Preserving reproductive capacity in young boys with...
5
REPRODUCTION www.trendsinurology.com TRENDS IN UROLOGY & MEN’S HEALTH MAY/JUNE 2013 8 W e can now cure more than 70 per cent of all childhood cancers, and this cure rate approaches 90 per cent for some tumours. 1 Enhanced supportive care for dose-intense treatment regimens imposed on a cancer incidence that has been stable over the past 40 years 2 is responsible for this success. Where survival is so high, however, further attempts to increase it must be balanced against the multi-organ toxicities to the majority of developing children. Though not necessarily impotent, 15–30 per cent of male survivors are rendered infertile, 3 either from hypothalamo–pituitary–gonadal exposure to chemoradiation 4 or from diseases such as Hodgkin’s lymphoma. 5 In today’s society, one in six healthy couples seeks help from reproductive clinics to conceive, 6 with rapid advancements in assisted reproductive technology (ART) having being made in the past two decades. These include cryopreservation of gametes and embryos prior to gonadotoxic cancer therapies to preserve fertility in adults. IMPACT OF CHILDHOOD CANCER TREATMENT ON MALE FERTILITY Spermatogenesis begins only at puberty. This process requires meiotic division of diploid spermatogonia to produce haploid spermatozoa, a process that continues thereafter throughout adult life. Spermatogenesis requires sufficient intratesticular testosterone production maintained by pituitary-derived follicular- stimulating hormone (FSH) and luteinising hormone (LH) with negative gonadal feedback from inhibin B (Sertoli cells) and testosterone (Leydig cells). Both disease- and treatment-related factors can damage the hypothalamo–pituitary–testicular axis at one or multiple levels (Figure 1), thereby compromising male reproductive capacity. Chemotherapy The rapidly dividing sperm-producing testicular seminiferous epithelium is highly susceptible to cytotoxic damage, its extent determined by drug type, cumulative drug In this article, the authors explore the possibilities and particular developmental and ethical issues surrounding sperm cryopreservation in young boys with cancer, and examine the unique legal implications of fertility counselling in adolescence. HOONG WEI GAN AND HELEN A. SPOUDEAS Preserving reproductive capacity in young boys with cancer Hoong Wei Gan, BM BS, BMedSci(Hons), MRCPCH, Specialty Registrar in Paediatrics, Honorary Research Fellow in Paediatric Neuroendocrine Late Effects of Childhood Cancer; Helen A. Spoudeas, MB BS, DRCOG, FRCP, FRCPCH, MD, Consultant in Neuroendocrine Late Effects of Childhood Cancer, Honorary Senior Lecturer in Paediatric Endocrinology, University College London Hospitals NHS Foundation Trust
-
Upload
nguyennhan -
Category
Documents
-
view
214 -
download
2
Transcript of Preserving reproductive capacity in young boys with...

REPRODUCTION
www.trendsinurology.com TRENDS IN UROLOGY & MEN’S HEALTH MAY/JUNE 2013
8
We can now cure more than 70 per centof all childhood cancers, and this cure
rate approaches 90 per cent for sometumours.1 Enhanced supportive care fordose-intense treatment regimens imposedon a cancer incidence that has been stableover the past 40 years2 is responsible for thissuccess. Where survival is so high, however,further attempts to increase it must bebalanced against the multi-organ toxicitiesto the majority of developing children.Though not necessarily impotent, 15–30 percent of male survivors are rendered infertile,3
either from hypothalamo–pituitary–gonadalexposure to chemoradiation4 or fromdiseases such as Hodgkin’s lymphoma.5
In today’s society, one in six healthy couplesseeks help from reproductive clinics to
conceive,6 with rapid advancements inassisted reproductive technology (ART)having being made in the past two decades.These include cryopreservation of gametesand embryos prior to gonadotoxic cancertherapies to preserve fertility in adults.
