Presentazione standard di PowerPoint · immunoprophylaxis in preventing MTCT. •High serum HBV DNA...
29
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida
Transcript of Presentazione standard di PowerPoint · immunoprophylaxis in preventing MTCT. •High serum HBV DNA...
Epatite B: fertilità, gravidanza ed allattamento,
aspetti clinici e terapeutici
Ivana Maida
• Positivity for HBsAg was found in 0.5% of tested women
• In the ‘70s and ‘80s, Italy was one of the European countries with the highest prevalence of hepatitis B. However, both the incidence and the prevalence of HBV and all parenterally transmitted viruses have impressively decreased over the last 30 years, as a consequence of the introduction – in 1991 – of the compulsory vaccination policy for all newborns and 12-year-old adolescents and the mandatory HBV screening of pregnant women, as well as the improvement of the hygiene and socioeconomic conditions and the introduction of public health measures
• The low prevalence of HBsAg found in our cohort clearly reflects the success and effectiveness of these implemented vaccination and surveillance policies
• the number of HBsAg carriers in our cohort was significantly higher among non-Italian than among Italian women (3%vs. 0.2%)
• In order to reduce the global burden of HBV infection, prevention of HBV vertical transmission is fundamental. Thus, particular efforts should be made to increase the awareness of young women, encouraging their adherence to screening and vaccination programs, with particular attention to the immigrant minorities
• HBV infection is an important global health problem.
• More than 240 million people worldwide are chronically infected with HBV.
• Most acquire their infections during the perinatal period or in early childhood in endemic areas.
• Exposure to HBV via MTCT and during early childhood is also associated with an increased risk of developing CHB.
• Perinatal hepatitis B virus (HBV) infection is associated with a 90% risk for chronic infection, which carries a 25% risk of death from liver failure and hepatocellular carcinoma
• Effectively preventing MTCT of HBV from pregnant women to their newborns within the perinatal period is an important and efficient approach to prevent CHB.
• Newborns have 90% chance to become chronic carriers after infection with HBV and in children less than 3 years old the chance is up to 50%, but in adults the chance is only up to 5%.
• HBV infection can still occur in ∼8.5% of children born to mothers with high HBV DNA levels
• Perinatal HBV infection has been shown to correlate linearly with increasing HBV DNA levels
• In addition, maternal health can also be adversely affected during pregnancy due to HBV reactivation.
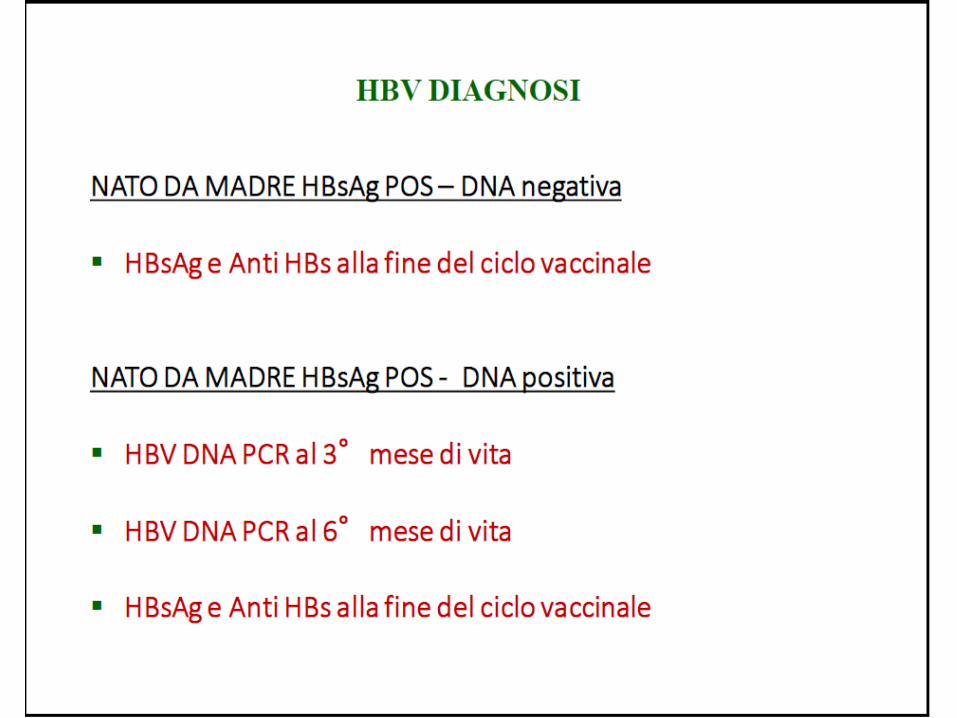
• Postnatal administration of HBV vaccination and immunoglobulin is now universally recommended to reduce the risk of perinatal transmission.


