Presentation to OHA : HealthAchieve Bonnie Burnes, … 2014/HSFR and Quality...Focus on COPD...
25
QBP Focus on COPD Presentation to OHA : HealthAchieve Bonnie Burnes,William Osler Health System November 5th, 2014
Transcript of Presentation to OHA : HealthAchieve Bonnie Burnes, … 2014/HSFR and Quality...Focus on COPD...
QBPFocus on COPD
Presentation to OHA : HealthAchieveBonnie Burnes, William Osler Health System
November 5th, 2014

Agenda Overview
1. Organizational Strategic and Clinical Context
2. QBP Governance & Phased Approach
3. COPD Case Study
4. Key Successes and Lessons Learned
2

3
A Typical Day at Osler
4
More than…
600
20
195
156
Emergency Visits
Babies born
Dialysis clinic visits
Surgeries
Osler’s Corporate Strategic Plan
5
Deliver exemplary care in the eyes of our patient and peers
Create health services with an unwavering commitment to patient inspired care
Foster bold innovative partnerships to create a unified health system
Create impact beyond our immediate community through education and innovation
SD 2 - Priorities:
1. Continually refine services to meet the needs of target populations
2. Ensure clinical best practices across the organization
3. Ensure sustainability by meeting the challenges of new funding models
5

Osler’s Clinical Priorities Plan
66
A system designed to support timely accessto appropriate care, across the continuum of care.
Effort to prevent onset and/or exacerbation of chronic diseases, such as diabetes, COPD and CHF.

Osler’s Clinical Priorities Plan
7
se Increased Scheduled Outpatient Activity
Reduce Unscheduled/ Avoidable Emergency Visits & Inpatient Admissions
7


QBP Governance Structure
Corporate Quality
Governance Council
QBP Steering Committee
COPD Expert Panel
CHF Expert Panel
Stroke Expert Panel
Hip FractureExpert Panel
Endoscopy Expert Panel
Senior Leadership Team (SLT)
Dr. Tamara Wallington, Co-ChairBonnie Burnes, Co-ChairCorporate Chief of EDDirector of Quality, Practice & Patient Safety (HHCC)Director of Client Services & Clinical Analytics (CW CCAC)Hospitalist LeadGeneral Internist LeadDirector of Nursing and Professional PracticeFinance/Case CostingDecision SupportCoding & Transcription
99
Quality Improvement
Plan
Osler Expert Panel
Core Team• CCE Rep• Pharmacy• Educator • Resource Nurse• Front line MD, Nurse• Nurse practitioner• Allied Health – OT/PT/SLP• CCAC• Decision Support• Discharge Planner• Clinical Informatics• Administrative support• Coding
10
Ad Hoc• Finance• Headwaters Health Care Centre• Palliative Care• Telehomecare• ED Chief and educators• Library staff• Lab• Palliative Care• Research
10

QBP Phases of Development
1111
Phase 1 Current State Assessment
Phase 2QBP
Assessment
Phase 3Gap Analysis
Phase 4Closing the
Gap
Phase 5 Monitor
Implementation Accountability/ Sustainability

Osler’s Progress with QBPs
12
Phase 1Current State Assessment
Phase 2QBP
Assessment
Phase 3Gap Analysis
Phase 4Closing the
Gap
Phase 5Implementation/Accountability/Sustainability
Jan 2014 Feb 2014 Mar 2014 May 2014 Aug 2014
COPD
Feb 2014 Mar 2014 Apr 2014 Jun2014 Aug 2014
CHF
May 2014 Jun 2014 Jul 2014 Aug 2014 Oct 2014
Hip Fracture
May 2014 Jul 2014 Aug 2014 Sep 2014
Stroke
Aug 2014 Oct 2014
GI Endoscopy


Current State and QBP Assessment
14
How do we create sustained improvement?

