Presentation1 final
70
1 Sodium Glucose Co-Transporter 2 Inhibitors. Presenter: Dr.Anupam Das, 3 rd yr. P.G., Dept of Pharmacology. Guide: Dr.K.S.N. Murthy,Prof. and HOD.
-
Upload
anupam-das -
Category
Health & Medicine
-
view
37 -
download
2
Transcript of Presentation1 final

1
Sodium Glucose Co-Transporter 2 Inhibitors.Presenter: Dr.Anupam Das, 3rd yr. P.G., Dept of Pharmacology.Guide: Dr.K.S.N. Murthy,Prof. and HOD.

INTRODUCTION
• Given the high importance of diabetes, the glucose homeostasis in human body has been deeply analyzed and investigated.
• The role of kidney in this procedure was until recently underestimated.
• Involvement of kidney in glucose regulation : glucose release from renal cortex via gluconeogenesis. glucose uptake and glycolysis from renal medulla for
satisfying kidney energy needs. glucose reabsorption from proximal convoluted tubule.

Renal Gluconeogenesis• Glucose, after moving into cells, is phosphorylated into
glucose-6-phosphate by enzymes like glucokinase or hexokinase.
• In this form, cells can trap glucose because cell membranes are impermeable to glucose-6-phosphate.
• Only cells containing the enzyme glucose-6-phosphatase, which hydrolyzes glucose-6-phosphate to glucose, are able to release glucose into the circulation.
• Glucose-6-phosphatase is present in the liver, the renal cortex and the intestinal epithelium giving the above tissues the ability to release glucose.
• The renal medulla lacks glucose-6-phosphatase, and does not have the capacity to release glucose into the circulation.
• On the other hand, the renal cortex holds gluconeogenic enzymes, synthesize glucose-6-phosphate from precursors, and is able to release glucose into the blood stream via glucose-6-phosphatase.

The Kidney Handles Glucose By Two Key Mechanisms

Hormone Regulation of Renal Gluconeogenesis
• Increased insulin levels suppress renal gluconeogenesis and enhance renal medulla glucose uptake.
• Glucagon has no effect on renal glucose release and uptake.
• Catecholamines prolong renal glucose release.
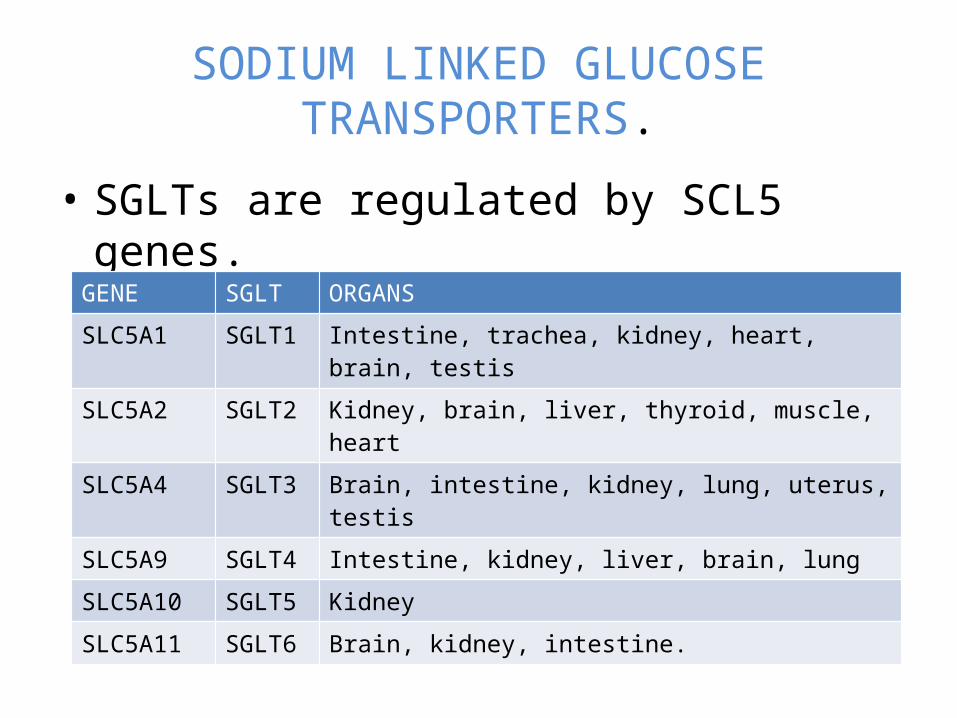
SODIUM LINKED GLUCOSE TRANSPORTERS.
• SGLTs are regulated by SCL5 genes.
GENE SGLT ORGANSSLC5A1 SGLT1 Intestine, trachea, kidney, heart, brain, testisSLC5A2 SGLT2 Kidney, brain, liver, thyroid, muscle, heartSLC5A4 SGLT3 Brain, intestine, kidney, lung, uterus, testisSLC5A9 SGLT4 Intestine, kidney, liver, brain, lungSLC5A10 SGLT5 KidneySLC5A11 SGLT6 Brain, kidney, intestine.
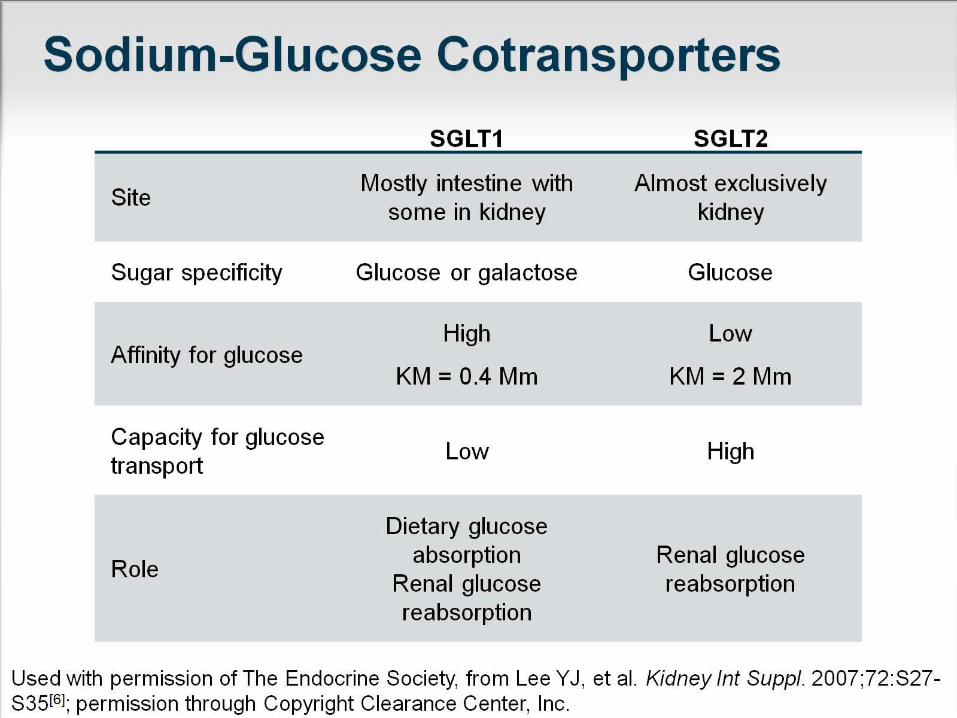
Sodium-Glucose Cotransporters
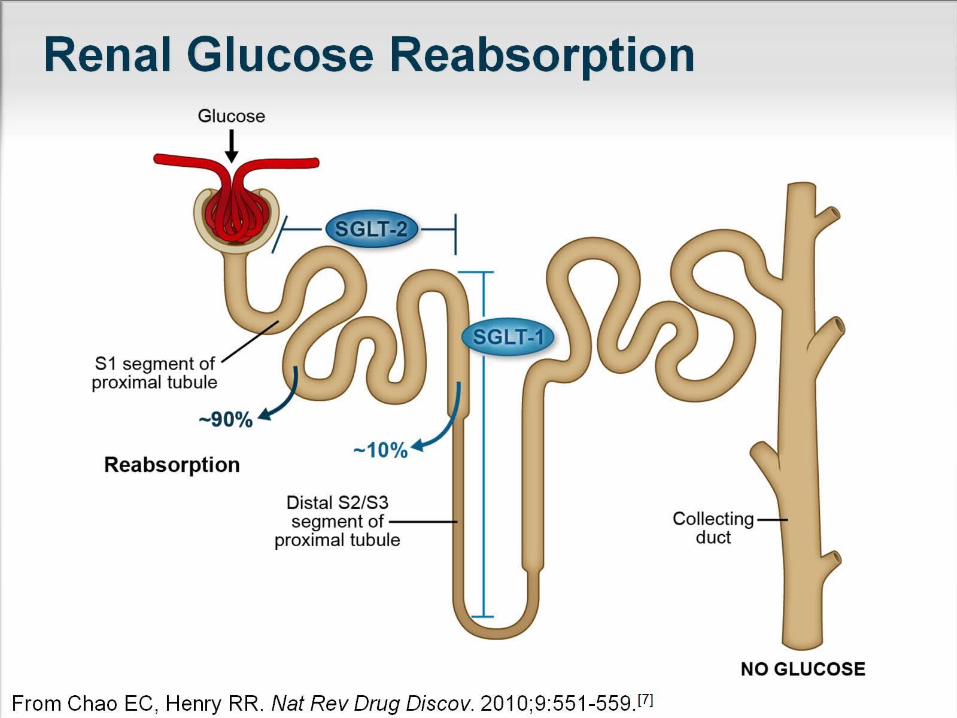
Renal Glucose Reabsorption