• Pregnant women have mechanisms that prevent rejection of the baby by the maternal immune system. Thus, there are significant immunologic changes that occur during pregnancy and the postpartum period, which may impact the natural history and clinical manifestations of chronic HBV infection. An increased production of hormones such as adrenal corticosteroids, estrogen, and progesterone has been reported during pregnancy which may lead to a relative immunosuppressed state and enhanced HBV DNA levels.
• Postpartum flares were common (25%) even in the absence of antiviral therapy, which were usually mild, asymptomatic, and usually resolved spontaneously by 12 months. HBeAg-positive women were twice as likely to have a flare postpartum.
• A proportion of HBsAg-positive mothers developed a severe acute exacerbation, which may even lead to fulminant hepatic failure. The risk for fulminant hepatic failure is higher in patients with unrecognized cirrhosis or advanced fibrosis.
• Therefore, more frequent monitoring during pregnancy and first 6-month postpartum is needed. No specific frequency has been recommended by most professional guidelines, but testing of HBV DNA and liver panel every 6 weeks during first 2 trimesters and every 4 weeks during the last trimester and first 3 months postpartum may be reasonable.
• The most significant potential outcome of postpartum flares is HBeAgseroconversion. A prospective study of 40 pregnancies has reported a higher than expected rate (12%) of HBeAg seroconversion in the early postpartum period. A sudden decrease in cortisol level immediately after delivery could be analogous to that in steroid withdrawal therapy, causing the reactivation episode associated with or without HBeAg seroconversion

• MTCT might occur either while the baby is still in the uterus (prenatal, antepartum, in utero, or intrauterine transmission), during the delivery process (natal or intrapartum transmission), or shortly after birth (postpartum or during childcare or through breast milk). Intrauterine transmission of HBV is considered to be the most important reason for the failure of passive-active immunoprophylaxis in preventing MTCT.
• High serum HBV DNA levels and HBeAg-positive status in pregnant mothers are key factors for indicating the increased risk of MTCT of HBV, especially in intrauterine transmission of HBV through villous capillary endothelial cells.
• HBeAg positivity is an independent risk factor for the MTCT of HBV. In fact, HBeAg can pass through the placenta via partial placental leakage or via the “cellular route.” The absence of HBeAg expression is associated with lower levels of viral replication and with a significantly lower risk of intrauterine transmission of HBV.
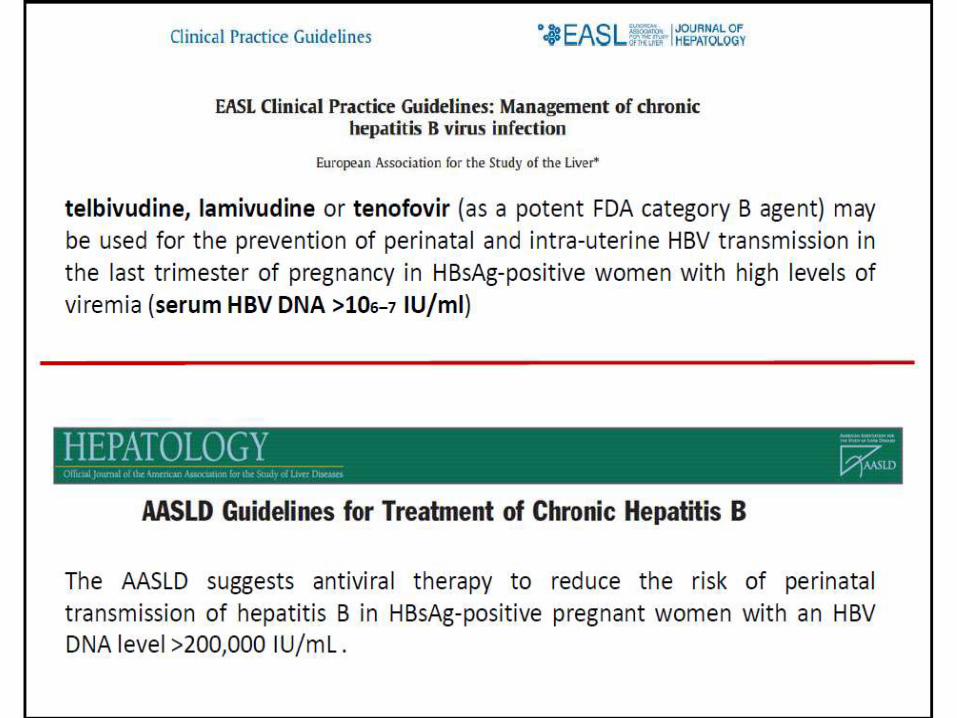
• Recent studies suggest that a HBV DNA levels >200,000 IU/mL is associated with a higher rate of MTCT of 8% to 30%.