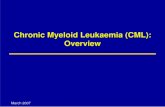
IMPACT OF CHILDHOOD CANCERTREATMENT ON MALE FERTILITYSpermatogenesis begins only at puberty. This process requires meiotic division ofdiploid spermatogonia to produce haploidspermatozoa, a process that continuesthereafter throughout adult life.Spermatogenesis requires sufficientintratesticular testosterone productionmaintained by pituitary-derived follicular-stimulating hormone (FSH) and luteinisinghormone (LH) with negative gonadalfeedback from inhibin B (Sertoli cells) andtestosterone (Leydig cells). Both disease- andtreatment-related factors can damage thehypothalamo–pituitary–testicular axis at oneor multiple levels (Figure 1), therebycompromising male reproductive capacity.
ChemotherapyThe rapidly dividing sperm-producingtesticular seminiferous epithelium is highlysusceptible to cytotoxic damage, its extentdetermined by drug type, cumulative drug
In this article, the authors explore the possibilities andparticular developmental and ethical issues surroundingsperm cryopreservation in young boys with cancer, andexamine the unique legal implications of fertilitycounselling in adolescence.
HOONG WEI GAN AND HELEN A. SPOUDEAS
Preserving reproductivecapacity in young boyswith cancer
Hoong Wei Gan, BM BS, BMedSci(Hons),MRCPCH, Specialty Registrar in Paediatrics,Honorary Research Fellow in PaediatricNeuroendocrine Late Effects of ChildhoodCancer; Helen A. Spoudeas, MB BS,DRCOG, FRCP, FRCPCH, MD, Consultant inNeuroendocrine Late Effects of ChildhoodCancer, Honorary Senior Lecturer inPaediatric Endocrinology, University CollegeLondon Hospitals NHS Foundation Trust
Gan reproduction_Layout 1 16/05/2013 14:58 Page 1

dosage and patient age at exposure. Bycontrast, the testosterone-producing Leydigcells are relatively robust. Consequently,pubertal sexual development may proceednormally (and sometimes early), the only signof gonadotoxicity and future subfertilitybeing small testicular volumes relative to thedegree of virilisation and pubertal stage.
Because cancer treatment protocols aremultidrug regimens, the individual effect ofspecific drug types has proved difficult todetermine accurately. However, most alkylatingagents (eg cyclophosphamide, busulfan,melphalan) and nitrosureas (eg lomustine)demonstrate dose-dependent gonadotoxicity;the UK Children’s Cancer and Leukaemia Group and the British Fertility Society (BFS)have provided helpful ‘guesstimates’ of the‘gonadotoxicity risk’ of current commonchildren’s cancer treatment regimens (Box 1)4,7
in three broad categories – low (<20 per cent),medium (20–80 per cent) and high (>80 percent). Alkylating agents (eg cyclophosphamide)are most likely to cause future subfertility,while protocols for acute lymphoblasticleukaemia (vincristine, methotrexate,cytarabine) are least likely to do so.
RadiotherapyRadiotherapy may affect fertility at more than one level on the hypothalamo–pituitary–testicular axis (see Figure 1). First,the testis is vulnerable to increasing doses ofirradiation, which differentially affect theseminiferous epithelium and Leydig cells(Table 1).8,9 In adults, fractionated doses aslow as 0.1 gray (Gy) may cause temporaryazoospermia, while doses of 2–3Gy are likely to prevent spermatic recovery longterm. Larger doses of 10–12Gy, as used in total body irradiation, damage both Leydig and Sertoli cell function and, if given concurrently with chemotherapy, have additive effects. Hypersecretion of LH can partially compensate for mild Leydig cell dysfunction with near-normal testosterone values (subclinicalhypergonadotrophic hypogonadism), but the long-term impact on bone strengthand cardiac health is unknown.
Cranial irradiation, used in high dose (>40Gy)and primarily for centrally positioned braintumours, may reduce hypothalamo–pituitaryfunction and result in hypogonadotrophichypogonadism.10 In the developing child this
manifests as pubertal delay or arrest,although in the context of pre-existingpituitary disease or tumour these are themore likely causative factors. By contrast,early or precocious puberty is a typicalmanifestation of any cranial injury to theyoung brain (including disease, surgery orirradiation), but its evolution does notpreclude later pubertal arrest and eventualgonadotrophin deficiency affecting both LH–testosterone and FSH–spermatogenicpathways and causing impotence andsubfertility, respectively. Only the former can be treated with testosterone replacement therapy.
