Presentation1, radiological imaging of trigeminal schwanoma.
Upload
abd-ellah-nazeerCategory
view
303download
7description

Radiological imaging of parkinsonism.
Dr/ ABD ALLAH NAZEER. MD.

Parkinson's disease described by James Parkinson in 1817. Parkinson’s disease is a chronic neurodegenerative movement disorder affecting voluntary and emotional movements and most commonly seen in the elderly, but is also found in the young and inexorably progresses leading to significant disability.Average age of onset is 62.5 years.Men and women affected equally.Pathogenesis:Four theories.Oxidative damage, Mitochondrial dysfunction, enhanced oxidative stress, proteosomal dysfunction causes cell death.Environmental toxins, MPTP-Methyl-phenyl tetrahydropyridine, Mutation in the gene located on chromosome 4.Genetic predisposition, Mutation in the gene located on chromosome 4.Accelerated aging.


Classification and Etiology.Idiopathic Parkinson’s diseaseParkinson-like syndromesDrug induced parkinsonismHypoxiaTumorTraumaVascular:MultiinfarctToxin:Mn, CO, MPTP and cyanidePost-encephalitic parkinsonism (von Economo’s encephalitis)Normal pressure hydrocephalusWilson’s disease, Hutington’s disease

Medications that can cause parkinsonian symptoms, but not PD itself, include the following:
Metoclopramide Domperidone Reserpine-containing antihypertensives Neuroleptics
Some evidence also indicates that certain environmental factors (including smoking and coffee drinking) may actually have protective associations.

Clinical features of Idiopathic Parkinson’s disease.
Major featuresResting tremor in hands, arms, legs, jaw, and Face. BradykinesiaRigidity- cogwheel or lead-pipe
Minor featuresBradyphreniaSpeech abnormalitiesDepressionDysautonomiaDystoniaConstipationHallucinationsDysphagia

Parkinson’s disease Symptomatology.

Tremor dominant
Tremor: Rest Fixed frequency 3-6 Hz Not a feature of old age Pill-rolling Usually starts in one limb, and then to other limbs Rarely starts in lower limbs Intermittent for many years They usually disappear briefly during
movement and do not occur during sleep.
• Tremors can also eventually occur in the head, lips, tongue, and feet. In younger patients tremor is usually predominant and often suggests a less aggressive form of the disease.

RigidityStriatal hand: Ulnar deviation, MCP flexion, IP extensionStriatal toe: Big toe dorsiflexionSitting en bloc: Collapses into a chair on attempting to sit down
PostureKyphosisFlexed elbows, knees and hipsHands held in front of bodyTrunk bent forwardHead bowed

BradykinesiaSlowness of motion (bradykinesia) is one of the classic symptoms of Parkinson's disease. Hypomimia- “masked facies”, expressionless face, blinkingSpeech abnormalities-Hypophonia: soft voiceAprosody of speech: monotonous and lack of inflectionTachyphemia: do not separate syllables together, running words togetherPatients may eventually develop a stooped posture and a slow, shuffling walk. The gait can be erratic and unsteady.

Motor fluctuationsFreezing phenomenon- Sudden, transient inability to perform active movements, lasting no more than a few seconds:Start hesitationTurn hesitationTarget hesitationPalilalia (speaking)Apraxia of eyelid openingWritingKinesia paradoxica-Despite severe rigidity and bradykinesia, they may rise suddenly and move normally.

Festinating gaitDrooling of salivaDysphagiaConstipationDementiaDepressionOrthostatic hypotension
Low resting blood pressure HTN NormotensiveSweating abnormalities-excessive perspirationBlepharospasm/ keratitis.

Investigations:The diagnosis is made clinically , as there is no diagnostic test for Parkinson's disease.Imaging (CT or MRI) of the brain needed if there are any features suggestive of pyramidal, cerebellar or autonomic involvement or the diagnosis is otherwise in dought (e.g to exclude stroke).
Routine brain imaging is unnecessary in patients with typical Parkinson’s disease.Dopamine transporter (DAT) imaging can help to differentiate patients with Parkinson’s disease from healthy individuals and patients with essential tremor or drug induced parkinsonismStructural MRI may be performed to rule out alternative diagnoses (including other neurodegenerative syndromes and structural or vascular lesions).



T1-weighted MR images show bilateral and symmetrical hyperintensities in the substantia nigra and cerebral peduncle (A), subthalamic region and hemispheric white matter (B), and the globus pallidus and putamen (C) in reversal parkinsonism patient following embolization of intra-hepatic venous shunt.

19-year-old man with secondary parkinsonism (carbon monoxide intoxication) 3 years after onset, with hyperintense lesion at the globus pallidus and atrophy of the substantia nigra.

Parkinsonism due to predominant involvement of substantia nigra in Japanese encephalitis

A 64-Year-Old Woman With Bradykinesia and Rigidity in epilepsy.

Reversible Acute Parkinsonism and Bilateral Basal Ganglia Lesions in a Diabetic Uremic Patient.

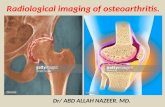
Differential diagnosis of parkinsonism using brain 18F-FP-CIT PET. Brain PET/CT images of 18F-FP-CIT uptake at level of striatum demonstrate different DAT density in different conditions. DAT density is decreased in PD patient (B), whereas DAT density is normal in healthy subject (A) and in patients with drug-induced parkinsonism (C) and essential tremor (D).

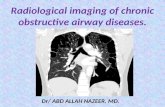
Color-coded diffusion-weighted MRI and (B) striatal 123I-2β-carbomethoxy-3β-(4-iodophenyl)-N-(3-iodophenyl) tropane uptake for a healthy individual, a patient with Parkinson’s disease (PD), and a patient with the atypical parkinsonian syndrome multiple system atrophy (MSA). The apparent diffusion coefficient (A) is normal in the striatum in PD but it is raised in MSA (arrows) because of the neuronal loss that targets the putamen. Dopamine transporter binding (B) is bilaterally reduced in the striata in both PD and MSA. In PD, the caudate is relatively spared compared with the putamen.

White matter lesions in Parkinson disease

Fluid-attenuated inversion recovery magnetic resonance imaging sequence of the brain in a patient with West Nile virus encephalitis with associated parkinsonism and tremor, displaying signal abnormality in the substantia nigra (short arrow), the mesial temporal lobe (long arrow) and right posterior thalamus (thick arrow).



Dual-Tracer Dopamine Transporter and Perfusion SPECT in Differential Diagnosis of Parkinsonism Using Template-Based Discriminant Analysis

Abnormal signal within the Substantia Nigra in Parkinson Disease.

Abnormal signal within the Substantia Nigra in Parkinson Disease.

Parkinson Disease with abnormal signal within the pars impacta at the substantia nigra.

Parkinson disease. Hypointensity involves entire putamina diffusely.

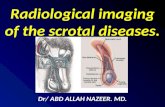
Left: an axial section through an averaged multispectral image at the level of the midbrain showing the substantia nigra (SN) in a healthy control participant. Right: magnified view of the SN in a healthy woman (top) and a woman with Parkinson disease (PD) (bottom); signal loss in the SN is striking in the PD brain (green arrow).

Magnetic Resonance Imaging (MRI) in Parkinson s Disease. ′

Neurocysticercosis presenting as Parkinsonism.

Thank You.