• Other risk factors carry a much lower risk for MTCT, including amniocentesis, delivery methods, preterm premature rupture of membranes, and breastfeeding.
JieLi,JClinGastroenterol, Volume 51, Number 9, October 2017



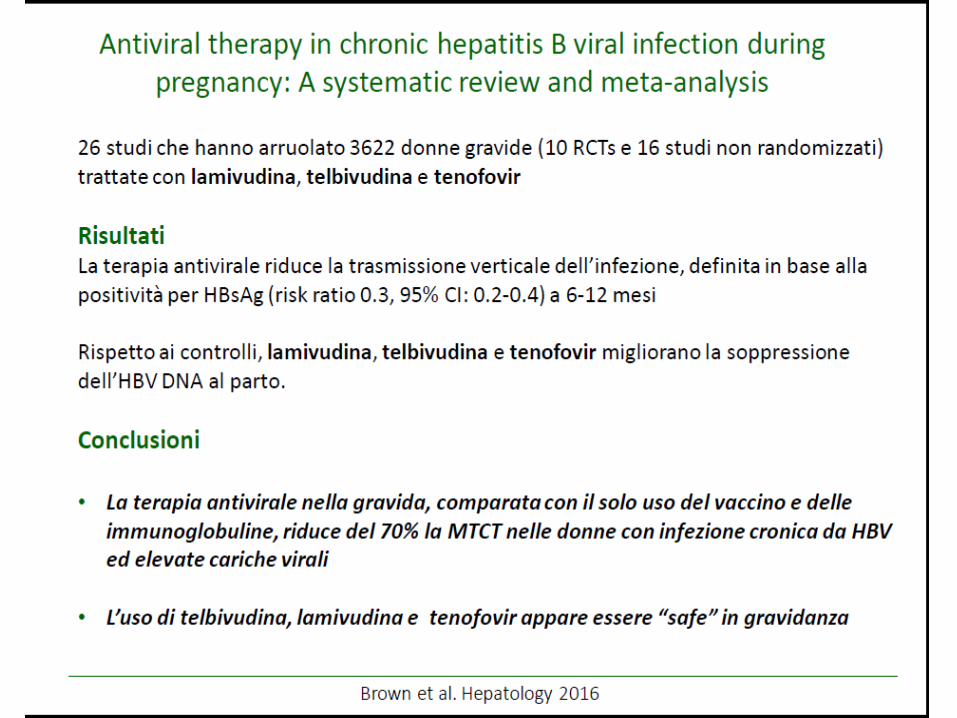
Three therapies are recommended for use in pregnancy: lamivudine (LAM), telbivudine (LdT), and tenofovirdisoproxilfumarate (TDF). Previously,LAM wascategorizedaspregnancycategory C, LdTwascategorizedaspregnancycategoryB, and TDF wascategorizedaspregnancycategory B.A recent meta-analysis that included 26 studies and 3622 pregnant women showed that the use of LdT, LAM, or tenofovir is effective and safe in pregnancy with no significant increased adverse maternal or fetal outcomes.Although therapy with LAM and LdT are also safe and effective in reducing MTCT their high resistance rates with long-term therapy limit their use. TDF is currently one of the therapies of choice for the prevention of MTCT because of its rapid HBV DNA reduction, high tolerability, and lack of risk in viral resistance, and without increase in the rate of birth defects.The rate of birth defects among the infants with exposure to TDF was 2.4%,which was similar to the rate in the general population (2.7%).
