Prepair2Perform (P2P) Assess, Align and Optimize Biomechanics
24
Prepair2Perform (P2P) Assess, Align and Optimize Biomechanics Chad Benson MSc, PTS Author VYPER HYPERSPHERE HYPERVOLT
Transcript of Prepair2Perform (P2P) Assess, Align and Optimize Biomechanics

Prepair2Perform (P2P) Assess, Align and Optimize Biomechanics Chad Benson MSc, PTS Author
VYPER
HYPERSPHERE
HYPERVOLT

The sitting disease and automation are killing our nervous systems, proprioception, function, metabolism, and mobility. Today more than ever, clients walk in the training door deactivated. Even those who work out regularly spend most of their day in low nervous system activation. In this seminar, you will learn how to assess ROM & Myoneural strength, as well as how to apply corrective movement therapies in order to:
1. Optimize movement via active range of motion 2. Optimize strength, power, footspeed & quickness 3. Optimize recovery between workouts 4. Individualize training programs
What is Vibration Therapy. It is a form of vibratory or percussive motion applied via an outside source. This motion can be applied via
Whole Body Vibration Muscle Specific Vibration
1. WBV (whole body vibration): is a general non-specific technique, traditionally applied by standing or planking (hands on a broad base)
2. MSV (muscle specific vibration). Is applied to specific body-parts via smaller portable devices with varying amounts / surface area.
a. VYPER – Frequency (level 1-3) are in alignment w WBV research
b. HYPERSPHERE – Frequency (level 1-3) are in alignment w WBV
research
3. Percussion therapy can be altered via a. Amplitude of shift, b. Frequency of shift & c. Direction of shift
4. How is Percussion different from TENS & Muscle Stimulation?
Vibration is mechanical stimulation, TENS is Transcutaneous electrical
nerve stimulation is the use of electric current produced by a device to
stimulate the nerves for therapeutic purposes. Muscle Stim is Electrical
muscle stimulation leading to muscle contraction via impulses

Benefits of Muscle Stimulation & Vibration: vibration therapy causes muscles to repeatedly eccentrically and concentrically contract resulting in nervous system activation, possible injury prevention & performance enhancement. The unused deactivated portion of the nervous systems loses the ability to generate force and restricts movement to protect itself from instability & excessive force. To better understand the benefits of activation and warm-up, the potential physiologic mechanisms must be reviewed. 1. Improved mobility & active ROM: to understand how vibration improves
ROM, we need to understand the difference between active & passive ROM.
a. Active range of motion is when a joint is moved through its range with
the person moving the joint him or herself.
b. Passive range of motion is when something or someone helps or
creates the movement. More importantly, it’s essential we assess ROM
& identify neurological “dead zones”.
The traditional way to perform release in at home or in a gym is foam rolling or
SMR (self myofascial release). Recent evidence has indicated myofascial
compression alone does not break or “release” fibrotic material commonly found
even at the most superficial muscular layers.
It likely leads to improved GLIDE
between the myofascial layers
IINTERFACES ARE ESSENTIALLY THE
FASCIAL PLANES BETWEEN LAYERS
LACK OF GLIDING IS THE ENEMY
CAUSED BY DEHYDRATION, REPETITIVE
STRESS, INCORRECT FIRING/LOADING
SEQUENCES, JOINT FUNCTION REVERSAL,
SLEEP PATTERNS
HYALURONIC ACID LAYER MEMBRANE
DISTORTION LEADS TO DIRECT FASCIA
CONTACT AND ADHESION
SMR / Foam Rolling is unlikely to create myofascial release:
IT TAKES APPROXIMATELY
2000LBS OF FORCE PER /INCH TO
MECHANICALLY DISTORT FASCIA…
ROBERT SCHLEIP [Cite your source here.]

