • Undisturbed sleep at night, w/o any negative effect s• Fully awake & engaged during the day, w/o negative effects
~ Goal: Reduce baseline average for 5 CMS QI/QMs a nd Vital ResearchQuestions, “Can you get up in the morning when you want?” , “Can you go to bed when you want?” , “Are you bothered by noise when you are in your room?” , “Are there things to do here that you enjoy?”
• 23 SNFs, 4 companies participate in PIPP, RSVP project
• RSVP Leader in each SNF reports to administratorwho oversees the program – it’s not a nursing progra m!
• Project completion date: 10/1/14
Restorative Sleep Vitality P rogram: Goal:
• Undisturbed sleep at night– without experiencing any negative effects

Restorative Sleep Vitality P rogram: Goal:
• Fully awake & engaged during the day– without experiencing any negative effects

How Do We Sleep?How Do We Wake?
The Etiology of Sleep and Wake:

Serotonin secretion starts
20:00 Serotonin secretion stops(8:00PM)
Human Circadian Clock: Ideal 24 Hours
Lowest blood pressure
Greatest healing and growth occurs
(3:30 PM)
(6:00 PM)

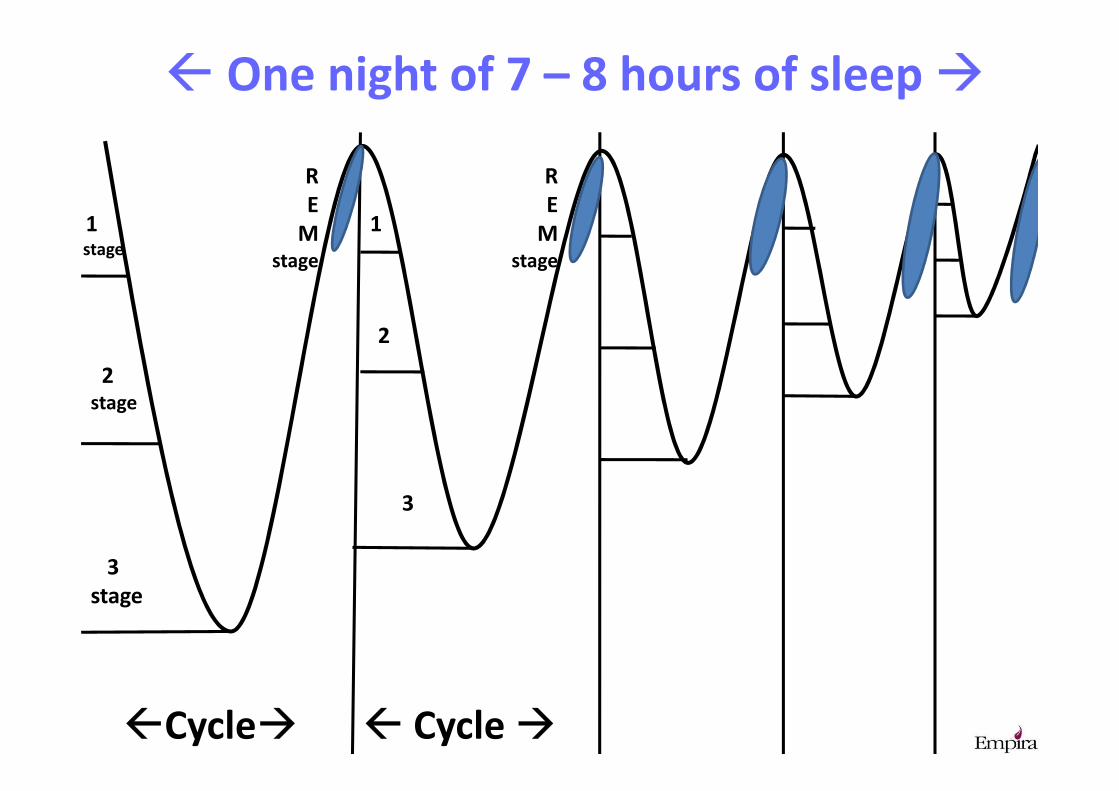
Sleep: Cycles & Stages
• In humans, an average 7 – 8 hour night’s sleep should contain 4 – 5 sleep cycles.
• Each cycle should last 90 to 120 minutes.
• Each cycle has 3 Non –REM stages and 1 REM stage of sleep.
• Each stage provides distinct physiological and emotional benefits for the body.
1stage
2stage
3
stage
R
E
Mstage
1
2
3
R
E
Mstage
�Cycle�
� One night of 7 – 8 hours of sleep �
� Cycle �

Tests for Sleep • Sleep, its stages and
characteristics, assessed by tests in sleep labs.
• Tests that identify the sleep and wake cycles include, polysomnography:Electroincephlogram (EEG) measuring the
electrical activity of the brain, or brain wavesElectrooculography (EOG) measuring eye
movements, Electromyography (EMG) measuring the skeletal
and muscle activity/tonicity,• Actigraphy

