Preventative telehealth supported services for early stage chronic obstructive pulmonary disease:...
24
Preventative telehealth supported services for early stage chronic obstructive pulmonary disease: Lessons from a pilot randomised controlled trial Deborah A. Fitzsimmons 1 Claire Bentley 2 , Gail A. Mountain 2 Jill Kenny 2 , Kinga Lowrie 2 , Stuart G Parker 2 , Mark S Hawley 2 1 School of Health Studies, University of Western Ontario, London, ON, Canada 4 School of Health and Related Research, University of Sheffield, Sheffield, UK
-
Upload
karen-wickers -
Category
Documents
-
view
217 -
download
0
Transcript of Preventative telehealth supported services for early stage chronic obstructive pulmonary disease:...

Preventative telehealth supported services for early stage chronic obstructive pulmonary disease: Lessons from a pilot
randomised controlled trial
Deborah A. Fitzsimmons1
Claire Bentley2, Gail A. Mountain2 Jill Kenny2, Kinga Lowrie2, Stuart G Parker2, Mark S Hawley2
1 School of Health Studies, University of Western Ontario, London, ON, Canada 4 School of Health and Related Research, University of Sheffield, Sheffield, UK
Faculty/Presenter Disclosure• Faculty: Deborah A. Fitzsimmons PhD
• Relationships with commercial interests: None
• This program has received financial support from:
The National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care, South Yorkshire (CLAHRC SY) in the form of grant funding for the research team.
• This program has received in-kind support from: NHS Barnsley and Barnsley Metropolitan Council in the form of staff time and the procurement of the devices.

UK trial - Barnsley
Barnsley characteristics
• Aging Population– 2008 – 2031: Population increase by 16%
65 – increase by 67%75 – increase by 80.5%