DiseaseOccasionally, the disease itself can causetesticular dysfunction. Hodgkin’s disease hasbeen associated with pre-treatmentabnormalities in semen quality even in theabsence of testicular infiltration.5 Thepathogenesis of this phenomenon is poorlyunderstood but is thought to relate todisease-induced inflammatory processes.
CURRENT FERTILITY PRESERVATIONSTRATEGIESIn mature adults, pre-treatment spermcryopreservation has been the mostsuccessful method of fertility preservationsince the 1950s. Spermatozoa are remarkablyresistant to storage and freeze–thawingprocesses, and healthy offspring withoutcongenital anomalies have been reportedfrom sperm stored for up to 28 years.11
Separately stored ‘straws’ of spermatozoacan be thawed as required and used infertility treatments, either directly byintrauterine insemination or byintracytoplasmic sperm injection, a techniqueavailable since 1992 that has markedlyreduced the number of viable spermatozoarequired to single numbers.12
Requesting and obtaining masturbatorysemen samples from older post-pubertalmales is relatively straightforward. However, even ill adults may fail to produce a specimen in this way. For these patients and younger boys unable
REPRODUCTION
TRENDS IN UROLOGY & MEN’S HEALTH MAY/JUNE 2013 www.trendsinurology.com
9
Hypothalamus
LHRH
Pituitary
LH FSH
Testes
Leydig cells(testosterone)
Sertoli cells (inhibin B),seminiferousepithelium
(spermatogenesis)
Chemotherapy and radiotherapy
>0.1–0.2GyRadiotherapy
>20Gy
SurgeryCranial
radiotherapy >35–45Gy
– -
Figure 1. Schematic representation of the hypothalamo–pituitary–testicular axis and potentialsites of disruption secondary to various cancer treatment modalities (red arrows). Thin bluearrows indicate physiological negative feedback mechanisms. LHRH, luteinising hormone-releasing hormone; LH, luteinising hormone; FSH, follicular-stimulating hormone; Gy, gray
Gan reproduction_Layout 1 16/05/2013 14:58 Page 2

to produce a sample because ofpsychological or sexual immaturity, religious or cultural beliefs, alternatives such as rectal electrostimulation, penilevibratory stimulation, surgical extractionunder general anaesthesia, and evenexperimental techniques such as testiculartissue storage have been considered but not widely practised.
To facilitate service delivery, what remainsunclear is exactly when during pubertalmaturation boys are able spontaneously toejaculate semen containing viable sperm.Spermaturia – the appearance of sperm inthe urine by retrograde ejaculation – hasbeen documented in healthy boys as youngas 11.7 years of age and at a minimumtesticular volume of 4.7ml, with little or no
pubic hair development (Tanner stage P1, G2)and before peak height velocity.13 The agerange for initial spermaturia, however, iswide and up to 17.5 years. Although it hasbeen used as an estimate of true spermarche,there is no documentation of what triggersspermatogenesis, its correlation withpubertal staging and the ability to donatesemen voluntarily, while spermatozoaobtained from urine are less viable and henceunsuitable for cryopreservation.
PIONEERING SERVICE FOR ADOLESCENT BOYS More than 10 years ago, with the support ofcolleagues in child psychiatry, reproductivehealth and haematology/oncologycontributing to the development of age-appropriate information leaflets, awarenesscampaigns and streamlined risk-assessmentsand referrals, we set up a pioneeringendocrine/fertility assessment andcounselling service for adolescents atUniversity College London Hospital. This was targeted at males with cancer aged 12–18 years referred to our tertiary centrefor high-dose therapies.
