Pressure Ulcer Management By Susan Yap, PT. Anatomy of the Skin Epidermis Dermis Subcutaneous Tissue...
26
Pressure Ulcer Management By Susan Yap, PT
-
Upload
allyson-hutchinson -
Category
Documents
-
view
220 -
download
0
Transcript of Pressure Ulcer Management By Susan Yap, PT. Anatomy of the Skin Epidermis Dermis Subcutaneous Tissue...
Pressure Ulcer Management
By Susan Yap, PT

Anatomy of the Skin
Epidermis Dermis Subcutaneous Tissue Fascia Muscle Tendon and Bone

Functions of the Skin
Protection Regulates Body Temperature Sensation

Effects of Aging on Skin
Dehydration Reduced Subcutaneous Fat Decreased Vascularization Decreased Elasticity

Physiology of Wound Healing
Healing by primary intention- wound edges are brought together and sutured
Healing by secondary intention- wound edges are not brought together and must heal by granulation, contraction and epithelialization

Phases of Wound Healing
1. Inflammatory Phase Acute Phase = Vasoconstriction and clot formation Followed by demolition phase Chronic inflammation results in wound is overwhelmed by necrotic tissue Characteristics: Edema, Erythema, Pain, Necrotic tissue and Exudate
2. Proliferative Phase Granulation Tissue fills wound bed Angiogenesis Epidermal cells migrate across granulation tissue Contraction of wound edges Characteristics: Deep red granulation tissue, Transudate, Epithelialization
occurring
3. Maturation Phase Increase in tensile strength through collagen synthesis Resulting scar tissue 70-80% as strong as original skin Characteristics: Decrease vascularization, Increase tensile strength,
Decrease size of scar

Pressure Ulcer
Any lesion cause by unrelieved pressure resulting in damage of underlying tissue ; usually over a bony prominence.
Risk Assessment Impaired circulation Impaired Mobility Predisposing Illness or medication that
impair healing Decrease mental status Incontinence Nutritional deficits Patients with existing pressure ulcer Non compliance

Early Intervention
Team Effort Address functional mobility and
ROM Continence training Education Positioning Pressure relieving/reducing devices
Mechanical Loading and Support Surfaces Bed bound Chair bound Avoid positioning directly on the
trochanters Positioning devices to relieve all pressure
from the heels and to prevent direct contact to bony prominences
Prevent sheer injury Ring cushions should be avoided Support surfaces

Initial Evaluation
Holistic approach Functional mobility and ROM Nutritional status Pain level Psychosocial health Common complications of pressure
ulcer
Wound Assessment
Etiology Location Size

Pressure Ulcer Stage I - Red non-blanchable Stage II - Partial thickness skin loss Stage III – Full thickness skin loss
involving underlying subcutaneous tissue
Stage IV – Full thickness skin loss with extensive destruction damage to muscle bone

Stage I

Stage II

Stage III
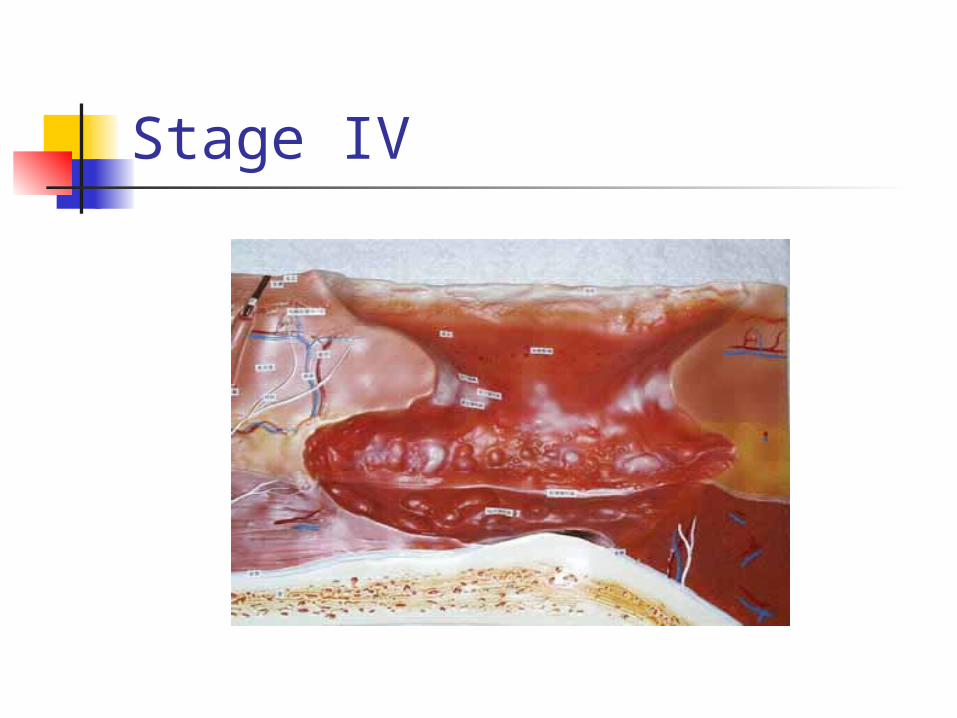
Stage IV

Viable Tissue
Granulation Epithelialization

Necrotic/Nonviable Tissue
Eschar Slough
Drainage/Exudate
Amount Transudate/serous Purulent
Odor
Describe Intensity Result of autolytic debridement or
dressing
Developing Goals
Process Oriented Measurable Time Oriented

Debridement
Mechanical Sharp Enzymatic Autolytic

Dressings
Cardinal rule keep ulcer tissue moist Eliminate dead space by loosely
packing Control exudate Cost effective Time effective Location of wound

Things to remember Communication
with Physicians Documentation Risk Management Education Quality
Improvement