Actigraphy:
• Measures Rest and Sleep• Measures Activity and Tonicity• Measures Light Source and Quantity of
Light source• Over a 24 Hour Period• Worn continuously for
multiple days• Worn on the wrist• Cost effective
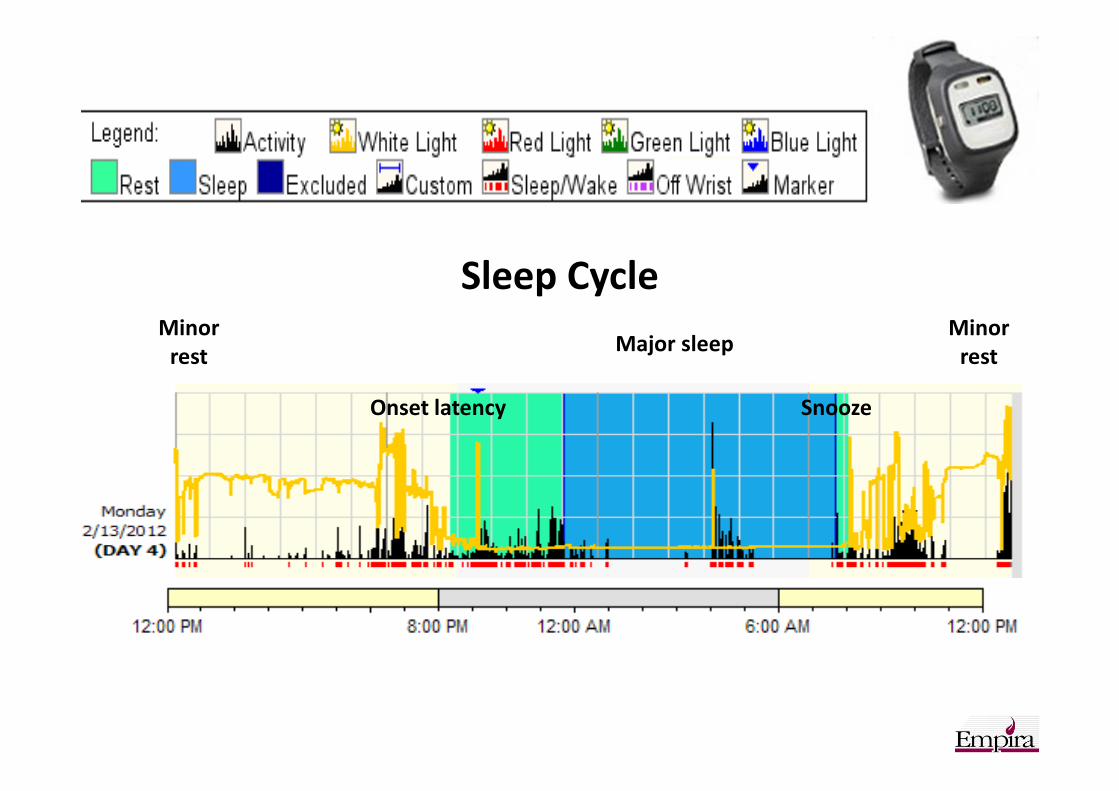
Sleep CycleMinor
rest
Minor
rest
Onset latency Snooze
Major sleep

The human body has evolved to function optimally in the upright position for about 16 hours a day. Average adult sleeps 7 - 8 hours a day , in a supine position.
Consistently sleeping for more than 9 hours or fewe r than 8 hours a day has a negative impact on physiological, psychological and cogni tive functions.
(Van Dongen et al, 2003)
gastric reflux and constipation
progressive slowing down of metabolic rate, reduction in insulin sensitivity
urinary retention,increased risk of urinary tract infections
increased anxiety, confusion and depression, impaired memory function
dehydration, progressive cardiac de-conditioning, postural hypotension
reduced lung function,increased susceptibility to respiratory infection
venous stasis and blood vessel damage
loss of muscle strength and endurance
osteoporosis
altered skin integrity

Implementing theRestorative Sleep Vitality Program
• What disturbs sleep?
– Identify environmental factors.
– Identify clinical factors.
– Identify operational factors.
• What keeps people awake?
– Identify environmental factors.
– Identify clinical factors.
– Identify operational factors.

Top Disturbances to Sleep
1. Noise
2. Light
3. Sleeping Environment: surface/mattress, temp, bedding
4. Napping
5. Medications
6. Continence Needs
7. Pain
8. Positioning
9. Inactivity/activity
10. DietHarvard Sleep Study, 2011

Root Cause Analysis: Disturbances to Sleep
• What are the causes for the disturbances to sleep?
• Eliminate the disturbances to sleep
• Prioritize – grab the low hanging fruit first
– do the easier, quicker successes first
– then take on the greater challenges

Greatest Challenge to Undisturbed Sleep at Night: Skin Conditions & Repositioning• Nancy Bergstrom, PhD., U of Texas at Houston,
“Turning for Ulcer ReductionN,” Journal of the
American Geriatrics Society, Vol. 61, Issue 10,
Pages 1705–1713, October 2013.
http://onlinelibrary.wiley.com/doi/10.1111/jgs.
12440/pdf
• Jeri Lundgren, RN, BSN, CWS. Wound Care Advisor,
“Turning Programs Hinder a Good Nights Sleep.”
March/April 2014, Vol. 3 No. 2.
http://woundcareadvisor.com/turning-programs-
hinder-a-good-nights-sleep-vol3-no2/

Greatest Challenge to Undisturbed Sleep at Night: Incontinence
• Increase fluid intake in the morning hours
• Taper fluid intake as day progresses
• Reduce fluid intake after the evening meal
• No bedside water pitcher after the evening
meal, unless requested by the resident or
indicated by medical condition
• Use correct “overnight” incontinent product

Did the Restorative Sleep Vitality Program
help to reduce falls even more?

