
PRESENTER:DR HAPUNDA SUPERVISOR: DR NYAGAH 17/12/13.
49
PRESENTER:DR HAPUNDA SUPERVISOR: DR NYAGAH 17/12/13
-
Upload
julius-mason -
Category
Documents
-
view
213 -
download
0
Transcript of PRESENTER:DR HAPUNDA SUPERVISOR: DR NYAGAH 17/12/13.

PRESENTER:DR HAPUNDA SUPERVISOR: DR NYAGAH
17/12/13

OBJECTIVES1.INTRODUCTION
2.CLASSIFICATON
3.EPIDEMIOLOGY
4.ETIOLOGY
5.DIAGNOSIS 6.MANAGEMENT AND REHABILITATION
7.FUTURE AND CONTROVERSIES

INTRODUCTIONDEFINITIONA congenital malformation is a congenital physical anomaly that is deleterious, i.e. a structural defect perceived as a problem. Anomalies of external and middle ears usually occur together External and middle ear anomalies are of major importance to both the patient and the otolgist 1
1 . Pediatric otolaryngology volume 1 , Bluestone , stool,kenna




CLASSIFICATIONSYNDROMIC EAR
MALFORMATIONA typical
combination of malformations affecting more than one body part
NON SYNDROMIC EAR MALFORMATION
OssicularNon-ossicular -Vascular -Non vascular

EPIDEMIOLOGYIn the ENT region 50% of the malformations
affect the earThe incidence of ear malformations is
approximately 1 in 3800 newbornsMalformations of the outer and middle ear
are predominantly unilateral ( 70-90%) and mostly involve the right ear
11-30 % of Inner ear malformation ass with outer and middle ear malformations.
3
3. Weerda H. Chirurgie der Ohrmuschel. Verletzungen, Defekte und Anomalien. Stuttgart: Thieme; 2004. pp. 105–226.
4
4. Swartz JD, Faerber EN. Congenital malformations of the external and middle ear: high-resolution CT findings of surgical import. AJR. 1985;144:501–506.

ETIOLOGY Genetic
Acquired : infections (viral , bacterial ) chemical agents, irradiation
Unknown origin.
5
5. Pediatric syndromic hearing loss , Grand rounds Presentation , UTMB,Dept of otolaryngology Sept 24 2009 Ryan Ridley ,MD

OSSICULAR ANOMALIESEmbryogenesis
Failure of mesenchymal absorption
Failure of embryogenesis
Failure of differentiation
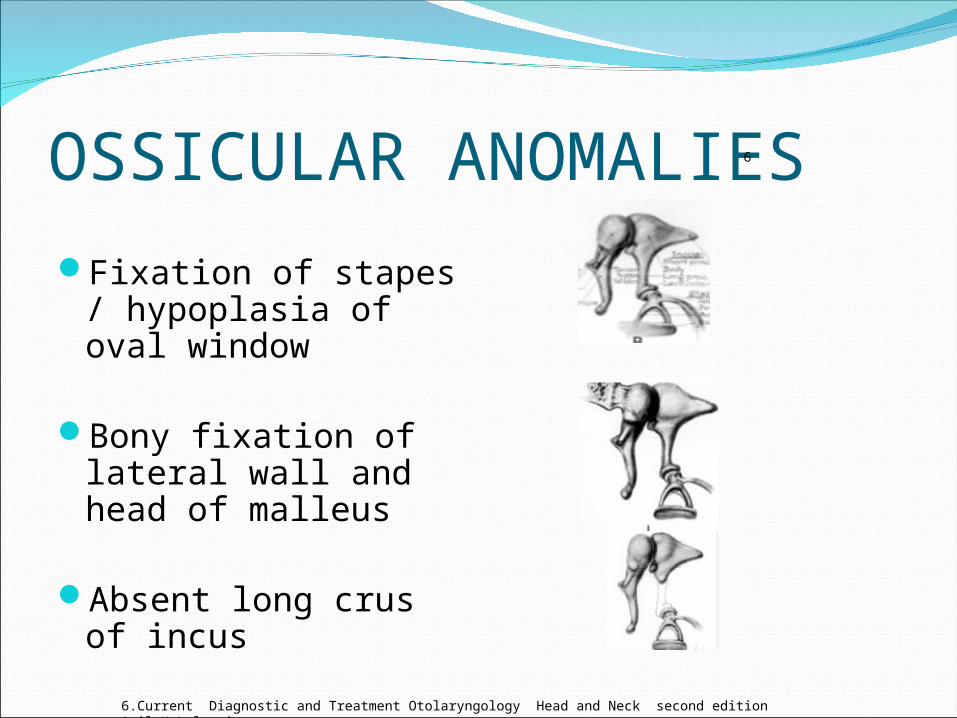
OSSICULAR ANOMALIESFixation of stapes /
hypoplasia of oval window
Bony fixation of lateral wall and head of malleus
Absent long crus of incus
6
6.Current Diagnostic and Treatment Otolaryngology Head and Neck second edition Anil K Lalwani
DIAGNOSISClinical manifestationAudiometryTympanometryImagingExploratory Surgery

