Preliminary care in maxillofacial injuries
61
PRELIMINARY CARE IN MAXILLOFACIAL INJURIES Presented by - Dr. SHEETAL KAPSE Moderator - Dr. RAJASEKHAR G .
-
Upload
sheetal-kapse -
Category
Health & Medicine
-
view
395 -
download
2
Transcript of Preliminary care in maxillofacial injuries

PRELIMINARY CARE IN
MAXILLOFACIAL INJURIES
Presented by -
Dr. SHEETAL
KAPSE
Moderator -
Dr. RAJASEKHAR
G.

INCLUSIONS
Introduction
Aim of trauma care
Pre hospital care
Triage
Initial assessment of the patient
Primary survey and resuscitation
ABCDE
BLS
Basic airway maneuvers
Advanced airway maneuvers
Surgical airway
Breathing and ventilation
Circulation and haemorrhage
Recognition of shock and management
Maxillofacial aspects
Exposure and environmental control
Primary survey
Secondary survey
Physical examination
Conclusion
References

Maxillofacial trauma- injury facial soft tissue or its
bony structure.
Commonly associated with multiple system
injuries.
Most common mechanisms of injury -blunt or
crush injuries caused by RTA or assault.
These injuries include cranial, spinal, Upper
and lower body injuries.
3
INTRODUCTION
• Leading cause of death from
birth to 44 yrs of age
1st
cancer
2nd
atherosclerosis
3rd
trauma

Identification of major trauma pts at the scene of the incident
Immediate intervention for safe transport
Rapid transfer to trauma centre for surgical management and critical care
Coordinated specialist reconstruction
Targeted comprehensive rehabilitation
AIM FOR TRAUMA MANAGEMENT

Trauma care continuum
Arrival of emergency
services
Transfer to hosp RR
RR management
Definitive care
Discharge
Long-term support
services
TraumaRR = resuscitation room

To identify & deliver pt to a place of a definitive care
safely & quickly
Ambulances are well equipped
Air ambulance facilities
Ambulance crew- paramedics
PRE HOSPITAL CARE

Triage is the sorting of patients based on their need
for treatment and the available resources to provide
the treatment
Starts at the accident scene itself
2 types
- Multiple casualties
- Mass casualties
TRIAGE
When the number of patients and the severity of
their
injuries do not exceed the ability of the facility to
provide
care.The situation in which the number of patients
and the severity of their injuries exceed the
capability of the facility and the staff.

If the number of trauma victims
exceeds the ability of the hospital to
handle them, a major incident is called,
and a pre-prepared and practiced
action plan is implemented whereby
neighbouring hospitals are alerted and
warned that they will also be receiving
patients.
PREPARATION AT THE RECIEVING HOSPITAL
All members should have
appropriate training, such as the
Advanced Trauma Life Support
(ATLS) course, which has become
the gold standard and common
language of trauma management.
Rescuer safety measures should be
followed.
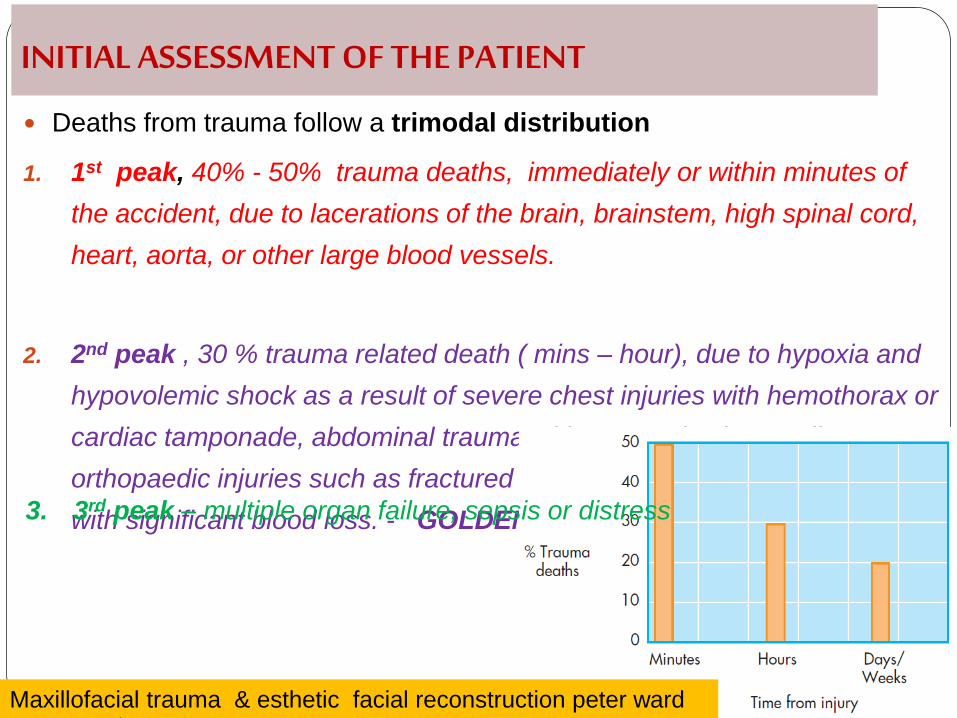
Deaths from trauma follow a trimodal distribution
1. 1st peak, 40% - 50% trauma deaths, immediately or within minutes of
the accident, due to lacerations of the brain, brainstem, high spinal cord,
heart, aorta, or other large blood vessels.
2. 2nd peak , 30 % trauma related death ( mins – hour), due to hypoxia and
hypovolemic shock as a result of severe chest injuries with hemothorax or
cardiac tamponade, abdominal trauma with ruptured spleen or liver, or
orthopaedic injuries such as fractured pelvis or long bones associated
with significant blood loss. - GOLDEN HOUR
INITIAL ASSESSMENT OF THE PATIENT
Maxillofacial trauma & esthetic facial reconstruction peter ward
booth , 11th ed
3. 3rd peak – multiple organ failure, sepsis or distress

