Presented in collaboration with Nebraska ICAP, …...2020/06/02 · •Rapid tests –antigen or...
30
Presented in collaboration with Nebraska ICAP, Nebraska DHHS HAI Team, Nebraska Medicine, and The University of Nebraska Medical Center Moderated by Mounica Soma Panelists: Dr. Trevor Van Schooneveld Angie Vasa, RN, BSN Kate Tyner, RN, BSN, CIC Margaret Drake, MT(ASCP),CIC Teri Fitzgerald RN, BSN, CIC Dr. Ishrat Kamal-Ahmed Guidance and responses were provided based on information known on 6/2/2020 and may become out of date. Guidance is being updated rapidly, so users should look to CDC and jurisdictional guidance for updates.
Transcript of Presented in collaboration with Nebraska ICAP, …...2020/06/02 · •Rapid tests –antigen or...

Presented in collaboration with Nebraska ICAP, Nebraska DHHS HAI Team, Nebraska Medicine, and
The University of Nebraska Medical Center
Moderated by Mounica Soma
Panelists:Dr. Trevor Van SchooneveldAngie Vasa, RN, BSNKate Tyner, RN, BSN, CICMargaret Drake, MT(ASCP),CICTeri Fitzgerald RN, BSN, CICDr. Ishrat Kamal-Ahmed
Guidance and responses were provided based on information known on 6/2/2020 and may become out of date. Guidance is
being updated rapidly, so users should look to CDC and jurisdictional guidance for updates.

Questions and Answer SessionUse the QA box in the webinar platform to type a question. Questions will be read aloud by the moderator
If your question is not answered during the webinar, please either e-mail it to NE ICAP or call during our office hours to speak with one of our IPs
A transcript of the discussion will be made available on the ICAP website
Panelists today are:
Dr. Trevor Van Schooneveld [email protected] Tyner, RN, BSN, CIC [email protected] Drake, MT(ASCP),CIC [email protected] Fitzgerald RN, BSN, CIC [email protected] Vasa, RN, BSN [email protected]. Ishrat Kamal-Ahmed [email protected]
https://icap.nebraskamed.com/coronavirus/https://icap.nebraskamed.com/covid-19-webinars/

Testing for SARS-CoV-2
Trevor Van Schooneveld, MD
Associate Professor, Infectious Diseases
6/2/20

Testing for SARS-CoV-2
Trevor Van Schooneveld, MD
Associate Professor, Infectious Diseases
6/2/20

How to Diagnose COVID-19
How do you diagnose viral infections?
• Clinically – symptom-based
• Imaging
• Serology – IgM, IgA, IgG
• Rapid tests – antigen or antibodies
• Culture
• Molecular Testing

