
Presentazione di PowerPoint - old.iss.itold.iss.it/binary/urcf/cont/MIRIAM_LICHTNER.pdf ·...
86
Dipartimento di Malattie Infettive e Sanità Pubblica Sapienza Università di Roma Polo Pontino Componente dell’ Italian National Focal Point – Infectious Diseases and Migrant”
-
Upload
trinhtuyen -
Category
Documents
-
view
216 -
download
0
Transcript of Presentazione di PowerPoint - old.iss.itold.iss.it/binary/urcf/cont/MIRIAM_LICHTNER.pdf ·...

Dipartimento di Malattie Infettive e Sanitagrave Pubblica Sapienza Universitagrave di Roma Polo Pontino Componente dellrsquo Italian National Focal Point ndash Infectious Diseases and Migrantrdquo
Ersquo ancora una patologia frequente
Spesso egrave non diagnosticata
Aumenta il rischio di morte
Riduce lrsquoaderenza alle terapie ARV
Riduce la qualitagrave di vita (QoL)
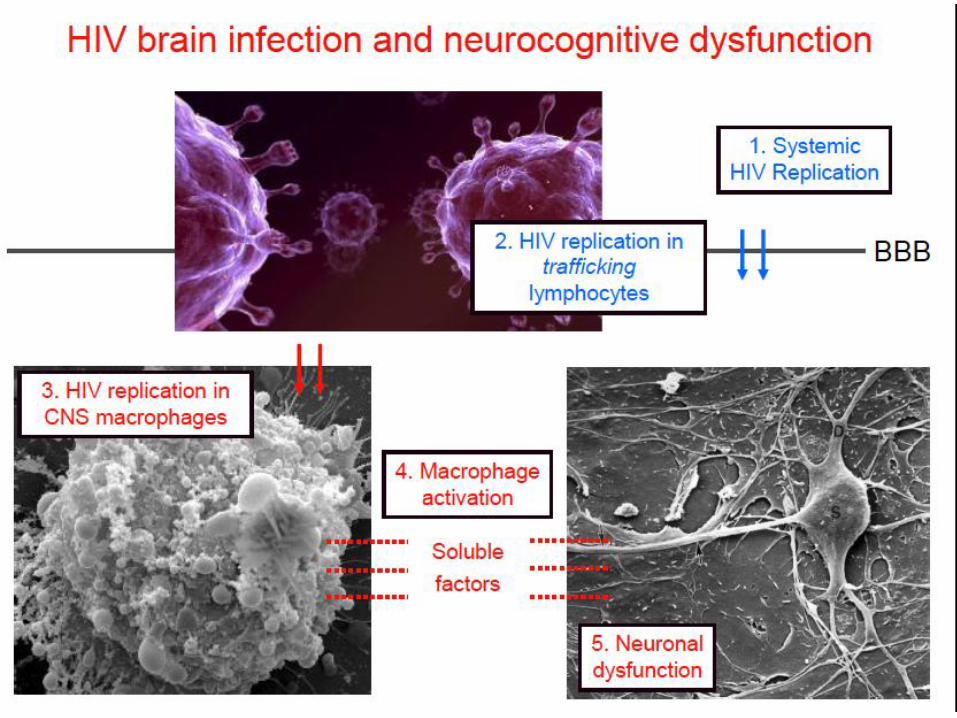
Come lrsquoHIV attacca il sistema nervoso
bull HIV easily crosses the blood-brain barrier
Dave R Pomerantz RJ (2005) HIV neuropathogenesis persistent infection persistent questions Science amp Medicine
bull HIV indirectly destroys cells in the nervous system
Kaul Garden amp Lipton (2001) Pathways to neuronal injury and apoptosis in HIV-associated dementia Nature 410 988-994
Come lrsquoHIV attacca il sistema nervoso
HIV come patologia immunoinfiammatoria
Hierachy of HAND
HIV associated dementia
NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Ersquo ancora una patologia frequente
Spesso egrave non diagnosticata
Aumenta il rischio di morte
Riduce lrsquoaderenza alle terapie ARV
Riduce la qualitagrave di vita (QoL)
Come lrsquoHIV attacca il sistema nervoso
bull HIV easily crosses the blood-brain barrier
Dave R Pomerantz RJ (2005) HIV neuropathogenesis persistent infection persistent questions Science amp Medicine
bull HIV indirectly destroys cells in the nervous system
Kaul Garden amp Lipton (2001) Pathways to neuronal injury and apoptosis in HIV-associated dementia Nature 410 988-994
Come lrsquoHIV attacca il sistema nervoso
HIV come patologia immunoinfiammatoria
Hierachy of HAND
HIV associated dementia
NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Come lrsquoHIV attacca il sistema nervoso
bull HIV easily crosses the blood-brain barrier
Dave R Pomerantz RJ (2005) HIV neuropathogenesis persistent infection persistent questions Science amp Medicine
bull HIV indirectly destroys cells in the nervous system
Kaul Garden amp Lipton (2001) Pathways to neuronal injury and apoptosis in HIV-associated dementia Nature 410 988-994
Come lrsquoHIV attacca il sistema nervoso
HIV come patologia immunoinfiammatoria
Hierachy of HAND
HIV associated dementia
NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