ClinicalSimilar to OMECHLOtoscopic exam : unremarkable except malleus –incus fusion, hypoplasia of malleus,M/E aplasia.General exam to r/o syndrome

AUDIOGRAM OSSICULAR ANOMALIES
7. Pediatric Ear Diseases: Diagnostic Imaging Atlas and Case Reports By Yasushi Naito
7



MANAGEMENTMedical tx Surgical txAUDITORY
REHABILITAION
Hearing AidBone anchored hearing aid
By dedicated otologist
Timing of surgery?
Preop Imaging imperative
Adequate preop anesthetic assessment

CLASSIFICATION OF CONGENITAL OSSICULAR ANOMALIES OF MIDDLE EAR8
8. Teunissen and Cremer
SURIGCAL MANAGEMENT FOR OSSICULAR ANOMALIESISOLATED STAPES FOOTPLATE FIXATION- Stapedectomy / Stapedotomy
STAPES ANKYLOSIS ASS WITH OTHER DEFORMITY
- Stapedectomy/Stapedotomy - Malleovestibulopexy
9
9. Scott_Brown’s otolaryngology Head and Neck volume 1 seventh edition

ISOLATED NON STAPES M/E ANOMLIES
Tympanoplasty
Attic fixation: atticotomy
Bony bar : laser , mircodrill or currette
Absence of long process of incus : prosthesis
CONGENITAL APLASIA OR SEVERE DYSPLASIA OF THE OVAL AND ROUND WINDOW
- Auditory rehabilitation with hearing aid or BAHA


NON OSSICULAR MIDDLE EAR CONGENITAL MALFORMATIONSPERSISTENT SATAPEDIAL ARTERYIncidence : 1 in 5000-10000 asymptomaticPulsatile tinnitus CHL
Retraction or avoidance may be the most prudentmanagement.
6
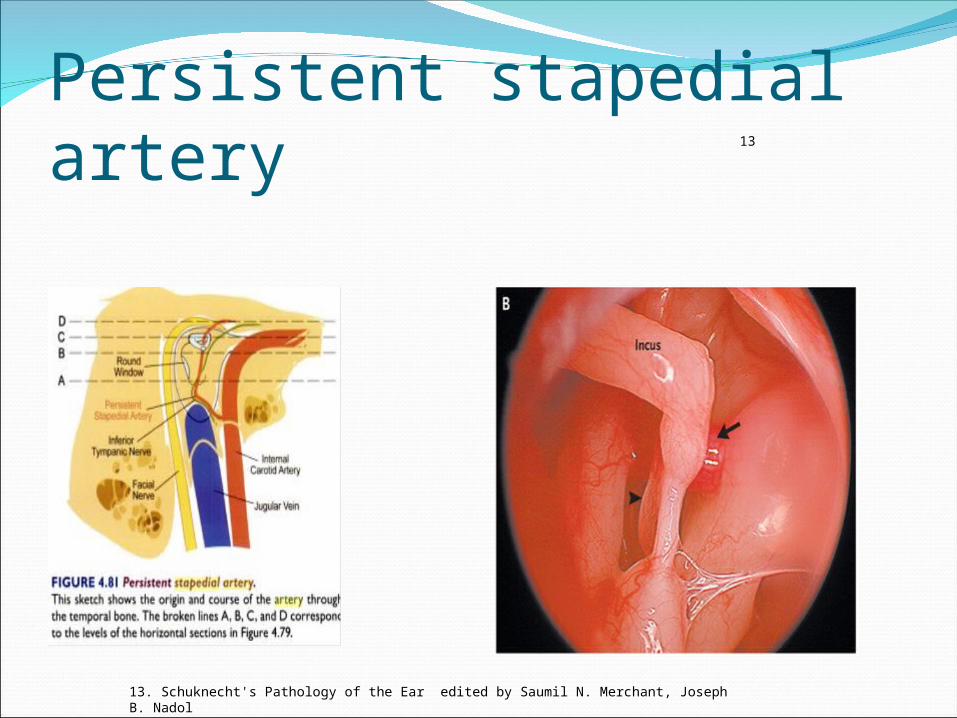
Persistent stapedial artery
13. Schuknecht's Pathology of the Ear edited by Saumil N. Merchant, Joseph B. Nadol
13