• History of coal mining history
• One of most deprived areas– Adverse lifestyle factors (diet, smoking)
• High incidence of COPD– 2.5% vs. UK avg. of 1.5%

ᬅ Patient uses Doc@HOMEtechnology to take daily readings
ᬅ�Readings are sent via telephone line to the
Doc@HOME secure server
ᬇ PCT staff access the server daily to check patient data and prioritise their workloadᬇ�PCT staff will contact
patients if an alert is triggered by the doc@HOME system
ᬉ doc@HOME system provides patient education through feedback of their readings
The Technology

COPD RCT
Time Line
Standard COPD
Service
(Control)
Tele-health
Supported COPD
Service
First home visit after hospital
discharge (Baseline (time 0)
Home visit Home visit
3 days Home visit Home visit
5 days Home visit Telehealthequipment
installed
2 weeksHome visit Remote review of
telehealthparameters
6 weeksHome visit
8 weeksDischarge Home
visitDischarge Home
visit
8 months Measurement of outcomes
Outcome measures
• Re-admitted to hospital with COPD
• Change in self-reported health status and quality of life at baseline, 8 weeks and eight months after start of service
• Requiring unscheduled healthcare support
• Cost effectiveness through quality adjusted life years (QALYs)

Innovative Partnership
Barnsley HospitalBarnsley Primary
Care Trust
Barnsley Metropolitan
Borough Council

Care Pathway
Patient admitted to hospital with COPD
Patient discharged from hospital
Patient accepted on COPD service
Patient discharged from service
8 week service
Equipment removed
Equipmentinstalled
Patient referred to COPD service
HOSPITAL PCT COUNCIL
Repairs / replacement
Equipment maintained /
cleaned
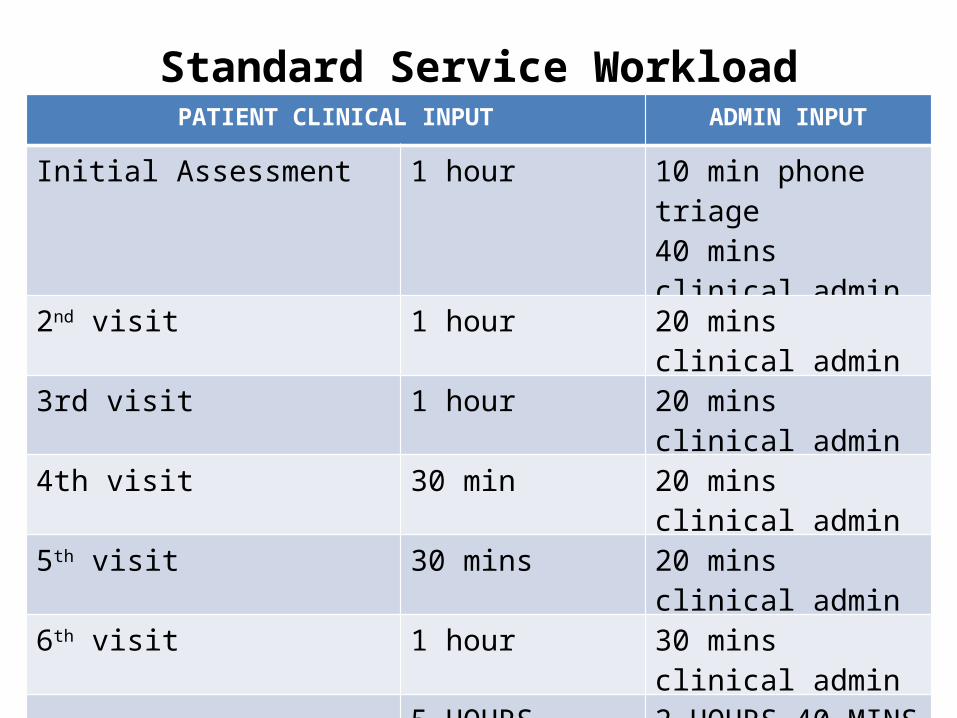
Standard Service WorkloadPATIENT CLINICAL INPUT ADMIN INPUT