bull HIV indirectly destroys cells in the nervous system
Kaul Garden amp Lipton (2001) Pathways to neuronal injury and apoptosis in HIV-associated dementia Nature 410 988-994
Come lrsquoHIV attacca il sistema nervoso
HIV come patologia immunoinfiammatoria
Hierachy of HAND
HIV associated dementia
NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
HIV come patologia immunoinfiammatoria
Hierachy of HAND
HIV associated dementia
NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
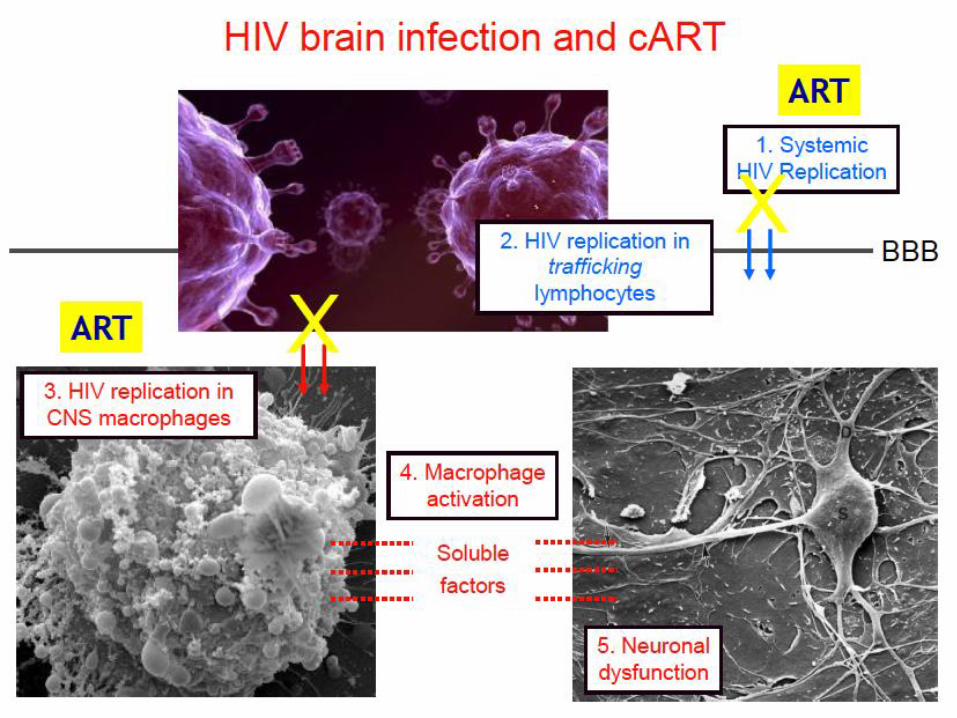
Hierachy of HAND
HIV associated dementia
NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

NIMH Panel Diagnostic Classification of HAND
Acquired impairment in cognitive functioning involving ge 2 ability domains documented by performance of ge 1 standard deviation below the mean for age education-appropriate norms on standardized neuropsychological tests including
Verbal language
Attention working memory
Abstraction executive
Memory (learning recall)
Speed of information processing
Sensory perceptual motor skills
Impairment does not interfere with everyday functioning
Impairment does not meet criteria for delirium or dementia
ANI
No evidence of another preexisting cause for the ANI
Acquired impairment in cognitive functioning as defined for ANI above
At least mild interference in daily functioning including ge 1 of the following
Self-reported reduced mental acuity inefficiency in work homemaking or social functioning
Observation by knowledgeable others of at least mild decline in mental acuity resulting in inefficiency at work homemaking or social functioning
Impairment does not meet criteria for delirium or dementia
MND
No evidence of another preexisting cause for the MND
Marked acquired impairment in cognitive functioning involving ge 2 ability domains (typically multiple domains) especially in learning new information slowed information processing and defective attention concentration Impairment must be ascertained by neuropsychological testing with ge 2 domains 2 standard deviations or greater than demographically corrected means
Marked interference with day-to-day functioning (work home life social activities)
Does not meet criteria for delirium (eg Clouding of consciousness not a prominent feature) or If delirium is present criteria for dementia need to have been met on a previous examination when delirium was not present
HIV-1 associated dementia
No evidence of another preexisting cause for the dementia (eg Other CNS infection CNS neoplasm cerebrovascular disease preexisting neurological disease or severe substance abuse)
Antinori A Arendt G Becker JT Brew BJ Byrd DA Cherner M Clifford DB Cinque P Epstein LG Goodkin K Gisslen M Grant I Heaton RK Joseph J Marder K Marra CM McArthur JC Nunn M Price RW Pulliam L Robertson KR Sacktor N Valcour V Wojna VE Updated research nosology for HIV-associated neurocognitive disorders Neurology 2007691789-99
Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Difficile diagnosi
The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

The old dayshellipfrequency of clinical
features in JHU HIV-D cases (n=300)
13
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
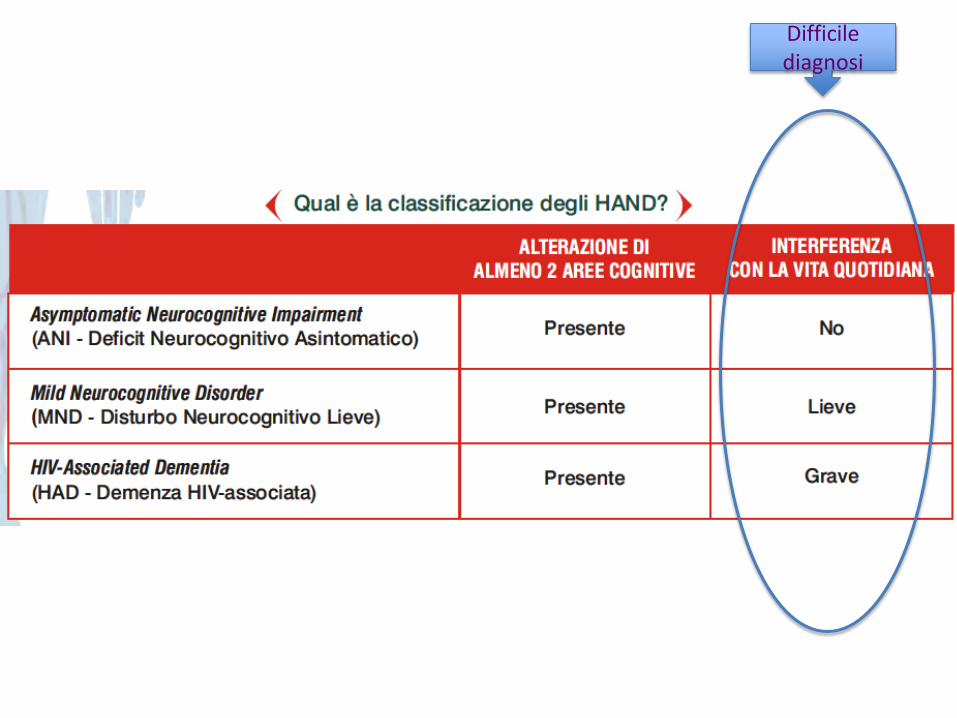
Slide 14
From JC McArthur MBBS MPH at 13th Annual Ryan White HIVAIDS Program Clinical Conference IASndashUSA
5 months mean survival in 1993-1995 to 385 months in 1996-2000
(Dore AIDS 2003)
Before HAART bull lsquoSub-corticalrsquo apathy and severe psychomotor
slowing memory loss Typically progressive bull Multinucleated giant cell encephalitis with neuronal
loss
After HAART bull Mixed lsquocortical and subcorticalrsquo features with milder
phenotype and frequent transitions and reversals bull Synaptodendritic injury with less CNS HIV replication
Todayhellipchanges in HIV dementia with HAART
Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Changing prevalence of HAND
Modified from Heaton R et al HIV-associated neurocognitive disorders (HAND) persist in the era of potent antiretroviral therapy The CHARTER Study and Heaton R J Int Neuropsychol Soc May 19951(3)231-251))
wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