The repeated three- to four-yearly auditcycles of service in a total of 222 boys over that time have demonstrated asurprisingly consistent and unchangingcounselling rate of some 70 per cent, butwith an appropriately greater prioritisation of those at highest ‘gonadotoxicity risk’ overtime. However, the relative paucity (30.0 percent) of documented pubertal clinicalexaminations persists to date, in spite ofgood biochemical marker measurements(70.3 per cent) and high patient acceptabilityof the counselling process (68.4 per cent).34.2 per cent of the total cohort (and 65.0per cent of those actually attemptingstorage) banked viable sperm produced bymasturbation, the youngest boys being 12.6 years at Tanner stage 3+ and/or with a testicular volume of ≥8ml (Gan HW,Williamson E, Cuddis Z, et al., personalcommunication). Importantly, it washormone parameters of virilisation (testicular volume, plasma LH and
REPRODUCTION
www.trendsinurology.com TRENDS IN UROLOGY & MEN’S HEALTH MAY/JUNE 2013
10
LOW RISK (<20%)l Acute lymphoblastic leukaemial Wilms’ tumourl Soft tissue sarcoma: stage Il Germ cell tumours: with gonadal preservation and no radiotherapyl Retinoblastomal Brain tumour: surgery only or cranial irradiation <24Gy
MEDIUM RISK (20–80%)l Acute myeloblastic leukaemial Hepatoblastomal Osteosarcomal Ewing’s sarcomal Soft tissue sarcoma: stage II–IIIl Neuroblastomal Non-Hodgkin’s lymphomal Hodgkin’s disease: alternating (‘hybrid’) therapyl Brain tumour: craniospinal radiotherapy or cranial irradiation >24Gy
HIGH RISK (>80%)l Total body irradiationl Chemotherapy conditioning for bone marrow transplantl Localised radiotherapy: pelvic/testicularl Hodgkin’s disease: alkylating agent-based therapyl Soft tissue sarcoma: metastatic/stage IVl Ewing’s sarcoma: metastatic/stage IV
BOX 1. Best estimate guidance for estimating risk of subfertility from varioustreatment modalities based on current regimens used in common childhood andadolescent cancers4,7
0.1–0.2 Transient impairment of spermatogenesis>4 Risk of permanent impairment of spermatogenesis20–30 Leydig cell dysfunction35–45 (cranial) Hypogonadotrophic hypogonadism
Dose of irradiation (Gy) Effects on fertility
Table 1. Effects of increasing doses of irradiation on hypothalamo–pituitary–testiculardysfunction. Note that the impact of total body irradiation is difficult to quantify8,9
Gan reproduction_Layout 1 16/05/2013 14:58 Page 3

testosterone concentrations), not age per se,that correlated with successful storage, whileparameters of spermatogenesis (plasma FSHconcentration) determined the normality ofsperm concentrations. The role of age cameinto play only as a surrogate marker ofpubertal development and was notindependently predictive of outcome.
Prepubertal boysThere are currently no proven fertilitypreservation techniques for prepubertal boys(testicular volume <4ml). Cryopreservation ofdiploid spermatogonial cells obtained bytesticular biopsy for later post-cure auto-transplantation or in vitro maturation tospermatozoa (as currently debated in youngwomen) is still experimental, withoutsuccessful conceptions, even in animalmodels. Auto-transplantation carries atheoretical risk of reintroducing malignantcells, particularly in haematologicalmalignancies where the testes are potentialsites of metastases. Other prophylactictechniques such as testicular shieldingduring radiotherapy or the administration of gonadotrophin-releasing hormoneanalogues or testosterone to render celldivision quiescent and less susceptible to cytotoxins have limited, if any, practical success.
LEGAL, ETHICAL AND PRACTICALCONSIDERATIONSThe storage and use of haploid gametes and embryos is governed by the HumanFertilisation and Embryology (HFE) Act14 –this mandates personal, not proxy, informedconsent in line with reproductive rights. Thus,unlike for other paediatric procedures – forinstance consenting for an appendicectomy– parents cannot give valid consent on ateenager’s behalf; any minor (under 18 or 16years of age respectively in England andScotland) must be judged intellectually(‘Gillick’) competent to consent withoutcoercion. Written consent to disclosure, HIV,hepatitis B and C testing and the use ofstored samples after death or mentalincapacitation is additionally required at thisdifficult time.
Paradoxically, the legal loophole in whichdiploid prepubertal testicular tissue does not fall under HFE jurisdiction until such time as it becomes haploid leavesprepubertal boys potentially open to harmfrom experimentation – such as surgicalremoval of premeiotic spermatogonia –under the common law of parental consent,even if the sole intent to preserve fertilityappears well intended.