SGLT KINETICS
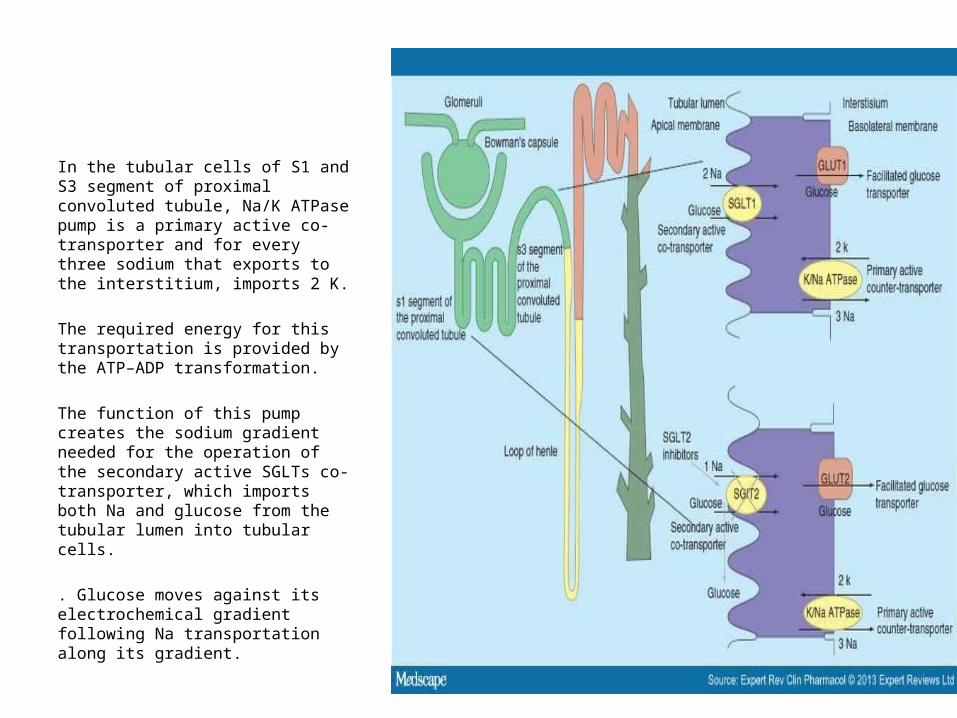
In the tubular cells of S1 and S3 segment of proximal convoluted tubule, Na/K ATPase pump is a primary active co-transporter and for every three sodium that exports to the interstitium, imports 2 K.
The required energy for this transportation is provided by the ATP–ADP transformation.
The function of this pump creates the sodium gradient needed for the operation of the secondary active SGLTs co-transporter, which imports both Na and glucose from the tubular lumen into tubular cells.
. Glucose moves against its electrochemical gradient following Na transportation along its gradient.

