
Press Conference - International Association for the Study...
46
Press Conference Wednesday, Sept. 9, 2015 9:45 a.m. – 10:45 a.m. MDT Dial-In Information & Agenda: wclc2015.iaslc.org/press-media/ Please hold all questions until the end.
Transcript of Press Conference - International Association for the Study...

Press ConferenceWednesday, Sept. 9, 2015
9:45 a.m. – 10:45 a.m. MDTDial-In Information & Agenda:
wclc2015.iaslc.org/press-media/Please hold all questions until the end.

David R. Gandara, MDUniversity of California Davis
Comprehensive Cancer Center
“Science Drives Advances in Lung Cancer” at WCLC 2015:
“Eating the Elephant”

“Eating the Elephant:”An analogy to defeating cancer
“ If you want to eat an elephant, you need a strategy”
“ If you try to do it in one bite, you willchoke on it”
M. Vestager. – May 25, 2015EU Antitrust Chief
& Danish politician

World Conference Lung Cancer (WCLC) 2015:Science Drives Lung Cancer Advances
WCLC 2015
Prevention, Screening,
Tobacco Control
Biology, Pathology, Molecular
Diagnostics
Treatment
Palliative Care,
Nursing, Advocacy
Plus Other Thoracic
Malignancies
Multidisciplinary Research Teams
“Transformative”-Clinical Practice
-Standards of Care
“Personalized Care”
“Bench to Bedside”

Refining the Concept of “Bench to Bedside”Basic
Laboratory Research
Translational Research
(Clinical Trials)Clinical Care
Discovery of “Driver”
Oncogenes
Development of Predictive Biomarkers
(Clinical Trials)
Biomarker-driven patient
care(e.g. EGFR TKIs)
Technology for Next
Generation Sequencing
(NGS)
Development of NGS for Predictive
Biomarkers(Clinical Trials)
NGS-driven patient care
(e.g. Genomic-driven therapy)
Understanding of PD-L1biology
Development of Predictive Biomarkers
(Clinical Trials)
PD-L1-directed patient care
(Biomarkers??)

The field of Oncology has never moved at a faster pace than now (The future is now)Basic
Laboratory Research
Translational Research
(Clinical Trials)Clinical Care
Technology for Next
Generation Sequencing
(NGS)
Development of tumor NGS for Predictive Biomarkers
(Clinical Trials)
NGS-driven patient care
(e.g. Genomic-driven therapy)
Technology for Next Generation
Sequencing (NGS)in plasma(cfDNA)
Development of plasma NGS for
Predictive Biomarkers
(Clinical Trials)
Plasma NGS-driven patient care
(e.g. Genomic-driven therapy)
Few would have predicted the rapid pace of these transitions which are “Transformative”

How did we get to this point so fast?Basic
Laboratory Research
Translational Research
(Clinical Trials)Clinical Care
Discovery of “Driver”
Oncogenes
Development of Predictive Biomarkers
(Clinical Trials)
Biomarker-driven patient
care(e.g. EGFR TKIs)
Technology for Next
Generation Sequencing
(NGS)
Development of NGS for Predictive
Biomarkers(Clinical Trials)
NGS-driven patient care
(e.g. Genomic-driven therapy)
Understanding of PD-L1biology
Development of Predictive Biomarkers
(Clinical Trials)
PD-L1-directed patient care
(Biomarkers??)

Li, Mack, Gandara et al. JCO. 2013 (adapted from Pao et al).
Evolution of NSCLC Subtyping From Histologic to Molecular-Based
NSCLCas one disease
EGFR

From Li, Gandara et al. JCO. 2013.
Integration of Biomarkers Into Clinical Practice: Past, Current & Future
Near-Future Approach (Patient-Based Therapy):Genomic profiling by high throughput next generation sequencing
for decision-making in individual patients
1. HistomorphologicalDiagnosis: Cancerous
Evolving Approach (Target-Based Therapy V2.0):Multiplexed molecular tests with increased sensitivity & output
for decision-making in individual patients
Current Approach (Target-Based Therapy V1.0):Single gene molecular testing for decision-making in individual
patients
2. Molecular Diagnosis:Extract tumournucleic acids:
Archival cancer specimensArchival FFPE tumour
specimens
Macro- or Micro-dissection of
Tumours
DNA and RNA
Empiric Approach (Past)(Compound-Based Therapy):
Clinical-histologic factors to select drugs for individual patients
Representative technologies:
Single Biomarker Tests:• Sanger DNA Sequencing
• RT-PCR• FISH• IHC
Multiplex, Hot Spot Mutation Tests:• PCR-based SNaPshot
• PCR-based Mass Array SNP• Sequenom
Initial High-Throughput Technologies:• SNP/CNV DNA microarray
• RNA microarray
Next-Generation Sequencing (NGS):• Whole Genome or Exome Capture Sequencing (DNA)• Whole or Targeted Transcriptome Sequencing (RNA)
• Epigenetic profiling
Plasma cfDNA by NGS