There are few, if any, adolescent-tailoredsperm banking and counselling facilities in the UK, and there is debate as to howadult services might be modified to meettheir specific needs (eg the environment,written information and pornographicmaterial provided). The increased press focus on fertility preservation and NICErecommendations suggest such a servicemight be offered more widely. However,while the young age of this increasingnumber of survivors would indicate a needfor longer-term storage, historically, fewstored samples have ever been used. Thiswould suggest adult survivors either retain or do not ultimately want fertility, but alsothat patients at highest risk of subfertility are those most heavily treated and likely todie from aggressive disease or treatment-related complications.
ADOLESCENT FERTILITY COUNSELLINGSERVICEOncologists may perceive reproduction astoo sensitive and inappropriate a topic tobroach with adolescents already undergoinga complex counselling and consent processfor cancer treatment.15 However, the fewstudies in this area indicate surprisingawareness among adolescents, who in fact welcome discussion and choice – apositive experience at this stage of theirdisease (Box 2).16
Pre-treatment fertility assessmentThe young teenager has unique ethicolegal,physical, psychosexual and intellectual needs that are very different from those ofthe fully mature adult. To be fit for purpose,any adolescent fertility service shouldroutinely, consistently and reliably measureand record pubertal staging and testicularvolumes; this is but one step further than theroutine examination of the testes required toexclude malignant involvement.
Paired with pre-treatment plasma endocrinebiochemistry (LH, FSH, testosterone ± inhibin Bwhere possible), this baseline assessmentshould form the gold standard against whichservice adherence might be judged andaudited. It is vital not only to inform the
REPRODUCTION
TRENDS IN UROLOGY & MEN’S HEALTH MAY/JUNE 2013 www.trendsinurology.com
11
PRE-TREATMENTl Counsel within adolescent-tailored facilities (ideally)l Counsel before commencement of treatmentl Allow sufficient opportunity to bank samples before treatmentl Clinical assessment – pubertal stage, testicular volume, best estimate of
subfertility riskl Biochemical assessment – LH, FSH, testosterone, inhibin Bl Gillick competence and informed consent including virology (HIV, hepatitis B
and C)
POST-TREATMENTl Streamlined late effects follow-up (may have other endocrine toxicities)l Encourage post-treatment semen analysis (do not bank before three months)l Contraceptive advicel Testicular self-examination
BOX 2. Summary of main points in the assessment and counselling for fertilitypreservation in adolescent boys
Gan reproduction_Layout 1 16/05/2013 14:58 Page 4

counselling process and the individualpatient’s chances of producing a viablesperm sample, but also to assess future serial change indicative of gonadotoxicityand/or spermatic recovery with time.
We have found that collecting spermimmediately after commencement ofchemotherapy (even after only six days’exposure) is likely to reduce sample viabilityby >75 per cent, and therefore this practiceshould be avoided. If it is to be successful inthose judged to be at high risk (see Box 1),fertility preservation should be given earlier and higher priority in the cancercounselling process, even to the point ofdelaying cancer treatment to allow severalattempts where possible.
Post-treatment fertility assessmentThe long-term follow-up of teenage cancersurvivors has not to date emphasised routinefertility assessment, semen analysis and/orsperm banking (against a future relapse) inthose still minors (<18 years) at the end ofcancer therapy.
However, counselling young boys andsupporting them to donate interval post-treatment semen samples, togetherwith routine pubertal and biochemicalassessment, would provide the data neededto inform future age-appropriate servicesand sperm storage facilities based on thetrue gonadotoxicity (and time to recovery) of different cancer treatment regimens andtheir clinical correlates.
This would concur with the 2003 BFSconsensus recommendation that wheresperm was not cryopreserved beforetreatment, a further opportunity at leastthree months from the end of treatment (to reduce the risk of DNA damage) should be offered.7
For the counselling process to be trulycomplete, it should ensure understanding ofthe difference between potency (likely to bepreserved or otherwise easily replaced) andfertility; for those unable or choosing not to
cryopreserve sperm pre-treatment, there is still well-documented potential forrecovery of natural fertility even five yearsafter treatment17 and the consequent need for contraception in all. Testicular self-examination should be encouraged inthe older teenager to monitor for tumourrelapse or secondary malignancies.