Initial Assessment 1 hour 10 min phone triage40 mins clinical admin
2nd visit 1 hour 20 mins clinical admin
3rd visit 1 hour 20 mins clinical admin
4th visit 30 min 20 mins clinical admin
5th visit 30 mins 20 mins clinical admin
6th visit 1 hour 30 mins clinical admin
5 HOURS 2 HOURS 40 MINS
10% tolerance for cancellations
45 MINS
TOTAL WORKLOAD 8 HOURS 25 MINS
UNIT CAPACITY 371 PATIENTS p.a.
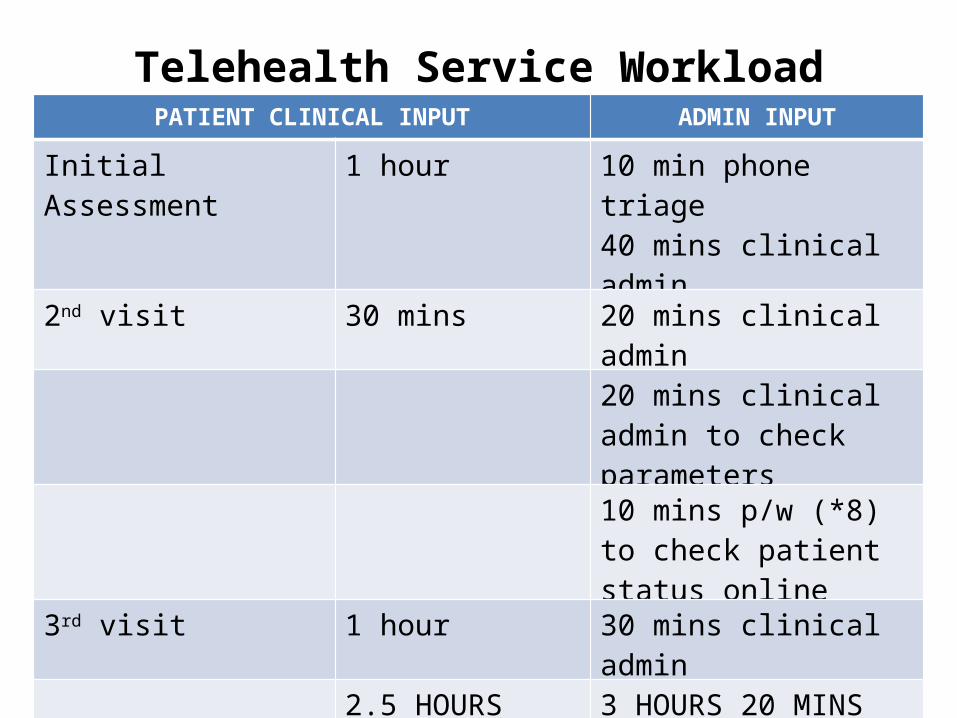
Telehealth Service WorkloadPATIENT CLINICAL INPUT ADMIN INPUT
Initial Assessment 1 hour 10 min phone triage40 mins clinical admin
2nd visit 30 mins 20 mins clinical admin
20 mins clinical admin to check parameters
10 mins p/w (*8) to check patient status online
3rd visit 1 hour 30 mins clinical admin
2.5 HOURS 3 HOURS 20 MINS
10% tolerance for cancellations
35 MINS
TOTAL WORKLOAD 6 HOURS 25 MINS
UNIT CAPACITY 487 PATIENTS p.a. 31.2% increase
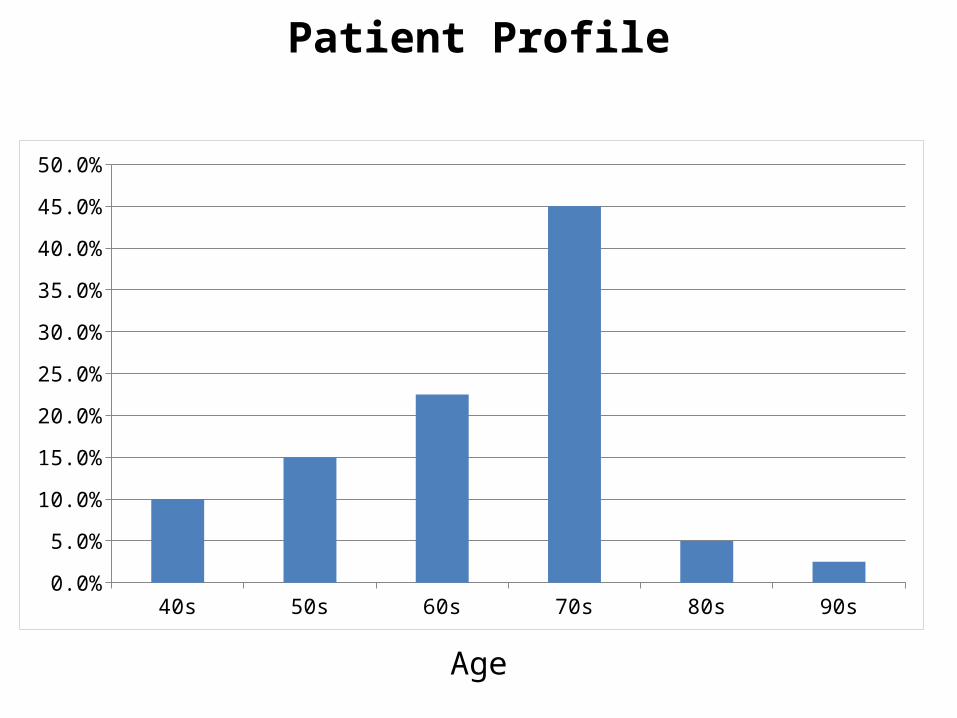
40s 50s 60s 70s 80s 90s0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
Patient Profile
Age

What do users really think of tele-health
monitoring? Quotes from interviews with users
with COPD
“It became a bit of a chore”
“I’m lost without it”
“I can stay at home and feel
safe”
“It didn’t do anything for me – it
didn’t build my confidence or anything like
that”
“It’s like having someone to
turn to”
“I knew someone was watching and any indication
that I was getting ill or anything, they’d get in
touch”
“I knew somebody was keeping an eye on me
which was the main thing – there’s somebody there
for you
“I haven’t been back to hospital since that machine
came in”
“It’s one of the best things... I showed it to the chap who lives two doors away... They are going to
put him on it”
“The best service I’ve ever had”
“It was quite simple to use...It’s not rocket
science is it?”