Intracellular glucose moves to the interstitium through GLUTs passive diffusion transporters, which are located at the basolateral membrane of the tubular cells.
Contrary to SGLT1, which is found at the S3 segment and has a stoichiometry of 2Na to 1 glucose, SGLT2 is situated at the S1 segment and has one to one stoichiometry.
Both transporters are located on the brush border of tubular cells.
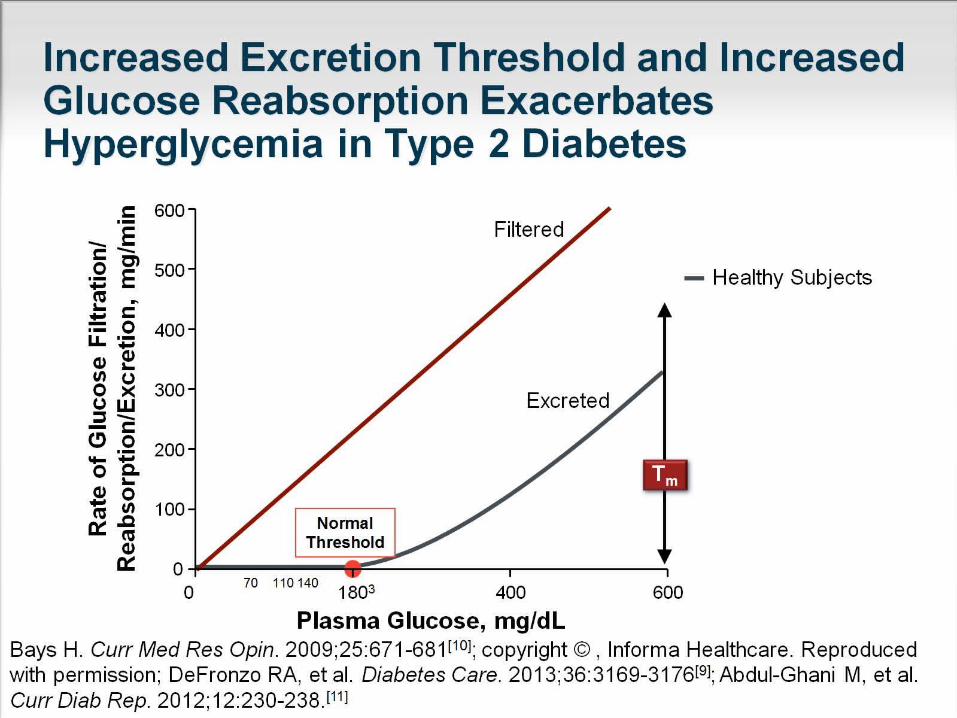
Increased Excretion Threshold and Increased Glucose Reabsorption Exacerbates Hyperglycemia in Type 2 Diabetes

Renal threshold in T2DM

Increased Excretion Threshold and Increased Glucose Reabsorption Exacerbates Hyperglycemia in Type 2 Diabetes
(cont)
• The increases in tubular reabsorption in individuals with T2DM lead to an increase in glucose flux into the blood, resulting in an exacerbation of hyperglycemia.
• Mean RTG is approximately 40 mg/dl higher in patients with T2DM than the commonly reported values of 180 to 200 mg/dL in healthy individuals.

Altered Renal Glucose Control in Diabetes

Renal SGLT2 Levels Are Increased in Type 2 Diabetes

Familial Renal Glucosuria
• Autosomal recessive deficiency of SGLT-2
• Characterized by persistent urinary glucose excretion, with normal plasma glucose concentration
• Urinary glucose excretion varies from a few grams to >100 grams per day
.

• No evidence of renal glomerular or tubular dysfunction
• Usually asymptomatic
• Hypoglycemia and hypovolemia are rarely, if ever, observed
• Normal lifespan
• The large majority of patients have no clinical manifestations– Both renal histology and renal function are normal– The incidence of diabetes, chronic renal failure, and
urinary tract infection are not increased
Familial Renal Glucosuria