Based on cfDNA analysis, patient tarted on clinical trial of 3rd gen EGFR TKI AZ9291Repeat PET scan 2 weeks later: Major Response.
Case Example: 50 y/o woman with EGFR-mutated lung cancerAt relapse after TKI, re-biopsy shows EGFR E19del, T790M-
Next Step: Plasma Next Gen Sequencing for cell free (cf)DNA
At start of AZD9291
2 weeks after
Lessons learned from this case?Rapid change in the diagnostic & therapeutic landscape
We better have our “running shoes” on if we are to keep up.

Rationale for Checkpoint Immunotherapy• Cancer cells have mutations that make them
recognizable by the immune system (neo-antigens)
• Cancer cells can evade immune surveillance by expressing proteins such as PD-L1 (a potential biomarker)
• Inhibiting PD-L1/PD-1 can restore anti-tumor T-cell activity, leading to
immune-mediated response
Cancer cells evade
T cell killing by
expressing PD-L1
XPD-1
PD-L1MHC I
T cell receptor
Tumor cell
CD8+ CytotoxicT Lymphocyte
(CTL)
Mutation
B7.1
PD-L1 biomarker correlates with response-True in Non-squamous-Not true in Squamous
lung cancer
Paz-Ares: ASCO 2015Spigel: ASCO 2015

GDC-0032 Vs SoC
PalbociclibVs SoC AZD4547
Vs SoC
FGFR1CDK4/61PI3K1
Non-matchImmunotherapy Sub-studies
Nivo/IpiNivolumab
BMN 673Vs SoC
GDC-0032 Palbociclib AZD4547 BMN 673
Stage 1
Stage 2
HRD2Checkpoint
Naive1
MEDI4736/Treme
Vs SoC
Checkpoint Refractory2
Matched Sub-studies
1 Revision #3: Expected September/October 2015 SoC: Standard of Care therapy2 Revision #4: Expected December 2015/January 2016
Lung-MAP (S1400) Trial for Genomic-driven Therapiesin Advanced Squamous Lung Cancer
(Updated for Fall 2015 with Revs # 3 & 4)
12
Tumor Analysis by Next Gen Sequencing (Foundation Medicine)
PIs: V. Papadimitrakopoulou, R. Herbst

“ If you want to eat(defeat) LUNG
CANCER, you needa strategy”
“Eating the Elephant:An analogy to defeating Cancer
There is no single solution to defeating Lung Cancer.
Like the elephant, it will take many bites.

PLEN04.03: Randomized phase III trial of adjuvant chemotherapy with or without bevacizumab in resectednon-small cell lung cancer (NSCLC): Results of E1505 – Heather Wakelee, USA
Randomized phase III trial of adjuvant chemotherapy with or without bevacizumab in resected non-small
cell lung cancer (NSCLC): Results of E1505
H.A. Wakelee1, S.E. Dahlberg2, S.M. Keller3, W.J. Tester4, D.R. Gandara5, S.L. Graziano6, A. Adjei7, N. Leighl8, S.C. Aisner9, J.M. Rothman10, J. Patel11, M.D. Sborov12, S.R. McDermott13, R. Perez-Soler14, A.M. Traynor15, C. Butts16, T.
Evans17, L. Horn18, S.S. Ramalingam19, J. Schiller20 on behalf of ECOG-ACRIN1Medicine (Oncology), Stanford Cancer Institute/Stanford University, Stanford, CA/USA, 2Dana-Farber Cancer Institute/Harvard University, Boston,
MA/USA, 3Cardiovascular and Thoracic Surgery, Montefiore Medical Center, Bronx, NY/USA, 4Albert Einstein Medical Center, Philadelphia, PA/USA, 5UC Davis Comprehensive Cancer Center, Sacramento/USA, 6Medical Oncology, SUNY Upstate Medical University, Syracuse, NY/USA, 7Medicine,
Roswell Park Cancer Institute, Buffalo, NY/USA, 8Princess Margaret Cancer Centre, Toronto, ON/Canada, 9Rutgers New Jersey Medical School, Newark, NJ/USA, 10The Regional Cancer Center, Erie, PA/USA, 11Northwestern University, Chicago, IL/USA, 12Edina Clinic, Edina/USA, 13Medical
Oncology, The Adelaide and Meath Hospital, Dublin, Dublin/Ireland, 14Oncology, Montefiore Medical Center, Bronx, NY/USA, 15University of Wisconsin, Madison, WI/USA, 16Division of Oncology, University of Alberta, Edmonton, AB/Canada, 17 University of Pennsylvania, Philadelphia, PA/USA,
18Vanderbilt University Medical Center, Nashville, TN/USA, 19Winship Cancer Institute, Emory University, Atlanta, GA/USA, 20Hematology/Oncology, UT Southwestern, Dallas/USA