wwwias2011org
Prevalence and risk factors for HIV
associated neurococognitive
disorders (HAND) 1996 to 2010
results from an observational
cohort
Balestra P Tozzi V Zaccarelli M Libertone R Cataldo G Liuzzi G
Menichetti S Giulianelli M Narciso P Lorenzini P Antinori A
Valerio Tozzi
National Institute for Infectious Diseases
L Spallanzani Rome Italy
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
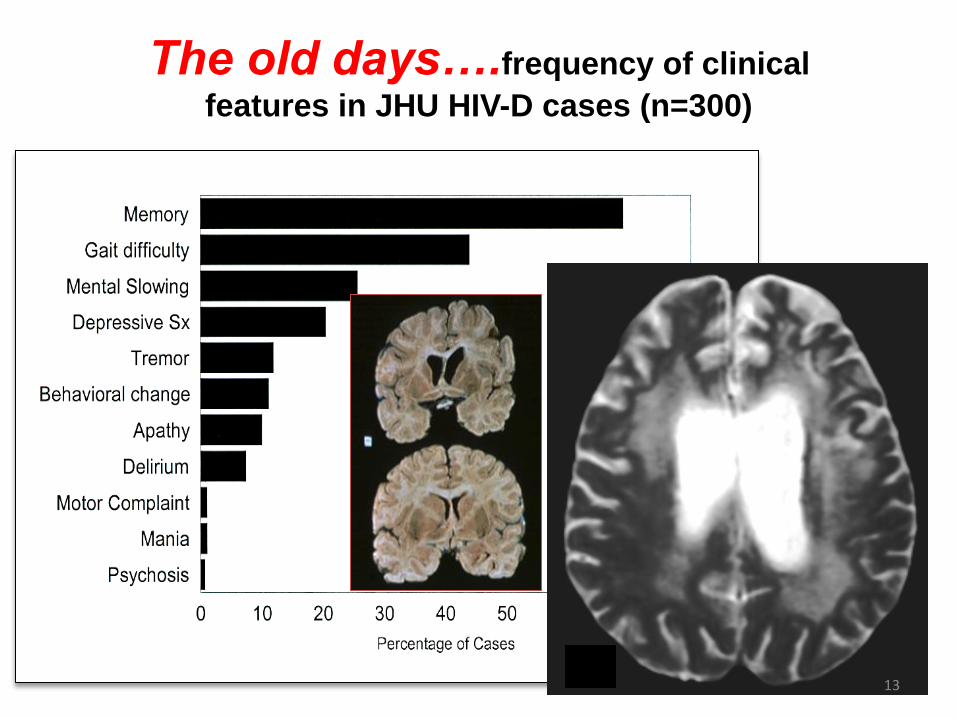
wwwias2011org
Patientrsquos characteristics (I)
N=1375 Total
Male gender 748
Education in years
lt10
10-15
gt15
367
477
156
Education in years median (IQR) 13 (8-13)
Age in years median (IQR) 42 (36-49)
Age in years
lt30
30-39
40-55
gt55
77
362
446
115
Age at 1deg HIV median (IQR) 33 (27-42)
Years of exposure to HIV median (IQR) 6 (16-122)
CDC stage C 345
wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

wwwias2011org
Proportion Impaired (HAND)
HAND (3 yrs incr) OR 092 (95 CI 085-099) p=0031
456 444 394 394 382
wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

wwwias2011org
bull Cognitive impairment persists
bull Small but significant downtrend in HAND
prevalence HAART protective
bull Strongest predictors of HAND
ndash Low HAART exposure HAART protective
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeciciency
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

wwwias2011org
bull Downtrend in prevalence of symptomatic (HADMND)
forms of HAND
evidences for milder forms of HAND
bull Strongest predictors of symptomatic (HADMND) vs
asymtomatic (ANI) forms of HAND
ndash Advanced age time-related cofactors
ndash Low education reduced cognitive reserve
ndash Previous AIDS immunodeficiency
ndash Low current CD4 persistent immunodeficiency
ndash Cardiovascular risk factors chronic inflammation
Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Chi egrave a rischio per HAND
bull Bassi CD4 allrsquoesordio
bull Assenza di terapia ART
bull Comorbiditagrave (alto rischio cardiovascolare)
bull Basso livello di istruzione
bull Scarsa aderenza alle terapie
bull Bassi CD4 allrsquoesordio bull Minor accesso alla
ART bull Comorbiditagrave
maggiori in alcune provenienze (alto rischio CV diabete nefropatia HIV)
bull Piugrave basso livello di istruzione ()
bull Peggiore aderenza alle terapie
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
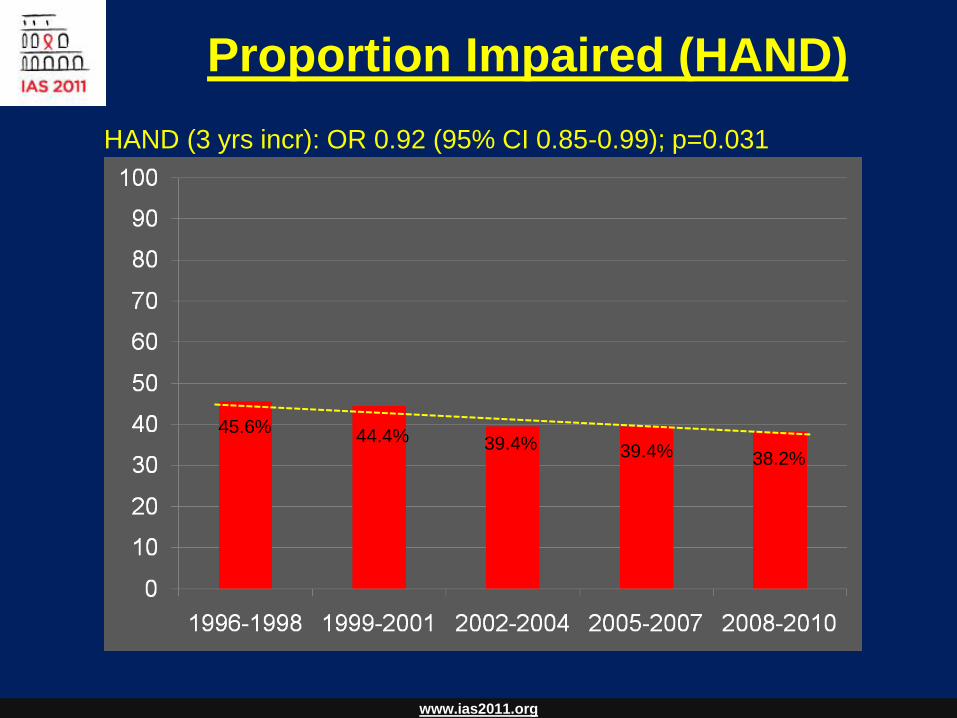
Il caso di Albert
bull M 56 aa di origine africana lavora in un importante ambasciata
africana a Roma vive a Latina (REGOLARE iscriz SSN)
bull Sposato con donna HIV+ di 37 aa 3 figli in abs
bull Diagnosi di infezione da HIV (B3) dal 2005 Eterosessuale
bull Ipertensione arteriosa
bull Insufficienza renale cronica con proteinuria (s nefrosica)
bull In trattamento con Ace-inibitori e sartani
bull Combivir + Kaletra
bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