Maxillofacial trauma &
esthetic facial reconstruction
peter ward booth , 11th
edition
INITIAL ASSESSMENT

BLS
Basic Life Support

General considerations
Adult chain of survival
Pediatric chain of survival
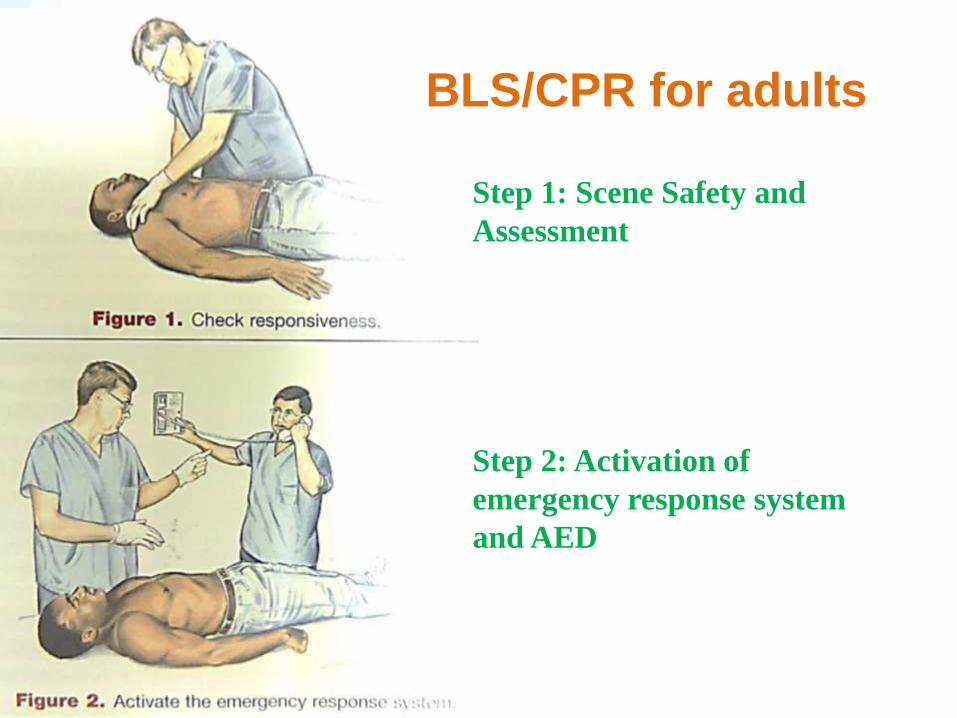
Step 1: Scene Safety and
Assessment
Step 2: Activation of
emergency response system
and AED
BLS/CPR for adults
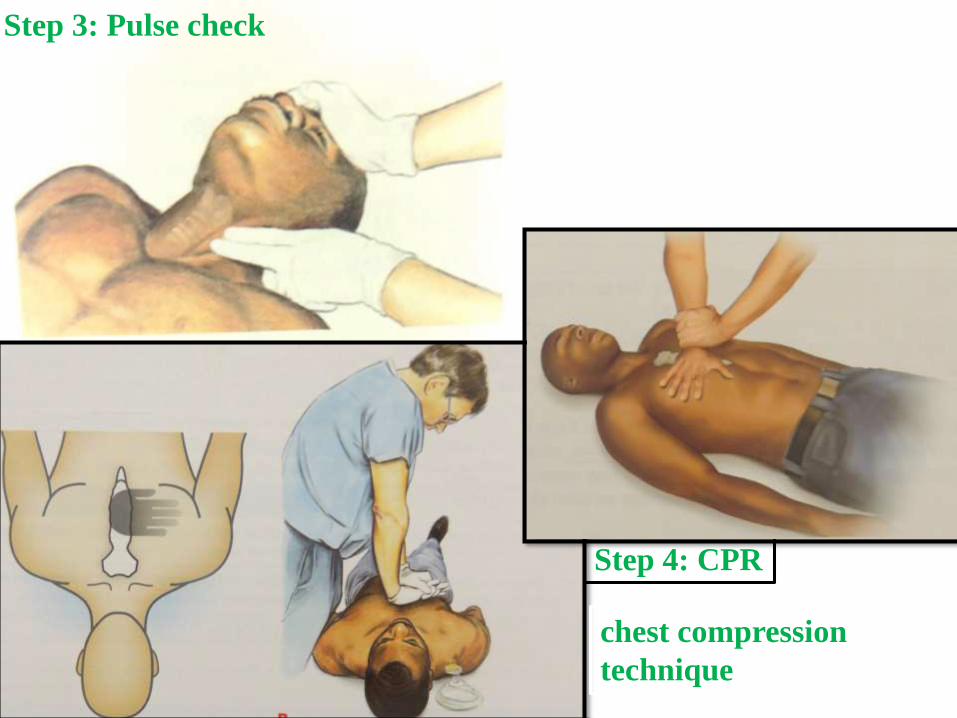
Step 3: Pulse check
Step 4: CPR
chest compression
technique