JieLi,JClinGastroenterol, Volume 51, Number 9, October 2017

Pan CQ, Duan Z, Dai E, Zhang S, Han G, Wang Y, et al. N Engl J Med 2016;374:2324–2334.
• Mothers should be informed that utilizing a NA to reduce their viremia levels increase the effectiveness to HBIG and vaccination. LAM, TBV or TDF prophylaxis has been used in this setting during the last trimester of pregnancy.
• Of them, TDF is the preferred agent.
• In a randomized study in pregnant HBsAg-positive women with high HBV DNA levels (>200,000 IU/ml), the rate of mother to child HBV transmission at post-partum week 28 was 0% in those treated with TDF compared to 7% in the placebo control group per protocol analysis having a similar safety profile.
• Tenofovir alafenamide (TAF) can potentially be another option in patients with HBV infection during pregnancy, especially given its more favorable bone profile, as maternal TDF use has been suggested to associate with significantly lower neonatal bone mineral content
• Preliminary data from the Antiretroviral Pregnancy Registry have reported no birth defects with exposure to TAF-containing regimens, but this currently only includes 4 patients with TAF exposure.
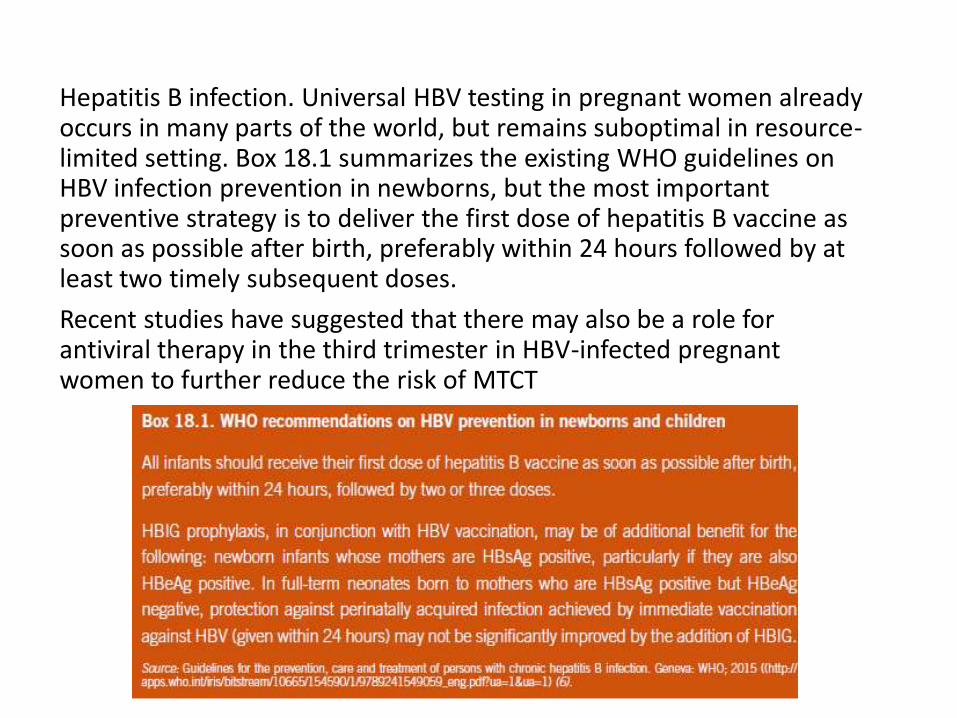
Hepatitis B infection. Universal HBV testing in pregnant women already occurs in many parts of the world, but remains suboptimal in resource-limited setting. Box 18.1 summarizes the existing WHO guidelines on HBV infection prevention in newborns, but the most important preventive strategy is to deliver the first dose of hepatitis B vaccine as soon as possible after birth, preferably within 24 hours followed by at least two timely subsequent doses.
Recent studies have suggested that there may also be a role for antiviral therapy in the third trimester in HBV-infected pregnant women to further reduce the risk of MTCT

• Pregnancy is associated with disturbed cellular immunity.