HIGH JUGULAR BULB

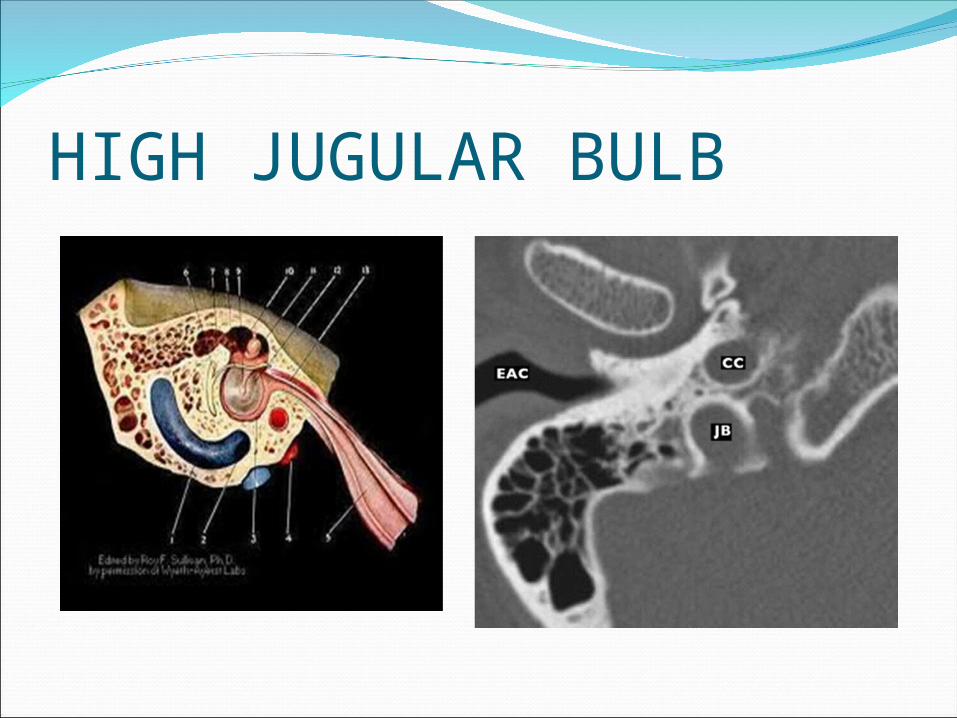
HIGH JUGULAR BULBThe bulb is subject to congenital dehiscence
and an aberrant position within the middle ear
A high riding jugular bulb is distinguished from an asymmetrically large jugular bulb by its dome (roof) reaching above the internal acoustic meatus (IAM.
If the sigmoid plate is deficient, the bulb is free to protrude into the middle ear cavity, and is then known as a dehiscent jugular bulb

HIGH JUGULAR BULB

HJBAsymptomaticTinnitusCHLD/D : aberrant ICA, PSA
glomus tympanicum tumor
Mgt: Ligation bone or cartlage
graft

ABBERANT INTERNAL CAROTID ARTERY
13

ABBERANT INTERNAL CAROTIDPulsatil tinnitusCHLOtalgiaBruit
Mgt: Covering an aberrant vessel withfascia, a bone graft, or a Silastic (ie, polymeric
silicone)sheet .

ANOMOLOUS COURSE OF FACIAL NERVETYMPANIC SEGMENT 8-11 mm Runs in facial canal, which is a Z shaped
canal running throulgh the temporal bone from the IAM to the stylomastiod foramen
Facial canal may have an anomalous course or may show dehiscent.
Facial nerve arises form otic capsule and 2nd brachial arch,cause of anomolous course is failure of fusion of the two.