bull Apparentemente inesistenti
bull Non parla quasi per niente italiano
bull Preferisce parlare solo francese
bull Mancato inserimento nella comunitagrave locale
Barriere culturali
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
bull Giugno 2008 dolore toracico Infarto Miocardico
Trattato con stenting
bull Da allora in terapia con statine e plavix
bull Neuropatia periferica
bull Switch da Combivir + Kaletra a 3TC + AZT + Sustiva
bull CD4= 91mmc
bull VLlt 40 copieml IMMUNOLOGICAL NON RESPONDERS
bull GFR= 18 mlmn Continua progressiva riduzione della funz renale
Dosi adattate a Cl Creat
3TC 150die
AZT 300 x 2
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
bull Inizia dialisi peritoneale in previsione trapianto renale
Peggioramento Neuropatia periferica
Cambiamento radicale della terapia
Intensificazione semplificazione
Raltegravir ATVr T-20 sc
(nessun aggiustamento per funz Renale)
CD4 troppo bassi
NOT SWITCH
bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

bull Dopo 1 mese CD4 201mmc
bull Dopo 3 mesi CD4 289mmc
bull HIV-RNA semprelt20 cpml
Notevole riduzione
della neuropatia
Qualitagrave della vita
Nessun evento CV ad 1 aa
Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Terapie NRTI sparing con RALTEGRAVIR
PRO
CONTRA
bull BASSA barriera genetica
bull Bassa penetrazione SNC
Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Terapie NRTI sparing con RALTEGRAVIR
PRO
bull Meccanismo drsquoazione innovativo
bull Rapida riduzione di HIV-RNA
bull Dati di efficacia a 144 settimane
bull Scarsi effetti collaterali
buon profilo lipidico
nessun effetto su grasso
corporeo
bull Poche interazioni farmacologiche
CONTRA
bull Somministrazione BID
COSTI
bull Alcune interazioni farmacologiche
bull Esperienza non a lungo termine
bull BASSA barriera genetica
bull Penetrazione SNC dibattuta
bull Assenza di coformulazioni
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
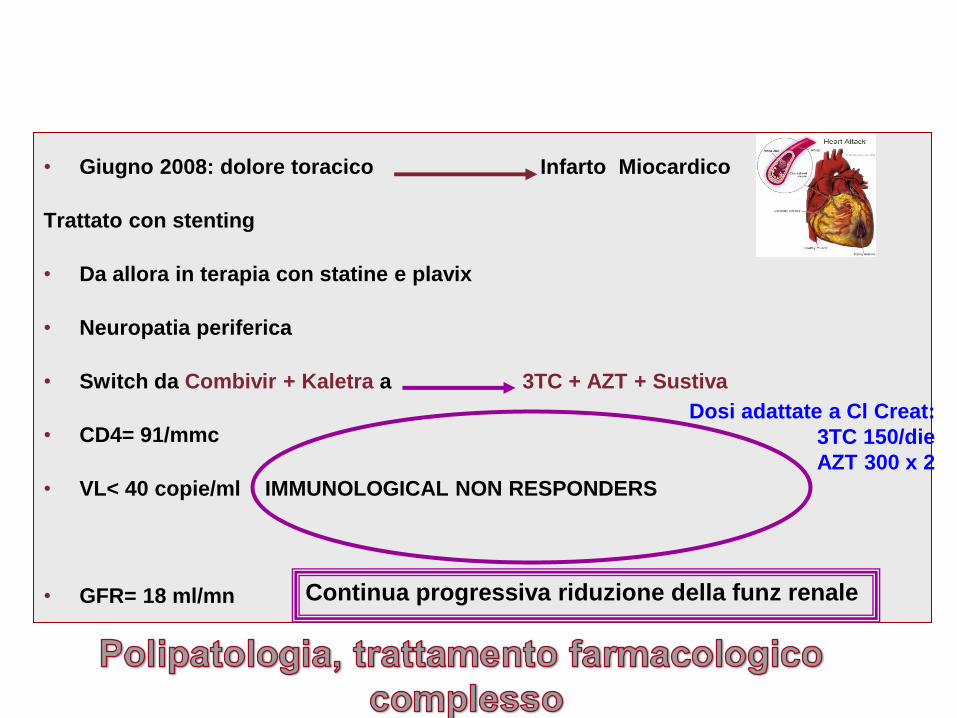
hellipdopo 6 mesi
bull Il paziente ha lasciato il lavoro sta sempre a casa
la moglie riferisce difficoltagrave ad assumere i farmaci e
a rispettare la dieta per IRC
bull Parla pocohellip
bull Ersquo chiuso in se stesso
20032012 Titolo Presentazione Pagina 31
Ogni dodici ore
Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women Schwartz RM Mansoor A Wilson TE Anastos K Everson-Rose SA Golub ET Goparaju L Hessol NA Mack WJ Lazar J
Depression is common in people with cardiovascular diseases (CVD) and those with HIV and is a risk factor for CVD-related mortality However little is known about whether HIV influences the relationship between depression and cardiovascular risk A total of 526 HIV-infected and 132 uninfected women from the Womens Interagency HIV Study were included in an analysis of women who completed twice-yearly study visits over 95 years CVD risk was calculated at baseline and