2. Improved circulation & muscle thermogenesis:
https://drive.google.com/file/d/0B37decpR5tu3OS1qWTZQTHRxejA/view
3. Improved proprioception, muscle co-contraction & joint stability: one the
major reasons for increased ROM with vibration, is increased joint stability.
This is most commonly seen amongst the mobility joints. Below is a great
illustration of the joints and therefore motions that are most likely to improve
via this mechanism. But how do we know that this is the mechanism we need
to work on???? This is the cool part: if you have identified a dead zone, then
stability / antagonist strength training is more important than flexibility / ROM
training 😊. In the links below, I have provided an example of active vs
passive ROM for 2 of the mobility joints (shoulder & hip) illustrated below:

4. Improved posture: the combination of low intensity (level 1) vibration is the
stimulation of postural / tonic / stabilizer muscle chains. When there is a shift
in the length of a muscle (i.e. posterior shoulder muscles become weak when
upper back kyphosis exist).
a. Initially, the tonic muscles work harder to reestablish joint alignment
b. Over time this battle leads to fatigue and a weakening of the tonic
muscles in that region.
c. Those muscles are hard to activate w traditional training methods.
Specialized low threshold training and NS activation work in
combination to correct postural distortion
5. Improved bone density: vibration and vibration platforms lead to G-force like
ground reaction forces that transmit through the joints that are in direct
contact with the platforms. Methods like standing, compressing between the
hands, squeezing between the knees are all create transmission of bone
density stimulation ground reaction forces on the vibratory
6. Improved force & power: when the nervous system is upregulated and not
being inhibited via instability / pain, the body is permitted to move more
aggressively. Therefore it can develop a greater portion of its available
strength and power.
a. Preconditioning exercise performed with WBV at 50 Hz seems to enhance on-ice
sprint performance in ice-hockey players.
b. 60s of WBV with partial squat enhanced the performance score on the
QFT (Dot drill)
7. Increased pain threshold: one of the major benefits is a temporary alteration
in the pain mediated nervous system inhibition. Through up regulation of
muscle & joint mechanoreceptor firing, the brain perceives that the joint &
affected tissue are functioning properly. The mistake, thinking the issue has
been removed. Pain signals are designed to protect us, but in combination
with good movement management & corrective programming, we can
permanently change posture, joint stability, tissue health and therefore
mechanoception.

Scope of Practice & Contraindications of Percussion & Vibration
Scope of Practice: falls into the scope of practice of your current certifications.
In general, the application of vibration should applied to healthy individuals, not
currently not suffering any form of acute muscular (i.e. injury) or chronic joint
pain.
Contrainidications (according to Theragun):
1. Vibration should not be applied over contused (bruised) soft tissue,
thrombus (blood clot), or the site of phlebitis or varicose vein,
because of the danger of additional thrombus development or the
precipitation of an embolus.
2. Do not apply vibration around the lips of children, even for
desensitization of the lips. Likewise, vibration should not be
applied to the S2, S3, or S4 sensory dermatomes of infants or
children with immature gastrointestinal systems.
3. The vibration of phalangeal (finger) joints will almost certainly
cause them to spontaneously swell (become edematous),
sometimes to a gross extreme. Edema may become so extreme
that pitting edema may become evident in both the phalanges and
in the metacarpal portions of the hand.
4. If vibration is used in combination with electrical stimulation for
the treatment of extrafusal muscle spasm, trigger point formation
referred pain, or to facilitate the lengthening of a muscle, apply it
after electrical stimulation.
5. My addition to this is not on pregnant women T7 to sacrum.
6. Not on genitalia and not above your head or above Adam's
apple/or C5 area of the neck. Not on or near a pace Maker.