Step 4: CPR
opening the airway for breaths : head tilt chin lift
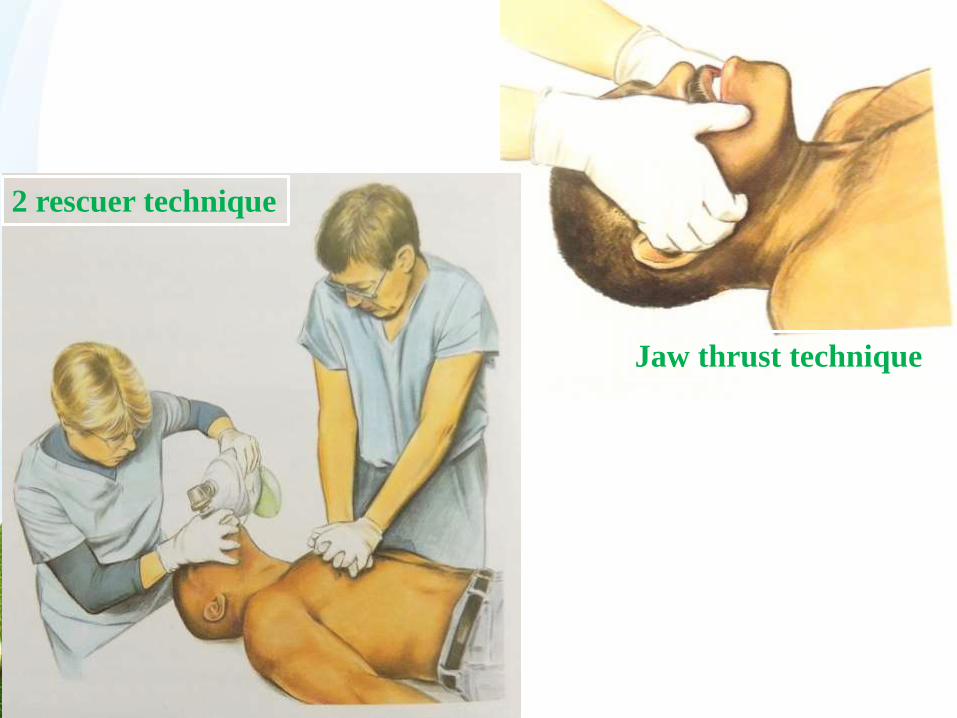
Jaw thrust technique
2 rescuer technique

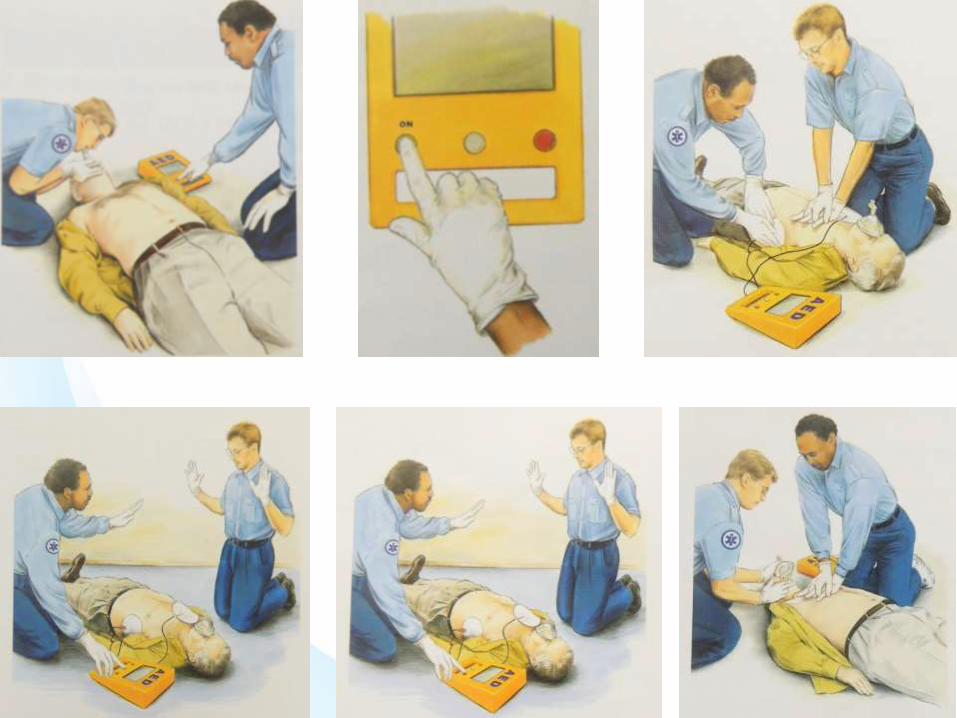
AED for adults and children > 8 years
1. Power on
2. Attach
3. Clear & Analyze
4. Shock if advisable
5. Immediately resume CPR
6. Reanalyze after 2 min (5 cycles of CPR)