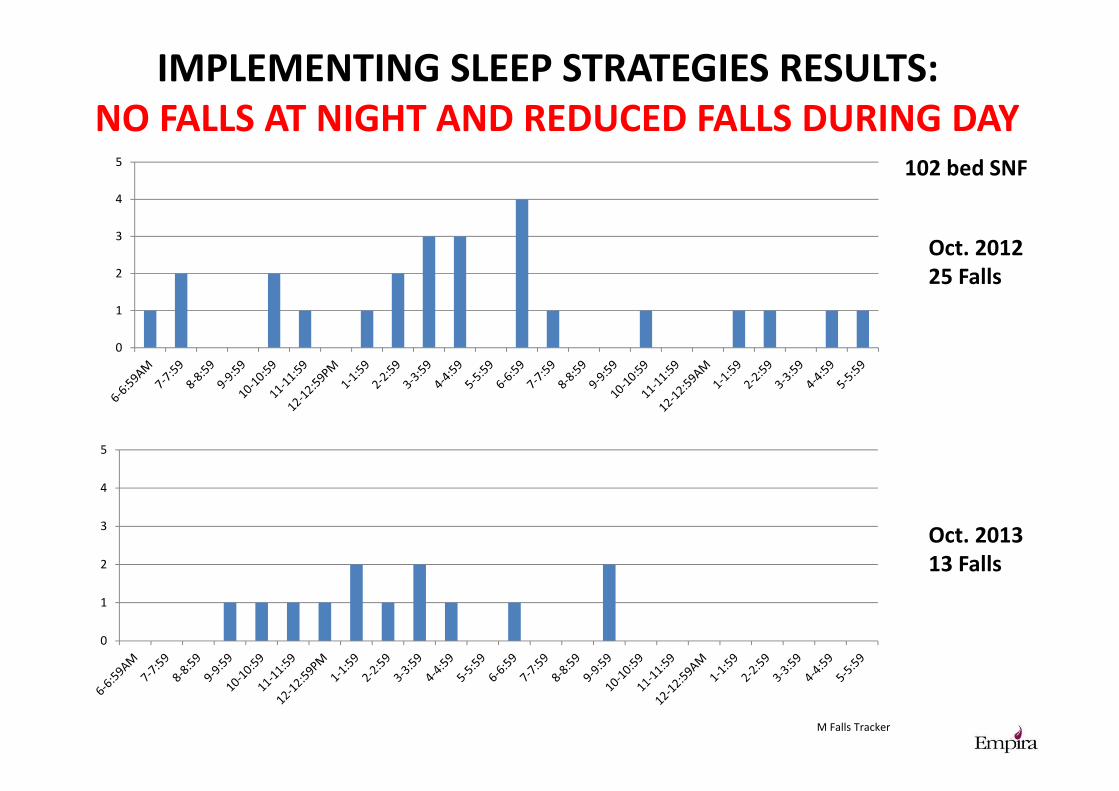
IMPLEMENTING SLEEP STRATEGIES RESULTS:
NO FALLS AT NIGHT AND REDUCED FALLS DURING DAY
0
1
2
3
4
0
1
2
3
4
December
2012
17 falls
December
2013
9 falls
SE Falls Tracker
65 bed SNF
IMPLEMENTING SLEEP STRATEGIES RESULTS:
NO FALLS AT NIGHT AND REDUCED FALLS DURING DAY
0
1
2
3
4
5
0
1
2
3
4
5
Oct. 2012
25 Falls
Oct. 2013
13 Falls
M Falls Tracker
102 bed SNF

Comparison Report: 2011 2012 2013
Awake in Room:
9 - 11p.m. 23% 25% 13%
11 - 1:00a.m. 14% 7% 8%
1 - 4:00a.m. 13% 2% 1%
4 - 6:00a.m. 8% 2% 1%
Personal Alarms Sounded:
9 - 11p.m. 9% 0% 0%
11 - 1:00a.m. 9% 0% 0%
1 - 4:00a.m. 9% 0% 0%
4 - 6:00a.m. 3.5% 0% 0%
Passing Water/Stocking Incontinent Products in Rooms:
9 - 11p.m. 100% 0% 0%
11 - 1:00a.m. 0% 0% 0%
1 - 4:00a.m. 0% 0% 0%
4 - 6:00a.m. 0% 0% 0%
Percentage of Residents who have 2 hour Checks and/or Change:
99% 58% 7%