PLEN04.03: Randomized phase III trial of adjuvant chemotherapy with or without bevacizumab in resectednon-small cell lung cancer (NSCLC): Results of E1505 – Heather Wakelee, USA
RANDOM IZE
1:1
STRATIFIED:
1) Cisplatin Doublet* 2) Stage (~25% IB,~ 50%II,~25% III)3) Histology (~30% Squam)4) Gender (~50:50)
Arm A:ChemotherapyX 4 cycles*
ELIGIBLE: Resected (N=1501)Early stage NSCLC6-12 weeks post-op
Arm B:Chemotherapyx 4 cycles* +Bevacizumab^X 1 year
*Investigator Choice of 4 chemotherapy regimens Cisplatin /Vinorelbine ~25%Cisplatin /Docetaxel ~25%Cisplatin /Gemcitabine ~20%Cisplatin /Pemetrexed ~30%^Bevacizumab 15 mg/kg IV q 3 weeks for up to 1 year
•Adjuvant cisplatin-based chemotherapy for completely resected early stage NSCLC provides a modest overall survival benefit of ~ 5%•Bevacizumab, VEGF antibody, improved response, PFS and OS in metastatic NSCLC when added to platinum-based chemotherapy (E4599)
Primary endpointoverall survival
No unexpected toxicitySignificant increase in neutropenia, hypertensionNo significant difference in treatment related deaths (2% vs 3%)

PLEN04.03: Randomized phase III trial of adjuvant chemotherapy with or without bevacizumab in resectednon-small cell lung cancer (NSCLC): Results of E1505 – Heather Wakelee, USA
0.0
0.2
0.4
0.6
0.8
1.0
Months from Registration
Ove
rall
Sur
viva
l Pro
babi
lity
0 12 24 36 48 60 72 84
Chemo (208 events/ 749 cases)Chemo + Bevacizumab (204 events/ 752 cases)
0.0
0.2
0.4
0.6
0.8
1.0
Months from Registration
Dis
ease
-Fre
e S
urvi
val P
roba
bilit
y
0 12 24 36 48 60 72 84
Chemo (338 events/ 749 cases)Chemo + Bevacizumab (334 events/ 752 cases)
Overall Survival Disease Free SurvivalOS hazard ratio (B:A): 0.99 95% CI: (0.81-1.21) p=0.93
DFS hazard ratio (B:A): 0.98 95% CI: (0.84-1.14) p=0.75

PLEN.07 : Stopping Smoking Reduces Mortality – Ugo Pastorino
Stopping Smoking Reduces Mortality in Low-Dose Computed Tomography
(LDCT) Screening VolunteersUgo Pastorino, Thoracic Surgery,
Istituto Nazionale dei Tumori, Milan, Italy
PLEN.07 - Presidential SymposiumPlenary Hall (Bellco Theatre) 09/09/2015, 11:51 AM
PLEN.07 : Stopping Smoking Reduces Mortality – Ugo Pastorino
Stopping smoking in LDCT screening3,381 subjects – 32,858 PY – median 8.7 yrs
EX = ex-smokerswho had stopped smoking at the time of accrual / randomization in the LDCTscreening study
QUIT = quitterswho were active smokers at the time of accrual / randomization, but stoppedsmoking at least one year before the end of follow-up or death
CURRENT = active smokerswho continued to smoke during LDCT screening period, or stoppedsmoking less than one year before the end of follow-up or death

PLEN.07 : Stopping Smoking Reduces Mortality – Ugo Pastorino
Smoking & mortality (Relative Risk adjusted by covariate/regression model)
Mort / 100,000 PY RR CI 95%
CURR vs EX/QUIT 846 vs 726 0.74 0.58- 0.95
CURR vs EX/QUIT > 2yrs* 846 vs 613 0.61 0.46- 0.80
CURR vs QUIT > 2yrs* 846 vs 565 0.57 0.38- 0.85
CURR vs EX > 2yrs* 846 vs 613 0.63 0.46- 0.88
* Excluding 239 quitters who stopped smoking < 2 yrs before the end of follow-up or death

PLEN.07 : Stopping Smoking Reduces Mortality – Ugo Pastorino
p-value Log-Rank test: 0.0572
Stopping smoking & mortality
CURRENT
EX / QUIT