Mechanism of Action
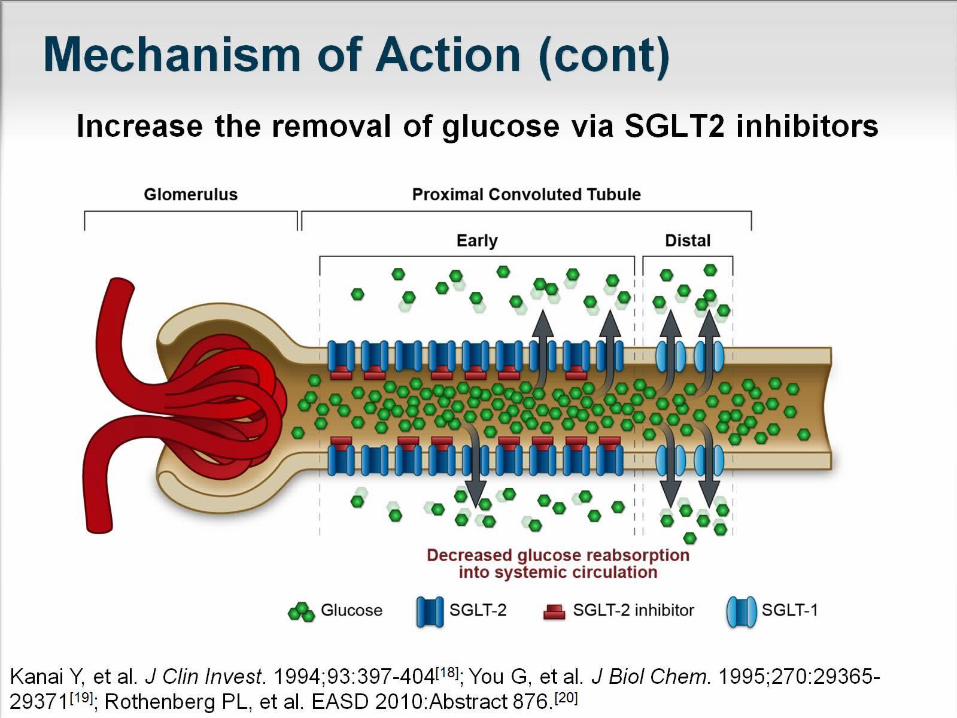
Mechanism of Action (cont)

Mechanism of Action (cont)


Phlorizin: The “Prototype” SGLT Inhibitor
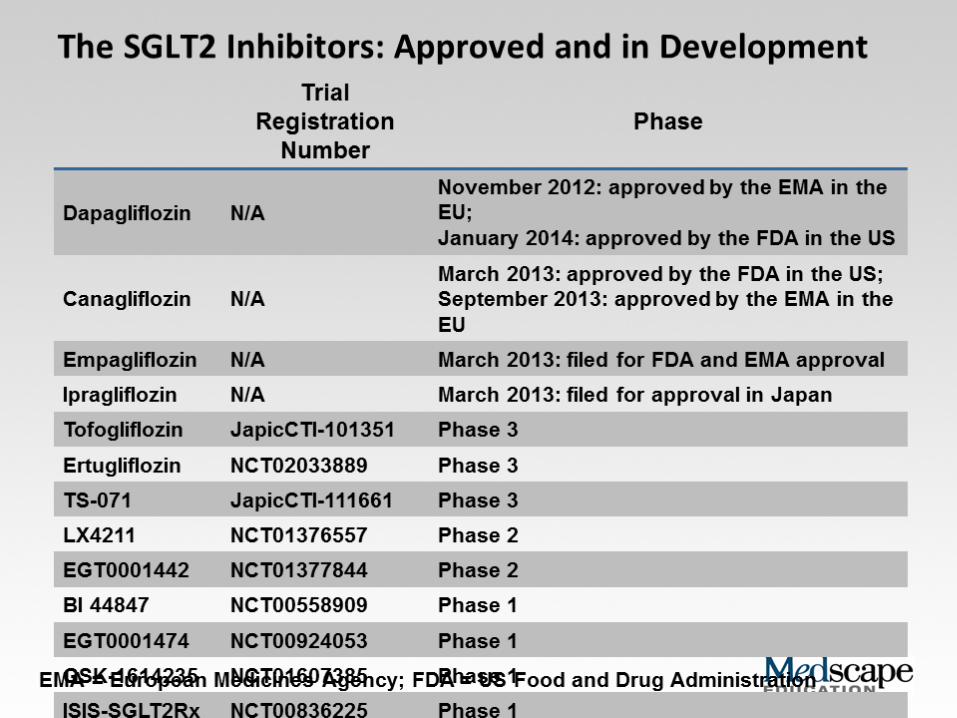

SGLT2 inhibitors.• Canagliflozin (Invokana)
– 100mg and 300mg• Avoid in CrCl <30- 45ml/min
• Dapagliflozin (Farxiga)– 5mg and 10mg
• Avoid in CrCl < 60ml/min
• Empagliflozin (Jardiance)– 10 and 25mg
• Avoid in CrCl < 45ml/min
CANAGLIFLOZIN

Canagliflozin Pharmacokinetics
• ORAL BIOAVAILABILITY: 65%• PEAK ACTION : 30-120 minutes.• Pharmacokinetics is independent of age, body
weight, gender, administration with food & mild to moderate hepatic impairment.
• Amount of glucose filtered in glomerulus depends not only on plasma glucose levels but also on GFR.
• Hence it can be expected that decrease in renal function can affect the activity of these drugs.
• In some clinical trials it was seen that patients with GFR values between 30-50 also showed significant reductions in HbA1c values, although they were smaller than those of patients with normal GFR.
• Dose adjustment: 100mg in patients with GFR less than 60.

• 40% is excreted unmetabolized in faeces.• Minor amount under goes o- glucorodination
and forms two inactive metabolites which are excreted by urine.
• Half life is 11-13 hours hence once daily dose is therapeutically sufficient.
• Dose: 100mg , 300mg.
Glycemic Efficacy
• Average reduction of:
– HbA1c: 0.5-1%
– Fasting plasma glucose (FPG): 15-40mg/dL
– 2-hour post-prandial glucose (PPG): 45-65mg/dL
• ***Take before first meal of the day***
• Weight loss 1-4%

Glycemic Efficacy of SGLT2s• Widely varying reductions in average HbA1c and FPG
depending on drug, dose and whether used as monotherapy or combination therapy
Drug HbA1c Reduction FPG Reduction
Canagliflozin -0.73 to -1.08% -22 to -47mg/dL
Dapagliflozin -0.52 to -0.59% -16 to -28mg/dL
Empaglifozin -0.62 to -0.66% -13 to -36mg/dL