Current State and COPD Process Map
15
Patient arrives Emergency(Walk-in/EMS/Transferred from
Outpatient Clinic)
Patient taken to ED (Placement based on CTAS score*)
Primary Care Nurse initiates Medical Directive
Patient assessed by Triage Nurse Patient assessed by ED Physician
Order written
Discharge Planning Referral to CCAC Referral to West Park
Decision? Admit to MAU
Referred to Internal Medicine
Discharge home
CTAS score
RESUS Acute Sub-Acute
* Patient Placement
OR OR ATC
Order executed
Decision made based on result
Patient with COPD automatically referred to Respirology Consultant
Patient goes home
Waiting time
Bed available?
Patient stays in ED
No Yes
Bed available?
Patient stays in ED
No
Patient transferred to Medical Unit
Yes
Patient admitted to Medical Unit OR
% of admitted to MAU
OR
Develop COPD Order Set
Patient transferred to MAU with Order Set filled by ER Physician
Patient transferred to MAU with handwritten order
Patient daily assessed by MD/NP
MAU is 48 hours Unit run by MD and supported by NP
Patient stays maximum 48 hrs starting from Triage point
Delay in ED depletes 48 hr time limit
Patient seen by ALC team (PT/OT/RT/Dietician/SW/Pharmacist/COPD Educator)
Discharge Planning: Transportation arrangement CCAC PFT referral Referral to other outpatient clinic Give Patient the copy of Lab/DI test result for revisit NP consultant notes sent to FP For Patient without FP: provide resource package and ask Patient come back to Urgent Care Clinic/ED
Decision?Admit to Medical Unit
Discharge home
Patient goes home With family By EMS By alternative transportation
Transportation Issues
Develop Order Set for Discharge
Patient transferred to Medical Unit
Confusion around the Primary Care Physician:
FP or Walk-in Clinic?
Connection to Telehomecare
Referral to COPD Education Clinic
Referral to Pulmonary Rehab
Care Connect
NRT
Respirology Patient goes to
other medical unit
Regular Inpatient Process followed(ALC Team: OT/PT/RT/Dietician)
As blend unit (GIM/Resp), Respirology receives a lot of non-Resp patient
Admission decision cohorts Patient to appropriate unit
Order Set Utilization
Having Respirologist on
the floor
Isolation beds shortage
Longer stay in ED may cause Patient not receiving appropriate
care; Patient could end to Critical Care Unit instead
Inconsistent process – Patient may/may not Come with Resp. Order Set Assigned to Resp. Hospitalist Have RT consultation Referred to Respirologist Get PFT Refer to COPD Education Clinic/
Pulmonary Rehab Clinic
% of Pt with short breath/chest complain/
COPD history
COPD Patient sits in waiting area with
other PatientsWaiting time
50% Patient with Order Set
Med
ical
Uni
tM
AU
Emer
genc
y
Measurements
Issues & Hot spots
Potential Leverage Points
% of Diagnosed % of Admitted
Typically COPD Patients are CTAS 2/3
Investigation and treatment initiated
Pulmonary baseline
GIM/Respirologist involves in
decision-making
% of Discharge
home
Patient admitted to Medical Unit
% of admitted to Medical Unit
CTAS 1
UCCOR
CTAS 2 CTAS 3 CTAS 4/5
Respirology Educuation
CCAC Responsible Nurse RT Consultant
Pharmacy Tech sees patient in MAU for BPMH
Closing the Gap – Leverage Points
16
• Streaming to Respirology Cluster• Spirometry: baseline• Consults: RT, Dietitian• Greater involvement with Specialists/ Referral to Respirologists• Nicotine Replacement Therapy Module & Smoking Cessation• COPD Order Set• Pulmonary Rehab Clinic• COPD education• Pharmacist consult for med rec• Vaccines: influenza and pneumococcal• Automatic referral to CCAC for Rapid Response Nurse program• Automatic referral to Telehomecare• Standardization of antibiotic ordering practices