PLEN.07 : Stopping Smoking Reduces Mortality – Ugo Pastorino
28% of baseline smokers stop during LDCT
pharmacological support is more effective
lung cancer causes < 30% of all deaths
stopping smoking reduces total mortality by > 25%
benefit is 3 to 5-fold greater than LDCT screening
next step: test prevention vs. screening
Conclusions

Multiregion whole exome and transcriptome sequencing defines the genomic spectrum of EGFR M+ NSCLC and
reveals novel mechanisms of TKI resistance
Daniel SW TAN1,2,3, R. Nahar2, A. Takano4, A. Khng2, T. Zhang2, T. Koh5, A. Gogna6, K.H. Lim4, W.A. Zaw1, X. Liu2, A. Teo2, C. Chan2, Y.Y. Lee2, N.G Iyer3, L.H. Chen2,3, M.K. Ang1, Q-S. Ng1, C-K. Toh1, R. Kanesvaran1,
A. Jain1, A. Devanand6, V. Krishnan2, P. Ng2, B.S. Tan5, C.H. Lim7, B. Chowbay8, W.T. Lim1, W.L. Tam2, B. Lim2, E.H. Tan1, W. Zhai2, A.M. Hillmer2
PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
1Division of Medical Oncology, National Cancer Centre Singapore; 2Genome Institute of Singapore; 3Cancer Therapeutics Research Laboratory, NCCS; 4Department of Pathology, Singapore General Hospital;
5Division of Surgical Oncology, NCCS; 6Department of Diagnostic Radiology, SGH; 6Department of Respiratory and Critical Care Medicine, SGH; 7Department of Cardiothoracic Surgery, NHCS; 8Clinical Pharmacology
Laboratory, NCCS

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
Disclosures• Advisory Role and Consultant: Novartis, Bayer, Boehringer Ingelheim• Travel fees: Novartis, Merck, Pfizer• Research Funding: Novartis

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
Background• EGFR mutations (M+) are amongst the commonest druggable alterations in NSCLC
• We sought to examine the genomic architecture and spectrum in treatment naïve and TKI resistant EGFR M+ NSCLC
ResectedTKI naïve
NSCLC Surgery
Cell population expansion
Cohort 1: Stage I & IIAim 1: Determine clonal architecture through multi-sector sequencing
EGFR TKI Resistant
BiopsiesEGFR TKI
Cohort 2: Stage IVAim 2: Elucidate mechanisms of EGFR TKI resistance through integrative omics

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
Methods• Aim 1: Multi-sector sequencing on spatially separated regions from resected
EGFR M+ lung adenocarcinoma (9 patients, 47 sectors)
Illumina Hi-Seq

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
Patient A021: EGFR L858R
EGFRTP53
R1 R2 R3 R4 R5
Tip (private)
Branch (shared)
Trunk (common)
LRP2EML5
ADCY8
CAPN8MED12
OR10C1
KCNK10
R2 R1
R3
R4
R5
MED12
EGFRTP53
LRP2EML5ASCY8
5
SNVs
Aim 1
PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
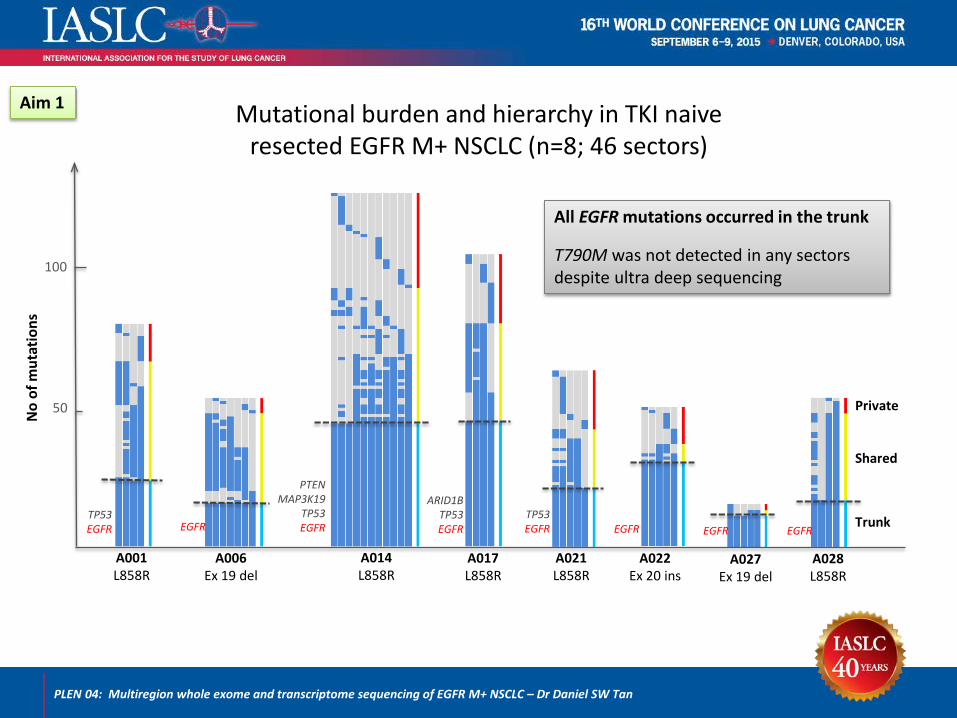
Mutational burden and hierarchy in TKI naiveresected EGFR M+ NSCLC (n=8; 46 sectors)
A001L858R
A006Ex 19 del
A014L858R
A021L858R
A017L858R
A027Ex 19 del
A022Ex 20 ins
A028L858R
TP53EGFR EGFR
PTENMAP3K19
TP53EGFR
ARID1BTP53EGFR
TP53EGFR EGFR EGFR EGFR
Mutation burdenPer sector: median 48 (9 – 98)Per tumor: median 77 (32–146)
Private
Shared
Trunk
100
No
of m
utat
ions
50
All EGFR mutations occurred in the trunk
T790M was not detected in any sectors despite ultra deep sequencing
Aim 1