Mobility Assessments (ROM + Stability = Mobility):
The 1st step in reactivating the nervous system is assessing the individuals ROM
and stability. Assessment is essential to safely and effectively individualizing a
client’s training experience.
Peripheral Myoneural Strength (Stability) & ROM Testing: healthy or
functionally specific ROM and muscle strength in muscles surrounding the ankle,
knee, hip, scapula, elbow and wrist are extremely important when performing any
functional performance task or exercise.
1. Keep your assessment simple and quick.
2. Combine constant observation with your baseline assessment, P2P
prescriptions can be modified as movement compensations change.
3. Assessment should be broken down from the whole into the parts:
a) Dynamic posture / during movement (not covered). For Ex FMS
b) Fascial line / kinectic chain movement efficiency
c) Individual movements, mobility & strength at eROM (end range of motion)
Lacks myoneural strength / stability at the eROM: a client’s functional
movement quality (i.e. performance) is dependent on muscle compliance and the
muscle's force capabilities at any given moment throughout their ROM. Muscle’s
without significant tissue restriction (scar tissue / fibrosis / trigger point) perform
well at mid-range of motion. If & When they hit functionally unused (due to
restriction / inactivity / limited ROM use ), they test as:
a) Weak (1 or 2)
b) Strong w major
compensation
c) Strong but lacks
endurance
Lacks ROM (see slides) when one muscle is not able to elongate to the degree
(i.e. comply) needed to produce the movement, compensations must occur to
produce that movement. Compensations tend to create inefficient movement and
(or) synergistic dominance of the smaller assistance muscles. Force couple of
imbalances (i.e. overactive antagonist & synergists), over time result in altered
motor recruitment coordination (i.e. synergistic dominance & overactive
stabilizers).
In order for movement to occur, the combination of strength / stability & flexibility / ROM must occur to safely support this movement. To better understand which is limiting the movement, both must be assessed. There are several easy ways to assess each.

Myoneural Strength Testing 101
• Muscle eccentric contractions are stronger than concentric.
• It is not a test of true strength, it’s a test of the Nervous System & it’s
current state.
• Muscles are tested & activated in their neurological “dead zone”,
typically in their eROM.
• This position is often weakened due to
1. tightness in the antagonist muscle or opposing motion /
movement.
2. Insufficient use of that ROM while performing in life sport or
fitness
Myoneural Strength Testing Observations
• Normal: turns-on / fires against the resistance
• Abnormal on / overactive: typically seen as spasm
• Abnormal on / overactive synergist: typically seen as a compensation
in a nearby joint.
• Abnormal off / underactive: seen as a failed muscle test
• Abnormal / Lacks endurance: typically seen as easy to fatigue w
continued contract resist cycles
Myoneural Testing: How To
1. If the muscle adapts / functions normally, the eROM will feel strong
(i.e. muscle resists well). If not, it “breaks” and gives way. This means
“something” is interrupting the sensorimotor signal.
2. Notes:
1. Use auditory, visual & tactile cues
2. Tests are performed in a specific plane & ROM to ensure that
the tests accurately isolate specific tissue.
3. Meet what the client gives & allow them .5 to 1sec to develop
tension, then overload by 10%
4. Retest if the client didn’t resist / understood the command
5. Give moderate adjacent joint stability but too much may create
a false negative & prevent compensations
6. Note any compensations & retest with instructions to control
the compensation
7. Tester begins in a biomechanically advantaged position.

3. Phase 1:The client is cued to create a strong concentric contraction…
“your line of drive is up, my line of drive is down…drive up strong,
hold, don’t let me move you”
4. Phase 2:When the eROM / shortened ROM is achieved, the tester
meets (i.e. hold) the client’s force and overloads it by approximately
10-15%.
ROM / Flexibility Testing 101: There are 2 two major types of
flexibility • Active: sometimes referred to as mobility, it refers to the ability of a person to
drive or create ROM without outside assistance from gravity, straps or an assistant. It requires a person to actively move their segment via muscular contraction via force couples (i.e. agonist, synergist and stabilizers).
• Passive: does not require active assistance on behalf of the participant. Gravity, straps & or an assistant cues the client to let all tension out of the movement before moving the segment into it’s eROM.
• eROM is a person’s end range of motion. It is best defined as the point when a client reaches an end position with a low level of restrictive tension (i.e. stretch reflex or pain).
Range of Motion Testing: 1. When performed by a skilled practitioner, passive ROM of motion testing can
help determine the difference between biomechanical (i.e. bone on bone & capsular restriction Vs muscular / fascial tension).
2. Determining an eROM via active ROM, is in my opinion requires less skill and is more effective for understanding the potential movement deficiencies.
The big 3 questions are: 1. Is a person’s movement deficiency (i.e. restricted or altered ROM in an
overhead squat the result of a 1. tissue extensibility or 2. muscular coordination issue.
2. Do we need more flexibility or stability?? 3. Once assessment has determined the movement issues, what can we do to
change the is