BLS/CPR for children 1 year to puberty
BLS/CPR for infants
• Compression rate and ratio for lone rescuer
• Compression rate and ratio for two rescuer
• Compression depth
• Compression technique
• When to activate the emergency response
system

BLS/CPR for children 1 year to
puberty
• Location of pulse check
• Compression rate and ratio for lone rescuer
• Compression rate and ratio for two rescuer
• Compression depth
• Compression technique
• When to activate the emergency response
system

AED for infants and children from 1-8
years


Mouth to mouth breaths
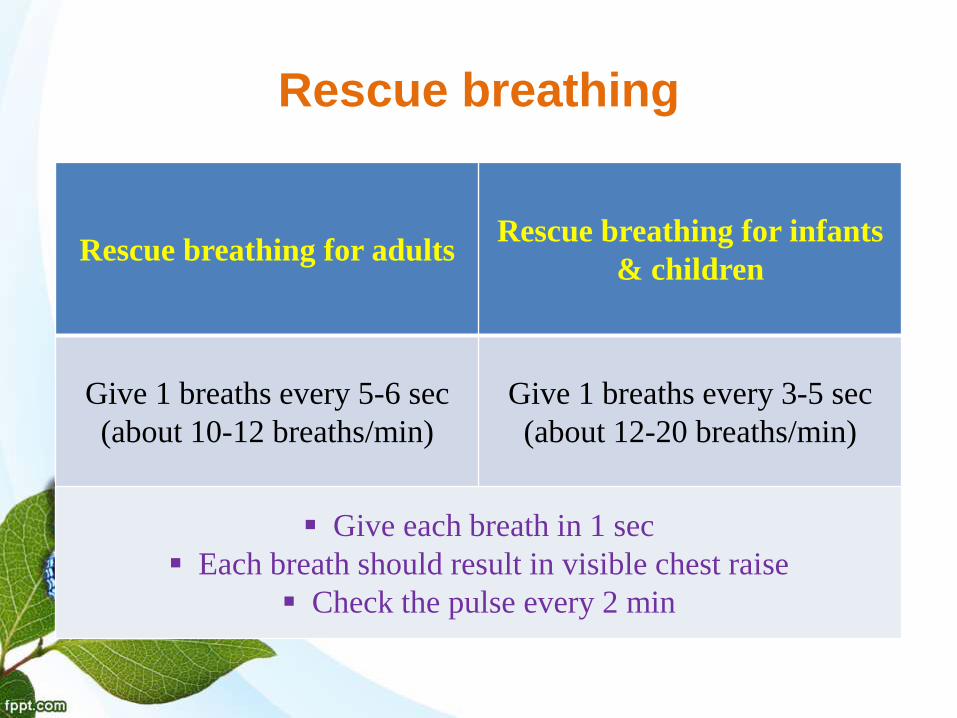
Rescue breathing
Pulse Breaths
Rescue breathing for adultsRescue breathing for infants
& children
Give 1 breaths every 5-6 sec
(about 10-12 breaths/min)
Give 1 breaths every 3-5 sec
(about 12-20 breaths/min)
Give each breath in 1 sec
Each breath should result in visible chest raise
Check the pulse every 2 min

Mechanisms of Injury
and
Suspected
Injury Patterns

SEQUENCE OF
MANAGEMMENTTrauma (Road traffic accident fall etc.)
↓
Primary Survey -> ABCDE defines
the specific prioritized evaluations and intervention that should be followed in all injured patients
↓
Secondary Survey
After initial survey has been accomplished and the patient has been stabilized
Involves more time – consuming tests and observations
Does not begin until primary survey is completed
9

A B C D E
A: Airway with cervical spine control
B: Breathing and Ventilation
C:circulation and haemorrhage control
D:Disability – (neurological status)
E: Exposure + environment – completely undress
the patient
F: Frequent Reassessment must be made

A: Airway with Cervical Spine
Control
High index of suspicion for cervical
spine injury in maxillofacial traumas
and multisystem trauma
15% of supraclavicular injury pt
5 % of head injury pt
spinal injuries most commonly
occur in the cervical region