Clinical Diagnosis
Symptoms Hospitalized Chinese (N=140) US HCW (N=9282)
Fever, cough, or SOB NA 92%
Cough 80% 78%
Fever 87% 68%
SOB 38% 41%
Myalgia 21% 66%
Headache 8% 65%
Sore Throat 5% 38%
Diarrhea, Nausea/vomiting 2%/1% 32%/20%
Loss of Smell or Taste NA 16%
Runny Nose 4% 12%
• Hospitalized Chinese - mostly older (63% >50 yo), 63% male• HCW - mostly younger (55% <45 yo), 73% female
Huang, C, et al. Lancet. 2020;395:497.Chen, N, et al. Lancet. 2020;395:507-13. CDC. MMWR. 2020;69:477-81.
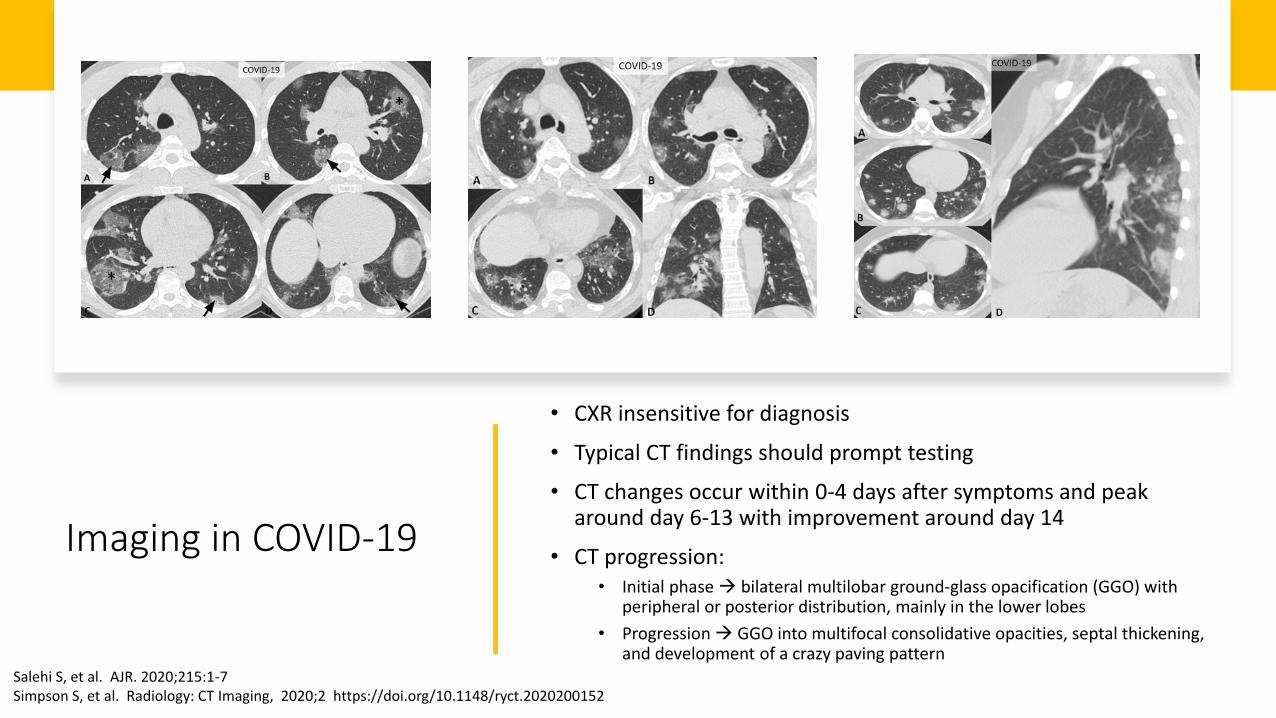
Imaging in COVID-19
• CXR insensitive for diagnosis
• Typical CT findings should prompt testing
• CT changes occur within 0-4 days after symptoms and peak around day 6-13 with improvement around day 14
• CT progression:• Initial phase bilateral multilobar ground-glass opacification (GGO) with
peripheral or posterior distribution, mainly in the lower lobes
• Progression GGO into multifocal consolidative opacities, septal thickening, and development of a crazy paving pattern
Salehi S, et al. AJR. 2020;215:1-7Simpson S, et al. Radiology: CT Imaging, 2020;2 https://doi.org/10.1148/ryct.2020200152

Testing Primer
• The sensitivity of a test means how well it can correctly identify those who have COVID-19 infection
• The specificity of a test means how well it can correctly identify those who do not have COVID-19 infection
• The positive predictive value of a test is the likelihood that a positive test result indicates that a person is truly positive for COVID-19 infection.
• The negative predictive value of a test is the likelihood that a negative test result indicates that a person is truly negative for COVID-19 infection.

Tests Available
• Molecular Tests (PCR, NAAT)• Amplify RNA of the virus• Use Case = Diagnosis of acute infection
• Antigen Tests• Detect viral antigens• Don’t amplify• Use Case = Rapid diagnosis of acute infection
• Serology• Detect antibodies made by the immune system• Detected after acute infection develops• Use Case = defining previous infection, population prevalence
• Culture • Grow the virus• Slow and not widely available• Use Case = Defining infectivity period

Serology
• What we know• Robust and rapid serologic response of IgM,
IgA and IgG
• IgM rises within 5-7 days symptom onset
• Seropositivity at 14 days: IgM (88-94%), IgG (94-100%)
• NM Serology Performance (IgG assay)• 0-5 days illness onset – 25% agreement
• 6-14 days – 90% agreement
• >15 days – 94.5% agreement
• Specificity 99.3%
• 16/214 positive (7.8%)
To, K, et al. Lancet. 2020 https://doi.org/10.1016/S1473-3099(20)30196-1
Serologic Response in Severe and Mild COVID-19 Infection (N=23)

Serology Questions
What we don’t know
• Utility in diagnosing acute infection?• IgG poor early• IgM assay cross-reactivity
• Performance in mild disease?
• Performance in asymptomatic?
• The false positive question
• Is a positive serology protective against subsequent infection and for how long?