• In particular, the maternal Th1 immune response may be suppressed during normal pregnancy to avoid rejection of the fetus, resulting in a predominant Th2 phenotype which allows the pregnancy to continue.
• While this Th2-dominant phenotype at the maternal–fetal interface allows fetal survival, the presence of anti-inflammatory cytokines such as interleukin (IL)-4 and IL-10 may predispose to increased risk of infection, including reactivation of latent viruses, such as HBV.



Breastfeeding
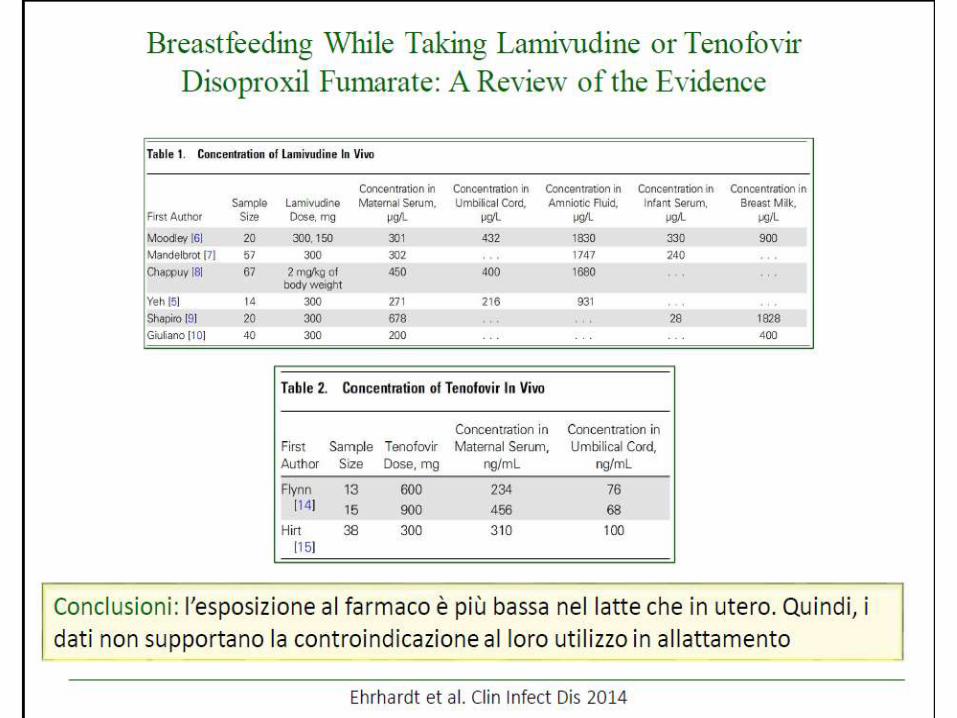
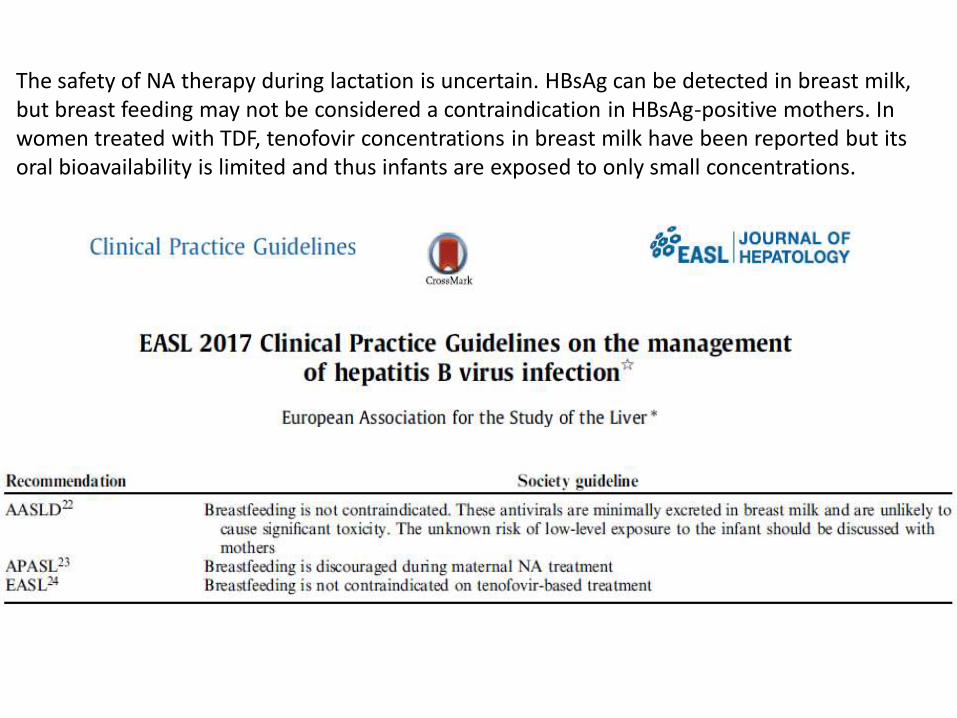
The safety of NA therapy during lactation is uncertain. HBsAg can be detected in breast milk, but breast feeding may not be considered a contraindication in HBsAg-positive mothers. Inwomen treated with TDF, tenofovir concentrations in breast milk have been reported but its oral bioavailability is limited and thus infants are exposed to only small concentrations.