“The questions, they were a bit puzzling sometimes... The (answers) ought to be more in-between instead of
black and white”
Patient Views of Tele-health


RCT Eligibility Criteria
• Male or female over age of 16• Discharged from hospital with COPD as
primary or secondary diagnosis• 1 – 3 hospital admissions in prior 12 months
for COPD including this discharge– PCT definition of early stage COPD
• Willing to use telehealth • Home landline in place• Able to read English (technology requirement)
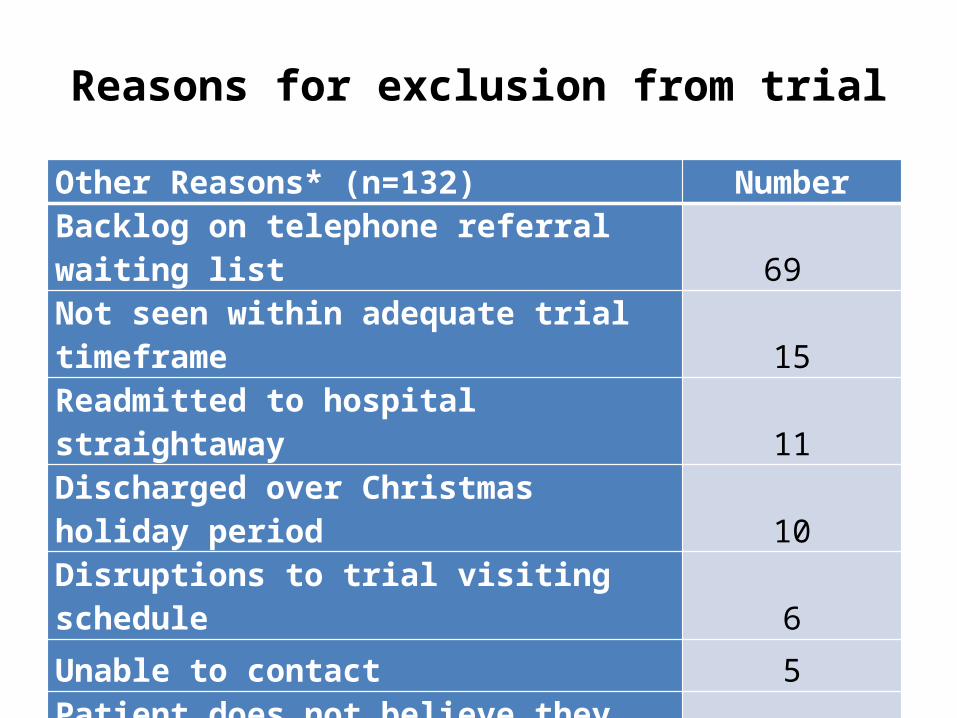
Reasons for exclusion from trial
Other Reasons* (n=132) Number
Backlog on telephone referral waiting list 69
Not seen within adequate trial timeframe 15
Readmitted to hospital straightaway 11
Discharged over Christmas holiday period 10
Disruptions to trial visiting schedule 6
Unable to contact 5
Patient does not believe they have COPD 4
Other 12
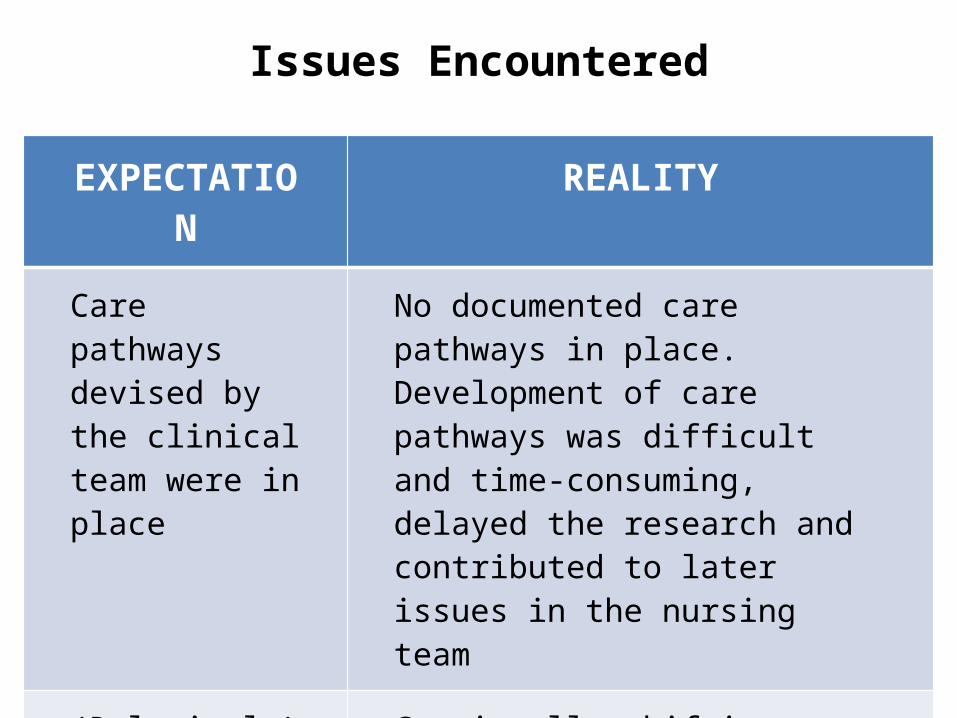
EXPECTATION REALITY
Care pathways devised by the clinical team were in place
No documented care pathways in place. Development of care pathways was difficult and time-consuming, delayed the research and contributed to later issues in the nursing team