Cervical spine assessment

Basic Airway Maneuvers
Supplemental oxygen
Look, Listen,and Feel.
jaw thrust
chin lift
Oro/ nasopharyngeal
airway

nasopharyngeal airway
Supplemental oxygen
Supplemental oxygen delivered through a well-
fitted reservoir (rebreathing) mask, at a rate of 15
L/min
LOOK LISTEN FEEL

JAW THRUST AND CHIN LIFT

Maxillofacial Injuries
• Up to 5% of patients presenting to
the emergency department have
facial injuries, and some may have
airway compromise.
• Maxillofacial trauma demands
aggressive airway management, and
it may be appropriate for the
maxillofacial surgeon to assist the
anesthetist in assessing and
securing the airway
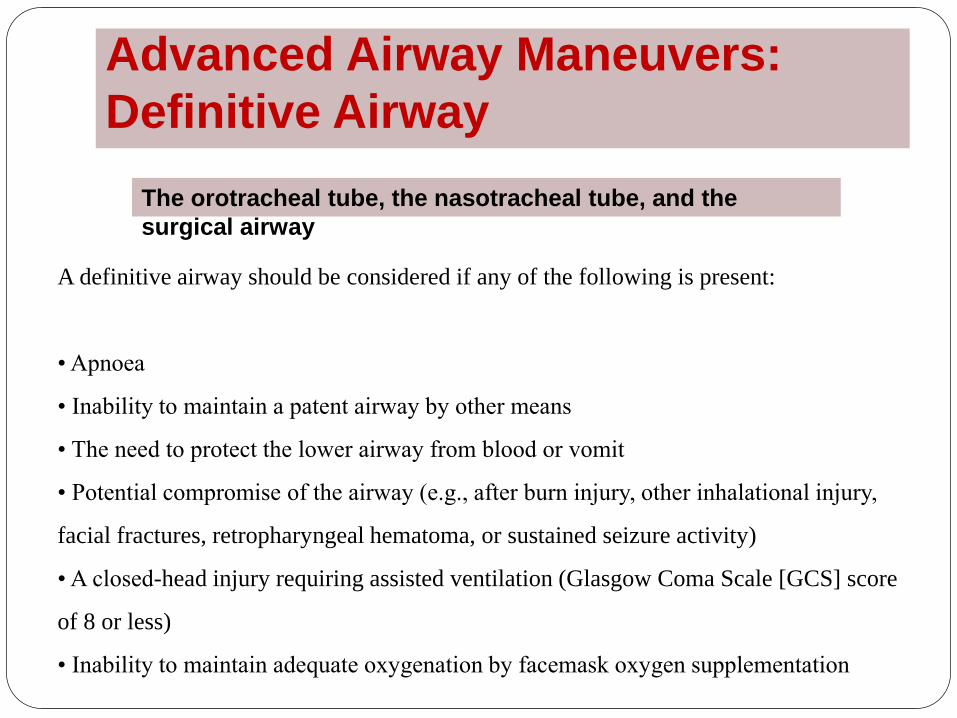
Advanced Airway Maneuvers:
Definitive Airway
The orotracheal tube, the nasotracheal tube, and the
surgical airway
A definitive airway should be considered if any of the following is present:
• Apnoea
• Inability to maintain a patent airway by other means
• The need to protect the lower airway from blood or vomit
• Potential compromise of the airway (e.g., after burn injury, other inhalational injury,
facial fractures, retropharyngeal hematoma, or sustained seizure activity)
• A closed-head injury requiring assisted ventilation (Glasgow Coma Scale [GCS] score
of 8 or less)
• Inability to maintain adequate oxygenation by facemask oxygen supplementation

Orotracheal Intubation
A size 8 tube is
usually suitable
for women and
a size 9 tube for
men