Canagliflozin
GroupHbA1c Reduction FPG Reduction
100mg 300mg 100mg 300mg
Monotherapy -0.91 -1.16 -36 -43
Add-on metformin
-0.62 -0.77 -30 -40
Add-on sulfonylurea
-0.74 -0.83 -30 -47
Add-on insulin -0.65 -0.73 -23 -29
Add-on 3 drug regimen
-0.71 -0.92 -22 -35

DapagliflozinGroup
HbA1c Reduction FPG Reduction5mg 10mg 5mg 10mg
Monotherapy -0.5 -0.7 -19.9 -24.7
Add-on metformin
-0.4 -0.5 -15.5 -17.5
Add-on glimepiride
-0.5 -0.7 -19.3 -26.5
Add-on pioglitazone
-0.4 -0.6 -19.5 -24.1
Add-on insulin -0.5 -0.6 -- -25
Add-on 3 drug regimen
-- -0.48 -- -27.9

Empagliflozin
GroupHbA1c Reduction FPG Reduction
10mg 25mg 10mg 25mg
Monotherapy -0.7 -0.9 -31 -36
Add-on metformin
-0.6 -0.6 -26 -29
Add-on pioglitazone
-0.5 -0.6 -23 -28
Add-on insulin -0.5 -0.7 -12.9 -17.9
Add-on 3 drug regimen
-0.6 -0.6 -29 -29
1

Monotherapy: HbA1c Reductions
CanagliflozinDapagliflozin
Empagliflozin
0
0.2
0.4
0.6
0.8
1
1.2
0.91
0.5
0.7
1.16
0.7
0.9
Low DoseHigh Dose
A1c
(%
) Red
uctio
n

Monotherapy: FPG Reductions
CanagliflozinDapagliflozin
Empagliflozin
0
5
10
15
20
25
30
35
40
45
36
19.9
31
43
24.7
36
Low DoseHigh Dose
FPG
(m
g/dL
) Red
uctio
n

Postprandial Reductions
canagliflozindapagliflozin
0
10
20
30
40
50
60
70
4847
64
51
low dosehigh dose
PPG
(m
g/dL
) Red
uctio
n
.

Weight Loss
Group Low Dose (kg) High Dose (kg)
Canagliflozin 2.2 3.3
Canagliflozin + Insulin 1.9 2.4
Dapagliflozin 2.2 2
Dapagliflozin + insulin 1 1.7
Empagliflozin 2.5 2.8
Empagliflozin + insulin 3 3
1

Hypoglycemia
• Insulin-independent mechanism of action– Low risk when used as monotherapy
– Comparable to that of metformin or sitagliptin
– Increased risk with insulin and insulin secretagogs
• SGLT2s lower the renal reabsorption of glucose
threshold without completely inhibiting it
• Renal threshold of < 70mg/dL
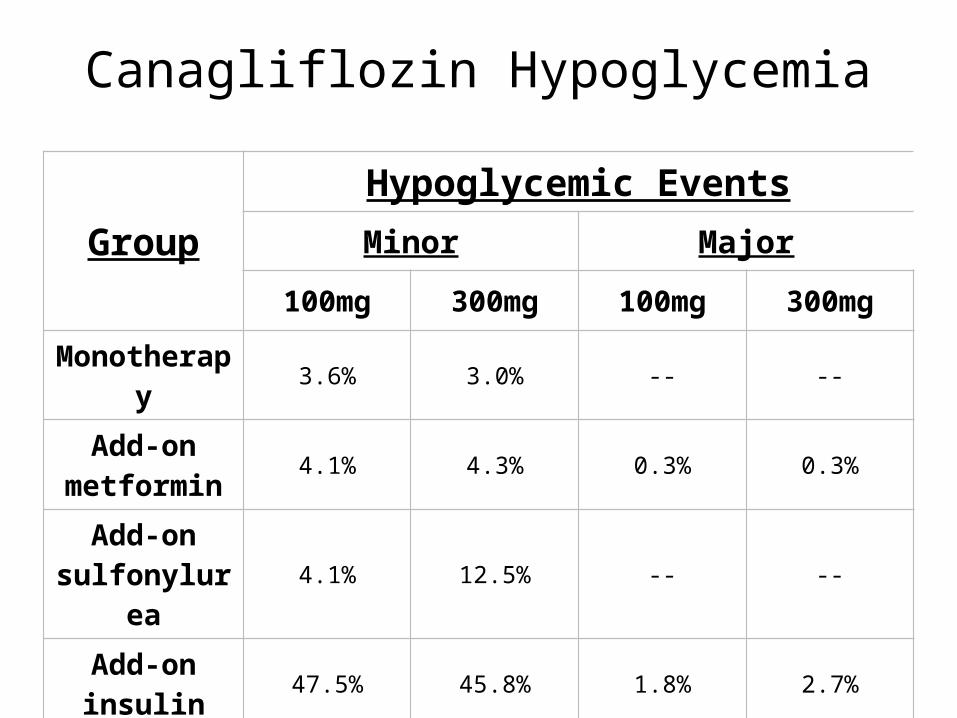
Canagliflozin Hypoglycemia
Group
Hypoglycemic Events
Minor Major
100mg 300mg 100mg 300mg
Monotherapy 3.6% 3.0% -- --
Add-on metformin 4.1% 4.3% 0.3% 0.3%
Add-on sulfonylurea 4.1% 12.5% -- --
Add-on insulin 47.5% 45.8% 1.8% 2.7%
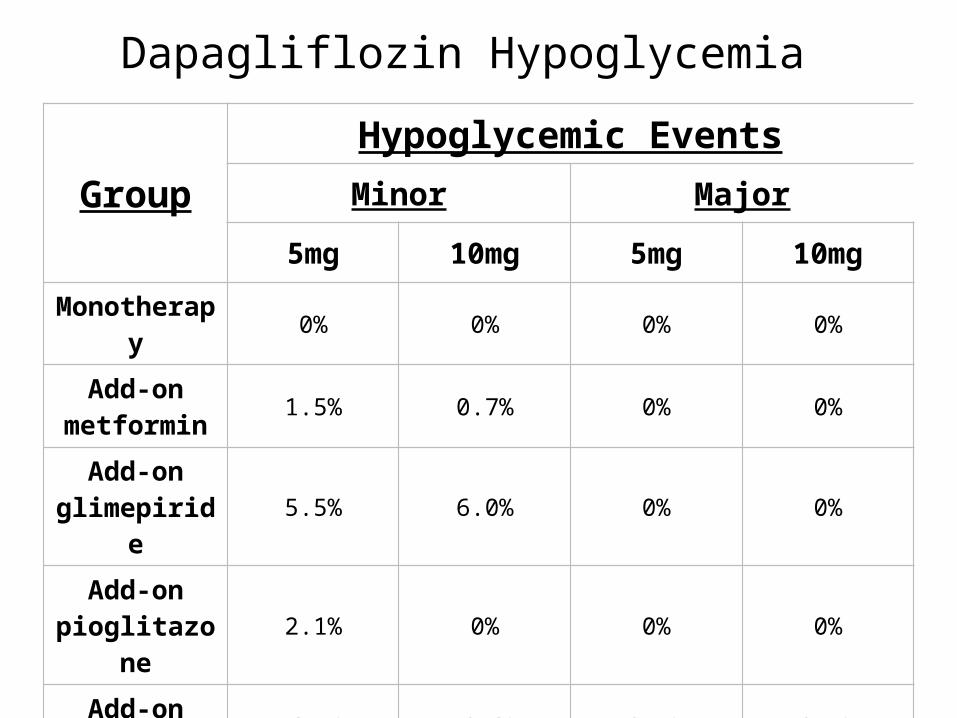
Dapagliflozin Hypoglycemia
Group
Hypoglycemic Events
Minor Major
5mg 10mg 5mg 10mg
Monotherapy 0% 0% 0% 0%
Add-on metformin 1.5% 0.7% 0% 0%
Add-on glimepiride 5.5% 6.0% 0% 0%
Add-on pioglitazone 2.1% 0% 0% 0%
Add-on insulin 43.4% 40.3% 0.5% 0.5%