approximately 95 years later using the Framingham Risk Score (FRS) Chronic depressive symptoms were defined as Center for Epidemiologic Studies Depression Scale scores of 16 or greater at ge75 of study visits Over the follow-up period 228 of HIV-infected women and 159 of HIV-uninfected women had chronic depressive symptoms (p=008) Baseline FRS was similar between HIV-infected and uninfected women (M=-570plusmnSE=030 vs M=-690plusmn SE=060 p=007) as was follow-up FRS (M=082plusmnSE=030 vs M=-044plusmn SE=073 p=011) Among HIV-infected and HIV-uninfected women together follow-up FRS was higher among women with chronic depressive symptoms as compared to those without (M=13plusmn SE=06 vs M=-03plusmn SE=040 plt001) after adjusting for baseline FRS and other covariates HIV status did not modify the relationship between chronic depressive symptoms and FRS Chronic depressive symptoms accelerated CVD risk scores to a similar extent in both HIV-infected and-uninfected women This implies that the diagnosis and treatment of depression may be an important consideration in CV risk reduction in the setting of HIV-infection The determination of factors that mediate the depressionCVD relationship merits further study
AIDS Care 2011 Sep 9
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
Racial and Ethnic Disparities in Depression Care in Community-Dwelling Elderly in the United States Ayse Akincigil et al
American Journal of Public Health February 2012 Vol 102 No 2 pp 319-328
Objectives We investigated racialethnic disparities in the diagnosis and treatment of depression among community-dwelling elderly Methods We performed a secondary analysis of Medicare Current Beneficiary Survey data (n = 33 708) for 2001 through 2005 We estimated logistic regression models to assess the association of raceethnicity with the probability of being diagnosed and treated for depression with either antidepressant medication or psychotherapy Results Depression diagnosis rates were 64 for non-Hispanic Whites 42 for African Americans 72 for Hispanics and 38 for others After we adjusted for a range of covariates including a 2-item depression screener we found that African Americans were significantly less likely to receive a depression diagnosis from a health care provider (adjusted odds ratio AOR+ = 053 95 confidence interval CI+ = 041 069) than were non-Hispanic Whites those diagnosed were less likely to be treated for depression (AOR = 045 95 CI = 030 066) Conclusions Among elderly Medicare beneficiaries significant racialethnic differences exist in the diagnosis and treatment of depression Vigorous clinical and public health initiatives are needed to address this persisting disparity in care
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
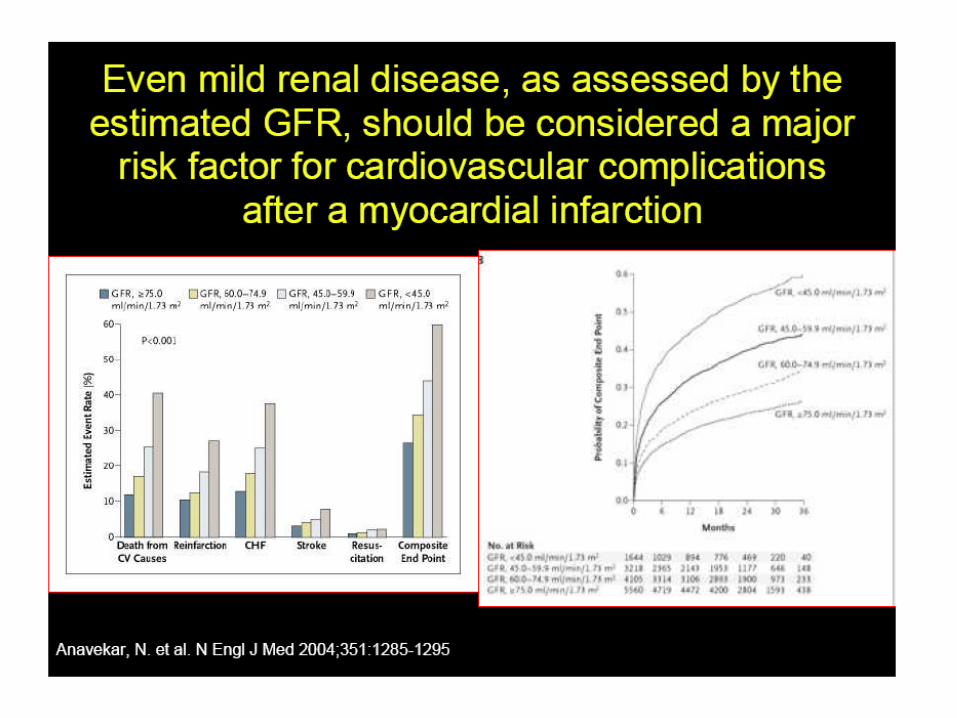
c
c
c
torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