Nasotracheal Intubation

Surgical Airway
Inability to intubate the trachea orally or nasally is a clear indication for creation of a
surgical airway
tracheostomyNeedle
cricothyroidotomy
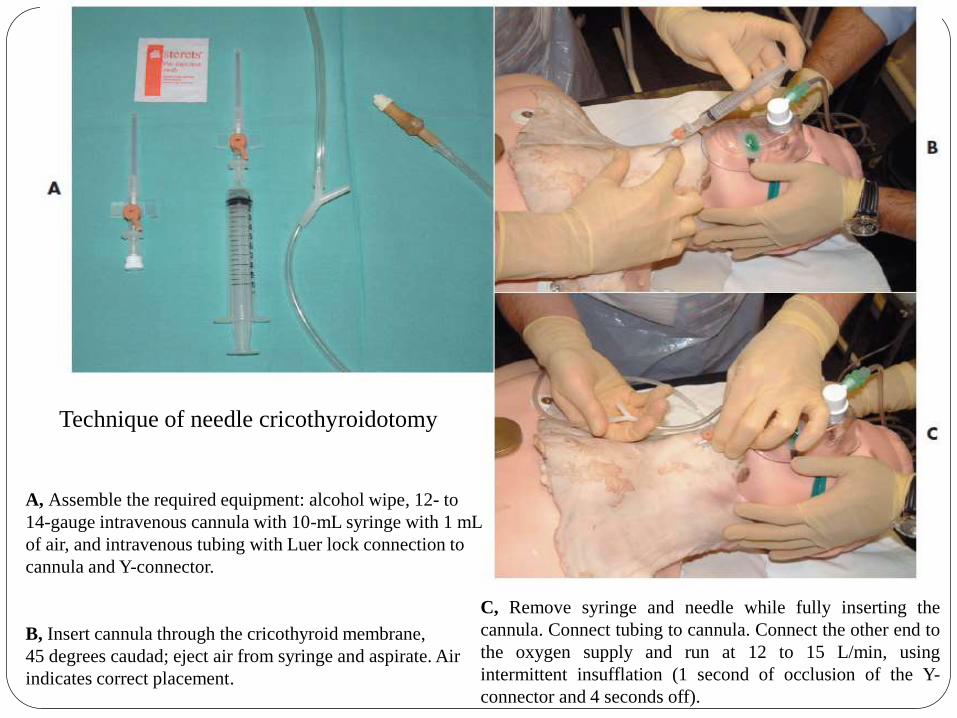
A, Assemble the required equipment: alcohol wipe, 12- to
14-gauge intravenous cannula with 10-mL syringe with 1 mL
of air, and intravenous tubing with Luer lock connection to
cannula and Y-connector.
B, Insert cannula through the cricothyroid membrane,
45 degrees caudad; eject air from syringe and aspirate. Air
indicates correct placement.
C, Remove syringe and needle while fully inserting the
cannula. Connect tubing to cannula. Connect the other end to
the oxygen supply and run at 12 to 15 L/min, using
intermittent insufflation (1 second of occlusion of the Y-
connector and 4 seconds off).
Technique of needle cricothyroidotomy

Technique of surgical
cricothyroidotomy
A, Assemble the required equipment:
local anesthetic with lidocaine
(lignocaine) and epinephrine
(adrenaline) for both anesthesia and
vasoconstriction.
B, Secure in-line immobilization of the
patient’s head by an assistant. Make a
3-cm horizontal incision through skin
over cricothyroid membrane (having first
removed the cannula if needle
cricothyroidotomy was performed).
C, Stab vertically down through
membrane and make a
1-cm incision.
D, Insert tracheal dilator horizontally
and open it, separating the thyroid and
cricoid cartilages. Suck out the
trachea with a Yankeur-type sucker.
E, Having checked that the cuff inflates,
insert the tracheostomy tube into the
trachea.
F, Remove the introducer, inflate the
cuff, and connect oxygen supply via
Ambu bag. Reassess and monitor O2
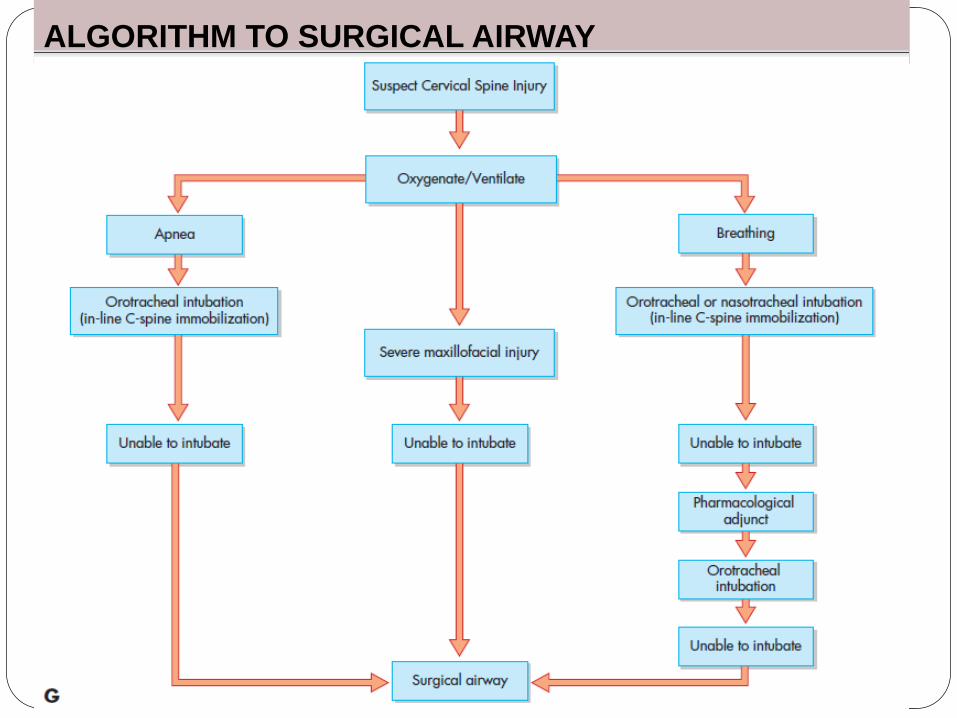
ALGORITHM TO SURGICAL AIRWAY

