Presented by Jodi McGraw, M.D. - Home | UW Health · 2017-06-22 · Cord dangling out of vagina or...
23
Presented by Jodi McGraw, M.D.
Transcript of Presented by Jodi McGraw, M.D. - Home | UW Health · 2017-06-22 · Cord dangling out of vagina or...

Presented by Jodi McGraw, M.D.

Gravida (gravidity)= number of pregnancies Para (parity)= number viable gestational age pregnancies Eg. G3P2 (third pregnancy & 2 deliveries) G5P2 (1,1,3,2)=full term, preterm, miscarriage or abortions, living
Trauma in OB, treat the Mom O2, 2x large bore IV’s, left lateral position if able based on trauma. Treat the injuries

Medical documentation obtained at Patient visits for patient record - Due date - Menstrual history - Prior pregnancy history - Medical history

Symptoms since LMP genetic screening Infection history physical exam

Additional notes for visit

Typical format for OB visit details

Labs & education at visits Blood type Infections GBS

Labs for 2nd & 3rd trimesters Anemia testing Gestational diabetes screen Rhogam if needed

Plans & education

19 yo G1P0 at 39 EGA, no local medical care, uncomplicated pregnancy, negative GBS at 36 weeks, no meds, NKDA, healthy Contractions q3 min Fluid leaking (?clear), but not bleeding +fetal movement
A few potential problems: Edema 60# weight gain Elevated blood pressure, leg swelling, Bleeding, abdominal pain, SOB
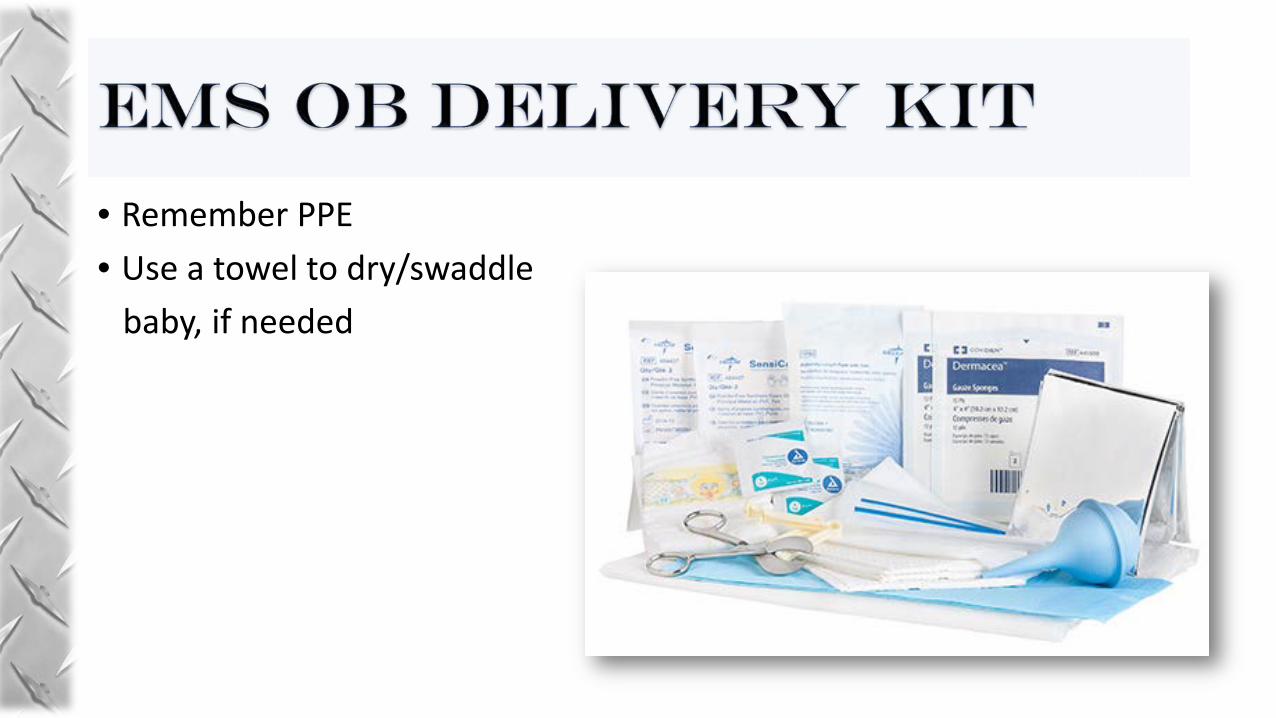
• Remember PPE • Use a towel to dry/swaddle baby, if needed