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
TKI resistance signature implicates co-existing trunk drivers in primary TKI resistance
A014: 67M/never smoker EGFR L858R/ Stage IBRelapsed within 5 months of surgery
Naïve (n=6) Resistant (n=20)Naïve (n=2)
EGFR L858RCLIP1PTEN splice siteMAP3K19

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
EGFR TKI resistant NSCLC is heterogeneous and therapeutically relevant subgroups co-exist
T790M negative
25%
MET13%
HER2+MET
4%HER2
4%
T790M+42%
T790M++HER2
4% T790M++MET
8%
High Mutation Burden, 16%• Smokers• APOBEC signature
n=24
Aim 2
T790M positive (54%)T790M negative (46%)

PLEN 04: Multiregion whole exome and transcriptome sequencing of EGFR M+ NSCLC – Dr Daniel SW Tan
CONCLUSIONS
• Genomic architecture of TKI naïve East Asian EGFR M+ NSCLC – EGFR mutations are truncal events– Low mutation burden– High clonal diversity (branch/private > trunk)
• Mutation burden is relatively higher in TKI resistant samples– Association with smoking and APOBEC signature in a subset of EGFR M+ NSCLC
• Multiple potential mechanisms of TKI resistance co-exist– e.g. MED12 alterations may be subclonal mediators of resistance– One patient with co-occurring trunk drivers demonstrated primary TKI resistance
A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or
Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced
Non-Small Cell Lung Cancer (NSCLC): SWOG S0819
3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
Roy S. Herbst, MD, PhD, Mary W. Redman, PhD, Edward S. Kim, MD, Thomas J. Semrad, MD, Lyudmila Bazhenova, MD, Gregory Masters, MD; Kurt Oettel, MD; Perry
Guaglianone, MD , Christopher Reynolds, MD, Anand Karnad, MD, Susanne M. Arnold, MD, Marileila Varella-Garcia, PhD, James Moon, MS, Philip C. Mack, PhD, Charles D.
Blanke, MD, Fred R. Hirsch, MD, PhD, David R. Gandara, MD

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
BACKGROUND: CETUXIMAB AND NSCLC
J. Mendelsohn Endocr Relat cancer 2001;8, 3-9P.M. Harari Endocr Relat Cancer 2004;11, 689-708

Cetuximab*Bevacizumab
PaclitaxelCarboplatinCetuximab
*Bevacizumab
*Bevacizumab
PaclitaxelCarboplatin
*Bevacizumab
OBJECTIVES
Co-Primary:• PFS in EGFR FISH+ patients• OS in entire study population
Secondary:• OS and PFS by Bevacizumab
appropriate/inappropriate• Safety/toxicity by treatment
arm
Exploratory (due to SQUIRE study):• OS and in entire study and
FISH+ for SCCA patients
RANDOMIZE
NSCLCAdv Stage
Tumor Tissueavailable
• Study accrual: 7/15/2009- 6/1/2014*In Bevacizumab Appropriate: as piloted in S0536
SWOG 0819: PHASE III SCHEMA
Stratification Factors: 1) Appropriate for
Bevacizumabtreatment: yes vs. no
2) Smoking status: current or former vs. never
3) Stage: M1a vs M1b
3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
EGFR FISH-positive
• ⩾40% of cells displaying ⩾4 copies of the EGFR signal, or
• EGFR to CEP7 ratio ⩾2 over all scored nuclei, or
• Gene clusters (⩾4 spots) or ⩾15 copies of the EGFR signals in ⩾10% of tumor cells.
BACKGROUND: COLORADO SCORING CRITERIA EGFR GENE AMPLIFICATION BY FISH
M. J. Varella-Garcia et al. Clin Pathol. 2009 Nov;62(11):970-977F.R. Hirsch et al. JCO 2008;26:3351-3357