torniamo ad Albert
Esami strumentali pre-trapianto
EGDS ldquo antropatia cronica attiva con polipo duodenalerdquo
Ecodoppler vasi epiaortici ldquo stenosi bilaterale
emodinamicamente significativerdquo
intervento di endoarteriectomia bilaterale
Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Blip viremici
A dicembre 2009 Genotipo
Proteasi L10M K20I M36IL 89M I93IL
Trascrittasi Inversa Nessuna
GP -120 K10R I12V H13RI14F R18Q
A18VT22AD29NH34Y
Test integrasi non amplificato
Note ldquonon segni di resistena a farmaci in uso correntehellipil
passaggio da T-20 a maraviroc egrave fattibile sulla base dei
risultati sul tropismohelliprdquo
Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Semplificazione della terapia
al fine di migliorare lrsquoaderenza
Test Trofile CCR5
Raltegravir Atavanavirrit Maraviroc
1 cpX2 2 cp +1 1 cp X2
- Linfociti T CD4+ 282mmc
- HIV-RNA 1149 Cml
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
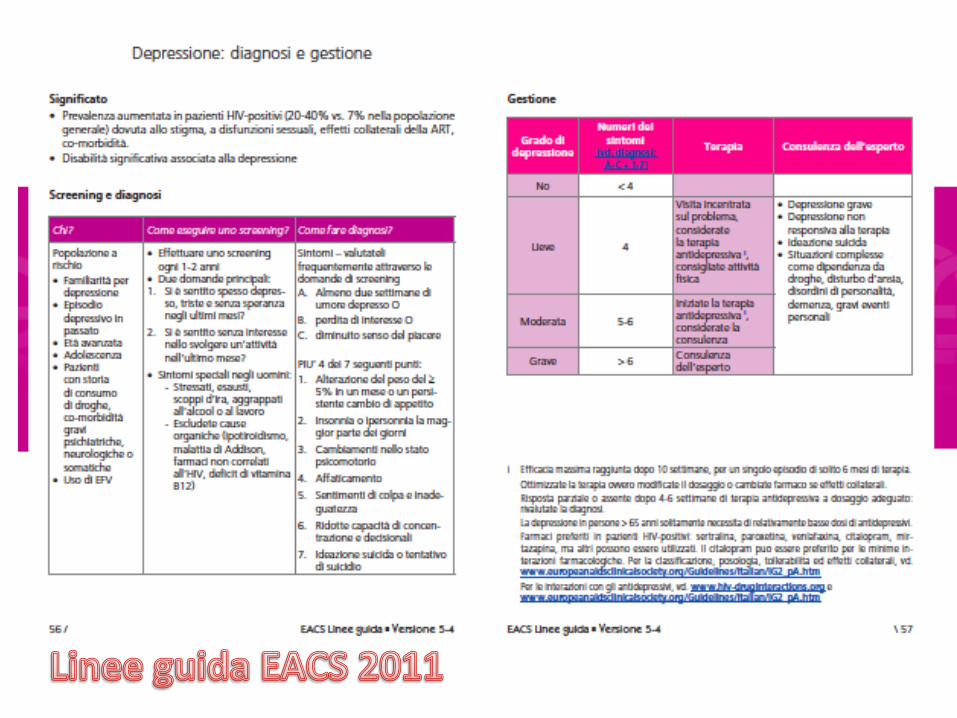
REGIMI CON MONOSOMMINISTRAZIONE E BASSO NUMERO DI PILLOLE SONO ASSOCIATI A MINORE NON-ADERENZA
78 92
286
31 94
247
163
408
93
208
252 261
465
134 163
0
5
10
15
20
25
30
35
40
45
50
Sub
ject
s re
po
rtin
g n
on
-ad
he
ren
ce (
)
QD lp QD hp BID
Drug holiday Non-adherence at refill
Timing deviation
Non-adherence last week
Adherence lt95
P=0006 P=0006
P=004 P=005
P=016
Ammassari Personal Data INMI 2008
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
bull La valutazione del medico relativamente al rispetto varia molto tra i pazienti ed egrave principalmente associata alla familiaritagrave piuttosto che a caratteristiche socio-demografiche
bull I medici che agiscono con piugrave rispetto nei confronti dei loro pazienti danno piugrave informazioni e esprimono piugrave slancio positivo nelle visite
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
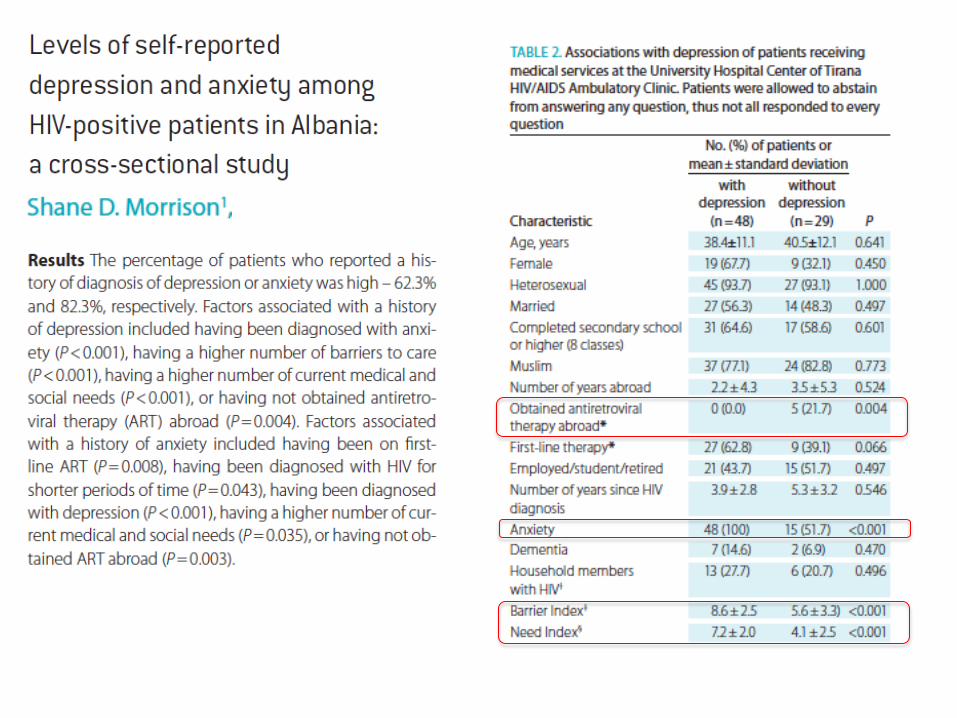
Pazienti di medici che erano piugrave motivati a conoscere altre culture nellrsquoambito della loro pratica erano piugrave bull soddisfatti con la visita medica (OR=21 95 CI=10ndash44) bull percepivano il loro medico come piugrave ldquofacilitanteldquo (β=04 p=002) bull riportavano di cercare e condividere piugrave informazione (β=02 p=003)
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
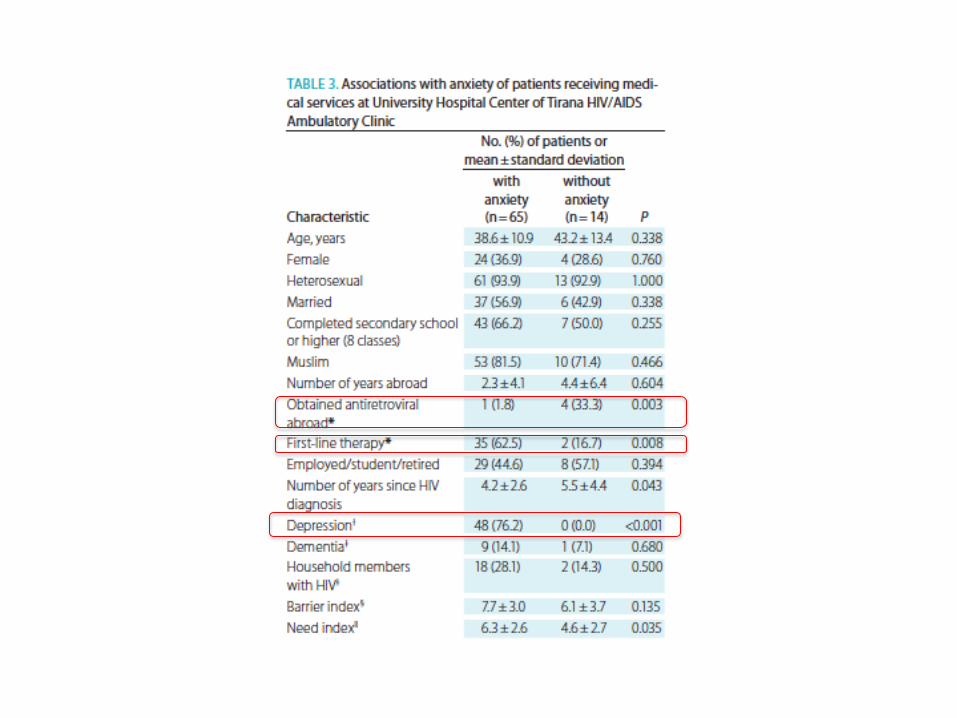
bull rispetto nei confronti del paziente
bull La capacitagrave di accettare gli aspetti culturali o le
scelte esistenziali individuali diverse
Per aumentare lrsquoaderenza e QUINDI lrsquoefficacia delle CURE Ersquo IMPORTANTE che il medico abbia
bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