CONCLUSIONSAs ART continues to evolve rapidly, fertilitycounselling in adolescence presents a specific and growing challenge. Government-level debate on the future role of the HFE Act would do well to give considerationto the needs of this cohort, who areincreasingly campaigning for protection of their reproductive rights through patient groups such as the Teenage Cancer Trust. Meanwhile, clinicians can be reassured that the large majority of young teenagers welcome the discussion and can exercise appropriate informed choice even in the context of a life-threatening illness. There should thus beample opportunity to discuss optionsavailable to them both before and aftercancer treatment with concurrentlyimproved documentation of consent andclinical examination to make the service truly tailored to the adolescent.
Declaration of interests: none declared.
REFERENCES1. Gatta G, Capocaccia R, Stiller C, et al.
Childhood cancer survival trends in Europe: aEUROCARE Working Group study. J Clin Oncol2005;23:3742–51.
2. Office for National Statistics. Cancer statisticsregistrations: registrations of cancerdiagnosed in 2009, England (MB1 40).London: Office for National Statistics, 2011.
3. Schrader M, Muller M, Straub B, Miller K. Theimpact of chemotherapy on male fertility: asurvey of the biologic basis and clinicalaspects. Reprod Toxicol 2001;15:611–17.
4. Wallace WH, Anderson RA, Irvine DS. Fertilitypreservation for young patients with cancer:who is at risk and what can be offered?Lancet Oncol 2005;6:209–18.
5. Rueffer U, Breuer K, Josting A, et al. Malegonadal dysfunction in patients withHodgkin’s disease prior to treatment. Ann Oncol 2001;12:1307–11.
6. Hull MG, Glazener CM, Kelly NJ, et al.Population study of causes, treatment, and outcome of infertility. Br Med J1985;291:1693–7.
7. Multidisciplinary Working Party convened by the British Fertility Society. A strategy for fertility services for survivors of childhood cancer. Hum Fertil (Camb)2003;6:A1–A39.
8. Shalet SM, Tsatsoulis A, Whitehead E, Read G.Vulnerability of the human Leydig cell toradiation damage is dependent upon age.J Endocrinol 1989;120:161–5.
9. Centola GM, Keller JW, Henzler M, Rubin P.Effect of low-dose testicular irradiation on sperm count and fertility in patients with testicular seminoma. J Androl1994;15:608–13.
10. Littley MD, Shalet SM, Beardwell CG, et al.Radiation-induced hypopituitarism is dose-dependent. Clin Endocrinol 1989;31:363–73.
11. Feldschuh J, Brassel J, Durso N, Levine A.Successful sperm storage for 28 years. Fertil Steril 2005;84:1017.
12. Palermo G, Joris H, Devroey P, VanSteirteghem AC. Pregnancies afterintracytoplasmic injection of singlespermatozoon into an oocyte. Lancet1992;340:17–18.
13. Nielsen CT, Skakkebaek NE, Richardson DW, et al. Onset of the release of spermatozoa(spermarche) in boys in relation to age,testicular growth, pubic hair, and height. J Clin Endocrinol Metab 1986;62:532–5.
14. Human Fertilisation and Embryology Act 1990(modified 2008). London: HMSO, 2008.
15. Anderson RA, Weddell A, Spoudeas HA, et al.Do doctors discuss fertility issues before they treat young patients with cancer?Hum Reprod 2008;23:2246–51.
16. Crawshaw MA, Glaser AW, Hale JP, Sloper P.Young males’ experiences of sperm bankingfollowing a cancer diagnosis – a qualitativestudy. Hum Fertil (Camb) 2008;11:238–45.
17. Bahadur G, Ozturk O, Muneer A, et al. Semenquality before and after gonadotoxictreatment. Hum Reprod 2005;20:774–81.
REPRODUCTION
www.trendsinurology.com TRENDS IN UROLOGY & MEN’S HEALTH MAY/JUNE 2013
12
Gan reproduction_Layout 1 16/05/2013 14:58 Page 5