ANOMOLOUS COURSE OF FACIAL NERVEFacial nerve partially
obliterates the stapes foot plate
Bifurcation of the facial nerve
Facial nerve rests on footplate with deformed stapes or oval window
Facial nerve rests on promontory14 Rohrt T ,Lorentzen P. Facial nerve displacement within the middle ear (report of 3 cases).Journal of
Laryngology and otology 1976 ;90:1093-8
14


CONGENITAL PERYLYMPHATIC FISTULA
Diagnosis-Controversial Fistula test, valsalva test , audiometry, ECOG,ENG, HRCT, MRI scan
-Weber et al define intraop diagnosis as being based on the identification of clear fluid which reacumulates with anesthetic valsalva or trendlenburg manoeuvre.-Beta transferrin positive samples 15 Weber PC ,Bluestone CD , Perez B . Outcome of hearing and vertigo after surgery for
congenital perilymphatic fistula in children . American Journal of Otolaryngoloy .2003;
15

CONGENITAL PERYLYMPHATIC FISTULATreatment As a result of difficulty in diagnosis , weber et
al suggest packing temporalis muscle around oval and round windows in all suspected cases, based on the finding that packing does not cause complications such as CHL.15

CONGENITAL CHOLESTEATOMACriteria of Derlaki
and Clemis -White mass medial
to an intact T/M-Normal pars tensa
and flaccida-No previous hx of
ear discharge, perforation or previous otological procedure

CONGENITAL CHOLESTEATOMAPathogenesis
ASQ : failure of normal involution of epidermoid tissue
PQ: posterior migration of ant epidermoid tissue
Amniotic cellular material in M/E Ingrowth of epithelium from EAC thru
defect TR
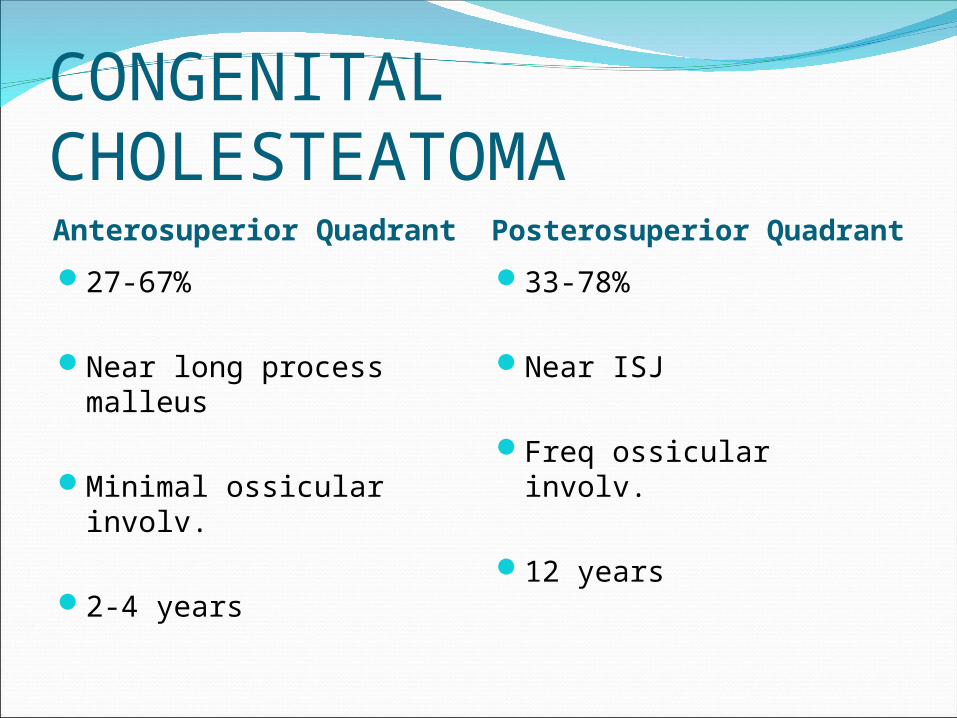
CONGENITAL CHOLESTEATOMAAnterosuperior Quadrant
Posterosuperior Quadrant
27-67%
Near long process malleus
Minimal ossicular involv.
2-4 years
33-78%
Near ISJ
Freq ossicular involv.
12 years

CONGENITAL CHOLESTEATOMACLASSIFICATIONType 1 – Confined to the
middle ear and do not involve the ossicles
Type 2 – Involve the posterior superior quadrants and attic, the site of the ossicular chain
Type 3 – Involve the sites of type 1 and 2 as well as the mastoid
STAGESStage I – Limited to one
quadrant
Stage II – Involving multiple quadrants without ossciular involvement
Stage III – Ossicular involvement without mastoid extension
Stage IV – Mastoid involvement (67% risk of residual cholesteatoma)
16.Nelson et. al Congenital Cholesteatoma: Classification, Management and Outcome. Arch Oto Head Neck Surg July 2002; 128: 810:814
17.Levenson MJ et al. Congenital cholesteatomas in children: an embryologic correlation. Laryngoscope. 1988; 98:949-955
16
17