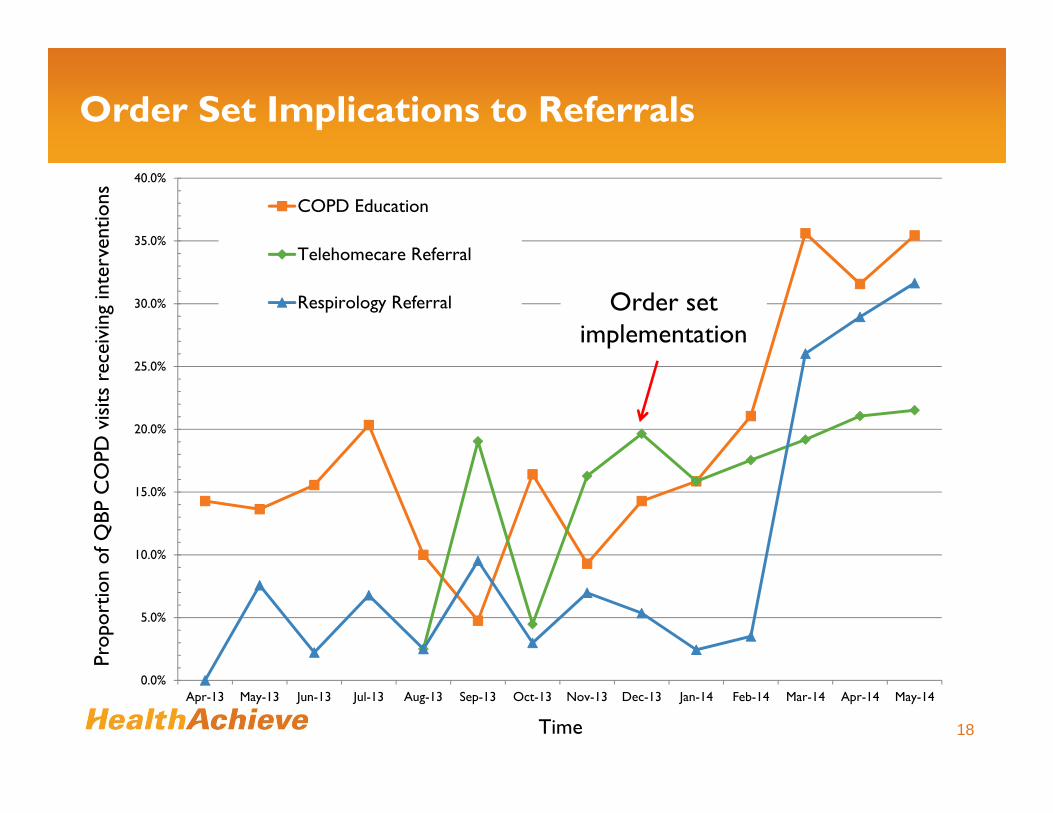
Order Set Implications to Referrals
18Time
Prop
ortio
n of
QBP
CO
PD v
isits
rec
eivi
ng in
terv
entio
ns
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14
COPD Education
Telehomecare Referral
Respirology Referral Order set implementation