BREATHING & VENTILATION
Once the airway has been secured, breathing and
ventilation must be assessed.
THORACIC INJURIES
A: Airway obstruction
T: Tension pneumothorax
O: Open pneumothorax
M: Massive haemothorax
F: Flail chest
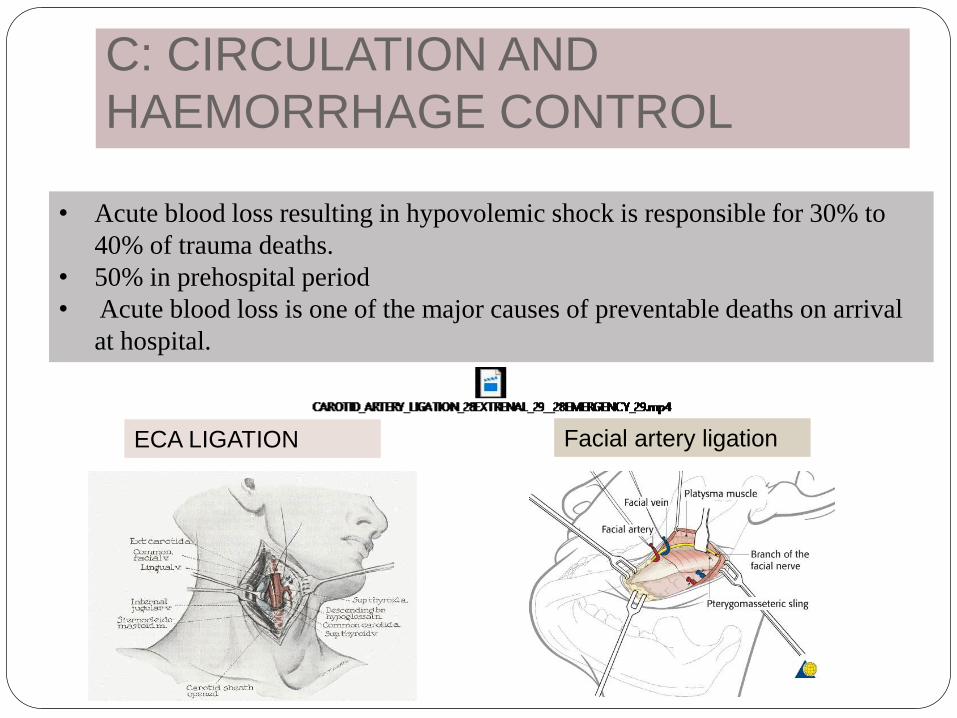
C: CIRCULATION AND
HAEMORRHAGE CONTROL
• Acute blood loss resulting in hypovolemic shock is responsible for 30% to
40% of trauma deaths.
• 50% in prehospital period
• Acute blood loss is one of the major causes of preventable deaths on arrival
at hospital.
ECA LIGATION Facial artery ligation

SHOCK
Metabolic acidosis
Hypothermia
Hypocoagulopathy
Recognition of shock
Tachycardia
Skin colour
Level of consciousness
Respiratory rate
Urine output


AMERICAN COLLEGE OF SURGEONS (2001),
Classification of acute hemorrhage
Committee on Trauma. Advanced Trauma Life Support Student
manual. 6th ed. Chicago. American College of Surgeons. 2001: 87-107.

Initial management of haemorrhagic shock
External
bleeding
Occult bleeding
The twin goals in resuscitation of the shock patient are prevention
of further blood loss and the earliest restoration of tissue perfusion
Posterior nasal pack
Packing using foley’s