Who to Test
• All persons with symptoms suspicious for COVID-19
• Previously testing was prioritized due to limited capacity• Patients being hospitalized• Healthcare workers and those who work in healthcare environments• Ambulatory patients at increased risk for poor outcomes or who work in high risk
environments• Older adults (age ≥ 65 years) • Those who are immunocompromised or have chronic medical conditions (e.g., diabetes,
chronic lung, heart, or kidney disease)• Long-term care facility residents or those who reside in other group settings (homeless
shelter, group home, etc.)• Public safety workers and first responders • Persons performing duties or administering care in settings where spread of COVID19 would
be particularly disadvantageous: group homes, prisons, assisted living facilities, long term care, etc.
TEST

Testing Asymptomatic Persons• Molecular tests
• Pre-organ transplant, bone marrow transplant• Not generally recommended outside of outbreak investigation
• LTCF, group settings, etc.• Being done widely…
• Admission screening• Likely low yield and potentially inaccurate in low prevalence settings
• Pre-procedural• Much debate, yield very low (false +?), potentially to preserve PPE
• Post-exposure testing not generally recommended• When and how often?• A negative doesn’t rule out subsequent development of disease
• Serology • May be a role• Define population prevalence, determine retrospectively if infected, monitor
healthcare workers, determine incidence of asymptomatic infection
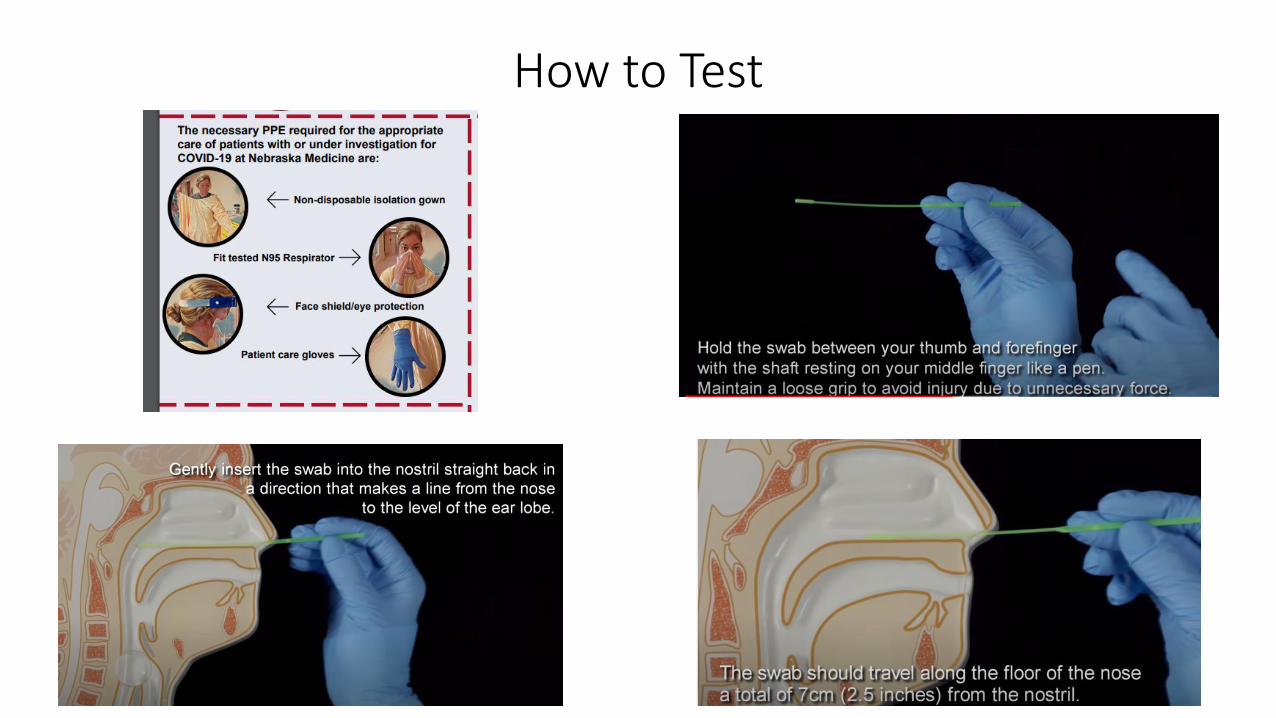
How to Test

Rapid Testing
• CLIA waived tests
• Results in 5-15 minutes
• Molecular
• Antigen and serologic coming
• Performance parameters undefined
• Reports of decreased sensitivity• Useful early in infection
• Good for ruling in, less so for ruling out
• Urgent care, ED, clinic??