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
S0819 RESULTS: ENTIRE STUDY POPULATION
35
EGFR FISH + PATIENTS
OS
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RegistrationPatients at Risk
656tuximab Arm 446tuximab Arm 287tuximab Arm 153tuximab Arm 76tuximab Arm 48tuximab Arm 28tuximab Arm 11tuximab Arm 5tuximab Arm 2tuximab Arm 1tuximab Arm657Control Arm 448Control Arm 246Control Arm 141Control Arm 94Control Arm 50Control Arm 36Control Arm 13Control Arm 6Control Arm 2Control Arm 1Control Arm
Cetuximab ArmControl Arm
N656657
Events536558
Medianin Months
10.99.4
95%Conf. Int.
(9.6 - 12.0)(8.7 - 10.3)
P = 0.34HR=0.94 (0.84-1.06)
Overall Survival Progression Free SurvivalOSHR=0.94 (0.84-1.06)
p=0.34
PFSHR=0.98 (0.87-1.09)
P=0.68
PFS
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RegistrationPatients at Risk
199C t i b A 78C t i b A 26C t i b A 10C t i b A 3C t i b A 1C t i b A 0C t i b A 0C t i b A 0C t i b A 0C t i b A 0C t i b A
Cetuximab ArmControl Arm
N199201
Events191197
Medianin Months
5.44.8
95%Conf. Int.(4.5 - 5.7)(3.9 - 5.5)
P = 0.37HR=0.91 (0.74-1.12)
OSHR=0.83 (0.67-1.04)
p=0.10
PFSHR=0.91 (0.74-1.12)
P=0.37
Overall Survival Progression Free Survival

All Bevacizumab Appropriate Patients
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RegistrationPatients at Risk
279mab Arm 201mab Arm 138mab Arm 74mab Arm 41mab Arm 23mab Arm 13mab Arm 7mab Arm 4mab Arm 2mab Arm 1mab Arm275ontrol Arm 212ontrol Arm 129ontrol Arm 79ontrol Arm 52ontrol Arm 32ontrol Arm 25ontrol Arm 10ontrol Arm 5ontrol Arm 2ontrol Arm 1ontrol Arm
Cetuximab ArmControl Arm
N279275
Events219220
Medianin Months
12.711.6
95%Conf. Int.
(10.9 - 13.4)(10.5 - 13.8)
P = 0.70HR=1.04 (0.86-1.25)
BEVACIZUMAB INAPPROPRIATE
3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
Bevacizumab Appropriate, FISH+
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RegistrationPatients at Risk
86Cetuximab Arm 71Cetuximab Arm 57Cetuximab Arm 32Cetuximab Arm 16Cetuximab Arm 10Cetuximab Arm 4Cetuximab Arm 3Cetuximab Arm 1Cetuximab Arm 1Cetuximab Arm 1Cetuximab Arm80Control Arm 64Control Arm 45Control Arm 31Control Arm 17Control Arm 12Control Arm 9Control Arm 2Control Arm 1Control Arm 0Control Arm 0Control Arm
Cetuximab ArmControl Arm
N8680
Events6763
Medianin Months
15.513.2
95%Conf. Int.
(13.4 - 18.4)(11.2 - 19.1)
P = 0.88HR=0.97 (0.69-1.38)
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RegistrationPatients at Risk
377tuximab Arm 245tuximab Arm 149tuximab Arm 79tuximab Arm 35tuximab Arm 25tuximab Arm 15tuximab Arm 4tuximab Arm 1tuximab Arm 0tuximab Arm 0tuximab Arm
Cetuximab ArmControl Arm
N377382
Events317338
Medianin Months
9.28.2
95%Conf. Int.
(8.2 - 10.9)(7.3 - 8.7)
P = 0.12HR=0.88 (0.76-1.03)
S0819 RESULTS: BEVACIZUMAB APPROPRIATE
Bev Appropriate, FISH + (OS)All Bev Appropriate OSHR=1.04 (0.86-1.25) p=0.70
Bev Appropriate FISH + OSHR=0.97 (0.69-1.38)
p=0.88
All Bev Appropriate Patients (OS)
All Bev Inappropriate OSHR=0.88 (0.76-1.03)
p=0.12
Bev Inappropriate FISH + OS
HR=0.75 (0.57-0.998) P=0.048
Bevacizumab Inappropriate, FISH+
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RegistrationPatients at Risk
Cetuximab ArmControl Arm
N113121
Events94
107
Medianin Months
11.28.7
95%Conf. Int.
(8.6 - 12.9)(5.9 - 9.7)
P = 0.048HR=0.75 (0.57-0.998)
Bev Inappropriate, FISH + (OS)All Bev Inappropriate (OS)