FLUID REPLACEMENT
In a shocked, hypotensive patient, the aim of fluid resuscitation should be to
restore critical organ perfusion until hemorrhage that is amenable to surgery is
stemmed.
• Responders
• Lost < 20% blood vol
• Respond well & return to
normalcy
• Transient Responders
• Vitals initially improve but
then deteriorate
• They are actively bleeding
from open or occult site
• Non Responders
• vitals don't improve
• Rate of blood loss = fluid being
replaced
• Central venous line should be
established
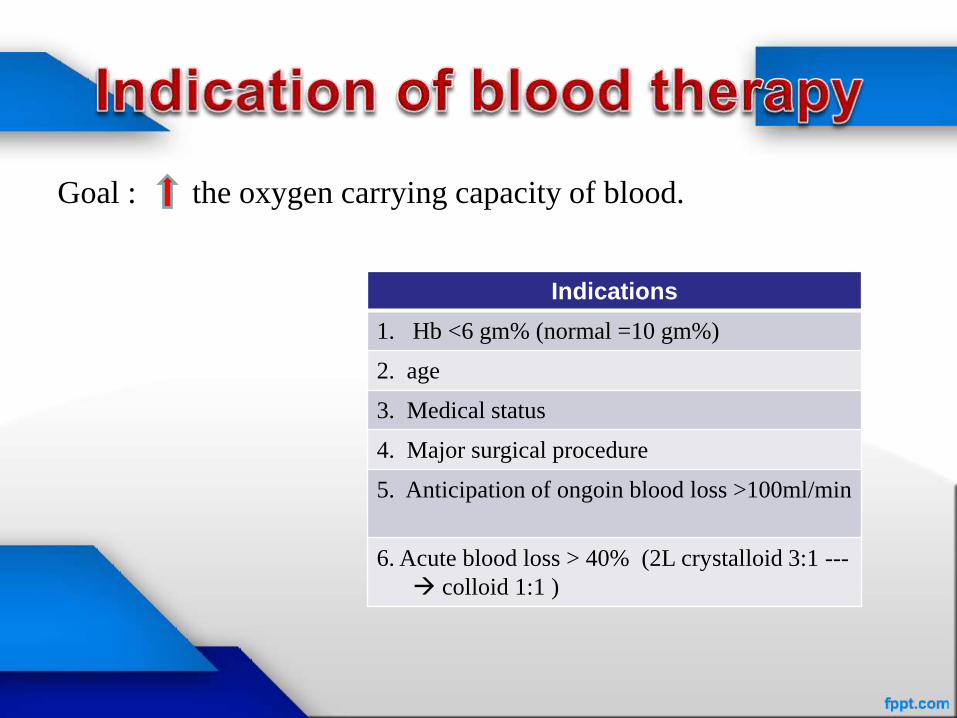
Goal : the oxygen carrying capacity of blood.
Indications
1. Hb <6 gm% (normal =10 gm%)
2. age
3. Medical status
4. Major surgical procedure
5. Anticipation of ongoin blood loss >100ml/min
6. Acute blood loss > 40% (2L crystalloid 3:1 ---
colloid 1:1 )

D : Disability
A rapid evaluation is performed at the end of the
primary survey, and this establishes the patient’s
level of consciousness.
A: Alert
V: responds to Vocal stimuli
P: responds to Painful
stimuli
U: Unresponsive to all
stimuli

E: EXPOSURE &
ENVIRONMENTAL CONTROL

SECONDARY SURVEY
It aims to identify and fully appreciate all other injuries that the
polytraumatized patient may have suffered that might otherwise go
unnoticed, particularly in the presence of a reduced GCS score.
History

Physical examination
SCALP
EYES
MAXILLOFACIAL
STRUCTURES
NECK AND CERVICAL SPINE
CHEST
ABDOMEN
PERINEUM, RECTUM , VAGINA
MUSCULOSKELETAL
ASSESSMENT
SPINAL CORD ASSESSMENT

Eyes
1. Direct injury to the globe (blunt or
penetrating injury)
2. Direct injury to the optic nerve (due to crush
or transection via bony injury at the orbital
apex)
3. Indirect injury to the optic nerve (from
deceleration or shearing force)
4. Critical reduction in tissue perfusion, either
generalized or local (systemic hypotension or
orbital compartment syndrome)

Maxillofacial Structures
• Examine the nose for deformity, pain, mobility, and difficulty in breathing,
which suggest bony or cartilaginous fractures.
• Epistaxis and, in particular, CSF rhinorrhoea suggests an anterior cranial
fossa fracture at the cranial base, the ears for hemotympanum and CSF
otorrhea.
• Bleeding from the external auditory canal soft tissue wall may be
secondary to mandibular condylar fracture with or without glenoid fossa
injury
• Lastly, examination of the mouth is performed. Buccal vestibule(zygoma),
the palate (maxilla), and the floor of the mouth(anterior mandible) is noted
CONCLUSION
As maxillofacial surgeons we are trained to
attend head and neck emergency situations in
the casualty. One should have thorough
knowledge about various protocols to manage a
trauma patient. And should attend BLS & ATLS
courses at regular intervals.

REFERENCES
Peter Ward Booth, Barry L. Eppley, Rainer Schmelzeisen. Maxillofacial Trauma and Esthetic Facial
Reconstruction. Churchill Livingstone, 2003 , 11th edition.
Oral and Maxillofacial Trauma, Volume 2. Raymond J. Fonseca,Robert V. Walker Snippet view - 1991 .
WILLIAMS, J. L., & ROWE, N. L. (1994). Rowe and Williams' maxillofacial injuries. Edinburgh, Churchill Livingstone.
Williams NS, Bullstrode CJ, O’connell PR. Bailey & Love’s short practice of surgery, 25th edn. Annals of the royal college of surgeons of england. 2010;92(2):178. Doi:10.1308/003588410x12628812459094.
Resuscitative strategies in traumatic hemorrhagic shock , bouglé et al. Annals of intensive care 2013, 3:1
Committee on trauma. Advanced trauma life support student manual. 6th ed. Chicago. American college of surgeons. 2001: 87-107.