Molecular Tests in Use at NM
• Numerous platforms available
• Nebraska Medicine currently using the following (TAT <18 hours)• Roche Cobas 6800 (COV19)• Laboratory developed test (NECoV19) • Regional Lab using a third platform
• NPHL using the CDC designed assay• Increasing capacity and batching
• Rapid testing (TAT <4 hours)• Biofire SARS-CoV-2 only• Biofire Respiratory Pathogen Panel with SARS-CoV-2 (coming soon)• Cepheid

2003
2019-20
Li X, et al. J Pharma Analysis. 2020; https://doi.org/10.1016/j.jpha.2020.03.001

Roche assay
Roche assayNM Assay
NPHL assayNM Assay
Li X, et al. J Pharma Analysis. 2020; https://doi.org/10.1016/j.jpha.2020.03.001

Test Results Interpretation
• Slight variations in how results are reported based on targets• Understand what is being reported at your facility
• Roche (E- and ORF1a-)• E- and ORF1a- not detected = COVID Not Detected• E- and ORF1a- detected = COVID Detected• Only E- detected = Presumptive positive
• E- is same in SARS-CoV-1 but this virus is not circulating• Invalid – test didn’t work Repeat swab
• NE COV Test (E- and N-)• E- not detected = Not Detected• E- detected Will be retested on next run for both E- and N-
• If either detected = COVID Detected• If neither detected = Inconclusive Repeat swab

Should I Get Two Tests in Symptomatic Person
• Depends on how well you did the swab
• Depends on the assay
• Depends on where you are in the illness course
• Early in the illness upper airway viral levels are very high but begin to decline after 7 days
• Numerous reports of patients presenting with typical symptoms and especially pneumonia and having a negative initial NP but then a second NP or lower respiratory tract specimen being positive
How good is the test?
Does our experience help us?
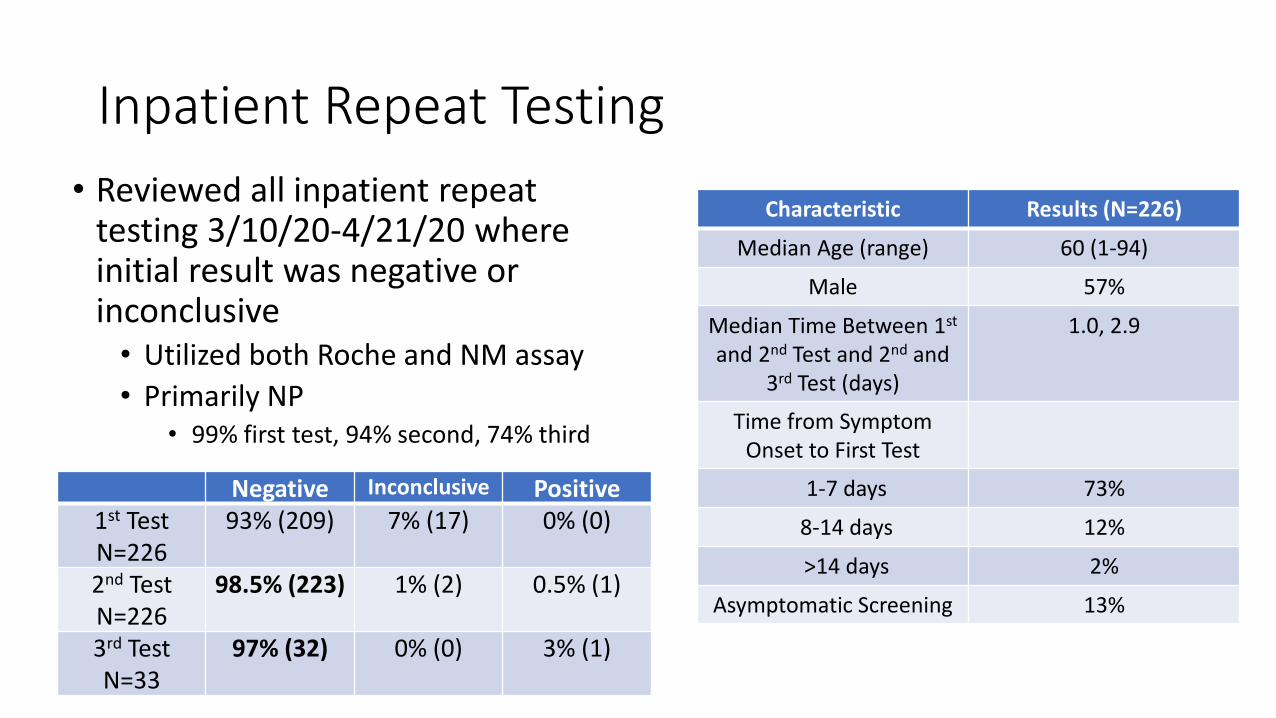
Inpatient Repeat Testing
• Reviewed all inpatient repeat testing 3/10/20-4/21/20 where initial result was negative or inconclusive• Utilized both Roche and NM assay
• Primarily NP• 99% first test, 94% second, 74% third
Characteristic Results (N=226)
Median Age (range) 60 (1-94)
Male 57%
Median Time Between 1st
and 2nd Test and 2nd and 3rd Test (days)
1.0, 2.9
Time from Symptom Onset to First Test
1-7 days 73%
8-14 days 12%
>14 days 2%
Asymptomatic Screening 13%
Negative Inconclusive Positive1st TestN=226
93% (209) 7% (17) 0% (0)
2nd TestN=226
98.5% (223) 1% (2) 0.5% (1)
3rd TestN=33
97% (32) 0% (0) 3% (1)