Empagliflozin Hypoglycemia
Group
Hypoglycemic Events
Minor Major
10mg 25mg 10mg 25mg
Monotherapy 0.4% 0.4% 0% 0%
Add-on metformin 1.8% 1.4% 0% 0%
Add-on pioglitazone 1.2% 2.4% 0% 0%
Add-on insulin 19.5% 27.1% 0% 1.3%
Add-on 3 drug regimen 16.1% 11.5% 0% 0%

SGLT2 Add-on Insulin Therapy
GroupHypoglycemic Events
Minor Major
100mg 300mg 100mg 300mg
Canagliflozin 47.5% 45.8% 1.8% 2.7%
Dapagliflozin 43.4% 40.3% 0.5% 0.5%
Empagliflozin 19.5% 27.1% 0% 1.3%

Side Effects
• Infection risk
• Polyuria
• Hypotension
• Hyperkalemia
• Impaired renal function
• Increase in LDL

Infection Risk
• Increased glucose in urine
• Genital mycotic > urinary tract infections (UTIs)
• At increased risk:– Females
• 11-15% F > 1-8% M
– Uncircumcised males
• Dose-independent
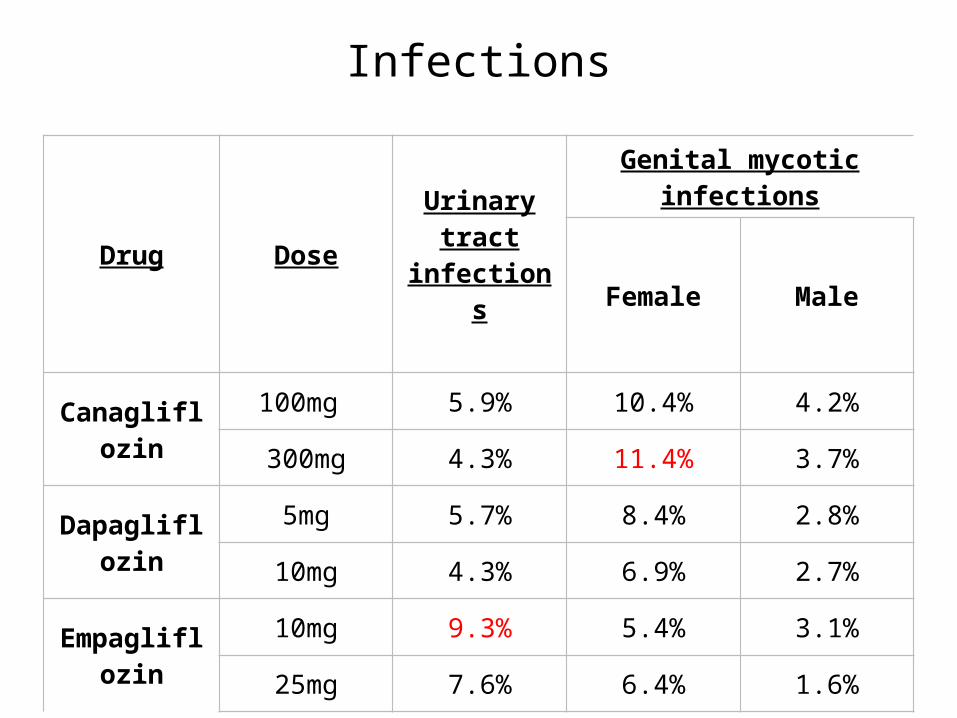
Infections
Drug Dose Urinary tract infections
Genital mycotic infections
Female Male
Canagliflozin100mg 5.9% 10.4% 4.2%
300mg 4.3% 11.4% 3.7%
Dapagliflozin5mg 5.7% 8.4% 2.8%
10mg 4.3% 6.9% 2.7%
Empagliflozin10mg 9.3% 5.4% 3.1%
25mg 7.6% 6.4% 1.6%