Conclusions• HBV transmission remains a global health issue despite the availability of an
effective and safe vaccine.
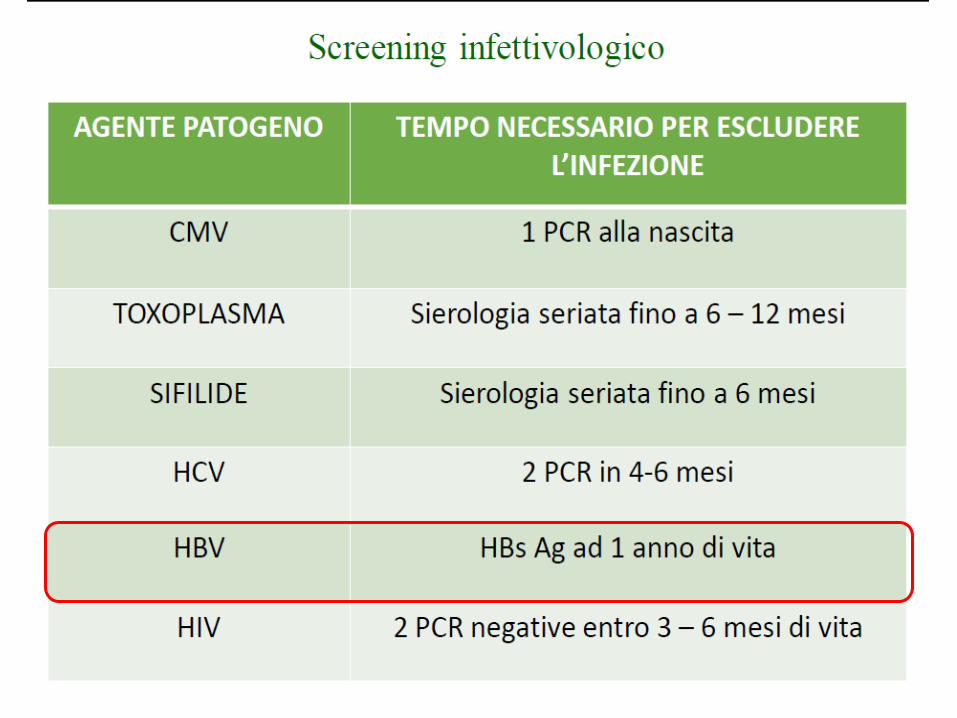
• Screening for HBsAg during first trimester of pregnancy is recommended.
• Current evidence suggest that antiviral therapy during pregnancy beginning at 24 to 28 weeks of gestation can reduce MTCT.
• TDF, LAM, and LdT have been proven to be effective in prevent MTCT without known increased risk of birth defects.
• If the standard passive-active immunoprophylaxis regimen is used; breastfeeding is safe in HBsAg-positive mothers.
• In addition, spontaneous flares during pregnancy and postpartum can occur and on rare occasions can lead to severe hepatic failure. Therefore, it is important to monitor HBV DNA and liver enzymes more frequently in HBV infected women during pregnancy and postpartum for at least 6 months, especially those who are HBeAg-positive or have stopped antiviral therapy recently