bull Peggioramento clinico progressivo fino ad una sindrome catatonica
ndash Il paziente non parla
ndash Il paziente non si muove si oppone al movimento passivo degli arti
ndash Il paziente egrave vigile risponde agli stimoli dolorosi
47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

47
Catatonia
a state of apparent unresponsiveness to
external stimuli in a person who is apparently
awake
difficult to differentiate from diffuse
encephalopathy and nonconvulsive status
epilepticus
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
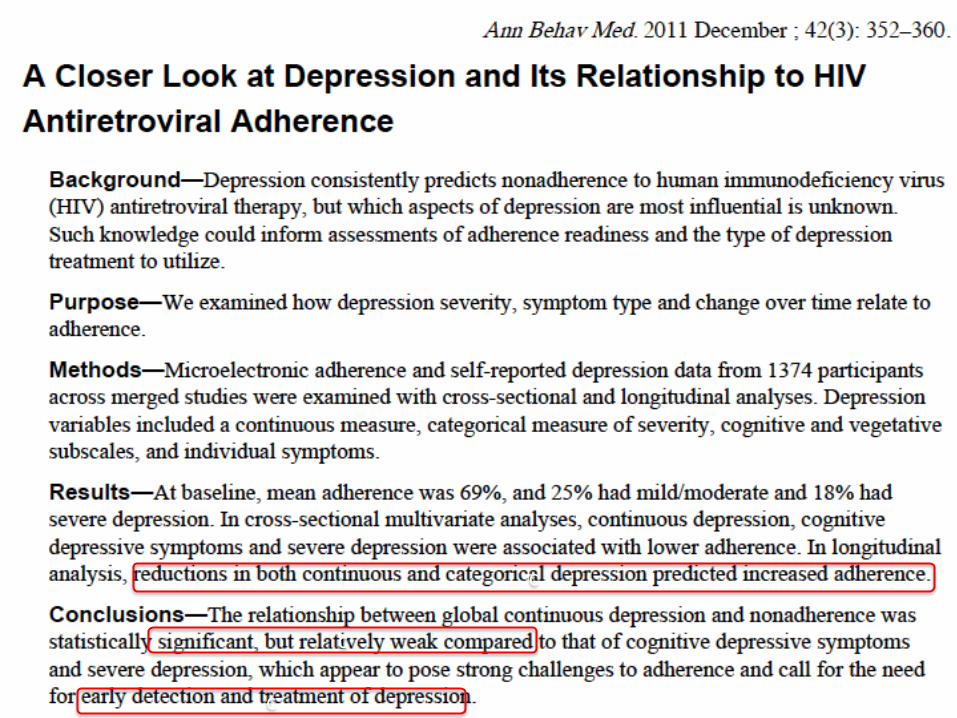
48
Catatonia
occurrence in children adolescents and adults
association with a heterogeneous group of
comorbid conditions
symptoms and signs of impairment of the
expression of voluntary thoughts and
movements
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
51
Treatable Causes of Catatonia
Neuroleptic malignant syndrome
Encephalitis
Nonconvulsive status epilepticus
Acute psychosis
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
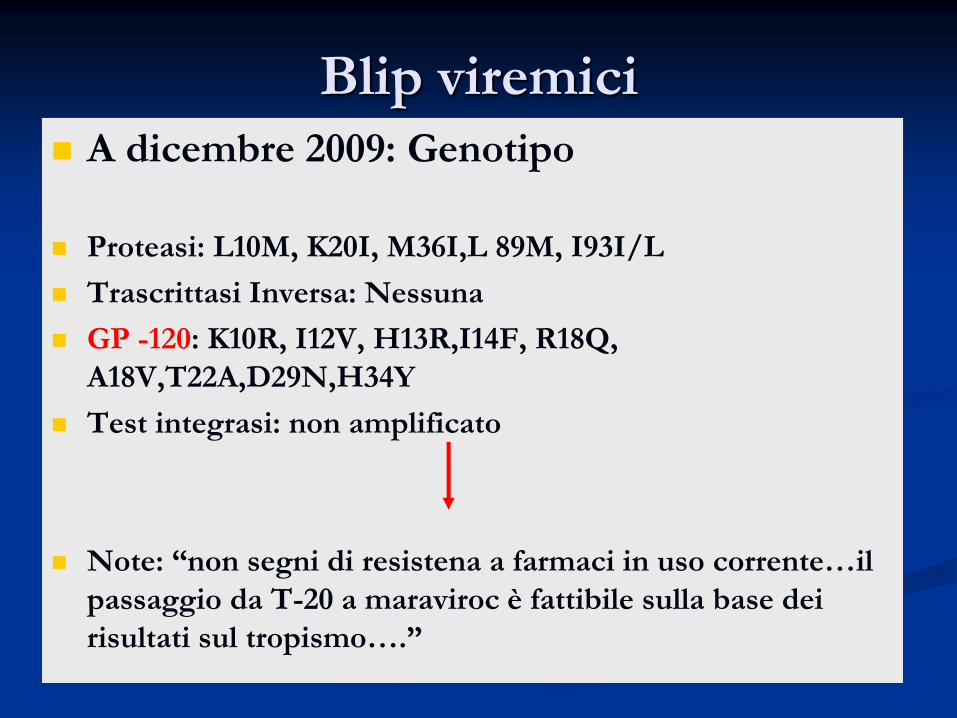
bull Esami ematici generali stabili
bull Peggioramento dellrsquoIRC
bull HIV-RNA plasmatico lt20
bull Linfociti CD4+=110 cellmmc
bull RMN encefalo negativa per masse encefalopatia multi infartuale diffusa
bull Valutazione NP sindrome catatonica
Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Esame del liquor
bull Liquor limpido
bull Pressione liquorale aumentata
bull Cellule 30 cellmmc
bull Glu 67 mgdl
bull Proteine 120 mgdl
bull CMV JC VZV HSV enterovirus neg
c
c
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
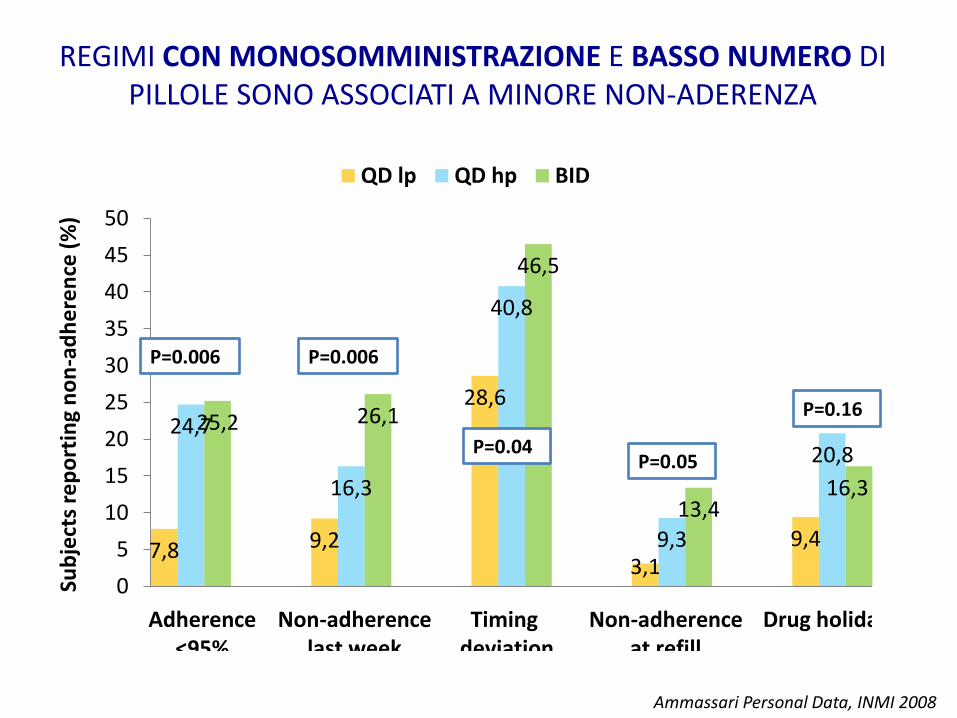
Despite successful suppression of plasma viremia with HAART HIV may replicate in CSF with development of CSF HIV resistance resulting in acute or subacute neurological manifestations
Nonstante la soppressione virologica plasmatica in corso di HAART lrsquoHIV puograve replicare nel CSF con lo sviluppo di resistenze Questa situazione puograve portare a manifestazioni neurologiche acute o subacute
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
FDDNP PET imaging of the HIV brain the first in vivo evidence of amyloid
Achim CL personal observation 2007
bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