Kidney Function
• Avoid use in CrCl < 30-60ml/min
• Dose-dependent decrease in eGFR (2-6ml/min)– However, improves overtime (1-3ml/min)
• Renoprotective effects- delays albuminuria .
• Glycemic efficacy declines with decreased renal function
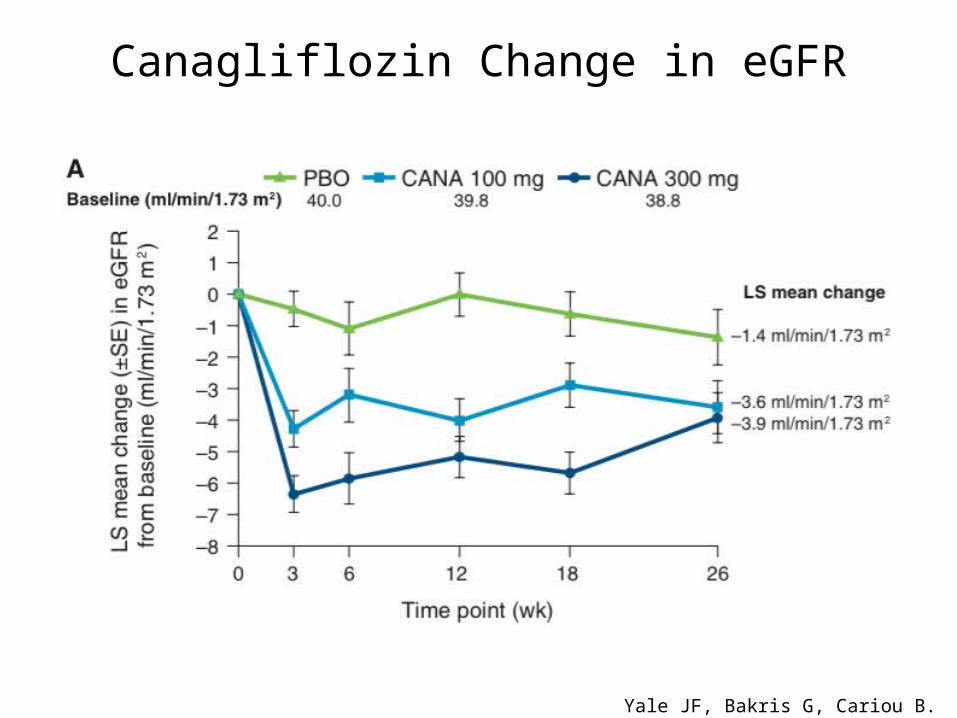
Canagliflozin Change in eGFR
Yale JF, Bakris G, Cariou B. Diab Ob Metab 2013;15:463-73

Kidney FunctionDrug Dose Change in SCr
(mg/dL)Change in eGFR
(mL/min/1.73m2)Canagliflozin 100mg
*Renal impaired0.020.16
-2.3-3.6
300mg *Renal impaired
0.030.18
-3.4-4.0
Dapagliflozin 5mg*Renal impaired
-0.0010.06
0.8-4.2
10mg*Renal impaired
0.0010.15
0.3-7.3
Empagliflozin 10mg 0.01 -0.6
25mg*Renal impaired
0.010.11
-1.4-2.8

Kidney Function
• Osmotic diuresis & volume depletion– Polyuria (including nocturia) resulting in
dehydration, hypovolemia, syncope, etc.
– Increased risk if > 75yo, eGFR < 60ml/min or on loop diuretics
• Dose-dependent decrease in blood pressure– Systolic BP 3-6mmHg
– Diastolic BP 1-2mmHg

Dyslipidemia
• Dose-dependent increase in LDL
– Canagliflozin: 4.5 – 10%
– Dapagliflozin: 1 – 9.5%
– Empagliflozin: 4.6 – 6.5%
• Increase in HDL 1.5 – 5%
• Decrease in TG -16% - +4%
Pregnancy and Lactation
• Category C
• Fetal renal development and maturation
• 2nd and 3rd Trimesters
• Can pass through breast milk






SGLT2 Inhibitors Lower Renal Threshold for Glucose Excretion
Place in DM Management: Non-Formulary Criteria
• T2DM with adequate renal function • Reduction of < 1% in HbA1c needed to reach goal
The patient is not a candidate for or inadequate control with:
MetforminSulfonylureasPioglitazoneDPP-4 inhibitors
Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitor (Canagliflozin and Dapagliflozin) Criteria For Use. VHA. Department of Veterans Affairs; May 2013.

Current Therapies Glycemic Efficacy
* SGLT2s average A1c reduction = 0.5 – 1 %
Drug Average HbA1c Reduction
Meglitidines 0.5-1.5%Biguanides 1-2%Sulfonylureas 1-2%TZDs 1-1.5%Alpha-glucosidase inhibitors 0.5-1%DPP-4s 0.5-1%GLP-1s 1-1.5%Amylin Agonists 0.5-1%