There are several ways to help determine whether it’s a Myoneural or Tissue related issue. Both techniques outlined below require an unloading of the nervous system & therefore the functional requirements. Both start by including the nervous system, then removing to see if ROM is improved.
a. If ROM is > it’s a strength / stability issue b. If ROM is = similar, it’s a ROM issue c. If ROM is > but not ideal, it’s likely both
1. A Dead Zone = the difference between active & passive ROM. i.e. if I lift my
arms overhead, this is active ROM. If a trainer can pull them further, then
passive ROM is greater than active. When this active passive difference exist,
it’s referred to as the neurological dead zone and is best illustrated via this
equation.
o Passive ROM – Active ROM = Dead Zone = Stability
Active paex
Passive
Dead Zone

Methods to inhibit overactive muscle. When a movement has restricted
extensibility, we can improve it, by removing the restriction. For the purposes of this course we will focus on inhibiting overactive muscle. The most common methods to inhibit overactive tissue are: 1. Stretching
• Agonist Stretching (2+ min static, PNF, stretch wave – not shown in this course)
2. Myofascial release (SMR) on the involved tissue / muscle. Typically, an acute bout of SMR of the quadriceps is an effective treatment to acutely enhance knee joint ROM without causing a deficit in quad muscle strength.
• (Post) SMR pin & hold: takes advantage of pressure sensors and signaling to & from the pain & movement centers of the brain
• (Pre) SMR pin & move Create glide amongst the moving & fascial surfaces of the skin, muscle, and fascial layers.
3. Vibratory alteration: using high frequencies for relatively long periods (45-90 sec) may cause a muscle to weaken temporarily. The overactive muscle becomes underactive, and permits the previously weak muscle to fire (i.e. myoneural upregulation)
Methods to activate & under overactive muscle: Below we examine best practice & training methods for nervous system activation. Whether the goal is athletic performance, body composition, aging gracefully or fascial fitness, progressive activation & client preparation is an essential component of an effective personal training experience. Increasing the activation of the Mechanoreceptors and Fast Twitch (FT) Muscle Fiber (some techniques not covered in this course)is an essential component of 1. protecting joints and 2. optimizing your client’s results. FT muscle fibers are bigger, react more quickly and more forcefully than slow twitch fibers. These muscle fibers help prevent injury in the gym and burn more calories than their slow twitch counterparts. Therefore, FT activation is an essential component of any training program. Several components listed below must be included into every client workout, and all of them within the weekly plan. Some of the key tools to muscle & workout activation include: 1. (PW) Vibration: creates easier depolarization & Co-contraction. It also
Reduces arterial stiffness and increases plasma Nitric Oxide concentration (i.e. blood flow -see benefits)
• The vibration elicits involuntary muscle stretch reflex = proprioception contractions leading to increased motor unit recruitment and synchronization of synergist muscles
• Vibration creates pressure & activation of vibratory receptors (Pacinian Corpuscles).

Spinal Peripheral Activation: stimulation to the peripheral nerves upregulates
signalling to up and down the nervous system
Application: slowly roll (i.e. 1 inch
/ sec speed) along the erector
spinae muscle group. Use light
pressure and at least 1inch of
separation from the spinal
column.
Appendage Peripheral Activation: Creating a closed chain btwn floor & or
another bodypart creates action reaction forces up the kinectic chain. This
works best on firm (but not hard surfaces.)
Application: perform movement while standing on, holding or trapping
vibratory device btwn bodyparts (i.e. knees, hand against chest)
MSV (muscle specific vibration)
Application: slowly roll (i.e. 1 inch / sec speed) along the belly & ideally line of
pull of the muscle.
Vibration at eROM:
Application: Use various stretch techniques to place muscle into weak but
required / optimal position. Directly apply vibration along the belly of the
muscle in a previously weak range.
2. Oscillatory Rolling / Massage: oscillation can stimulate an automatic nervous
trigger known as the myotatic stretch reflex. Quickly motioning in short
strokes stimulates the mechanoceptors in the muscle below.
Application: multidirectional shifting of tissue w a foam roller (no vibration
req’d)
3. Agonist Strengthening: also known as corrective exercise is designed to
slowly increase gamma & alpha motor recruitment (i.e. increased firing
frequency and motor unit recruitment). By strengthening a weak
movement pattern, you both inhibit overactive and activate underactive
muscles. Remember it’s the execution of an exercise, not the exercise
itself that creates activation and therefore joint alignment.