Our Recommendation on Second Test
• Outpatient repeat testing not usually indicated unless change in status (worsened, admitted, etc.)
• Inpatients are in a higher risk environment• Patients who have recently developed symptoms (7 days) usually can be ruled
out with one test• Implemented algorithm for determining who can be ruled out with one test
• Those who have a high-risk clinical presentation (typical symptoms, classic CT findings, known exposure, etc.), high risk exposure, or evidence of pneumonia should generally have a second test obtained• Preferably from lower respiratory tract if possible

Testing and Duration of Isolation
• Symptom-based vs. Test-based
• Symptom-based • Can exit isolation when symptoms resolve/improve• CDC = can exit isolation 10 days after symptom onset and 3 days after symptoms
subsidence (no fever, other symptoms improving)• Outpatient we are using 10 + 5 and immunocompromised 14 + 7
• Test-based• Require 2 tests done at least 24 hours apart to be negative• Inpatient we are using test-based strategy
• Evidence of prolonged viral RNA shedding (days to weeks)• Is this infectious virus???

Testing and Duration of Isolation• Emerging evidence that viral shedding ceases around day
10 after symptom onset• Detection of viral RNA vs. Detection of viable virus
• COVID19 patients who exited isolation based on symptoms and subsequently tested positive (N=285). • 108 underwent viral culture and no viable virus was detected• 790 contacts of were traced with zero confirmed transmissions.
• 73 COVID-19 positive patients, viable virus could not be isolated or cultured after day 11 of illness.
Viral Culture Detection After Symptom Onset
Wölfel, R. et al. Nature https://doi.org/10.1038/s41586-020-2196-x (2020).https://www.cdc.gov/coronavirus/2019-ncov/community/strategy-discontinue-isolation.htmlhttps://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030https://www.ams.edu.sg/view-pdf.aspx?file=media%5c5556_fi_331.pdf&ofile=Period+of+Infectivity+Position+Statement+(final)+23-5-20+(logos).pdf
UnknownsImmunocompromisedElderly
“Virus has not been successfully cultured more than 9 days after onset of illness. The statistically estimated likelihood of recovering
replication-competent virus approaches zero by 10 days”

Retesting in Patients with Resolved Infection
• Not generally recommended for at least 3-6 months
• Duration of immunity is unknown

Monday – Friday
7:30 AM – 9:30 AM Central Time
2:00 PM -4:00 PM Central Time
Call 402-552-2881
IP Office Hours

Questions and Answer SessionUse the QA box in the webinar platform to type a question. Questions will be read aloud by the moderator
If your question is not answered during the webinar, please either e-mail it to NE ICAP or call during our office hours to speak with one of our IPs
A transcript of the discussion will be made available on the ICAP website
Panelists today are:
Dr. Trevor Van Schooneveld [email protected] Tyner, RN, BSN, CIC [email protected] Drake, MT(ASCP),CIC [email protected] Fitzgerald RN, BSN, CIC [email protected] Vasa, RN, BSN [email protected]. Ishrat Kamal-Ahmed [email protected]
https://icap.nebraskamed.com/coronavirus/https://icap.nebraskamed.com/covid-19-webinars/