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After Registrationatients at Risk
Cetuximab ArmControl Arm
N5556
Events5052
Medianin Months
11.86.4
95%Conf. Int.
(8.6 - 13.5)(4.2 - 8.7)
P = 0.006HR=0.56 (0.37-0.84)
S0819 RESULTS: Squamous Cell Carcinoma (SCCA) FISH +
SCCA FISH+ OSHR=0.56 (0.37-0.84) p=0.006
SCCA FISH + (OS)
S0819Adverse Events
Cetuximab Arm Control ArmNo Bev (N=365) Bevacizumab (N=262) No Bev (N=367) Bevacizumab (N=265)
Grade 3/4 Grade 5 Grade 3/4 Grade 5 Grade 3/4 Grade 5 Grade 3/4 Grade 5Blood/Bone Marrow 44% 44% 33% 37%
Metabolic/Laboratory 18% 20% 12% 14%Gastrointestinal 14% 16% 1% 10% 16%
Infection 9% 1% 11% 1% 9% 1% 11%Pulmonary/Upper Respiratory 7% 1% 8% 3% 1% 5%
Dermatology/Skin 7% 17% 0.3% 0.4%Allergy/immunology 7% 6% 2% 1%Renal/Genitourinary 1% 1%
TOTAL 66% 4% 77% 6% 54% 2% 69% 2%

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
Summary1. Co-Primary Objective: No Benefit in OS for entire study
population (N=1333, HR=0.94, p=0.34)2. Co-Primary Objective: No benefit in PFS in EGFR FISH +
population (n=400, HR=0.91, p=0.37)3. Secondary Objective: Indication of benefit for OS in EGFR
FISH + population, but not statistically significant (n=400, HR=0.83, p=0.10)
4. Secondary Objective: Indication of benefit on OS among Bevacizumab – inappropriate, EGFR FISH + patients (n=759, HR=0.75, p=0.048)
5. Exploratory Objective: In squamous cell FISH + patients, a significant improvement in OS (n=321, HR=0.56, p=0.006)

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
IMPLICATIONS AND FUTURE PLANS1. Large Intergroup study completed – acceptable toxicity of
the regimen2. These data along with the recent SQUIRE results suggest a
role for EGFR FISH in selecting patients for therapy with EGFR antibodies (Cetuximab and Necatumab)- especially when Bevacizumab is not used
3. Analysis of EGFR H Score and KRAS mutation ongoing, to be presented at ASCO 2016
4. Squamous Cell is an important area- Lung MAP is the next step!

3612: A Randomized, Phase III Study Comparing Carboplatin/Paclitaxel or Carboplatin/Paclitaxel/Bevacizumab with or without Concurrent Cetuximab in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): SWOG S0819 – R. Herbst
Presentation Number: Presentation Title – Presenting Author
• Public private partnership• Leverages NCTN Network• Biomarker selected trials• >100 million of industry support• FDA collaboration- seeks to get
drugs approved and to patients!• Genomic profiling delivered to the
community• A new paradigm for drug
development and scientific discovery
S1400DFGFR
FGFR ampl,mut, fusion
S1400CCDK4/6
CCND1, CCND2, CCND3, cdk4 ampl
ScreeningSquamous Cell Lung Cancer
S1400ANon-match
S1400BPI3K
PIK3CA mut
1 GDC-0032 2 Docetaxel
1 Palbociclib2 Docetaxel
1 AZD45472 Docetaxel
1:11:11:1
Arm1
Arm2
Arm1
Arm2
Arm1
Arm2
Arm1
1 Medi4736
Current Trial Schema[Revision #2 Activated 5/26/15]
GDC-0032 SoC
PalbociclibSoc
AZD4547SoC
GDC-0032 Palbociclib AZD4547
FGFR1CDK4/61PI3K1
Non-matchSub-studies
Nivo/IpiNivolumab
BMN 673SoC
BMN 673
Stage 1
Stage 2
HRD2 Checkpoint Naive1
MEDI4736
CheckpointRefractory2
Matched Sub-studies
1 Revision #3: Expected September/October 20152 Revision #4: Expected December 2015/January 2016
Updated Lung-MAP Trial Schema(Expected with Revisions # 3 & 4)