How to muscle activate via corrective exercise & movement: • Manage
• Posture / alignment
• ROM
• Speed of Motion (SOM)
• Complexity
• Load of Motion (LOM)
• Fatigue of Motion (FOM)
• Minimal shaking or spasm
• Use low threshold / slow twitch training methods before high
threshold (i.e. LOM & SOM)
• Do not go to the point of pain (i.e. pain free ROM)
• All Core Activation movements should progress from floor to the
specific actions required to function in life sport or workout.
Corrective Exercise Training Guidelines & Reminders
Motor Learning Process is a step-by-step process in which we can integrate vibratory and taping procedures to reinforce the learning process
End goal is to create permanent lasting functional movement free of dysfunction for our specific body
Biomechanics are as individual Create movement symmetry and therefore joint stability Level the pelvis (i.e. bridge, side plank, plank) Core neutral is the foundation from which strong movement is created.
Learn to ACTivate your local, global & movement core musculature Time your core bracing and forced exhalation with maximal force
requirement. This will help create spinal & pelvic stability. Take a 360’ / muscle balanced approach to training and preparation. Manage movement & the killers of function (speed, ROM, intensity,
complexity & volume) The optimal activation sequence is:
a. WBV (not shown) + SMR (pin & move) + MSV = 3-5 min each https://youtu.be/gIInxp70OJY
b. Core Activation / Active Isolated/ End Range of Motion = 5 min c. Dynamic Warm-up = 5 min https://youtu.be/LGrd2oNLFHk


Straight Leg Raise P2P Assessment: Active Passive ROM
Difference
Step 1. Assess active & passive Pelvic Stability & Hamstring ROM & determine
which ft is lowest. Give that side preferential treatment.
Step 2. If there is difference between active & passive ROM, apply vibration
Step 3. Reassess ROM. If no difference after Activation try an inhibitory SMR,
non-vibratory protocol (see previous table)
Step 1. Asses
Active: Pre MSV
Step 2. MSV Origin & Insertion Activation
Step 3. Reassess

No Active Passive ROM Difference: Use Pin & Move Protocol
Assess Pelvic
Stability &
Hamstring ROM
If no difference in
active & passive
ROM, apply non-
vibratory,
inhibitory SMR
1. Calves
2. Low
Hamstrings
SMR bottom & top
of long muscles
Each position is
held w subtle slow
movements,
typically assisted
by trainier
Reassess ROM
If no difference
after SMR, try the
stabilization /
activation protocol

Shoulder Abduction & Retraction Assessment
Step 1. Assess Shoulder Stability & Pec ROM
Step 2. If there is a difference in active & passive ROM, apply vibratory Activation
to the weak muscle / unstable joint
Step 3. Reassess ROM: If no difference after activation, try an inhibitory SMR,
non-vibratory protocol for pec major, minor & lats
o DZ = Low Trap & Rhomboid (MSV) o DZ = Plank + Side Plank + Back Hollow o No DZ = Mobilize Pecs & Lats (Ant Humerus)
Step 1.
Active: Pre MSV
Step 2.
Step 3. Active: Post MSV

Corrective Pin & Move
Step 1. Assess ROM
Step 2. No Active Passive
Difference
Step 3. Move along tissue at
parallel to line of pull of tissue
until sensitive or hard tissue is
found
Step 4. Melt into tissue at a 5-7
threshold & perform 2-3
diaphramatic breaths
Step 5. Perform programming 4-
6 slowly executed reps of the
listed movements
Step 6. Reassess ROM
Images: ©Trigger Point Therapy