bull Esegue dialisi standard
bull Inizia Prezista 400 mg 2 cp100mg 1 cp+ Emtriva (fTC)200 1 cp retrovir 300 mg 1 cp die
bull Supporto psicologico francofono
bull Terapia antidepressiva
torniamo ad Albert
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
Letendre et al 17degCROI 2010
SCORE Prezista 3 Emtriva 3 Retrovir 4 TOT 10
SCORE Enfuvirtide 1 Reyataz 2 Raltegravir 3 TOT 6
Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Esame del liquor DOPO 1 MESE
bull Liquor limpido
bull Pressione liquorale normale
bull Cellule 4 cellmmc
bull Glu 67 mgdl
bull Proteine 90 mgdl
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip
DOPO 1 MESE HIV-RNA sangue 3720 Cml CD4 246 (11) cpml
DOPO 3 MESI HIV-RNA sangue lt20 Cml CD4 288( 20)
DOPO 12 MESI HIV-RNA sangue lt20 Cml CD4 248( 25) Buona cenestesi
bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

bull Il paziente ha una buona cenestesi
bull Ha ripreso regolarmente la dialisi peritoneale notturna
bull Assume la terapia ARV e medica rispetta la dieta
MAhelliphellip
si sta battendo per far rimanere i suoi figli in Italia
ha perso il suo lavoro in ambasciata in attesa di pensione
egrave in attesa di TRAPIANTO renale
Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Come si poteva prevenire
DIAGNOSI precoce
Dei
Disturbi neurocognitivi
Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Take messages
bull I disturbi neurocognitivi sono frequenti nei pazienti HIV
anche in epoca post-ART
bull Alcuni fattori di rischio per HAND sono gli stessi che si
ritrovano con maggior frequenza nella popolazione migrante
HIV
bull Difficile diagnosi
bull Difficile gestione terapetica multidisciplinare
bull Importanza degli aspetti psicosociali del RAPPORTO medico-
paziente MA
bull escludere SEMPRE CAUSE organiche in HIV
Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip

Il caso di un giovane migrante italiano morto a Parigi
Modigliani malato dai 14 anni malato di TB
polmonare
muore a Parigi a 35 anni di MENINGITE
TUBERCOLARE
scambiata inizialmente
per un delirio alcolico-farmacologicohelliphellip


