This is what our OB tray looks like Basic EMS kit will have essentials

• Record and document events as able
• Most important times: infant birth time placenta delivery time
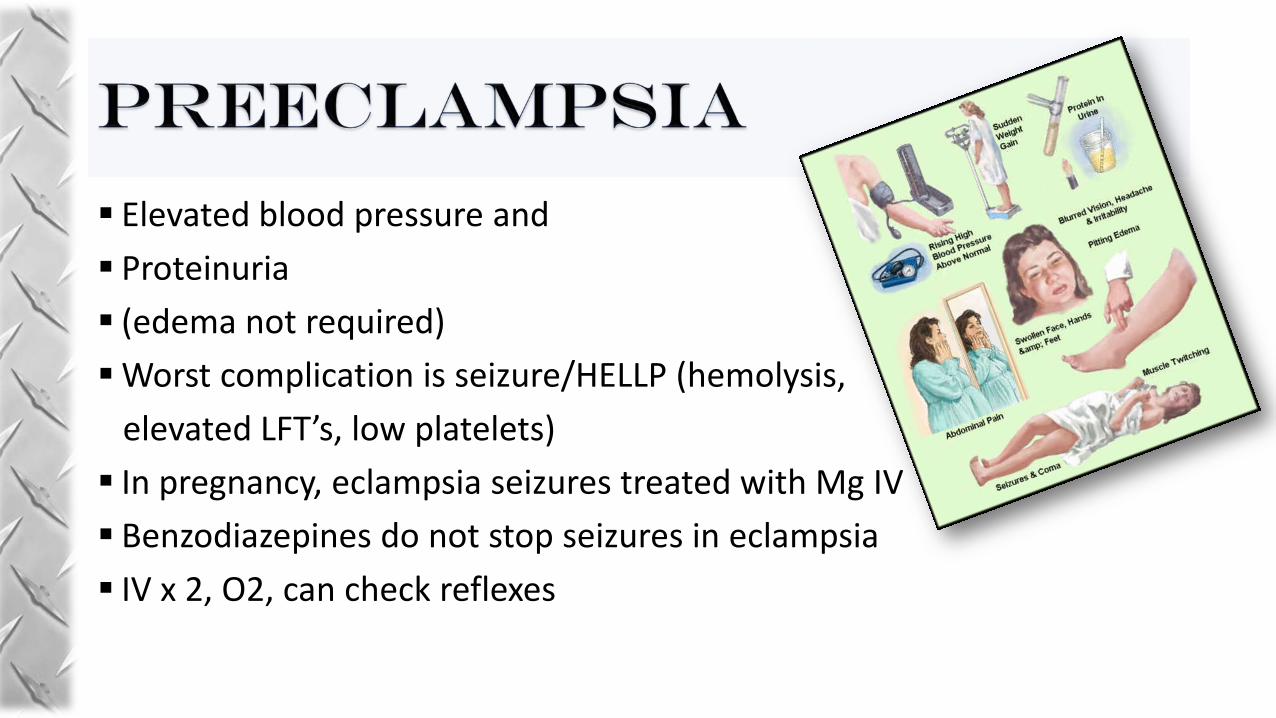
Elevated blood pressure and Proteinuria (edema not required) Worst complication is seizure/HELLP (hemolysis, elevated LFT’s, low platelets) In pregnancy, eclampsia seizures treated with Mg IV Benzodiazepines do not stop seizures in eclampsia IV x 2, O2, can check reflexes

Cord dangling out of vagina or cervix Compresses baby’s lifeline EMERGENCY! Notify ER! Elevate pelvis and manually Push infants head off the cord Without compressing the cord Emergent Cesarean! IV x 2, O2

Typically severe abdominal pain (not just with contractions) Bleeding extent may not be apparent EMERGENCY! Start O2, IV x 2, position

Pushing can be >2 hours in primiparous Patient, but may be 1-2 hours in multiparous May be precipitous If preterm, expect precipitous & consider Malpresentations- eg breech Chin first does not deliver! Neck can not hyperextend Clamp x 2 & cut cord between clamps Placenta may take ~1-20 minutes

3-4% of deliveries, injuries e.g. clavicle fractures more common Prematurity is risk Deliver spontaneous until umbilicus is at introitus Then, support trunk Remove 1 arm at a time Head most difficult: Flex neck

HELLPER H- call for extra Help EL- elevate legs- McRobert’s P- suprapubic Pressure to reduce the anterior shoulder Enter- rotational maneuvers R- Reverse rotation (consider hands to knees)

2nd & 3rd trimester bleeding: placenta previa uterine rupture placenta abruption vasa Previa
Postpartum hemorrhage- compress
O2, IV x 2, compression, position

Awesome! Please feel welcome to participate and ask questions

Good history Evaluate for complications Shoulder dystocia Bleeding/hemorrhage DVT Pre-eclampsia delivery

With Great Appreciation for all you do! Questions? Practice with mannequin?