(Relatively) stable NHS environment with a team that had been in place for some years
Continually shifting structures within the NHS and internal politics between teams (e.g. new COPD community nursing service perceived as threatening existing service)
Issues Encountered

EXPECTATION REALITY
Technical procedures and necessary resources for the service were in place
Resources/routines between the partners delivering the service to manage de/installation and cleaning of units took time to establish
Readings can be automatically sent via telephone line to the secure server
Technical issues prevented use of the device with certain landline companies
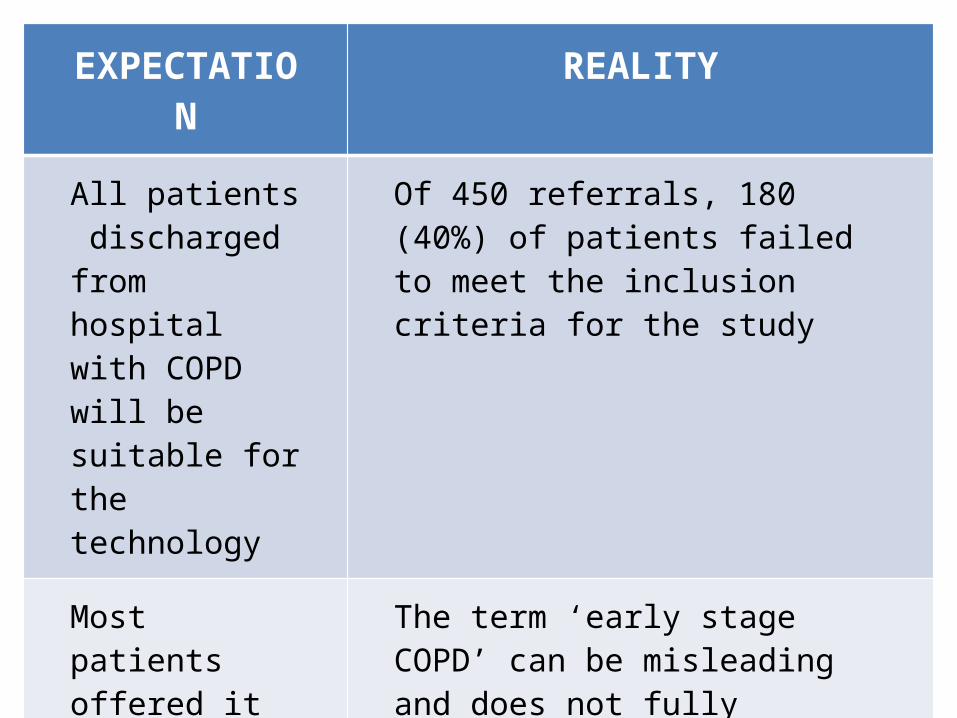
EXPECTATION REALITY
All patients discharged from hospital with COPD will be suitable for the technology
Of 450 referrals, 180 (40%) of patients failed to meet the inclusion criteria for the study
Most patients offered it will accept the technology
The term ‘early stage COPD’ can be misleading and does not fully reflect the state of ill health experienced by this patient population. Many participants were simply too ill to take part at the time that they were provided with information about the services
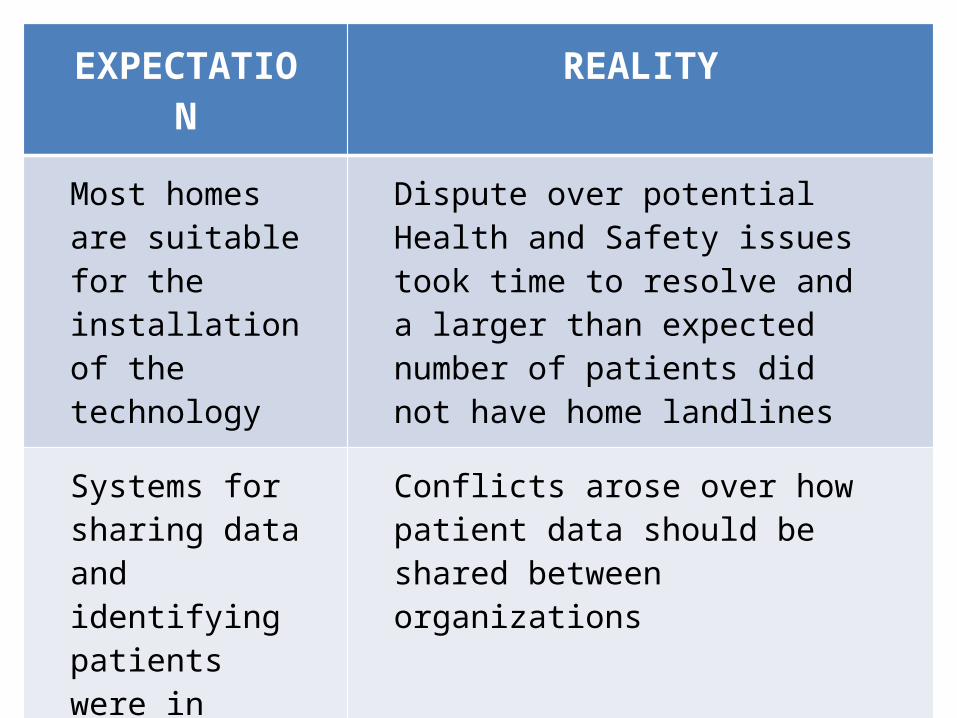
EXPECTATION REALITY
Most homes are suitable for the installation of the technology
Dispute over potential Health and Safety issues took time to resolve and a larger than expected number of patients did not have home landlines
Systems for sharing data and identifying patients were in place
Conflicts arose over how patient data should be shared between organizations
Common language base
Miscommunications occurred between different teams, possibly due to different vocabularies, priorities and team changes
EXPECTATION REALITY
Working with a small team would facilitate training and operationalizing the trial
Staff illness and absence had a higher impact in terms of capacity and morale

Outcomes of the Pilot
• Planned to recruit 60 patients in 3 months (30 per arm)
• Recruited 63 (randomized 5 with no/unsuitable landline) so needed to recruit 65 patients in total but this took 12 months
• Lack of funding and support for full trial– Staff to be reassigned in organization shuffle– Testing alternate technology / approach introduced
by new department management
References
Telehealth RCT protocol:Fitzsimmons, D.A., Thompson, J., Hawley, M., Mountain, G.A.,
http://www.trialsjournal.com/content/12/1/6.
Thank you
Any questions?