Fred R. Hirsch*
Theresa Boyle, Nick Thatcher, Luis Paz-Ares, Marileila Varella-Garcia, Ashley Kowalewski, Rebecca R. Hozak, Gu Mi, Symantha Melemed,
Charles W. Caldwell, Raffael Kurek, Mark A. Socinski
*Presenting author
Presentation Number: EGFR IHC and FISH correlative analyses (SQUIRE Trial) – Dr. Fred Hirsch
32.05: EGFR IHC and FISH Correlative Analyses (SQUIRE trial): Necitumumab + Gemcitabine-Cisplatin vs Gemcitabine-Cisplatin in 1st-
line Squamous NSCLC
32.05: EGFR IHC and FISH Correlative Analyses (SQUIRE Trial) – Fred Hirsch

SQUIRE: Necitumumab in Advanced 1st-line Squamous NSCLC1
• Primary endpoint: overall survival• Mandatory tissue collection from archived tumor
Necitumumab is a second-generation human IgG1 anti-EGFR monoclonal antibody.
Dosing regimen: GC (G=1250 mg/m2 IV days 1, 8; C=75 mg/m2 IV day 1) + N (800 mg absolute dose IV) or GC alone (every 21 days up to 6 cycles)
Randomization (R) stratified by: ECOG PS and region
CRPRSD
Gem-Cis + NECI (GC+N)(N = 545)
Maximum of 6 cycles
1093 patients• First-line Stage IV
sq- NSCLC
• ECOG PS 0-2
NECI (N)
Gem-Cis (GC) N = 548
RPD
PD
PD
1Thatcher N, et al. Lancet Oncol 2015;16(7):763-74
Presenter
Presentation Notes
Speaker notes EGFR protein positivity was not required for enrollment EGFR protein expression has not been shown to be predictive

0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
0
20
40
60
80
100
SQUIRE Primary Outcome: Overall Survival ITT1
GC+NN=545
GCN=548
Stratified HR (95% CI) 0.84 (0.74, 0.96)Stratified p-value (log-rank) 0.01Median, months (95% CI) 11.5 (10.4, 12.6) 9.9 (8.9, 11.1)
Time Since Randomization (Months)
Ove
rall
Surv
ival
(%)
GC+N GC
1Thatcher N, et al. Lancet Oncol 2015;16(7):763-74
Presenter
Presentation Notes
Speaker notes SQUIRE was a positive trial with meaningful OS benefit Primary objective was met, Median survival with Gem-Cis + Neci significantly longer than with Gem-Cis with 16% reduction in the risk of death in favor of neci arm OS benefit was observed across clinically relevant subgroups PFS was also significantly longer in the Gem-Cis + Neci group

Overall Survival in EGFR FISH Positive* Patients
GC+N GC
GC+NN=111
GCN=97
Unstratified HR (95% CI) 0.70 (0.52, 0.96)Median, months (95% CI) 12.6 (11.5, 15.9) 9.2 (7.2, 12.1)
*Based on Colorado Classification (Varella-Garcia M, et al. J Clin Pathol 2009;62(11):970-7)
Time Since Randomization (Months)0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
Ove
rall
Sur
viva
l (%
)
0
20
40
60
80
100
Tumor samples were available with valid FISH results obtained for 51% of ITT population
Presenter
Presentation Notes
Speaker notes

Subgroup Analysis for Positive or Negative EGFR Copy Number Gain
Positive* Negative*
GC+N(N=111)
GC(N=97)
GC+N(N=171)
GC(N=178)
OSmOS, months 12.6 9.2 11.1 10.7
HR within expression level (95% CI) 0.70 (0.52-0.96) 1.02 (0.80-1.29)
Interaction p-value 0.066PFS
mPFS, months 6.1 5.1 5.6 5.5
HR within expression level (95% CI) 0.71 (0.52-0.97) 1.04 (0.82-1.33)
Interaction p-value 0.057*Based on Colorado Classification (Varella-Garcia M, et al. J Clin Pathol 2009;62(11):970-7)
Tumor samples were available with valid FISH results obtained for 51% of ITT population
Presenter
Presentation Notes
Speaker notes Assessed correlation between treatment effect with EGFR copy number gain in the 51% of patients who had available results For both OS and PFS, we observed a trend for greater treatment effect in EGFR copy number gain positive patients than in the negative patients For both OS and PFS, the effects were not statistically significant EGFR copy number gain will also be assessed further in future trials Considerations: p-values were not adjusted for multiplicity across clinical endpoints, marker cutpoints, or different markers we have assessed

Q & A


