Order Set Implications to RIW and Readmissions
19Time
Res
ourc
e In
tens
ity W
eigh
t
0
0.05
0.1
0.15
0.2
0.25
0.3
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50
1.60
1.70
1.80
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14
RIW
Readmissions
Order Set Implementation
Rea
dmis
sion
Rat
e
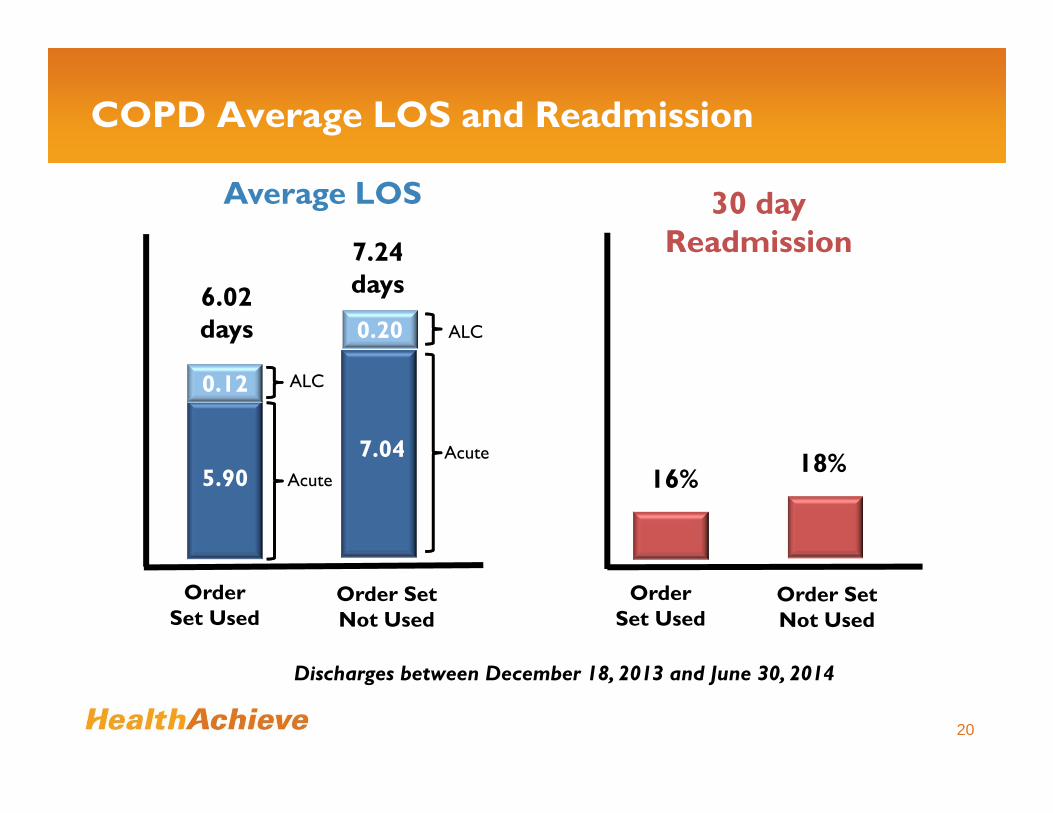
COPD Average LOS and Readmission
20
Order Set Used
6.02 days
Average LOS
Order Set Not Used
7.24 days
0.12
5.90
ALC
Acute
7.04
0.20 ALC
Acute
Order Set Used
16%
30 day Readmission
Order Set Not Used
18%
Discharges between December 18, 2013 and June 30, 2014
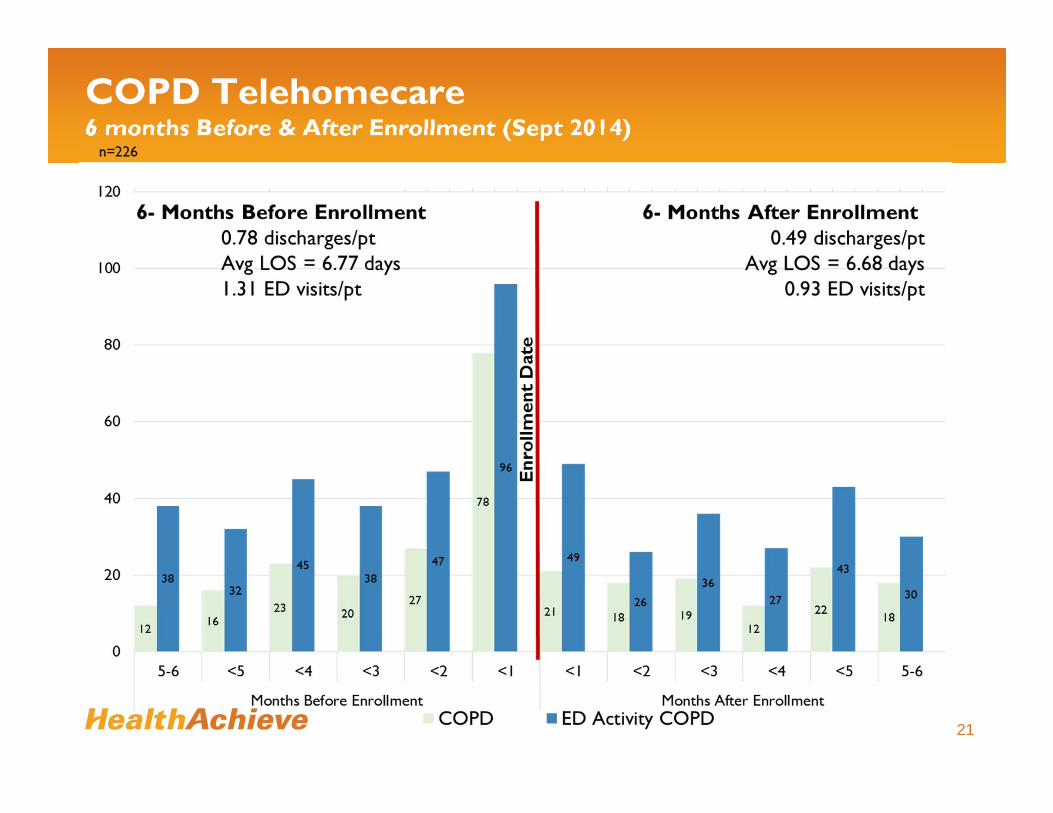
COPD Telehomecare6 months Before & After Enrollment (Sept 2014)
21

Sustainability
22
Outcome Measures:1. Readmissions to Osler within 28 days post discharge for COPD2. Average total LOS for acute inpatients 3. Volumes of COPD QBP acute inpatients4. Resource Intensity Weights
Process Measures:1. Number of patients enrolled in Telehomecare 2. Number of referrals to the Rapid Response nurse (24 hrs. discharge)3. % patients admitted to Respirology unit4. Order set utilization5. Referral to COPD education and Pulmonary Rehab

Osler Lessons Learned
23
• Team and front line ownership is critical
• Broad team representation is necessary to achieve buy in
• Changing behaviours is challenging
• It takes time to implement and sustain change
• Benefits to having a structured governance approach across all QBP’s
• Standardized process has provided tremendous learning and consistency for the organization

Questions and Comments
24

25