SUMMARY & CONCLUSION
• SGLT2 inhibitors are a new strategy for the treatment of type II diabetes mellitus.
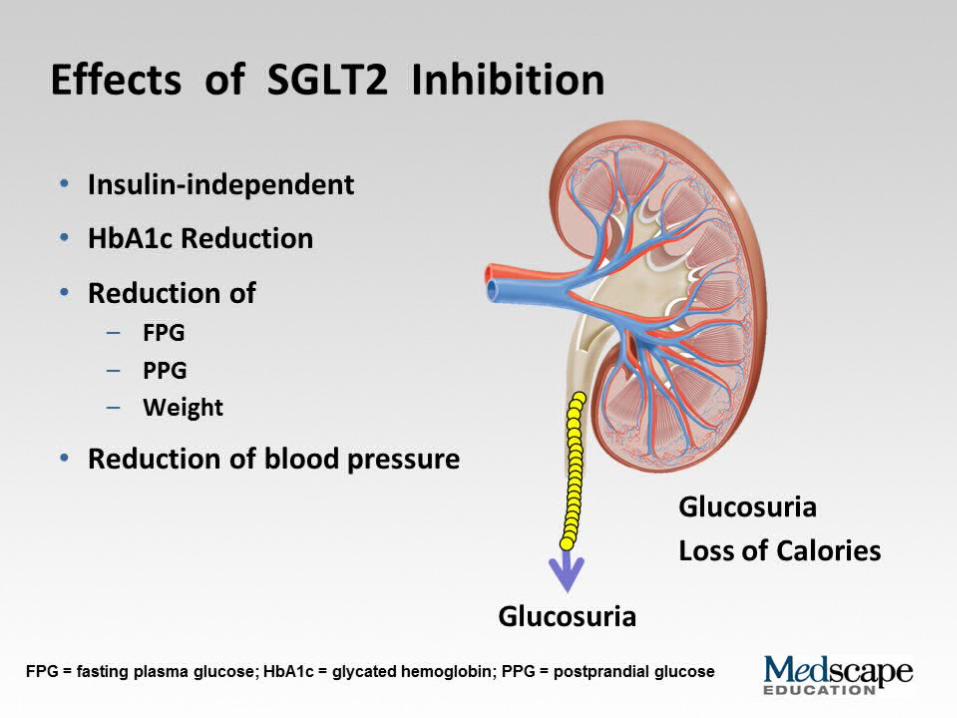
• Their novel mechanism of action is based on the blockage of SGLT2 Na+/glucose co-transporters of renal tubular cells which as a result has glucosuria and excess calories' loss.
• The accompanying beneficial effects of this phenomenon are: the regulation of fasting and postprandial blood glucose levels HbA1c reduction body weight loss reduction of systolic blood pressure.

• However it is associated with genital and urinary tract infections.
• Due to this innovation, the new category of agents can be combined with the existing treatments for type 2 diabetes mellitus (TIIDM) and be an effective weapon for the management of uncontrolled diabetes.

FDA warning issued on 15/03/2015
• “The US Food and Drug Administration (FDA) warned today that sodium-glucose cotransporter-2 (SGLT2) inhibitors used to treat type 2 diabetes may lead to ketoacidosis requiring hospitalization.”
• Ketoacidosis is not typically observed in patients with type 2 diabetes, the FDA notes, and the DKA case presentations were "atypical in that glucose levels were only mildly elevated at less than 200 mg/dL in some reports, while patients with type 1 diabetes who have DKA typically have glucose levels greater than 250 mg/dL."

The FDA advice
• "Healthcare professionals should evaluate for the presence of acidosis, including ketoacidosis, in patients experiencing these signs or symptoms; discontinue SGLT2 inhibitors if acidosis is confirmed; and take appropriate measures to correct the acidosis and monitor sugar levels."

Summary of Ongoing Cardiovascular Outcomes Trials with SGLT-2 Inhibitors
Canagliflozin Dapagliflozin Empagliflozin
Name NCT-01032629 NCT-01730534 NCT-01131676
Status Ongoing Recruiting Ongoing
No. patients 4330 17,150 7000
Primary outcome
Major cardiovascular (CV) events,
CV death, nonfatal MI,
nonfatal stroke
Time to CV death, MI, or
ischemic stroke
Time to CV death, nonfatal
MI, nonfatal stroke
Estimated completion June 2018 April 2019 March 2018

REFERENCES1. Jung CH, Jang JE, Park JY. A novel therapeutic agent for type II diabetes mellitus: SGLT2 inhibitor.
Diabetes Metab J 2014;38261-73.2. Fujita Y, Inagaki Y. Renal sodium glucose cotransporter 2 inhibitors as a novel therapeutic
approach to treatment of type 2 diabetes: clinical data and mechanism of action. J Dibetes Invest. 2014;5:265-75.
3. Chen LH, Leung PS. Inhibition of the sodium glucose cotransporter 2 its beneficial action and potential combination therapy for type 2 diabetes mellitus. Diabetes Obes Metab. 2013;15:392-402.
4. Invokana® (capagliflozin) package insert. Titusville (NJ): Janssen Pharmaceuticals; May 2014.5. Farxiga® (dapagliflozin) package insert. Prineton (NJ): Bristol-Myers Squibb; Aug 2014.6. Jardiance® (empagliflozin) package insert. Ridgefield (CT): Boehringer Ingelheim; Aug 2014.7. Vasilakou D, Karaglannis T, Athanasiadou E, et al. Sodium-glucose cotransporter 2 inhibitors for
type 2 diabetes systematic review and meta-analysis. Ann Intern Med. 2013;159:262-74.8. Hass et al; Efficacy, safety and regulatory status of SGLT2 Inhibitors;Nutrition & Diabetes 2014;(4)
e143.9. Vasileios Andrianesis; John Doupis,The Role of Kidney in Glucose Homeostasis — SGLT2 Inhibitors,
a New Approach in Diabetes Treatment.Expert Rev Clin Pharmacol; 2013;6(5):519-539. 10. www.medscape.com/ fda/ sglt2 inhibitors/ warning.

THANK YOU.






![Presentation1.ppt [โหมดความเข้ากันได้] · Title: Microsoft PowerPoint - Presentation1.ppt [โหมดความเข้ากันได้]](https://static.fdocuments.us/doc/165x107/5ec776d210d7bd5f6f00774b/aaaaaaaaaaaaaaaaaa-title-microsoft-powerpoint.jpg)