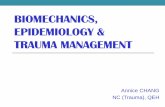
Myofascial Lines Superficial Back
Line (SBL)
• Flexor digitorum
• Brevis
• Gastrocnemius
• Hamstrings
• Sacrotuberous
ligament
• Erector spinae
• Scalp fascia
Superficial Front Line
(SFL)
• Extensor
digitorum—
longus and brevis
• Tibialis anterior
• Patellar tendon
• Quadriceps
(including the
rectus femoris)
• Rectus
abdominis
• Sternalis
• Sternocleidomast
oid
Lateral Line (LL)
• Peroneus longus
and brevis
• Anterior ligament of
the fibular head
• IT band, TFL, glute
max
• Lateral abdominal
• External and
internal intercostals
• Splenius capitis
and
sternocleidomastoi
Front & Back Arm Lines
Stock Imagary: © istockphoto.com
Medical images © Fitness Professionals

Fascial Integration: Assessment Superficial Back Line (SBL) Assess (ROM) Toe Touch & Straight Leg Raise
Assess (My) Glute Max Sagittal
P2P (Sp) PLantar Fascia
P2P Hamstrings
(V) TLF / Low Back Si2Si Knee Drops
(Sp / V) Rec Femoris
Link: https://youtu.be/Rndv7Rh92G4 Link: https://youtu.be/kgadNRE2_Yg
Movement: Chin Tucks (M)
Movement: MR Prone Cobra (S)
Movement: Down Dog (M) Movement: Assisted Bridge (S)
Notes:

Fascial Integration: Superficial Front Line (SFL) Assess (ROM) Modified Thomas Test
Assess (My) Rectus Femoris
P2P (Sp / V) Tibialis Anterior
NB* See Rec Fem in SBL
P2P (V) High Quad Pin & Move
(V) TFL
(Sp) 2 way Hip Extension
Link: https://youtu.be/xH-3bfrZYw4
Link: https://youtu.be/ua3PnM8wx2E
Movement: Prone Cobra (M)
Movement: Assisted Bridge (S)
Notes:

Fascial Integration: Lateral Line Assess (ROM) Kneeling Side Bend
(My) Glute Med (posterior fibers)
P2P (Sp) QL’s
P2P (Sp / V) Adductors
(V) IT Band / Lateral Thigh
Link: https://youtu.be/X1utzRrkk3Y Link: https://youtu.be/GD_jVt847RQ
Movement: 10 & 2 Child’s Pose Side Bend (M)
Movement: Hinging Kneeling Side Plank (S)
Notes:

Exercise Library / Protocol Exercise Library / Protocol Upper Pin & Move
• Lats + Sweeps & Back Scratch
• QL + Side Bends
• Psoas + Back Ext + Leg Ext
• Traps / Neck + 3D (no vibration)
Lower Pin & Move
• Plantar Fascia Roll & Twist
• IT / Lat Thigh + Ham Curl
• Piriformis + Hip Flexion + Clam
• Quad + Ham Curl

REFERENCES Pamukoff DN, Ryan ED, Blackburn JT. The acute effects of local muscle vibration frequency on peak torque, rate of torque development, and EMG activity. J Electromyogr Kinesiol 24: 888–894, 2014. The acute effects of local muscle vibration frequency on peak torque, rate of torque development, and EMG activity.
Whole Body and Local Muscle Vibration Reduce Artificially Induced Quadriceps Arthrogenic Inhibition Pamukoff, D. et al. (2016). Whole-Body and Local Muscle Vibration Immediately Improve Quadriceps Function in Individuals With Anterior Cruciate Ligament Reconstruction, Physical Medicine & Rehabilitation, Volume 97, Issue 7, Pages 1121–1129. Acute Effect of Whole-Body Vibration Warm-up on Footspeed Quickness Donahue, Ryan B.; Vingren, Jakob L.; Duplanty, Anthony A.; More Journal of Strength & Conditioning Research. 30(8):2286-2291, August 2016.
Contact Information:
Chad Benson 778-999-8586 [email protected] Instagram @prepair2perform
Gareth Bryson 604-798-0100 [email protected] Instagram @primalfreak
Product Information: Bands – Loops – Tubing: https://www.360conditioning.com/fitness-conditioning/training-and-toning/resistance-bands-en.html Hyperice: https://www.360conditioning.com/fitness-conditioning/shop-by-brand/hyperice.html