Questions and Answer SessionUse the QA box in the webinar platform to type a question. Questions will be read aloud by the moderator, in the order they are received
A transcript of the discussion will be made available on the ICAP website
Dr. Trevor Van Schooneveld
Kate Tyner, RN, BSN, CIC
Margaret Drake, MT(ASCP),CIC
Teri Fitzgerald RN, BSN, CIC
Angie Vasa, RN, BSN
Dr. Ishrat Kamal-Ahmed
Moderated by Mounica Soma, MHA https://icap.nebraskamed.com/resources/

Responses were provided based on information known on 6/2/2020 and may become out of date.
Guidance is being updated rapidly, so users should look to CDC and NE DHHS guidance for updates.
NETEC – NICS/Nebraska DHHS HAI-AR/Nebraska ICAP Small and Critical Access Hospitals-Outpatient Region VII Webinar on COVID-19 6/2/2020
1. We want to use a MDI spacer for multiple patients in our respiratory disease clinic. How do we
disinfect the spacer to use it for different patients?
Nebraska Medicine has a process that includes taking the canister portion out and cleaning that
part of the spacer. Check the manufacturer’s instructions for the MDI portion of the equipment
to see if they say it is something that can be reprocessed. You will know that it can’t be
reprocessed if it has a “2” with an “X” through it - . This means the device cannot be used
for more than one patient. You can’t try to reuse it. If it does have some disinfection guidance
you need to follow those manufacturer’s direction. The canister of drug could be removed and
disinfected and reused but the plastic component would be difficult to clean. You are bound to
follow the manufacturer’s rules.
2. Some employers are requiring a negative test after infection prior to return to work. But they
have been finding the test may be positive for several weeks even though the staff member is
asymptomatic and meets clinical criteria to return to work. What is the recommendation in
these cases?
For people like that, you can’t dictate employer policy; but that is the problem using a test-out
(test based) strategy, because there are people who are shedding viruses for a long period of
time. That is why the CDC made that very clear statement. Nebraska Medicine is allowing
healthcare workers to return to work; we use universal masking and no test to return to work
policy is in place. Dr. VanSchooneveld’s personal opinion is -- The one question might be
immune-compromised workers, but in general, for workers who are better and meet the CDC
criteria, they can return to work at Nebraska Medicine.
3. Our lab is being told that VTM is still on short supply. Is this true throughout the state?
Dr. VanSchooneveld said that he has heard that viral transport material is in short supply.
Nebraska Medicine has been manufacturing some of their own. There have been shortages of
all Testing supplies.
4. Why is there so little info on presence of immunity or duration of protective effects? Can
you summarize any current practices for postpositive staff returning to work in your system?
The reason for there is so little information on immunity is that this virus has only been around
since December 2019. We only have 6 months of experience to study it. Animal studies are
going on, which will help us understand this. That is why we don’t know the duration of
immunity. Current practice for post-positive depends on the decision a facility makes on what
criteria is being used, whether test-based or symptom-based and do they meet your criteria.
Make sure your people follow your safety practices. Our experience is that the most
problematic are staff members who have mild symptoms and continue to work anyway, not
doing anything about it and exposing other people.

5. If you have an employee who is testing positive and they are off the recommended amount of
time, do you retest them before coming back to work? Do you treat them differently
depending on whether they are symptomatic versus asymptomatic?
For symptomatic, they need to meet the criteria for symptomatic return. For asymptomatic,
Nebraska Medicine has said they are off work 10 days post-positive test. We want to give
people time to make sure that even if they are asymptomatic at the time of the test, they could
still develop symptoms later and then would have to stay out even longer. You need to set your
policy, test-based or symptom-based, and that may look different depending on your work
environment and safety practices at your work.
6. Does Dr. VanSchooneveld have an opinion about the Italian doctor’s report that the virus is
"weakening"?
Dr. VanSchooneveld is not familiar with that report. A virus can certainly mutate, and some
think it may mutate and become less lethal (more like a common cold), but others think the
opposite, that it could mutate and get worse. It has stayed about the same throughout the
outbreak so far in his experience.
7. Do you have any recommendations on isolation precautions for patients who have had a
negative Covid result, but has symptoms that may indicate the post-COVID syndrome?
There are complications that can occur with COVID, but if they don’t have a positive molecular
test (which we have found is so sensitive that it can stay positive for weeks after people can
cause infection to other people). If a person has had two negative tests, at least 24 hours apart,
then that person doesn’t need any additional isolation.
We recommend staying abreast of changes in testing. Test strategies are going to continue to
evolve. What we are doing today may be different two months from now. That is pretty typical,
so we need to be willing to stay dynamic. Dr. VanSchooneveld doesn’t think acute infections are
going to go away. All of our screening protocols may change in the future, though.