CONGENITAL CHOLESTEATOMAmanagementType 1 – Controlled by extended tympanotomy.
No second-look re-operation.
Type 2 – Extended tympanotomy. Possibly atticotomy and canal wall up tympano-mastoidectomy with or without opening of the facial recess. Require second look. Possible ossicular reconstruction.
Type 3 – Similar to type 2, but occasionally need a canal wall down tympanomastoidectomy
17

OTHER M/E ANOMALIESTYMPANIC MEMBRANE ANOMALIEST/M replaced by fibrous tissueSmall T/MDistorted T/MEUSTACHIAN TUBE ANOMALIESAbsenceAbnormally narrowCongenital tumor(polyp)Collapsed lumen of ET

MASTOID ANOMALIESAbsence of mastoid antrumPoorly developed mastoid antrumSmall mastoid process

SYNDROMIC MIDDLE EAR CONGENITAL MALFORMATIONHearing loss is one of the most common
congenital anomalies, occurring in approximately 2-4 infants per 1000
Approximately one-third of children with genetic hearing loss will display phenotypic characteristics of a syndrome while two-thirds will be nonsyndromic
Whether the hearing loss is syndromic or
nonsyndromic, it is of the utmost importance to identify these patients early

DOWNS SYNDROMEThe hearing loss in DS is usually conductive secondary to the chronic middle ear disease but can also be due to ossicular chain abnormalities, especially the stapes
Middle ear : thickening of malleus as a result of bone hyperplasia , fusion of the malleolar head to the body of the incus, spongy apperance of the long process of the incus, and abnormalities of the stapes.

OSTEOGENSIS IMPERFECTA
Causative mutations involve the COL1A1 or COL1A2 gene which regulate formation of type I collagen. The conductive component of the hearing loss is attributed to the thickened and fixed stapes footplate, similar to what is seen in otosclerosis.
TREACHER COLLIN
Hearing loss in this syndrome is usually conductive with a wide array of middle ear anomalies present such as monopodal stapes, ankylosed foot plate,

1. History TakingExaminationInvestigationsBehavioural hearing assessment,
Electrophysiological hearing tests, Tympanometry
ManagementMedical, Surgical, Rehabilitation (hearing aids)
and Follow-up

REFERENCES 1. Pediatric otolaryngology volume 1 , Bluestone , stool,kenna 2.Surgery of the Ear Glasscock-Shambaugh 3. Weerda H. Chirurgie der Ohrmuschel. Verletzungen, Defekte und Anomalien. Stuttgart: Thieme; 2004.
pp. 105–226 4. Swartz JD, Faerber EN. Congenital malformations of the external and middle ear: high-resolution CT
findings of surgical import. AJR. 1985;144:501–506.Current Diagnostic and Treatment Otolaryngology Head and Neck second edition Anil K Lalwani
5.Pediatric syndromic hearing loss , Grand rounds Presentation , UTMB,Dept of otolaryngology Sept 24 2009 Ryan Ridley ,MD
6.Current Diagnostic and Treatment Otolaryngology Head and Neck second edition Anil K Lalwani 7. Pediatric Ear Diseases: Diagnostic Imaging Atlas and Case Reports By Yasushi Naito 8. Teunissen and Cremer 9. Scott_Brown’s otolaryngology Head and Neck volume 1 seventh edition 10 surgical atlas of Pediatric Otolaryngology Bluestone and Rosenfeld 11.Van der Hoeve J, de Kleyn A. Blaue skleren, knochenbruchigkeit und schwerhohrigkeit. Arch Ophthalmol
1918; 95:81-93. [German 12. Clinical audiology Brad A Stach 13. Schuknecht's Pathology of the Ear edited by Saumil N. Merchant, Joseph B. Nadol 14 Rohrt T ,Lorentzen P. Facial nerve displacement within the middle ear (report of 3 cases).Journal of
Laryngology and otology 1976 ;90:1093-8 15 Weber PC ,Bluestone CD , Perez B . Outcome of hearing and vertigo after surgery for congenital
perilymphatic fistula in children . American Journal of Otolaryngoloy .2003; 16.Nelson et. al Congenital Cholesteatoma: Classification, Management and Outcome. Arch Oto Head Neck
Surg July 2002; 128: 810:814 17.Levenson MJ et al. Congenital cholesteatomas in children: an embryologic correlation. Laryngoscope.
1988; 98:949-955

FUTURE AND CONTROVERSEYDevelopments in middle ear implantation
may render corrective surgery almost redundant
The incidence , aetiology and pathogensis of congenital ossicular abnormalities is poorly understood.


















